Embed Size (px)
Citation preview

Orbital recurrence of retinoblastoma followingenucleation
J W Kim,1 V Kathpalia,1 I J Dunkel,2 R K Wong,1 E Riedel,3 D H Abramson1
1 Ophthalmic Oncology Service,Memorial Sloan-KetteringCancer Center, New York, USA;2 Department of Pediatrics,Memorial Sloan-KetteringCancer Center, New York, USA;3 Department of Epidemiologyand Biostatistics, MemorialSloan-Kettering Cancer Center,New York, USA
Correspondence to:Dr J W Kim, OphthalmicOncology Service, MemorialSloan-Kettering Cancer Center,1275 York Ave, New York, NY10021, USA;[email protected]
Presented at the InternationalSociety of Ocular Oncology, 27June 2007, Siena, Italy andAmerican Academy ofOphthalmology Annual Meeting12 November 2007, NewOrleans, LA, USA.
Accepted 6 August 2008Published Online First29 August 2008
ABSTRACTBackground/aims: To determine the incidence, clinicalpresentation and histopathological profile of patientsdeveloping orbital recurrence following enucleation forretinoblastoma.Methods: A cohort of 1674 consecutive patientsundergoing enucleations between 1914 and 2006 wasretrospectively reviewed to identify cases of orbitalrecurrence. A detailed chart review of all identifiedpatients with orbital recurrence following enucleation wasperformed. The main outcome measures were histo-pathological features of the enucleated globe, clinicalpresentation, status of metastatic disease and clinicaloutcomes of treatment at last follow-up.Results: There were 71 cases of orbital recurrenceidentified in the study, for an incidence of 4.2% (71 of1674 cases). The diagnosis of orbital recurrence wasmade between 1 and 24 months after enucleation (mean6 months), with 69 of the 71 patients (97%) beingdiagnosed within the first 12 months. Over a follow-upperiod of 3–208 months (mean 34.8 months), 60 of 71patients developed metastatic disease (85%), and 53 of71 patients died from metastatic retinoblastoma (75%).For the subgroup of cases diagnosed as having orbitalrecurrences after 1984, 10 of 11 patients (91%) are aliveand well.Conclusions: All patients undergoing enucleation forretinoblastoma need to be followed carefully for the first2 years after surgery for the possibility of orbital relapse.The majority of retinoblastoma patients with orbital tumourrecurrence develop systemic metastatic disease, althoughmortalities appear to be improving in the modern era.
Retinoblastoma is the most common primaryintraocular cancer in the paediatric population.Survival rates for retinoblastoma patients varywidely between modernised and developingnations, with figures as high as 90–98% in theUnited States and Europe and as low as 24% insome African countries.1–6 The reported disparitybetween survival rates has been attributed to theadvanced stage of diagnosis in less industrialisednations, often in the form of orbital retinoblas-toma. Whereas orbital disease may be observed inup to 50% of newly diagnosed cases in poornations,5 7 orbital retinoblastoma is not as com-monly encountered in developed countries, withan incidence of 5.0–9.5% reported from severallarge referral centres.8–10 Patients with orbitalretinoblastoma are thought to have a poorsystemic prognosis, with mortalities reaching 90–100% of biopsy-confirmed cases.10–12 Such discoura-ging survival rates are comparable with the highdeath figures for retinoblastoma patients reportedby Hirschberg in 1869,13 suggesting that little
progress has been made in managing patients withthe orbital form of the disease.
As pointed out by Ellsworth in 1974, orbitalretinoblastoma may be diagnosed when a patientpresents with extraocular disease or as a form oflocal recurrence following enucleation.10 When apatient presents with intraocular retinoblastoma,primary enucleation is thought to offer cure ratesof 90–95%.14 15 Orbital tumour recurrence follow-ing enucleation is considered a relatively rarecomplication, although its true incidence has onlybeen estimated.8 16 There have also been efforts todemonstrate an association between certain histo-pathological features of enucleated eyes and therisk for local and systemic relapse, although aconsensus on these putative risk factors is lack-ing.9 15–19 Other than isolated case reports, fewstudies have described the clinical profiles ofpatients who present with an orbital tumourrecurrence after an uncomplicated enucleation.20 21
The aim of our study was to systemically analysethe clinical and histopathological features ofpatients developing orbital relapse following enu-cleation for retinoblastoma. To examine this groupof patients, we reviewed the clinical, radiographicand pathological data of orbital recurrence casesidentified from a large series of retinoblastomapatients undergoing enucleations at our institu-tion.
MATERIALS AND METHODSWe examined the records of enucleated cases fromthe registry of retinoblastoma patients at theMemorial Sloan-Kettering Cancer Center to iden-tify cases of orbital tumour recurrence. Thedatabase is also maintained by the NationalCancer Institute (NCI) and includes all casesenucleated by our service from 1914 to 2006. Allcases with extraocular disease diagnosed at pre-sentation by clinical examination or radiographiccharacteristics were excluded. The enucleationtechnique utilised by our service has been describedpreviously.22 23 Approval for this retrospectivestudy was obtained from the InstitutionalReview Board at the Memorial Sloan-KetteringCancer Center.
Once the cases were identified, both demo-graphic and pathological data were collected froma retrospective chart review. Results of thesystemic metastatic work-up (at the time of orbitalrecurrence diagnosis) were classified as follows: (1)metastatic disease (any evidence of retinoblastomaoutside the orbit), (2) bone disease (evidence ofretinoblastoma involving the bone or bone marrowand (3) central nervous system (CNS) disease(evidence of retinoblastoma in the intracranial
Clinical science
Br J Ophthalmol 2009;93:463–467. doi:10.1136/bjo.2008.138453 463
group.bmj.com on August 31, 2014 - Published by bjo.bmj.comDownloaded from

cavity or spinal column). For each patient, the predominantsymptom(s) or sign(s) that led to the diagnosis of orbitalrecurrence was recorded in the following categories: (1) localorbital or socket signs or symptoms (ie, proptosis, eyelidswelling, or problems with the prosthesis), (2) orbital or socketmass noted on routine examination by the physician, (3) eyelidecchymosis or bleeding from the socket, (4) non-localisingsymptoms such as lethargic behaviour, fever or other constitu-tional complaints and (5) contralateral orbit/ocular signs orsymptoms. In bilateral enucleation cases, both surgical dateswere recorded, and the side of orbital recurrence was noted.
RESULTSThere were 71 biopsy-confirmed cases of orbital recurrenceidentified in the study. The overall incidence of orbitalrecurrence following enucleation for retinoblastoma was 4.2%(71 cases/1674 enucleated patients) (table 1). A subgroupanalysis revealed that the incidence of orbital recurrence before1960 was 5.0%, whereas the incidence after 1960 was 4.0%,suggesting a possible decrease in the incidence of orbitalrecurrence in the modern era. However, when the incidencewas calculated for approximate 20-year periods, the rate variedbetween 3.7 and 5.1% (table 1), without any apparent down-ward trend in incidence over time.
The clinical profiles of the orbital recurrence cases arepresented in table 2. The age of retinoblastoma diagnosis forthe 71 cases ranged between 1 and 78 months (mean23.1 months); there were 34 bilateral retinoblastoma cases and37 unilateral retinoblastoma cases. Among the 71 identifiedpatients with orbital recurrences, there were 93 enucleatedglobes (22 bilateral enucleations), and histopathological datawere available for 77 globes (both partial and complete). Whenthe pathological report was absent or there was no specificcomment regarding a risk category (optic nerve invasion,choroidal invasion, sclera invasion), the globe was marked as‘‘data not available’’ for that histopathological feature. A reviewof the histopathological data of the enucleated eyes showed thefollowing: 35 specimens had confirmed evidence of optic nerveinvasion past the lamina cribrosa (negative in 35 globes, datanot available in 23 globes), and seven of these eyes had a positiveoptic nerve margin. Two globes had confirmed evidence oftumour erosion into or through the sclera (negative in 73 globes,data not available in 18 globes), and 32 globes demonstratedchoroidal invasion (negative in 34 globes, data not available in27 globes). There were 11 cases of orbital recurrence (with dataavailable in all three categories) that demonstrated no evidenceof optic nerve invasion, choroidal invasion or scleral invasion.
Table 3 demonstrates the clinical outcomes of the 71retinoblastoma patients with orbital tumour recurrences. Thediagnosis of orbital recurrence was made between 1 and24 months after enucleation (average 6 months), with 69 ofthe 71 patients being diagnosed within the first 12 months. The
patient that had the longest time period between the enuclea-tion and orbital recurrence was case 29; this was a bilateral case,with the ipsilateral side being enucleated 24 months prior to theorbital recurrence and the contralateral side being enucleated3 months before the orbital recurrence. Overall, metastaticwork-up performed at the time of orbital recurrence diagnosisrevealed that 44 of 71 cases had evidence of systemic disease(62%); at the end of the follow-up period, 60 of 71 cases haddeveloped metastatic disease (85%). The total length of follow-up was determined from the date of diagnosis to the lastexamination in the chart or the date of death due to metastaticdisease; the range of follow-up in this group of patients was 3–208 months (average 34.8 months). During the period offollow-up, 61 of the 71 cases died (86%). However, there wereeight cases in this group of 61 patients who survived more than2 years (after orbital recurrence diagnosis), and four of the eightcases were confirmed to have mortality related to secondcancers. Assuming that a survival of .24 months is equivalentto a cure, the adjusted metastatic death rate was determined tobe 53 of 71 cases (75%). For the subgroup of patients diagnosedas having orbital recurrences after 1984, 10 of 11 cases are aliveand well (as of the last follow-up date).
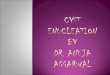
Table 4 displays the clinical presentations of patientsdiagnosed as having orbital recurrences. For the group of 71patients, the most common presentation was a local symptomor sign related to a mass lesion in the orbit, such as eyelidswelling, an ill-fitting prosthesis, visible mass or proptosis (33cases). The second most common category was a diagnosismade on routine examination during a scheduled follow-upappointment; typically an asymptomatic mass was visualised orpalpated in the socket after removal of the prosthesis (23 cases).Other patients were diagnosed during a work-up of non-localising, constitutional symptoms such as lethargy, somno-lence, fever, anorexia or headache, prompting a clinicalexamination of the socket or a neuroimaging study which ledto the diagnosis (seven cases). Other patients presented withbleeding from the socket or eyelid ecchymosis (five cases) (figs 1,2). Finally, three patients presented with proptosis or eyelidswelling involving the contralateral orbit.
DISCUSSIONIn 1974, Ellsworth reported the largest series of patients withorbital retinoblastoma, when he described 110 cases with orbitaldisease identified from the database of patients treated at theEdward S. Harkness Eye Institute in New York.10 In thatlandmark paper, 110 patients were identified from a total seriesof 1160 cases of retinoblastoma, for an overall incidence of 9.5%.Published under the rubric of ‘‘orbital retinoblastoma,’’Ellsworth included patients who presented with obvious orbitaldisease on clinical examination or on radiographic imaging,cases with an extraocular mass encountered at the time ofenucleation, orbital extension diagnosed only on histopathologyand finally patients with orbital relapse following enucleationfor intraocular disease. Because this latter group of patients hastraditionally been categorised with cases presenting withextraocular disease, the exact incidence of orbital recurrencefollowing enucleation has been difficult to estimate. In 1987,Hungerford et al reported an incidence of 5% for orbitalretinoblastoma in a group of 317 children referred forretinoblastoma, although they acknowledged that some ofthese cases already had extraocular disease at presentation.8
Khelfaoui et al reported a slightly higher incidence of 7.6% in172 enucleated eyes, although again, some of these cases werereferred for extraocular disease and had evidence of metastasis
Table 1 Incidence of orbital recurrence following enucleation
Time Enucleated patients Recurrences Incidence (%)
1910–1929 27 1 3.7
1930–1949 157 8 5.1
1950–1969 717 32 4.5
1970–1989 551 19 3.4
1990–2006 222 11 4.9
Before 1960 462 23 5.0
1960 and after 1212 48 4.0
Totals 1674 71 4.2
Clinical science
464 Br J Ophthalmol 2009;93:463–467. doi:10.1136/bjo.2008.138453
group.bmj.com on August 31, 2014 - Published by bjo.bmj.comDownloaded from

at presentation.9 The analysis of 1674 patients enucleated byour service from 1914 to 2006 showed an orbital relapse rate of4.2%, which may be more accurate than previous reports due tothe large number of patients in our series and the inclusion ofonly biopsy-confirmed cases of orbital recurrence followingenucleation. However, it should be acknowledged that ourstudy may have included cases with subclinical orbital disease atthe time of enucleation, since there were seven cases with apositive optic nerve margin and two cases with scleral invasion.A subgroup analysis did not reveal a downward trend inincidence over time (for 20-year periods), suggesting that therate of orbital recurrence has remained relatively constant in ourdatabase of patients undergoing enucleations. Interestingly,several groups have published smaller series of enucleatedpatients treated with prophylactic chemotherapy with muchlower rates of orbital recurrence, suggesting that adjuvanttherapy of patients with ‘‘high-risk’’ histopathological featuresfollowing enucleation may decrease this type of tumourrelapse.15 19 Our retrospective study was not designed to analysethe issue of prophylactic chemotherapy and whether adjuvanttreatment decreases the incidence of orbital relapse, animportant issue which can only be addressed with a prospective,randomised study.
In our group of 71 cases, the timing of the orbital tumourrecurrence following enucleation was always within the first2 years after surgery, with approximately 97% of patientspresenting within the initial 12 months (69 of 71). The shortinterval for the development of this complication was alsodescribed by Ellsworth10, and Hungerford et al found that themean interval from enucleation to orbital recurrence in theirseries was 6.7 months.8 The most common presentation was aclinical complaint such as eyelid swelling or chemosis, suggest-ing that clinicians should not attribute periocular or orbitalsymptoms during the first year after enucleation as a sign of abenign conjunctivitis or preseptal cellulitis. A problem with theocular prosthesis was also a frequent mode of presentation inthese patients, and extrusion or displacement of a previouslysatisfactory prosthesis should be considered a suspicious sign forpossible tumour recurrence. In the socket, the characteristic
lesion was a subconjunctival mass with a purplish hue, due tothe prominent vascularity of the tumour mass.24 The vascularitymay also explain the finding of periocular ecchymosis or frankbleeding from the socket in five patients. A significant numberof patients were also diagnosed on routine examinations, andthe practice of removing the prosthesis in asymptomaticpatients during follow-up evaluations seems justified, particu-larly within the first 2 years after enucleation. There were sevenpatients with non-localising signs that eventually led to thediagnosis of orbital tumour recurrence, and several patientspresented with a mass lesion in the contralateral orbit,reinforcing the importance of being vigilant for unusualsymptoms in patients with a history of retinoblastoma.
Our study confirms the findings of Ellsworth and Hungerfordet al that retinoblastoma patients with tumour recurrence in theorbit are likely to have other sites of extraocular relapse.8 10 Inour series, 75% of patients with orbital recurrence eventuallydied from systemic metastatic disease. Ellsworth reported anoverall survival rate of only 9.4% for patients with biopsy-confirmed orbital retinoblastoma, although this figure includedpatients who presented initially with extraocular disease.10 InHungerford’s series of orbital recurrence cases diagnosedbetween 1970 and 1984, only one of 16 patients survived(6%).8 In our series, 91% of patients diagnosed as having anorbital tumour recurrence after 1984 are alive and well. Theimproved survival data for patients with orbital retinoblastomain the last two decades can be attributed to the aggressivesystemic approach implemented by our group in the 1980s.Ellsworth was the first to recognise the value of systemicchemotherapy in improving the survival of patients with orbitalretinoblastoma.10 In Hungerford et al’s series of 16 patients withorbital recurrences, the only patient to survive was one of thefour cases that received chemotherapy.8 Our treatment strategyfor extraocular retinoblastoma has evolved into a multimodalapproach for all patients with orbital tumour recurrence.24 25
When a patient is confirmed to have orbital disease followingenucleation, our current protocol is to perform a metastaticevaluation with a brain MRI, abdominal CT scan, lumbarpuncture, bone scan and bone-marrow aspirate and biopsy.
Table 2 Clinical and histopathological data
Total orbitalrecurrencecases
Unilateral/bilateralRB
Age ofretinoblastomadiagnosis (months) Optic-nerve invasion Choroidal invasion Scleral invasion
Patients = 71 Unilateral = 37 1–12 months = 17 Yes = 35 Yes = 32 Yes = 2
Enucleatedglobes = 93
Bilateral = 34 13–24 months = 25 No = 35 No = 34 No = 73
25–36 months = 23 Margin+ = 7 Data NA = 27 Data NA = 18
37–48 months = 5 Data NA = 23
.48 = 1
Mean = 23.1
NA, not available.
Table 3 Clinical outcomes of 71 orbital recurrence cases
Enucleation to OR(months)
Metastatic diseaseat presentation Bone disease CNS disease Outcome Follow-up (months)
0–3 = 15 Yes = 44 Yes = 28 Yes = 12 Deceased = 61 0–12 = 28
4–6 = 31 No = 22 No = 32 No = 48 Alive = 10 13–24 = 26
7–12 = 23 Data NA = 5 Data NA = 11 Data NA = 11 25–36 = 1
37–48 = 1
.12 = 2 .49 = 15
Mean = 6 Mean = 34.8
NA, data not available; OR, orbital recurrence.
Clinical science
Br J Ophthalmol 2009;93:463–467. doi:10.1136/bjo.2008.138453 465
group.bmj.com on August 31, 2014 - Published by bjo.bmj.comDownloaded from

Because of the high risk of metastatic disease, patients found tohave only local disease in the orbit receive systemic multiagentchemotherapy as well as orbital radiotherapy. Patients withdisseminated disease such as bone-marrow involvement receivehigh-dose multiagent chemotherapy with stem-cell rescue,while those with CNS disease may also receive intrathecalradioimmunotherapy.
Several histopathological features of enucleated eyes havebeen recognised as risk factors for extraocular relapse inretinoblastoma patients. There appears to be universal agree-ment that optic-nerve invasion with tumour involvement of theresection margin and extrascleral spread are highly predictivemarkers for extraocular relapse.26 27 The prognostic value ofother extraretinal features, such as choroidal invasion andretrolaminar optic-nerve invasion (with a negative margin), hasbeen debated, although there is general agreement that thesefeatures increase the risk for systemic disease.9 18 In our series oforbital recurrence cases, 35 of the 70 globes (with data available)demonstrated evidence of optic nerve invasion, and 32 of 66globes (with data available) had choroidal invasion, indicating ahigher risk of metastatic disease in this cohort of patients thanother published series of retinoblastoma patients undergoingenucleations.15 16 26 Interestingly, only seven enucleated globeswere identified as having a positive optic nerve margin, and twoglobes had evidence of scleral invasion in this group of 71 orbitalrecurrence cases. Additionally, there were 11 cases without anyhistopathological risk factors (ie, choroidal invasion, scleralinvasion or optic nerve invasion). One explanation is thatmicroscopic invasion through the sclera or optic nerve bytumour cells may have been missed when the globe wasexamined histopathologically. However, the finding of threecases of contralateral orbital recurrence in our series suggeststhat non-contiguous tumour spread may be an under-recog-nised mechanism for orbital relapse in some of these cases.Haematogenous metastasis to the ipsilateral or contralateral
orbit has been reported as a mechanism for orbital recurrence,particularly to the orbital bones28 29
Patients developing orbital tumour recurrence followingenucleation for advanced intraocular disease represent a uniquesubset of patients, and they should be distinguished frompatients who present with extraocular retinoblastoma. Orbitalrecurrence following enucleation represents a type of tumourrelapse that occurs from either local or non-contiguous spread tothe orbit, often in the setting of systemic metastatic disease.The incidence of orbital tumour recurrence in our study of 1674patients undergoing enucleations was 4.2%, and patients andtheir families should be warned about the possibility of tumourrelapse during the preoperative discussion. Based on these data,histopathological risk factors are not always reliable in predict-ing which patients will ultimately develop orbital tumourrecurrence. Therefore, all patients undergoing enucleations forintraocular retinoblastoma require careful follow-up during thefirst 2 years after surgery, and clinicians should be aware thatpatients may be asymptomatic or present with subtle, non-localising or even contralateral symptoms. The majority ofpatients diagnosed as having orbital recurrence followingenucleation eventually develop metastatic disease, emphasisingthe need for a careful systemic work-up of these cases once theyhave been identified. With intensive systemic treatment, theprognosis for retinoblastoma patients with orbital tumourrecurrence appears to be improving in the modern era.
Competing interests: None.
Ethics approval: Ethics approval was provided by the Institutional Review Board atthe Memorial Sloan-Kettering Cancer Center.
Patient consent: Obtained.
REFERENCES1. de Sutter E, Havers W, Hopping W, et al. The prognosis of retinoblastoma in terms of
survival. A computer assisted study. Part II. Ophthalmic Paediatr Genet 1987;8:85–8.2. Ajaiyeoba IA, Akang EE, Campbell OB, et al. Retinoblastomas in Ibadan: treatment
and prognosis. West Afr J Med 1993;12:223–7.3. Abramson DH, Niksarli K, Ellsworth RM, et al. Changing trends in the management
of retinoblastoma: 1951–1965 vs 1966–1980. J Pediatr Ophthalmol Strabismus1994;31:32–7.
4. Tamboli A, Podgor MJ, Horm JW. The incidence of retinoblastoma in the UnitedStates: 1974 through 1985. Arch Ophthalmol 1990;108:128–32.
Table 4 Clinical presentation of orbital recurrence cases
No of patients (%) Clinical presentation
33 (46) Local orbital symptoms/problems with prosthesis
23 (32) Routine examination
7 (10) Non-localising/constitutional symptoms
5 (7) Eyelid ecchymosis/bleeding from socket
3 (4) Contralateral orbit/socket
71 total
Figure 1 Clinical photograph showing chemosis and eyelid ecchymosisin a patient with an orbital tumour recurrence following enucleation.
Figure 2 Coronal magnetic resonance imaging study (T1 withgadolinium) of the same patient in fig 1 demonstrating a subperiostealtumour recurrence to the marrow space of the orbital floor.
Clinical science
466 Br J Ophthalmol 2009;93:463–467. doi:10.1136/bjo.2008.138453
group.bmj.com on August 31, 2014 - Published by bjo.bmj.comDownloaded from

5. Bowman RJ, Mafwiri M, Luthert P, et al. Outcome of retinoblastoma in east Africa.Pediatr Blood Cancer 2008;50:160–2.
6. Gatta G, Capocaccia R, Stiller C, et al. Childhood cancer survival trends in Europe: aEUROCARE Working Group study. J Clin Oncol 2005;23:3742–51.
7. Abramson DH, McCormick B. Neoplasms of the eye. 4th edn. Baltimore: Williams &Wilkins, 1997.
8. Hungerford J, Kingston J, Plowman N. Orbital recurrence of retinoblastoma.Ophthalmic Paediatr Genet 1987;8:63–8.
9. Khelfaoui F, Validire P, Auperin A, et al. Histopathologic risk factors inretinoblastoma: a retrospective study of 172 patients treated in a single institution.Cancer 1996;77:1206–13.
10. Ellsworth RM. Orbital retinoblastoma. Trans Am Ophthalmol Soc 1974;72:79–88.11. Hopping W, Waubke TN, Sack H. Orbital involvement in retinoblastoma. Mod Probl
Ophthalmol 1975;14:382–7.12. Rootman J, Ellsworth RM, Hofbauer J, et al. Orbital extension of retinoblastoma: a
clinicopathological study. Can J Ophthalmol 1978;13:72–80.13. Hirschberg J. Anatomisch untersuchungen. Ueber glioma retinae. Arch Ophthalmol
1868;14:30.14. Howarth C, Meyer D, Hustu HO, et al. Stage-related combined modality treatment of
retinoblastoma. Results of a prospective study. Cancer 1980;45:851–8.15. Honavar SG, Singh AD, Shields CL, et al. Postenucleation adjuvant therapy in high-
risk retinoblastoma. Arch Ophthalmol 2002;120:923–31.16. Chantada GL, Dunkel IJ, de Davila MT, et al. Retinoblastoma patients with high risk
ocular pathological features: who needs adjuvant therapy? Br J Ophthalmol2004;88:1069–73.
17. Kopelman JE, McLean IW, Rosenberg SH. Multivariate analysis of risk factors formetastasis in retinoblastoma treated by enucleation. Ophthalmology 1987;94:371–7.
18. Stannard C, Lipper S, Sealy R, et al. Retinoblastoma: correlation of invasion of theoptic nerve and choroid with prognosis and metastases. Br J Ophthalmol1979;63:560–70.
19. Uusitalo MS, Van Quill KR, Scott IU, et al. Evaluation of chemoprophylaxis inpatients with unilateral retinoblastoma with high-risk features on histopathologicexamination. Arch Ophthalmol 2001;119:41–8.
20. Karcioglu ZA, Mullaney PB, Millar LC. Extrusion of porous polyethyleneorbital implant in recurrent retinoblastoma. Ophthal Plast Reconstr Surg1998;14:37–44.
21. Stevenson KE, Hungerford J, Garner A. Local extraocular extensionof retinoblastoma following intraocular surgery. Br J Ophthalmol1989;73:739–42.
22. Abramson DH, Ellsworth RM. The surgical management of retinoblastoma.Ophthalmic Surg 1980;11:596–8.
23. Abramson DH, Schefler AC. Update on retinoblastoma. Retina 2004;24:828–48.24. Grabowski EF, Abramson DH. Intraocular and extraocular retinoblastoma. Hematol
Oncol Clin North Am 1987;1:721–35.25. Dunkel IJ, Aledo A, Kernan NA, et al. Successful treatment of metastatic
retinoblastoma. Cancer 2000;89:2117–21.26. Magramm I, Abramson DH, Ellsworth RM. Optic nerve involvement in
retinoblastoma. Ophthalmology 1989;96:217–22.27. Shields CL, Shields JA, Baez KA, et al. Choroidal invasion of retinoblastoma:
metastatic potential and clinical risk factors. Br J Ophthalmol 1993;77:544–8.28. Mohan K, Gupta A, Saini JS, et al. Retinoblastoma metastatic to the contralateral
orbit. Br J Ophthalmol 1990;74:311–12.29. MacKay CJ, Abramson DH, Ellsworth RM. Metastatic patterns of retinoblastoma.
Arch Ophthalmol 1984;102:391–6.
Access all our original articles online even before they appear in a print issue!
Online First is an exciting innovation that allows the latest clinical research papers to go fromacceptance to your browser within days, keeping you at the cutting edge of medicine.
Simply follow the Online First link on the homepage and read the latest Online First articles that areavailable as unedited manuscripts in downloadable PDF form. The articles are peer reviewed, acceptedfor publication and indexed by PubMed but not yet included in a journal issue, so you’ll be among thefirst to read them!
Clinical science
Br J Ophthalmol 2009;93:463–467. doi:10.1136/bjo.2008.138453 467
group.bmj.com on August 31, 2014 - Published by bjo.bmj.comDownloaded from

doi: 10.1136/bjo.2008.13845329, 2008
2009 93: 463-467 originally published online AugustBr J Ophthalmol J W Kim, V Kathpalia, I J Dunkel, et al. following enucleationOrbital recurrence of retinoblastoma
http://bjo.bmj.com/content/93/4/463.full.htmlUpdated information and services can be found at:
These include:
References http://bjo.bmj.com/content/93/4/463.full.html#ref-list-1
This article cites 28 articles, 6 of which can be accessed free at:
serviceEmail alerting
the box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in
CollectionsTopic
(899 articles)Epidemiology � (622 articles)Eye (globe) �
Articles on similar topics can be found in the following collections
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on August 31, 2014 - Published by bjo.bmj.comDownloaded from




![The Technique of Tonsil Enucleation - Semantic Scholar...Dec., 1936] TECHNIQUE OF TONSIL ENUCLEATION: WILLIAMSON 727 Special Article THE TECHNIQUE OF TONSIL ENUCLEATION By H. WILLIAMSON,](https://img.dokumen.tips/doc/110x75/5e9dc57b42f70b199c246bec/the-technique-of-tonsil-enucleation-semantic-scholar-dec-1936-technique.jpg)