Embed Size (px)
Citation preview
http://css.sciedupress.com Case Studies in Surgery 2016, Vol. 2, No. 3
CASE REPORTS
Endoscope-assisted enucleation and guided boneregeneration of a recurrent aneurysmal bone cyst inthe mandibular condyle
Xiao-Jie Diao1, Hua-Ming Mai2, Lei Zhang3, Xu-Dong Wang∗3
1Department of Stomatology, Traditional Chinese Medical Hospital of Xinjiang Uygur Autonomous Region, Urumqi, Xinjiang,People’s Republic of China2Department of Oral and Maxillofacial Surgery, College of Stomatology,Guangxi medical University, Nanning, People’s Republicof China3Department of Oral & Cranio-maxillofacial Science, Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School ofMedicine, Shanghai Key Laboratory of Stomatology, Shanghai, People’s Republic of China
Received: December 28, 2015 Accepted: March 27, 2016 Online Published: April 18, 2016DOI: 10.5430/css.v2n3p1 URL: http://dx.doi.org/10.5430/css.v2n3p1
ABSTRACT
Aneurysmal bone cyst (ABC) is a locally destructive, expansive, benign bone disease which most commonly occurs in themetaphyseal region of the long bones of children and adolescents, only 1% to 3% of ABCs have been described in the jaws. Theaim of this study was to explore the minimal invasive surgical technique of treating ABC occurring in the mandibular condyle.Here we present a 10-year-old girl with recurrent ABC in her left condyle and adjacent ramus. She was treated by curettage viaan extraoral endoscopic-assisted surgical approach and guided bone regeneration. The patient had an uneventful postoperativeperiod with no injury to the facial nerves and minimal scarring. No recurrence was found in 4 years (from 2011). Computedtomography (CT) showed bone formation and remodeling of the condyle and ramus. Endoscopic-assisted curettage combinedwith guided bone regeneration can achieve an ideal effect in the treatment of ABC of the mandibular condyle and ramus.
Key Words: Aneurysmal bone cyst, Mandibular condyle, Endoscope
1. INTRODUCTION
Aneurysmal bone cyst (ABC) is a locally destructive, expan-sive, benign bone disease which most commonly occurs inthe metaphyseal region of the long bones of children andadolescents. ABC constitutes approximately 1% of all bonetumors; only 1% to 3% of ABCs have been described inthe jaws.[1] The incidence of ABC is 0.14 per million. It isinfrequently found in the mandibular condyle among all thecystic lesions.
The temporomandibular joint (TMJ) region contains a num-ber of important and vulnerable structures including branchesof the facial nerve. Compared with open surgery, endoscopic-assisted technique recently was implemented in the TMJregion for fractures and other disorders has the benefit ofless visible scarring, reduction in facial nerve deficit, andquicker functional rehabilitation.[2] But the application ofcurettage of condylar cysts has been rarely reported. Thisclinical report describes a rare ABC involved in the mandibu-
∗Correspondence: Xu-Dong Wang; Email: [email protected]; Address: Department of Oral & Cranio-maxillofacial Science, ShanghaiNinth People’s Hospital; Shanghai Jiao Tong University School of Medicine, Shanghai Key Laboratory of Stomatology, No.639 Zhizaoju Road, Shanghai200011, People’s Republic of China.
Published by Sciedu Press 1
http://css.sciedupress.com Case Studies in Surgery 2016, Vol. 2, No. 3
lar condyle and ramus with the final treatment of curettageunder endoscopic vision and introduction of bovine hydrox-yapatite (Bio-Oss, Geistlich, Switzerland).
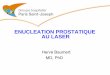
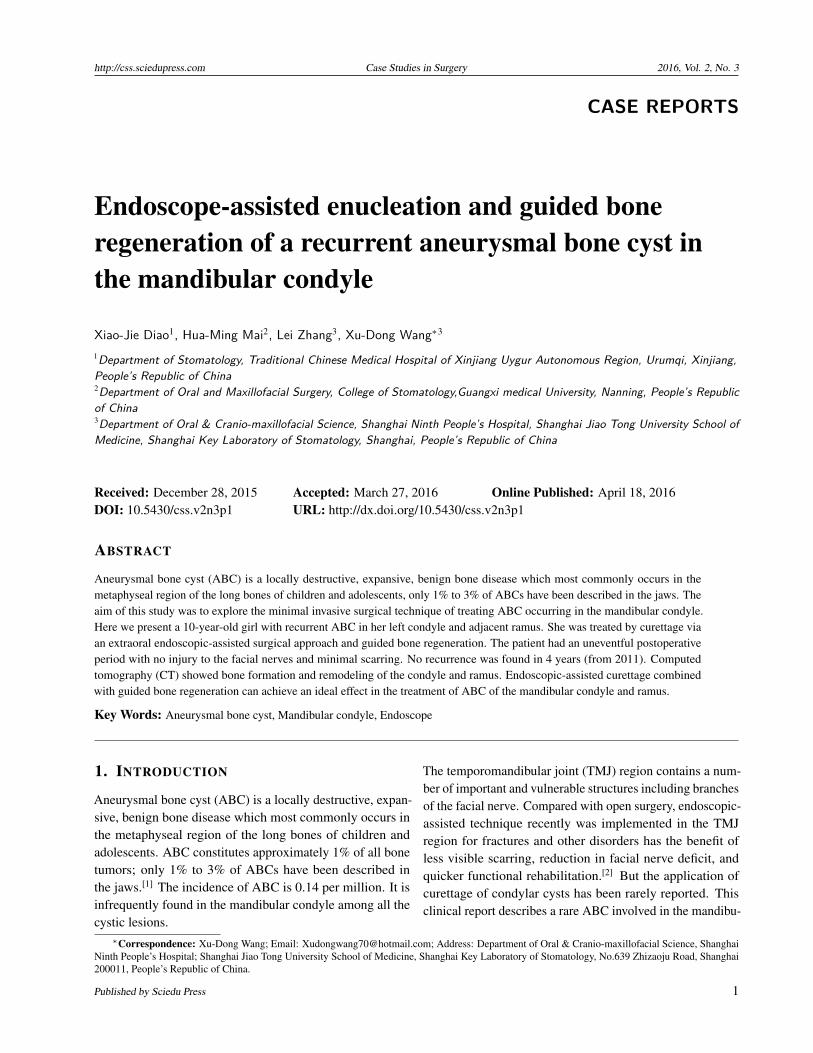
2. CASE REPRESENTATION2.1 PatientA 10-year-old, otherwise healthy Chinese girl with no historyof trauma or other TMJ problems presented to our hospitalwith a 2-month history of a painless swelling of the left TMJregion in February 2010. Preoperative Magnatic ResonanceImaging (MRI) showed a T1 hypointense and T2 hyperin-tense homogenous lesion with some internal septation in theleft condyle and adjacent ramus (see Figure 1A). The lesionwas measured 29 mm × 22 mm. A computed tomography(CT) scan showed thinned, but intact, cortical bone with mul-tiple, thickened septations within the lesion (see Figures 1Band 1C). Three-dimensional CT reconstruction revealed amultiloculated cystic mass in the condyle and upper half ofthe ramus (see Figure 1D). Radiologic differential diagnosisincluded cystic lesion and benign giant cell lesion. Frozen-section examination revealed a hemorrhagic fibrovascularcyst wall with hemosiderin deposition and abundant multinu-cleated giant cells, features consistent with ABC. Therefore,curettage of the lesion was performed through the conven-tional submandibular incision. Eighteen months postsurgery,a follow-up CT scan revealed a destructive radiolucent lesionin the left condyle (see Figure 2A). The lesion was 28 mm× 15 mm × 7 mm in size, larger than the 19 mm-lesionscanned 6 months postoperatively. MRI (see Figure 2B) re-vealed two separate, T2 hyperintense homogenous massesin the condyle, without symptoms or patient discomfort. Di-agnosed with a relapsed ABC, the girl was subjected to asecond surgery in August 2011.
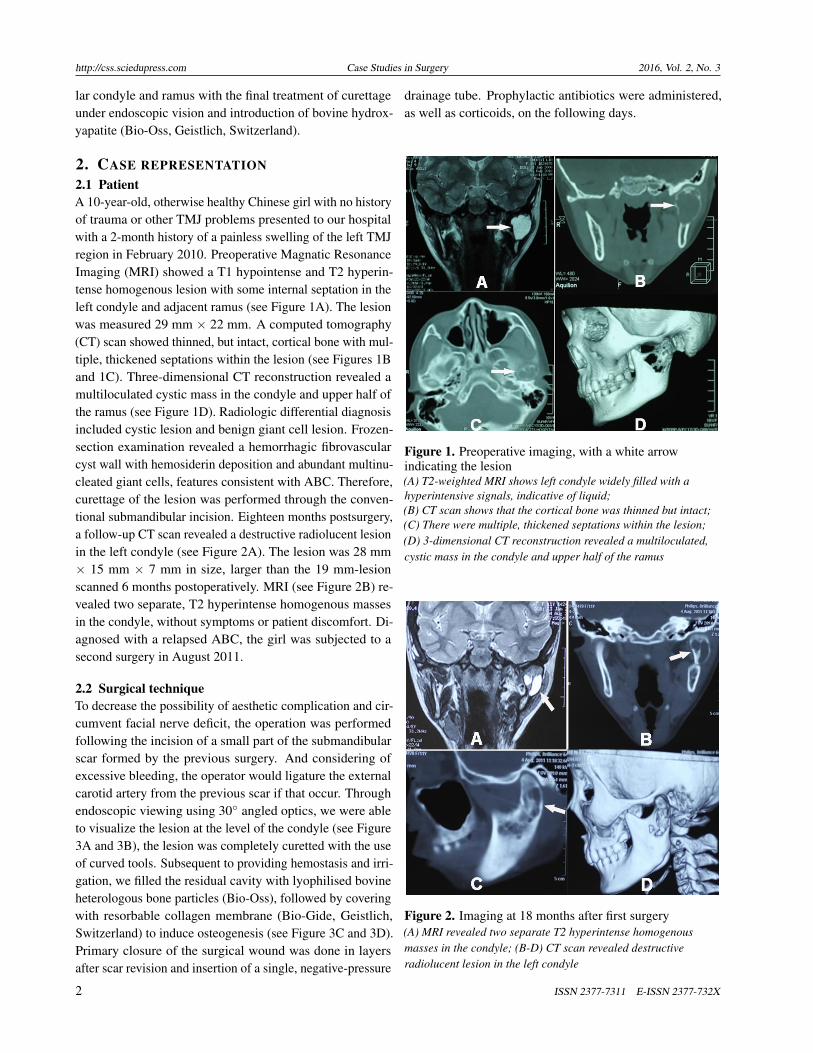
2.2 Surgical techniqueTo decrease the possibility of aesthetic complication and cir-cumvent facial nerve deficit, the operation was performedfollowing the incision of a small part of the submandibularscar formed by the previous surgery. And considering ofexcessive bleeding, the operator would ligature the externalcarotid artery from the previous scar if that occur. Throughendoscopic viewing using 30◦ angled optics, we were ableto visualize the lesion at the level of the condyle (see Figure3A and 3B), the lesion was completely curetted with the useof curved tools. Subsequent to providing hemostasis and irri-gation, we filled the residual cavity with lyophilised bovineheterologous bone particles (Bio-Oss), followed by coveringwith resorbable collagen membrane (Bio-Gide, Geistlich,Switzerland) to induce osteogenesis (see Figure 3C and 3D).Primary closure of the surgical wound was done in layersafter scar revision and insertion of a single, negative-pressure
drainage tube. Prophylactic antibiotics were administered,as well as corticoids, on the following days.
Figure 1. Preoperative imaging, with a white arrowindicating the lesion(A) T2-weighted MRI shows left condyle widely filled with ahyperintensive signals, indicative of liquid;(B) CT scan shows that the cortical bone was thinned but intact;(C) There were multiple, thickened septations within the lesion;(D) 3-dimensional CT reconstruction revealed a multiloculated,cystic mass in the condyle and upper half of the ramus
Figure 2. Imaging at 18 months after first surgery(A) MRI revealed two separate T2 hyperintense homogenousmasses in the condyle; (B-D) CT scan revealed destructiveradiolucent lesion in the left condyle
2 ISSN 2377-7311 E-ISSN 2377-732X
http://css.sciedupress.com Case Studies in Surgery 2016, Vol. 2, No. 3
Figure 3. Stages of endoscope-assisted surgery with a bluearrow indicating the lesion(A) Visualisation of the lesion in the condyle; Residual cavity (B)was filled with Bio-Oss (C), followed by covering with Bio-Gidecollagen membrane (D)
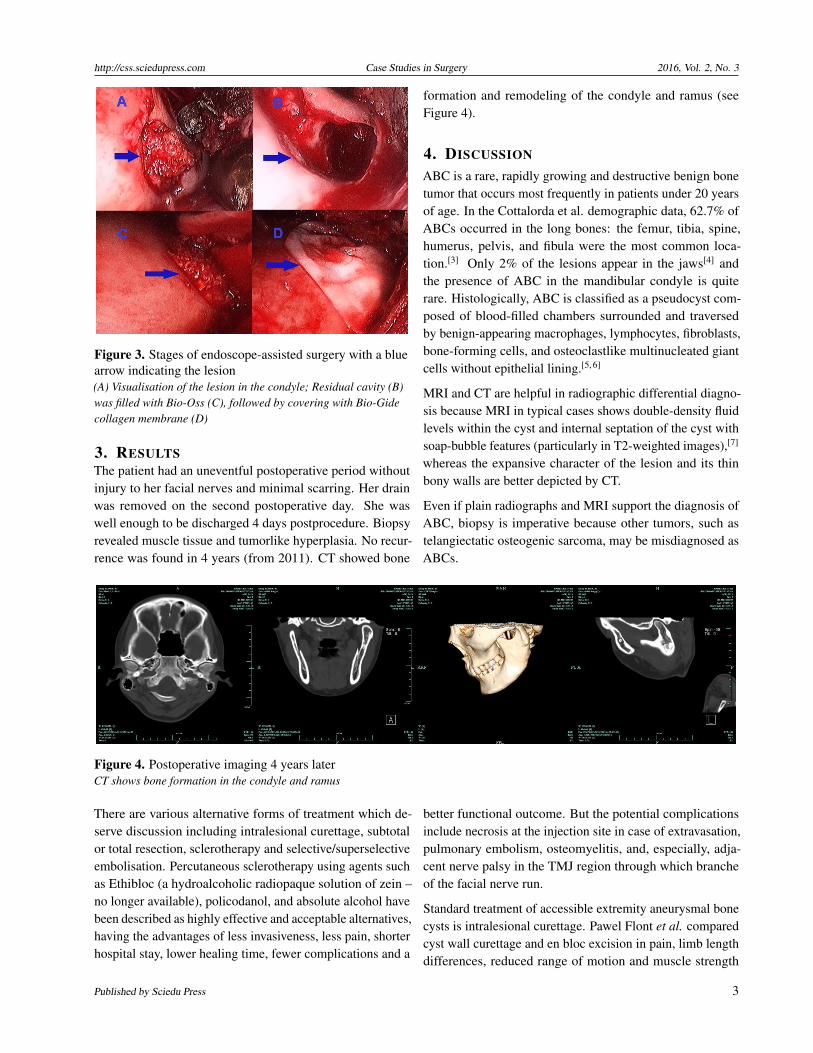
3. RESULTSThe patient had an uneventful postoperative period withoutinjury to her facial nerves and minimal scarring. Her drainwas removed on the second postoperative day. She waswell enough to be discharged 4 days postprocedure. Biopsyrevealed muscle tissue and tumorlike hyperplasia. No recur-rence was found in 4 years (from 2011). CT showed bone
formation and remodeling of the condyle and ramus (seeFigure 4).
4. DISCUSSION
ABC is a rare, rapidly growing and destructive benign bonetumor that occurs most frequently in patients under 20 yearsof age. In the Cottalorda et al. demographic data, 62.7% ofABCs occurred in the long bones: the femur, tibia, spine,humerus, pelvis, and fibula were the most common loca-tion.[3] Only 2% of the lesions appear in the jaws[4] andthe presence of ABC in the mandibular condyle is quiterare. Histologically, ABC is classified as a pseudocyst com-posed of blood-filled chambers surrounded and traversedby benign-appearing macrophages, lymphocytes, fibroblasts,bone-forming cells, and osteoclastlike multinucleated giantcells without epithelial lining.[5, 6]
MRI and CT are helpful in radiographic differential diagno-sis because MRI in typical cases shows double-density fluidlevels within the cyst and internal septation of the cyst withsoap-bubble features (particularly in T2-weighted images),[7]
whereas the expansive character of the lesion and its thinbony walls are better depicted by CT.
Even if plain radiographs and MRI support the diagnosis ofABC, biopsy is imperative because other tumors, such astelangiectatic osteogenic sarcoma, may be misdiagnosed asABCs.
Figure 4. Postoperative imaging 4 years laterCT shows bone formation in the condyle and ramus
There are various alternative forms of treatment which de-serve discussion including intralesional curettage, subtotalor total resection, sclerotherapy and selective/superselectiveembolisation. Percutaneous sclerotherapy using agents suchas Ethibloc (a hydroalcoholic radiopaque solution of zein –no longer available), policodanol, and absolute alcohol havebeen described as highly effective and acceptable alternatives,having the advantages of less invasiveness, less pain, shorterhospital stay, lower healing time, fewer complications and a
better functional outcome. But the potential complicationsinclude necrosis at the injection site in case of extravasation,pulmonary embolism, osteomyelitis, and, especially, adja-cent nerve palsy in the TMJ region through which brancheof the facial nerve run.
Standard treatment of accessible extremity aneurysmal bonecysts is intralesional curettage. Pawel Flont et al. comparedcyst wall curettage and en bloc excision in pain, limb lengthdifferences, reduced range of motion and muscle strength
Published by Sciedu Press 3

http://css.sciedupress.com Case Studies in Surgery 2016, Vol. 2, No. 3
impairment. The result is that the differences were not sta-tistically significant (p > .05).[8] Curettage with or withoutbone grafting is the mainstay of treatment.[9] Recurrencerates after curettage have varied widely in different reports.According to a review of 690 ABCs treated with curettageand bone grafting and summarised by Cottalorda et al.,[10]therecurrence rate in this series varied from 18% to 59%; theoverall recurrence rate was 31%. However, in a retrospectiveclinical study of 17 cases of ABCs of the mandible treatedwith complete surgical curettage without bone grafting, therewere no recurrences. The recurrence rate may be related tothe location of the lesions, diameter of the cortical window,and individual operative procedures. Before entering thelesion, one should adequately expose it to enable a rapidcurettage. The large diameter of the cortical window mayfacilitate observation of the interior of the cyst and result ina low recurrence rate.[11] En bloc resection is the treatmenthaving the lowest risk of local recurrence, but it must be con-sidered only when there is no other treatment option becauseof the loss of the condyle and subsequent growth arrest ofthe mandible in such case.
With the advantages of minimally invasive surgery – de-creased morbidity, improved visualisation, surgical precision,reduction in facial nerve deficit, and quicker functional re-habilitation – endoscopic surgery has been developed in thespecialty of maxillofacial surgery mostly for trauma, orthog-nathic surgery, sialoendoscopy, and TMJ disease. However,only two papers describe the removal of mandibular or condy-lar lesions; the present case is the first case describing theapplication of curettage of ABCs. Because of the need to trim
the scar left by the first surgery, extroral access was designedto insert the endoscope through a small submandibular scarincision and smoothly reach the operating field, providing adetailed magnification of the images. Thus, complete curet-tage of the lesion was attained with reliable instrumentalsupport.
Given that there was a deep cavity left after curettage of thecyst and there had been recurrence, the cavity was filled withBio-Oss (a natural bone substitute obtained from the mineralportion of bovine bone that closely resembles human bone),resulting in effective bone regeneration. This idea was en-couraged by the reports of Delloye and coworkers,[12, 13]whodescribed 13 cases of ABCs receiving grafts of demineralisedbone and autogenous bone marrow to induce healing of thecyst without curettage. Eleven cases had successful healingafter a mean follow-up period of 3.9 years. The rationale un-derlying this intralesional treatment was the expectation thatthe bone-grafting material would reverse cystic expansion bypromoting ossification through a bone-induction mechanism.To our knowledge, this is the first case describing the clini-cal application of guided bone regeneration of a cyst of themandiblular condyle.
5. CONCLUSIONS
Although this procedure needs more long-term follow-upconfirmation, endoscopic-assisted curettage combined withgrafting of bovine heterologous bone particles may becomethe ideal treatment for the ABC of the mandibular condyleand ramus.
REFERENCES[1] Jundt G, Prein J. Bone tumors and tumor-like lesions of the jaw.
Findings from the Basel DOSAK reference registry. Mund KieferGesichtschir 2000; 4 Suppl 1: S196-207. PMid: 10938660. http://dx.doi.org/10.1007/PL00014541
[2] Schmelzeisen R, Cienfuegos-Monroy R, Schon R, et al. Patient bene-fit from endoscopically assisted fixation of condylar neck fractures–arandomized controlled trial. J Oral Maxillofac Surg. 2009; 67: 147-158. PMid: 19070761. http://dx.doi.org/10.1016/j.joms.2008.09.019
[3] Cottalorda J, Kohler R, Sales de Gauzy J, et al. Epidemiology ofaneurysmal bone cyst in children: a multicenter study and literaturereview. J Pediatr Orthop B. 2004; 13: 389-94. PMid: 15599231.http://dx.doi.org/10.1097/01202412-200411000-00008
[4] Kaffe I, Naor H, Calderon S, et al. Radiological and clinical featuresof aneurysmal bone cyst of the jaws. Dentomaxillofac Radiol. 1999;28: 167-172. PMid: 10740472. http://dx.doi.org/10.1038/sj.dmfr.4600434
[5] Mendenhall WM, Zlotecki RA, Gibbs CP, et al. Aneurysmal bonecyst. Am J Clin Oncol. 2006; 29: 311-15. PMid: 16755186. http:
//dx.doi.org/10.1097/01.coc.0000204403.13451.52
[6] Mankin HJ, Hornicek FJ, Ortiz-Cruz E, et al. Aneurysmal bone cyst:a review of 150 patients. J Clin Oncol. 2005; 23: 6756-6762. PMid:16170183. http://dx.doi.org/10.1200/JCO.2005.15.255
[7] Sullivan RJ, Meyer JS, Dormans JP, et al. Diagnosing aneurys-mal and unicameral bone cysts with magnetic resonance imag-ing. Clin Orthop Relat Res. 1999: 186-190. PMid: 10627734.http://dx.doi.org/10.1097/00003086-199909000-00024
[8] Flont P, Kolacinska-Flont M, Niedzielski K. A comparison of cystwall curettage and en bloc excision in the treatment of aneurysmalbone cysts. World Journal of Surgical Oncology. 2013; 11(10): 238-242. PMid: 23701661. http://dx.doi.org/10.1186/1477-7819-11-109
[9] Dios AMVD, Bond JR, Shives TC, et al. Aneurysmal bone cyst. Aclinicopathologic study of 238 cases. Cancer. 1992; 69(12): 2921-2931. http://dx.doi.org/10.1002/1097-0142(19920615)69:12<2921::AID-CNCR2820691210>3.0.CO;2-E
[10] Cottalorda J, Bourelle S. Current treatments of primary aneurys-mal bone cysts. J Pediatr Orthop B. 2006; 15: 155-167.
4 ISSN 2377-7311 E-ISSN 2377-732X

http://css.sciedupress.com Case Studies in Surgery 2016, Vol. 2, No. 3
PMid: 16601582. http://dx.doi.org/10.1097/01.bpb.0000210588.50899.29
[11] Dormans JP, Hanna BG, Johnston DR. Surgical treatment and recur-rence rate of aneurysmal bone cysts in children. Clin Orthop RelatRes. 2004: 205-211. PMid: 15123949. http://dx.doi.org/10.1097/01.blo.0000126336.46604.e1
[12] Delloye C, De Nayer P, Malghem J, et al. Induced healing of aneurys-
mal bone cysts by demineralized bone particles. A report of two cases.Arch Orthop Trauma Surg. 1996; 115: 141-145. PMid: 8861578.http://dx.doi.org/10.1007/BF00434541
[13] Docquier PL, Delloye C. Treatment of aneurysmal bone cysts byintroduction of demineralized bone and autogenous bone marrow.J Bone Joint Surg Am. 2005; 87: 2253-2258. PMid: 16203891.http://dx.doi.org/10.2106/JBJS.D.02540
Published by Sciedu Press 5


![The Technique of Tonsil Enucleation - Semantic Scholar...Dec., 1936] TECHNIQUE OF TONSIL ENUCLEATION: WILLIAMSON 727 Special Article THE TECHNIQUE OF TONSIL ENUCLEATION By H. WILLIAMSON,](https://img.dokumen.tips/doc/110x75/5e9dc57b42f70b199c246bec/the-technique-of-tonsil-enucleation-semantic-scholar-dec-1936-technique.jpg)