Embed Size (px)
Citation preview

4/27/12
1
Ocular and periocular infections
Tina Rutar M.D. Assistant Professor,
Department of Ophthalmology Department of Pediatrics
University of California San Francisco
Course outline
• Review basic anatomy of eye and orbit • Review vision threatening signs • Review orbital danger signs • Infections
– Blepharitis – Conjunctivitis – Corneal infections – Periorbital vs. orbital cellulitis – Endophthalmitis
Eye anatomy
www.thecountymedicalexaminers.com
Eye anatomy
4/27/12
2
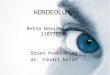
Orbital anatomy
www.wikidoc.org http://upload.wikimedia.org/wikipedia/commons/8/8e/Eye_orbit_anatomy_superior.jpg
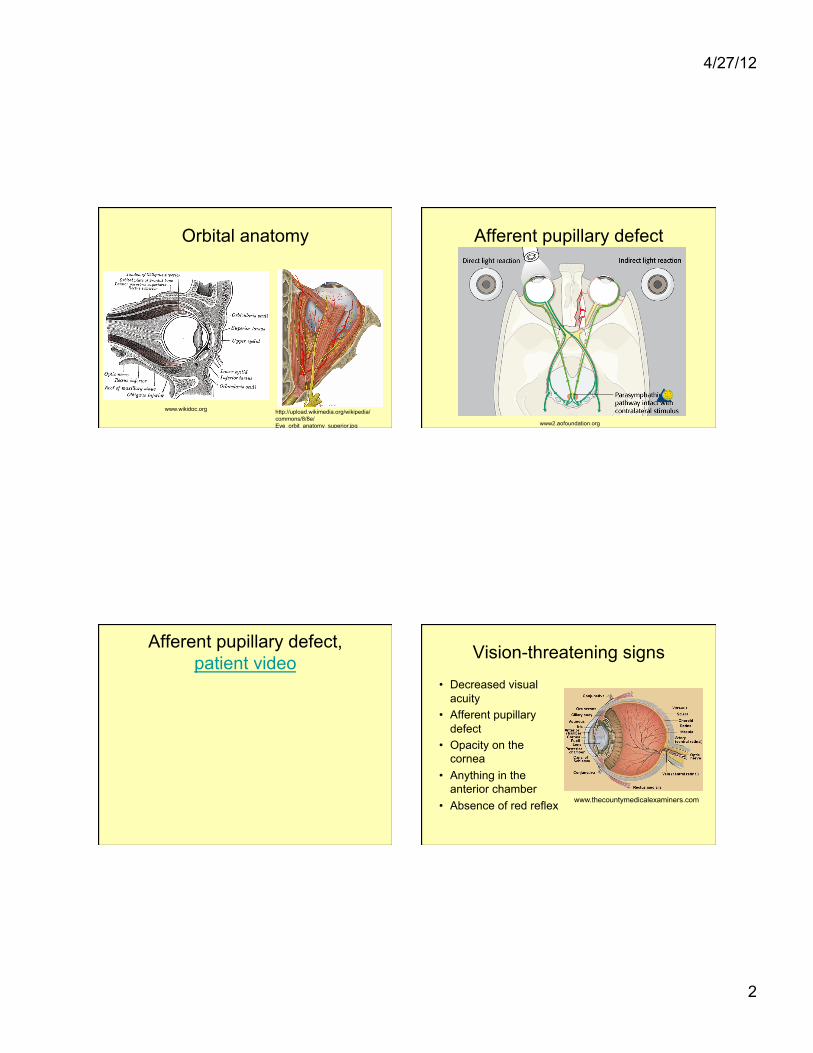
Afferent pupillary defect
www2.aofoundation.org
Afferent pupillary defect, patient video Vision-threatening signs
• Decreased visual acuity
• Afferent pupillary defect
• Opacity on the cornea
• Anything in the anterior chamber
• Absence of red reflex www.thecountymedicalexaminers.com
4/27/12
3
Orbital danger signs
• Decreased visual acuity
• Afferent pupillary defect
• Proptosis • Limited motility
www.wikidoc.org
Ocular and periocular infections
• Blepharitis • Conjunctivitis • Corneal infections • Periorbital vs orbital cellulitis • Endophthalmitis
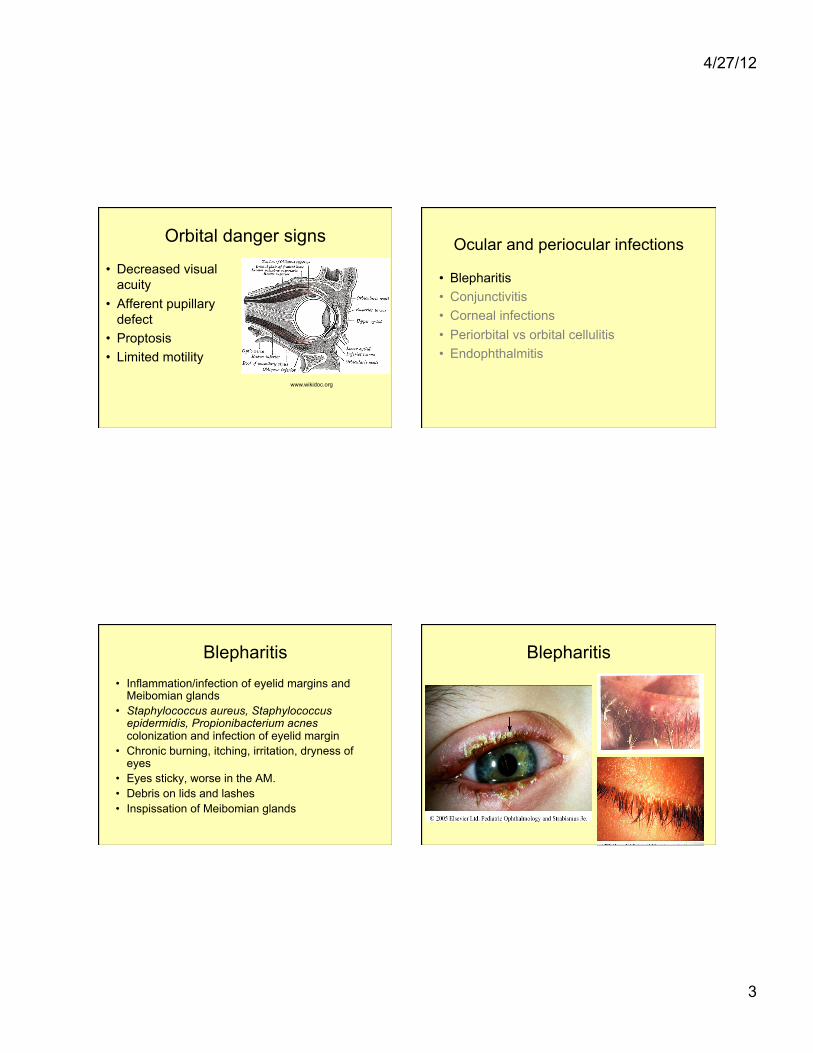
Blepharitis • Inflammation/infection of eyelid margins and
Meibomian glands • Staphylococcus aureus, Staphylococcus
epidermidis, Propionibacterium acnes colonization and infection of eyelid margin
• Chronic burning, itching, irritation, dryness of eyes
• Eyes sticky, worse in the AM. • Debris on lids and lashes • Inspissation of Meibomian glands
Blepharitis

4/27/12
4
Meibomitis
http://www.contactlens.org.nz http://www.mastereyeassociates.com
Hordeola (styes)
Chalazia Treatment
• Hot compresses • Eyelid hygiene • Bacitracin ophth ointment to lashes bid x
10 days • Artificial tears • Meibomitis associated with rosacea:
doxycycline PO or azithromycin PO • Topical corticosteroid eye drops and
ointments
4/27/12
5
Chalazia – surgical treatment Ocular and periocular infections
• Blepharitis • Conjunctivitis • Corneal infections • Periorbital vs orbital cellulitis • Endophthalmitis
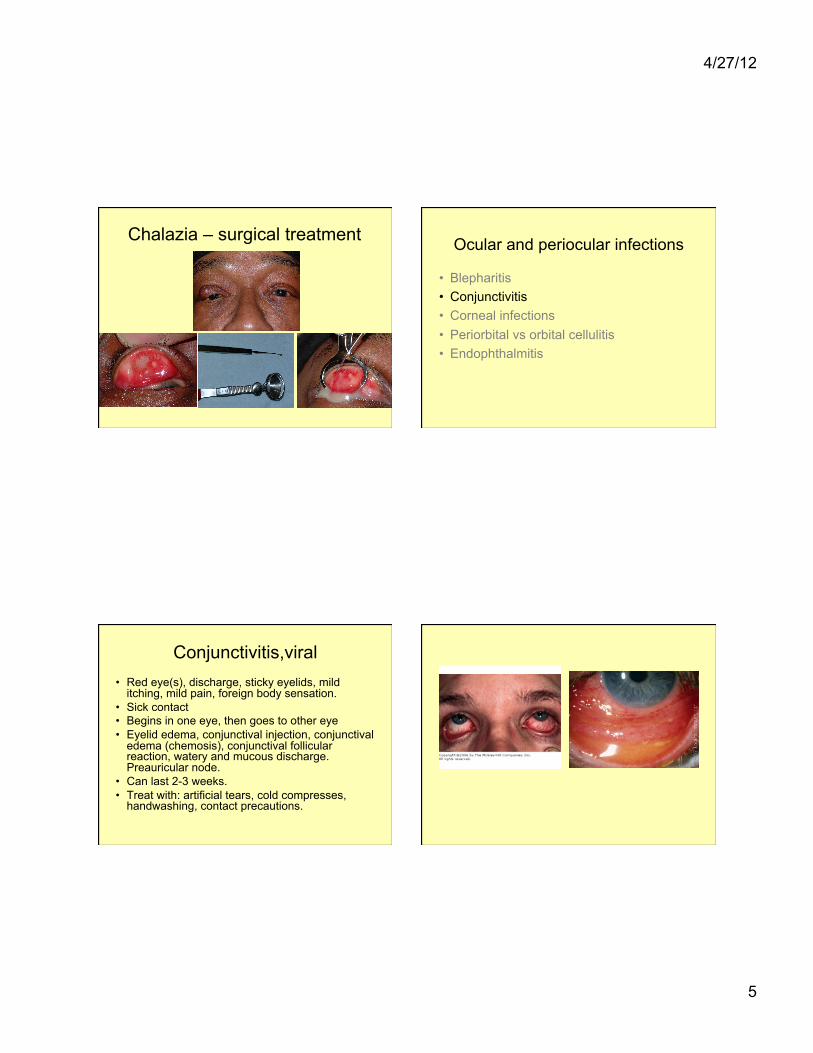
Conjunctivitis,viral • Red eye(s), discharge, sticky eyelids, mild
itching, mild pain, foreign body sensation. • Sick contact • Begins in one eye, then goes to other eye • Eyelid edema, conjunctival injection, conjunctival
edema (chemosis), conjunctival follicular reaction, watery and mucous discharge. Preauricular node.
• Can last 2-3 weeks. • Treat with: artificial tears, cold compresses,
handwashing, contact precautions.

4/27/12
6
Conjunctivitis,viral • Subtypes requiring additional treatments • Adenovirus - occasionally topical steroids for corneal
subepithelial infiltrates • HSV conjunctivitis - oral acyclovir 200-400 mg PO five
times daily or valacyclovir 500 mg PO bid-tid • Recurrent VZV conjunctivitis – oral acyclovir 800 mg PO
five times daily or valacyclovir 1000 mg PO tid • Molluscum contagiosum – treated with incision, cautery,
cryotherapy; if recurrent or multiple lesions, work up for immunocompromised state
Conjunctivitis, bacterial • Eye redness, foreign body sensation, copious discharge • Conjunctival injection, conjunctival chemosis, purulent
discharge • Staphylococcus aureus, Staphylococcus epidermidis,
Streptococcus pneumoniae, Haemophilus influenzae, Neisseria gonorrhoeae, Chlamydia trachomatis
• Treat with: topical antibiotic (polymyxin trimethoprim, ciprofloxacin)
• Systemic antibiotic for Neisseria gonorrhoeae (ceftriaxone IM/IV) and Chlamydia trachomatis (azithromycin PO/erythromycin PO)
Cochrane review on antibiotic treatment of bacterial conjunctivitis
• Topical antibiotics compared to placebo are responsible for faster recovery clinically and microbiologically
• Most bacterial conjunctivitis is self limited, and it is not visually threatening
• 2/3 improved within 2-5 days in placebo arm
• No adverse events reported in either the antibiotic or placebo groups
4/27/12
7
Ocular and periocular infections
• Blepharitis • Conjunctivitis • Corneal infections • Periorbital vs orbital cellulitis • Endophthalmitis
Distinguish conjunctivitis from keratitis
http://www.optometric.com/archive
Causes of keratitis
• Infectious keratitis: bacterial, fungal, viral, acanthamoeba.
• Many noninfectious causes of keratitis. • Risk factors for infectious keratitis:
– Decreased corneal sensation: diabetes, CN5 palsy, herpes infection
– Overnight contact lens wear and poor contact lens hygiene
– Corneal abrasions/trauma – Prior eye or eyelid surgery – Poor eyelid closure
4/27/12
8
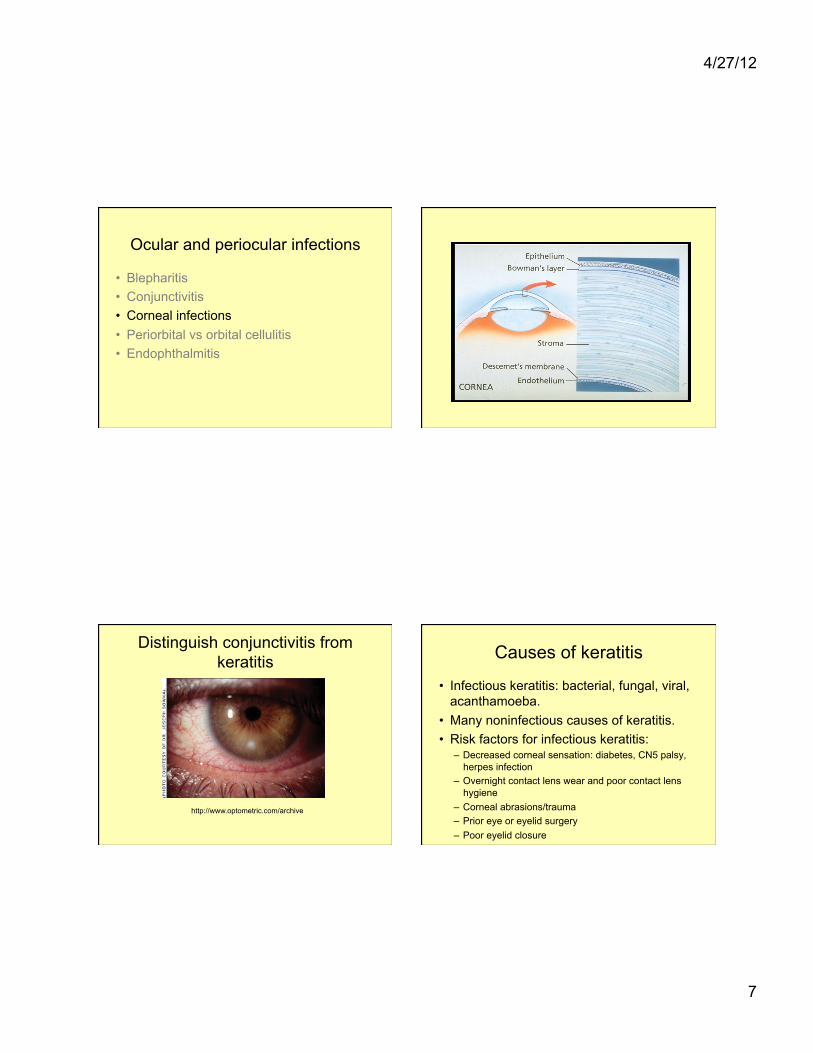
Bacterial corneal ulcer Bacterial corneal ulcer • Infection of the corneal stroma (overlying
epithelial defect) • Diagnosis: corneal Gm stain and culture • Highly virulent organisms: Pseudomonas,
Streptococcus pneumoniae, gonococcus • Treatment:
– hourly broad-spectrum antibiotic (moxifloxacin or gatifloxacin) or fortified topical antibiotics (vancomycin + tobramycin or gentamycin)
– discontinue contact lens wear
Ocular and periocular infections
• Blepharitis • Conjunctivitis • Corneal infections • Periorbital vs orbital cellulitis • Endophthalmitis
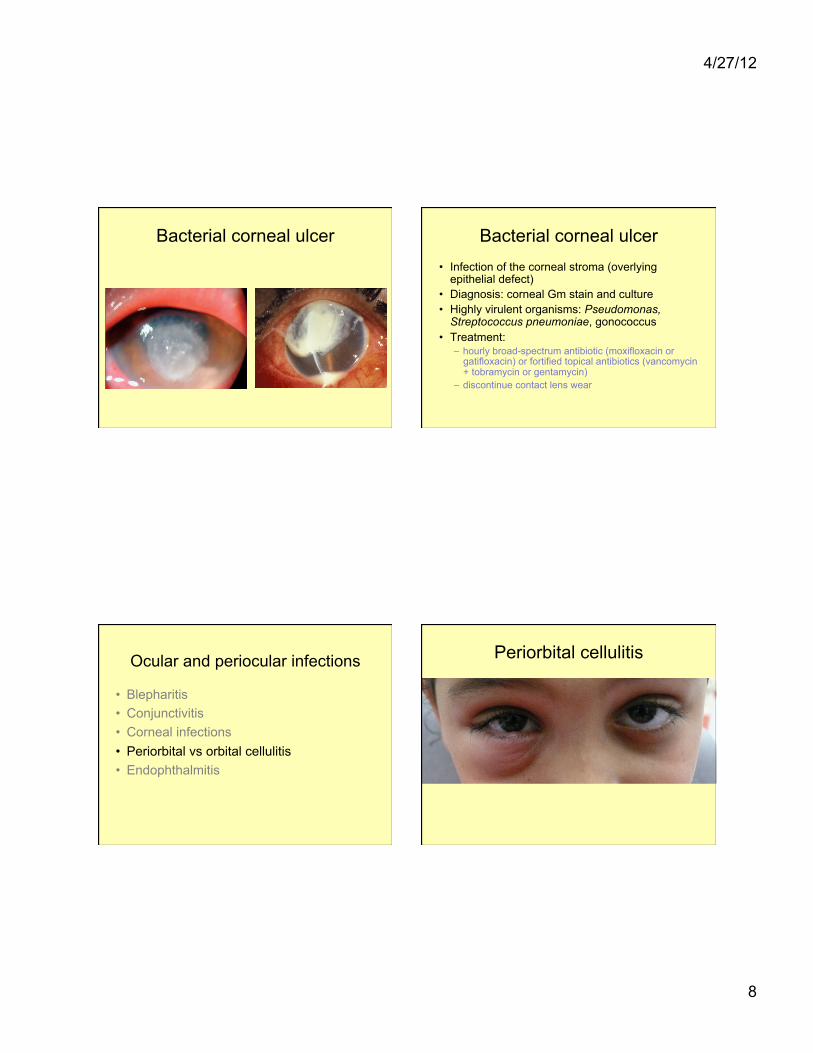
Periorbital cellulitis

4/27/12
9
Periorbital cellulitis Periorbital cellulitis
http://meded.ucsd.edu/clinicalimg
Periorbital cellulitis • Infection that is anterior to the orbital septum involving
the periorbital soft tissue and the eyelids • Edema, erythema, tenderness affecting eyelids/periorbita • Quiet eye (noninjected conjunctiva) • Associated sinusitis, hordeolum, violation of the skin • Treatment
– PO antibiotics: no fever, age >1 year • Oral clindamycin or trimethoprim/sulfamethoxazole in community MRSA-
prevalent area • Oral cephalexin with close follow up if low likelihood of MRSA, mild infection
– IV antibiotics: fever, elevated WBC/neutrophil count, infant, worsening
Orbital cellulitis

4/27/12
10
Orbital cellulitis Orbital cellulitis • An infection posterior to the orbital septum with involvement of
orbital structures (can affect extraocular muscles, sensory and motor nerves and the optic nerve )
• Decreased vision • Afferent pupillary defect • Proptosis • Limited motility, pain w motility, diplopia • Conjunctival injection/chemosis • Associated sinusitis, bacteremia, antecedent periorbital cellulitis,
dental infection • Treatment and work up
– Hospital admission – IV antibiotics (vancomycin + piperacillin/tazobactam) – Blood cultures, cultures of orbital abscess or sinuses – Orbital imaging (orbital/sinus CT with contrast) – Surgery (drainage of orbital abscess, sinus drainage)
Ocular and periocular infections
• Blepharitis • Conjunctivitis • Corneal infections • Periorbital vs orbital cellulitis • Endophthalmitis
Endophthalmitis
• Infection involving the vitreous cavity (+other parts of the eye)
• Pain, decreased vision, conjunctival injection, hypopyon, poor red reflex
4/27/12
11
Endophthalmitis, post trauma Endophthalmitis, post surgical
Scott and Flynn. http://www.retinalphysician.com
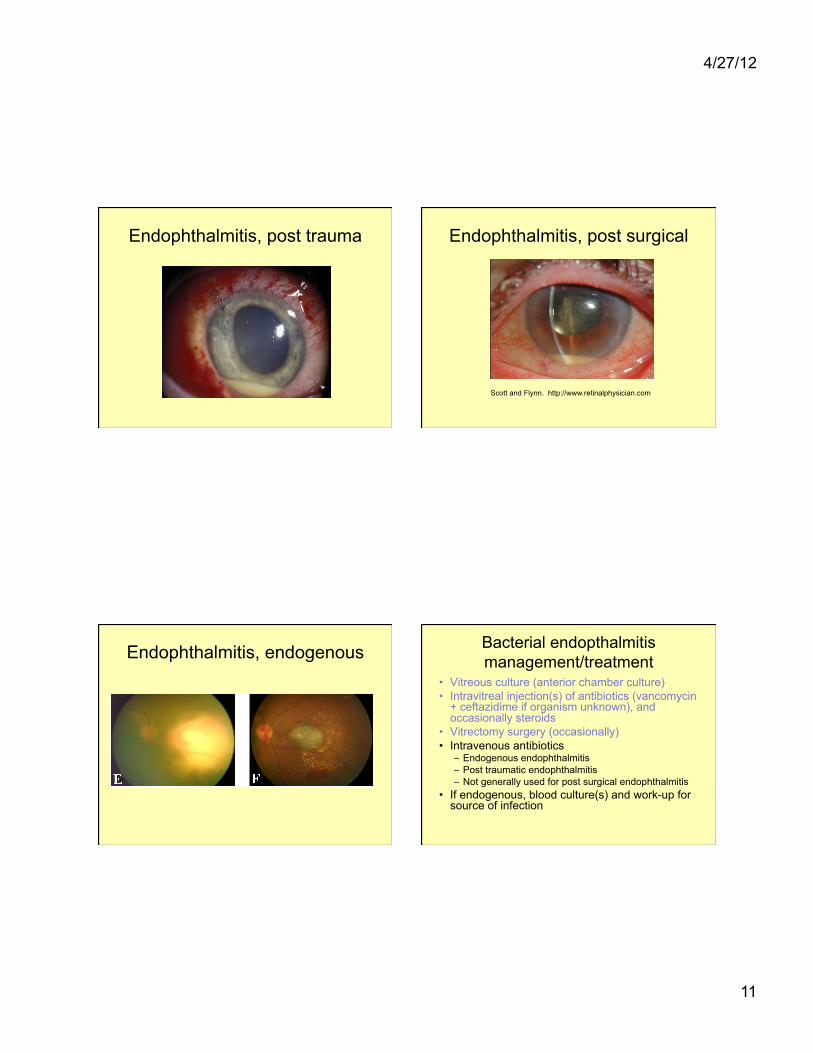
Endophthalmitis, endogenous Bacterial endopthalmitis management/treatment
• Vitreous culture (anterior chamber culture) • Intravitreal injection(s) of antibiotics (vancomycin
+ ceftazidime if organism unknown), and occasionally steroids
• Vitrectomy surgery (occasionally) • Intravenous antibiotics
– Endogenous endophthalmitis – Post traumatic endophthalmitis – Not generally used for post surgical endophthalmitis
• If endogenous, blood culture(s) and work-up for source of infection

4/27/12
12
When to refer ocular and periocular infections to ophthalmology
• Vision threatening signs – Decreased visual acuity – Afferent pupillary defect – Opacity on the cornea – Anything in the anterior chamber – Absence of red reflex
• Orbital danger signs – Decreased visual acuity – Afferent pupillary defect – Proptosis – Limited motility
• History of prior eye surgery