Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Treatment of Intracerebral Hemorrhagein Animal Models: Meta-Analysis
Joseph Frantzias, BSc, Emily S. Sena, PhD, Malcolm R. Macleod, PhD,
and Rustam Al-Shahi Salman, MA, PhD
Objective: Interventions that improve functional outcome after acute intracerebral hemorrhage (ICH) in animalsmight benefit humans. Therefore, we systematically reviewed the literature to find studies of nonsurgical treatmentstested in animal models of ICH.Methods: In July 2009 we searched Ovid Medline (from 1950), Embase (from 1980), and ISI Web of Knowledge(from 1969) for controlled animal studies of nonsurgical interventions given after the induction of ICH that reportedneurobehavioral outcome. We assessed study quality and performed meta-analysis using a weighted meandifference random effects model.Results: Of 13,343 publications, 88 controlled studies described the effects of 64 different medical interventions(given a median of 2 hours after ICH induction) on 38 different neurobehavioral scales in 2,616 treated or controlanimals (median 14 rodents per study). Twenty-seven (31%) studies randomized treatment allocation, and 7 (8%)reported allocation concealment; these studies had significantly smaller effect sizes than those without theseattributes (p < 0.001). Of 64 interventions stem cells, calcium channel blockers, anti-inflammatory drugs, ironchelators, and estrogens improved both structural outcomes and neurobehavioral scores in >1 study. Meta-regression revealed that together, structural outcome and the intervention used accounted for 65% of the observedheterogeneity in neurobehavioral score (p < 0.001, adjusted r2 ¼ 0.65).Interpretation: Further animal studies of the interventions that we found to improve both functional and structuraloutcomes in animals, using better experimental designs, could target efforts to translate effective treatments for ICHin animals into randomized controlled trials in humans.
ANN NEUROL 2011;69:389–399
The global burden of acute spontaneous (nontrau-
matic) intracerebral hemorrhage (ICH) and its out-
come appear unchanged over the past quarter century,1,2
despite the improvements in outcome that can be
achieved by organized stroke unit care and neurosurgical
hematoma evacuation.3–6 The quest for other effective
therapies has been fuelled by the recent failures of
recombinant activated factor VII and the neuroprotectant
drug NXY-059 to improve outcome after acute ICH in
humans.7,8 Randomized controlled trials of medical
therapies such as blood pressure lowering are ongoing,9
but the search for other candidate interventions may best
start with methodologically robust laboratory research in
animal models that accurately mimic human ICH.10
Therefore, we aimed to undertake a systematic review
of nonsurgical interventions in controlled studies of animal
models of ICH reporting neurobehavioral outcomes, to
explore their methodological quality, and to perform a
meta-analysis of the effects of each class of intervention.
Subjects and Methods
Eligibility CriteriaWe sought controlled studies, regardless of their language of
publication, of nonsurgical interventions given to wild-type
(nontransgenic) animals after the induction of ICH using auto-
logous blood or collagenase injection11 that reported neuro-
behavioral outcome.
Information SourcesIn July 2009, we searched Ovid Medline (from 1950), Ovid
Embase (from 1980), and ISI Web of Knowledge (from 1969)
using comprehensive electronic search strategies (Supporting
View this article online at wileyonlinelibrary.com. DOI: 10.1002/ana.22243
Received Jun 22, 2010, and in revised form Aug 2, 0000. Accepted for publication Aug 27, 2010.
Address correspondence to Dr Salman, Bramwell Dott Building, Division of Clinical Neurosciences, Western General Hospital, Crewe Road, Edinburgh
EH4 2XU, United Kingdom. E-mail: [email protected]
From the Division of Clinical Neurosciences, Centre for Clinical Brain Sciences, University of Edinburgh, Edinburgh, United Kingdom.
Additional supporting information can be found in the online version of this article.
VC 2011 American Neurological Association 389

Information Table 1). We also searched the proceedings of the
Society for Neuroscience and the first and second International
Symposia on Cerebral Hemorrhage using the ISI Web of Knowl-
edge Conference Proceedings Citation Index. We screened the
bibliographies of eligible studies for other eligible studies. We
contacted authors to clarify study eligibility, where necessary.
Study SelectionOne investigator (J.F.) screened all titles and available abstracts
for eligibility, and removed duplicates. Studies that appeared to
be eligible were read in full by 2 investigators (J.F., and E.S.S. or
R.A.-S.S.), and disagreements were resolved by either discussion
or arbitration by a third investigator (M.R.M.). We obtained
translations of studies that were not written in English.
Data CollectionTwo investigators independently extracted data on experimental
design, study quality attributes, intervention characteristics, func-
tional outcome (neurobehavioral score, measured on any scale),
and structural outcomes (brain water content, or hematoma size).
We recorded these data in the Collaborative Approach to Meta-
Analysis and Review of Animal Data from Experimental Stroke
(CAMARADES) Microsoft Access 2003 data manager applica-
tion. For every treatment comparison (a given dose of an inter-
vention at a given time of administration after ICH), we
extracted the number of animals in each treatment group, the
mean outcome score, and the standard deviation or standard error
of the mean. We extracted all neurobehavioral outcomes at the
latest time of assessment, as well as at 7 6 2 days after the induc-
tion of ICH (if reported) and structural outcome data at the lat-
est time when animals were culled. We extracted outcome data
on untreated sham groups (in which ICH had not been induced)
from experiments where these were included; in experiments that
did not, we inferred sham neurobehavioral scores for functionally
unimpaired animals, sham hematoma volumes of zero, and sham
brain water content values corresponding to the contralateral
brain region of the control/vehicle group. Unless outcomes were
quantified at the relevant time points, we measured them from
publications’ figures (using Adobe measuring tools). We contacted
authors to obtain unpublished or missing data.
Quality AssessmentWe assessed each study’s quality according to the CAMARADES
10-item checklist,12 which consists of reporting of a sample size
calculation; use of animals with comorbidities (eg, hypertension or
diabetes); control of animals’ temperature; use of anesthetics other
than ketamine (because of its marked intrinsic neuroprotectant ac-
tivity13); randomized treatment allocation; treatment allocation
concealment; blinded assessment of outcome; publication in a
peer-reviewed journal; statement of compliance with regulatory
requirements; and statement of potential conflicts of interest.
Data Analysis
META-ANALYSIS. The prespecified primary outcome was
functional outcome as measured by neurobehavioral score at
the latest time point after ICH induction. Prespecified second-
ary outcomes were structural measures of brain injury: either
brain water content or hematoma volume. We quantified effect
sizes with the normalized (weighted) mean difference summary
statistic, using the summary measures of outcome provided in
the individual comparisons in studies where sufficient data were
available to allow this analysis (outcome reported for [1] animals
with ICH receiving the intervention, [2] control animals with
ICH receiving vehicle, and [3] sham animals neither undergoing
ICH nor receiving treatment). If the same group of animals was
assessed using several neurobehavioral scores or structural out-
comes in 1 study, we combined these using fixed effects meta-
analysis and used this pooled measure for further analysis. We
used the DerSimonian and Laird weighted mean difference ran-
dom effects model to aggregate the weighted summary statistic
for each individual comparison into a pooled estimate of effect
size,14 grouping interventions by their main putative mechanism
of action as attributed by the authors of individual studies.
SENSITIVITY ANALYSES. We assessed the effect of key
methodological study attributes by stratifying the pooled estimate
of effect in all studies by the use of randomization, allocation
concealment, and blinded assessment of outcome. For each class
of intervention, we assessed whether the pooled estimate of pri-
mary (neurobehavioral) outcome at the last time point of assess-
ment was modified if we restricted analyses to outcome data pro-
vided at 7 6 2 days after ICH induction. In a post hoc
sensitivity analysis, we explored whether the addition of studies
that administered interventions prior to the induction of ICH
affected the pooled estimate of effect on the primary outcome.
ASSESSMENT OF HETEROGENEITY. We used the chi-
square statistic to assess the significance of differences between
studies (with n � 1 degrees of freedom), and used the Bonfer-
roni correction to calculate significance, taking into account the
number of comparisons performed.
META-REGRESSION. We identified studies describing
functional and structural outcomes in the same group of ani-
mals. We used meta-regression to explore the relationship
between functional and structural outcome and: aspects of
study quality; the intervention tested; the time of treatment;
and the time of outcome assessment. Meta-regression extends
the random effects meta-analysis model by taking into account
1 or more study-level covariates and determines how much het-
erogeneity can be explained by taking into account both within-
and between-study variance.15 We performed meta-regression
using STATA 10 with the linear function metareg. We built the
regression model in a hierarchal manner, by running the regres-
sion analysis 1 variable (or group of dummy groups) at a time.
The variable with the most significant change in the F ratio was
the first variable to enter the model. The second variable was
then chosen by the largest change in the F ratio in the model
that already contained the first variable. This process was iter-
ated until there were no significant changes in the F ratio. The
adjusted R2 value provided indicates how much residual hetero-
geneity is accounted for by the covariates.
ANNALS of Neurology
390 Volume 69, No. 2

Results
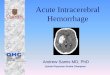
Our searches identified 98 potentially eligible studies of
the effect of nonsurgical interventions on neurobehavioral
outcome (Fig 1). We excluded 10 studies because ICH
was not induced using collagenase or autologous blood
injection,16–18 outcome data could not be extracted or
obtained,19 variance values of zero precluded meta-analy-
sis,20,21 or interventions were administered before the
induction of ICH22–25 (although we included 3 of these
studies in a post hoc sensitivity analysis24–26). After cor-
responding authors clarified the data in 2 studies,27,28 we
included 88 studies reporting 151 different treatment
comparisons (87 of which had sham groups) that
described the effects of nonsurgical interventions on neu-
robehavioral outcome in 2,616 treated or control rodents
with ICH (Supporting Information Table 1).26–113
Study CharacteristicsThe most frequently used animal model of ICH was col-
lagenase injection (53 [60%] studies; see Supporting Infor-
mation Table 1), and ICH was induced in the striatum in
all but 1 study (99%).51 The median number of treated or
control animals used in each study was 14 (interquartile
range, 12–21; full range, 6–100). Only 2 studies
reported deaths prior to the planned time of culling: 7 of
63 animals died during ICH induction in 1 study, and 5
of 18 died during another (representing a case fatality
rate of 15%).86,94 Sixty-four different interventions were
given at a median interval after ICH induction of 2
hours (interquartile range, 20 minutes to 6 hours). The
included studies reported outcome using 38 different
neurobehavioral scales (see Supporting Information Table
1), most often the forelimb placing test (10%), neurolog-
ical severity score (10%),114 corner turn test (9%), and
modified limb-placing test (9%). Brain water content
was the most frequently reported structural outcome (38
[43%] studies, most of which [89%] used wet and dry
brain weights to quantify it), and hematoma volume was
reported in 30 (34%) studies (and was measured by sev-
eral techniques including a variety of histological meth-
ods, spectrophotometry, or magnetic resonance imaging).
Risk of Bias of Included StudiesThe median study quality score was 4/10 (interquartile
range, 3–5). Of 88 publications, 27 (31%) reported ran-
dom allocation to group, 7 (8%) reported allocation con-
cealment, and 43 (49%) reported the blinded assessment
of outcome. No study reported a sample size calculation,
only 1 study reported the use of animals with comorbid-
ities, and 28 (32%) used ketamine, which is an anes-
thetic agent with intrinsic neuroprotective properties.13
For neurobehavioral score, studies that did not report
random allocation to group were associated with larger
effect sizes (32%; 95% confidence interval [CI], 26–39;
n ¼ 107) compared to those that did (21%; 95% CI,
13–29; n ¼ 42; chi-square ¼ 437; df ¼ 1; p < 0.0001).
FIGURE 1: Summary of study selection.
Frantzias et al: ICH Animal Models
February 2011 391

Similarly, studies that did not report allocation conceal-
ment were associated with larger estimates of effect
(31%; 95% CI, 26–37; n ¼ 132) compared to studies
that did (20%; 95% CI, 6–33; n ¼ 17; chi-square ¼ 33,
df ¼ 1, p < 0.0001). The reporting of blinded assess-
ment of outcome accounts for a significant proportion of
between-study heterogeneity (chi-square ¼ 43, df ¼ 1,
p < 0.001), but there was no difference in effect sizes
between studies that did blind outcome assessment and
those that did not (29%; 95% CI, 22–36 vs 30%; 95%
CI, 21–38).
Neurobehavioral OutcomesStem cells, calcium channel blockers, anti-inflammatory
drugs, iron chelators, growth factors, thrombin inhibi-
tors, and peroxisome proliferator-activated receptor
gamma agonists improved neurobehavioral scores at the
last time point of assessment, although there was signifi-
cant between-study heterogeneity in several of these
classes of intervention (Fig 2). In a sensitivity analysis re-
stricted to studies reporting neurobehavioral outcome at
7 6 2 days after interventions delivered within 24 hours
of ICH (using 44% of the data used to evaluate the pri-
mary outcome), the improvement of neurobehavioral
outcome became statistically significant for some inter-
ventions (anti-oxidants, glutamate receptor antagonists,
heme oxygenase inhibitors, and minocycline) and insig-
nificant for others (calcium channel blockers, thrombin
inhibitors, and tumor necrosis factor (TNF)-a inhibitor
antisense oligonucleotide). In a post hoc sensitivity analy-
sis of the primary outcome in studies of interventions al-
ready included in the meta-analysis, also including stud-
ies that treated animals prior to ICH induction had no
significant impact on the pooled estimate for the 3 inter-
vention groups (antioxidants, estrogens, and TNF-a in-
hibitor antisense oligonucleotides) reporting both pre-
and post-ICH delivery of intervention (see Fig 2).24–26
We did not further analyze data from 2 studies that
treated animals prior to the induction ICH with agents
that had not also been administered after ICH
induction.22,23
Structural OutcomesIn the studies that reported brain water content in addi-
tion to neurobehavioral scores (Fig 3), the pooled reduc-
tion of brain water content was 34% (95% CI, 25–43)
in 78 comparisons involving 867 animals, with substan-
tial heterogeneity between studies (chi-square ¼ 956, p <
0.0001). Among 19 classes of intervention, 12 (63%)
significantly reduced brain water content (see Fig 3), and
8 of these also significantly improved neurobehavioral
scores (see Fig 2): stem cells, calcium channel blockers,
anti-inflammatory drugs, iron chelators, estrogens, micro-
glial inhibitors, propofol, and an angiotensin II receptor
blocker. Of these 8 interventions, the angiotensin II re-
ceptor blocker (81%; 95% CI, 68–94) and anti-inflam-
matory drugs (19%; 95% CI, 0.5–38) also reduced he-
matoma volume. There was neither an improvement in
neurobehavioral outcome nor a reduction in brain water
content for antioxidant drugs, glutamate receptor antago-
nists, hypothermia, and gap junction inhibitors. The
effects of the remaining 11 interventions on functional
and structural outcomes were discordant.
Meta-Regression of Structural andNeurobehavioral OutcomesFifty-three comparisons reported both a functional and a
structural outcome in the same group of animals. Struc-
tural outcome explained 38% of the observed heteroge-
neity in functional outcome (s2 ¼ 816, adjusted r2 ¼0.38, Fig 4). In a multivariate model, structural outcome
and the intervention used accounted for 65% of the
observed heterogeneity in neurobehavioral score (F15, 37
¼ 5.31, p < 0.001, df ¼ 52, s2 ¼ 286, adjusted r2 ¼0.65). Relative to structural benefit, additional functional
benefit was observed when animals were treated with
anti-inflammatory drugs (30%; 95% CI, 8–51), antia-
poptotic drugs (38%; 95% CI, 11–65), and albumin
(67%; 95% CI, 22–112) compared to antioxidants as
the reference group (chosen because this group contained
the largest quantity of data). Gap junction inhibitors
reduced functional benefit (�30%; 95% CI, �54 to
�7). These findings were not affected by whether the
structural outcome reported was hematoma volume or
brain water content. Study quality had no effect on the
relationship between structural and functional outcome.
Discussion
In a systematic review and meta-analysis of 88 controlled
studies describing the effects of 64 different nonsurgical
interventions on 38 different neurobehavioral scales in
2,616 rodents, interventions that improved both neuro-
behavioral score and structural outcome(s) in 2 or more
animal studies (albeit with some between-study heteroge-
neity) included stem cells, calcium channel blockers,
anti-inflammatory drugs, estrogens, and iron chelators.
We benefited from comprehensive search strategies
without language bias, prespecified outcomes and analytic
approaches, sensitivity analyses, and correction of statisti-
cal tests for multiple comparisons. Other reviews have
not meta-analyzed existing data.11,115 Nevertheless, publi-
cation bias is known to result in an overestimation of
effect sizes in animal models,116 and may have affected
ANNALS of Neurology
392 Volume 69, No. 2

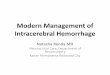
FIGURE 2: Weighted mean difference meta-analysis of the effects of nonsurgical interventions on neurobehavioral outcome incontrolled animal studies. Diamonds represent grouped estimates of effect (and their associated 95% confidence intervals) foreither classes of intervention or several studies of the same intervention. Effect estimates are organized by classes ofintervention followed by individual interventions, in descending order of sample size. Heterogeneity between studies withineach class of intervention is indicated in parentheses. Squares represent point estimates of effect, and horizontal lines aretheir 95% confidence intervals. Details of interventions and experimental design in the individual studies are provided inSupplementary Table 1. ATSC 5 adipose tissue-derived stromal cells; BMSC 5 bone marrow stem cells; NSC 5 nonspecificsuppressor cells; VEGF 5 vascular endothelial growth factor; MSC 5 mesenchymal stem cells; UCBC 5 umbilical cord bloodculture; GCSF 5 granulocyte colony-stimulating factor; GABA 5 gamma-aminobutyric acid; TNF 5 tumor necrosis factor.

our findings. Although the use of weighted mean differ-
ence meta-analysis allows the combination and compari-
son of outcomes across a large number of neurobehavio-
ral scales, these scales measure different functions, and
the findings presented here represent a summary of
available data.
FIGURE 3: Weighted mean difference meta-analysis of the effects of nonsurgical interventions on brain water content incontrolled animal studies. Diamonds represent grouped estimates of effect (and their associated 95% confidence intervals) foreither classes of intervention or several studies of the same intervention. Effect estimates are organized in the same order asFigure 2. Heterogeneity between studies within each class of intervention is indicated in parentheses. Squares represent pointestimates of effect, and horizontal lines are their 95% confidence intervals. Details of interventions and experimental design inthe individual studies are provided in Supplementary Table 1.
FIGURE 4: Meta-regression of functional (neurobehavioral score) and structural (brain water content or hematoma size)outcomes that were measured in the same groups of animals. The size of each point reflects the precision of each comparison.
ANNALS of Neurology
394 Volume 69, No. 2

Methodological problems known to affect animal
studies were evident in the studies included in our analy-
ses.117 Their methodological quality was generally poor
(median score, 4/10), but variation among studies
enabled us to confirm the potent influences of random-
ization and allocation concealment on effect sizes. No
study reported a sample size calculation, the use of keta-
mine anesthesia was frequent despite its known intrinsic
neuroprotective properties,13 and every study bar 1 used
only healthy animals, which is known to bias animal stud-
ies of stroke.118 Furthermore, young animals without
comorbidities are unrepresentative of humans who suffer
ICH,9 and the predominantly striatal location of ICH
induction in the included studies did not fully represent
ICH in humans, which occurs in lobar regions and the
posterior fossa, may extend into other brain compartments,
and often causes hydrocephalus. Studies used a diverse array
of neurobehavioral scales, and several used only 1 scale
when a battery of tests might have given a more complete
description of neurobehavioral outcome.119 Many of the
scales have not been validated and rely on primarily motor
tasks. Moreover, the neurobehavioral scale used should
relate to whether an ICH is cortical or striatal, because the
neurological impairments arising from ICH vary by the an-
atomical location of the ICH.119 Furthermore, because
rodents have proportionately less white matter than
humans,11 and may have greater neuroplasticity,115 there
may be problems with the relevance of the animal models
to human ICH. There are differences between the 2 main
rodent models of ICH,120 but we found no evidence that
1 was any more relevant to the human condition than the
other. There was a general shortage of external validation of
interventions that appeared to improve outcome.
We have used meta-analysis to derive summary esti-
mates of efficacy from a collection of relatively small
studies, many of which were not sufficiently powered to
detect modest treatment effects. Where possible, we have
used weighted rather than standardized mean differences,
because this is a more powerful statistical approach when
the size of contributing studies is small.121 The use of
meta-analysis to aggregate data for neurobehavioral out-
comes described using ordinal scales is well established
(and indeed many of the contributing studies use para-
metric statistics to analyze these data), and is justified
because parametric analyses of nonparametric data
becomes more valid when large numbers of studies are
aggregated in this way.122
Importantly, only 40% of the variation in treatment
effect on neurobehavioral outcome was attributable to
the observed effect on structural outcome, increasing to
65% when drug-specific effects were also taken into
account. Although this provides some basis for the use of
structural outcomes in clinical trial programs, it does sug-
gest first that such structural outcomes capture only a
proportion of efficacy, and second that the relationship
between structural and functional outcome—and there-
fore the utility of such structural outcome measures—
may vary substantially between different drug classes.
Discordance has previously been reported between
animal and human studies in other diseases,123 and we
have shown that this is also the case for ICH. Of the
interventions that improved both structural outcomes
and neurobehavioral scores in animal models (see Figs 2
and 3), anti-inflammatory drugs have not improved out-
come in humans.124 Similarly, recombinant activated fac-
tor VII did not improve outcome in humans, and indeed
the first evidence of benefit on structural outcomes in
animals was reported after the start of human trials.7,125
For progress to be made in translational ICH
research, the quality of animal studies must improve.126
We have reasonable understanding of some of the patho-
physiological processes underlying ICH in animals,3,127
but future research might usefully focus on understand-
ing to what extent these mechanisms are important in
humans, allowing drug development to be targeted at the
key processes. Furthermore, we need animal models of
ICH that better mimic important pathophysiologic proc-
esses in humans, including hematoma expansion and re-
currence,3,10,115 and we need these experiments to be
conducted in such a way as to minimize the risk of study
quality bias. Only then may the translational paradigm
be reliable enough for effective treatments in animal
models to be tested in randomized controlled trials in
humans.
Acknowledgment
R.A.-S.S. was funded by a clinician scientist fellowship
from the UK Medical Research Council. M.R.M.
acknowledges the support of the MRC Trials Methodol-
ogy Hub.
We thank E. Lebedeva, A. Wong, and Dr C. Four-
naris for their generous assistance with translating studies
for this review.
Potential Conflicts of Interest
Nothing to report.
References1. van Asch CJ, Luitse MJ, Rinkel GJ, et al. Incidence, case fatality,
and functional outcome of intracerebral haemorrhage over time,according to age, sex, and ethnic origin: a systematic review andmeta-analysis. Lancet Neurol 2010;9:167–176.
Frantzias et al: ICH Animal Models
February 2011 395

2. Feigin VL, Lawes CM, Bennett DA, et al. Worldwide stroke inci-dence and early case fatality reported in 56 population-basedstudies: a systematic review. Lancet Neurol 2009;8:355–369.
3. Qureshi AI, Mendelow AD, Hanley DF. Intracerebral haemor-rhage. Lancet 2009;373:1632–1644.
4. Stroke Unit Trialists’ Collaboration. Organised inpatient (strokeunit) care for stroke. Cochrane Database Syst Rev 2007;(4):CD000197.
5. Candelise L, Gattinoni M, Bersano A, et al. Stroke-unit care foracute stroke patients: an observational follow-up study. Lancet2007;369:299–305.
6. Terent A, Asplund K, Farahmand B, et al. Stroke unit care revis-ited: who benefits the most? A cohort study of 105,043 patientsin Riks-Stroke, the Swedish Stroke Register. J Neurol NeurosurgPsychiatry 2009;80:881–887.
7. Al-Shahi Salman R. Haemostatic drug therapies for acute sponta-neous intracerebral haemorrhage. Cochrane Database Syst Rev2009;(4):CD005951.
8. Lyden PD, Shuaib A, Lees KR, et al. Safety and tolerability ofNXY-059 for acute intracerebral hemorrhage: the CHANT Trial.Stroke 2007;38:2262–2269.
9. Al-Shahi Salman R, Labovitz DL, Stapf C. Spontaneous intracere-bral haemorrhage. BMJ 2009;339:b2586.
10. NINDS ICH Workshop Participants. Priorities for clinical researchin intracerebral hemorrhage: report from a National Institute ofNeurological Disorders and Stroke workshop. Stroke 2005;36:e23–e41.
11. James ML, Warner DS, Laskowitz DT. Preclinical models of intra-cerebral hemorrhage: a translational perspective. Neurocrit Care2008;9:139–152.
12. Macleod MR, O’Collins T, Howells DW, et al. Pooling of animalexperimental data reveals influence of study design and publica-tion bias. Stroke 2004;35:1203–1208.
13. Takeshita H, Okuda Y, Sari A. The effects of ketamine on cere-bral circulation and metabolism in man. Anesthesiology 1972;36:69–75.
14. Dersimonian R, Laird N. Meta-analysis in clinical trials. ControlClin Trials 1986;7:177–188.
15. Egger M, Smith G, Altman D. Systematic reviews in health care.Meta-analysis in context. 2nd ed. London, UK: BMJ, 2001.
16. Liu DZ, Cheng XY, Ander BP, et al. Src kinase inhibitiondecreases thrombin-induced injury and cell cycle re-entry in stria-tal neurons. Neurobiol Dis 2008;30:201–211.
17. Gong Y, Xi GH, Keep RF, et al. Complement inhibition attenu-ates brain edema and neurological deficits induced by thrombin.Acta Neurochir Suppl 2005;95:389–392.
18. Zheng A, Ye Q-Y, Huang H-P, et al. Randomized and controlledstudy of Naoxieling in improving dyskinesia of rats with acutecerebral hemorrhage [in Chinese]. Chin J Clin Rehabil 2003;7:3426–3427.
19. Lyden PD, Jackson-Friedman C, Lonzo-Doktor L. Medical therapyfor intracerebral hematoma with the gamma-aminobutyric acid-Aagonist muscimol. Stroke 1997;28:387–391.
20. Wu W-B, Hu C-L, Guo F-Q, et al. Effect of hirudo extract on his-topathological changes and behaviors in experimental intracere-bral hematoma absorption [in Chinese]. Chin J Clin Rehabil2004;8:121–123.
21. Tan Y, Liang Q-H, Li X-L, et al. Effect of Pinggan Xifeng Tang onmembrane potential of hippocampal mitochondria and neurolog-ical function following intracerebral hemorrhage in rats. Chin JClin Rehabil 2004;8:1396–1398.
22. Ardizzone TD, Zhan X, Ander BP, et al. SRC kinase inhibitionimproves acute outcomes after experimental intracerebral hem-orrhage. Stroke 2007;38:1621–1625.
23. Sinn DI, Chu K, Lee ST, et al. Pharmacological induction of heatshock protein exerts neuroprotective effects in experimental in-tracerebral hemorrhage. Brain Res 2007;1135:167–176.
24. Auriat A, Plahta WC, McGie SC, et al. 17beta-Estradiol pretreat-ment reduces bleeding and brain injury after intracerebral hem-orrhagic stroke in male rats. J Cereb Blood Flow Metab 2005;25:247–256.
25. Peeling J, Yan HJ, Chen SG, et al. Protective effects of free radi-cal inhibitors in intracerebral hemorrhage in rat. Brain Res 1998;795:63–70.
26. Mayne M, Ni W, Yan HJ, et al. Antisense oligodeoxynucleotideinhibition of tumor necrosis factor-alpha expression is neuropro-tective after intracerebral hemorrhage. Stroke 2001;32:240–248.
27. Hartman RE, Rojas HA, Lekic T, et al. Long-term effects of mela-tonin after intracerebral hemorrhage in rats. Acta NeurochirSuppl 2008;105:99–100.
28. Wu J, Yang S, Xi G, et al. Minocycline reduces intracerebral hem-orrhage-induced brain injury. Neurol Res 2009;31:183–188.
29. Ma J, Dong Z, Li Q-G, et al. Protective effect of propofol againstintracerebral hemorrhage injury in rats [in Chinese]. Yaoxue Xue-bao 2009;44:344–349.
30. Jung KH, Chu K, Lee ST, et al. Blockade of AT1 receptor reducesapoptosis, inflammation, and oxidative stress in normotensiverats with intracerebral hemorrhage. J Pharmacol Exp Ther 2007;322:1051–1058.
31. Rodrigues CM, Sola S, Nan Z, et al. Tauroursodeoxycholic acidreduces apoptosis and protects against neurological injury afteracute hemorrhagic stroke in rats. Proc Natl Acad Sci U S A 2003;100:6087–6092.
32. Power C, Henry S, Del Bigio MR, et al. Intracerebral hemorrhageinduces macrophage activation and matrix metalloproteinases.Ann Neurol 2003;53:731–742.
33. Szymanska A, Biernaskie J, Laidley D, et al. Minocycline and in-tracerebral hemorrhage: influence of injury severity and delay totreatment. Exp Neurol 2006;197:189–196.
34. Sinn D-I, Kim S-J, Chu K, et al. Valproic acid-mediated neuropro-tection in intracerebral hemorrhage via histone deacetylase inhibi-tion and transcriptional activation. Neurobiol Dis 2007;26:464–472.
35. Sinn DI, Lee ST, Chu K, et al. Combined neuroprotective effectsof celecoxib and memantine in experimental intracerebral hem-orrhage. Neurosci Lett 2007;411:238–242.
36. Chu K, Jeong SW, Jung KH, et al. Celecoxib induces functionalrecovery after intracerebral hemorrhage with reduction of brainedema and perihematomal cell death. J Cereb Blood FlowMetab 2004;24:926–933.
37. Lema PP, Girard C, Vachon P. Evaluation of dexamethasone forthe treatment of intracerebral hemorrhage using a collagenase-induced intracerebral hematoma model in rats. J Vet PharmacolTher 2004;27:321–328.
38. Li Z, Liang G, Xue Y, et al. Effects of combination treatment ofdexamethasone and melatonin on brain injury in intracerebralhemorrhage model in rats. Brain Res 2009;1264:98–103.
39. Del Bigio MR, Yan HJ, Campbell TM, et al. Effect of fucoidantreatment on collagenase-induced intracerebral hemorrhage inrats. Neurol Res 1999;21:415–419.
40. Lema PP, Girard C, Vachon P. High doses of methylprednisoloneare required for the treatment of collagenase-induced intracere-bral hemorrhage in rats. Can J Vet Res 2005;69:253–259.
41. Rynkowski MA, Kim GH, Garrett MC, et al. C3a receptor antago-nist attenuates brain injury after intracerebral hemorrhage.J Cereb Blood Flow Metab 2009;29:98–107.
42. Titova E, Ostrowski RP, Sowers LC, et al. Effects of apocynin andethanol on intracerebral haemorrhage-induced brain injury inrats. Clin Exp Pharmacol Physiol 2007;34:845–850.
ANNALS of Neurology
396 Volume 69, No. 2

43. Nakamura T, Kuroda Y, Yamashita S, et al. Edaravone attenuatesbrain edema and neurologic deficits in a rat model of acute in-tracerebral hemorrhage. Stroke 2008;39:463–469.
44. Rojas H, Lekic T, Chen W, et al. The antioxidant effects of mela-tonin after intracerebral hemorrhage in rats. Acta NeurochirSuppl 2008;105:19–21.
45. Tsuchiyama R, Sozen T, Manaenko A, et al. The effects of nico-tinamide adenine dinucleotide on intracerebral hemorrhage-induced brain injury in mice. Neurol Res 2009;31:179–182.
46. Peeling J, Del Bigio MR, Corbett D, et al. Efficacy of disodium4-[(tert-butylimino)methyl]benzene-1,3-disulfonate N-oxide (NXY-059), a free radical trapping agent, in a rat model of hemor-rhagic stroke. Neuropharmacology 2001;40:433–439.
47. Titova E, Ostrowski RP, Rowe J, et al. Effects of superoxide dis-mutase and catalase derivates on intracerebral hemorrhage-induced brain injury in rats. Acta Neurochir Suppl 2008;105:33–35.
48. Yamamoto M, Sakamoto N, Iwai A. Pharmacological action ofYM737, a new glutathione analogue, in rats with experimentalhematoma. Arch Int Pharmacodyn Ther 1990;308:178–184.
49. Galaeva IP, Garibova TL, Voronina TA, et al. Neuroprotectiveeffects of afobazol in experimental cerebral hemorrhage. BullExp Biol Med 2005;140:535–537.
50. James ML, Sullivan PM, Lascola CD, et al. Pharmacogenomiceffects of apolipoprotein e on intracerebral hemorrhage. Stroke2009;40:632–639.
51. Kleiser B, Van RJ, Van DB, et al. Favourable effect of flunarizineon the recovery from hemiparesis in rats with intracerebral hema-tomas. Neurosci Lett 1989;103:225–228.
52. Suzuki M, Hayashi A, Sasamata M. Nicardipine, a calcium antag-onist, does not aggravate intracerebral haemorrhage in an intra-cerebral haemorrhage model in rats. J Pharm Pharmacol 2005;57:483–488.
53. Ma B, Zhang J. Nimodipine treatment to assess a modifiedmouse model of intracerebral hemorrhage. Brain Res 2006;1078:182–189.
54. Chang S-J, Yin L, Xin S-M. Effects of nimodipine on expressionsof caspase-3 in perihematomal tissues of rats [in Chinese]. Chin JClin Rehabil 2006;12:110–112.
55. Kleiser B, Gortler M, Horn E, et al. Time window for the treat-ment of cerebral hematomas with R 56865 in rats. Neurol Psychi-atry Brain Res 1997;5:27–30.
56. Lyden P, Shin C, Jackson-Friedman C, et al. Effect of ganaxolonein a rodent model of cerebral hematoma. Stroke 2000;31:169–175.
57. Manaenko A, Lekic T, Sozen T, et al. Effect of gap junction inhi-bition on intracerebral hemorrhage-induced brain injury in mice.Neurol Res 2009;31:173–178.
58. Titova E, Ostrowski RP, Zhang JH, et al. Effect of amantadine sul-phate on intracerebral hemorrhage-induced brain injury in rats.Acta Neurochir Suppl 2008;105:119–121.
59. Kleiser B, Diepers M, Geiger S, et al. Combined therapy with flu-narizine and memantine of experimental intracerebral hemato-mas in rats. Neurol Psychiatry Brain Res 1995;3:219–224.
60. Lee S-T, Chu K, Jung K-H, et al. Memantine reduces hematomaexpansion in experimental intracerebral hemorrhage, resulting infunctional improvement. J Cereb Blood Flow Metab 2006;26:536–544.
61. Terai K, Suzuki M, Sasamata M, et al. Effect of AMPA receptorantagonist YM872 on cerebral hematoma size and neurologicalrecovery in the intracerebral hemorrhage rat model. Eur J Phar-macol 2003;467:95–101.
62. Lee ST, Chu K, Sinn DI, et al. Erythropoietin reduces perihemato-mal inflammation and cell death with eNOS and STAT3 activa-
tions in experimental intracerebral hemorrhage. J Neurochem2006;96:1728–1739.
63. Park HK, Chu K, Lee ST, et al. Granulocyte colony-stimulatingfactor induces sensorimotor recovery in intracerebral hemor-rhage. Brain Res 2005;104:125–131.
64. Zhang L, Shu X-J, Zhou H-Y, et al. Protective effect of granulo-cyte colony-stimulating factor on intracerebral hemorrhage in rat.Neurochem Res 2009;34:1317–1323.
65. Gong Y, Tian H, Xi G, et al. Systemic zinc protoporphyrin admin-istration reduces intracerebral hemorrhage-induced brain injury.Acta Neurochir Suppl 2006;96:232–236.
66. Seyfried D, Han Y, Lu D, et al. Improvement in neurological out-come after administration of atorvastatin following experimentalintracerebral hemorrhage in rats. J Neurosurg 2004;101:104–107.
67. Jung KH, Chu K, Jeong SW, et al. HMG-CoA reductase inhibitor,atorvastatin, promotes sensorimotor recovery, suppressing acuteinflammatory reaction after experimental intracerebral hemor-rhage. Stroke 2004;35:1744–1749.
68. MacLellan CL, Davies LM, Fingas MS, et al. The influence ofhypothermia on outcome after intracerebral hemorrhage in rats.Stroke 2006;37:1266–1270.
69. Fingas M, Clark DL, Colbourne F. The effects of selective brainhypothermia on intracerebral hemorrhage in rats. Exp Neurol2007;208:277–284.
70. Kawanishi M, Kawai N, Nakamura T, et al. Effect of delayed mildbrain hypothermia on edema formation after intracerebral hem-orrhage in rats. J Stroke Cerebrovasc Dis 2008;17:187–195.
71. MacLellan C, Shuaib A, Colbourne F. Failure of delayed and pro-longed hypothermia to favorably affect hemorrhagic stroke inrats. Brain Res 2002;958:192–200.
72. MacLellan CL, Girgis J, Colbourne F. Delayed onset of pro-longed hypothermia improves outcome after intracerebral hem-orrhage in rats. J Cereb Blood Flow Metab 2004;24:432–440.
73. MacLellan CL, Grams J, Adams K, et al. Combined use of a cyto-protectant and rehabilitation therapy after severe intracerebralhemorrhage in rats. Brain Res 2005;1063:40–47.
74. Peeling J, Yan HJ, Corbett D, et al. Effect of FK-506 on inflam-mation and behavioral outcome following intracerebral hemor-rhage in rat. Exp Neurol 2001;167:341–347.
75. Masuda T, Hida H, Kanda Y, et al. Oral administration of metalchelator ameliorates motor dysfunction after a small hemorrhagenear the internal capsule in rat. J Neurosci Res 2007;85:213–222.
76. Okauchi M, Hua Y, Keep RF, et al. Effects of deferoxamine on in-tracerebral hemorrhage-induced brain injury in aged rats. Stroke2009;40:1858–1863.
77. Hua Y, Nakamura T, Keep RF, et al. Long-term effects of experi-mental intracerebral hemorrhage: the role of iron. J Neurosurg2006;104:305–312.
78. Nakamura T, Keep RF, Hua Y, et al. Deferoxamine-induced attenu-ation of brain edema and neurological deficits in a rat model of in-tracerebral hemorrhage. Neurosurg Focus 2003;15:ECP4.
79. Wan S, Zhan R, Zheng S, et al. Activation of c-Jun-N-terminal ki-nase in a rat model of intracerebral hemorrhage: the role of iron.Neurosci Res 2009;63:100–105.
80. Wan S, Hua Y, Keep RF, et al. Deferoxamine reduces CSF freeiron levels following intracerebral hemorrhage. Acta NeurochirSuppl 2006;96:199–202.
81. Strbian D, Tatlisumak T, Ramadan UA, et al. Mast cell blockingreduces brain edema and hematoma volume and improves out-come after experimental intracerebral hemorrhage. J CerebBlood Flow Metab 2007;27:795–802.
82. Wang J, Tsirka SE. Neuroprotection by inhibition of matrix metal-loproteinases in a mouse model of intracerebral haemorrhage.Brain 2005;128:1622–1633.
Frantzias et al: ICH Animal Models
February 2011 397

83. Wang J, Tsirka SE. Tuftsin fragment 1-3 is beneficial when deliv-ered after the induction of intracerebral hemorrhage. Stroke2005;36:613–618.
84. Kositsyn NS, Svinov MM, Goloborod’ko EV, et al. Efficacy of cer-ebrolysin in cerebral hemorrhage model in rats [in Russian]. EkspKlin Farmakol 2006;69:27–30.
85. Zhao X, Sun G, Zhang J, et al. Transcription factor Nrf2 protectsthe brain from damage produced by intracerebral hemorrhage.Stroke 2007;38:3280–3286.
86. Nguyen AP, Arvanitidis AP, Colbourne F. Failure of estradiol toimprove spontaneous or rehabilitation-facilitated recovery afterhemorrhagic stroke in rats. Brain Res 2008;1193:109–119.
87. Nakamura T, Xi G, Keep RF, et al. Effects of endogenous and ex-ogenous estrogen on intracerebral hemorrhage-induced braindamage in rats. Acta Neurochir Suppl 2006;96:221.
88. Belayev L, Obenaus A, Zhao W, et al. Experimental intracerebralhematoma in the rat: characterization by sequential magneticresonance imaging, behavior, and histopathology. Effect of albu-min therapy. Brain Res 2007;1157:146–155.
89. Zhao X, Zhang Y, Strong R, et al. 15d-Prostaglandin J2 activatesperoxisome proliferator-activated receptor-gamma, promotesexpression of catalase, and reduces inflammation, behavioraldysfunction, and neuronal loss after intracerebral hemorrhage inrats. J Cereb Blood Flow Metab 2006;26:811–820.
90. Zhao X, Sun G, Zhang J, et al. Hematoma resolution as a targetfor intracerebral hemorrhage treatment: role for peroxisome pro-liferator-activated receptor gamma in microglia/macrophages.Ann Neurol 2007;61:352–362.
91. Makarenko AN, Kositsin NS, Nazimov IV, et al. A comparativestudy of antistroke activity of the new drug ‘‘cerebral’’ and itsfractions in rats [in Russian]. Eksp Klin Farmakol 2005;28:15–20.
92. Clark W, Gunion-Rinker L, Lessov N, et al. Citicoline treatmentfor experimental intracerebral hemorrhage in mice. Stroke 1998;29:2136–2140.
93. Auriat AM, Colbourne F. Influence of amphetamine on recoveryafter intracerebral hemorrhage in rats. Behav Brain Res 2008;186:222–229.
94. Altumbabic M, Del Bigio MR. Transplantation of fetal brain tissueinto the site of intracerebral hemorrhage in rats. NeuroscienceLett 1998;257:61–64.
95. Kim J-M, Lee S-T, Chu K, et al. Systemic transplantation ofhuman adipose stem cells attenuated cerebral inflammation anddegeneration in a hemorrhagic stroke model. Brain Res 2007;1183:43–50.
96. Seyfried DM, Han Y, Yang D, et al. Mannitol enhances deliveryof marrow stromal cells to the brain after experimental intracere-bral hemorrhage. Brain Res 2008;1224:12–19.
97. Seyfried D, Ding J, Han Y, et al. Effects of intravenous adminis-tration of human bone marrow stromal cells after intracerebralhemorrhage in rats. J Neurosurg 2006;104:313–318.
98. Lee HJ, Kim KS, Park IH, et al. Human neural stem cells over-expressing VEGF provide neuroprotection, angiogenesis and func-tional recovery in mouse stroke model. PLoS One 2007;2:e156.
99. Jeong SW, Chu K, Jung KH, et al. Human neural stem cell trans-plantation promotes functional recovery in rats with experimentalintracerebral hemorrhage. Stroke 2003;34:2258–2263.
100. Lee HJ, Kim KS, Kim EJ, et al. Brain transplantation of immortalizedhuman neural stem cells promotes functional recovery in mouse intra-cerebral hemorrhage stroke model. Stem Cells 2007;25:1204–1212.
101. Lee S-T, Chu K, Jung K-H, et al. Anti-inflammatory mechanism ofintravascular neural stem cell transplantation in haemorrhagicstroke. Brain 2008;131:616–629.
102. Lee HJ, Kim MK, Kim HJ, et al. Human neural stem cells geneti-cally modified to overexpress Akt1 provide neuroprotection and
functional improvement in mouse stroke model. PLoS One 2009;4:e5586.
103. Fatar M, Stroick M, Griebe M, et al. Lipoaspirate-derived adultmesenchymal stem cells improve functional outcome during in-tracerebral hemorrhage by proliferation of endogenous progeni-tor cells stem cells in intracerebral hemorrhages. Neurosci Lett2008;443:174–178.
104. Nagai A, Kim WK, Lee HJ, et al. Multilineage potential of stablehuman mesenchymal stem cell line derived from fetal marrow.PLoS One 2007;2:e1272.
105. Nan Z, Grande A, Sanberg CD, et al. Infusion of human umbilicalcord blood ameliorates neurologic deficits in rats with hemor-rhagic brain injury. Ann N Y Acad Sci 2005;1049:84–96.
106. Tang Z-P, Guo S-G, Kang H-C, et al. Proliferation of neural pro-genitor cells and evaluation of neurologic function in cerebralhemorrhagic rats after transplantation of olfactory ensheathingcells. Chin J Clin Rehabil 2005;9:236–238.
107. Qi L, Dong Z, Ma J. Neuroprotective effect of batroxobin on ex-perimental intracerebral hemorrhage in rats [in Chinese]. YaoxueXuebao 2009;44:338–343.
108. Nakamura T, Miyamoto O, Toyoshima T, et al. 3CB2, a markerof radial glia, expression after experimental intracerebral hemor-rhage: role of thrombin. Brain Res 2008;1226:156–162.
109. Hua Y, Schallert T, Keep RF, et al. Behavioral tests after intrace-rebral hemorrhage in the rat. Stroke 2002;33:2478–2484.
110. Yamamoto M, Shimizu M, Kawabata S, et al. Effects of YM-14673, a new TRH analogue, on neurological deficits in rats withexperimental cerebral hematoma. Arch Int Pharmacodyn Ther1989;299:55–64.
111. Okauchi M, Xi G, Keep RF, et al. Tissue-type transglutaminase andthe effects of cystamine on intracerebral hemorrhage-induced brainedema and neurological deficits. Brain Res 2009;1249:229–236.
112. Liu B-R, Xiao J, Ding X-S. Expressions of complement 9 and nu-clear factor-kappa B65 in perihematomal tissue following intracerebral hemorrhage in rats and the interventional effect of as-tragalus polysaccharides [in Chinese]. Chin J Cerebrovasc Dis2007;4:26–31.
113. Luo T-L, Li X-Q. Protective effect of traditional Chinese medicinenao-yi-an granule in experimental rats with hemorrhagic stroke[in Chinese]. Hunan Yi Ke Da Xue Xue Bao 2000;25:245–247.
114. Chen J, Sanberg PR, Li Y, et al. Intravenous administration ofhuman umbilical cord blood reduces behavioral deficits afterstroke in rats. Stroke 2001;32:2682–2688.
115. Andaluz N, Zuccarello M, Wagner KR. Experimental animal mod-els of intracerebral hemorrhage. Neurosurg Clin N Am 2002;13:385–393.
116. Sena ES, van der Worp HB, Bath PM, et al. Publication bias inreports of animal stroke studies leads to major overstatement ofefficacy. PLoS Biol 2010;8:e1000344.
117. van der Worp HB, Sena ES, Donnan GA, et al. Hypothermia inanimal models of acute ischaemic stroke: a systematic reviewand meta-analysis. Brain 2007;130:3063–3074.
118. Crossley NA, Sena E, Goehler J, et al. Empirical evidence of biasin the design of experimental stroke studies: a metaepidemio-logic approach. Stroke 2008;39:929–934.
119. MacLellan CL, Auriat AM, McGie SC, et al. Gauging recovery af-ter hemorrhagic stroke in rats: implications for cytoprotectionstudies. J Cereb Blood Flow Metab 2006;26:1031–1042.
120. MacLellan CL, Silasi G, Poon CC, et al. Intracerebral hemorrhagemodels in rat: comparing collagenase to blood infusion. J CerebBlood Flow Metab 2008;28:516–525.
121. Wu, X. Combining the evidence from different drug trials. Availableat: http://www.camarades.info/index_files/Page332.htm Accessedon 8 October 2010.
ANNALS of Neurology
398 Volume 69, No. 2

122. Lord FM. On the statistical treatment of football numbers. AmPsychol 1953;8:750–751.
123. Perel P, Roberts I, Sena E, et al. Comparison of treatment effectsbetween animal experiments and clinical trials: systematic review.BMJ 2007;334:197.
124. Feigin VL, Anderson N, Rinkel GJ, et al. Corticosteroids foraneurysmal subarachnoid haemorrhage and primary intracerebralhaemorrhage. Cochrane Database Syst Rev 2005;(3):CD004583.
125. Kawai N, Nakamura T, Nagao S. Early hemostatic therapy usingrecombinant factor VIIa in a collagenase-induced intracerebral hem-orrhage model in rats. Acta Neurochir Suppl 2006;96:212–217.
126. van der Worp HB, Howells DW, Sena ES, et al. Can animal mod-els of disease reliably inform human studies? PLoS Med 2010;7:e1000245.
127. Xi G, Keep RF, Hoff JT. Mechanisms of brain injury after intrace-rebral haemorrhage. Lancet Neurol 2006;5:53–63.
Frantzias et al: ICH Animal Models
February 2011 399