-
7/26/2019 Dm Ulkus Jurnal
1/14
Open access publishingThe Journal of Diabetic Foot
Complications
Role of combination cell therapy in non-healing diabetic ulcers
in
patients with severe peripheral arterial disease a preliminary
report
on ve casesAuthors:
The Journal of Diabetic Foot Complications, 2013; Volume 5,
Issue 1, No. 1, Pages 1-14 All rights reserved.
Chandra Viswanathan1, Prathibha Shetty1, Shabari Sarang1,
Khushnuma Cooper1, Deepa Ghosh1,
Arun Bal2
Abstract:
Key words: Mesenchymal stem cells, Haematopoietic stem cells,
Combinational stem cell therapy,
Peripheral arterial disease
Corresponding author:
Dr. Chandra Viswanathan
Reliance Life Sciences Pvt Ltd,
Dhirubhai Ambani Life Sciences Centre,
R-282, TTC Area of MIDC,
Thane Belapur Road,
Rabale, Navi Mumbai- 400701.
Tel: +91-22-67678352; Fax: +91-22-67678099;
Email:[email protected]
Afliations:
1. Regenerative Medicine Group, Reliance life Sciences Pvt
Ltd,
Dhirubhai Ambani Life Sciences Centre, R-282 TTC area of MIDC,
Thane
Belapur Road, Rabale, Navi Mumbai-400701.
2. Dhanvantari Hospital and Research Center, D. L. Vaidya Road,
Shivaji
Park, Dadar (West), Mumbai-400028.
1
Background:Peripheral arterial disease (PAD) is a growing
medical problem and its management can be
a clinical challenge. Complications like non-healing ulcers are
more challenging. Despite recent advances
in surgical and radiologic procedures, a large number of
patients are not eligible for revascularization
procedures. In many such cases, amputation becomes inevitable.
Recent evidences indicate that adult stem
cells are potentially new therapeutic targets. The present
report is a summary of responses to combination
stem cell administration on 5 cases of PAD with non-healing
ulcers. This is the rst report, depicting the
usefulness of different adult stem cell type combination, to
address this unmet need.
Methods: Five patients with severe PAD and non-healing ulcers,
in whom amputation was the only option,were considered for this
short study. Here, we present short-term results of multiple
intramuscular injections of
mesenchymal stem cells from umbilical cord matrix (UCMSC) and
haematopoietic stem cells (HSCs, CD34+)
from the human umbilical cord blood, into the affected lower
limbs, while allogeneic neonatal broblasts
were directly applied on the non-healing foot ulcers, Ankle
brachial indices (ABI) were calculated before and
after the procedure, improvement in pain scores, wound closure,
and prevention of limb loss were taken as
indicators of success.
Results:An average improvement of 0.2 to 0.45 in ABI
measurements was noted, with no amputation of
the affected limb. Complete wound healing was achieved within
three months in all patients. No recurrence
of ulcer was evident during this period. One patient voluntarily
reported 14 months later, showing sustained
improvement. All patients demonstrated a decrease in the
severity of symptoms as evidenced by alleviation
of rest pains and improvement by at least one level in
Rutherford classication. There were also no adverse
events reported.
Conclusions: Thus, usefulness and effectiveness of this
combination therapy to prevent limb loss in patients
with severe PAD, and non healing ulcer was demonstrated. A large
multicenter study will be necessary to get
answers on the optimal dose, frequency and the ideal cell type
to be used.
-
7/26/2019 Dm Ulkus Jurnal
2/14
Open access publishingThe Journal of Diabetic Foot
Complications, 2013; Volume 5, Issue 1, No. 1, Pages 1-14
2
Peripheral arterial disease (PAD), arte-
riosclerosis obliterans and thromboangitis
commonly affect the arteries supplying blood
to the leg. It is one of the major manifestations
of systemic atherosclerosis affecting the lowerextremities and
often culminating in critical limb
ischemia (CLI). Based on the severity of the
symptoms, usually two clinical presentations
are distinguished: intermittent claudicating (IC),
which is characterized by pain upon walking
while CLI is a more severe form in which pain
occurs at rest and is accompanied by necrosis
and ulceration1. CLI is characterized by a more
than 50% risk of major amputation within one
year without revascularization
2
and a poorprognosis with regard to survival. A substantial
number of patients with CLI remain unresponsive
to pharmacological therapies and are also un-
suitable candidates for endovascular or surgical
revascularization3, 4, 5.
PAD is estimated to develop in 500-1000
individuals per million persons per year. Seventy
to eighty percent of affected individuals are
asymptomatic; only a minority ever requires
revascularization or amputation6. One in 3diabetics over the age
of 50 are affected by PAD.
Diagnosis is critical, as people with PAD have
a four to ve times higher risk of heart attack or
stroke. Despite its prevalence and cardiovascu-
lar risk implications, only 25% of patients with
PAD actually seek treatment. The incidence of
symptomatic PAD increases with age and as-
sociated risk factors, from about 0.3% per year
for men aged 4055 years to about 1% per year
for men aged over 75 years. As PAD progresses,
leg pains at rest and/or ischemic ulceration
are hallmark presentations. Treatments vary
from simple conservative lifestyle alterations to
complex invasive endovascular or open surgical
interventions in severe cases. Experience shows
that the end stage PAD is difcult to treat by tra-
ditional methods, leaving major limb amputation
as the only treatment option7.
The development of novel therapies to
stimulate neovascularization, a strategy known
as therapeutic angiogenic factors or recently
the use of stem cells, may represent an option
to promote revascularization and/or remodel-ing of collaterals,
with the aim of ameliorat-
ing symptoms, promoting the regeneration of
damaged tissues and preventing amputation8,9.
Mesenchymal stem cells (MSCs) have
dependable differentiating properties, and can
change the milieu that promotes and helps
regeneration10. The hematopoietic and mesen-
chymal cells secrete growth factors that promote
neoangiogenesis and endothelialization leadingto development of
collateral vascular networks11,
12, 13.
Our previously published studies on animal
models with ischemic limb disease [ILD] have
demonstrated that implantation of MSCs
improved tissue perfusion. MSCs signicantly
enhanced perfusion of ischemic tissue and
collateral remodeling, reduced tissue damage
and improved limb function14. A large number
of experiments in mice and larger animals havedemonstrated the
feasibility and efcacy of cells
both MSCs and HSCs in restoring blood ow to
the ischemic limb15, 16, 17 .
MSCs are also immunomodulatory in nature
and hence are very good candidates for re-
generative medicine applications even in the
allogeneic setting. Autologous stem cells have
several advantages; however limitations such
as bone marrow collection, patients age, stem
cell isolation, preparation, and the consequent
variations in quality and quantity cannot be
overlooked. To overcome these inconsistencies,
several groups, including ours have investigated
the use of an alternative source for deriving
MSCs that overcomes all the above shortcom-
ings and consider their usage in the allogeneic
mode. Mesenchymal stem cells derived from the
Introduction
-
7/26/2019 Dm Ulkus Jurnal
3/14
Open access publishingThe Journal of Diabetic Foot
Complications, 2013; Volume 5, Issue 1, No. 1, Pages 1-14
3
umbilical cord have distinct advantages be-
cause of their good growth kinetics, differen-
tiation potentials, banking ability, naivety and
immunomodulatory functions, as compared to
most other adult stem cell types18. Similarly,
CD34+ cells from ones own bone marrow
would have been desirable, but not feasible inall cases. This
limitation could be due to rea-
sons such as advancing age, debility, anemia
and infection that decrease bone marrow aspira-
tion opportunities. Hence both CD34+ cells and
MSCs from allogeneic sources are more desir-
able.
Fibroblasts derived from an allogeneic
source like the neonatal foreskin have been
extensively used in the regeneration of wounds.
Dermal broblasts of allogeneic origin do not
evoke an immune response, making it possible
to use allogeneic dermal broblasts as skin
substitutes19, 20. The lack of immune response
to allogeneic dermal broblasts has been attrib-
uted primarily to the absence of expression of
human leukocyte antigen (HLA)DR by the cells
and co-stimulatory molecules such as CD40 and
CD8021.
We have also previously reported that
the neonatal broblasts did not stimulate T-cellproliferation
even in the presence of Interferon
gamma (IFN-), thus indicating the safety of the
broblasts in wound treatment22.
This brief report elucidates the role of
allogeneic stem cell combination in improving
the ischemic condition in PAD patients, who
otherwise had no treatment option but amputa-
tion. Autologous cell based studies have shown
favorable results, most of them being MSCs from
the bone marrow. This report is based on using
the combination cell type consisting of MSCs and
CD34+ positive cells derived from nave source,
which have proven immunomodulatory behavior.
This study was aimed at evaluating
the usefulness of a combination of allogeneic
stem cells (UCMSC + CD34+) implantation in5 consecutive patients
with severe PAD with
an impending limb or a toe amputation; and to
evaluate the role of local application of neonatal
broblasts in the treatment of nonhealing ulcers.
Patient details:
At the time of commencement of this study,
all ve patients had received signicant medical
therapy for PAD, and were under the discretion
of the managing vascular surgeon. They wereincluded in the study
if they had severe limb-
threatening PAD, dened as ABI less than 0.5
with presence of non-healing ischemic ulcers.
They had documented stenosis or occlusion of
any two of the following lower extremity arteries:
anterior tibial, posterior tibial, and/or peroneal.
Additional stenosis or occlusion may be present
proximal to these vessels. They may or may not
have undergone peripheral vascular angioplas-
ties or bypasses as a part of therapy.
All the biological samples used for the study
were obtained with approval from the Institution-
al Ethics Committee and informed consent from
donors.
A) Umbilical cord mesenchymal stem cell
preparation
Mesenchymal stem cells were prepared
from the human umbilical cord matrix .The
cord matrix was serially cut in a cross sectionalmanner and 4 to
5 explants of the matrix
ranging from 1-2 cm in size were placed in 100
mm tissue culture dishes with 2-3 ml of culture
medium. Adherent MSCs were harvested and
characterized by ow cytometry as per the inter-
national standards and cryopreserved in liquid
nitrogen until further requirement23.
METHODS
-
7/26/2019 Dm Ulkus Jurnal
4/14
B) CD34+ cell preparation
The CD34+ cells were sorted from Mono-
nuclear cells (MNCs) using sterile magnetic
beads (Miltenyi Biotech, Germany) following
the manufacturers protocol. For every 100x106
cells, 100l of FcR blocking reagent was added
to the MNC pellet and resuspended in 300l of
MACS Buffer (1xPBS with 4% serum) and mixed
well. One-hundred l of CD34+ microbeads
were also added to the cell suspension and
was incubated at 40C for 30-40 minutes. The
cells were then resuspended in MACS buffer
and passed through the magnetic column. The
positive fraction of CD34+ cells was collected
by depletion strategy in a fresh sterile centrifuge
tube. The cells thus collected, were counted and
characterized before expansion to conrm theirpurity. The pure
population of CD34+ cells were
co-cultured with human mesenchymal stem cells
obtained from the human umbilical cord tissue
(UCMSCs) for a period of two weeks in Iscoves
Modied Dulbeccos Medium (IMDM) (Invitro-
gen, Singapore) with 10% Fetal Bovine Serum
(FBS) (Hyclone, USA), 10ng/ml SCF, 10ng/ml
Flt3, 10ng/ml TPO (Peprotech, USA) and 1ng/
ml bFGF (R&D systems, USA) with 1mM L-glu-
tamine (Invitrogen, Singapore)24. The expanded
CD34+ cells were then characterized by immu-nophenotyping for
purity and viability.
C) Neonatal Fibroblast preparation
Human dermal broblasts were isolated
from neonatal foreskin biopsies. The dermis
was separated from the epidermis by treatment
with Dispase (Sigma-Aldrich, St. Louis, MO).
The dermis was digested with 0.017% collage-
nase (Gibco, Grand Island, NY) in DulbeccosModied Eagles Medium
(DMEM) (SAFC Bio-
sciences, Lenexa, KS) with 10% Fetal FBS;
(Hyclone Labs, South Logan, UT) overnight. The
digested material was pelleted at 1000 rpm for
10 min, the pellet was resuspended in DMEM
10% FBS and then cells were allowed to attach
in a culture ask (Nunc, Roskilde, Denmark).
Cells were cultured in DMEM 10 % FBS at 37oC
in 5% CO2 and subcultured using 0.25% Tryp-
sin-EDTA solution (SAFC Biosciences).
The cell derivation and nal characteristics
in all the above cell types are compliant with the
international recommendations.
D) Stem cell dose and administration of stem
cell combination:
The total cell dose of UCMSCs and CD34+
cells was calculated at 2 million per kg body
weight, in the ratio of 80:20 respectively, to be
given intramuscular, along the travel path of the
vascular track approximately at 2-inch distances
as shown in Figure 1.
MSCs and CD34+ cells are transported in
dry ice at -80o C. These cells were mixed after
rapid thawing at 37oC and diluted in 24 ml of
saline. The surgeon was handed over loaded
syringes of stem cells for transplantation. Pre-
caution was taken to waste no time between
thawing, loading the syringe, and the injection
process.
Administration of stem cells:
Local skin preparation was done as per
routine procedure. The injection sites were
selected according to the angiographic ndings
to localize and understand the level of the
occlusion; Intramuscular injections were given
above and below this site. Thus approximately
Figure 1- The points of injection marked above and
below the block along the vascular track
4
Open access publishingThe Journal of Diabetic Foot
Complications, 2013; Volume 5, Issue 1, No. 1, Pages 1-14
-
7/26/2019 Dm Ulkus Jurnal
5/14
1 to 1.5 ml of cell volume was injected per site,
and about 10 sites at a distance of 2-3 inches
from each other. Marking was done ahead of
time to help expedite the procedure. The intra-
muscular (IM) injection thus was made into the
calf muscles (soleus and gastrocnemius) and the
popliteal fossa along the path of the blood owas shown in Figure
1. The cells were delivered
intramuscularly into the ischemic limb using 25G
needle in all cases, except in one case where it
was administered using a blunt lumbar puncture
needle to help with better cell dispersion.
Light pressure was applied after every IM
injection to ensure that the cells were dispersed
well into the tissues. All procedures were
performed by the treating senior surgeon.
For broblast implantation, the surface of the
wound bed was debrided. The broblasts were
suspended in saline adequate to inject 0.1 ml at
multiple sites along the ulcer bed and the walls.
The wound was then covered with ReliHeal-G,
a hydrogel dressing (Reliance Life Sciences,
India).
The gel was secured using Tegaderm (3M Health
Sciences, USA). The dressing was changed at
regular intervals of 1, 4, 8 and 12 weeks until
complete wound closure.
Safety and efcacy parameters post
transplantation:
Success following cell implantation was
dened as fulllment of at least three of the
following four criteria:
1. Improvement of ABI measurements
2. Healing and decrease in the ulcer size (clas-
sied as per the Wagner classication, (Table 1)
and appearance of fresh granulation tissue
3. Minimum of a one grade improvement in Ruth-
erford classication (Table 2)
4. Prevention of major limb amputations at the
three month follow up
This short study had three female and
two male patients. The mean age of this group
was 66.5 years. None of them were smokers.
Four of them were diabetic for at least 15 years
(Patient1, 2, 4 & 5) and one female patient
(Patient 3) was not diabetic (Figure 2). Three
of them were on dialysis for at least 2 years
and two of them were not. Four had rest pain
and varying sizes of non-healing ulcers prior to
being included into our study, and one female
patient had an impending ulcer on the foot, with
gangrene setting in on the great toe (Patient 4).
(Table 3 and Table 4)
5
Table 1: WAGNER CLASSIFICATION OF DIABETIC
FOOT ULCERS
Table 2: The Rutherford classication for ischemic
limb
Grade Conditions
0 No ulcer in a high risk foot
I Supercial ulcer involving the full skin thickness
but not underlying tissues
II Deep ulcer, penetrating down to ligaments and
muscle, but no bone involvement or abscess formation
III Deep ulcer with cellulitis or abscess formation, often
with osteomyelitis
IV Localized gangrene
V Extensive gangrene involving the whole foot
Stages Conditions
0 Asymptomatic
1 Mild claudication
2 Moderate claudication The distance that delineates
mild, moderate and severe claudication is not specied
in the Rutherford classication, but is mentioned in the
Fontaine classication as 200 meters.
3 Severe claudication
4 Rest pain
5 Ischemic ulceration not exceeding ulcer of
the digits of the foot
6 Severe ischemic ulcers or frank gangrene
RESULTS
Open access publishingThe Journal of Diabetic Foot
Complications, 2013; Volume 5, Issue 1, No. 1, Pages 1-14
-
7/26/2019 Dm Ulkus Jurnal
6/14
Patient
NumberAge and Gender (years) Grade of ulcer Conditions
1 70/F I 5
2 58/F II 4
3 75/M III 4
4 75/M III 5
5 65/M III 5
Patient
Number
Cerebrovascular
eventsCAD, RAD
Other risk
factorsHTN
Hypercholesterolae-
mia, hyperlipidaemia
Prior vascular
procedures,
Major procedures
Open endovascular
1 Old history of Transient
ischemic attack (TIA)
CAD, RAD Non Smoker,
Diabetic
Y Present Yes No
2 Absent On dialysis non Diabetic,
Non Smoker
Y Present Yes No
3 Old Cerebrovascular
accident (CVA), H/O
transient ischemia
CABG
(1 year) Non Smoker,
Diabetic
Y Present Yes, plasty
on the cur-
rent leg
By pass
done, on the
other leg
4 Ejection fraction-19%,
lacunar infarcts
Absent Diabetic ,non
smoker
Y Present Plasty ad-
vised,
None
5 No history On dialysis,
hyperbaric O2
for non healing
ulcers
Non Smoker,
Diabetic
Y Present Present Vascular
bypass
done, plasty
performed
on one leg
Table 3: Clinical details about
the patients pretreatment
Table 4: Co-morbidities and prior vascular procedures in the
patients
CAD (Coronary artery disease), RAD (Renal artery disease), HTN
(hypertension)
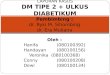
A:Great toe showing marked discoloration, swelling, edema.B:
Same toe after three months of stem cell
injection showing no further deterioration and there is a marked
decrease in swelling and discoloration.
CDE: Left sole of the heel showing an impending ulcer; The heel
area also shows varying grades of
discoloration. F: Three months post stem cell transplant, heel
showing near normal foot with no swelling, or
ulcer formation.
Figure 2: Patient 1
6
Open access publishingThe Journal of Diabetic Foot
Complications, 2013; Volume 5, Issue 1, No. 1, Pages 1-14
-
7/26/2019 Dm Ulkus Jurnal
7/14
Ulcers were present in three of them and
one female patient had an impending gangrene
of the great toe with a large impending ulcer on
the other foot (Figure 2). Co-morbidities and
prior vascular procedures are listed on a per-
patient basis in Table 4. Both the male patients
had previous endovascular procedures. Allpatients had
hypertension, and diabetes was
present in four of the 5 for over 15 years. All
patients with diabetes were insulin dependent.
One female patient who was non-diabetic
showed a complete improvement of the wound
within three months post stem cell treatment.
The improvement involved good wound closure
on the plantar side accompanied by granulation
(Figure 3). The oldest patient had undergone
coronary bypass surgery, had old cerebrovascu-
lar episode, and was on dialysis for over a year.
Two of the patients had undergone peripheral
angioplasty on the same extremity under discus-sion, and
angioplasty was being contemplated
for the contra lateral extremity at the time of this
study. Impending gangrene, inevitable ampu-
tation decision and non-healing large wounds
prompted their enrollment into the study.
In all ve subjects, no immediate or delayed
local or systemic complications were reported,
after stem cell injections. The ulcers weremanaged and monitored
more closely and
frequently, whereas the other post-procedure
objective evaluations were done at week 4, 8
and 12. In all cases, Doppler-guided arterial
segmental pressure of the dorsalis pedis artery
and posterior tibial artery were measured prior
to the procedure. Ankle brachial indices were
calculated separately for each of the lower
extremity arteries by dividing the ankle systolic
pressure of the individual artery by the brachial
artery systolic pressure. The differences werecompared with the
pre-implantation measure-
ments. Although nominal improvement in ABI
measurements was observed at three months
after stem cell implantation, none reached
normal values. A clear improvement, albeit non
uniform rise in the ankle pressure was certainly
a positive development. There was no rest pain
in all ve patients at 3 months follow up
A:Wound with gangrene reaching the centre of the foot, three
toes seen, two toes were amputated,B: Wound cleaned debridement
done
prior to stem cell treatment. C: Stem cell application, IM
injection and topical instillation, Cell Injection, Cell
Instillation. D: Wound 7 days post
stem cell injection, clean wound granulation tissue, E: Wound
one month post transplant showing good healing. F: ( >) Wound
almost closed
from the plantar side, ( >) very good granulation tissue, (
>) hard bone, No slough or foul smell.
Figure 3: Patient 2
7
Open access publishingThe Journal of Diabetic Foot
Complications, 2013; Volume 5, Issue 1, No. 1, Pages 1-14
-
7/26/2019 Dm Ulkus Jurnal
8/14
Patient Number ABI index
CAD, RAD
Other risk factors
HTN
Rutherford
Category
Pre Post Size Pre Post @3 months Amputation Pre Post
1 0.36 0.9 Impending ulcer, on the heel;
4x5cm;blackened great toe,
amputation of the left small toe
in the past.
At 3 months, great toe
shows reduced blacken-
ing and heel looking
normal
None 5 4
2 0.50 0.8 10x12x2cm
Heel area, severe pain in the leg,
ulcer area etc.
100% wound totally
healed
None 4 1
3 0.3 0.7 15x10x5cm,
Calcaneum exposed, deep sub-
cutaneous and muscular tissue
exposed, infected, foul smelling.
Amputation of small toe done 1year ago
100% wound closure, skin
grafting done. Patient well
and ambulatory
At 14 months
visit no new
ulcers seen.
No amputa-
tion
4 2
4 0.36 0.8 Heel area- 6x6cm No
amputation
Good granulation tissue,
size reduced to 2cmx2cm
None 5 3
5 0.45 0.7 80% wound healing , 2
mm area remaining at 6
months
At 6 months
no new
lesions, no
amputation
5 1
evaluation. All subjects exhibited an improve-
ment by at least one grade increase from the
pre-procedure evaluation as per the Rutherford
classication. In addition, improvement in wound
healing in all the patients ranged between 80-
90% within three months. The granulation tissue
was healthy and was seen along the sides andat the base of the
ulcer. There was no evidence
of infection, abscess or accumulation of pus in
any of these cases at this time point. No local
itching, pain or swelling was reported. One of
the 5 patients was reported 14 months later to
show sustained improvement. (Figure 4). He is
ambulatory and well. At six months follow up, be-
yond the planned time point, the second patient
had presented with a completely healed wound.
No new amputation decision or new ulcer was
reported in the follow up period. The other 3 pa-tients are also
doing well, and are under obser-
vation of the senior surgeon even after the stated
time point (Table 5).
Table 5: ABI measurements, rest pain, and ischemic ulceration
status before and after stem cell implantation and current
amputation
status listed patient wise
CAD (Coronary artery disease), RAD (Renal artery disease), HTN
(hypertension)
A: Ulcer, bone deep, exposing tissues underneath, calcaneus
exposed prior to stem cell treatment
B: Same ulcer showing less inammation, healthy granulated
tissue, but calcaneus still exposed.
C: Three months post calcaneal shaving, an almost closed wound,
5% remaining area showing healthy granulation tissue
D: Completely healed wound showing a signicantly changes in
contour 8
Open access publishingThe Journal of Diabetic Foot
Complications, 2013; Volume 5, Issue 1, No. 1, Pages 1-14
Figure 4: Patient 3
-
7/26/2019 Dm Ulkus Jurnal
9/14
9
Open access publishingThe Journal of Diabetic Foot
Complications, 2013; Volume 5, Issue 1, No. 1, Pages 1-14
Chronic non-healing wounds are a cause
of signicant morbidity and mortality and pose a
large nancial burden on the healthcare system.
Such patients with underlying severe PAD in
whom conservative management and surgicalinterventions such as
endovascular or open
procedures have failed, are advised to undergo
limb amputation as a nal option. Proper
cutaneous wound repair requires a well coordi-
nated response of inammation, neovasculariza-
tion, extracellular matrix formation, and epithe-
lialization. Failure of any of this process due to
ischemia, reperfusion injury, bacterial infection,
or aging can result in chronic inammation and
a non-healing wound25. Despite the most recent
advances in wound management, up to 50% of
chronic wounds still fail to heal26. One hypothesis
for this problem is that resident cells in non-heal-
ing wounds are intrinsically impaired and dem-
onstrate increased senescence and decreased
response to growth factors27.
Beginning in 2000, several animal model
studies of limb ischemia reported successful
outcomes using stem cell therapy to improve
peripheral blood circulation. These studies sub-sequently
spurred early clinical trials in Asia and
Europe involving injection of mononuclear bone
marrow stem cells to treat severe PAD patients.
These preliminary trials were very promising,
which then led investigators to believe that stem
cells have a role in PAD.
Promising results have been shown in
patients with PAD using autologous BM-MNC
(bone marrow mononuclear cells), BM-MSC
(bone marrow mesenchymal cells) and G-CSF(granulocyte
colony-stimulating factor) mobilized
PB-MNC (peripheral blood mononuclear cells), a
new treatment option for these patients. Several
clinical trials are consistent in their ndings on
clinical benets including improvements of ABI,
TcPO2, reduction of pain and reduced need for
amputation26. While the advantage of using au-
tologous MNCs and MSCs cannot be disputed,
there are several challenges in getting consistent
bone marrow and cell yields from the type of
patients who present with PAD. Hence the need
to look for easier and dependable sources for
these cells.
Wound healing studies have also looked at
MSCs as contributing to cutaneous regeneration
Studies in both mice and humans have consis-
tently demonstrated enhanced wound repair
following treatment with bone marrow derived
MSCs. This is yet more evidence supporting
MSC-based therapies for cutaneous wound
healing and future directions to bring their poten-
tials to the clinical setting.
The application of MSCs for the tissue repair
had ranged from intravenous infusion to reduce
the size of brain infarcts in a rat stroke model28 to
implantation of cells in the myocardium to reduce
left ventricular dysfunction in a swine model of
myocardial ischemia29. Our own experience in
preclinical models of PAD, Diabetes and Par-
kinsons diseases in small animals has showed
substantial improvement when mesenchymal
stem cells alone or in combination with CD34+
cells were used14
.
A recent report hypothesized that implanted
cells stimulate muscle cells to produce angio-
genic factors, thereby promoting neovascular-
ization30. Marrow and peripheral blood CD34+
haematopoietic stem cells express (Vascular
Endothelial Growth Factor Receptors) VEGFR
and Tie 2 (tyrosine kinase-2), when cultured ex
vivo, these cells differentiate into endothelial
cells expressing the Von Willebrand factor31.
Vascular development is regulated by growthfactors such as VEGF,
angiopoietin-1 that bind a
tyrosine kinase receptor Tie-2 involved in com-
pleting the vascular architecture32. Asahara et al
demonstrated that co-culture of CD34+ cells with
the CD34- cells in an in-vitro 3-D matrix model
using microvascular endothelial cells signicantly
enhanced neovascularization11.
DISCUSSION
-
7/26/2019 Dm Ulkus Jurnal
10/14
Fibroblasts are increasingly used in various
cosmetic applications for their cytokine prole.
Autologous broblasts are difcult to harvest, but
not impossible. Allogeneic broblasts give equal
efcacy and their immunomodulatory nature
makes it much easier for ready use22. These
patients with non-healing foot ulcers were admin-istered 2
million per cm2neonatal broblasts by
inltration and local application.
Thus, mesenchymal stem cells alone or in
combination with the haematopoietic stem cells
represent yet another promising modality sup-
porting new concepts in cellular therapy. This
report on ve patients with non-healing foot
ulcers was to assess the efcacy and feasibil-
ity of an allogeneic stem cell combination com-
prising the MSCs and CD34+ cells with useof broblasts cells for
local application. These
ve patients showed decrease in severity of
symptoms three months after the procedure,
as evidenced by alleviation of rest pain and
improvements in Rutherford scores. Two of the
patients had a three level improvement, while
two others had 2 level improvements and the
remaining one patient showed a one level im-
provement in the Rutherford category.
Prior to the therapy, there was a distinct
demarcation of the cold and the warm area of
the leg, which improved after stem cell injection.
We saw good granulation along the borders
and the oor of the ulcer, and overall, the tissue
had a healthy look. No infection was observed
and borders of the ulcers were all normal and
patients were advised to wear special shoes
before weight bearing. The patient with the
longest follow up period of about 14 months
is ambulatory, and goes for frequent dialysis;cannot walk much
due to the low cardiac ejection
fraction. The second patient at 6 months follow
up is walking within the house and is very
energetic and feeling well. The third patient
at 3-months follow up is better and has been
advised to walk but is still wheelchair bound due
to fear. The ulcer has completed healed but a toe
still has some residual blackening. The rest of
the patients at 3 months are feeling very comfort-
able, with reduced pain and no new ulcers. No
special post stem cell treatment Doppler exami-
nations were performed.
No procedure-related complications, local or
systemic were reported during the procedure or
at the follow-up evaluations. Mean improvements
of dorsalis pedis artery (DPA) and posteriortibial artery (PTA)
0.13 and 0.09 in ABI were
observed after the cell implantation at three
months. Although only nominal improvement was
observed in the ABI measurements before and
after one dose of the stem cell product, there
was denite progress. All important biochemical
parameters remained within normal range during
follow up, and there was no signicant differ-
ence from the pretreatment values, indicating no
adverse effect of MSC implantation on plasma
glucose, liver, or renal functions.
To our knowledge, this is the rst report of
an early clinical experience of this type of stem
cell combination therapy for PAD with ulcers.
While there are several reports of autologous
bone marrow derived mononuclear cells into
various low-oxygenated ischemic sites of the
lower extremity, a combination cell type using
allogeneic cells has greater signicance. Readily
available and immunomodulatory properties
make UCMSCs very attractive for clinical ap-
plications. CD34+ cells are normally used for
hematopoietic reconstitution after an HLA match.
But local application of CD34+ cells in such smal
quantities does not require HLA match33. The
goal of this type of combination stem cell therapy
thus probably helped promote neoangiogen-
esis, endothelial formation, thereby increasing
the collaterals to the affected organs, reducing
symptoms, and facilitating wound healing in
patients with PAD.
Our study population is more heterogeneous
than those in the other studies, and therefore,
may better represent the general PAD patient
population as a whole. A signicant improve-
ment in ABI and TcPO2 along with the pain free
walking time was reported in trials in which au-
tologous bone marrow mononuclear cells were
transplanted to bring out the therapeutic10
Open access publishingThe Journal of Diabetic Foot
Complications, 2013; Volume 5, Issue 1, No. 1, Pages 1-14
-
7/26/2019 Dm Ulkus Jurnal
11/14
In conclusion, all patients showed at
least one level of clinical improvement after stem
cell implantation, suggesting the therapeutic
goal of improving limb perfusion is truly possible.
Complete wound healing was achieved within
three months in several patients. These short-
term results indicate the immense potential of
MSC+HSC combination, with broblasts for
local repair. In the light of these encouraging
observations, and based on results in the litera-
ture, the authors feel the need to initiate stem
cell procedure earlier on in the treatment plan
in patients with severe ischemia or non-healing
ulcers to achieve best results.
The authors acknowledge Reliance
Life Sciences Pvt. Ltd (www.rellife.com), for
providing the infrastructure and nancial support
to work on this project. The authors would also
like to thank Dr. S. K Rane and Dr. D. Hattanga-
di for their support during the conduct of this
study.
11
Open access publishingThe Journal of Diabetic Foot
Complications, 2013; Volume 5, Issue 1, No. 1, Pages 1-14
CONCLUSION
ACKNOWLEDGEMENTS
angiogenesis in patients with critical limb isch-
emia.
All these studies reported proved that
the autologous implantation of bone marrow-
mononuclear cells could be safe and effective
for achievement of therapeutic angiogenesis,because of the
natural ability of marrow cells to
supply endothelial progenitor cells and to secrete
various angiogenic factors or cytokines34-38.
A clinical trial using autologous mesenchy-
mal stem cells alone for limb ischemia has been
reported in the clinical trial.govsite. Similarly,
another trial using CD34+ cell alone for critical
limb ischemia has been reported in the clinical
trial website. Both the studies have been
completed but results of both these trials have
not yet been published39-40.
The present study demonstrated that alloge-
neic implantation which includes the MSCs and
the CD34+ cells combination is a simple, safe,
and effective tool to treat chronic non healingulcers in cases
of PAD. Pain relief was satisfac-
tory and there was a signicant decrease in ulcer
size and increase in pain-free walking distance in
the stem cell treated group as compared to the
untreated group. The role played by broblasts
needs to be noted. Feasibility of MSC and hae-
matopoietic stem cells (HSC) application, their
availability, safety, and absence of any adverse
effects is encouraging.
1. Norgren L, Hiatt WR, DormandyJA et al: Inter-society
consensus for the management of peripheral
arterial disease (TASC II). Eur J Vasc Endovasc Surg; 2007;33
(Suppl 1): S1-S75.
2. Second European Consensus Document on chronic critical leg
ischemia. Circulation. 1991;84(4
Suppl): p. IV126.
3. Zijang Y, Stefan DS and Christoph K: Swiss Medical weekly;
2010; 140:w13130.
References
-
7/26/2019 Dm Ulkus Jurnal
12/14
Open access publishingThe Journal of Diabetic Foot
Complications, 2013; Volume 5, Issue 1, No. 1, Pages 1-14
4. Norgren L et al: Inter-society consensus for the management
of peripheral arterial disease(TASC
II). J Vasc Surg. 2007;45 (Suppl 1): S5-S67.
5. BaumgartnerI, Schainfeld R, Grazianni L; Management of
peripheral arterial disease. Ann Rev
Med. 2005; 56: 249-72.
6. Hooi JD, Stoffers HE, knottnerus JA et al; The prognosis of
non-critical limb ischemia; a systemicreview of population- based
evidence.Br J gen Pract; 1999; 49: 49:55.
7. Randall W. Franz, Alan Parks, Kaushal J. Shah et al; Use of
autologous bone marrow mononuclear
cells as alimb salvage procedure in patients with severe
arterial disease. J Vasc Surg 2009;50:
1378-90.
8. Henry TD. Therapeutic angiogenesis. Br Med J. 1999; 318:
1536-6.
9. Isner JM, Asahara T. Angiogenesis and vasculogenesis as
therapeutic strategies for post natal
neovasculrization. J clin Invest. 1999; 103(9): 1231-6.
10 Ippokratis p, Giannoudis PV. Biology of mesenchymal stem
cells in injury. Int J care Injured 36S:
S8-S12.
11. Asahara T, Masuda H, Takahashi T, et al. Bone marrow origin
of endothelial progenitor cells
responsible for postnatal vasculogenesis in physiological and
pathological neovascularization. Circ
Res 1999; 85:221-28.
12. Prockop DJ. Marrow stromal cells as stem cells for non
haematopoietic tissues. Science1997;
276: 71-4.
13. Kudo FA, Nishibe T, Nishibe M, et al. Autologous
transplantation of peripheral blood endothelial
progenitor cells (CD34+) for the therapeutic angiogenesis in
patients with critical limb ischemia. Int
Angiol 2003;22: 344-348.
14. Shetty P, Anirban T, Viswanathan C et al. Directed
therapeutic angiogenesis by mesenchymal
stem cells from umbilical cord matrix in preclinical model of
ischemic limb disease. Stem cell studies
2010; 1 (16): 97-104.
15. Kinnaird T, Stabile T, Burnett MS et al. local delivery of
marrow derived stromal cells augments
collateral perfusion through paracrine mechanisms. Circulation
2004; 109;1543-1549.
16. Kinnaird T, Stabile T, Burnett MS et al. Marrow derived
stromal cells express genes encoding a
broad spectrum of arteriogenic cytokines and promote in vitro
and in vivo aeteriogenesis through
paracrine mechanisms. Circulation Res 2004; 94: 678-685.
17. Li S, Zhou B, Han ZC. Therapeutic neovascularization by
transplantation of mobilized peripheral
blood mononuclear cells for limb ischemia. A comparison between
CD34+ and CD34- mononuclear
cells. Thromb Hae,ost 2006; 95: 301-311.
12
-
7/26/2019 Dm Ulkus Jurnal
13/14
Open access publishingThe Journal of Diabetic Foot
Complications, 2013; Volume 5, Issue 1, No. 1, Pages 1-14
18. Tipnis S, Viswanathan C, SenMajumdar A. Immunosuppressive
properties of human umbilical
cord derived mesenchymal stem cells Role of B7-H1 and IDO.
Immunol Cell Biol 2010; 88:795-806.
19. Marston WA, Hanft J, Norwood P, et al. Diabetic Foot Ulcer
Study Group. The efcacy and
safety of Dermagraft in improving the healing of chronic
diabetic foot ulcers: Results of a prospective
randomized trial. Diabetes Care 2003; 26: 17015.
20. Veves A, Falanga V, Armstrong DG, et al. Apligraf diabetic
foot ulcers study. Graftskin, a human
skin equivalent, is effective in the management of noninfected
neuropathic diabetic foot ulcers: A
prospective randomized multicenter clinical trial. Diabetes Care
2001; 24: 2905.
21. Mansbridge J. Tissue-engineered skin products. In Lanza R,
Langer R and Vacanti J (eds).
Principles of Tissue Engineering (edition 3). San Diego,
Elsevier Academic, 2007).
22. Manisha Deshpande, Shabari Tipnis, Prathibha Shetty et al.
Immunologic properties of human
dermal broblasts Human Immunology 2010;71:10891098.
23. Shetty P, Cooper K, Viswanathan C.Comparison of
proliferative and multilineage differentiationpotentials of cord
matrix cord blood and bone marrow derived mesenchymal stem cells.
Asian J
Transf Sci 2010; 4: 14-24.
24. Tipnis S, Viswanathan C. Umbilical cord matrix derived
mesenchymal stem cells can change the
cord blood transplant scenario. Intl J Stem Cells 2010; 3 (2),
103 118
25. Mustoe TA, OShaughnessy k and Kloeters O. Chronic wound
pathogenesis and current
treatment stratergies: a unifying hypothesis. Plast.Reconstr.
2006; Surg. 117,35S-41S.
26. Cha J, and Falanga V. Stem cells in cutaneous wound healing.
Clin. Dermataol. 2007; 25, 73-78.
27. Hasan A, Murata H, Falabella A, et al. Dermal broblasts from
venous ulcers are unresponsive to
the action of transforming growth factor-beta-1. 1997;
J.Dermataol.Sci.16,59-66.
28. Li Y, Chen J, Zahng CL et al. Gliosis and brain remodeling
after treatment of stroke in rats with
marrow stromal cells. 2005; Glia 49, 407-417.
29. Amadao LC, Saliaris AP, Schuleri KH et al. Cardiac repair
with intramyocardial injection of
allogeneic mesenchymal stem cells after myocardial
infarction.2005; Proc. Natl. Acad. Sci USA 102,
11474-11479.
30. Tateno K, Minamino T, Toko H et al. Critical role of
muscle-secreted angiogenic factors in
therapeutic neovascularization. Circ Res; 2006;98:
1194-1202.
31. Kanayasu-Toyoda T, Yamaguchi T, Oshizawa T et al. CD31
(PECAM-1) bright cells derived from
AC133-postive cells in human peripheral blood as endothelial
precursor cells. 2003; J Cell Physiol;
195: 119-129.
32. Folkman J, DAmore PA. Blood vessel formation: what is the
molecular basis? 1996; Cell; 87:
1153-1155.by 3autologous transplantation of bone marrow cells. a
pilot study and a randomized
clinical trial. 2002; Lancet; 360: 427-435. 13
-
7/26/2019 Dm Ulkus Jurnal
14/14
33. Yang W, Zhang Y, Wu F et al. Safety evaluation of allogeneic
umbilical cord blood mononuclear
cell therapy for degenerative conditions. 2010; Journal of
Translational Medicine, 8:75-80.
34. Amann B, Schachnigar V, Teupe C et al. Design and rationale
of a randomized, double blind
placebo controlled phase III study for autologous bone marrow
cell transplantation in critical limb
ischemia: the Bone Marrow outcomes trial in critical limb
ischemia (BONMOT-CLI). VASA 2008; 37:
319-325.
35. Tateishi-YuyamaE, Matsubara H, Murohara T et al. Therapeutic
angiogenesis using cell
transplantation(TACT) study investigators .Therapeutic
angiogenesis for patients with limb ischemia
36. Higashi Y, Kimura M, Hara K et al. Autologous bone marrow
mononuclear cell implantation
improves endothelium dependent vasodilation in patients with
limb ischemia.2004; Circulation; 109:
1215-1218.
36. Higashi Y, Kimura M, Hara K et al. Autologous bone marrow
mononuclear cell implantation
improves endothelium dependent vasodilation in patients with
limb ischemia.2004; Circulation; 109:
1215-1218.
37. Bartsch T, Falke T, Brehm M et al. Intra-arterial and
intramuscular transplantation of adult
autologous bone marrow stem cells. Novel treatment for therapy
refractory peripheral arterial
occlusive arterial disease.2006; Med Wochenschr; 131:79-83.
38. Kajiguchi M, Kondo T Izawa et al. Safety and efcacy of
autologous progenitor cell transplantation
for therapeutic angiogenesis of in patients with critical limb
ischemia.2007; Circ J; 71: 196-201.
39. Comparison of Autologous Mesenchymal Stem Cells and
Mononuclear Cells on Diabetic Critical
Limb Ischemia and Foot Ulcer- NCT00955669, clinical
trial.gov.
40. Injection of Autologous CD34-Positive Cells for Critical
Limb Ischemia- NCT00616980, clinical
trial.gov.
14
Open access publishingThe Journal of Diabetic Foot
Complications, 2013; Volume 5, Issue 1, No. 1, Pages 1-14