Embed Size (px)
Citation preview
EVISCERATION ,ENUCLEATION ,EXENTRATIONAND
CYCLODESTRUCTIVE PROCEDURESDr. Reshma Peter
SURGICAL PROCEDURES IN THE REMOVAL OF AN EYEClassified into three categories
EVISCERATIONRemoval of the contents of the
globe
leaves the sclera ,fat,EOM, and other adjacent structures of the
eye intact and sometimes the cornea in place.
ENUCLEATION
Removal of the eye
leaves EOM and remaining orbital contents intact.
EXENTERATION
Removal of the entire contents of the orbit
including EOM
EVISCERATION
• A surgical technique by which all intraocular contents are removed
• Scleral shell, EOM attachments, surrounding orbital adnexa preserved
• The surgery often includes placement of an implant into the cavity to maintain appropriate orbital volume.
Indications
• Panophthalmitis, Endophthalmitis
• Penetrating ocular trauma
• Blind, painful eye
• Expulsive Choroidal haemmorhage
• Bleeding Anterior Staphyloma
Contraindications
• Known or suspected intraocular malignancy
Relative Contraindications
• Phthisis bulbi
• Microphthalmia
• Careful pre-operative evaluation to ensure there is no intraocular malignancy in the operative eye
• Performed under GA or in some cases,
IV monitored sedation.
• Retrobulbar anesthesia with epinephrine is often given to reduce intraoperative bleeding and postoperative pain.
Surgical Technique
• A 360-degree conjunctival peritomy is then made at the limbus utilizing Wescott scissors undermine the conjunctiva and Tenon’s capsule
• A full-thickness incision is then made at the limbus so that scissors may be introduced to excise the cornea in a circumferential manner.
• All intraocular contents, including uveal tract, crystalline lens, vitreous humor, and retina are then removed by using an evisceration spoon, spatula, suction.
• These contents are sent for histopathologic examination.
• Sclera is swabbed with Absolute Alcohol to denature adherent uveal remnants and irrigated properly to remove alcohol
• Hemostasis of the nerve and vortex veins may then be achieved with cautery and direct pressure.
• In some cases, a posterior sclerotomy or radial scleral relaxing incisions to allow for a larger implant to be placed.
• The best implant size to restore orbital volume is selected while ensuring appropriate position.
• Implant material is made of different materials like acrylic, PMMA, silicone, and hydroxyapatite.
• The implant may be placed directly into the scleral shell
• The anterior sclera, Tenon’s capsule, and conjunctiva is then carefully closed in a layered approach before placement of a conformer.
• Sclera is sutured with interrupted 6-0 Vicryl•
• Conjunctiva with running mattress 6-0 Vicryl
• A temporary tarsorrhaphy may be performed to help the conformer remain in place to maintain the fornices till prosthesis can be placed
• Perioperative antibiotics are often administered and are especially important in the setting of endophthalmitis.
• A pressure patch may be applied and kept in place for approximately 5 days following surgery.
• Ice cold compresses help with post-operative edema and comfort
• Once the conjunctiva closure has healed, generally about 4-8 weeks postoperatively, patients are referred to an ocularistfor fitting of an ocular prosthetic fitting.
4-petal technique of Evisceration
It has several advantages over the traditional evisceration technique.
• allows placement of a larger implant
• enables double-breasting of scleral cover
• eliminates the need for a myo-conjunctival technique.
• The vertical closure of the conjunctiva retains the depth of the lower fornix, which is of importance to retain the ocular prosthesis.
Frill evisceration Technique
only 3mm frill of sclera is left around Optic Nerve
• If a scleral buckle or glaucoma drainage device is present in the eviscerated eye, it should be removed.
• If silicone oil is present within the eye, the limbus can be incised and the silicone oil irrigated from the eye prior to peritomy.
• Evisceration with removal of cornea done for those with corneal sensation /pain or in CT disorders/ RA –chances of corneal thinning
Complications
• Retrobulbar hemorrhage
• Orbital edema
• Dissemination of unexpected intraocular neoplasm
• Extrusion of implant
Advantages of Evisceration over Enucleation1. Shorter operative time
2. More cost efficient
3. A technically simpler procedure
4. A less invasive procedure (important in cases when GA is contraindicated or in bleeding disorders)
5. Less disruption of orbital tissues
– chance of injury to EOM ,nerves and fat atrophy is reduced
– Relationships between the muscles, globe, eyelids, and fornices remain undisturbed
– Less chance of spread of infection to nervous system
6. Less painful
7. Better cosmesis
8. Good motility of the prosthesis- EOM remain attached to the sclera
9.Lower rate of migration, extrusion, reoperation and socket complications
10.Preferred by some surgeons in cases of endophthalmitis as drainage of the ocular contents can be done without invasion of the orbit.
• The chance of contamination of the orbit with orbital cellulitis or intracranial extension is therefore theoretically reduced.
Disadvantages of Evisceration over Enucleation
• Risk of sympathetic ophthalmia
• Risk of dissemination of intraocular tumors
• Offers a less complete specimen for pathologic examinations.
• Not every patient is a candidate.
C/I if intraocular tumours are suspected and in Severe Pthisis
ENUCLEATION
• A surgical procedure that involves removal of the entire globe and its contents.
• all other periorbital and orbital structures including parts of EOM and orbital fat preserved.
Indications
• Eye donation
• Intraocular malignancy or high suspicion for intraocular malignancy (most commonly uveal melanoma and retinoblastoma)
• Trauma
• Blind, painful eye
• Sympathetic ophthalmia
• Microphthalmia
• Phthisis bulbi
• Endophthalmitis
• Cosmetic deformity
• Performed under GA or LA
• A retrobulbar block of local anesthetic with epinephrine is administered to aid in hemostasis and postoperative pain management.
• Lateral canthotomy to get adequate space (especially in paediatric RB)
Surgical Technique
• A 360 degrees limbal conjunctival peritomy is performed with Wescott scissors
• Blunt dissection in the sub-Tenon's plane is then carried out in each of the oblique quadrants.
• Each rectus muscle is then identified, isolated with a muscle hook, secured with double arm 6-0 vicryl suture, and cut at the insertion to the globe leaving an adequate stump with traction suture
• The superior and inferior oblique muscles are isolated and transected.
• Once the globe is determined to rotate freely, the optic nerve is identified, strummed, and cut with enucleation scissors or an enucleation snare wire.
• A long segment of the optic nerve is cut , particularly in intraocular malignancy for histologic examination. Curved scissors inserted orbital apex palpated with tip, withdraw slightly, confirm Optic N. which is severed with a single cut
• Additional hemostasis achieved with direct pressure in the intraconal space and cautery of the optic nerve if needed.
• Needles of double armed recti sutures passed through respective fornices and tied on ant surface of conjunctiva thus securing recti to fornix.
• An implant is then placed in the intraconal space to replace volume lost, achieve cosmetic symmetry with the fellow socket, and allow for motility of the prosthesis.
• To determine appropriate diameter of the implant, the formula axial length-2 mm has been shown to provide for adequate replacement of lost volume and minimize superior sulcus deformity and enophthalmos.
• In severe infection,implant is placed in a second surgery.
• A two-layered closure with 6-0 vicryl is then carried out with absorbable sutures, first of tenon’s capsule (interrupted suture)and then of the conjunctiva(running mattress suture).
• Antibiotic ointment is applied, a clear plastic conformer is placed over the closed conjunctiva
• A pressure patch is placed over the socket.
• Once the conjunctiva closure has healed,about 4-8 weeks postoperatively, patients are referred to an ocularist for fitting of an ocular prosthetic fitting.
• Patients will require regular follow up with both an oculoplastic surgeon and an ocularist to maintain the health of their socket.
Advantages
• Enucleation allows for histologic examination of an intact globe and optic nerve.
• This is important in biopsy of proven or suspected intraocular malignancy, where it is essential to determine the margins of the malignancy and invasion of the optic nerve, if any.
• Enucleation classically has been thought to decrease the risk of sympathetic ophthalmia as it avoids exposure to uveal antigens that may occur during an evisceration.
Disadvantages
A reduction in implant motility is often noted in enucleation.
ComplicationsIntraoperative
• Removal of the wrong eye
• Damage to or loss of extraocular muscles
• Hemorrhage
Postoperative• Infection• Hemorrhage• Wound dehiscence• Extrusion of the conformer• Contraction of the fornices• Exposure of the implant• Extrusion of the implant• Migration of the implant• Ptosis• Ectropion• Entropion• Hollow or deep superior sulcus• Poorly fitting prosthesis• Enophthalmos• Socket contracture• Orbital cellulitis
EXENTRATION
• A surgical procedure involving removal of the entire globe and its surrounding structures including muscles, fat, nerves, and eyelids (extent determined by disease being treated)
• The goal is to remove all lesions along with appropriate margins of adjacent tissue while retaining as much healthy tissue as possible.
• The technique selected depends on the pathologic process.
Varieties of orbital exenteration
Subtotal :
The eye and adjacent intraorbital tissues are removed such that the lesion is locally excised (leaving the periorbita and part or all of the eyelids).
This technique is used for some locally invasive tumors, for debulking of disseminated tumors, or for partial treatment in selected patients.
Total:
All intraorbital soft tissues, including periorbita, are removed, with or without the skin of the eyelids.
Extended:
All intraorbital soft tissues are removed, together with adjacent structures(usually bony walls and sinuses).
Varieties of orbital exenteration
• Anterior (part or full eyelids, conjunctiva, eyeball, anterior orbit)
• Anterior and short of apex• Total/radical (all the above upto apex)• Extended (orbit and one of the paranasal sinuses)• Super (exenteration with orbitectomy)• Eyelid-sparing (can be used with any of the above).
Following removal of the orbital contents, the bony socket may be allowed to spontaneously granulate and epithelialize or covered by a split-thickness skin graft, which may be
placed onto bare bone or over a temporalis muscle or temporoparietalfascial flap.
Indications• Orbital malignancies
Cutaneous tumours with orbital adnexa invasion
including squamous cell carcinoma, basal cell carcinoma, and sebaceous cell carcinoma.
Less common tumors include conjunctival malignant melanoma, adenoid cystic carcinoma of the lacrimal gland, and uveal melanoma with extrascleral extension
Intraocular melanomas or retinoblastomas
• Painful or life-threatening orbital infections
• Mucormycosis
• Chronic orbital pain
• Orbital deformities
Lid Sparing Exenteration Technique• GA should be used if possible.
• If GA is C/I ,local retrobulbar, infraorbital, and periorbital nerve blocks may be used
• A 4-0 black silk suture is passed through the skin, orbicularis muscle, and superficial tarsus of the upper and lower lids and tied together to close the eyelids and to provide tractionduring the procedure.
• A skin incision is outlined 2 mm above and below the upper and lower lash line and extended to just beyond the medial and lateral canthi
• The incision is placed only through the eyelid skin and orbicularis oculi muscle, which is then undermined superiorly and inferiorly until the periosteum just outside the orbital rim is exposed for 360°.
• An incision is then made through the periosteum for 360°about 2 mm outside of the orbital rim to expose the underlying bone.
• A periosteal elevator is used to free the periosteum for 360°around the bony orbital margin and into the orbital cavity.
• Small bleeding vessels posteriorly between the periosteum and the bone may be difficult to control.
• When the periosteum is free posteriorly, the enucleation scissors are inserted between the periosteum and bone on the inferonasal side and gently advanced to the orbital apex.
• The tissues are then cut as near to the orbital apex as possible, and the orbital contents are removed by continued traction on the silk sutures in the eyelids while cutting the residual adhesions in the posterior orbit.
• The socket is immediately packed with moist gauze, which is left in place for 5 to 10 minutes.
• The gauze is then removed and the orbital apex inspected.
•
• Residual soft tissue at the orbital apex is removed piecemeal, and Bovie cautery and repeat packing are used until there is no further bleeding.
• A rubber drain is placed in the socket after complete hemostasis, and the skin of the upper and lower eyelids are sutured together with interrupted 5-0 silk sutures.
• This leaves the residual orbital cavity filled with air.
• One skin suture is tied to the drain.
• The drain suture is removed in 12 to 24 hours, and the drainis removed in 24 to 48 hours, depending on when drainage has ceased.
• The skin sutures are removed in about 1 week, and dressings are not required.
• The remaining eyelid skin gradually retracts into the socket and provides a more cosmetically acceptable lining of the socket after exenteration.
• An orbital prosthesis can be fitted within 3 to 4 weeks.
Advantages to a lid-sparing technique
• The wound heals faster
• less postoperative follow-up is required.
• The quicker healing allows radiotherapy where required.
• A smooth healthy surface of the socket allows the use of a stick-on orbital prosthesis, rather than a spectacle mounted one.
Total Exenteration Technique
• Two 4-0 silk tarsorrhaphy sutures are placed which will also act as traction sutures throughout the case.
• A monopolar cautery is then used to make an incision through the skin and orbicularis muscle at the orbital rim 360 degrees.
• Dissection is the carried out to the orbital rim laterally as well as inferiorly.
• The superior orbital rim is identified and the periosteum is elevated. The lateral orbital rim is incised along the periosteum.
• Laterally the periosteum is elevated from the lateral orbital rim and lateral wall.
• In this area one will usually encounter structures corresponding to the zygomatico facial and zygomaticomaxillary neurovascular bundles.
• The supraorbital neurovascular bundle is identified and transected with the monopolar cautery.
• Medially, the anterior ethmoidal neurovascular bundle is identified and cauterized.
• Posteriorly, the posterior ethmoidal neurovascular bundle is identified and cauterized.
• After transection of the infraorbital fissure as well as the nasolacrimal duct, the curved scissors are used to transect the posterior obit.
• One can apply a snare prior to transection as the ophthalmic artery is transected and there will be significant bleeding.
• Hemostasis is attained with the bipolar cautery.
• A posterior orbital biopsy can be obtained if needed.
• The area is then packed for hemostasis prior to harvesting of the split thickness skin graft.
Complications
• Extensive bleeding, rarely necessitate a blood transfusion.
• Fracture of thin ethmoid bones during the surgery, leading to an opening between the orbit and the nasal cavity.
• Postoperative infection-appropriate antibiotics.
• Sloughing of the skin graft.
• Sino orbital fistula
• Intracranial infections –CSF leakcan be eliminated by obliterating the cavity in its entirety with soft-
tissue free-flaps which provides a safer and more therapeutic management of the socket leading to
improved postoperative management and cosmetic outcome. protective barrier that protects the cranium from a potential infection.
Ideal anophthalmic socket
1. A socket lined with healthy conjunctiva and fornices deep enough to retain a prosthesis and to permit horizontal and vertical movements of an artificial eye
2. Eyelids with normal position ,appearance and adequate tone to support a prosthesis
3. A supratarsal eyelid fold that is symmetric with that of the C/l eyelid
4. Normal position of the eyelashes and eyelid margin
5.A centrally placed, well-covered, buried implant of adequate volume, fabricated from a bio-inert material
6. Good transmission of motility from the implant to the overlying prosthesis
7. A comfortable ocular prosthesis that looks similar to the sighted, contralateral globe and in the same horizontal plane
CYCLODESTRUCTIVE PROCEDURES
• Destruction of the ciliary body has been used to treat glaucoma since the 1930s.
• In cyclodestructive procedures, the secretory epithelium of the ciliary epithelium is damaged, which leads to reduced aqueous humor secretion and lower IOP.
• Coagulation of proteins of epithelial cells ,closing nearby capillariesablation of ciliary epithelium without destroying ciliary body
• Because the ciliary epithelium can regenerate, multiple treatments are necessary in some patients to achieve the desired long term IOP lowering effect.
The different modalities to achieve cyclodestruction are: diathermy, surgical excision, cryotherapy, ultrasound, and laser light
Cyclophotocoagulation (CPC) is the most common procedure to perform cyclodestruction. It can be performed using different laser wavelengths
• CPC was first performed by Beckman using a ruby laser (693 nm wavelength).
• Nd:YAG laser (1064 nm wavelength has been used either with non-contact or contact methods to achieve cyclodestruction.
Contact Nd Yag-
• Uses hand held probe placed on conjunctiva to to allow energy transmission directly to ocular surface
• lesser power required as contact pressure increases scleral transparency
• 32 to 40 spots over 360 degrees
• 7 watts for 0.7 seconds for each spot
Non Contact Nd Yag-
• Transmits laser through air from slitlamp delivery system
• 32 to 40 spots over 360 degrees
• 8 Joules for 20 msec
• Presently, diode laser (810 nm wavelength) either transsceral or with an endoscopic probe is used to perform CPC.
• The diode laser is preferred over other wavelengths since the melanin in the ciliary epithelium better absorbs this wavelength than others and therefore causes more targeted destruction with less inflammation.
• It requires 50 %lesser power than with Nd Yag
There are 3 basic approaches to cyclodestruction(cycloablation):
• Cyclocryotherapy
• Trans-scleral laser cycloablation
• Endoscopic laser cycloablation
All 3 techniques share the common goal of decreased aqueous production, and all share the possible side effects of inflammation (including possible sympathetic ophthalmia), ineffective treatment, and over-treatment with resultant hypotony or even phthisis.
• cycloablation procedures mostly reserved for those cases refractory to, or not amenable to angle surgery, glaucoma drainage implant surgery, and trabeculectomy
• For Refractory pediatric glaucoma , cyclodestructionrepresents a valid method of attempting control of glaucoma that threatens residual vision or causes ongoing damage to the structure of the child's eye.
• Conventionally used only in eyes with poor visual potential, but can be employed in cases with reasonable vision to prevent severe glaucomatous damage occurring whilst neovascularization is brought under control.
• Lowering IOP improves comfort, and clearing corneal oedema may facilitate an adequate retinal view for PRP
• Recently TS-CPC has been performed in patients with good vision with good results.
CYCLOCRYOTHERAPY
Indications• Other treatment modalities exhausted
• Cases when TDC or ECP is anatomically challenging to perform
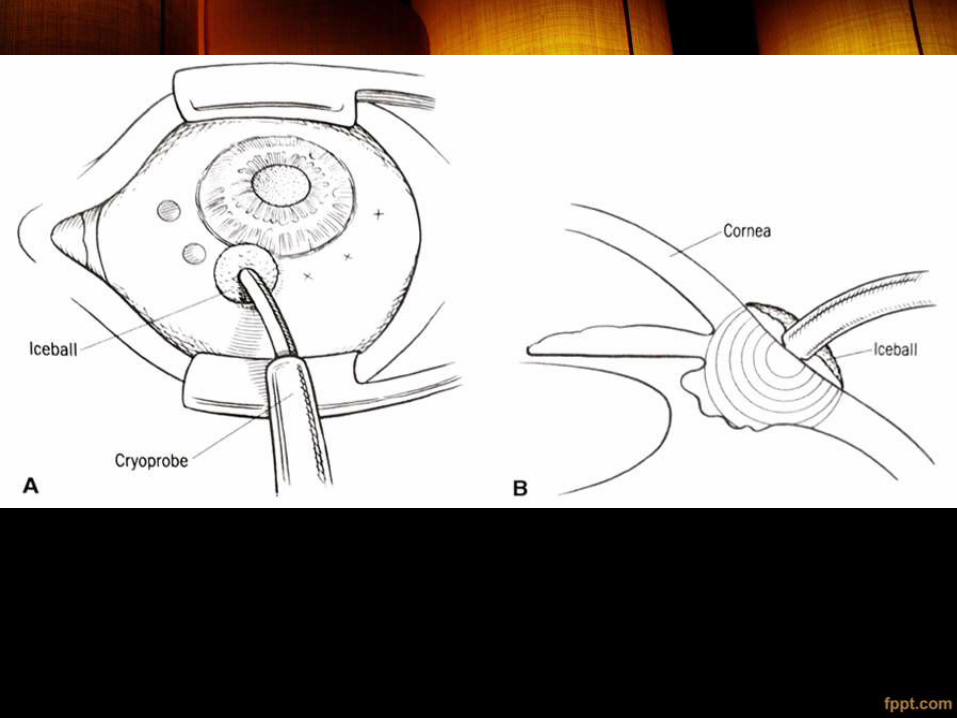
Technique• The oldest cyclodestructive method
• involves freezing the ciliary processes from an external approach
• reserved for those refractory pediatric glaucoma cases in which anatomy limits the likelihood of successful ciliary body treatment with either trans-scleral or endoscopic cyclophotocoagulation or access to these technologies is truly unavailable and incisional surgery is impossible
• cyclocryotherapy in pediatric eyes should be limited to a maximum of 6 clock hours (180 degrees of the eye's circumference) at any 1 session, using approximately 1 freeze-spot per clock-hour (45–60 seconds each at 280ºC)
• Given with the anterior edge of a "large" 2.5-mm diameter cryoprobe attached to liquid Nitrogen supplyplaced at 1–1.5 mm posterior to the limbus in a nonbuphthalmic globe
• avoid the 3 and 9 o'clock locations to minimize damage to the long posterior ciliary vessels.
• Extent of freeze ball -10 -12 mm , extending up to corneal limbus
• Any especially thin area of the limbus should also be avoided
• care should be taken to avoid contact with adjacent lid tissue and to shorten treatment if the "freeze zone" gets larger than approximately 1 cm, which can happen as the entire eye "cools down" with sequential freeze applications.
• Where limbal anatomy is distorted or difficult to evaluate, transillumination can help identify the proper treatment location.
• During cyclocryotherapy repeat sessions, care should be taken to leave at least 1 quadrant untreated because with overtreatment, chronic hypotony or phthisis can be permanent.
Advantages
• Short surgical time and rapid rehabilitation
• Technically easy
Disadvantages
• Often needs to be repeated due to ciliary body recovery
• Most patients remain on medical therapy.
• Risk of phthisis bulbi
• Scleral thinning at cryo sites can affect future drainage device surgery.
• Proinflammatory and can accelerate cataract formation
• Post op IOP spike- due to volumetric change in intraocular contents caused by intravitreal iceball.
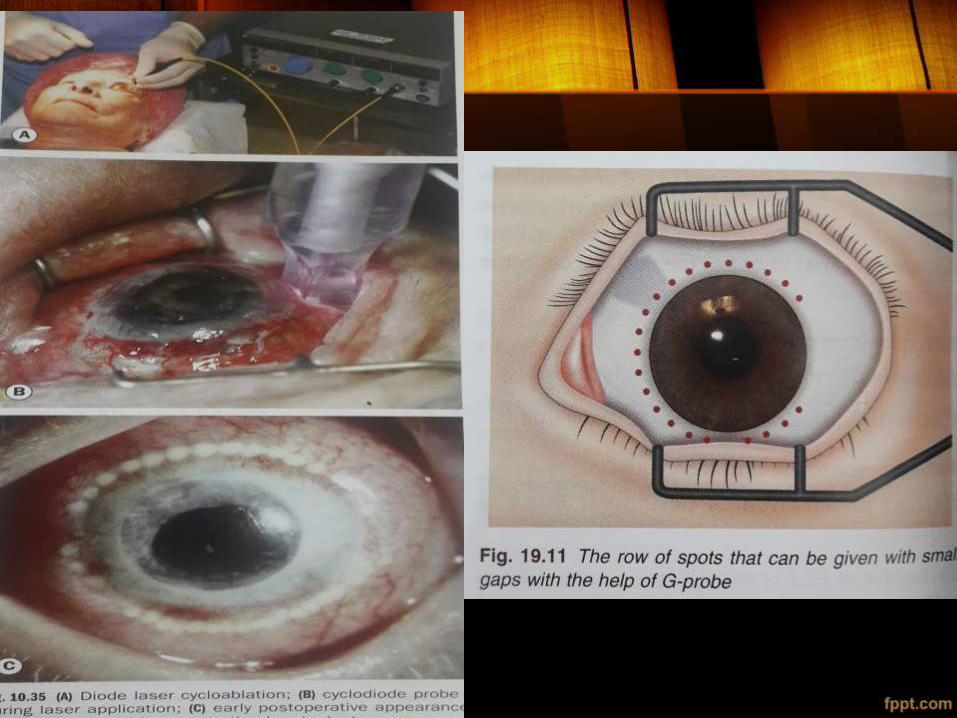
TRANS-SCLERAL DIODE-LASER CYCLOPHOTOCOAGULATION (DIODE TS-CPC)
• Laser energy can be directed through the sclera to treat the ciliary processes using a probe in contact with the sclera over the intended treatment site.
• Used in pediatric glaucoma, refractory to other measures using both the Nd:YAG laser and the diode laser.
• Although reported to produce less inflammation than cyclocryotherapy in adults, risks of serious complications
• Ultrasound biomicroscopy recently has been described as a guide to proper placement of the probe for TDC
TRANS-SCLERAL DIODE-LASER CYCLOPHOTOCOAGULATION (DIODE TS-CPC)
• The only eligibility requirement-eye must have some degree of functioning aqueous outflow.
• TSCPC decreases aqueous outflow , thereby decreasing IOP
• C/I in Uveitis
• Preop vasoconstriction with Alpha agonist (Alphagan P) decrease energy absorption by conjunctival vesselslesslikelihood of SCH
Indications for TranscleralCyclophotocoagulation• Elevated IOP with poor vision or poor visual potential• Pain relief due to elevated IOP in a blind painful eye• Uncontrolled glaucoma in the presence of conjunctival scarring
from previous surgery• Patient's medical condition preclude going to operating room• Patient refuses surgery in OT• Failed angle surgery and minimal visual potential• Failed trabeculectomy and/or aqueous drainage with poor central
vision• Inadequate IOP control after drainage device• Anatomy precluding trabeculectomy or glaucoma drainage device,
e.g., disorganized anterior segment, thin limbus• Gravely ill children, poor follow-up, blind in fellow eye from
complication of intraocular surgery• Uncontrolled IOP post surgery in Primary open-angle
glaucoma,Angle-closure glaucoma,Neovascularglaucoma,Pseudophakic/aphakic glaucoma,Pediatricglaucoma,Glaucoma after penetrating keratoplasty,Uveiticglaucoma,Silicone oil induced glaucoma
Procedure
• Diode TS-CPC can be performed in a minor procedure room or in an OT.
• Retrobulbar or peribulbar anesthesia is needed, as the procedure is painful.
• A lid speculum helps to provide better exposure to the peri-limbal area.
• A semi-conductor solid state diode laser with a wavelength of 810 nm
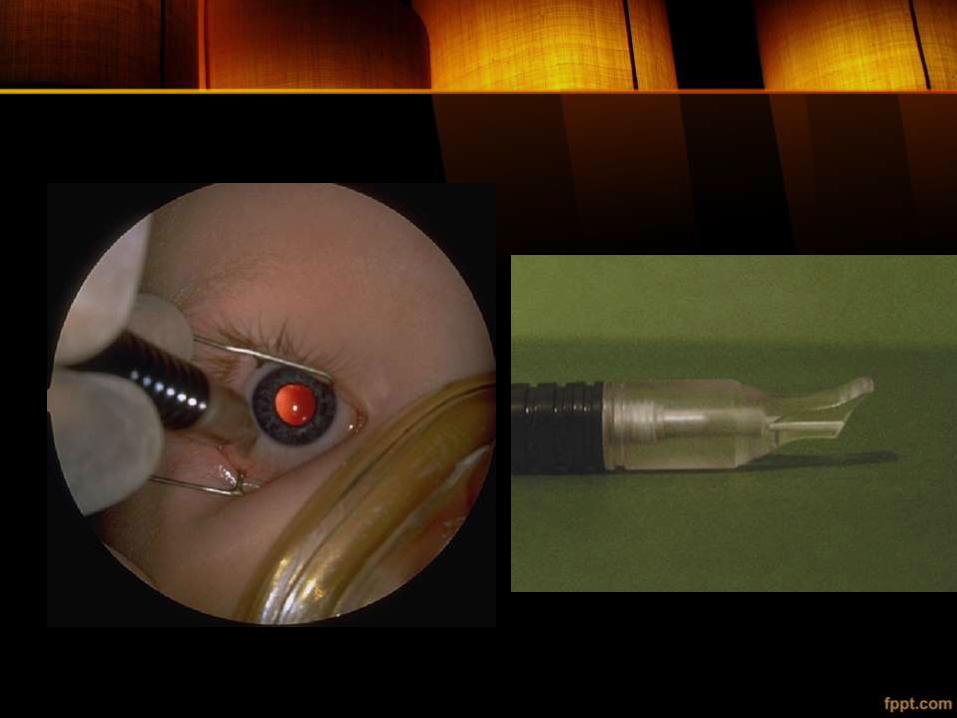
• A handpiece –G probe is used to deliver the laser
energy.
• G probe- 600u diameter Quartz glass fibre , placed 1mm posterior to limbus, mild pressure to indent conj and sclera
• Initial power of 1250 mW and duration of 4 seconds.
• The power is increased in 150 mW increments until an audible “pop” is heard.
• The audible “pop” signifies tissue explosion of the ciliary process, the iris root, or the retina

• When a “pop” is heard the power is decreased by 150 mW until there is no audible “pop”.
• The maximum power used is 2250 mW.
• Others will start at 2000 mW and 2 seconds and titrate the energy down. Generally 6 spots are used per quadrant for a total of 18 spots.

• Some surgeons recommend treating only 3 quadrants to avoid anterior segment necrosis and many recommend sparing the 3:00 and 9:00 positions.
• After completion of the procedure a topical antibiotic, steroid, and cycloplegic agents are placed on the eye.
• The eye should be patched after a block is used to protect the cornea.
• The patient is seen the next day for follow-up.
Advantages
• Short surgical time and rapid rehabilitation
• Technically easy
• Lesser power as compared with cryo as more efficiently absorbed by ciliary body
In cryodiffusely absorbed by all structures
• Contact method-less scatter , thus less energy required
Disadvantages
• Often needs to be repeated due to ciliary body recovery
• Most patients remain on medical therapy.
• Risk of phthisis bulbi, but less than cryo
• Beware risk of perforation at sites of scleral thinning.
• Proinflammatory and can accelerate cataract formation
Complications
• IOP spikes –Preop and post op oral CAI –Azetazolamideor Methazolamide
• Pain is usually transient and controlled with analgesics
• Hyphema more frequently in neovascular glaucoma patients.
• Iridocyclitis occurs commonly after TS-CPC. Few patients can develop a chronic low-grade anterior chamber inflammation due to a breakdown in the blood-aqueous barrier.
• Conjunctival burns rarely if conjunctival surface becomes dry during laser with high energy settings ,in darkly pigmented conjunctiva and due to the use of defective, damaged, or soiled laser probes.
• Hypotony
• Vision loss can occur after TS-CPC
• Phthisis bulbi is a rare complication
• Malignant glaucoma
• necrotizing scleritis
• sympathetic ophthalmia
• Scleral perforation has been reported with TDC so care should be taken to ensure that the probe surface is clean of debris and to avoid areas of obvious scleral thinning and the site of previous surgeries (do not laser where the tube passes and the previous trabeculectomysite).
Variation in clinical response
• Variation in pressure exerted over sclera
• Difference in scleral thickness
• Variation in probe inclination
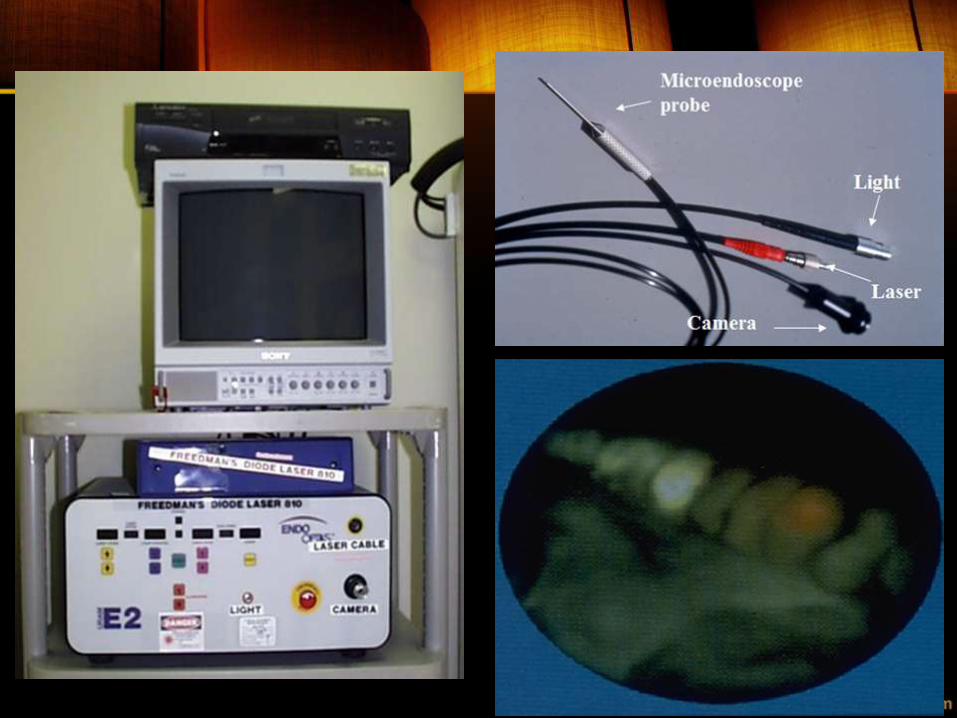
ENDOCYCLOPHOTOCOAGULATION (ECP)Employs fibreoptic cable to deliver pulsed continuous wave diode laser energy to ciliary processes under direct endoscopic visualization using video monitor
• Used as a treatment for refractory pediatric glaucoma, allowing more precise localization of the target and treatment with much lower energy than required for trans-scleral laser.
• The most commonly used system uses a diode laser equipped with a 20-gauge probe, within which is housed fiber optics for a video monitor, diode laser endophotocoagulation, and illumination
• ECP can be combined with phacoemulsification to treat cataract and glaucoma at the same time In combined cases ECP can be performed before or after inserting the intraocular lens in the lens bag.
Indications for Endocyclophotocoagulation
• Same indications as TDC but anatomy of eye allowing limbal or pars plana approach to ciliary processes but beware of cataract in phakic eyes
• To Consider after TDC has failed.
• Patients who are poor candidates for glaucoma filtration surgery or glaucoma drainage implant
• Distorted anterior segments
• In uncontrolled Primary open-angle glaucoma,Pseudoexfoliation glaucoma,Neovascularglaucoma,Pseudophakic glaucoma,Glaucoma after penetrating keratoplasty,Glaucoma associated with retinal surgery,Pediatric glaucoma,Angle-closure glaucoma
Technique
• The ECP laser unit has 4 different components, the diode laser (pulsed continuous-wave energy at 810 nm), a xenon light source, a helium-neon laser aiming beam, and video monitor and recorder.
• The probe is 20 gauge with a full view of 110 degrees and depth of focus of 1-30mm.
• The equipment console consists of the video camera, light source, video monitor, and the video recorder.
• Initially the laser probe is placed into the anterior chamber by looking through the surgical microscope.
• Then the surgeon looks through the video monitor to locate the ciliary processes and perform the laser photocoagulation
• The goal of each laser application is to whiten and shrink the ciliary process.
• The entire ciliary process should be treated.
• Generally 270-360 degrees of the ciliary processes are treated.
• Gas bubble formation, pigmentary dispersion, audible “pops”, photocoagulation of non-ciliary process tissue should be avoided
• The laser settings are as follows: Power 0.2 W, continuous-wave mode.
• The power is titrated to achieve whitening and shrinkage of the ciliary process by positioning the probe either closer or further from the processes.
• Ideally, 3 processes should be within view during treatment.
• ECP can be performed in phakic, pseudophakic, or aphakic eye with the endolaser probe through the limbus or pars plana.
In the limbal approach,
• a 1.5-2.0 mm incision is made in the clear cornea or sclera.
• A cohesive viscoelastic is injected posterior to the iris and anterior to the lens capsule to deepen the ciliary sulcus space.
• Next the probe is placed in the anterior chamber.
• The ciliary processes are visualized and treated.
• The viscoelastic is removed.
• In phakic patients great care should be taken not to nick the anterior lens capsule.
• In pseudophakic/aphakic eyes, the pars plana approach is advantageous since the ciliary processes are better visualized.
• The incision is made 3.5-4.0mm posterior to the limbus.
• Infusion port through pars plana
• 2 superior entries for vitrectomy and illumination
• Anterior vitrectomy is performed for adequate and safe access to ciliary processes
• Then cyclophotocoagulation with the endolaser probe is performed.
Post-operative Management
• Cycloplegics (atropine 1% BD for 2 weeks)
• Topical corticosteroids (prednisolone acetate 1% QID; In extensive anterior chamber inflammation increase frequency)
• Topical antibiotics
• Subtenon’s steroid injection and/or oral steroids
• The pre-laser glaucoma medications continued post-operatively and tapered based on the IOP lowering effect of the laser.
• Miotics should be stopped because they can enhance the inflammatory response and cause posterior synechiae.
• Consideration stopping PG analogs if IOP is well controlled since they can cause anterior chamber inflammation.
Advantages
• Short surgical time and rapid rehabilitation
• Allows precise treatment due to direct visualization and avoids risk of scleral perforation
• Important in Severe Congenital Glaucoma where eyeball is enlarged and ciliary processes may be displaced
• Can produce less inflammation and collateral tissue damage than TDC and cryo
• less power needed
Disadvantages
• Often needs to be repeated due to ciliary body recovery
• Most patients remain on medical therapy
• Risk of phthisis bulbi, but less than TDC and cryo
• Proinflammatory, but less than TDC and cryotherapy
• Intraocular approach with risk of endophthalmitis and cataract formation
Complications
• IOP spikes
• Fibrin exudates
• Hyphema
• Cystoid edema
• Vision loss of 2 lines or more
• Hypotony
• Zonular damage
• Rarely ,phthisis bulbi, endophthalmitis, or sympathetic ophthalmia
• Retinal detachment
• Serous and haemorrhagic choroidal detachment
• Traumatic injury to the iris Mechanical trauma/ laser improperly applied to the iris
Transpupillary cyclophotocoagulation
• In people with visible ciliary processes
• In traumatic aniridia and in people with large iridectomies
• in advanced neovascular glaucoma, when iris is pulled ant and peripherally
• With a slit lamp delivery system through Goldmann 3 mirror lens
• Using Argon green or Nd YAG
• 3-4 applications to coagulate all visible portion
• End point is blanching of ciliary body, blisters,/effusion of pigment
• Cyclodestruction has limited success and the risk of severe complications when used for treatment of refractory pediatric glaucoma.
• Nonetheless, this modality retains an important role in the management of selected eyes with refractory glaucoma.
• Cyclodestruction in the treatment algorithm depends on several factors
visual potential
anatomic features
prior surgical interventions
glaucoma severity
overall health
• Both TDC and ECP can represent adjunctive techniques after prior glaucoma drainage device surgery has incompletely controlled the IOP and can be reasonable primary surgery in selected eyes with challenging anatomy for other intraocular glaucoma procedures.
• Cyclodestruction should be used with extreme caution in eyes with uveitis because all 3 techniques produce significant inflammation as well as the potential to produce retinal detachment, hypotony, phthisis, and even sympathetic ophthalmia.
References
1. Bosniak –Ophthalmic Plastic and reconstructive Surgery
2. AAO series –Orbit
3. Stellard’s Eye Surgery
4. Becker schaffer’s Diagnosis and therapy of Glaucomas
5. Kanski ‘s Clinical Ophthalmology
6. Post Graduate Ophthalmology by Zia CHaudhuri
6. AAO series- Glaucoma

THANK YOU !!