Embed Size (px)
Citation preview
Henry Ford Hospital Medical Journal Henry Ford Hospital Medical Journal
Volume 32 Number 3 Special Issue on Medical Computing Article 11
9-1984
Intracerebral Hemorrhage After Carotid Endarterectomy Intracerebral Hemorrhage After Carotid Endarterectomy
José Biller
Andrew C. Hayes
Fred N. Littooy
William H. Baker
Follow this and additional works at: https://scholarlycommons.henryford.com/hfhmedjournal
Part of the Life Sciences Commons, Medical Specialties Commons, and the Public Health Commons
Recommended Citation Recommended Citation Biller, José; Hayes, Andrew C.; Littooy, Fred N.; and Baker, William H. (1984) "Intracerebral Hemorrhage After Carotid Endarterectomy," Henry Ford Hospital Medical Journal : Vol. 32 : No. 3 , 197-203. Available at: https://scholarlycommons.henryford.com/hfhmedjournal/vol32/iss3/11
This Article is brought to you for free and open access by Henry Ford Health System Scholarly Commons. It has been accepted for inclusion in Henry Ford Hospital Medical Journal by an authorized editor of Henry Ford Health System Scholarly Commons.
H e n r y Ford H o s p M e d j Vo l 32, N o 3, 1984
Case Reports Intracerebral Hemorrhage After Carotid Endarterectomy
Jose Biller, MD,* Andrew C. Hayes, PA-C,** Fred N. Littooy, MD,** and William H. Baker, MD**
Intracerebral hemorrhage (ICH) is a rare complication of carotid endarterectomy (CE). In our multicenter series of 1,180 CE (Baker-Littooy), three ICH occurred, of which two were fatal. One patient was receiving anticoagulants because ofa prosthetic aortic valve; another had rupture of a known ipsilateral intracranial aneurysm. Both occurred more than six weeks post
operatively. The third patient, who was hypertensive, had a nonfatal ipsilateral thalamic hemorrhage on the third postoperative day. Though these three patients represent only 0.25% of our series, they constitute 12% of our total strokes. ICH constitutes the largest percentage of nontechnically-related strokes and non-cardiac deaths after CE.
s t r o k e af ter ca ro t i d e n d a r t e r e c t o m y is usual ly ascr ibed to o c c l u s i o n o f t h e ca ro t i d a r te ry , e m b o l i z a t i o n , i n t ima l f lap f o r m a t i o n , o r h e m o d y n a m i c fac to rs . In t racran ia l h e m o r r h a g i c c o m p l i c a t i o n s a f te r th is p r o c e d u r e are c o n s i d e r e d rare. They e m b r a c e h e m o r r h a g i c i n f a r c t i o n , in t racerebra l h e m a t o m a s w i t h o r w i t h o u t ven t r i cu la r o r s u b a r a c h n o i d p e n e t r a t i o n , a n d i n s t a n c e s o f h e m or rhag ic ce reb rosp ina l f l u i d assoc iated w i t h increased in t racran ia l p ressu re . B r u e t m a n and associates (1) rep o r t e d six h e m o r r h a g i c c o m p l i c a t i o n s a m o n g 900 (0.66%) pat ien ts surg ica l ly t rea ted f o r ca ro t i d s tenosis o r o c c l u s i o n . M o r e recen t l y S u n d t , et al (2,3) n o t e d f ive cases in a series of 1,145 (0.43%) ca ro t i d endar te rec -t o m i e s . W e n o t e d t h r e e cases in o u r series of 1,180 (0.25%) ca ro t i d e n d a r t e r e c t o m i e s and repo r t o u r exper ience in c o n j u n c t i o n w i t h a rev iew of 36 p rev ious l y p u b l i s h e d cases.
Case Reports Case 1
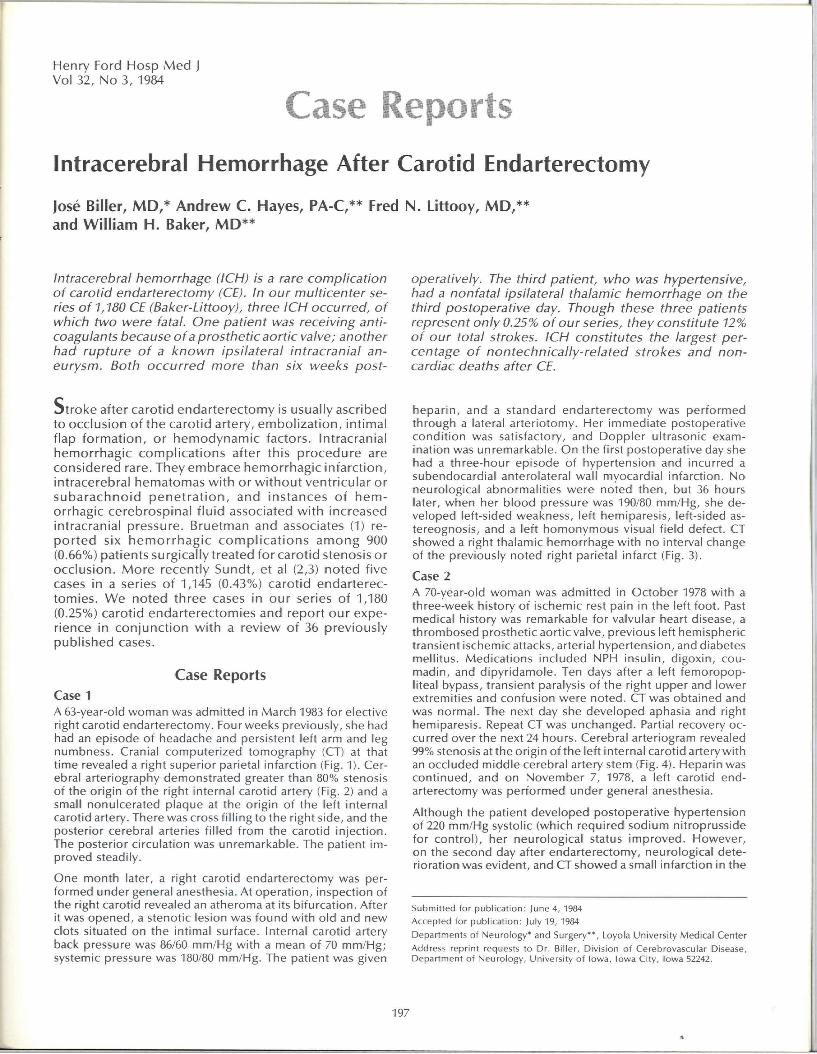
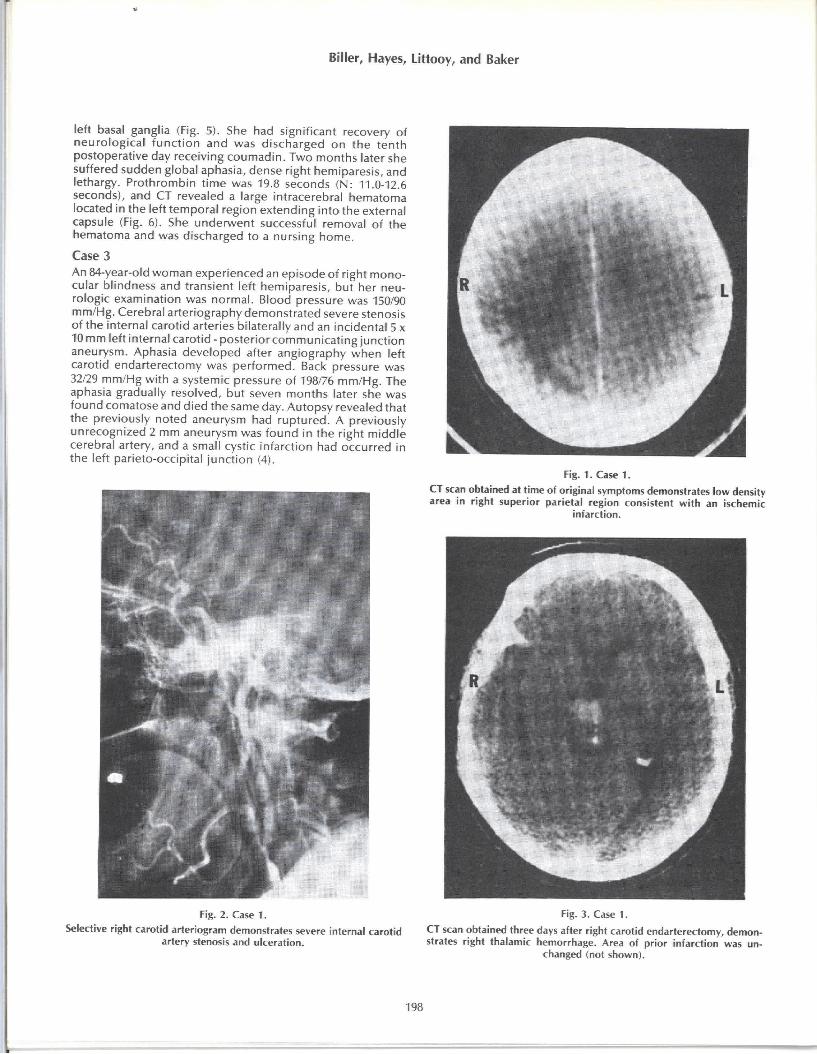
A 63-year-oId woman was admitted in March 1983 for elective right carotid endarterectomy. Four weeks previously, she had had an episode of headache and persistent left arm and leg numbness. Cranial computer ized tomography (CT) at that t ime revealed a right superior parietal infarction (Fig. 1). Cerebral arteriography demonstrated greater than 80% stenosis of the origin of the right internal carotid artery (Fig. 2) and a small nonulcerated plaque at the origin of the left internal carotid artery. There was cross f i l l ing to the right side, and the posterior cerebral arteries f i l led f rom the carotid inject ion. The posterior circulation was unremarkable. The patient improved steadily.
One month later, a right carotid endarterectomy was performed under general anesthesia. At operat ion, inspection of the right carotid revealed an atheroma at its bi furcat ion. After it was opened, a stenotic lesion was found wi th old and new clots situated on the intimal surface. Internal carotid artery back pressure was 86/60 mm/Hg wi th a mean of 70 mm/Hg; systemic pressure was 180/80 mm/Hg. The patient was given
hepar in , and a standard endarterectomy was per formed through a lateral arteriotomy. Her immediate postoperative condi t ion was satisfactory, and Doppler ultrasonic examination was unremarkable. On the first postoperative day she had a three-hour episode of hypertension and incurred a subendocardial anterolateral wall myocardial infarction. No neurological abnormalit ies were noted then, but 36 hours later, when her b lood pressure was 190/80 mm/Hg, she developed left-sided weakness, left hemiparesis, left-sided as-tereognosis, and a left homonymous visual f ield defect. CT showed a right thalamic hemorrhage wi th no interval change of the previously noted right parietal infarct (Fig. 3).
Case 2 A 70-year-old woman was admitted in October 1978 with a three-week history of ischemic rest pain in the left foot. Past medical history was remarkable for valvular heart disease, a thrombosed prosthetic aortic valve, previous left hemispheric transient ischemic attacks, arterial hypertension, and diabetes mell itus. Medications included NPH insul in, digoxin, Coumadin, and dipyr idamole. Ten days after a left femoropopliteal bypass, transient paralysis of the right upper and lower extremities and confusion were noted. CT was obtained and was normal. The next day she developed aphasia and right hemiparesis. Repeat CT was unchanged. Partial recovery occurred over the next 24 hours. Cerebral arteriogram revealed 99% stenosis at the origin o f t he left internal carotid artery wi th an occluded middle cerebral artery stem (Fig. 4). Heparin was cont inued, and on November 7, 1978, a left carotid endarterectomy was performed under general anesthesia.
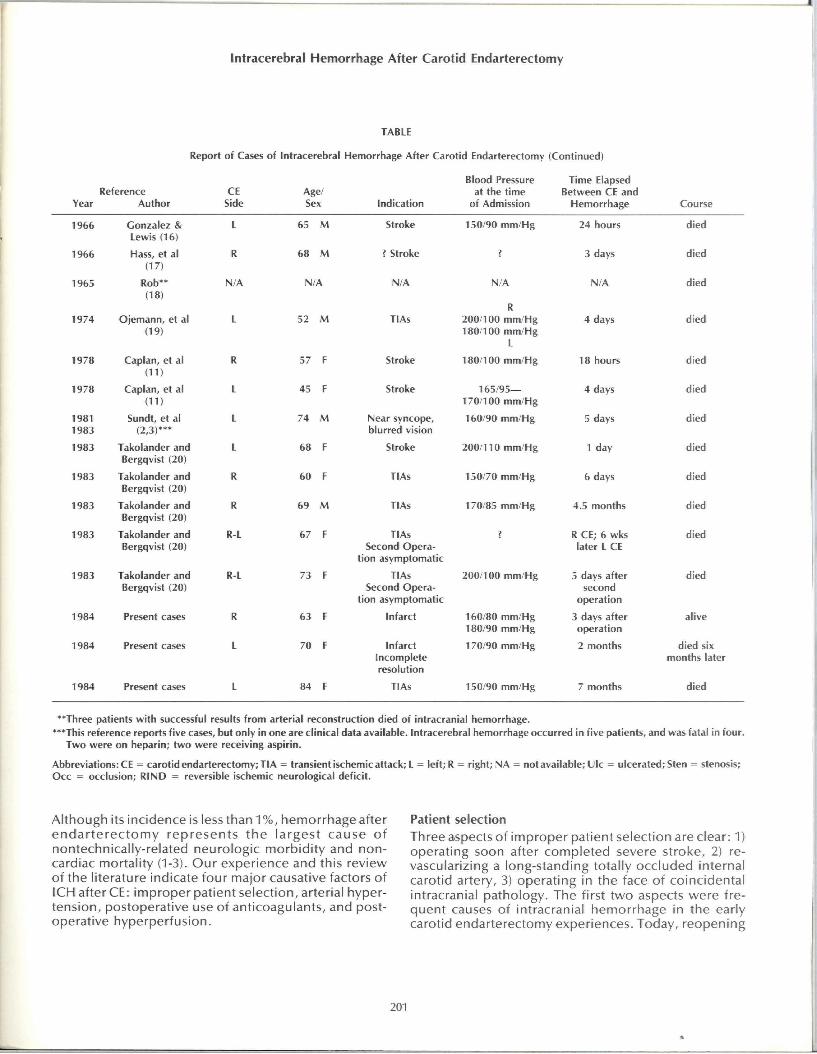
Al though the patient developed postoperative hypertension of 220 mm/Hg systolic (which required sodium nitroprusside for contro l ) , her neurological status improved. However, on the second day after endarterectomy, neurological deterioration was evident, and CT showed a small infarction in the
Submit ted for pub l i ca t ion ; j une 4, 1984
Accepted for pub l i ca t ion : ju ly 19, 1984
Departments of Neurology^ and Surgery^^, Loyola Universi ty Medica l Center
Address repr int requests to Dr, Bil ler, Div is ion of Cerebrovascular Disease, Department of Neuro logy, Universi ty of lowa, lowa City, lowa 52242,
197
Biller, Hayes, Littooy, and Baker
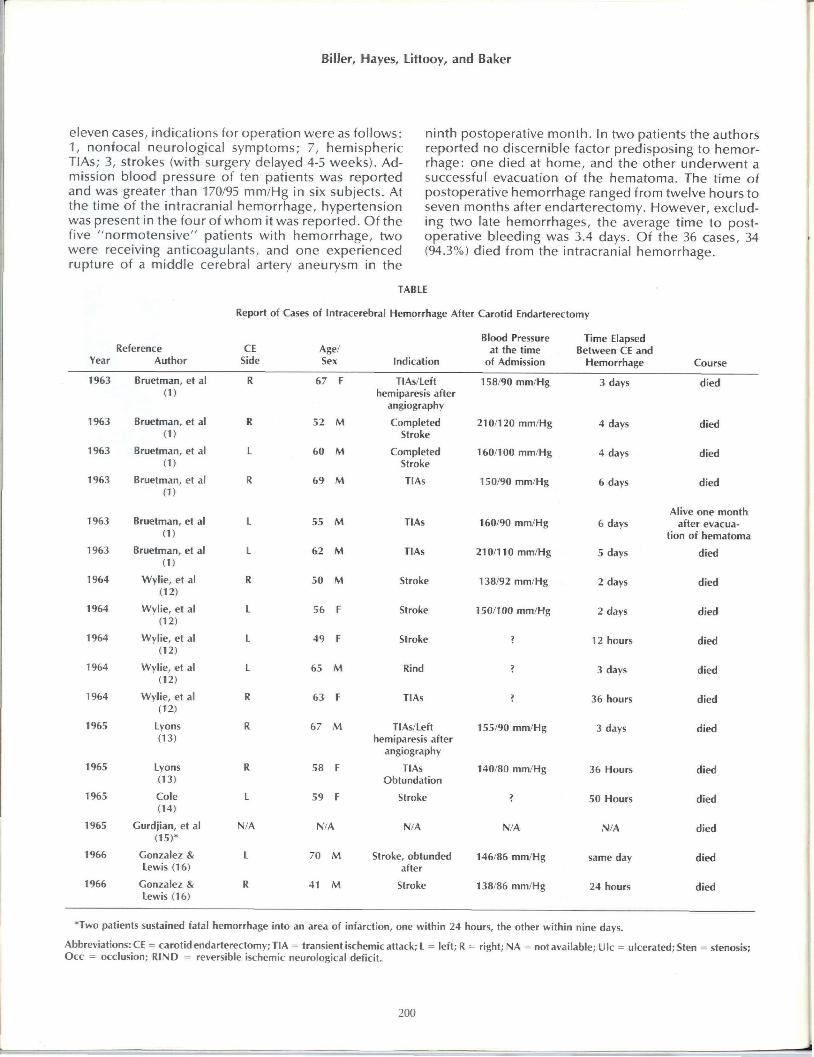
left basal ganglia (Fig. 5). She had significant recovery of neurological func t ion and was discharged on the tenth postoperative day receiving Coumadin. Two months later she suffered sudden global aphasia, dense right hemiparesis, and lethargy. Prothrombin t ime was 19.8 seconds (N: 11.0-12.6 seconds), and CT revealed a large intracerebral hematoma located in the left temporal region extending into the external capsule (Fig. 6). She underwent successful removal of the hematoma and was discharged to a nursing home.
Case 3 An 84-year-old woman experienced an episode of right monocular blindness and transient left hemiparesis, but her neurologic examination was normal. Blood pressure was 150/90 mm/Hg. Cerebral arteriography demonstrated severe stenosis of the internal carotid arteries bilaterally and an incidental 5 x 10 mm left internal carotid - posterior communicat ing junct ion aneurysm. Aphasia developed after angiography when left carotid endarterectomy was per formed. Back pressure was 32/29 mm/Hg wi th a systemic pressure of 198/76 mm/Hg. The aphasia gradually resolved, but seven months later she was found comatose and died the same day. Autopsy revealed that the previously noted aneurysm had ruptured. A previously unrecognized 2 mm aneurysm was found in the right middle cerebral artery, and a small cystic infarction had occurred in the left parieto-occipital junct ion (4).
Fig. 1. Case 1.
CT scan obtained at time of original symptoms demonstrates low density area in r ight superior parietal region consistent w i th an ischemic
infarction.
Fig. 2. Case 1.
Selective right carotid arteriogram demonstrates severe internal carotid artery stenosis and ulceration.
Fig. 3. Case 1.
CT scan obtained three days after right carotid endarterectomy, demonstrates right thalamic hemorrhage. Area of prior infarction was un
changed (not shown).
198
Intracerebral Hemorrhage After Carotid Endarterectomy
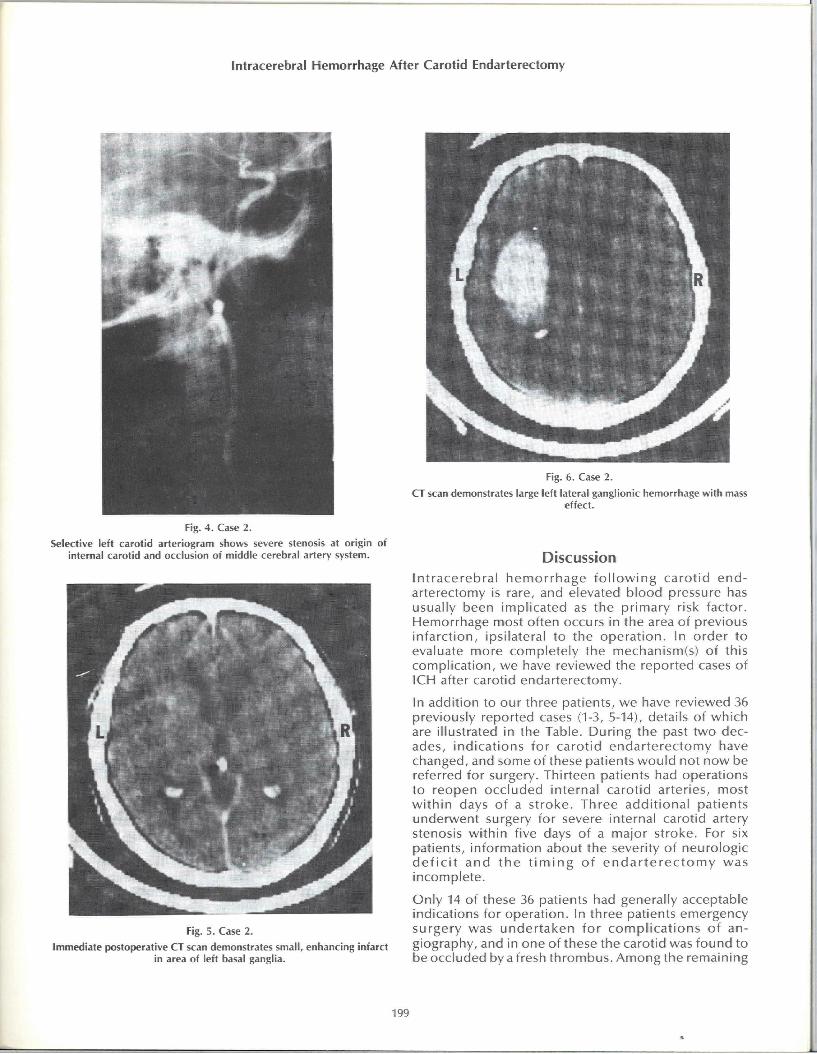
Fig. 4. Case 2.
Selective left carotid arteriogram shows severe stenosis at origin of internal carotid and occlusion of middle cerebral artery system.
Fig. 5. Case 2.
Immediate postoperative CT scan demonstrates small, enhancing infarct in area of left basal ganglia.
Fig. 6. Case 2.
CT scan demonstrates large left lateral ganglionic hemorrhage with mass effect.
Discussion In t racerebra l hemor rhage f o l l o w i n g carot id end arterectomy is rare, and elevated b lood pressure has usually been implicated as the pr imary risk factor. Hemorrhage most often occurs in the area of previous in farct ion, ipsilateral to the operat ion. In order to evaluate more completely the mechanism(s) of this complicat ion, we have reviewed the reported cases of ICH after carotid endarterectomy.
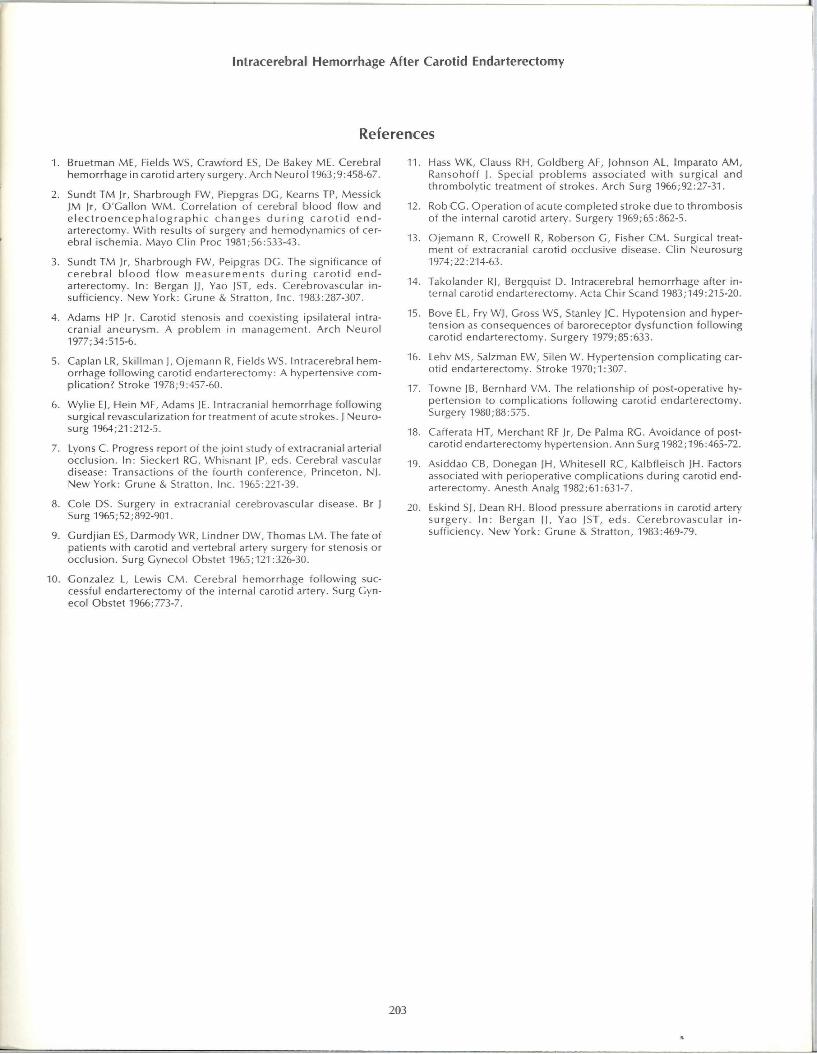
In addition to our three patients, we have reviewed 36 previously reported cases (1-3, 5-14), details of which are illustrated in the Table. During the past two decades, indicat ions for carot id endar terectomy have changed, and some of these patients wou ld not now be referred for surgery. Thirteen patients had operations to reopen occluded internal carot id arteries, most w i th in days of a st roke. Three addi t ional patients underwent surgery for severe internal carotid artery stenosis wi th in five days of a major stroke. For six patients, information about the severity of neurologic d e f i c i t and t he t i m i n g of e n d a r t e r e c t o m y was incomplete.
Only 14 of these 36 patients had generally acceptable indications for operat ion. In three patients emergency surgery was under taken for compl ica t ions of angiography, and in one of these the carotid was found to be occluded by a fresh thrombus. Among the remaining
199
Biller, Hayes, Littooy, and Baker
eleven cases, indications for operation were as fol lows: 1, nonfocal neurological symptoms; 7, hemispheric TIAs; 3, strokes (with surgery delayed 4-5 weeks). Admission blood pressure of ten patients was reported and was greater than 170/95 mm/Hg in six subjects. At the time of the intracranial hemorrhage, hypertension was present in the four of whom it was reported. O f t h e five "normotens ive" patients with hemorrhage, two were receiving anticoagulants, and one experienced rupture of a middle cerebral artery aneurysm in the
ninth postoperative month. In two patients the authors reported no discernible factor predisposing to hemorrhage: one died at home, and the other underwent a successful evacuation of the hemato ma. The time of postoperative hemorrhage ranged from twelve hours to seven months after endarterectomy. However, excluding two late hemorrhages, the average time to postoperative bleeding was 3.4 days. Of the 36 cases, 34 (94.3%) died from the intracranial hemorrhage.
TABLE
Report of Cases of Intracerebral Hemorrhage After Carotid Endarterectomy
Year Reference
Author CE
Side Age/ Sex Indication
Blood Pressure at the time
of Admission
Time Elapsed Between CE and
Hemorrhage Course
1963 Bruetman, et al (1)
R 67 F TIAs/Left hemiparesis after
angiography
158/90 mm/Hg 3 days died
1963 Bruetman, et al (1)
R 52 M Completed Stroke
210/120 mm/Hg 4 days died
1963 Bruetman, et al (1)
L 60 M Completed Stroke
160/100 mm/Hg 4 days died
1963 Bruetman, et al (1)
R (,9 M TIAs 150/90 mm/Hg 6 days died
1963 Bruetman, et al (1)
L 55 M TIAs 160/90 mm/Hg 6 days Alive one month
after evacuation of hematoma
1963 Bruetman, et al (1)
L 62 M TIAs 210/110 mm/Hg 5 days died
1964 Wylie, et al (12)
R 50 M Stroke 138/92 mm/Hg 2 days died
1964 Wylie, et al (12)
L ,->(> F Stroke 150/100 mm/Hg 2 days died
1964 Wylie, et al (12)
E 49 F Stroke ? 12 hours died
1964 Wylie, et al (12)
L 65 M Rind ? 3 days died
1964 Wylie, et al (12)
R 63 F TIAs ? 36 hours died
1965 Lyons (13)
R 67 M TIAs/Left hemiparesis after
angiography
155/90 mm/Hg 3 days died
1965 Lyons (13)
R .58 F TIAs Obtundation
140/80 mm/Hg 36 Hours died
1965 Cole (14)
L 59 F Stroke 7 50 Hours died
1965 Gurdjian, et al (15)*
N/A N/A N/A N/A N/A died
1966 Gonzalez & Lewis (16)
L 70 M Stroke, obtunded after
146/86 mm/Hg same day died
1966 Gonzalez & Lewis (16)
R 41 M Stroke 138/86 mm/Hg 24 hours died
•Two patients sustained fatal hemorrhage into an area of infarction, one within 24 hours, the other within nine days.
Abbreviations: CE = carotid endarterectomy; TIA = transient ischemic attack; L = left; R = right; NA = not available; Ulc = ulcerated; Sten = stenosis; Occ = occlusion; RIND = reversible ischemic neurological deficit.
200
Intracerebral Hemorrhage After Carotid Endarterectomy
TABLE
Report of Cases of Intracerebral Hemorrhage After Carotid Endarterectomy (Continued)
Year Reference
Author CE
Side Age/ Sex Indication
Blood Pressure at the time
of Admission
Time Elapsed Between CE and
Hemorrhage Course
1966 Gonzalez & Lewis (16)
L 65 M Stroke 150/90 mm/Hg 24 hours died
1966 Hass, et al (17)
R 68 M ? Stroke 3 days died
1965
1974
Rob** (18)
Ojemann, et al (19)
N/A
L
N/A
52 M
N/A
TIAs
N/A
R
200/100 mm/Hg 180/100 mm/Hg
L
N/A
4 days
died
died
1978 Caplan, et al
(11)
Caplan, et al (11)
R 57 F Stroke 180/100 mm/Hg 18 hours died
1978
Caplan, et al
(11)
Caplan, et al (11)
L 45 F Stroke 165/95— 170/100 mm/Hg
4 days died
1981 1983
Sundt, et al (2,3)***
L 74 M Near syncope, blurred vision
160/90 mm/Hg 5 days died
1983 Takolander and Bergqvist (20)
L 68 F Stroke 200/110 mm/Hg 1 day died
1983 Takolander and Bergqvist (20)
R 60 F TIAs 150/70 mm/Hg 6 days died
1983 Takolander and Bergqvist (20)
R 69 M TIAs 170/85 mm/Hg 4.5 months died
1983 Takolander and Bergqvist (20)
R-L 67 F TIAs Second Opera
tion asymptomatic
> R CE; 6 wks later L CE
died
1983 Takolander and Bergqvist (20)
R-L 73 F TIAs Second Opera
tion asymptomatic
200/100 mm/Hg 5 days after second
operation
died
1984 Present cases R 63 F Infarct 160/80 mm/Hg 180/90 mm/Hg
3 days after operation
alive
1984 Present cases L 70 F Infarct Incomplete resolution
170/90 mm/Hg 2 months died six months later
1984 Present cases L 84 F TIAs 150/90 mm/Hg 7 months died
**Three patients wi th successful results from arterial reconstruction died of intracranial hemorrhage. ***This reference reports five cases, but only in one are clinical data available. Intracerebral hemorrhage occurred in five patients, and was fatal in four.
Two were on heparin; two were receiving aspirin.
Abbreviations: CE = carotid endarterectomy; TIA = transient ischemic attack; L = left; R = right; NA = not available; Ulc = ulcerated; Sten = stenosis; Occ = occlusion; RIND = reversible ischemic neurological deficit.
Although its incidence is less than 1 % , hemorrhage after enda r te rec tomy represents the largest cause of nontechnically-related neurologic morbidi ty and non-cardiac mortality (1-3). Our experience and this review of the literature indicate four major causative factors of ICH after CE: improper patient selection, arterial hypertension, postoperative use of anticoagulants, and postoperative hyperperfusion.
Patient selection Three aspects of improper patient selection are clear: 1) operating soon after completed severe stroke, 2) re-vascularizing a long-standing totally occluded internal carotid artery, 3) operating in the face of coincidental intracranial pathology. The first two aspects were frequent causes of intracranial hemorrhage in the early carotid endarterectomy experiences. Today, reopening
201

Biller, Hayes, Littooy, and Baker
a chronically occluded artery is infrequently per formed, and carotid endarterectomy after infarction wi th good neurologic recovery is now usually deferred a min imum of 4-6 weeks. These changes reflect awareness of the risk factors involved. Concomitant intracranial pathology includes aneurysms or mass lesions. Even in the presence of these lesions, some patients may nevertheless require endarterectomy. Cases 2 and 3 in this report are examples of these risk factors.
Hypertension and hyperperfusion Arterial hypertension fol lowing carotid endarterectomy is a serious clinical problem with observed incidence between 20% and 56% (15-17). These differences in part reflect the variable def ini t ion of hypertension. Caf-ferata, etal (18) consider hypertension asan elevation in systolic blood pressure greater than 40 mm/Hg above baseline, whi le Towne and Bernhard (17) regard the condit ion as a persistent rise in systolic blood pressure to greater than 200 mm/Hg. We define hypertension as an elevation of blood pressure greater than 10% above the highest preoperative pressure. Assidao and associates (19) noted that hypertension after carotid endarterectomy occurred more frequently among patients with preoperative blood pressures greater than 170/95 mm/Hg. Hypertension may result f rom carotid sinus baroreceptor dysfunction, neurogenic factors, or hy-percarbic anesthesia (20). Bove, et al (15) observed that hypertension resul t ingfrom carotid sinus baroreceptor dysfunction peaked 2.3 hours after endarterectomy. This occurrence three days earlier than the average onset of hemorrhage (3.4 days in our review) suggests that this cause of hypertension may not play an important role in the hemorrhage.
Neurogenic hypertension is believed to be a secondary reflex rise in blood pressure, responding to an increase in intracranial pressure. It has been theorized that during a previous cerebral infarction, neurons and blood vessels were hypoxic and hypoperfused and that restoration of full vascular pressure wi th in the area leads to hemorrhage. Caplan and associates (5) advanced the theory that the vascular bed distal to severe arterial stenosis is protected f rom the effects of hypertension and that the reestablishment of higher perfusion pressure leads to vascular rupture and hemorrhage. In our cases 1 and 2, there was evidence of hypertension in the postoperative per iod. However, in case 1, the high carotid artery back pressure suggests that eliminating the offending carotid lesion did not alter the regional pressure. Sundt, et al (2,3) found no association between changes in blood pressure and postoperative
hemorrhage, but noted that an increased cerebral blood f low (measured by xenon techniques) was a risk factor. They have labeled this postoperative increase in cerebral blood f low the "hyperperfusion syndrome." We did not measure the regional cerebral blood f low in our patients, but none developed other clinical manifestat ions c o m m o n to this syndrome, seizures or migraine headaches. Hypercarbic general anesthesia, included as a possible cause of postoperative hypertension, is of historical interest only.
Postoperative anticoagulation Among the patients wi th ICH after CE reported by Sundt, et al (2,3), two were receiving anticoagulants, and two were receiving antiplatelet medications at the time of hemorrhage. One of our patients with delayed postoperative intracranial hemorrhage and one other reported patient were receiving anticoagulants when they experienced intracerebral bleeding after carotid endarterectomy. In our patient, previous thrombus formation by an aortic valve prosthesis had mandated this therapy.
In summary, postendarterectomy hemorrhagic complications have mult iple causes. Hyperperfusion secondary to revascularization of a severely stenotic artery and systemic hypertension play a predominant role. The use of anticoagulants or antiplatelet medications can be implicated in some cases. Inappropriate t iming of operation was a major cause of complicating intracranial hemorrhage early in the experience with carotid endarterectomy. Recognizing this led to changes in the t iming of and indications for the operat ion. After cerebral infarction, regional changes may include hyperemia, venous congestion, diapedesis, vascular fragility, and consequently intracerebral hemorrhage. These events may explain the t ime delay of hemorrhage after carotid endarterectomy.
Al though the major emphasis for safe carotid endarterectomy has been technical excellence and intraoperative brain protect ion, postoperative intracerebral hemorrhage constituted 12% of the strokes in our series. Recognition of this problem and its causes may lead to safer operations.
Acknowledgments The authors thank Bernadette Spurgeon and Joyce Wi l l -neff for manuscript preparation.
202
Intracerebral Hemorrhage After Carotid Endarterectomy
References
1, Bruetman ME, Fields WS, Crawford ES, De Bakey ME, Cerebral hemorrhage in carotid artery surgery. Arch Neurol 1963;9:458-67,
2, Sundt TM )r, Sharbrough FW, Piepgras DG, Kearns TP, Messick JM jr, O'Gal lon W M , Correlat ion of cerebral b lood f low and e l e c t r o e n c e p h a l o g r a p h i c c h a n g e s d u r i n g c a r o t i d e n d arterectomy. Wi th results of surgery and hemodynamics of cerebral ischemia. Mayo Clin Proc 1981;56:533-43,
3, Sundt TM Jr, Sharbrough FW, Peipgras DG, The significance of ce reb ra l b l o o d f l o w m e a s u r e m e n t s d u r i n g c a r o t i d e n d arterectomy. In: Bergan Jj, Yao JST, eds. Cerebrovascular insuff iciency. New York: Crune & Stratton, Inc, 1983:287-307,
4, Adams HP Jr, Carotid stenosis and coexisting ipsilateral intracranial aneurysm, A p rob lem in management . Arch Neuro l 1977;34:515-6,
5, Caplan LR, Skillman J, Ojemann R, Fields WS, Intracerebral hemorrhage fo l lowing carotid endarterectomy: A hypertensive complication? stroke 1978;9:457-60,
6, Wyl ie E|, Hein MF, Adams JE, Intracranial hemorrhage fo l lowing surgical revascularization for treatment of acute strokes, J Neurosurg 1964;21:212-5,
7, Lyons C, Progress report of the joint study of extracranial arterial occlusion. In : Sieckert RC, Whisnant JP, eds. Cerebral vascular disease: Transactions of the four th conference, Princeton, NJ, New York: Grune & Stratton, Inc, 1965:221-39,
8, Cole DS, Surgery in extracranial cerebrovascular disease, Br J Surg 1965;52;892-901,
9, Gurdj ian ES, Darmody WR, Lindner DW, Thomas LM, The fate of patients wi th carotid and vertebral artery surgery for stenosis or occlusion, Surg Gynecol Obstet 1965;121:326-30,
10. Gonzalez L, Lewis C M . Cerebral hemorrhage fo l l ow ing successful endarterectomy of the internal carot id artery. Surg Gynecol Obstet 1966:773-7,
Hass WK, Clauss RH, Goldberg AF, Johnson AL, Imparato A M , Ransohoff J, Special prob lems associated w i t h surgical and thrombolyt ic treatment of strokes. Arch Surg 1966;92:27-31,
Rob CC, Operat ion of acute completed stroke due to thrombosis of the internal carotid artery. Surgery 1969;65:862-5,
Ojemann R, Crowell R, Roberson G, Fisher C M , Surgical treatment of extracranial carotid occlusive disease, Clin Neurosurg 1974;22:214-63,
Takolander RJ, Bergquist D, Intracerebral hemorrhage after internal carotid endarterectomy. Acta Chir Scand 1983;149:215-20,
Bove EL, Fry WJ, Gross WS, Stanley JC, Hypotension and hypertension as consequences of baroreceptor dysfunct ion fo l lowing carotid endarterectomy. Surgery 1979;85:633,
Lehv MS, Salzman EW, Silen W, Hypertension compl icat ing carot id endarterectomy. Stroke 1970;1:307,
Towne JB, Bernhard V M , The relat ionship of post-operative hypertension to complicat ions fo l lowing carotid endarterectomy. Surgery 1980;88:575,
18, Cafferata HT, Merchant RF Jr, De Palma RG, Avoidance of post-carotid endarterectomy hypertension, Ann Surg 1982;196:465-72,
19, Asiddao CB, Donegan JH, Whitesel l RC, Kalbfleisch JH, Factors associated wi th perioperative compl icat ions dur ing carotid endarterectomy, Anesth Analg 1982;61:631-7,
20, Eskind SJ, Dean RH, Blood pressure aberrations in carotid artery surgery . I n : Bergan JJ, Yao JST, eds. Cerebrovascu la r in sufficiency. New York: Grune & Stratton, 1983:469-79,
11
l i .
13.
14,
15.
16,
17.
203