Embed Size (px)
Citation preview
Journal of Clinical Virology 16 (2000) 135–144
Comparison of PanBio Dengue Duo Igm and IgG CaptureELISA and Venture Technologies Dengue IgM and IgG
Dot Blot
A.J. Cuzzubbo a, D.W. Vaughn b,1, A. Nisalak b, T. Solomon c,2,S. Kalayanarooj d, J. Aaskov e, N.M. Dung f, P.L. Devine a,*
a PanBio Pty Ltd, 116 Lutwyche Rd., Windsor 4030, Qld, Australiab Armed Forces Research Institute of Medical Sciences (AFRIMS), Bangkok, Thailand
c Wellcome Trust Clinical Research Unit, Centre for Tropical Diseases, Cho Quan Hospital, 190 Ben Ham Tu, Quan 5,Ho Chi Minh City, Vietnam
d Queen Sirikit National Institute of Child Health (Bangkok Children’s Hospital), Raji6ithi Road, 10400 Bangkok, Thailande School of Life Sciences, Queensland Uni6ersity of Technology, Brisbane, Australia
f Pediatric Intensi6e Care Unit, Centre for Tropical Diseases, Cho Quan Hospital, 190 Ben Ham Tu, Quan 5,Ho Chi Minh City, Vietnam
Received 20 May 1999; received in revised form 11 November 1999; accepted 22 November 1999
Abstract
Background : A number of commercial ELISA for dengue diagnosis have recently become available, though directcomparison between these assays have not been published. Objecti6es : The Venture Technologies Dengue IgM andIgG Dot Blot assays and the PanBio Dengue Duo IgM and IgG Capture ELISA were compared. Study Design :Paired sera from patients with dengue (n=20) and Japanese encephalitis (JE, n=10), and single sera from patientswith typhoid (n=10), leptospirosis (n=10) and scrub typhus (n=10) were assayed according to the manufacturer’sinstructions. Results : The Dot Blot IgM ELISA showed higher sensitivity than the PanBio IgM ELISA (100 vs. 95%),while the PanBio IgM ELISA showed higher specificity in JE (100 vs. 20%) and non-flavivirus infections (100 vs.97%). Defining elevation of either IgM or IgG as a positive result, the Dot Blot and ELISA tests both showed 100%sensitivity in dengue infection, while the PanBio test showed superior specificity in JE (70 vs. 0%) and non-flavivirus
www.elsevier.com/locate/jcv
Abbre6iations: ANOVA, Analysis of variance; CSF, Cerebrospinal fluid; DHF, Dengue haemorrhagic fever; ELISA, Enzyme-linked immunosorbent assay; HIA, Haemagglutination inhibition assay; JE, Japanese encephalitis; RT, Room temperature; S1, Seraat hospital admission; S2, Sera at hospital discharge.
* Corresponding author. Tel.: +61-7-33571177; fax: +61-7-33571222.E-mail addresses: [email protected] (D.W. Vaughn), [email protected] (T. Solomon), peter–de-
[email protected] (P.L. Devine)1 Present address: Walter Reid Army Institute of Research, Washington DC 20307, USA. Tel.: +1-202-7823655; fax: +1-202-
7820442.2 Present address: Department of Neurological Science, University of Liverpool, Walton Centre for Neurology and Neurosurgery,
Fazakerley, Liverpool L9 7LJ, UK. Tel.: +44-151-5253611, ext. 2147; fax: +44-151-5295465
1386-6532/00/$ - see front matter © 2000 Elsevier Science B.V. All rights reserved.
PII: S 1386 -6532 (99 )00071 -2

A.J. Cuzzubbo et al. / Journal of Clinical Virology 16 (2000) 135–144136
infections (100 vs. 67%). Conclusions : Both assays are useful aids to the serological diagnosis of dengue infection. Theclinical setting, user preference and local conditions will be important in determining which test is more appropriate.© 2000 Elsevier Science B.V. All rights reserved.
Keywords: ELISA; Dot blot; Dengue infection
1. Introduction
Serology is commonly used in the diagnosis ofdengue infections (Lam, 1993; Vorndam andKuno, 1997). Haemagglutination inhibition assay(HIA) has been used traditionally, but enzyme-linked immunosorbent assay (ELISA) has gainedacceptance as a faster and more convenient alter-native (Gubler, 1996).
Primary infection is characterised by a rise inspecific IgM 3–5 days after the onset of infectionand this is generally detectable for 30–90 days.IgG levels rise after IgM and are detectable forlife (Innis, 1997). In contrast, the IgM response insecondary dengue infection can be slower, weakerand shorter lived, and some patients do not showa detectable IgM (Ruechusatawat et al., 1994;Innis, 1997; Vaughn et al., 1997; Vorndam andKuno, 1997). However, IgG levels rise rapidly tohigher levels than observed in primary or pastdengue infection and remain at these levels for30–40 days (Gubler, 1996; Innis, 1997). Conse-quently, the combined use of IgM and IgG hasbeen proposed as an effective strategy for theserological diagnosis of dengue virus infection(Innis et al., 1989; Kuno et al., 1991; Ruechusat-awat et al., 1994; Devine et al., 1997; Vaughn etal., 1997; Sang et al., 1998b; Vaughn et al. 1998).
Two commercial ELISA have been developedthat utilize this strategy for IgM and IgG detec-tion: the Venture Technologies Dengue IgM andIgG Dot Blot kits (Venture Technologies, Penang,Malaysia) (Lam, 1993; Chong et al., 1994; Car-dosa et al., 1995; Lam et al., 1996; Kuno et al.,1998) and the PanBio Dengue Duo IgM Captureand IgG Capture ELISA (PanBio Pty Ltd, Bris-bane, Australia) (Lam and Devine, 1998; Sang etal., 1998b; Vaughn et al., 1999). However, directcomparison between the two assays has not beenreported. In this study, these tests were comparedusing sera taken from patients with primary and
secondary dengue infection, Japanese encephalitis(JE) infection, and non-flavivirus infections.
2. Materials and methods
2.1. Case definitions for dengue and Japaneseencephalitis
In children experiencing a febrile illness consis-tent with dengue fever or dengue hemorrhagicfever (DHF), dengue infections were defined asthe isolation of a dengue virus, the detection ofIgM to dengue (as opposed to IgM to JE), or asustained elevation (]1:2560) or fourfold rise indengue virus HIA antibody titre (Innis et al.,1989). Dengue infection was categorised as pri-mary or secondary according to the World HealthOrganisation criteria and the standard operatingprocedure for the reference EIA (Innis et al.,1989; World Health Organisation, 1997). JE wasdefined as a febrile illness associated with a de-crease in consciousness and the presence of IgMto JE virus in the CSF.
2.2. Serum samples
Serum from patients with a suspected dengueinfection was collected at the time of admission tohospital and at discharge from either the QueenSirikit National Institute of Child’s Health(Bangkok Children’s Hospital) or the KamphaengPhet Provincial Hospital, Thailand, and frozen at−70°C prior to assay. Paired sera from 20 pa-tients with dengue (10 primary and 10 secondaryinfections) were used in this study. The intervalbetween the collection of the first and second serain patients with dengue ranged from 1–6 days(mean 2.4 days). Paired sera from 10 patients withJapanese encephalitis (JE) were collected from theCentre for Tropical Diseases, Ho Chi Minh City,

A.J. Cuzzubbo et al. / Journal of Clinical Virology 16 (2000) 135–144 137
Vietnam. The interval between the collection ofthe first and second sera ranged from 3–11 days(mean 7 days). A panel of single sera from nonflavivirus infections was also included. These rep-resented widal felix test positive cases of typhoidfrom Malaysia (n=10), indirect immunoperoxi-dase positive cases of rickettsial scrub typhusfrom Thailand (n=10), and microscopic aggluti-nation test positive cases of leptospirosis fromAustralia (n=10).
2.3. PanBio Dengue Duo ELISA
The PanBio Dengue Duo IgM and IgG Cap-ture ELISA (Product Code DEC-100) was per-formed by AC at PanBio Pty Ltd according to themanufacturer’s instructions (tested once). Twomicrotitre plates were supplied, one containingstabilised dengue virus antigen types 1–4 (antigenplate) and the other containing either anti-humanIgM or anti-human IgG bound to separate mi-crowells (assay plate). Peroxidase labelled anti-dengue monoclonal antibody (125 ml/well) wasadded to the antigen plate to resuspend the anti-gens and form antibody–antigen complexes. Con-currently 100 ml/well of patient sera, diluted 1:100in the diluent provided, was added to the assayplate containing either bound anti-human IgM oranti-human IgG, and human IgM or IgG in thepatient’s sera was captured. Both plates were in-cubated for 1 h at room temperature (antigenplate) or 37°C (assay plate), after which time theassay plate was washed, and 100 ml/well anti-body–antigen complexes are transferred from theantigen plate to the assay plate. These complexeswere then captured by dengue specific IgM or IgGduring an incubation of 1 h at 37°C. The platewas then washed and bound complexes were visu-alized through the addition of a 100 ml/well te-tramethylbenzidine substrate. After 10 min,the reaction was stopped by the addition of100 ml/well 1 M phosphoric acid, and the stripswere read at 450 nm using a microtitre platereader.
Positivity was determined by comparison toIgM and IgG reference sera provided (cutoff cali-brators). A positive sample was defined as havinga sample:calibrator absorbance ratio ]1.0 and a
negative sample with a ratio B1.0. Dengue infec-tion was characterised by the elevation of eitherIgM or IgG, with a negative sample defined ashaving both IgM and IgG ratios B1.0. The cut-off sera in the IgG ELISA represented a HIA titreof 1:2560 — the titre used to distinguish sec-ondary dengue virus infection from primary orpast dengue virus infection (World Health Organ-isation, 1997).
2.4. Venture Technologies Dengue IgM and IgGDot Blot Tests
The Dot Blot tests were performed by AC atPanBio Pty Ltd according to the manufacturer’sinstructions. Each sera was tested once and theresults were read without knowledge of the clini-cal diagnosis or results of other tests. IgM wasdetermined using an antibody capture format as-say, while IgG was determined using an indirectformat assay. In the IgM Dot Blot, nitrocellulosemembrane coated with a spot of anti-humanIgM was incubated for 2 h at room temp-erature (RT, 23°C) in patient sera diluted 1:100 inthe diluent provided. After washing for 3×5 minin the buffer provided, the membrane wasincubated with dengue antigen overnight at 4°C.The membrane was washed again and then incu-bated with anti-dengue monoclonal antibody for1 h at RT before washing again and incubatingwith conjugate for 1 h at RT. After washing,reactivity was visualised by incubation of themembrane for 30 min at RT in the substratesolution provided. The reaction was stopped bywashing with distilled water after aspirating thesubstrate. In the IgG test, sera was sera wasdiluted 1:1000 in the diluent provided and incu-bated with membrane-bound dengue antigen for60 min at RT. After washing, conjugate wasadded for 60 min at room temperature to detectbound IgG and colour development was per-formed as described above. Dots produced bydifferent sera were compared to reactive and non-reactive controls, with any sign of colorinterpreted as a positive result. The dots werescored arbitrarily as negative, weak positive andpositive.
A.J. Cuzzubbo et al. / Journal of Clinical Virology 16 (2000) 135–144138
2.5. Data analysis
The proportion of patients with antibody levelsabove the designated cutoff for ELISA was deter-mined. The Fisher’s Exact Test was performed tocompare sensitivity, specificity and F-values.ANOVA was used to compare the mean assayvalues of different diagnostic groups. Statisticswere performed using Instat® (Graphpad Soft-ware Inc, San Diego, CA, USA).
3. Results
3.1. Sensiti6ity and specificity of IgM assays
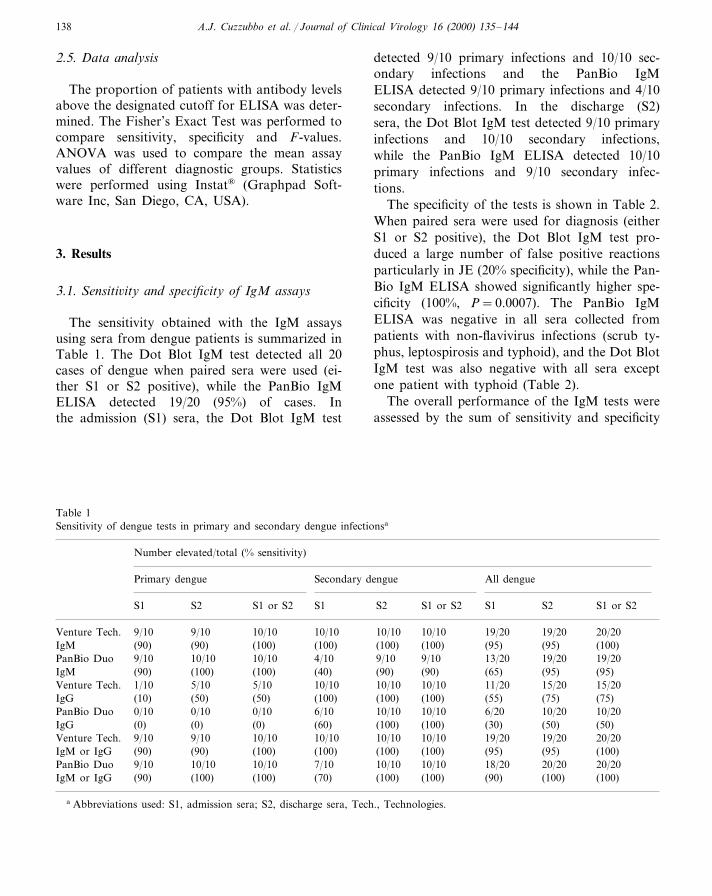
The sensitivity obtained with the IgM assaysusing sera from dengue patients is summarized inTable 1. The Dot Blot IgM test detected all 20cases of dengue when paired sera were used (ei-ther S1 or S2 positive), while the PanBio IgMELISA detected 19/20 (95%) of cases. Inthe admission (S1) sera, the Dot Blot IgM test
detected 9/10 primary infections and 10/10 sec-ondary infections and the PanBio IgMELISA detected 9/10 primary infections and 4/10secondary infections. In the discharge (S2)sera, the Dot Blot IgM test detected 9/10 primaryinfections and 10/10 secondary infections,while the PanBio IgM ELISA detected 10/10primary infections and 9/10 secondary infec-tions.
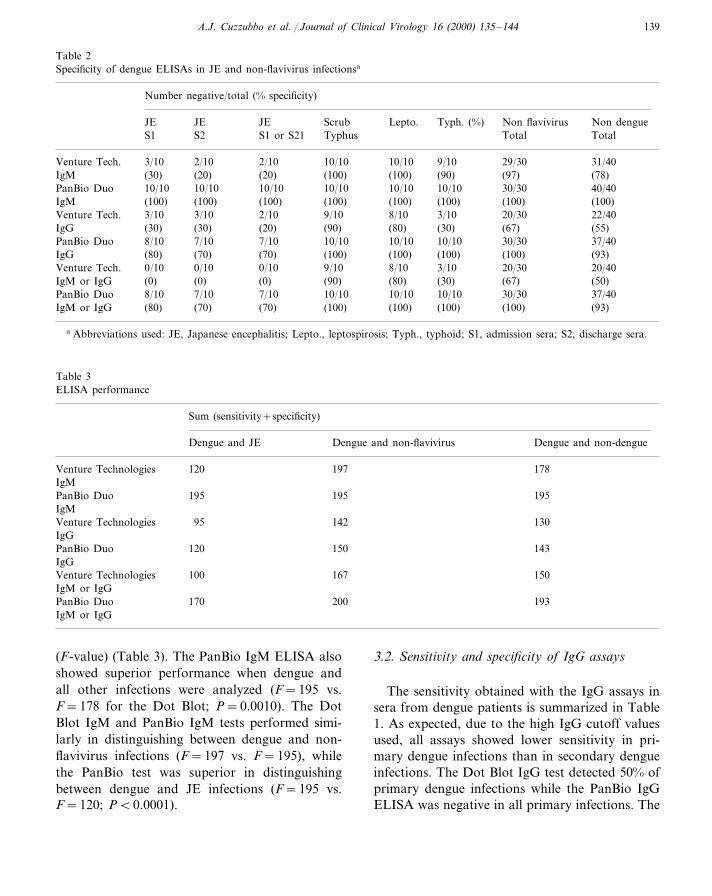
The specificity of the tests is shown in Table 2.When paired sera were used for diagnosis (eitherS1 or S2 positive), the Dot Blot IgM test pro-duced a large number of false positive reactionsparticularly in JE (20% specificity), while the Pan-Bio IgM ELISA showed significantly higher spe-cificity (100%, P=0.0007). The PanBio IgMELISA was negative in all sera collected frompatients with non-flavivirus infections (scrub ty-phus, leptospirosis and typhoid), and the Dot BlotIgM test was also negative with all sera exceptone patient with typhoid (Table 2).
The overall performance of the IgM tests wereassessed by the sum of sensitivity and specificity
Table 1Sensitivity of dengue tests in primary and secondary dengue infectionsa
Number elevated/total (% sensitivity)
All denguePrimary dengue Secondary dengue
S1 S2 S1 or S2 S1 S2 S1S1 or S2 S1 or S2S2
20/209/10 10/10 10/10 10/10 10/10Venture Tech. 19/209/10 19/20(100)(90) (100) (100) (100) (100)IgM (95)(90) (95)19/2019/2013/209/109/10PanBio Duo 4/1010/1010/109/10(95)IgM (100)(90) (100) (40) (90) (90) (65) (95)
Venture Tech. 15/2015/2011/2010/1010/1010/105/105/101/10(75)(55)(100)(100) (75)(100)(50)(50)(10)IgG
10/200/10 0/10 6/10PanBio Duo 10/100/10 10/10 6/20 10/20(0) (0) (0) (60)IgG (100) (100) (30) (50) (50)
Venture Tech. 9/10 9/10 10/10 10/10 10/10 10/10 19/20 19/20 20/20(90) (100)(95)(95)(100)(100)(90) (100)IgM or IgG (100)
9/10 10/10 10/10 7/10PanBio Duo 10/10 10/10 18/20 20/20 20/20(100)(90) (100)IgM or IgG (90)(100)(100)(70)(100)(100)
a Abbreviations used: S1, admission sera; S2, discharge sera, Tech., Technologies.
A.J. Cuzzubbo et al. / Journal of Clinical Virology 16 (2000) 135–144 139
Table 2Specificity of dengue ELISAs in JE and non-flavivirus infectionsa
Number negative/total (% specificity)
JE JE ScrubJE Lepto. Typh. (%) Non flavivirus Non dengueS2S1 S1 or S21 Typhus Total Total
2/10 2/10 10/10Venture Tech. 10/103/10 9/10 29/30 31/40IgM (30) (20) (20) (100) (100) (90) (97) (78)
10/10 10/10 10/10 10/10PanBio Duo 10/1010/10 30/30 40/40(100) (100) (100) (100)(100) (100)IgM (100) (100)3/10 2/10 9/10 8/10Venture Tech. 3/103/10 20/30 22/40(30) (20) (90) (80)(30) (30)IgG (67) (55)
8/10PanBio Duo 7/10 7/10 10/10 10/10 10/10 30/30 37/40(70) (70) (100) (100)(80) (100)IgG (100) (93)
0/10Venture Tech. 0/10 0/10 9/10 8/10 3/10 20/30 20/40IgM or IgG (0)(0) (0) (90) (80) (30) (67) (50)
7/10 7/10 10/10 10/108/10 10/10PanBio Duo 30/30 37/40(70) (70) (100)IgM or IgG (100)(80) (100) (100) (93)
a Abbreviations used: JE, Japanese encephalitis; Lepto., leptospirosis; Typh., typhoid; S1, admission sera; S2, discharge sera.
Table 3ELISA performance
Sum (sensitivity+specificity)
Dengue and non-flavivirus Dengue and non-dengueDengue and JE
Venture Technologies 120 197 178IgM
195195 195PanBio DuoIgM
142 130Venture Technologies 95IgG
150PanBio Duo 143120IgG
100Venture Technologies 167 150IgM or IgG
170PanBio Duo 200 193IgM or IgG
(F-value) (Table 3). The PanBio IgM ELISA alsoshowed superior performance when dengue andall other infections were analyzed (F=195 vs.F=178 for the Dot Blot; P=0.0010). The DotBlot IgM and PanBio IgM tests performed simi-larly in distinguishing between dengue and non-flavivirus infections (F=197 vs. F=195), whilethe PanBio test was superior in distinguishingbetween dengue and JE infections (F=195 vs.F=120; PB0.0001).
3.2. Sensiti6ity and specificity of IgG assays
The sensitivity obtained with the IgG assays insera from dengue patients is summarized in Table1. As expected, due to the high IgG cutoff valuesused, all assays showed lower sensitivity in pri-mary dengue infections than in secondary dengueinfections. The Dot Blot IgG test detected 50% ofprimary dengue infections while the PanBio IgGELISA was negative in all primary infections. The

A.J. Cuzzubbo et al. / Journal of Clinical Virology 16 (2000) 135–144140
Dot Blot test produced a positive result with allS1 and S2 sera from secondary dengue, while thePanBio ELISA produced positive results with 6/10 (60%) S1 sera and all ten S2 sera.
The specificity of the IgG ELISAs is shown inTable 2. When paired sera were used for diagnosis(either S1 or S2 positive), the Dot Blot IgG testproduced a number of false positive reactionswith sera from JE patients (20% specificity); whilethe PanBio IgG ELISA showed higher specificity(70%; P=0.0698). The PanBio IgG ELISA wasnegative with all sera collected from patients withnon-flavivirus infections, while the Dot Blot IgGtest produced false positive reactions in patientswith scrub typhus (90% specificity), leptospirosis(80% specificity) and typhoid (30% specificity)(Table 2).
The overall performance of the IgG tests wasassessed by the sum of the sensitivity and specific-ity (F-value) (Table 3). The F-values for the IgGtests were lower than the IgM tests (Table 3) dueto the poor sensitivity of the IgG tests in primarydengue (Table 1).
3.3. The combined use of IgM and IgG assays
The sensitivity obtained if detection of eitheranti-dengue IgM or IgG was regarded as a posi-tive result is summarized in Table 1. Both PanBioand Venture Technologies assays showed highsensitivity in dengue infections. The Dot Blot andPanBio tests detected all twenty dengue infectionsusing paired sera. The combined use of the IgMand IgG Dot Blot tests gave false positive resultsin sera from all JE patients (0% specificity), whilethe PanBio Duo ELISA showed significantlyhigher specificity (70%; P=0.0031). All sera col-lected from patients with non-flavivirus infectionswere negative in the PanBio Duo ELISA (100%specificity), while the combined use of the DotBlot IgG and IgM tests showed a significant rateof false positive reactions with sera from patientswith scrub typhus (90% specificity), leptospirosis(80% specificity) and typhoid (30% specificity)(P=0.0008) (Table 2). The overall specificity inthe PanBio Duo ELISA was 93%, while in theDot Blot IgM and IgG tests specificity was 50%(PB0.0001).
The overall performance of the IgM/IgG com-bination was assessed by the sum of the sensitivityand specificity (F-value) (Table 3). The PanBiotests showed superior performance to the dot blottests when dengue was compared to either JE ornon-flavivirus infections (PB0.0001 for both).
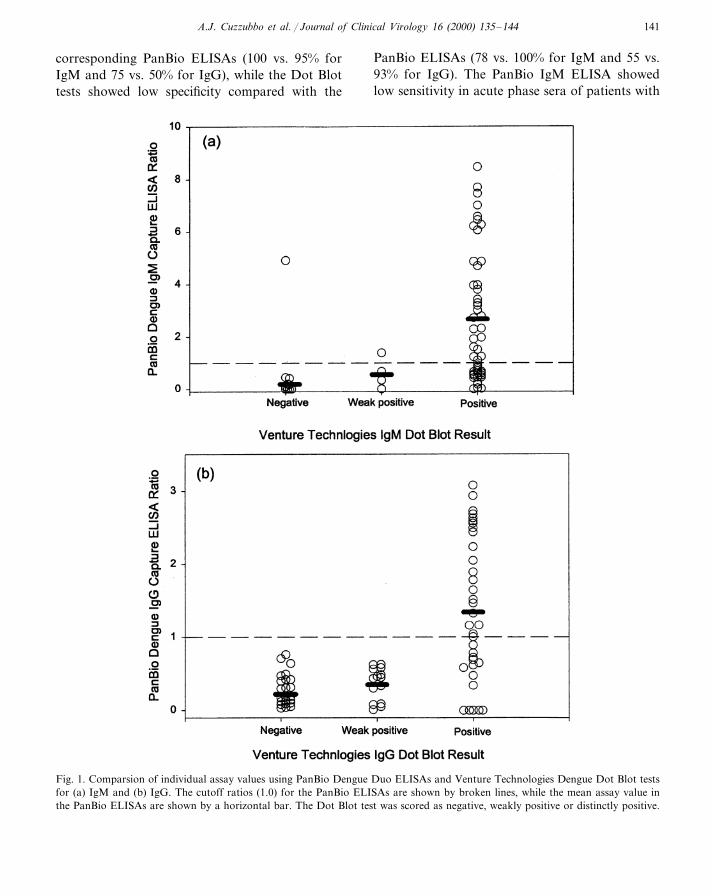
3.4. Correlation analysis
The individual results of the Dot Blot andELISA were well correlated using either the IgMor IgG tests (Fig. 1). There was a significantassociation between the mean ELISA ratio andthe Dot Blot score (ANOVA: F=18.52, PB0.0001 for IgM; F=27.30, PB0.0001 for IgG).However, it was apparent that many ELISA nega-tive samples were positive in the Dot Blot test,suggesting that the cutoffs used in the Dot Blottests were set below that of the ELISAs.
4. Discussion
IgM is the marker of choice in dengue diagno-sis, but some patients with secondary dengue havebeen reported to produce low or undetectablelevels of IgM, and the IgM response in somesecondary cases may be slow and short lived(Ruechusatawat et al., 1994; Innis, 1997; Vaughnet al., 1997; Vorndam and Kuno, 1997). To over-come this, it has been suggested that IgG be usedas an adjunct to IgM, with the cutoff level set todetect high levels of IgG characteristic of sec-ondary dengue but not primary or past denguevirus infection (Innis et al., 1989; Ruechusatawatet al., 1994; Vaughn et al., 1998). In this study,two commercial tests for both IgM and IgG werecompared (PanBio Dengue Duo IgM and IgGCapture ELISA and the Venture TechnologiesIgM and IgG Dot Blot).
The PanBio Dengue Duo ELISA gave the bestdistinction between dengue and other infections,as judged by the sum of sensitivity and specificity.The PanBio and Venture Technologies’ assaysdetected all dengue virus infections, but the Pan-Bio Duo ELISA showed superior specificity (93vs. 50%). The Venture Technologies IgM and IgGDot Blot tests showed higher sensitivity than the
A.J. Cuzzubbo et al. / Journal of Clinical Virology 16 (2000) 135–144 141
corresponding PanBio ELISAs (100 vs. 95% forIgM and 75 vs. 50% for IgG), while the Dot Blottests showed low specificity compared with the
PanBio ELISAs (78 vs. 100% for IgM and 55 vs.93% for IgG). The PanBio IgM ELISA showedlow sensitivity in acute phase sera of patients with
Fig. 1. Comparsion of individual assay values using PanBio Dengue Duo ELISAs and Venture Technologies Dengue Dot Blot testsfor (a) IgM and (b) IgG. The cutoff ratios (1.0) for the PanBio ELISAs are shown by broken lines, while the mean assay value inthe PanBio ELISAs are shown by a horizontal bar. The Dot Blot test was scored as negative, weakly positive or distinctly positive.

A.J. Cuzzubbo et al. / Journal of Clinical Virology 16 (2000) 135–144142
secondary dengue infections (40%). However, sig-nificant levels of anti-dengue IgG antibody wasdetected in sera from many of these patients withthe PanBio IgG ELISA (overall sensitivity of IgMand IgG combination in S1 sera was 70%). Simi-lar results using the PanBio Dengue Duo ELISAhave been reported previously (Lam and Devine,1998; Sang et al., 1998b; Vaughn et al., 1999).
The low specificity of the Venture TechnologiesIgM Dot Blot was due mainly to false positivereactions with sera from JE patients. High levelsof cross-reactivity (80%) have been reported previ-ously using the Dot Blot test when CSF and serafrom flavivirus infections other than dengue (JEand yellow fever) were used (Kuno et al., 1998).In addition, another study with the Dot Blot IgMtest showed high levels of cross reactivity (23%) insera collected from patients with malaria (Lam etal., 1996). Apart from the differences in cutoffvalues, the differences observed between the twoassays with sera from JE infections may havebeen due to the differences in incubation timesand procedures used in these two tests. In the DotBlot IgM test antigen was incubated overnightwith captured IgM, while the PanBio IgM ELISAantigen was incubated for only 1 h with capturedantibody. It is possible the longer incubation timeused in the Dot Blot IgM test led to capture ofdengue antigen by lower affinity IgM producedduring JE infection. Alternatively, differences inthe timing of conjugate addition in the two assaysmay affect the binding of dengue antigen to anti-JE IgM. That is, in the Dot Blot IgM test conju-gated monoclonal antibody is added after thebinding of antigen by captured IgM, while in thePanBio test dengue antigen and conjugate arecomplexed before incubation in the capture plate.The latter method has been reported previously tohalve the number of incubation steps required inthe dengue IgM capture ELISA without affectingthe correlation of the assay with HAI (Chong etal., 1994).
The Venture Technologies IgG Dot Blot testproduced false positive reactions with sera col-lected from patients with JE (80%), scrub typhus(10%), leptospirosis (20%) and typhoid (70%).High levels of cross reactivity (29%) have alsobeen reported previously in patients with rubella
infections (Lam, 1993). These studies highlight theimportance of selecting appropriate serum panelswhen evaluating dengue diagnostic assays. Of par-ticular importance are other flavivirus infections(e.g. JE, yellow fever) and non-flavivirus infec-tions with similar clinical presentation (e.g. scrubtyphus, typhoid, leptospirosis and perhapsrubella).
Comparison of the individual assay values re-vealed that the cutoffs used in the IgM and IgGDot Blot tests were set below those used in thecorresponding PanBio ELISAs. This resulted inbetter sensitivity but much poorer specificity inthe Dot Blot tests. Similarly, another study con-cluded that the cutoff of the Dot Blot IgM testwas too low and it was shown that a higher cutoffvalue would have improved performance (Kunoet al., 1998). The inverse relationship betweensensitivity and specificity has been well docu-mented (Metz, 1978; Greiner et al., 1995; Xu etal., 1997). Consequently, manufacturer’s of com-mercial assays need to set the cut-off to maximizesensitivity and/or specificity, depending on thetarget disease. One method that has been sug-gested regarding cut-off determination is to maxi-mize the combined sensitivity and specificity(F-value) (Greiner et al., 1995; Xu et al., 1997). Inthis study the PanBio Dengue Duo ELISAshowed superior performance (highest F-value) indistinguishing between dengue and other infec-tions and this was significantly higher than theF-value obtained with the Dot Blot tests.
Measurement of the relative levels of anti-dengue IgM and IgG has been suggested previ-ously to be useful in distinguishing betweenprimary and secondary dengue virus infections(Innis et al., 1989; Ruechusatawat et al., 1994;Vaughn et al., 1998). By employing this approach,the PanBio Dengue Duo ELISA has a high pre-dictive value in distinguishing between primaryand secondary dengue virus infections (Devine etal., 1997; Lam and Devine, 1998; Sang et al.,1998b; Vaughn et al., 1999). In this study, serafrom all primary dengue infections assayed withthe PanBio Duo ELISA contained anti-dengueIgM but not anti-dengue IgG, while all secondarydengue virus infections detected in the PanBio testwere IgG positive. In contrast, the Dot Blot test
A.J. Cuzzubbo et al. / Journal of Clinical Virology 16 (2000) 135–144 143
could not be used for this purpose as 50% ofprimary dengue infections and all secondarydengue infections showed elevation of both IgMand IgG. Similarly, 29% of primary dengue caseshave been detected when the IgG Dot Blot testwas used in another study (Lam, 1993) and thisrose to 61% when paired sera were used fordiagnosis of primary dengue virus infections (Car-dosa and Tio, 1991).
The pattern of IgM and IgG reactivity detectedwith the PanBio ELISA could also be used todistinguish between dengue and other infectionssince 19/20 (95%) of dengue patients showed ele-vation of IgM, while patients with non-dengueinfections (including JE) did not show elevation ofIgM. Consequently, a positive IgM test in thePanBio Dengue Duo ELISA had a positive pre-dictive value of 100% for dengue virus infectionand cross-reactivity was only of concern in theminority of patients with dengue virus infectionwho were IgM negative, IgG positive. In contrast,the Dot Blot test could not be used in this waysince cross-reactivity was observed in both IgMand IgG tests.
The ELISA and Dot Blot tests described herehave utility as aids in the diagnosis of denguevirus infections. The ELISA is particularly suitedto the diagnostic pathology laboratory where au-tomated equipment is available. In addition, theELISA is rapid and simple to perform, largenumbers of samples can be accommodated easilyand interpretation of results is more objectivethan the Dot Blot test. Similar problems with theDot Blot test have been reported previously (Lamet al., 1996). However, the Dot Blot test is moreappropriate in a field setting as it does not requiresophisticated equipment. Another commerciallyavailable test for dengue has been described thatis also well suited to this application (Devine etal., 1997; Lam and Devine, 1998; Sang et al.,1998a; Vaughn et al., 1998). The dot blot test mayalso have utility in areas of low dengue prevalence(e.g. returning travellers from non-endemic areas)since higher sensitivity is needed. However, trialswith asymptomatic donors and appropriate dis-ease controls from these regions would be neededto confirm this.
Acknowledgements
This work was supported by the US ArmyMedical Research and Materiel Command andPanBio Pty, Ltd (Brisbane, Australia) through aco-operative research and development agree-ment. The opinions or assertions contained hereinare the private ones of the authors and are not tobe construed as official or as reflecting the viewsof the US Government. The Dengue Duo ELISAwas developed through an Australian Govern-ment sponsored Cooperative Research Centre forDiagnostic Technologies.
We thank Ms Panor Srisongkram for perform-ing the AFRIMS reference ELISA; Mr MingChoohong for performing the hemagglutinationinhibition assay; Dr Rachel Kneen for specimenand data management; Ms Tipawan Kungvanrat-tana for data entry; and the Directors and staff ofthe Queen Sirikit National Institute of Child’sHealth and the Centre for Tropical Diseases, andProfessor Nicholas White for their support. Wealso thank Dr George Watt, Department ofMedicine, AFRIMS, Bangkok, Thailand for theprovision of sera from patients with rickettsialscrub typhus; Mr William Winslow, Institute forMedical and Veterinary Science, Adelaide, Aus-tralia for the provision of sera and MAT resultsfrom patients with leptospirosis; and Dr RodneyJones, Gribbles Pathology, Kuala Lumpur,Malaysia, for the provision of Widal felix positivesera from patients with typhoid.
References
Cardosa MJ, Tio PH. Dot enzyme immunoassay: as alterna-tive diagnostic aid for dengue fever and dengue haemor-rhagic fever. Bull WHO 1991;69:741–5.
Cardosa MJ, Baharudin F, Hamid S, Hooi TP, NimmanityaS. A nitrocellulose membrane based IgM capture enzymeimmunoassay for etiological diagnosis of dengue virusinfections. Clin Diagn Virol 1995;3:343–50.
Chong CF, Ngoh BL, Tan HC, Yap EH, Singh M, Chan L,Chan YC. A shortened dengue IgM capture ELISA usingsimultaneous incubation of antigen and peroxidase-labeledmonoclonal antibody. Clin Diagn Virol 1994;1:335–41.
Devine P, Cuzzubbo A, Marlborough D. Dengue fever testing.Today’s Life Sci 1997;9:26–30.
A.J. Cuzzubbo et al. / Journal of Clinical Virology 16 (2000) 135–144144
Greiner M, Sohr D, Gobel P. A modified ROC analysis forthe selection of cut-off values and the definition of interme-diate results of serodiagnostic tests. J Immunol Methods1995;185:123–32.
Gubler DJ. Serological diagnosis of dengue haemorrhagicfever. Dengue Bull 1996;20:20–3.
Innis BL, Nisalak A, Nammanitya S, Kusalerdchariya S,Chongswasdi V, Suntayakorn S, Puttisri P, Hoke CH. Anenzyme-linked immunosorbant assay to characterisedengue infections where dengue and Japanese encephalitiscocirculate. Am J Trop Med Hyg 1989;40:418–27.
Innis B. Antibody responses to dengue virus infection. In:Gubler DJ, Kuno G, editors. Dengue and Dengue Haem-orrhagic Fever. New York: CAB International, 1997:221–43.
Kuno G, Gomez I, Gubler DJ. An ELISA procedure for thediagnosis of dengue infections. J Virol Methods1991;33:101–13.
Kuno G, Cropp CB, Wong-Lee J, Gubler DJ. Evaluation ofan IgM Immunoblot kit for dengue diagnosis. Am J TropMed Hyg 1998;59:757–62.
Lam SK. Rapid dengue diagnosis and interpretation. Malays JPathol 1993;15:9–12.
Lam SK, Fong MY, Chungue E, Doraisingham S, Igarashi A,Khin MA, Kyaw ZT, Nisalak A, Roche C, Vaughn DW,Vorndam V. Multicentre evaluation of dengue IgM dotimmunoassay. Clin Diagn Virol 1996;7:93–8.
Lam SK, Devine PL. Evaluation of capture ELISA and rapidimmunochromatographic test for the determination of IgMand IgG antibodies produced during dengue infection. ClinDiagn Virol 1998;10:75–81.
Metz CE. Basic principles of ROC analysis. Semin Nucl Med1978;8:283–98.
Ruechusatawat K, Morita K, Tanaka M, Vongcheree S, Ro-janasuphot S, Warachit P, Kanai K, Thongtradol P, Nim-nakorn P, Kanungkid S, Igarashi A. Daily observation ofantibody levels among dengue patients detected by en-
zyme-linked immunosorbent assay (ELISA). Jpn J TropMed Hyg 1994;22:9–12.
Sang CT, Lim SH, Cuzzubbo A, Devine PL. Clinical evalua-tion of rapid immunochromatographic test for the diagno-sis of dengue infection. Clin Diagn Lab Immunol1998a;5:407–9.
Sang CT, Cuzzubbo A, Devine PL. Evaluation of commercialcapture enzyme-linked immunosorbent assay for the detec-tion of Immunoglobulin M (IgM) and IgG antibodiesproduced during dengue infection. Clin Diagn Lab Im-munol 1998b;5:710.
Vaughn DW, Green S, Kalayanarooj S, Innis BL, Nirnman-nitya S, Suntayakorn S, Rothman AL, Ennis FA, NisalakA. Dengue in early febrile phase: viremia and antibodyresponses. J Infect Dis 1997;176:322–30.
Vaughn DW, Nisalak A, Kalayanarooj S, Solomon T, DungNM, Cuzzubbo A, Devine PL. Evaluation of rapid im-munochromatographic test for diagnosis of dengue virusinfection. J Clin Microbiol 1998;36:234–8.
Vaughn DW, Nisalak A, Kalayanarooj S, Solomon T,Kalayanarooj S, Dung NM, Kneen R, Cuzzubbo A, De-vine PL. Rapid serological diagnosis of dengue virus infec-tion using a commercial capture enzyme-linkedimmunosorbent assay that distinguishes primary and sec-ondary infections. Am J Trop Med Hyg 1999;60:693–98.
Vorndam V, Kuno G. Laboratory diagnosis of dengue virusinfections. In: Gubler DJ, Kuno G, editors. Dengue andDengue Haemorrhagic Fever. New York: CAB Interna-tional, 1997:313–33.
World Health Organisation. Dengue haemorrhagic fever diag-nosis, treatment, prevention and control. Geneva: WHO,1997.
Xu H, Lohr J, Greiner M. The selection of ELISA cut-offpoints for testing antibody to Newcastle disease by two-graph receiver-operating characteristic (TG-ROC) analysis.J Immunol Methods 1997;13:61–4.
.





















![IGM janfeb11-Ipatov[1]](https://img.dokumen.tips/doc/110x75/63457d2b596bdb97a908f42a/igm-janfeb11-ipatov1.jpg)







