Embed Size (px)
Citation preview
![Page 1: The Technique of Tonsil Enucleation - Semantic Scholar...Dec., 1936] TECHNIQUE OF TONSIL ENUCLEATION: WILLIAMSON 727 Special Article THE TECHNIQUE OF TONSIL ENUCLEATION By H. WILLIAMSON,](https://reader030.dokumen.tips/reader030/viewer/2022040603/5e9dc57b42f70b199c246bec/html5/thumbnails/1.jpg)
Dec., 1936] TECHNIQUE OF TONSIL ENUCLEATION: WILLIAMSON 727
Special Article
THE TECHNIQUE OF TONSIL ENUCLEATION
By H. WILLIAMSON, o.b.e., m.d., f.r.c.s.e., m.r.c.p.,
MAJOR, I.M.S.
Foreign and Political Department, Government of India
Although this operation is simple, safe, short and effective, and needs only such
instruments as are to be found in any Indian
hospital, it seems to be done by surprisingly few people. As any examination of school
children's throats will show that there is no
lack of material, it must be assumed that there is a lack of familiarity with the details of
technique, careful attention to which is neces-
sary for success, so it may be helpful to set
these forth.
A full discussion of the indications for
tonsillectomy is beyond the scope of this article, but it is generally agreed that tonsils should be removed when they obstruct respiration, become frequently inflamed, or cause more than
temporary enlargement of the glands behind the jaw. Inflamed, cedematous tonsils should not be mistaken for chronically enlarged ones, as their removal may be followed by severe
haemorrhage, so in doubtful cases it is best to
try the effect of a week's gargling. Fibrotic
atrophied '
septic-focus ' tonsils should be dis-
sected out, but large tonsils are more loosely attached, especially in children, and can be
easily and completely removed with the blunt guillotine. The wise beginner will operate first on children, preferably about five years old: | he will also enquire about any history of
bleeding. uU
Instruments
The guillotines supplied to Indian hospitals are usually sharp, but the blade can be suit -
ably blunted on a file and oilstone, or a
bazaar mistri will do it for a few annas. The
perfect blade is as blunt as a silver butter
knife, in fact it is difficult to make it too blunt. When the blade has been blunted the surgeon should see that it shuts properly; if it does
not, the slot in the shaft should be lengthened with a small file until the blade goes well home into the ring of the instrument. Except for
enormous tonsils, guillotines of the two smaller sizes suffice, as too large a guillotine is apt to
damage the soft palate or uvula, and the tonsil cannot be crowded into it, while too small a
one will not take the whole tonsil.
Doyen's mouth gag is very satisfactory, as
it gives a good view and does not get ̂
in the
way. A tonsil punch forceps is useful in case
the lingual or pharyngeal tonsil does not come
away cleanly. An adenoid curette, some
Spencer Wells and Kocher's forceps, some
swabs and a bowl of iced water complete the outfit. I use forceps instead of swab holders as they are quicker to load, stronger, and less liable to drop a swab. The best light is a
good headlight, but a powerful electric torch held by an intelligent nurse or assistant does
very well.
Position of the patient The patient lies on his back with the head
well extended.
Anaesthetic
It should be remembered that when chloro- form is given to children, especially if they go under quickly, the anaesthesia may deepen for about two minutes alter the mask is removed. This may be a source of great danger from
asphyxia due either to the chloroform itself or
to obstruction of the airway by blood clots. It is therefore safest to give a preliminary injection of atropin and to use a chloroform- ether mixture. As soon as the patient's jaw relaxes the mask is removed, the Doyen's gag inserted and the operation begun. With a
perfect anaesthetic the coughing reflex is hardly lost and the patient begins to '
gag' as the second tonsil is removed. I have not found basal anaesthesia very suitable as the patient is unconscious for longer than necessary and the depth of anaesthesia is difficult to control. A local anaesthetic is more suitable for dis- section, but I have used it once or twice for enucleation in nervous adults.
The operation
Step 1.?Doyen's gag is inserted between the patient's incisor teeth, with the handle on the left cheek, and is opened wide enough to give a good view of the back of the throat. Two
points require attention, breathing should not
be obstructed and the jaw should not be dis- located. A quick operator does not worry much about the former, which can be prevented by twisting the gag a little so as to bring the lower jaw forward, or the gag may be closed
slightly. Dislocation of the jaw, it need hardly be said, should not occur, but if it does, reduc- tion should be deferred till the operation is finished, and is quite easy under the anaesthetic. I have seen it happen once or twice, but no ill effects seemed to follow, though it cannot
be called beneficial.
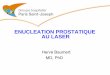
Step 2 (figure 1).?The operator stands at
the patient's right side, facing the mouth. The
closed guillotine held in the right hand is
inserted, the back of the patient's tongue pressed well down, and both tonsils examined.
Step 3 (figure 2).?The right tonsil is dealt
with first. The blade of the guillotine is opened and the ring pushed underneath the tonsil, between it and the posterior pillar of the fauces.
![Page 2: The Technique of Tonsil Enucleation - Semantic Scholar...Dec., 1936] TECHNIQUE OF TONSIL ENUCLEATION: WILLIAMSON 727 Special Article THE TECHNIQUE OF TONSIL ENUCLEATION By H. WILLIAMSON,](https://reader030.dokumen.tips/reader030/viewer/2022040603/5e9dc57b42f70b199c246bec/html5/thumbnails/2.jpg)
728 THE INDIAN MEDICAL GAZETTE [Dec., 1936
The tonsil is now lifted towards the naso-
pharynx, the operator's left thumb helping to engage it in the guillotine.
Step 4 (figures 3 and 4).?This is the most
important step of all, and on its correct per- formance depends the completeness with which the tonsil is removed.
The guillotine is turned so that it lies as
nearly as possible across the mouth, with the blade facing the operator, who pushes the ring of the instrument into the space between the tonsil and the posterior pillar, and at the same time presses the distal end, and hence the
tonsil, well forward, while his left thumb continues to press the tonsil lightly into the hole in the guillotine. The instrument is now drawn towards the opposite side, thus bringing the tonsil towards the mid line and stretching the anterior pillar. When this is done the
surgeon's left thumb presses the tonsil firmly and completely into the hole in the guillotine. The effect of this manoeuvre, which perhaps sounds intricate but is really quite simple, is not only to engage the tonsil fully, but also to turn the pillars of the fauces practically inside out, a point not always realized: the
line of cleavage is thus made straight or
slightly convex. Figure 4 shows the position in horizontal section. It also shows how the anterior pillar may be damaged if the guillotine is not lying across the mouth, or button-holed if the left thumb presses too hard. When the manoeuvre is correctly carried out the left thumb will feel a very distinct dimple as soon as the whole tonsil has passed through the ring. Until this dimple is felt the operator can be sure that the tonsil is not fully engaged, and must not close the blade. A careful watch should be kept to see that the uvula is not dragged in too.
The smallest guillotine that will fit the tonsil
snugly is the best, in fact the smallest size
supplied to hospitals does for most cases, but if the tonsil is so big that it cannot be pushed right in and thus produce a good dimple a
larger instrument should be used. When the tonsil is thus properly engaged
the blade of the guillotine is pushed firmly home, care being taken that it passes exactly between the tonsil and the anterior pillar, while the left thumb keeps the tonsil in position. As the blade passes under the thumb the pressure of the latter should be suitably relaxed to
prevent button-holing of the anterior pillar, and when the blade is home the left thumb is removed. From now until the tonsil is outside the
mouth it is absolutely essential to keep the blade of the guillotine tightly pressed home,
Fig. 1.?Inspecting the tonsils. Fig. 1.?Inspecting the tonsils.
Fig. 2.?Lifting the tonsil on to the guillotine. Fig. 2.?Lifting the tonsil on to the guillotine.
30*
Fig. 3.?Pressing the tonsil forward with the guillotine and pressing it into the ring with the left thumb.
Fig. 3? Pressing the tonsil forward with the guillotine and pressing it into the ring with the left thumb.
To S TE0IO# ? WALL ?P TKAgyAlX
TasTCKioR ) Plt-LA R. ofL , , ._5 rAvcej j
AtVTE.RrOfi) .
PlLI.AR.y
"SUAiC OP1
G-v I ui-0-rtrtB
ANreKtoK) TiLLAKJ
Fig. 4.?Horizontal section through figure 3, showing the tonsil in position for enucleation. The upper figure
shows the normal position by way of contrast.
Fig. 4.?Horizontal section through figure 3, showing the tonsil in position for enucleation. The upper figure
shows the normal position by way of contrast.
![Page 3: The Technique of Tonsil Enucleation - Semantic Scholar...Dec., 1936] TECHNIQUE OF TONSIL ENUCLEATION: WILLIAMSON 727 Special Article THE TECHNIQUE OF TONSIL ENUCLEATION By H. WILLIAMSON,](https://reader030.dokumen.tips/reader030/viewer/2022040603/5e9dc57b42f70b199c246bec/html5/thumbnails/3.jpg)
Dec., 1936] TECHNIQUE OF TONSIL ENUCLEATION: WILLIAMSON 729
otherwise the tonsil will slip and be incom-
pletely removed, in fact, I use both hands and press with both thumbs, as this gives more command of the guillotine and increases the pressure on the blade. With the blunt blade there is no danger that the surgeon will cut
through the tonsil prematurely and have the mortification of seeing it disappear down the
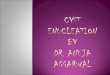
pharynx. Step 5 (figure 5).?The tour de maitre, so
named by Samuel Whillis, the inventor of the operation", is begun as follows: the operator's right hand is pronated and the left supinated,
so that the tonsil, now lying on the back 01
the instrument, is twisted upwards towards the naso-pharynx, and drawn out of its bed.
Step 6 {figure 6) .?The tour de maitre is con- tinued until the right wrist is fully pronated and the left fully supinated, so that the back of the guillotine, with the tonsil on it, faces
the hard palate. A fairly sharp yet purpose- ful tug towards the opposite side now com-
pletely avulses the tonsil, which usually comes ?ut '
dragging its tail behind itThe final
pull may need a little force, a point not always realized at first, but a little practice teaches one just how much to use. One must also
remember to maintain the pressure on the
blade with the thumbs. Step 7 (removing the left tonsil).?The
operator stands by the patient's right shoulder, facing the left one, and the guillotine is again taken in the right hand, but the tour de maitre is of course carried out by supinating the right wrist and pronating the left, so as to turn the tonsil up towards the naso-pharynx as before.
I have noticed that beginners often find the
left tonsil harder to remove than the right, but the trouble is overcome if, as pointed out in
step 4 above, the tonsil and anterior pillar are drawn well into the mid line and at the same |
time pressed firmly forward by the guillotine; this also helps to make the tonsil more visible by clearing it of the blood at the back of the mouth. The anterior pillar flattens out and the dimple is easy to make with the left thumb. If it is difficult to engage the tonsil in the ring of the guillotine the left index finger should be passed under the lower pole and guided in.
Step 8.?The tonsil beds are now felt care-
fully with the finger, or swabbed out and
inspected. If any small pieces have been left behind they are removed with the punch forceps, while a larger fragment, if attached to the back of the anterior pillar, may be pressed into the guillotine and avulsed. If the opera- tion has been well done the tonsil beds will feel quite smooth, but tags of muscle must
not be mistaken for pieces of tonsil. Removal of adenoids.?The right forefinger
is passed up behind the uvula, and the posterior wall of the naso-pharynx palpated. For some reason adenoids are far less common among Indians than are enlarged tonsils, but if they are present they are felt as definite soft masses on the back wall of the naso-pharynx. If adenoids are to be removed, the left forefinger, with the pad towards the operator, replaces the right and firmly hooks the uvula and soft
palate forward. The adenoid curette is in- serted well up behind the soft palate and not more than two firm sweeps made down the back wall of the naso-pharynx. If the patient is 'gagging' this may be a little difficult, and the operator must make sure that the curette
is behind the soft palate and not in front of it ! It should be remembered that as the cage of the curette is curved the handle should be held towards the patient's head, so that the blade and not the heel of the instrument is
against the adenoids. I like St. Clair Thom- son's curette, as the teeth of the cage prevent the adenoids from dropping. The blade must be sharp. The operation being now finished, the
patient is turned on his side, with the head lowered enough to allow the blood to run out of the mouth and nose, but not so as to impede the venous return. The face is now well
splashed with iced water, which usually stops the bleeding, and the gag is removed.
Haemorrhage As the blunt blade crushes the vessels instead
of cutting them excessive haemorrhage is rare
if the tonsils are not actively inflamed or the patient a bleeder.
Occasionally, however, severe bleeding may occur, and the surgeon should have a definite
plan of campaign. I have found the following method successful. Some more antesthetic is
given and the mouth gag re-inserted. The
patient's tongue is now well depressed, the
pharynx well swabbed, and a hot swab on
forceps firmly pressed into each tonsillar fossa
/
Fig. 5.?Beginning of the tour de maitre.
The tonsil is being twisted out of its bed. Fig. 5.?Beginning of the
tour de maitre.
The tonsil is being twisted out of its bed.
3&>'
Fig. 6.?The tour de maitre is completed and the tonsil is avulsed.
Fig. 6.?The tour de maitre is completed and the tonsil is avulsed.
![Page 4: The Technique of Tonsil Enucleation - Semantic Scholar...Dec., 1936] TECHNIQUE OF TONSIL ENUCLEATION: WILLIAMSON 727 Special Article THE TECHNIQUE OF TONSIL ENUCLEATION By H. WILLIAMSON,](https://reader030.dokumen.tips/reader030/viewer/2022040603/5e9dc57b42f70b199c246bec/html5/thumbnails/4.jpg)
730 THE INDIAN MEDICAL GAZETTE [Dec., 1936
and held there for five minutes by the clock. One swab is now removed and if no bleeding occurs the other is removed also. If a bleed-
ing point can be seen it is caught in Kocher's forceps. If for any reason it is impossible to see exactly where the blood is coming from, the upper and lower poles of each tonsillar fossa are caught in Kocher's forceps: as the blood supply of the tonsils comes from these
points this manoeuvre stops the bleeding, though if the mouth is well opened and the tongue
well depressed it is usually possible to see the bleeding points. The forceps should be left on for three or four hours, or the tissue caught in them tied off with a slip knot run down the blades of the forceps. As this is not so
easy as it sounds those who have not practised it are advised to leave the forceps in position for a few hours, during which some morphia and hsemoplastin may be given subcutaneously and 10 c.cm. of 10 per cent calcium chloride
intravenously.