-
Behavior Change
Dr. Oryzati Hilman Agrimon, MSc.CMFM, PhD (C) PhD Candidate in
General Practice/ Family Medicine, the University of Adelaide,
Australia Lecturer Department of Public Health and Family Medicine
Faculty of Medicine and Health Sciences Universitas Muhammadiyah
Yogyakarta
-
Discussion Topics Background for Behavior Change
The Behavior Change Model
The Ladder of Change
Lifestyle Modification Counseling
-
Is changing (unhealthy) behaviors easy or difficult to
do...?
-
What can a doctor do to help the patient change his/her
unhealthy behaviors...?
-
Background for Behavior Change .The health profession must find
the most effectivemeans of extending the benefits of good health
for allIt is necessary to find ways to extend the benefits ofgood
health to the most vulnerable and promote responsible behavior and
the adoption of lifestylesthat are conducive to good health
-
. Helping patients change behavior is an important role for
family physicians. Change interventions are especially useful in
addressing lifestyle modification for disease prevention, long-term
disease management and addictions. The concepts of "patient
noncompliance" and motivation often focus on patient failure
Understanding patient readiness to make change, appreciating
barriers to change and helping patient anticipate relapse can
improve patient satisfaction and lower physician frustration during
the change process.
-
Behavior Change .Behavior change is rarely a discrete, single
event; the patient moves gradually from being uninterested
(pre-contemplation stage) to considering a change (contemplation
stage) to deciding andpreparing to make a change. Most people find
themselves "recycling" through the stages of change several times
("relapsing") before the change becomes truly established.
-
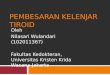
Behavior Change Model(Prochaska & DiClemente, 1992) .
-
Pre-Contemplation Stage . During the pre-contemplation stage,
patients do not even consider changing Smokers who are "in denial"
may not see that the advice applies to them personally. Patients
with high cholesterol levels may feel "immune to the health
problems that strike others. Obese patients may have tried
unsuccessfully so many times to lose weight that they have simply
given up.
-
Contemplation Stage . During the contemplation stage, patients
are ambivalent about changing. Giving up an enjoyed behavior causes
them to feel a sense of loss despite the perceived gain During this
stage, patients assess barriers (e.g., time, expense, hassle, fear,
"I know I need to, doc, but ...") as well as the benefits of
change.
-
Preparation Stage . During the preparation stage, patients
prepare to make a specific change. They may experiment with small
changes as their determination to change increases. For example,
sampling low-fat foods may be an experimentation with or a move
toward greater dietary modification. Switching to a different brand
of cigarettes or decreasing their drinking signals that they have
decided that the change is needed.
-
Action Stage . The action stage is the one that most physicians
are eager to see their patients reach. Many failed New Year's
resolutions provide evidence that if the prior stages have been
glossed over, action itself is often not enough. Any action taken
by patients should be praised because it demonstrates the desire
for lifestyle change.
-
Maintenance & Relapse Prevention
Maintenance and relapse prevention involve incorporating the new
behavior "over the long haul." Discouragement over occasional
"slips" may halt the change process and result in the patient
giving up. However, most patients find themselves "recycling"
through the stages of change several times before the change
becomes truly established.
-
Stages of Change Model .Stage in transtheoretical Patient stage
Incorporating other explanatory/ model of change treatment
models.
Pre-contempla-tion Not thinking about change May be resigned
Feeling of no control Denial: does not believe it applies to self
Believes consequences are not serious Locus of Control Health
Belief Model Motivational interviewingContemplation Weighing
benefits and costs of behavior, proposed change Health Belief Model
Motivational interviewingPreparation Experimenting with small
changes Cognitive-behavioral therapyAction Taking a definitive
action to change Cognitive-behavioral therapy 12-Step
programMaintenance Maintaining new behavior over time
Cognitive-behavioral therapy 12-Step programRelapse Experiencing
normal part of process of change Usually feels demoralized
Motivational interviewing 12-Step program
-
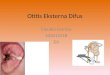
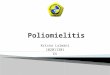
The Ladder of Change (Bohtello, 2004) .
-
.
Step 1: Building a partnership:Developing empathy, clarifying
roles & responsibilities and using relational skills
effectively Step 2: Negotiating an agenda: Using preventive or
problem-based approaches to negotiate a shared agenda
-
.
Step 3: Assessing resistance & motivation:Asking about
patients readiness to change, their reasons for staying the same
(resistance) and their reasons for change (motivation), and their
levels of resistance & motivationStep 4: Enhancing mutual
understanding: Understanding & addressing how you & your
patients have differences in perceptions & values about reasons
for staying the same and for changing; or, reducing patients
resistance, increasing their motivation, and thereby helping them
to take charge of their health
-
.
Step 5: Implementing a plan for change:Negotiating an
appropriate plan with your patients based on your mutual
understanding; for example, thinking more about change, preparing
to change and taking baby steps or giant leaps toward changeStep 6:
Following through: Negotiating about the need and timing for
futureclinical encounters
-
Lifestyle Modification Counseling
-
Hal-hal yang Diperlukan untuk Konseling Perubahan Perilaku
A. Gabungan Komunikasi Verbal & Komunikasi Non-Verbal B.
Sikap Empati & Dapat Dipercaya C. Ketrampilan Mendengar AktifD.
Memahami konsep the Behavior Change Model & the Ladder of
Change
-
A. Komunikasi Verbal dan Non-Verbal 1. Komunikasi Verbal
Kata-kata yang diucapkan secara lisan2. Komunikasi Non-Verbal
Menjaga tatapan mata Ekspresi wajah ramah, tersenyum Postur tubuh
terbuka Artikulasi suara jelas & intonasi tepat Penampilan
bersih & rapi
-
B. Sikap Empati dan Dapat Dipercaya 1. Empati Kemampuan untuk
mengenali, memahami dan merasakan secara langsung emosi orang
lain2. Dapat Dipercaya Bisa menunjukkan integritas profesi sesuai
dengan kompetensi dokter Memelihara dan menjaga harga diri pasien,
hal-hal yang bersifat pribadi, dan kerahasiaan pasien sepanjang
waktu
-
C. Ketrampilan Mendengarkan Aktif Ketrampilan mendengarkan
secara aktif dengan melakukan: Refleksi Isi Refleksi Perasaan
-
D. Memahami konsep the Behavior Change Model & the Ladder of
Change
-
Thank you for your attention!Questions are most welcome!
Wassalamu alaikum Wr.Wb
**