Embed Size (px)
Citation preview

Complications after primary intracerebral
hemorrhage
Academic dissertation to be presented with assent of the Doctoral Training committee of Health and Biosciences of the University of Oulu for public defence in Auditorium 1 of
Oulu University Hospital on 29 May 2020 at 12 noon

Supervised by Docent Sami Tetri Docent Seppo Juvela Juha Huhtakangas, MD., PhD
Reviewed by Docent Leena Kivipelto Docent Antti Ronkainen
Opponent Professor Jaakko Rinne
ISBN 978-952-94-3351-3 (nid.) ISBN 978-952-94-3352-0 (PDF)
University of Oulu Graduate School; University of Oulu,Faculty of medicine;Medical research center Oulu;Oulu University Hospital

Qian, Cheng
Complications after primary intracerebral hemorrhage.
University of Oulu Graduate School; University of Oulu, Oulu University Hospital, Department of Neurosurgery Oulu, Finland

Qian Cheng, Complications after primary intracerebral hemorrhage Faculty of Medicine, Institute of Clinical Medicine, Department of
Neurology, Department of Neurosurgery, University of Oulu, P.O. Box 5000, FI-90014, University of Oulu, Finland
Abstract
Primary intracerebral hemorrhage (ICH) is a devastating disease associated with high morbidity and mortality despite modern medicine. Complications such as infections, epileptic seizures and thromboembolic events following ICH worsen an already dim outcome. The purpose of this thesis is to investigate complications following ICH and its treatment. In our population-based study of 961 ICH patients we found that high CRP level was associated with poor outcome in ICH patients. This effect was apparent even after excluding infectious diseases. Patients who later developed pneumonia and had increased CRP levels on consecutive days had poor outcome. High CRP at admission, in the absence of silent aspiration pneumonia may suggest severe brain injury in ICH patients. We also studied factors predicting seizures over a different timeline after ICH. In patients with young age, subcortically located hematoma and low Glasgow coma score (GCS) at admission increased the risk of epileptic seizures after ICH. Hematoma evacuation seemed to be associated with late-onset seizures (>2 weeks). We suggest that prophylactic antiepileptic drug (AED) should be considered for the subgroups of patients mentioned above. In our most recent, double blinded, randomized trial with 139 patients we found that in ICH patients, thromboembolic complications are rare when adequate medical and mechanical thrombosis prophylaxis are applied. Administering low-molecular-weight heparin (LMWH) enoxaparin 20mg x 2/day early (1 day after onset) does not increase the risk of rebleeding. Administering enoxaparin later (3 days after onset) is not associated with higher risk of thromboembolic events.
Keywords: Intracerebral hemorrhage, complications, seizures, infections, C-reactive protein, deep vein thrombosis, pulmonary embolism, anticoagulation, low-molecular-weight heparin.

3
Qian, Cheng, Aivoverenvuotopotilaiden komplikaatiot. Oulun yliopiston tutkijakoulu; Oulun yliopisto, Lääketieteellinen tiedekunta, Neurokirurgian klinikka, Neurologian klinikka ; Oulun yliopistollinen sairaala Acta Univ. Oul. D Oulu
Tiivistelmä
Spontaani aivoverenvuoto (ICH) on vakava akuutti sairaus, johon liittyy korkea morbiditeetti ja mortaliteetti nykyaikaisista lääketieteellisestä hoidoista huolimatta. ICH:n jälkeiset komplikaatiot kuten infektiot, kouristukset ja laskimotromboosit huonontavat potilaiden ennustetta. Tämän väitöskirjan tarkoituksena on tutkia tarkemmin ICH:n komplikaatioiden esiintyvyyttä ja niiden hoitoa. Laajassa retrospektiivisessa 961 potilasta kattavassa populaatiopohjaisessa tutkimuksessa havaitsimme, että potilaan korkea CRP-arvo sairaalaan tullessa korreloi huonontuneen ennusteen kanssa. Tämä vaikutus oli selvä, vaikka poissuljettiin myöhemmässä vaiheessa kehittyneet infektiot. Potilailla, jotka saivat myöhemmässä vaiheessa keuhkokuumeen, oli huonontunut ennuste; heillä CRP-arvo nouseekin yleensä tulovaiheen jälkeisinä päivinä merkittävästi. Niillä, jotka eivät kehittäneet keuhkokuumetta, tulovaiheen korkea CRP voi olla merkki vaikeasta aivovauriosta. Tarkastelimme myös ICH-potilaiden kouristusten esiintyvyyttä ja ajankohtaa aivoverenvuodon jälkeen. Epileptisten kohtausten riskiä lisääviä tekijöitä ovat nuori ikä, matala tajunnantaso ja ICH:n subkortikaalinen sijainti. Leikkaushoito lisäsi riskiä saada epileptisiä kouristuskohtauksia myöhemmässä vaiheessa (>2vk vuodosta). Edellä mainituille potilaille suosittelemme profylaktisen kouristusestolääkityksen aloittamista ICH:n toteamisen yhteydessä. Syvän laskimotukoksen ja keuhkoembolian esiintyvyyttä spontaani ICH -potilailla ja niitä ennalta ehkäisevien lääkehoitojen komplikaatioita tutkittiin prospektiivisessa randomisoidussa kaksoisokkoutetussa tutkimuksessa. Havaitsimme, että syvät laskimotukokset ja keuhkoemboliat olivat hyvin harvinaisia komplikaatioita ICH:n jälkeen nykyaikaisten laskimotukoksia ehkäisevien lääkehoitojen ansiosta. Aikainen (1vrk vuodosta) enoksapariini-hoidon aloitus (20mgx2/päivä) ei näyttänyt lisäävän vuotojen laajenemista tai uusintavuotoja. Enoksapariini-hoidon myöhäinen (3vrk vuodosta) aloitus ei altistanut lisääntyneelle tukosriskeille.

Asiasanat: Aivoverenvuoto, komplikaatiot, epileptiset kouristuskohtaukset, infektiot, CRP, syvälaskimotukos, keuhkoembolia, antikoagulaatio, enoxaparin

To my family

8

9
Acknowledgments First of all, I want to express my sincere gratitude for my supervisor, Associate professor Sami Tetri. Without his patient guiding hands, this thesis would be impossible task for me to accomplish. His fatherely guidence to me in both research world and vascular neurosurgery will never be forgotten. Thank you for my first clipping of ruptured MCA aneurysm. I thank Juha Huhtakangas for his enlightning views of research and the field of neurology. I owe my gratitude to Seppo Juvela whos scientific mind has no rival in neurosurgical field. I would like to thank emeritus professor Matti Hillbom that he saw potential in me and gave me ideas for the works of this thesis.
I am in forever debt to my great reviewers, Leena Kivipelto and Antti Ronkainen. Your advices made this thesis three thousand times better than it would have been.
As a mentor of mine and a great influence in both neurosurgery and life, I would like to dedicate my gratitude to chief of neurosurgery Timo Kumpulainen. Without you, instead of living my vascular neurosurgery life I would still be just dreaming about it. I want also thank another mentor of mine, interventional radiologist Matti Isokangas for supporting me in both academic and clinical field of vascular neurosurgery. The stoic calmness of both Timo and Matti has many times saved me and my patients from catastrofic outcomes.
I would like to thank my collaborators and fellow researchers Tatlisumak Turgut, Savolainen Marika, Numminen Heikki, Ollikainen Jyrki, Luostarinen Liisa and Kupila Laura for providing valueble additional data for our projects. I thank you for your patience toward my never-ending projects. I owe my gratitude to the finest radiologists in the world; Michaela Bode, Kari Palosaari and Harri Littow. Thank you for the teachings of neuroradiology and vascular neuroradiology for novice such as myself. I thank Vesa Kiviniemi for his enthusiastic and inspiring view toward science and life itself. Facebook updates of his are legendary. I thank Anna-Maija Lahti and Tommi Korhonen for showing me the way to become better scientist.
For Susanna Yli-luukko and Niina Salokorpi I thank for supporting me in a difficult period of my life. Their understanding of my shortcomings is unprecedented in the relationship of employer employees. I thank professor Ville Leinonen for his enthusiastic views on academic neurosurgery and his support to my vascular neurosurgery career path.

10
Leinonen for his enthusiastic views on academic neurosurgery and his support to my vascular neurosurgery career path.
I thank Anna-Leena Heula and Juho Tuominen for their support and enlightning conversations throughout the years. For Tatu Koskelainen, I still remember to laugh everytime I come accross to a Tom of Finland bed shields. I thank Dr Mcdreamy of Oulu, Mikko Kauppinen for his support and teachings especially in trauma and spinesurgery. For Maija Lahtinen, thank you for sharing with me your enthusiastic attitude toward neurosurgery and your moral compass that point nowhere else than toward right direction. I hope that some day I would become more like you without the component of OCD. Other half of DBS duo of Oulu is of course the great Jani Katisko. I thank him for his wise advices for me throughout the years. I would like to thank fellow neurosurgeon and best dancer I have ever known, Mirva Nätynki for her views in life which have forced me to grow as a both person and a parent. I thank Jenni Määttä for her friendship, ideas and technical support in the making of this thesis. For Ansku Suutari, I thank for her friendship and support during this extraordinary period of my life. Samurai life forever! I also thank young Padawan Antti Knuutinen for his friendship and technical support. A big shout out for the younger generation of neurosurgeons Miro Jänkälä, Susanna Piiroinen and Jukka Puolitaival. Thank you for your friendship and support. I thank Sari Kukkamaa for her wise words. I thank Tuija Keinänen for her friendship.
I owe my gratitude to Ulla Ollila. She has made a dent in my universe by helping me to rediscover my past and hopefully reshape my future.
Finally my deepest gratitude goes to my family. I thank my parents for raising me from a weak boy to an imperfect man as I am today. The task was undoubtly haunting and with many sacrifices. I can only hope that i could be even a fracture of a good parent to Eeli than you were for me. I thank the cutest boy of all galaxy Eeli Hao Xuan for his love and trialing. I hope in the years to come you will preserve your curiosity for life, search for true happiness and be more like your mother. Lastly but not the least, I owe my greatest debt to Henna Qian. Without her undying love and support, none of my personal and academic achievement would have been possible. You have endured a trip to hell and back with me and there are simply not enough words to describe what an extraordinary human being you are.
This thesis was financially supported by Oulu university and Maire Taponen foundation.

11
10.04.2020 Cheng Qian

12

13
Abbreviations AF Atrial fibrillation AHA/ASA American heart association / American stroke association AVM Arteriovenous malformation AED Antiepileptic drug AMI Acute myocardial infarction APOE Apolipoprotein-E ASA Acetylsalicylic acid BP Blood pressure CAA Cerebral amyoloid angiopathy cEEG Continous electroencephalogram CT Computer tomography CTA Computer tomography angiography CTPA Computer tomography pulmonary angiography CRP C-reactive protein CSF Cerebrospinal fluid CNS Central nervous system DSA Digital subtraction angiography DVT Deep vein thrombosis ECG Electrocardiogram EEG Electroencephalogram EVD External ventricular drain ETV Endoscopic third ventriculostomy GCS Glasgow coma scale GI Gastrointestinal GOS Glascow Outcome Scale ICH Intracerebral hemorrhage IVH Intraventricular hemorrhage ICP Intracranial pressure INR International normalized ratio ICU Intensive care unit IPC Intermittent pneumatic compression LMWH Low-molecular-weight heparin MRI Magnetic resonance image MRA Magnetic resonance angiogram MI Myocardial infarction

14
MIS Minimally invasive surgery mRS Modified rankin score NSM Neurogenic stunned myocardium NSAID Nonsteroidal anti-inflammatory drug NIHSS National institutes of health stroke scale OAT Oral anticoagulation therapy OR Odds Ratio PCC Prothrombin complex concentrate PCI Percutaneous coronary intervention PE Pulmonary embolism pICH Primary ICH RCT Randomized controlled trial rFVII Recombinant factor VII rtPA recombinant tissue-type plasminogen activator SAH Subarachnoidal hemorrhage SBP Systolic blood pressure SD Standard deviation SSRI Selective serotonin reuptake inhibitor TIA Transient ischemic attack UTI Urinary tract infection VTE Venous thrombotic event

15
Original publications This thesis is based on the following publications, which are referred to throughout the text by their Roman numerals:
I Löppönen P, Qian C, Tetri S, Juvela S, Huhtakangas J, Bode MK, Hillbom M. (2014). Predictive value of C-reactive protein for the outcome after primary intracerebral hemorrhage. Journal of neurosurgery, 121(6), 1374-9. II Immediate, early and late seizures after primary intracerebral hemorrhage.
Qian C, Löppönen P, Tetri S, Huhtakangas J, Juvela S, Turtiainen HM, Bode MK, Hillbom. (2014). Immediate, early and late seizures after primary intracerebral hemorrhage. Epilepsy Res.108(4):732-9.
III Qian C., Huhtakangas J., Juvela S., Bode M., Tatlisumak T., Numminen H., Ollikainen J., Luostarinen L., Kupila L., Tetri S. Early vs. late enoxaparin for prevention of venous thromboembolism in patients with ICH. Manuscript.

16
Contents Abstract Tiivistelmä Acknowledgments 9 Abbreviations 13 Original publications 15 Contents 16 1 Introduction 19 2 Review of the literature 21
2.1 Intraventricular hemorrhage and hydrocephalus ..................................... 21 2.1.1 Treatment of intraventricular hemorrhage and acute
hydrocephalus ............................................................................... 23 2.1.2 Treatment of chronic hydrocephalus ............................................ 24 2.1.3 Intraventricular clot lysis ................................................................ 24
2.2 Enlargement of intracerebral hematoma ................................................. 26 2.2.1 Definition ...................................................................................... 26 2.2.2 Risk factors ................................................................................... 27 2.2.3 Pathophysiology ........................................................................... 27 2.2.4 Radiological signs ........................................................................ 28 2.2.5 Medical treatment ......................................................................... 30 2.2.6 Surgical treatment ......................................................................... 32
2.3 Infection .................................................................................................. 37 2.3.1 Infections and outcome ................................................................. 39 2.3.2 Role of CRP .................................................................................. 40
2.4 Seizures ................................................................................................... 41 2.4.1 Definition ...................................................................................... 41 2.4.2 Classification of seizure types ...................................................... 41 2.4.3 Incidence of seizures .................................................................... 41 2.4.4 Treatment of seizures .................................................................... 42 2.4.5 Prophylactic anti-epileptic drugs .................................................. 43 2.4.6 Effect on outcome ......................................................................... 44
2.5 Thromboembolic complications .............................................................. 45 2.5.1 Pathophysiology of venous thrombotic events ............................. 45 2.5.2 Diagnosis of deep venous thrombotic events ............................... 45 2.5.3 Diagnosis of pulmonary embolism ............................................... 46 2.5.4 General treatment of venous thrombotic events ........................... 47

17
2.5.5 Thrombosis treatment in ICH patients ......................................... 47 2.5.6 Resuming anticoagulation after ICH ............................................ 48 2.5.7 Thrombosisprophylaxia in intracerebral hemorrhage
patients .......................................................................................... 49 2.6 Cardiac complications ............................................................................. 51
2.6.1 Myocardial infarction ................................................................... 51 2.6.2 Neurogenic stunned myocardium ................................................. 52 2.6.3 Atrial fibrillation ........................................................................... 53
3 Aims of the research 55 4 Methods 56
4.1 Population based cohort (I-II) ................................................................. 56 4.1.1 Clinical data - Study I ................................................................... 56 4.1.2 Clinical data - Study II ................................................................. 57 4.1.3 Neuroradiological methods .......................................................... 57 4.1.4 Outcome measurements ................................................................ 58 4.1.5 Statistical methods ........................................................................ 58
4.2 Prospective randomized study (III) ......................................................... 59 4.2.1 Study population ........................................................................... 59 4.2.2 Radiological methods ................................................................... 60 4.2.3 Randomization .............................................................................. 60 4.2.4 Administration of medicine .......................................................... 61 4.2.5 Outcome measurements ................................................................ 61
5 Results 63 5.1 Infection after intracerebral hemorrhage (I) ............................................ 63
5.1.1 Effect of infections on outcome .................................................... 63 5.1.2 Effect of admission CRP level on outcome .................................. 64
5.2 Seizures after intracerebral hemorrhage (II) ........................................... 66 5.2.1 Seizure groups .............................................................................. 66 5.2.2 Risk factor for different seizures groups ...................................... 67 5.2.3 Outcome and mortality between seizure groups ........................... 68
5.3 Thromboembolic complications after intracerebral hemorrhage (III) .......................................................................................................... 70
6 Discussion 74 6.1 Main findings .......................................................................................... 74
6.1.1 Study I .......................................................................................... 74 6.1.2 Study II ......................................................................................... 76 6.1.3 Study III ........................................................................................ 78

18
7 Summary and conclusions 81 References 83 Original publications 104

19
1 Introduction
Primary intracerebral hemorrhage (ICH) is a hemorrhagic form of stroke which is a result of a spontaneous rupture of a small vessel located often in the parenchyma of the brain matter. In Finland the incidence is around 31/100000 (Fogelholm, Nuutila, & Vuorela, 1992). Conditions such as long-term untreated hypertension or cerebral amyloidangiopathy (CAA) may exacerbate the risk of primary ICH (Fogelholm et al., 1992; Juvela, S., Hillbom, & Palomäki, 1995; Juvela, S., 1996). Anticoagulation and antiplatelet medication has been seen to increase ICH volume rapidly and worsens already dim outcome of ICH patient (Feigin, Lawes, Bennett, Barker-Collo, & Parag, 2009; Fogelholm et al., 1992). ICH often results in catastrofical neuronal tissue damage as blood gushes with significant velocity and tears certain parts of the brain apart. This often leaves patients with severe neurological impairment. Almost half of patients die within the first month and 80% of survivors are dependent on a caregiver (van Asch et al., 2010).
Medical treatment of ICH mostly consist of lowering blood preassure to minimize toxic edema and the risk for hematoma enlargement. Systolic blood preassure is kept often at 140mmHg to 160mmHg to reduce the risk for hematoma enlargement (Anderson et al., 2008; Anderson et al., 2013; Qureshi & Palesch, 2011). Patients with anticoagulant or antiplatelets are cessed and reversed accordingly. Platelet transfusion has shown to lower patient outcome and is thus not recommended (Baharoglu et al., 2016).
Surgery has rather limited role in treatment of supratentorial ICH. Although some retrospective studies has shown that craniotomy may lower patient mortality, the effectivness of conventional craniotomy has not been proven in randomized studies (Mendelow et al., 2005; Mendelow et al., 2013). Contrary to supratentorial hematomas, in cerebellar ICH, surgery has seen to improve patient outcome (Firsching, Huber, & Frowein, 1991; Kuramatsu et al., 2019). In recent years attention has been toward more mini-invasive techniques such as endoscopic approach for ICH evacuation. Endoscopic surgery has seen to improve patient functional outcome compared to conventional craniotomy or standard medical treatment (Zhou et al., 2012).
Patients with ICH and paresis are at risk for thromboembolic events (Di Nisio, van Es, & Büller, 2016). Patients who are bedridden and with low consciousness can find their immunological system affected, resulting in many

20
types of infectious disesases such as pneumonia (Lord et al., 2014). Usage of a urinal catheter is a independent risk for urinary tract infection (Lord et al., 2014). After the onset of ICH, patients have been seen to have more cardiovascular complications such as myocardial infarction, arythmias and heart failure (Hasegawa et al., 2012). These conditions lower the overall survival of ICH patients.
Because of the limited role of prevention and treatment of ICH, more attention should be paid to preventing the complications of ICH. Effective treatment of ICH patient complications has a significant effect on patient morbidity and mortality (Balami & Buchan, 2012). The main focus of this thesis is to investigate complications in ICH and how to manage them efficently.

21
2 Review of the literature
2.1 Intraventricular hemorrhage and hydrocephalus
Hydrocephalus occur in about 23% of ICH patients. If ICH has an intraventricular hematoma (IVH) component, 55-67% of these patients will develop hydrocephalus (Fig 1) (Mendelow et al., 2005 ;Bu et al., 2016 ;Diringer, Edwards, & Zazulia, 1998a; Hemphill, J. C., Bonovich, Besmertis, Manley, & Johnston, 2001a). It has been found that IVH risk is increased if ICH is located at the basal ganglia and thalamus region near to the lateral ventricle system (Engelhard, Andrews, Slavin, & Charbel, 2003; Hallevi et al., 2008). Purely intraventricular hemorrhage with no parenchyma extension is a rare form of ICH and constitutes only 2% of all ICH cases (Bu et al., 2016). Compared to ICH with mainly parenchymal location, pure IVH has a higher probability (21%) for secondary causes such as vascular anomalies of arterial-venous malformations or intracerebral aneurysms (Weinstein, Ess, Sirdar, Song, & Cutting, 2017).
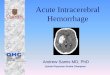
Hydrocephalus is categorized as non-communicated and communicated form (Bu et al., 2016). In acute phase non-communicated (obstructed) form occurs when a blood clot disrupts CNS outflow in the ventricle system( Fig 1). This can lead to headache, nausea and lower mental status which is a result of increased intracranial preassure (ICP) (Weinstein et al., 2017). In time, blood products and debris causes scarring of arachnoid granulations and ependymal linings and subsequently reduces its ability to absorb CSF from the ventricle system, resulting in the development of chronic (communicating) hydrocephalus (i.e., risk of permanent shunting) (Fig 2). Both types of hydrocephalus are possible following ICH with IVH extension. It has been shown in many publications that IVH and hydrocephalus lowers patients’ outcome (Bhattathiri, Gregson, Prasad, & Mendelow, 2006; Diringer et al., 1998; Hemphill, J. C., Bonovich, Besmertis, Manley, & Johnston, 2001b; Hwang et al., 2012; Stein, M. et al., 2010). Only 15% of ICH patients with IVH extension had a good outcome (Mendelow et al., 2005; Mendelow et al., 2013). Mortality rate increases two-fold in ICH patients with IVH extension compared to patients without IVH (Gaberel, Magheru, & Emery, 2012).

22
Fig. 1. Blood clot in the ventricle system as seen in head CT can in later phase cause hydrocephalus.

23
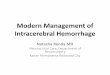
Fig. 2. 3 weeks from IVH, due to resorption malfunction, chronic hydrocephalus occurs. In head CT, the size of ventricles increase and periventricular edema may occur.
2.1.1 Treatment of intraventricular hemorrhage and acute hydrocephalus
In the acute setting of IVH leading to hydrocephalus, patients are generally associated with a lower GCS score and higher ICP compared to patients without IVH (Diringer, Edwards, & Zazulia, 1998b). There is limited data regarding treatment of high ICP and hydrocephalus in the IVH setting. In a prospective paper by Diringer et al., hydrocephalus patients with EVD were compared to patients receiving only standard medical care (Diringer et al., 1998). It shows that although patients with hydrocephalus had higher in-hospital mortality and worse outcome, EVD treatment has no effect on patient outcome compared to conservative treatment. This study, though, has limitations. As it was not randomized, more moribund patients were treated with EVD and thus the positive effect of EVD may not be seen. However, based on data regarding a higher mortality rate for hydrocephalus and the current guidelines for treatment in traumatic brain injury associated with high ICP, the AHA/ASA still recommend ventricular drainage for patients with hydrocephalus, especially those with a decreased level of consciousness (Hemphill, J. Claude et al., 2015). European guidelines do not make any strong recommendations about EVD placement for ICH patients in the absence of RCTs (Steiner et al., 2014).

24
2.1.2 Treatment of chronic hydrocephalus
Overall, 13 % of ICH patients require EVD during the acute phase to treat hydrocephalus (Diringer, Edwards, & Zazulia, 1998b). In the later phase, 23% of these patients will develop communicated hydrocephalus that requires permanent CSF diversion (Kuo et al., 2018). Patients persisted with elevated ICP, extensive amount of intraventricular component, and thalamic location of their hemorrhage are at increased odds of developing persistent hydrocephalus, necessitating permanent ventricular shunt placement (Kuo et al., 2018; Zacharia et al., 2012). Ventriculoperitoneal shunting is not a procedure without complication. Infectious complication occurs in between 5-15% with permanent shunting as well as epileptic seizures, intracerebral hemorrhage, and malfunction of shunt (Robertson, Maraqa, & Jennett, 1973).
Endoscopic third ventriculostomy (ETV) has emerged as an alternative for ventriculoperitoneal shunting. In the event of primary failure or complication of permanent CSF diversion, ETV may be more suited than conventional shunting. Long term retrospective analysis has shown ETV to be effective as the success rate is as high as 73-87%. The complication rate was a relatively low 2-11% and most of those were minor complications (Isaacs et al., 2016; Waqar et al., 2016).
2.1.3 Intraventricular clot lysis
It has been shown that the risk of developing later hydrocephalus and the need for permanent CSF diversion, correlates with the extent of blood clot in the ventricle system (Kuo et al., 2018). Animal studies have shown that administering intraventricular fibrinolytic agents, including recombinant tissue-type plasminogen activator (rtPA) and urokinase in IVH, reduces mortality and accelerates blood clot lysis (Fountas et al., 2005; Lapointe & Haines, 2002; Naff et al., 2004; Nieuwkamp, de Gans, Rinkel, & Algra, 2000; Pang, Sclabassi, & Horton, 1986). Smaller retrospective and prospective analysis data has shown a reduction in mortality from 30-44% to 10% in patients given rtPA (Dunatov, Antoncic, Bralic, & Jurjevic, 2011; King et al., 2012). Adverse reaction such as ventriculitis from intrathecal drug delivery is around 11% (Castaño Ávila et al., 2013). CLEAR-IVH randomized trial was conducted with 26 patients randomized

25
to receiving intraventricular rtPA and 22 receiving placebo (Naff et al., 2011). Although clot lysis was more efficient in rtPa group, there was no statistically significant differences in mortality between groups (18% rtPa vs. 23% placebo). Symptomatic bleeding occurred more frequently in rtPa group (23% rtPa vs. 5% placebo). In a phase III randomized trial from Hanley et al. (CLEAR -III), 251 patient was assigned to receiving intraventricular rtPA and 249 patient receiving placebo (0.9% saline) (Hanley et al., 2017). In 180 days follow up, patients mortality in rtPA group was lower than in placebo group (18% rtPA vs. 29% placebo, P=0.006). However greater amount of patients had poorer functional outcome in rtPA group (17% rtPA vs. 9% placebo, p=0.007). There wasn’t different in symptomatic bleeding between two groups and serious adverse events and ventriculitis was lower in rtPA group. There seems to be a trend in better outcome for patients with over 80% reduction in hematoma volume (Hanley et al., 2017). Patients receiving rtPA treatment had reduced intracranial pressure, fewer EVD obstructions that required re-operations and a non-significant shorter duration of EVD (Ziai et al., 2012). Authors concluded although intraventricular clot lysis seems to be safe method, routine use of intrathecal thrombolysis could not be recommended as there is no data to support better functional outcome. In another CLEAR-IVH subanalysis, intraventricular hematoma lysis has no significant effect on reducing the need for permanent CSF diversion (Murthy, Awad et al., 2017). In a meta-analysis investigating the role of intraventricular fibrinolytic treatment, mortality was lower at 30 days in treatment arm (P < 0.001), 180 days (P = 0.001), 365 days (P = 0.40), and overall (P < 0.001). Functional outcome was also better in treatment group (p=0.02) (Baker et al., 2018). Basing on available data, AHA/ASA states that although it is relatively safe for intraventricular rtPA treatment, there is not sufficient evidence to say that this treatment increases patient outcome (Hemphill et al., 2015). Also, European guidelines cannot make any strong recommendation for intrathecal thrombolysis in spontaneous ICH (Steiner et al., 2014).
There is research of other treatment options for IVH such as endoscopic surgical evacuation of hematoma directly from ventricular space. One study compared 48 patients treated with endoscopic evacuation of IVH with the historical results of patients treated with EVD alone. They found a reduction of permanent shunting procedures from 50% to 17% in favor of the endoscopic group (Basaldella et al., 2012). Other small studies showed similar results as endoscopy seems to reduce the need for permanent shunting (Chen et al., 2011; Zhang, Z. et al., 2007). However, these kinds of mini-invasive clot evacuation

26
procedures did not seem to have a significant effect on overall morbidity and mortality compared to EVD alone.
2.2 Enlargement of intracerebral hematoma
2.2.1 Definition
Hematoma volume and its enlargement is calculated mostly with ABC/2, planimetry and 3Dvolume rendering techniques (Brouwers & Greenberg, 2013). CT has been utilized in the majority of cases at the acute setting, because of its easy availability and good accuracy for the purpose of calculating hematoma volume. Different definitions have been used across studies to describe hematoma growth between the initial (baseline) CT and the follow-up CT, which is normally acquired within 24 – 72 hours after the first CT was obtained. The most used definition of hematoma enlargement is growth of hematoma volume >33% or >12.5ml in follow-up CT (Delcourt et al., 2010; Qureshi & Palesch, 2011).
The frequency of hematoma enlargement varies in different studies and depends on various techniques to calculate hematoma volumes and the time of onset to CT. Hematoma enlargement occur at some degree in 73% of patients if the first head CT was obtained within 3 hour of symptom onset (Davis et al., 2006). If the first CT was obtained over 6 hours after onset, only 11% will have hematoma enlargement (Brouwers & Greenberg, 2013). Overall, it is estimated that 25- 38% of ICH patients experience significant hematoma enlargement (Davis et al., 2006; Brott et al., 1997). Majority of them occurred within 24h of onset (Brott et al., 1997).
Hematoma enlargement is widely associated with a higher risk of morbidity and mortality (Brouwers & Greenberg, 2013). Mortality rises 5% for every 10% increase in ICH volume. For every ml of increase in hematoma volume, 7% of patients are more likely to digress/regress from independency to dependency (Brouwers & Greenberg, 2013). The speed of hematoma growth has seen to affect patient outcome as >5ml/h growth lowers outcome 2-fold compared to hematoma growth <5ml/h (Sato et al., 2014).

27
2.2.2 Risk factors
Antithrombotic and anticoagulation medication is associated with hematoma enlargement (Al-Shahi Salman et al., 2018; Saloheimo et al., 2006). Consumption of ASA at the time of onset has been seen to increase the risk of hematoma enlargement 2-fold. Anticoagulants increase mortality from 52% to 68% (Saloheimo et al., 2006). It is possible that some of the morbid outcome can be explained by the fact that patients who have been prescribed ASA suffer diabetes and cardiovascular diseases pre ictus. Those comorbidities have been proven to independently lower patient outcome and increase mortality (Nilsson, Lindgren, Brandt, & Säveland, 2002; Ostábal, Sanz-Sebastián, Suárez-Pinilla, & del Río-Ligorit, 1996; Tetri, Mäntymäki et al., 2008; Tetri, Juvela, Saloheimo, Pyhtinen, & Hillbom, 2009). Other factors associated with hematoma growth are coagulopathia such as liver disease, (Fang, Lin, & Ko, 2005; Kuramatsu et al., 2015a; Takahashi, Urano, Nagai, Takada, & Takada, 1998) high blood pressure (Rosand, Eckman, Knudsen, Singer, & Greenberg, 2004) and thrombocytopenia (Fang et al., 2005).
2.2.3 Pathophysiology
Hematoma enlargement has long been often conceptualized as a single vessel rupture which continues to bleed (Brouwers et al., 2013). However, this theory fails to explain later expansion of bleeding that may happen hours and days after onset. In addition, there is no histopathological proof for this theory. C.Miller Fisher explained hematoma enlargement through his “avanlanche theory” in which the hematoma enlarges by secondary mechanical shearing of adjacent vessels caused by the expansion of the initial hemorrhage (Fisher, C. M., 1971). Essentially, based on this theory, after the initial vessel rupture or ruptures, the hematoma causes a chain reaction cascade to its adjancent small cerebral vessels and also induces them to rupture. This causes the hematoma to grow larger than it originally would. There has been genetic research that support this theory as apolipoprotein (APOE) e2 allel has been found at the hematoma cavity. E2 allel appears to be within those fragile vessels in amyloidangiopathy patients

28
(Greenberg et al., 1998; McCarron et al., 1999). It is also not uncommon that spot signs are seen in different locations of the hematoma cavity as two active bleeding appears to be simultaneously occurring in more than one place (Brouwers, Biffi et al., 2012; Delgado Almandoz et al., 2009).
2.2.4 Radiological signs
Spot sign is a focal contrast accumulation on CTA representing active bleeding and extravasation (Fig 3). This is represented as a gathering of contrast material inside the hematoma (Nagasaka, Inao, & Wakabayashi, 2013). Spot sign increases the risk of hematoma enlargement and by itself is a sign of bad outcome and mortality (Goldstein, J. N. et al., 2007; Kim et al., 2008; Murai, Ikeda, Teramoto, & Tsuji, 1998). However, it is criticized for low sensitivity as half of all patients who suffer hematoma enlargement do not have spot sign on their initial CTA (Demchuk et al., 2012). Positive predictive value of spot sign in CTA taken 2 hours after onset is 61%. Negative predictive value of early spot sign is 78% (Demchuk et al., 2012). Other signs, such as island sign in native CT, has also been found to be a predictive factor for hematoma enlargement (figure 4) (Li, Q. et al., 2017).

29
Fig. 3. Head CT without contrast shows deep seated ICH (left picture). CTA from the same patient shows spot sign inside the ICH (the green arrow) indicating active bleeding (right picture).

30
Fig. 4. In head CT, Island sign is shown in basal ganglia hematoma patient. Island sign is defined as ≥3 smaller hematomas separated from the main hematoma or ≥4 smaller hematomas some or all of which are connected to the main hematoma. Note 3 smaller hematomas (arrows) separate from the main hematoma (Li et al., 2017).
2.2.5 Medical treatment
In medical therapy for preventing hematoma enlargement, a randomized trial of recombinant factor VIIa (rFVIIa) conducted in 2005 was among the most anticipated (Mayer et al., 2005). 399 ICH patient were randomized to receive either placebo or rFVIIa at 4 hour of initial symptom onset. Hematoma enlargement was assessed at 24 hour from baseline. Clinical outcome were assessed at 90 days. In this trial it showed promising results for reducing the risk of hematoma growth (14% in rFVII vrs 29% in placebo group hematoma size

31
grew in 24h, p= 0.01). Bad outcome (mRANKIN 4-6) were significantly more in placebo group than in rFVIIa group (69% placebo vs. 49% rFVIIa, p=0.004). Mortality at 90 days were lower in rFVIIa group compared to placebo group (18% rFVIIa vs. 29% placebo, p=0.02). There were no significant differences in serious adverse effect between groups (p=0.12). Encouraged by positive preliminary results, phase III trial was conducted with 841 patient randomized to receive rFVIIa or placebo (Mayer et al., 2008). Clinical outcome were assessed at 180 days. In this trial, statistically significant reduction in growth of hematoma volume was associated with patients who received 80 µg/kg compared to placebo group (11% rFVIIa vs 26% placebo, p<0.001). However, administering rFVIIa did not have any effect on overall patient outcome (29% in rFVII and 24% in placebo group had bad outcome) (Mayer et al., 2008). One possible explanation for this could be that patients with a higher risk of hematoma enlargement were not adequately identified. Patients who would have been initially low risk for hematoma enlargement, i.e., with negative spot sign were also given rFVIIa, therefore submitting patients to non-necessary thromboembolic complications. Serious arterial thromboembolic event occurred in 9% of the rFVII group versus 4% in the placebo group ( p=0.04) (Mayer et al., 2008).
Another interesting topic is whether lowering blood pressure (BP) can reduce the risk of hematoma enlargement. The theory is that high BP prolongs bleeding from a ruptured vessel, which increases the risk of hematoma enlargement (Manno, Atkinson, Fulgham, & Wijdicks, 2005). High BP may also aggravate more cerebral edema, which also affects patient outcome (Manno, Atkinson, Fulgham, & Wijdicks, 2005; Rasool, Rahman, Choudhury, & Singh, 2004). A large randomized study (INTERACT) was conducted in 2008 to compare the efficiency and safety for intensively lowering BP (target systolic BP 140mmHg) versus standard recommendation of BP (systolic BP 180mmHg) (Anderson et al., 2008). It showed that mean hematoma growth differs between groups as in the intensive group hematoma volume grew 13.7% and in the guideline group 36.3% (p=0.04) respectively. The relative risk of hematoma growth was also 36% lower in the intensive group compared to the guideline group (p=0.05) (Anderson et al., 2008). Although intensive BP-lowering treatment seems to lower the risk of hematoma enlargement and didn’t show any risk of adverse events, there was not any significant effect on mortality and functional outcome (Anderson et al., 2008; Anderson et al., 2013; Martí-Fàbregas et al., 2008). Although extensively reducing high systolic blood preassure didn’t seem to affect patient outcome, systolic blood preassure variability seem to associate with poor outcome in ICH

32
patients (Manning et al., 2014). Particularly avoiding peaks and reducing systolic blood preassure in smooth fashion is speculated to improve patient outcome (Manning et al., 2014).
Oral Anticoagulation therapy (OAT)’s worst side effect is ICH. Patients with anticoagulation therapy at the time of onset have been seen to have more hematoma growth and worse outcome (Kuramatsu et al., 2015b). Patients with INR <1.3 4h after onset had less hematoma enlargement versus patients with INR > 1.3 (19.8% vrs 41.5%, p<0.001) (Kuramatsu et al., 2015). Patients with anticoagulants or antitrombotic medicatios are ceased at the occurrence of ICH. Patients with warfarin are administered with prothrombin complex concentrate (PCCs) for fast reversal of anticoagulant effect. Besides infusing clotting factors directly (PCCs), K1-vitamin is given to sustain clotting effects by activating existing clotting factors. In the situation where a patient requires surgical evacuation of hematoma, both medicines have been proven to be both safe and efficient for lowering the risk of catastrofic intraoperative active bleeding (Curtis, Schweitzer, & van Vlymen, 2015). Contrary to reversing anticoagulation therapy, reversial of antiplatelet medication with platelet transfusion has been proven to be associated with poor outcome. In a phase 3 randomized trial (PATCH), 190 ICH patients with prior usage of antiplatelet medication were randomized to receive either platelet transfusion or standard care within 90 minutes of diagnostic brain imaging (Baharoglu et al., 2016). The odds of death or dependency at 3 month were higher in the platelet transfusion group compared to standard care group (OR 2.05, 95% Cl 1.18-3.56, p=0.0114). Platelet transfusion patients suffered more serious adverse effect than standard group (42% vs. 29%). In a meta-analysis reviewing 16 clinical trials, administering platelet transfusion to antiplatelet patients was associated with increased thromboembolic events with no clear beneficial effect on outcome (Brogi et al., 2020).
2.2.6 Surgical treatment
There is contradicting results as to whether surgery has any positive effect in supratentorial ICH. (Table 1) It is thought that if conservatively treated hematoma grow in follow up CT, hematoma evacuation surgery is an option as it would locate the source of bleeding, cauterize it and also treat the “avalanche” effect mentioned earlier. Also, early surgery is thought to diminish expansion and

33
the toxic effect of surrounding edema and normalize perfusion of adjacent brain tissue (Nagasaka et al., 2013). A population based study consisted of 982 patients were conducted to explore whether surgery improve ICH patients outcome (Löppönen et al., 2013). In multivariable analysis, hematoma evacuation via craniotomy seems to lower 3 month mortality compared to those treated conservatively (HR 0.62 Cl; 0.43-0.88, p<0.03). This was apparent especially in subgroup patients of < 70 years and with > 30ml hematoma volume (HR 0.26, Cl; 0.14-0.49, p<0.001). However patients were not randomized and there were clear bias toward younger patient, subcortically situated hematomas in surgical group as these are the factors considered to increase patient outcome. Surgery did not improve patients functional outcome. Because of rather inconsistent results from retrospective studies and smaller randomized studies, a large multicentral international surgical trial in intracerebral heaemorrhage (STICH) randomized study was performed in 2005 (Mendelow et al., 2005). 1033 patients from 27 countries were enrolled to STICH I study from half of which were randomized to surgery and other half were conservatively treated. At 6 months follow up, 26% in surgery group and 24% in conservatively treated group had favorable outcome (p=0.414). Authors concluded that although in subgroup of patients with superficially located hematomas (<1cm from the surface) could benefit from early surgery, overall benefit from surgical evacuation of ICH could not be justified over conservative treatment. Regardless of the considerable sample size of STICH study, it has been widely critisized. Main criticism is that patients recruited to this study are those that neurosurgeon is uncertain of wheather should be treated surgically or medically hence over 3300 patients were excluded from randomization. Quarter of patients initially signed to conservative group were later treated surgically. Emergency surgery lowered these patients mortality rate. However, because they were initially allocated to conservatively treated group, the effect of reduced fatality was registered for medical treatment group. Another criticism is that patients with both superficially and deeply seated hematomas was operated via craniotomy. For deep hematomas such as located in basal ganglia and thalamus, benefit from conventional surgery is diminished because of invasive disruptive nature of functional cortical brain tissue in order to evacuate hematomas. These criticism has led to STICH II study, which analyzed whether concisous patients with superficial lobar intracerebral hematoma of 10-100ml volume could benefit from early surgery (Mendelow et al., 2013). 601 patients were randomized to either early surgery or initial conservative treatment. Follow up rate was 98% achieved at 6 months.

34
Unfavorable outcome occurred 59% in surgery group and 62% in conservative treatment group (p=0.367). A slightly better survival was shown in surgical group as mortality rate at 6 month was 18% in surgery group versus 24% in conservative group (p=0.095). In subgroup analysis, patients with initially thought to be poor prognosis (10x admission GCS–age (years)–0.64 x volume[mL], predefined cutoff; <27,67) were more likely to benefit from early surgery (for favorable outcome: OR 0.49, Cl 0.26-0.92, p=0.02). Although STICH II corrected many issues in STICH I such as including surgery only for patients with superficially located hematomas, it still suffers some flaws. Crossover between groups is still apparent as 21 % of patients initially assigned to conservative group had surgery later in the course of treatment. Majority of these patients had already deteriorated by the time of surgery and had worse neurological deficits than those with initially assigned to early surgery. The crossover to late surgery may have saved these patients life and reduced mortality rate, but because of the intention to treat analysis they remained in the initial conservative treatment group. Another factor that may diminish surgery’s effect is that patients included to this study were at “too good” conditions as all of them were concisous before surgery. As seen in subgroup of patients with pre determined poor prognosis benefit better from early surgery (p=0.03) but this analysis was not prespecified.
After the STICH findings further investigation was warranted as to whether mini-invasive techniques such as endoscopy could bring any advantage versus conventional craniotomy in surgical treatment of ICH. (Table 2) A meta-analysis of 12 high-quality randomized trials was conducted (Zhou et al., 2012). In this meta-analysis, minimally invasive surgery showed improved outcome compared to conventional craniotomy as both dependence and death were reduced (Dependence OR, 0.54, p<0.00001; Death OR 0.53, P< 0.00001) (Zhou et al., 2012). Patients who may benefit most from MIS are age 30-80 years with superficially located hematomas, GCS score over 9, hematoma volume of 25-40ml and within 72 hours after onset of symptoms. Patients who undergoes stereotactic aspiration seems to have better outcome than endoscopic surgery.
Similarly as in STICH trials, MISTIE trial was conducted as international multicentric randomized trial to investigate whether image guided minimally invasive catheter hematoma evacuation followed by rtPA thrombolysis is compared to medical treatment (Hanley et al., 2016). 54 patient were randomized to surgical group and 42 to medicine group. Minimally invasive catheter evacuation and thrombolysis achieved more rapid hematoma volume reduction

35
compared to medicine group. Patients in surgical group also showed better functional outcome at 180 days (mRANKIN <3 was 21% for the medical group and 33% for the MIS group, p=0.05). Reducing remaining clot volume is crucial as each 10ml of addition clot remaining at the end of treatment is associated with a relative reduction in the odds of a good 180 day outcome by almost 50%. Asymptomatic hemorrhage was more common in the surgical group compared to the medical group (22% vrs 7%, P=0.05). There were no difference between groups regarding frequency of serious adverse effect such as symptomatic bleeding, mortality and brain infections. Regardless of its encouraging results, this study suffers from its small sample size and short follow up period. In the endpoint phase III MISTIE trial, with 255 patient allocated to MISTIE group and 251 to medicine group, catheter evacuation and thombolysis did not show any improvement in patient outcome compared to medical treatment at 365 days (mRANKIN 0-3 MIS group 45% vrs medical group 41%, p=0.33) (Hanley et al., 2019). Serious adverse event were more common in surgical group than in medicine group (p=0.012). Although there seems to be a trend for better outcome (mRANKIN <3) in surgical group patients with residual clot volume of less than 15ml, catheter evacuation and clot lysis can not be recommended for routine use. A small randomized trial compared endoscopically treated patients (n = 14) to control group from MISTIE study (Vespa et al., 2016). It showed that endoscopically treated patients had better outcome compared to non surgically treated patients (mRANKIN 0-3; 42.9% vs. 23.7%, p=0.19). Due to its small sample size, no definitive conclusion could be drawn from this.
A large recent meta-analysis involving 2152 patients from 15 high-quality randomized trials, including MISTIE II and ICES (intraoperative stereotactic computed tomography-guided endoscopy surgery) studies showed that minimally invasive surgery was superior compared to other treatment modalities (Scaggiante, Zhang, Mocco, & Kellner, 2018). Minimally invasive surgery (MIS) showed increased chance of independency (2.2 x) and survival (1.7 x) compared to medial treatment. MIS evacuation increased the chance of independency and survival at the follow-up 2.3x and 1.8x compared to craniotomy evacuation. Endoscopic technique demonstrated even better results: 2.5 x increased functional independence and 2.7x increased survival compared to craniotomy. Patients undergoing ultra-early (<24 hours) hematoma evacuation are more likely to regain functional independecy compared to early (<72 hours) hematoma evacuation ( 2.8 times more likely vs. 2 times more likely).

36
Table 1. Large randomized trials comparing craniotomy versus conservative treatment in ICH patients
Trials Surgery (n=number
of patient)
Other treatment
(n=number of
patient)
Outcomes
Mendelow et al., 2005 (STICH I) Craniotomy (468) Medical treatment
(496)
No differences in
outcome
Mendelow et al., 2013 (STICH II) Craniotomy (297) Medical treatment
(286)
Surgery may have
small survival
advantage in
superficial ICH
without IVH
Batjer el al., 1990 Craniotomy (8) Medical treatment
(9)
No differences were
found between
groups
Juvela el al., 1989 Craniotomy (26) Medical treatment
(26)
Mortality was lower in
surgical group
Morgenstern et al., 1998 Craniotomy (7) Medical treatment
(34)
Mortality was lower in
surgical group
Table 2. Large randomized trials comparing minimally invasive technique versus conventional / conservative treatment in ICH patients
Trials Minimally invasive
surgery (n= number
of patient)
Other treatment
(n= number of
patient)
Outcomes
Zhou et al., 2011 Craniopuncture(90) Conventional
craniotomy(78)
Rebleeding was
smaller and
functional outcome
better in MIS group
Sun et al., 2010 Craniopuncture plus
urokinase infusion
(159)
Conventional
craniotomy (145)
Rebleeding and
mortality was lower in
MIS group
Wang et al., 2009 Craniopuncture
(195)
Medical treatment
(182)
Functional outcome
was better in MIS
group
Kim et al., 2009 Stereotactic
aspiration (204)
Medical treatment
(183)
Functional outcome
was better in MIS
group

37
Miller et al., 2008 Endoscopic
surgery(6)
Medical treatment
(4)
Mortality was lower in
MIS group
Cho et al., 2006 Endoscopic surgery
plus stereotactic
aspiration (60)
Conventional
craniotomy (30)
Functional outcome
was better in MIS
group
Hattori et al., 2004 Stereotactic
aspiration (121)
Medical treatment
(121)
Functional outcome
was better in MIS
group
Teernstra et al., 2003 Stereotactic
aspiration (36)
Medical treatment
(34)
A significant
hematoma volume
reduction was
achieved in MIS
group
Auer et al., 1989 Endoscopic surgery
(50)
Medical treatment
(50)
Mortality rate was
lower and functional
outcome better in
MIS group
Feng et al., 2016 Endoscopic surgery
(93)
Conventional
craniotomy (91)
Functional outcome
was better in MIS
group
Zhang et al., 2014 Endoscopic surgery
(21)
Conventional
craniotomy (24)
Functional outcome
was better in MIS
group
Hanley et al., 2016 (MISTIE II) MIS + rt-PA (54) Medical treatment
(42)
MIS group had better
functional outcome
with higher incidence
of asymptomatic
bleeding
Hanley et al., 2019 (MISTIE III) MIS +rt-PA(250) Medical treatment
(249)
Not overall difference
in outcome. MIS
group had better
functional outcome if
residual clot is less
than 15ml
2.3 Infection

38
Numerous studies have found that stroke patients have a increased risk for infectious diseases (Lord et al., 2014; Westendorp, Nederkoorn, Vermeij, Dijkgraaf, & van de Beek, 2011). A meta-analysis comprising all types of strokes found a 30% occurrence of infections, the majority of which were pneumonia and urinary tract infections (Westendorp et al., 2011). Patients suffering ICH will develop infectious disease in 20-50% of cases (Lord et al., 2014; Murthy et al., 2016). Pneumonia is the most common infection in ICH patients, comprising of up to 15-24% of all infections (Lord et al., 2014; Murthy et al., 2016). The second most common infection is urinary tract infection which has been found in 7-16% of all ICH patients (Lord et al., 2014; Murthy et al., 2016). Others comprised sepsis, multiple infections and surgical site infections (Lord et al., 2014; Murthy et al., 2016; Divani et al., 2015; Saloheimo, Lapp, Juvela, & Hillbom, 2006; Ohwaki, Yano, Nagashima, Nakagomi, & Tamura, 2008; Westendorp et al., 2011).
Patients with ICH tend to have some degree of neurological deficiency which affects their mobility. It is speculated that immobilization can increase the risk of infectious disease. This can be seen especially in patients with a larger volume of ICH and lower GCS-score at onset that are more prone to be bedridden in the course of ICH treatment period (Lord et al., 2014). Intubation itself with prolonged immobilization carries a greater risk of respiratory infections (Divani et al., 2015). Patients with lower consciousness upon admission might also suffer unnoticed aspiration that may lead to the development of pneumonia, which itself may cause respiratory distress, prolonging intubation and ICU-stay. Post ICH pneumonia may result from aspiration caused by impaired consciousness or reduced bulbar reflexes with consecutive oropharyngeal dysphasia (Ionita et al., 2011 ;Sykora et al., 2011). A further explanation for post-ICH infection is immunosuppressive syndrome (Sykora et al., 2011). There is an increasing amount of data from animal models and human research that shows stroke and ICH induce immunodeficiency via hypothalamus-pituitary axis and sympathetic nervous system activation (Prass et al., 2003; Meisel, Schwab, Prass, Meisel, & Dirnagl, 2005). After brain injury catecholamine surge is present. The extensive activation of sympathetic innervations of the immune system organs and the presence of adrenergic receptors on lymphocytes and neutrophiles results in leukcocyte depletion, reduced NK-cell activity and decreased HLA –DR expression on monocytes (Klehmet et al., 2009; Prass et al., 2003; Urra et al., 2009). Thus enhanced sympathetic activation results in suppressed immune function and may be a key factor in post-stroke infections.

39
As shown in a prospective ERICH study, hematoma volume increases the risk of infection OR 1,02 per ml, 95% Cl 1,01-1,03 (Lord et al., 2014). Thromboembolic events are also risk factors for post ICH infections. Besides immobilization that follows DVT, it has been hypothesized that DVT is associated with infection, probably due to fever response from DVT-prompted infectious investigation (Lord et al., 2014). Other factors correlating with infection are IVH, EVD, craniotomy, central venous and urinary catheters, nasogastric feeding (Lord et al., 2014 ;Ohwaki et al., 2008).
Patients with ICH are more prone to require different catheters, which by itself increases the risk of bacterial colonization. A urinary catheter is inserted in ICH patients with limb paresis and low consciousness. From the catheter route, bacteria can make its way to the urinary tract system, causing urinary tract infections in ICH patients. Dysphagia and pulmonary edema may lead to PEG and intubation, which itself increases the risk of respiratory infections (Lord et al., 2014).
2.3.1 Infections and outcome
Infectious diseases affect ICH patient outcome and prolongs hospital stays has been proven in many studies (Lord et al., 2014; Murthy et al., 2016 ;Divani et al., 2015; Saloheimo et al., 2006). It is estimated that nosocomial pneumonia in ICH patients increases hospital stay from 4 to 20 days (p<0,0001) (Divani et al., 2015). Infectious disease is an independent factor to predict longer ICU stays even after taking into account other known variables such as age, GCS score and surgical procedures (p<0,001) (Ohwaki et al., 2008). Mortality has been found to be higher in patients with infection compared to no infection (16% vrs 8%, p=0,001) (Lord et al., 2014; Westendorp et al., 2011). In ERICH study respiratory infection was found to increase patient risk for poor outcome more than UTI (OR 4,0 95%, Cl 2,3-7,3 vrs OR 1,7 95% Cl 1,1-2,8) (Lord et al., 2014).
Since infectious disease prolongs hospital stay and lowers patient outcome in ICH patients, it has been hypothesized whether prophylactic antibiotics have any role in improving overall dim outcome in ICH patients. In a randomized, double-blinded, placebo-controlled trial with 80 patients suffering stroke was conducted,

40
patients received either intravenous moxifloxacin (400mg daily) or placebo for 5 days. Prophylactic antibiotic reduced infection rates significantly compared to the placebo group (17.1% versus 41.9%, P=0.032). However, there were no significant differences in overall outcome or mortality between the two groups (Harms et al., 2008).
Based on the theory of immunodepression syndrome after stroke, in animals various bacterial infections can be prevented using beta-blockers (Prass et al., 2003). Very few human trials have been carried out concerning this subject. One small retrospective trial showed that stroke patients with beta-blocker treatment had reduced pneumonia after stroke compared to those without beta-blockers (Dziedzic, Slowik, Pera, & Szczudlik, 2007). Usage of betablocker in this study reduced 30-day mortality rate compared to those not treated with betablockers (6.8% vs. 19.0%, p<0.01). However most of this effect is mediated through cardiovascular diseases.
2.3.2 Role of CRP
CRP is produced by hepatocytes in response to cytokines such as interleukin. CRP has also been found to be elevated in ischemic cardiovascular events (Lowe et al., 2004). In the event of ischemic stroke, high CRP-level was associated with severity of stroke (p=0,02) and a higher mortality rate (p<0,002) (Idicula, Brogger, Naess, Waje-Andreassen, & Thomassen, 2009). In subarachnoidal hemorrhage patients, high admission CRP-level has been seen to correlate with poor outcome (Juvela, Seppo, Kuhmonen, & Siironen, 2012). It is not clear how CRP-level correlates with patient outcome in the setting of intracerebral hemorrhagic events. Elevated CR-protein has been found in the tissue surrounding intracerebral hematomas (Di Napoli et al., 2012). Theoretically it can be a sign of larger cerebral tissue damage and thus correlate with poor outcome. In a paper by Diedler et al, maximal CRP level seems to correlate with poor long term functional outcome in ICH patients (Diedler et al., 2009). In this series higher CRP levels were associated with infectious diseases such as pneumonia and urinary tract infections (156mg/dl and 78,8mg/dl respectively). However, it is not clear whether the high admission CRP level predictive value of outcome in ICH patients is based on their infectious disease, or itself predicts poor outcome irrespective of other causes.

41
2.4 Seizures
2.4.1 Definition
Seizures are defined as excessive or synchronous neuronal activity on the brain resulting in transient neurological signs and/or symptoms (Fisher, R. S. et al., 2014). Immediately after ICH the mechanism behind seizure is contributed by mass effect, edema, focal ischemia and blood products. On the later course of ICH, scarring of brain tissue occurs and with irritability of cerebral neural tissue increases the risk of seizures. Most seizures occur during the first 1-3 days of onset due to possible hematoma enlargement and neuronal irritation from cortical ICH (Bladin et al., 2000; Neshige et al., 2015; Vespa et al., 2003).
2.4.2 Classification of seizure types
Classically post stroke seizures are classified as immediate seizure when it occurres within 24 hours of onset. Cutoff for early and late seizure is arbitrary between 1 day to 1 month from ICH onset (Neshige et al., 2015a ;Passero, Rocchi, Rossi, Ulivelli, & Vatti, 2002). Recurrent seizure is defined when epileptic seizure occurs at least, 1), one month after onset of initial seizure or, 2), two or more seizures occur more than 1week after ICH and the time between the initial and recurrent seizure is over 1 week (Neshige et al., 2015).
2.4.3 Incidence of seizures
The incidence of different types of seizures varies a lot depending on the definition of different seizure types (Bladin et al., 2000; De Reuck, Hemelsoet, & Van Maele, 2007; Lamy et al., 2003; Lossius, Rønning, Slapø, Mowinckel, & Gjerstad, 2005; Neshige et al., 2015). 2.7%-18.7% of patients with ICH suffer

42
some kind of seizure at some point (Andaluz & Zuccarello, 2009; Bladin et al., 2000; De Reuck et al., 2007). Immediate seizures occur in 7% (De Herdt et al., 2011). Incidence of early seizure is 4.3-14% and late seizure 2-26,9% (Andaluz & Zuccarello, 2009; Bladin et al., 2000; De Reuck et al., 2007). 2-28% of patients after initial seizure will experience recurrent seizures during hospitalization (Bladin et al., 2000; De Reuck et al., 2007).
Multiple studies have demonstrated that cortical lesion, volume of hemorrhage/stroke and severe neurological deficiency are risk factors for post-ICH seizure occurrence (De Herdt et al., 2011; Garrett et al., 2009; Neshige et al., 2015b). Cortical lesion being the most potent risk factor increasing over 7-fold the risk of seizure occurrence after ICH (Neshige et al., 2015). Large hematoma volume is one of the few risk factors for recurrent seizures probably due to extensive irreversible cerebral neural injury (Neshige et al., 2015). A history of alcohol abuse has been seen in many studies to correlate strongly with the occurrence of seizures after ICH (Goswami, Karmakar, & Ghosh, 2012; Madžar et al., 2014). In the subgroup of lobar location of ICH, pre-stroke alcohol usage has been seen to increase post stroke seizures 5 fold (95% Cl 1,25-21,78) (Madžar et al., 2014). A possible mechanism behind this could be that long-term alcohol consumption lowers the seizure threshold and metabolized blood product breakdown increases neuronal irritation (Bråthen, Brodtkorb, Helde, Sand, & Bovim, 1999; Hillbom, 1980; Madžar et al., 2014). Infectious disease such as sepsis may facilitate seizure occurrence through septic encephalopathy (Madžar et al., 2014; Oddo, Carrera, Claassen, Mayer, & Hirsch, 2009). Certain antibiotics such as cephalosporin and penicillin administered for sepsis, have also been reported to lower the seizure threshold and provoke epileptic seizures in this subgroup of ICH patients (Grill & Maganti, 2011; Madžar et al., 2014).
2.4.4 Treatment of seizures
Patients with impaired consciousness in the setting of especially non- expansive hematoma should be suspected of epileptic seizures. Continuous -EEG should be performed at ICU setting. If patient do not regain conciousness with first two line of AED treatment, sedation and 12-24h burst suppression shoud be initiated. Treatment algorithm is described in detail at figure 5.

43
Fig. 5. Treatment algorithm for acute epileptic seizure. Table modified from its original source (Trinka & Kälviäinen, 2017).
2.4.5 Prophylactic anti-epileptic drugs
The effect of prophylactic AED on preventing seizures and improving ICH patient outcome varies in different publications (Gilmore, Choi, Hirsch, & Claassen, 2010; Messé et al., 2009a; Neshige et al., 2015; Passero et al., 2002; Reddig, Nixdorf, & Jensen, 2011). Passero et al. showed that prophylactic AED reduced clinical seizures in patients with lobar ICH (Passero et al., 2002). However, multiple other studies were not able to show the same effect (Messé et al., 2009; Naidech et al., 2009; Reddig et al., 2011). Also, the majority of studies have not been able to show that prophylactic AED has any effect on overall patient morbidity and mortality (Andaluz & Zuccarello, 2009; De Herdt et al.,

44
2011; De Reuck et al., 2007; Szaflarski et al., 2008). Furthermore, a large retrospective study with a total of 1920 consecutive patients did not show any effect of prophylactic AED preventing recurrent seizures (Neshige et al., 2015). In a subgroup of patients with lobar ICH and/or alcohol abuse, there might be some positive effect with prophylactic AED, as both risk factors are independent predictors for epileptic seizure in stroke patients (Madžar et al., 2014). In a clinical trial cohort of 295 patients, prophylactic AED use was associated with poor outcome (OR 6.8; 95% Cl: 2.2-21.2, P=0.001) after taking into account other known factors affecting outcome (Messé et al., 2009). However most of the AEDs used in this study is phenytoin, so negative result from this study can’t be generalized to all antiepileptic drugs. Based on the available literature, American guidelines conclude that prophylactic AED is not to be recommended (Hemphill et al., 2015). Lacking level 1 RCT studies, European guidelines concluded that there is not sufficient evidence to make a strong recommendation on whether prophylactic AED should be used after ICH for the prevention of seizures (Steiner et al., 2014).
2.4.6 Effect on outcome
Whether epileptic seizures affect outcome remains unknown and research has shown contradictory results. In a prospective cohort study, including 3216 patients with ICH, the presence of seizure was associated with atrial fibrillation (p=0.004), pneumonia (P=0.001) and poorer functional outcome at 12-month (p=0.001) follow up (Li, Z. et al., 2015). Six month mortality was also higher if seizure occurred after ICH onset (P=0.005) (Li et al., 2015). A retrospective study with 464 patients found that functional outcome was slightly worse if patients suffered seizure post-ICH (P=0.059) (Madžar et al., 2014). This however didn’t achieve statistical significant. Majority of the studies comes to a conclusion that although post stroke epileptic seizure may have a slight trend toward poor functional outcome, it is not statistically significant when taking account of all other risk factors (Andaluz & Zuccarello, 2009; Bladin et al., 2000; Claessens et al., 2017; De Herdt et al., 2011; Mullen, Kasner, & Messé, 2013).

45
2.5 Thromboembolic complications
2.5.1 Pathophysiology of venous thrombotic events
Lower limb deep vein thrombosis (DVT) affects 1-2% of hospitalized patients (Line, 2001). Worldwide around 10 million patients suffer venous thrombotic event (VTE) every year, thus being the third largest vascular disease after myocardial infarction and stroke (Di Nisio, van Es, & Büller, 2016). People over 45 years of age and black people appear to be at higher risk of DVT (Di Nisio et al., 2016). The cause of thrombus formation relies on the unique venous valve structure as it encourages thrombus formation together with low intraluminal pressure (Line, 2001). Normally small thrombus deposits are formed and washed away by the compressing force of muscles surrounding the vessels. However, especially in an immobilized state and hospitalized patients, vascular compression effect in lower limb muscles does not occur. This may lead to thrombus formation at the lower limb deep veins.
Symptoms caused by DVT are mediated via the obstruction of venous outflow, vascular inflammation and pulmonary embolization. When venous thrombi dislodge from its initial site in the pelvic or lower limb vein, moving to respiratory circulation and most commonly affect the pulmonary vessel, extremely large emboli can in rare cases clot the pulmonary artery (Goldhaber, 2004). Pathophysiological effects following pulmonary vessel embolus are increased pulmonary vascular obstruction, impaired gas exchange caused by increased alveolar dead space, hypoxemia and impaired transfer of carbon monoxide (Goldhaber, 2004). This may all result in lung edema, lung hemorrhage and, depending on the size of embolus, right ventricular dysfunction causing cardiac failure and sudden death (Goldhaber, 2004).
2.5.2 Diagnosis of deep venous thrombotic events
Over 70% of symptomatic pulmonary embolism is related to DVT (Di Nisio et al., 2016). The majority of morbidity and mortality from DVT is explained by PE complications. With a mortality rate of 17.4-28% VTE is a life-threatening

46
disease and crucial to recognize in clinical work (Goldhaber, 2004). Both DVT and PE can be notoriously asymptomatic and difficult to detect. Diagnosis for DVT is made by clinical findings and radiological imaging. Patients with tenderness of the calves, swelling and presence of collateral veins should be suspected of having DVT. In patients with no known risk factors D-dimer is obtained. If its value is high, compression ultrasonography should be performed. In hospitalized patients, especially with recent surgery or comorbidities, D-dimer sensitivity is quite low and a radiological method such as ultrasound is preferred as the first line diagnostic tool. Normally veins completely collapses when pressed upon, but if thrombus is formatted inside the lumen it prevents it from collapsing when compressed (Line, 2001).
2.5.3 Diagnosis of pulmonary embolism
Symptoms from PE can be quite subtle and be masked behind comorbidities such as heart disease or pneumonia. Classical symptoms, such as short of breath and hypoxemia, can be a cause of various diseases (Goldhaber, 2004). However, patients with a long period of immobilization and known DVT should prompt further investigation for PE if pulmonary symptoms or hemodynamic problems occur. Initial testing such as electrocardiogram is useful to exclude other diseases and in large PE pulmonary hypertension and the right ventricular signs can be detected using ECG. PE can cause hypoxemia in arterial gas testing but it has been shown that 20% of angiographically proven PE patients have normal arterial oxygen results (Stein, P. D., Goldhaber, & Henry, 1995). Normal D-Dimer has a very high negative value for excluding PE in low-risk patients. However high D-dimer is not only specific for PE as myocardial infarction, sepsis, pneumonia and cancer may also elevate it (Goldhaber, 2004). If PE is suspected, the first line radiological diagnostic tool is CT pulmonary angiography (CTPA) (Di Nisio et al., 2016).

47
2.5.4 General treatment of venous thrombotic events
When VTE is diagnosed, anticoagulation is started for at least 3-6 months depending on the patient’s individual risk profile for hemorrhagic complications and recurrence of embolic event (Goldhaber & Bounameaux, 2012). During the acute phase, subcutaneous low-molecular weight heparin (LMWH) or unfractionated heparin is administered with oral anticoagulation until international normalized ratio (INR) is 2-3. After INR is repeatedly above 2, LMWH is discontinued and continued with solely oral anticoagulation (Di Nisio et al., 2016). In the setting of unstable hemodynamic, patients with large PE can be considered for possible thrombolysis with i.v. heparin and thrombolectomy (Goldhaber & Bounameaux, 2012 ;Di Nisio et al., 2016).
2.5.5 Thrombosis treatment in ICH patients
The prevalence of symptomatic venous thrombosis in stroke patients is established around 0.5-2.9% (Goldstein, Joshua N. et al., 2009; Skaf et al., 2005; Zeng, Hu, & Zhang, 2015). Intracerebral hemorrhage event poses a clinical challenge for VTE treatment. On the other hand, it is known that ICH patients are at greater risk of VTE because of immobilization caused by neuronal damage, resulting limb paresis and also when surgery is imposed on these patients. However, because of active intracranial bleeding anticoagulation is contra-indicated in the acute phase of treatment. In the event of thrombosis, LWMH has established a lower risk profile than conventional anticoagulant and is therefore more preferable as an acute phase treatment in ICH patients. Vena cava filter is considered instead of anticoagulation if in patient follow-up CT reveals hematoma enlargement indicating active bleeding and/or with a risk of recurrent pulmonary embolism (Di Nisio et al., 2016). In the acute phase of ICH, thrombolysis should be avoided as it increases the risk of hematoma enlargement.

48
2.5.6 Resuming anticoagulation after ICH
The incidence of ICH varies 0.6% to 1.0% annually, when a patient is on anticoagulant therapy (Becattini, Sembolini, & Paciaroni, 2016). It is not well known whether resuming anticoagulation therapy after ICH increases the risk of recurrent hematoma. Combining the possible theoretical risk of hematoma recurrence after resuming anticoagulation post-ICH and the fact that anticoagulation worsens ICH outcome, protocols for anticoagulation resumption after ICH vary to a large extent.
There are risk assessment scores such as the HASBLED-score to assess the risk of major bleeding after resuming anticoagulants (Table 3). The HASBLED score takes account of hypertension, renal/liver function, stroke, bleeding history, INR, elder age, drugs/alcohol concomitantly (Roldán et al., 2013). It has seen that when assessing the bleeding profile in patients with anticoagulants for VTE, HASBLED >3 are at increased risk of major bleeding events (OR: 13.05, 95% CI: 0.96-692.58, P=0.028) compared to patients with a HASBLED-score of less than three (Rief et al., 2018). However, its sensitivity in the setting of ICH is controversial. In multiple studies a HASBLED- score of over 3 has indeed shown increased risk of ICH recurring, but as the score rises it also predicts more thromboembolic complications as many of the variables in HASBLED is similar as in CHA2DS2 -VASc score (Table 3) (Hylek, Evans-Molina, Shea, Henault, & Regan, 2007; Poli et al., 2007).
CHA2DS2 -VASc score is usually utilized to assess a patient’s individual thromboembolic risks (Table 3) (Becattini et al., 2016). A patient with a CHA2DS2
-VASc score of 0-1 is considered a low-risk patient, whereas CHA2DS2 -VASc >2 are considered high-risk for later thromboembolic events (Becattini et al., 2016). Patients with a prosthetic heart valve are at greater ischemic risk of VTE compared to atrial fibrillation (AF), 4% vs 0.8% (Becattini et al., 2016). There are no prospective studies to evaluate the long-term effect of the cessation of anticoagulant therapy after ICH. In retrospective studies, there seems to be a significantly lower incidence of ischemic event and lower mortality rate in ICH patients resuming anticoagulant compared to patients with cessation of anticoagulant after ICH event (Nielsen et al., 2015; Witt et al., 2015). There is a trend that resuming anticoagulant after ICH increases the risk of recurrent hematoma, but this was not statistically significant (p=0.48) (Becattini et al., 2016).

49
Based on the above data, AHA/ASA guideline has recommended that patients with a prosthetic heart valve have an absolute indication for resuming anticoagulation as soon as possible (Hemphill et al., 2015). The risk of ischemic events after cessation of anticoagulants for 1-2 weeks has been found to be low (Becattini et al., 2016). Balancing the risk of ischemic events and the risk for recurrent ICH, it seems reasonable to resume full dosage of anticoagulants 2 weeks from ICH onset for prosthetic valve patients (Kuramatsu et al., 2015). Non- valvular AF Patients with lobar ICH with no previous ischemic events, long-term anticoagulation should be avoided (Hemphill et al., 2015). For AF patients, anticoagulation can be also considered, particularly with high risk patients, for prevention of thromboembolic events (Becattini et al., 2016; Murthy et al., 2017). Current AHA/ASA guidelines recommend avoidance of anticoagulants for at least 4 weeks after the onset of ICH in AF patients (Hemphill et al., 2015). Heparin can be administered as thrombosisprophylaxis before resuming full dosage of anticoagulation 3 days after ICH onset with a low risk of rebleeding (Becattini et al., 2016).
Table 3. CHA2DS2 -VASc and HASBLED score
CHA2DS2-VASc Score HAS-BLED Score
Congestive heart
failure
1 Hypertension 1
Hypertension 1 Abnormal renal/liver function 1 or 2
Age ≥ 75 years 2 Stroke 1
Diabetes melitus 1 Bleeding tendency 1
Stroke/TIA 2 Labile INR 1
Vascular disease 1 Age > 65 years 1
Age 65-74 years 1 Drugs (ASA or NSAID) or alcohol 1 or 2
Female gender 1
Maximum score 9 9
2.5.7 Thrombosisprophylaxia in intracerebral hemorrhage patients
The efficiency and safety of mechanical DVT prophylaxis, such as intermittent pneumatic compression device (IPC), is well established in many studies (Dennis

50
et al., 2013; Lacut et al., 2005; Zeng et al., 2015). By compressing lower limbs in interval fashion and increasing venous blood flow, it has been shown to significantly reduce the incidence of VTE, especially when combined with LMWH (Lacut et al., 2005; Lewis et al., 1976; Zeng et al., 2015). IPC has been seen as a relatively safe method with rare adverse effects. Both European and AHA/ASA guidelines recommend using IPC for thrombosis prophylaxis in ICH patients (Hemphill et al., 2015; Steiner et al., 2014).
In multiple retrospective studies, there seems to be a trend that administering heparin (unfractioned or low molecular) decreases the risk of VTE with no significant risk of hematoma enlargement or rebleeding (Kiphuth, Köhrmann, Huttner, & Schellinger, 2009; Orken et al., 2009; Tetri, Hakala et al., 2008). One shortcome in these studies is that they often included other causes of ICH (Cavernoma, AVM). In addition, the time from ICH onset to anticoagulation varies considerably. No large randomized controlled trial has been carried out on this subject. An early study by Dickman 1988 included 46 patients, half of which received heparin (3 x 5000 unit /d) 4 days after ICH and the other half 10 days after ICH. The trial, however, is not inclusive of primary ICH but also included secondary causes of ICH such as cavernomas and AVM (Dickmann et al., 1988). Thromboembolic events occurred in 18 patients and fourteen of them had PE. They did not find any increased risk of rebleeding in the early heparinized group, neither were there any differences in the outcome. In 1991 Boeer added 22 patients to this trial to receive heparin as early as 2 days after ICH onset (Boeer, Voth, Henze, & Prange, 1991). They also found no difference in rebleeding or hematoma enlargement between the groups. However, patients receiving heparin 2 days after onset showed significantly less PE (1,5%) compared with later groups (22% and 39% respectively). The largest RCT to date was carried out by Orken and included 75 patients. In this trial patients were randomized into two groups; 39 of them received enoxaparin 40mg/d s.c. 48 hours after ICH onset and 36 patient only received long compression socks (Orken et al., 2009). No hematoma growth was observed in either group. 4% had symptomatic DVT in the LMWH group. No differences was found between groups in VT events. It concluded that administering enoxaparin is relatively safe in the setting of ICH.
Due to the lack of a large RCT on thrombosisprophylaxis in ICH patients, European guidelines could not make any strong recommendation as to when to administer anticoagulation for thrombosisprophylaxis (Steiner et al., 2014). Recent American guidelines (2015) have stated that based on small RCT, mentioned earlier, it seems to be relatively safe to administer LMWH 1-4 days

51
after ICH onset (Hemphill et al., 2015). On the basis of current data, the optimal guidance for a clinical decision on the subject remains unclear. Due to the lack of any strong recommendation as to when thrombosis prophylaxis should be administered, clinicians are reluctant to start any anticoagulation in fear of hematoma enlargement. In a US based analysis, less than 20% of ICH patients are on any thrombosisprophylaxia (Prabhakaran et al., 2015). Patients are therefore submitted to unnecessary thrombotic events due to inadequate thrombosis prophylaxia, which worsens ICH patients’ already dim outcome. High quality randomized double blinded studies are required to give more information as to when it is safe to administer anticoagulation in ICH patients.
2.6 Cardiac complications
2.6.1 Myocardial infarction
Patients with stroke or intracranial hemorrhage are at risk of acute myocardial infarction (AMI) due to either exacerbation of underlying coronary disease or interval development of stress-induced myocardial injury (Alqahtani et al., 2017). Although only 0.3- 1.6% of all stroke patients develop AMI during their hospital stay, mortality increases 3-fold compared to those without AMI (Alqahtani et al., 2017; Gattringer et al., 2014). Patients suffering AMI also had a higher incidence of pneumonia and progressive stroke. Older patients, those with a history of coronary disease, renal insufficiency and previously documented arrhythmia are at increased risk of in-hospital AMI for stroke patients (Alqahtani et al., 2017). Treatment for AMI in stroke and ICH patient poses a clinical dilemma. There is no convincing data nowadays as to how to optimally treat acute ICH patients with AMI. Although PCI has shown to be associated with lower mortality in ischemic stroke patient suffering AMI (p<0.001), it is rarely performed for stroke patients (2%) in fear of perioperative complications and hemorrhagic complications following antithrombotic medications (Alqahtani et al., 2017). In a large retrospective study consisting of 13573 ischemic stroke patients who subsequently suffered AMI, PCI procedure followed by antithrombotic medication did not increase the risk for hemorrhagic complication compared to those without PCI (Alqahtani et al., 2017).

52
2.6.2 Neurogenic stunned myocardium
A well-known cardiac complication after stroke is reversible left ventricular dysfunction or better known as neurogenic stunned myocardium (NSM). NSM is pathognomic in stroke and intracranial hematoma patients that have suffered autonomic dysregulation from a hypothalamus injury (Alqahtani et al., 2017; Kerro, Woods, & Chang, 2017; Temes et al., 2010). In patients with NSM, instead of atherosclerosis clotting the cardiac vasculature, excessive catecholamine surge leads to myocardial injury (Alqahtani et al., 2017; Kerro et al., 2017; Temes et al., 2010). Although left ventricular dysfunction and cardiomyopathy is usually reversible in NSM, it can sometimes result in pulmonary edema, heart failure, arrythmia and myocardial infarction (Kerro et al., 2017). Takotsubo cardiomyopathy has the same pathophysiology and presentation as NSM, but instead of global hypokinesis of NSM, in takotsubo regional apical hypokinesis occurs. Both are a subgroup of stress-induced cardiomyopathy (Guglin & Novotorova, 2011).
There is no specific diagnostic tool for NSM. Symptoms are quite similar to traditional AMI; shortness of breath, arrhythmias and chest pain. An above normal troponin level does not by itself indicate AMI, as in the setting of stroke cerebral tissue injury can also elevate troponin enzymes (Ahmadian et al., 2013; Hays & Diringer, 2006). Compared to traditional atherosclerosis AMI, in NSM troponin levels do not usually rise as high as in traditional AMI. Higher troponin levels have been found in several papers to be independent risk factors of mortality after stroke and ICH (Ahmadian et al., 2013; Garrett et al., 2010; Hays & Diringer, 2006). In NSM, ECG changes are non-specific. The most common ECG changes in NSM are tachycardia, repolarization and prolonged QTc interval (Ahmadian et al., 2013; Kerro et al., 2017).
Although it mimics AMI, the same treatment protocol does not apply in NSM. Treatment for NSM consists of hemodynamic support along with administering inotropen medicine such as doputamine and milrinone. Intra-aorta pump is sometimes utilized with patients in cardiogenic shock (Kerro et al., 2017). It is also important to recognize patients with NSM from an elevated

53
troponin level as it may increase the likelihood of later development of hemodynamic and cardiopulmonary problems, especially in patients undergoing surgery (Garrett et al., 2010).
2.6.3 Atrial fibrillation
Atrial fibrillation (AF) is rather common among patients with ICH. Approximately one third of ICH patient have AF during the 3-month follow up (Horstmann, S. et al., 2014). Although in multivariable analysis, AF does not seem to correlate with mortality in ICH patients, it is however correlated with ischemic events post ICH. However, it has been problematic for clinicians to decide whether it is safe to start oral anticoagulation (OAC) in newly diagnosed AF in the setting of post-ICH. It has been shown that clinicians are reluctant to start OAC even in the setting of increased ischemic complications (CHA2DS2 -VASc score >2) (Horstmann et al., 2014). HASBLED score has been used to evaluate individual risk of hemorrhagic complications, although the score has not been validated for recurrent ICH and does not take into account possible vascular pathologies such as cerebral amyloid angiopathy (CAA) (Horstmann et al., 2014). It has been suggested that ICH patient should be considered with OAC for newly developed AF, if they have a low HASBLED score, CHA2DS2 -VASc >2 and with no sign of amyloid angiopathy in MRI (Horstmann et al., 2014). NOAC (new oral anticoagulation) and left atrial appendage closure (LAAC) represent an interesting new frontier in AF patients with a history of ICH. Studies have shown that NOAC reduces the risk of ICH over 50% compared to conventional anticoagulation (Becattini et al., 2016; Murthy, Gupta et al., 2017). The mechanism behind it may be its lower suppression on thrombin generation and reduced penetration of the blood-brain barrier making it the optimal choice for ICH patients with AF (Becattini et al., 2016). In atrial fibrillation patients with prior ICH and a high risk of stroke, LAAC could be considered in selected cases to avoid the risk of hemorrhagic complications from anticoagulations (Fayos-Vidal et al., 2017; Horstmann, Solveig et al., 2014; Li, X. et al., 2016; Nielsen-Kudsk et al., 2017; Renou et al., 2017). It has been seen to be an effective and safe method for preventing stroke (Fayos-Vidal et al., 2017; Horstmann et al., 2014; Renou et al., 2017). In a large meta-analysis consisting of total 87831 patients, LAAC was compared to conventional anticoagulation and NOAC

54
(Sahay et al., 2017). LAAC is more efficient in preventing stroke (HR 0.44, 95% Cl 0.23-0.86, p=0.017) and death (HR 0.58, 95% Cl 0.37-0.91, p=0.0018) than warfarin in AF patients. It is comparable to NOAC in preventing stroke and mortality. It shows similar or less bleeding profile than NOAC (0.80, 95% Cl 0.33-1.94, p=0.615).

55
3 Aims of the research - Are elevated CRP levels on admission (<24 hours after ictus) associated with an unfavourable outcome in ICH patients? - Which factors predict immediate, early and late seizures in ICH patients? - How do seizures affect a ICH patient’s outcome and the occurrence of infectious and thromboembolic complications? - Does early (24 hours after onset) medical thrombosis prophylaxis increase hematoma enlargement in ICH patients? - Does late (72 hours after onset) medical thrombosis prophylaxis increase thrombosis events in ICH patients?

56
4 Methods
4.1 Population based cohort (I-II)
4.1.1 Clinical data - Study I
For the first two publications, we formed a registration of all pICH patients treated at Oulu University Hospital from January 1, 1993 to December 31, 2008. The hospital is the only one in northern Finland serving acute stroke patients and had a catchment area of 356,026 in 1993 and 389,671 in 2008. Altogether 961 patients with first-ever pICH were identified. Six patients died before reaching the hospital, the diagnoses were confirmed by autopsy. We excluded ICH caused by trauma. Vascular anomalies and tumors were identified and excluded by CTA / DSA / MRI.
For the first study, from the 961 patients we excluded patients whose first CRP levels were measured late ( >24 hours from onset). We included 114 patients who underwent surgery, except for 6 of them whose CRP levels were not obtained before surgery. Hematoma evacuation surgery were done either via burrholes or craniotomy. Data were collected on the additional need for external ventricular drainage (EVD). No patients were treated with decompressive craniectomy or neuroendoscopic surgery. A total of 807 patients (84%) were included in the first study.
Patients’ clinical condition was assessed utilizing the Glasgow Coma Scale (GCS) score. CRP blood test was obtained in the emergency room upon patient arrival at the hospital or the next morning in the hospital ward. During hospitalization, CRP – values were measured on a daily basis. CRP was analyzed using turbidimetric method (normal values < 10 mg/L, coefficient of variation < 6%; Siemens Activa). The patient’s history, comorbidities, blood pressure history, use of anticoagulants and other medications were extracted from hospital records. The patients were considered to be hypertensive if their blood pressure readings preceding the index stroke had repeatedly exceeded 160/90 mm Hg, in accordance with the WHO/ISH (World Health Organization/International Society of Hypertension) statement or if they were taking antihypertensive medication (Whitworth et al., 2003). Patients were recorded as having diabetes mellitus if they were taking oral hypoglycemic agents or insulin. Cardiac diseases included

57
myocardial infarction, coronary artery disease, heart failure, and/or atrial fibrillation.
4.1.2 Clinical data - Study II
The clinical data was collected as same as described in study I. Patients’ usage of antiepileptic drugs (AEDs) and occurrence of first epileptic seizures were collected for all patients up to December 31, 2008. We excluded 25 patients with known previous epileptic seizures. From 935 patients that did not have previous seizures, we identified 130 patients that had their first seizure after ICH. Alcohol consumption was well-defined, and this data was collected from the patient and/or their relatives. Recent heavy drinking was defined as the weekly ingestion of at least 300g of ethanol during the month preceding the stroke. Patients are registered as having seizures if they developed their first seizures after stroke and having a need for AEDs or sedatives. Seizures are categorized as immediate if they had seizure within 24h of admission, early if they had a seizure >24 h but <2 weeks after ictus, and late if they had seizures >2weeks after admission. The use of AEDs before and after seizures was collected from hospital records.
4.1.3 Neuroradiological methods
Primary ICH was diagnosed with a CT scan obtained on admission. It was examined by an experienced neuroradiologist. The location and the presence of intraventricular hemorrhage was recorded. The measurement of ICH volumes was performed either with a sum of individual slice volumes2 or with an easier ABC/2 method (Kothari et al., 1996). The presence of IVH was dichotomized (yes or no). If secondary causes such as aneurysm, malformations and tumors are suspected, then a CTA, MR and/or DSA was performed immediately. Structural abnormalities were also checked at late follow-up imaging (CT/MRI) at 2-3 months after ictus.

58
4.1.4 Outcome measurements
Death records were obtained from the Causes of Death Register and were checked for the entire patient series. Patients were followed up for 3 months at our out-patient clinic or on the hospital’s rehabilitation ward, with the exception of some who showed exceptionally good recovery on discharge and were assumed to have maintained this state for at least 3 months unless they were readmitted. All patients who experienced deterioration or rebleeding were readmitted to our hospital. The outcome was assessed according to the Glasgow Outcome Scale (GOS); In study I, patients with a score of 5 (good recovery) were considered to have a favourable outcome, whereas patients with scores of 1–4 (death, persistent vegetative state, or severe or moderate disability) were considered to have an unfavourable outcome (Jennett et al., 1975). In study II, patients with GOS score of 4-5 (moderate disability or good recovery) were in favourable outcome group and GOS 1-3 (death, persistent vegetative state or severe disability) were in unfavourable outcome group.
4.1.5 Statistical methods
Data was analyzed using IBM SPSS Statistics for Windows (version 20.0, IBM Corp.). Categorical variables were compared by conventional statistical methods including Pearson’s chi-square test and Fisher’s exact test, and continuous variables were compared by t-tests, the Mann-Whitney U-test, a 1-way ANOVA, and/or the Kruskal-Wallis test for nonparametric ANOVA. Uni-variate associations between continuous variables were tested using Spearman rank correlation coefficients (rs). Predictors of an unfavourable outcome 3 months after primary ICH were searched for using unconditional logistic regression. Maximum-likelihood forward-elimination procedures were used, with the variables selected on the basis of their probability values (p < 0.05). The following variables were tested: sex, age, presence of cardiac disease, presence of diabetes mellitus, hypertension, AMI, VTE, hematoma size (per ml), GCS score (per unit), IVH, subcortical hematoma location, hematoma evacuation, use of warfarin, prior ischemic stroke and CRP level (per 10 mg/L) on admission. For study II, heavy drinking, infectious complications, seizures were also included in

59
analysis. All significant predictors found in stepwise logistic regression were included in the final model. A 2-tailed p value < 0.05 was considered statistically significant.
4.2 Prospective randomized study (III)
4.2.1 Study population
Our third study was done as a national multi-centric study in collaboration with Oulu University Hospital, Helsinki University Hospital, Tampere University Hospital and Lahti Central Hospital. In the setting of prospective double-blinded randomization, we aimed to study whether is it safe to administer thrombosis prophylaxis (enoxaparin 40mg/d) for pICH patients 24 hours or 72 hours after ICH. We conducted this study between 2009 and 2015. All patients with pICH shown in head CT or MRI were considered for this study in all the above-listed hospitals. The inclusion criteria for this study required a minimum age of 18 with a National Institutes of Health Stroke Scale (NIHSS) over 2 due to lower extremity paresis. The patient also had to be admitted to hospital under 12 hours of the onset of the symptoms.
We excluded patients with no significant lower limb paresis (NIHSS<2), comatose (GCS<8), had severe disability prior onset of pICH (mRS >2) or admitted late to hospital (over 12 hours after onset). We did not include patients with secondary causes of ICH such as aneurysm, AVM or tumor. If suspected of secondary causes, we conducted CTA, MRA/DSA immediately in the emergency room. Patients who needed immediate neurosurgical intervention were also excluded from this study. If a patient was first included in this study and a follow up CT taken 24 hours after admission showed significant hematoma enlargement, we excluded the patient from this study as, in these situations, we would not normally routinely administer any medical thrombosis prophylaxis either way until proven that immediate hematoma enlargement had ceased.
Patients receiving oral anticoagulant, aspirin or clopidogrel before onset are discontinued immediately and the effect of warfarin counteracted with Vitamin K and/or prothrombin complex concentrate. Patients who are eligible for this study

60
are either asked directly or, if not capable, their closest relative’s consent was obtained for this trial.
4.2.2 Radiological methods
All patients included in this study had their head CT obtained at least three times, at admission, 24 hours after admission and before leaving the hospital. The head CT was also taken if the patient deteriorates or develops a new neurological symptom. If hematoma size grows over 33% in any follow up CT scans, it is considered clinically relevant and leads to the cessation of placebo / enoxaparin medication.
The location of ICH was divided into the following groups: subcortical, putaminal, thalamic, combined (extension of a putaminal hematoma into the thalamus and/or extensively into the subcortical white matter), caudate nucleus, cerebellar or pontine. Hematoma volumes were calculated with the method described in our earlier studies. Intraventricular hemorrhage (IVH) was classified as: grade 0, no IVH; grade 1, a small amount of blood in the occipital horns or in III or IV ventricles; grade 2, blood occupying most of one lateral ventricle with or without blood in the III or IV ventricles; and grade 3, major IVH with blood filling all ventricles and frequently distending to ventricular system (Hallevi et al., 2009; Juvela et al., 1995).
All patients included in this study had lower limb compression ultrasonography performed if any signs of DVT appeared and routinely before discharging from our hospital. If suspected of pulmonary embolism CTPA was obtained.
4.2.3 Randomization
All eligible patients received an IPC device immediately in the emergency room. They were then randomized into two groups: enoxaparin and placebo group. The

61
doctor on-call collected a coded set of ampules from the hospital pharmacy. The appearance of these ampules is exactly the same and neither the pharmacist nor doctor on-call could tell them apart from each other. After collecting the ampules the doctor marked the code of the medicine and patient ID on the front of a sealed envelope containing information of the contents of the ampules (enoxaparin or placebo). The envelop was only opened in the case of emergency (clinically relevant hematoma enlargement after administering medicine), or at the end of this study under witnessed meeting. This method ensured that both the investigators and on-call doctors were equally blinded to the group (enoxaparin or placebo) the patient was assigned to. The desired sample size was calculated on the basis of 35% expected incidence of the primary end point in the placebo group and 10% incidence in enoxaparin group. Approximately 138 patients (69 in each group) would be needed to detect these differences by a margin of 25% at 𝛼 level of 0.05 (two-tailed) and 𝛼ß level of 0.2. After recruiting the first 80 patients, an independent safety committee analyzed the observations. Non- significant difference was observed between the enoxaparin and placebo groups and the safety committee gave permission to continue patient recruitment.
4.2.4 Administration of medicine
In the enoxaparin group subcutaneous enoxaparin 20 mg (2000IU) was administered twice a day 24 hours after the onset of ICH. The placebo group received saline injections according to the same regimen. After receiving double-blinded enoxaparin or saline injections for 2 days, both groups were then continued with a regular regimen of enoxaparin 20mg twice daily until the patient was able to walk independently or if severe rebleeding occurred.
4.2.5 Outcome measurements

62
The primary endpoint in this study was the occurrence of DVT or symptomatic PE during the 3 months after onset. The secondary endpoint included significantly enlarged ICH (>33%), recurrent bleeding, any other significant bleeding complications or death occurring within the treatment period. If death occurred in hospital settings, an autopsy was performed. If death occurred outside the hospital area, an autopsy is strongly recommended. All patients had follow-up checks three months after onset and a head CT was obtained. The outcome was assessed according to the modified Glasgow Outcome Scale (GOS); patients with a score of 1–3 (normal, minimal disability, moderate disability) were considered to have a favourable outcome, whereas patients with scores of 4-6 (severe disability, vegetative state, dead) were considered to have an unfavourable outcome.

63
5 Results
5.1 Infection after intracerebral hemorrhage (I)
5.1.1 Effect of infections on outcome
A total of 192 patients (24%) had a favourable outcome and 615 had an unfavourable outcome (76%) in our pICH series. Baseline and clinical characteristics are shown in table 4.
Table 4. Baseline and clinical characteristics of patients with primary ICH, according to the outcome. Values are the number of patients (%) unless noted otherwise. Mean values are presented as the mean ± SD. INR=international normalized ratio.
Variable Favourable
outcome (n=192)
Unfavourable
outcome (n= 615)
Total
(n=807)
P Value
Mean age in years 64 ±11 71 ±12 69 ±12 <0.001
Men 116 (60) 320 (52) 436 (54) 0.042
Previous diseases
Hypertension 124 (65) 390 (63) 514 (64) 0.769
Diabetes 20 (10) 125 (20) 145 (18) 0.002
Cardiac disease 52 (27) 257 (42) 309 (38) <0.001
Warfarin medication 19 (10) 128 (21) 147 (18) <0.001
Mean INR on arrival in units 1.2 ±0.6 1.6 ±1.1 1.5 ±1.0 <0.001
Mean CRP value per mg/L 7.3 ±5.5 12.6 ±26.0 11.3
±23.0
0.005
Median GCS score (25th, 75th percentiles) 15 (14,15) 13 (6, 15) 14 (10,
15)
<0.001
Mean hematoma vol in ml 12 ±16 41 ±45 34 ±42 <0.001
Intraventricular hemorrhage 31 (16) 339 (55) 370 (46) <0.001
Subcortical hematoma 64 (33) 173 (28) 237 (29) 0.167
Hematoma evacuation 11 (6) 98 (16) 109 (14) <0.001
Infectious complications
Urinary tract infection 8(4) 80(13) 88(11) <0.001
Pneumonia 3(2) 125(20) 128(16) <0.001
Dead within 3 month 0(0) 280(46) 280(35) <0.001

64
Infectious diseases such as pneumonia and urinary tract infections tend to have a trend for unfavourable outcome. (Table 4). In our paper, infectious complications were observed in 216 patients of which 205/615 (33%) had unfavourable outcome and 11/192 (6%) had good outcome. 88 patients overall developed UTI of which 8/192 (4%) patients had a good outcome and 80/615 (13%) had a bad outcome (p<0.001). Of the 128 patients who developed pneumonia, 3/192 patients (2%) had a good outcome and 125/615 (20%) had bad outcome (p<0.001). The patients with unfavorable outcome were significantly more often women and older than those with a favorable outcome. These patients also significantly more often had diabetes mellitus, cardiac disease, warfa- rin medication, a higher CRP value on admission, a lower GCS score, a larger hematoma, intraventricular bleeding, an evacuated hematoma, and infectious complications (Table 4).
In multivariable analysis, significant predictive factors of unfavourable outcome are higher age, diabetes mellitus, a higher CRP value on admission, a lower admission GCS score, a larger hematoma, deep seated hematoma and IVH. (Table 5)
Table 5. Predictors of an unfavourable outcome after primary ICH. Unfavourable outcome denotes moderate disability or worse outcome according to the GOS.
Variable Univariable OR (95%
Cl)
Multivariable OR
(95% Cl)
Age (per yr) 1.05 (1.04-1.06) ¶ 1.06 (1.04-1.08)¶
Cardiac disease 1.93 (1.35-2.76) ¶ 0.96 (0.60-1.53)
Diabetes mellitus 2.19 (1.33-3.63) § 1.99 (1.09-3.64) §
GCS (per unit) 0.65 (0.58-0.73) ¶ 0.75 (0.67-0.84)¶
Hematoma size (per ml) 1.05 (1.04-1.07)¶ 1.05 (1.03-1.07)¶
Presence of intraventricular hemorrhage 6.40 (4.22-9.71)¶ 2.70 (1.66-4.38)¶
Subcortical hematoma location 0.78 (0.55-1.11) 0.33 (0.20-0.54)¶
CRP on admission (per 10mg/L) 1.37 (1.10-1.70)† 1.41 (1.09-1.81)†
‡ The ORs in the multivariate analysis were also adjusted for sex. ¶ p< 0.001.§ p<0.005, † p<0.01
5.1.2 Effect of admission CRP level on outcome

65
Admission CRP level was high in patients with diabetes, cardiac disease, warfarin treatment and poor 3-month outcome (Table 6). Both univariable and multivariable analysis showed us that CRP on admission predicted an unfavourable outcome after excluding infectious diseases (OR 1.45 per 10mg/L [95% CI 1.10-1.90], p<0.01). This is shown in table 5. For every 10mg/L increase in CRP, the risk of an unfavourable outcome increases 1.4 fold (OR 95% CI; 1.41(1.09-1.81)). There seems to be a threshold for CRP for poorer outcome being 12.6 mg/L (p<0.001). The size of hematoma is related to admission CRP (rs = 0.084, p= 0.018). Admission GCS-score does not correlate with admission CRP but rather correlates only to CRP levels taken 24 hours after admission (at admission: rs =0.067, P= 0.060; after 24 hours; rs =0.0237, p<0.001). High admission CRP levels did not clearly predict later development of an infectious disease. However, patients who later developed pneumonia (n=128) had a very high CRP level after ICH onset compared to those who did not develop pneumonia (47.9±68.0 vs 21.5±35.8 within 48 hours and 67.3±59.1 vs 25.5±42.5 within 96 hours, p<0.001 for both).
Table 6. Admission CRP value according to patient characteristics and outcomes
Variable No. of patients Mean admission
CRP value per
ml/L †
P Value
‡
All patients 807 11.3 ± 23.0
Sex NS
Men 436 12.7± 28.6
Women 371 9.7 ± 13.6
Hypertension NS
Yes 514 10.1 ± 20.2
No 293 13.4 ± 27.1
Diabetes 0.049
Yes 145 12.9 ± 20.5
No 662 10.9 ± 23.5
Cardiac disease 0.002
Yes 309 12.9 ± 25.8
No 498 10.3 ± 21.0
Warfarin 0.02
Yes 147 13.1 ± 20.8
No 660 10.9 ± 23.4
Urinary tract infection 0.038

66
Yes 88 13.4 ± 20.7
No 715 11.1 ± 23.3
GOS score 0.004
5 192 7.3 ± 5.5
4 143 10.6 ± 17.6
3 189 9.9 ± 14.7
2 6 6.8 ± 3.4
1 277 15.5 ± 34.4
Hematoma size NS
< 30ml 511 9.7 ± 14.7
>30ml 295 14.1 ± 32.5
Intraventricular hemorrhage NS
Yes 370 13.0 ± 29.6
No 436 9.9 ± 15.2
Pneumonia NS
Yes 128 17.1 ± 37.7
No 675 10.2 ± 18.8
Hematoma evacuation NS
Yes 109 14.6 ± 41.6
No 698 10.8 ± 18.4
GCS score NS
3-8 172 13.4 ± 23.3
9-12 140 11.3 ± 21.6
13-15 489 10.0 ± 19.2
¥ NS = not significant. † Presented as ± SD. ‡ Mann-Whitney, except for GCS and GOS scores, where
Krudkal-Wallis ANOVA was used.
5.2 Seizures after intracerebral hemorrhage (II)
5.2.1 Seizure groups
In our register 130 out of 935 (14%) patients had seizures for the first time. 51 patients suffered immediate seizure (<24 h after ICH), 21 early seizures (> 24 h to 2 weeks after ICH) and 58 late seizures (>2 weeks after ICH). The baseline is shown in table 7. Patients who suffered immediate and late seizures were significantly younger than those with early seizures (p<0.05). The early seizure

67
group had significantly more diabetics than the immediate and late seizure groups.
Table 7. Baseline characteristics of subjects with new-onset seizures.
Subjects without
seizures (n= 805)
Subjects with seizures Total
(n=935) Immediate
(n=51)
Early
(n=21)
Late
(n=58)
Mean age, yr ± SD * 70 ± 12 64 ± 16 73 ± 11 63 ± 10 69 ± 12
Men, n(%) 431 (54) 25 (49) 13 (62) 32 (55) 501 (54)
Previous diseases, n(%)
Diabetes* 145 (18) 6 (12) 9 (43) 8(14) 168 (18)
Ischemic stroke 167 (21) 10 (20) 7 (33) 12 (21) 196 (21)
Hypertension 510 (63) 32 (63) 13 (62) 22(38) 587 (63)
Cardiac disease 325 (40) 15 (29) 10 (48) 19 (33) 369 (39)
Lifestyle factors, n(%)
Current smoking 68 (8) 8 (16) 1 (5) 4 (7) 81 (9)
Heavy drinking 94 (12) 8 (16) 0(0) 5 (9) 107 (11)
Warfarin medication 158 (20) 8 (12) 5 (24) 5 (9) 174 (19)
*significant heterogeneity between the groups, p<0.05
5.2.2 Risk factor for different seizures groups
Our study showed low GCS score on admission (p<0.001), subcortical location of the hematoma (p<0.001) and age inversely (p<0.01) to be independent risk factors of immediate seizures in multivariable analysis. Subcortical location was the only independent risk factor of early seizures (p<0.001). Subcortical location (p<0.001), age inversely (p<0.01) and hematoma evacuation (p<0.05) were independently predictive of late seizures (Table 8).

68
Table 8. Predictors of immediate, early and late seizures in ICH patients. Odds ratios in the multivariate analysis have been adjusted for sex and the variable lists in the table.
Variable Univariable OR (95%
Cl)
Multivariable OR (95%
Cl)
Immediate seizure
Hematoma size (per ml) 1.00 (0.99-1.01) 0.99 (0.97-1.00)‡
GCS on admission (per unit) 0.88 (0.83-0.93)* 0.83 (0.77-0.89)*
Subcortical location 2.21 (1.25-3.89)# 2.93 (1.6-5.39)*
Age (per year) 0.97 (0.95-0.99)# 0.97 (0.95-1.00)#
Early seizure
Hematoma size (per ml) 0.99 (0.97-1.00) 0.99 (0.96-1.00)
GCS on admission (per unit) 1.09 (0.96-1.25) 1.01 (0.87-1.18)
Subcortical location 3.98 (1.63-9.71)# 5.42 (2.15-13.62)*
Age (per year) 1.03 (0.99-1.07) 1.03 (0.99-1.07)
Hematoma evacuation 0.32 (0.04-2.40) 0.41 (0.04-3.71)
Late seizure
Hematoma size (per ml) 1.00 (0.99-1.01) 1.00 (0.99-1.00)
GCS on admission (per unit) 1.07 (0.99-1.51) 1.09 (0.989-1.20)
Subcortical location 3.16 (1.84-5.41)* 2.90 (1.60-5.29)*
Age (per year) 0.96 (0.94-0.98)* 0.96 (0.94-1.00)#
Hematoma evacuation 3.24 (1.79-5.85)* 2.47 (1.12-5.45)¶
OR, odds ratio; Cl, confidence interval. *p<0.001. #p<0.01. ‡p<0.02. ¶p<0.05.
5.2.3 Outcome and mortality between seizure groups
There are differences in outcome among different seizure types. Patients who suffered a seizure <24 hours after ictus had the poorest outcome (63%). In the late seizure group, only 36% experienced poor outcome (P<0.05). In the early seizure group, 48% had poor outcome and patients without seizures 58% had a poor outcome (table 9).

69
Table 9. Clinical characteristics and outcome of ICH subjects, by time of new-onset seizures after the index stroke
Subjects without
seizures (n= 805)
Subjects with seizures Total
(n=935) Immediate
(n=51)
Early
(n=21)
Late
(n=58)
Median GCS, (25 and
75% percentiles)
14 (10,15) 10 (5,14)¶ 13 (12,15) 14 (12,15) 14 (10,15)
Mean hematoma volume,
ml±SD
34±43 32±41 19±19‡ 30±28 33±42
Intraventricular
haemorrhage, n(%)
366 (46) 25 (49) 6 (29) 19 (33) 416 (45)
Subcortical location* 209 (26) 24 (47) 13 (62) 32 (55) 278 (30)
Complications, n(%)
Cardiac 58 (7) 6 (12) 4 (19) 2 (3) 70 (7)
Thromboembolic** 16 (2) 3 (6) 0 4 (7) 23 (2)
Infection* 192 (24) 19 (37) 13 (62) 14 (24) 238 (25)
Urinary tract infection 77 (10) 8(16) 4 (19) 10 (17) 99 (11)
Pneumonia* 111 (14) 12 (24) 9 (43) 7 (12) 139 (15)
Hematoma evacuation,
n(%)*
97 (12) 9 (18) 1 (5) 18 (31) 125 (13)
Prophylactic AED N/A 1 (2) 1 (5) 11 (19) N/A
Epilepsy after PICH 0/0 11 (22) 8 (38) 49 (84) 68 (7)
GOS, n (%)**
Favourable 338 (42) 19 (37) 11 (52) 37 (64) 405 (43)
Unfavourable 463 (58) 32 (63) 10 (48) 21 (36) 526 (56)
Dead within 3 months,
n(%)*
283 (35) 25 (49) 5 (24) 0 (0) 313 (33)
AED = antiepileptic drug. N/A = not available. *significant heterogeneity between groups, p<0.001.
**significant heterogeneity between groups, p<0.05. ¶lower mean GCS than in other groups, p<0.001.
‡smaller volume than in subjects without seizures (p=0.003 equal variances not assumed).
Other factors which predicted poor outcomes are large hematoma volume
(p<0.001), presence of IVH (p<0.001), low GCS on admission (p<0.001), high age (p<0.001), diabetes (p<0.05) and infections (p<0.001) (Table 10). Logistic regression analysis showed immediate seizures (OR 1.96, 95% CI 1.05—3.66, p<0.05), early seizures (OR 4.47, 95% Cl 1.79—11.18, p<0.01), thromboembolism (OR 2.83, 95% Cl 1.21—6.67, p<0.05), and cardiac complications (OR 2.37, 95% Cl 1.39—4.03, p<0.01) to be independently associated with the occurrence of an infectious complication.

70
Table 10. Predictors of poor outcome. Odds ratios in the multivariate analysis have been adjusted for sex and the variable listed in the table. OR, odds ratio; Cl, confidence interval; IVH, intraventricular hemorrhage
Variable Multivariable OR (95% Cl)
Hematoma size (per ml) 1.03 (1.02-1.04)*
Presence of IVH 2.63 (1.79-3.86)*
GCS on admission (per unit) 0.75 (0.69-0.81)*
Age (per year) 1.05 (1.04-1.07)*
warfarin treatment 1.36 (0.82-2.25)
Immediate seizures 0.67 (0.29-1.54)
Early seizures 0.34 (0.12-0.97)#
Late seizures 0.47 (0.23-0.96)#
Cardiac disease 1.23 (0.81-1.86)
hypertension 0.80 (0.54-1.17)
diabetes 1.79 (1.10-2.93)#
Post – PICH infections 2.92 (1.95-4.41)*
Thromboembolic complication 1.34 (0.46-3.85)
*p<0.001.#p<0.05.
Although seizures do not seem to increase mortality, patients having
immediate seizure had the highest fatality rate: 25 out of 51 (49%) died within 3 months, whereas none died in the late seizure group during that period of time. 5 out of 21 patients (24%) in the early seizure group died within 3 months (Table 9).
5.3 Thromboembolic complications after intracerebral hemorrhage (III)
Overall, 139 patients enrolled in this trial. All completed their follow up. After randomization 68 patients were in the enoxaparin group (received enoxaparin 24 h after onset) and 71 patients were in the placebo group (received enoxaparin 72h after onset). In the placebo group more patients consumed NSAID (non-ASA) before onset compared to the enoxaparin group (9vs 0, p<0.005). 4 patient had suffered VTE before onset compared to none of the placebo group patient had history of VTE. Baseline characteristics and clinical characteristics are shown in

71
Tables 11 and 12. There were no statistically significant differences in patients clinical characteristics between groups.
Table 11. Baseline characteristics of the patients with primary ICH
Placebo n=68 Enoxaparin n=71 Total n=139
Male n(%) 36 (53) 36 (51) 72 (52)
Mean age, y(±SD) 68±6 66±19 67±11
Previous disease (%)
Hypertension 54 (79) 52 (73) 106 (76)
Cardiac disease 18 (26) 14 (20) 32 (23)
Atrial fibrillation 12 (18) 6 (8) 18 (13)
Diabetes 9 (13) 16 (23) 25 (18)
Cancer 2 (3) 5 (7) 7 (5)
Brain infarction/TIA 11 (16) 11 (15) 22 (16)
Epilepsy 2 (3) 2 (3) 4 (3)
Heavy drinking n(%) 4 (6) 2 (3) 6 (4)
VTE in history n(%)* 0 (0) 4 (6) 4 (3)
Previous medications n(%)
Anticoagulants 11 (16) 11 (15) 22 (16)
Aspirin 19 (28) 29 (41) 48 (35)
Clopidogrel 2 (3) 4 (6) 6 (4)
Dipyridamol 1 (1) 3 (4) 4 (3)
SSRI 5 (7) 4 (6) 9 (6)
NSAID* 9 (13) 0 (0) 9 (6)
*p<0.05
Table 12. Clinical characteristics and outcome of ICH patients. GI = gastrointestinal, BP = blood preassure
Placebo n=68 Enoxaparin n=71 Total n=139
Hematoma volume, ml(±SD) 21±23 28±31 24±27
Location of hematoma, n(%)
Subcortex 10 (15) 20 (28) 30 (22)
Thalamus 18 (27) 14 (20) 32 (23)
Basal ganglia 32 (47) 31 (44) 63 (45)
Combined 7 (10) 6 (9) 13 (9)
Other 2 (3) 1 (1) 3 (2)

72
Primary endpoint was rare in this trial as only one patient in the placebo
group (1%) and two in the enoxaparin group (3%) developed DVT (Table 12). There were no statistical differences between the two groups as regards the development of VTE. No symptomatic PE was observed. All three patients that developed DVT had been taking aspirin as a regular medicine before onset and none of them had been on anticoagulation before ictus. All three patients had poor outcome (GOS 4-6). (Table 13).
Table 13. Baseline, Clinical characteristics and outcome of 3 DVT patients.
Patient 1 Patient 2 Patient 3
Age (y.) 66 95 71
ICH volume, ml 49 50 45
ICH score 2 1 1
GCS
NIHSS
11
22
14
21
15
8
Hematoma location Subcortical Putaminal Basal ganglia
Previous disease
Cardiac disease No No No
Atrial fibrillation No Yes No
Diabetes Yes No Yes
Previous medications
Anticoagulants No No No
ASA Yes Yes Yes
Intraventricular hemorrhage, n(%) 45 (66) 53 (75) 98 (71)
Later hematoma evacuation, n(%) 2 (3) 3 (4) 5 (4)
Mean ICH score, (±SD) 1.4±1.0 1.4±1.1 1.4±1.0
Mean GCS score, (±SD) 14±2 13±3 13±2
Complications, n(%)
Hematoma enlargement 33% 8 (12) 8 (11) 16 (12)
GI-bleeding 0 (0) 0 (0) 0 (0)
Seizure 4 (6) 3 (4) 7 (5)
DVT 1 (1) 2 (3) 3 (2)
PE 0 (0) 0 (0) 0 (0)
Outcome
GOS 1-3 (good) 29 (42) 31 (44) 60 (43)
GOS 4-6 (poor) 39 (57) 40 (56) 79 (57)
Death within 3 months 12 (18) 11 (15) 23 (17)

73
Complications
Hematoma enlargement No No No
Pneumonia No Yes No
Outcome
GOS 6 5 4
Dead within 3 months Yes No no
Receiving enoxaparin early did not affect patient hematoma enlargement as 8
patients in both groups had hematoma enlargement (P=0.0927). Outcome (GOS 1-3; 29 in enoxaparin vrs 31 in the placebo group, p=0.904) and mortality (12 (18%) in enoxaparin vrs 11 (15%) in the placebo group, p=0.733) did not differ significantly between the two groups. (Table 12).

74
6 Discussion
6.1 Main findings
6.1.1 Study I
Elevated CRP level has been shown to predict poor outcome in patients after ischemic stroke and aneurysm subarachnoid hemorrhage (Idicula et al., 2009.;Juvela et al., 2012). Our study has demonstrated that a high level admission- CRP level is an independent predictor of poor outcome in ICH patients. This effect remains after taking into account pre-existing heart disease, severity of bleeding and infectious diseases.
CRP is produced by hepatocytes in response to cytokinesis. It is a sensitive nonspecific marker of body reacting to tissue damage, inflammation and infection (Sproston & Ashworth, 2018; Griselli et al., 1999). CRP usually arises and peaks at 48 hours after initial stimulus and falls to baseline in 7-12 days (Nordestgaard & Zacho, 2009). Large hematoma volume (>30ml), representing significant cerebral tissue damage, correlates with elevated CRP levels in our study. High level of CRP were found around the hemorrhagic clot in patients with large hematomas who died within 48 hours of primary ICH (Di Napoli et al., 2012). In acute setting within hours of onset, CRP is released from damaged neurons and glial cells. Within the first two days, interleukin such as IL-6 is released which promote hepatocytes to produce excessive CRP. This can be then measured from plasma. CRP itself can maintain cerebrovascular inflammation and brain injury by inducing leucocytes chemotaxis. By binding neutrophils and macrophages, direct apoptosis can be induced (Alexandrova et al., 2011). This could be an explanation for poor outcome in ICH patients with higher CRP level. Larger hematoma and thus severe cerebral tissue injury disturb certain pro- and anti-inflammatory pathwas triggering a severe self-destructive inflammatory reaction (Alexandrova et al., 2011).
In previous studies, mildly elevated CRP values were found in stroke patients with the following preconditions: hypertension, diabetes, heart disease and smoking (Elkind et al., 2009). In our series, high-level admission CRP was found in patients with comorbidities such as cardiac disease and diabetes mellitus. Cardiovascular diseases and diabete mellitus have been found to associate with

75
poor outcome in ICH patients in other publications (Tetri et al., 2008; Tetri et al., 2009). However, in our data, cardiac disease was not associated with poor outcome, suggesting that primary ICH itself influences CRP more than does cardiac disease.
Patients who later developed pneumonia had only slightly elevated admission CRP level. They were also mostly with poor neurological condition immediately after onset. Many of them may suffer from silent aspiration and CRP level increases in the following days after admission. Besides predicting pneumonia, higher growth of CRP level taken on consecutive days was also a prediction of poor outcome. This can partially be explained by the later development of pneumonia as infectious diseases also affect patient outcome in ours and other studies (Bercault & Boulain, 2001; Lord et al., 2014).
After taking account of heart disease, diabetes mellitus and infectious diseases, multivariable analysis showed that high admission CRP value remains an independent factor predicting unfavourable outcome. This was apparent even after excluding patients who later developed pneumonia. However, our study does not directly explain the mechanism behind the independent relationship between CRP level and poor outcome. We believe that based on available data, CRP rises due to larger cerebral tissue damage (Alexandrova & Danovska, 2011).
The strength of this study lies in its large sample size, homogenous population and strict inclusion criteria. Radiological evaluation was carried out by an experienced neuroradiologist who was blinded to its case history. We also took account of all well-known factors affecting outcome of ICH patients. Follow up was performed meticulously with an experienced neurologist and patient neurological symptoms were evaluated. We excluded 16% of patients from the original data due to a lack of admission CRP data. However, the hematoma volume size sample was comparable as our patient sample size so this should not have caused any notable selection bias. The limitation of this study is its retrospective observational study design. However, because of our large sample size, statistical power to show significant independent associations between CRP levels on admission and the outcome following ICH is sufficient enough. The outcome did not change even after we excluded patients who later developed pneumonia.

76
6.1.2 Study II
We found that 5.5 % of ICH patients had immediate seizures, 8 % suffered a seizure within two weeks of ictus and 6 % had seizure after 2 weeks from onset. Subcortical location seems to be the only factor able to predict immediate, early and late seizures. This finding is in line with other publications as lobar lesions situated in subcortical space is a well known risk factor for seizure development in ICH patients (Faught, Peters, Bartolucci, Moore, & Miller, 1989; Passero et al., 2002; Rossi et al., 2013; Weisberg, Shamsnia, & Elliott, 1991). Impaired consciousness was found on admission in many patients with immediate seizures. It was, however, unclear whether this was due to a non-convulsive status epilepticus in some patients as we did not routinely perform cEEG in our ICU.
Young age seems to be a risk factor for immediate and late seizure. Age inversely has also been shown to increase the risk of seizure complications in other studies (Passero et al., 2002; Reddig et al., 2011; Yang et al., 2009a). One explanation for this could be that younger patients are more likely to go through with surgery than older patients. Surgery seems to be associated with the risk for late seizures. Hematoma evacuation causes additional trauma to the subcortical brain matters, leading to loss of functional components and neuronal dysfunction that may contribute to later seizure development. Surgery is performed on patients with a lower GCS score and subcortical hematomas, which are factors that contributes to later seizure development. In addition, hematoma evacuation surgery has been seen to prolong patient lifespan with the expense of functional outcome (Löppönen et al., 2013b). Therefore, patients who undergo surgery are more likely to develop epileptic seizure at a later stage, as time goes by they will have more possibilities for seizure occurrence.
There have been conflicting results as to whether seizures affect ICH patients outcome (Cervoni et al., 1994; De Reuck, 2009; Kase, Williams, Wyatt, & Mohr, 1982; Lipton, Berger, Lesser, Lantos, & Portenoy, 1987). In our study epileptic seizure by itself did not seem to increase patient mortality rates. Early and late seizures were predictors of favourable functional outcome and none of the patients in the late seizure group died within 3 months. This is explained by the definition of seizure types; those who survive beyond 48h will have a better outcome.
Our study has shown that smaller hematoma volume is associated with immediate seizure occurrence. Our study, however, does not give an explanation

77
for this. It has been shown in other studies that cortical lobar hematoma have often smaller volume than deep seated hematomas due to etiology of ICH and vessel anatomy (p<0.001). This can offer an explanation why smaller size hematoma may be associated with increased risk for immediate seizure (Passero et al., 2002). There are conflicting results from the literature regarding the correlation between hematoma volume and seizures. In retrospective studies from Passero and Faught, patients with smaller hematomas seem to to have higher incidence of seizure occurrence compared to larger hematomas (Passero et al., 2002; Faught et al., 1989). In a large retrospective analysis of 1920 patients, larger volume of hematoma was a risk factor for recurrent seizures (OR 1.03; 95%CI 1.00-1.05; P=0.027) (Neshige et al., 2015). In another retrospective study of 243 patients, an increase of 1.3 ml in ICH volume increased the seizure rate by 2.7% (Yang et al., 2009b).
Although infectious disease did not affect patient outcome, it was associated with an increased risk for immediate seizure, however. The explanation might be that patients with immediate seizure tended to have poor admission neurological status, which is by itself a risk factor for silent aspiration and later development of pneumonia (Hu, Lee, Pianosi, & Ryu, 2015; Masiero, Pierobon, Previato, & Gomiero, 2008; Zhao, Liu, & Li, 2015).
In our study, a relatively large proportion of seizures occurred immediately after ictus as 39% had seizures <24 h after ICH. Other studies have shown significantly fewer immediate seizures and is probably due to the fact that we did not routinely administer prophylactic AED as did many other institutes (Passero et al., 2002; Reddig et al., 2011; Woo, K., Yang, & Cho, 2012). Prophylactic AED is given sporadically in our institute as only 2% in the immediate seizure group received any kind of prophylactic AED. Valproic acid, phenytoin or leveracetamine were commonly used as prophylactic AED. There is conflicting data regarding whether prophylactic seizure medication prevents the later onset of seizures in ICH patients. Recent prospective RCT has shown that prophylactic valproic acid in ICH patients reduced the risk of early seizures (2.7% vs 11.1% p=0.4) and improved their functional outcome (p=0.002) (Gilad, Boaz, Dabby, Sadeh, & Lampl, 2011). The incidence of early seizure didn’t reach statistical significant between valproic acid and placebo group probably due to small number of early seizures (one in valproic acid group vs four in placebo group). However, the authors suggest that the neuroprotective effect of valproic acid may have improved ICH patient outcome. Other studies have shown a contrary effect as prophylactic AED did not improve patient outcome, and in some cases seemed

78
to even worsen patient outcome (OR 6.8, 95% Cl 2.2-21.2, p=0.001) after adjustment for other known predictors of outcome after ICH (Messé et al., 2009b). It is noteworthy that many of the publications used phosphenytoin as a prophylactic AED, and it is known for its many side effects which could affect patient outcome. In our study, we have found that young patients with subcortical hematoma and undergoing surgery are at risk of seizure complications. In this subgroup of patients, consideration should be given to administering prophylactic AEDs.
The strength of our study lies on its long follow up. This enabled us to identify the occurrence of late seizures and to ascertain definite diagnosis of epilepsy after pICH as accurately as possible. Other strengths of our study lie in its meticulous radiological evaluation and large population-based observational study design. This study, though, has some limitations. Continuous EEG was seldom used in ICU. Therefore, some non-convulsive seizures could have been missed. Prophylactic AED is seldom used in our hospital. This, however, gave us an opportunity to observe the natural course and incidence of immediate and early seizures without the effect of AEDs. Also, a variety of AEDs were used to treat seizures and the duration of AED medication was determined individually. There was a lack of specific data of different seizure types. Only a few subjects had a routine second CT scan to rule out hematoma enlargement. The association between hematoma enlargement and seizure complications therefore remains unclear.
6.1.3 Study III
Our study has found thromboembolic events to be a rare complication nowadays when adequate thrombosis prophylaxis measures are utilized, as less than 3% of patients suffered DVT and none of the ICH patients had PE. Earlier studies have shown that about half of all stroke patients will develop VTE if none of the thrombosis prophylaxis methods are utilized (Clagett, Anderson, Levine, Salzman, & Wheeler, 1992; Warlow, Ogston, & Douglas, 1976). By introducing long compression socks and later on IPC devices, thrombotic events were significantly lowered (Arabi et al., 2013; Dennis et al., 2013; Zhang, D., Li, Li, & Du, 2018) . The safety of these devices are proven rigorously in many studies.

79
Both AHA/ASA and European guidelines strongly recommend usage of them to prevent VTE in ICH patients (Hemphill et al., 2015; Steiner et al., 2014).
Anticoagulants such as heparin have routinely been used in ischemic stroke patients for thrombosis prophylaxis (Dizon & De Leon, 2018; McCarthy, Turner, Robertson, Hawkey, & Macey, 1977). However, in ICH patients clinicians are reluctant to start any kind of anticoagulant even at a small dosage in fear of hemorrhagic complications (Prabhakaran et al., 2015). The issue of when it is safe to start anticoagulation for thrombosis prophylaxis in ICH patients has not been scrutinized under strict scientific research.
Our study is the largest prospective randomized study to investigate when and whether it is safe to administer anticoagulants for thrombosis prophylaxia in ICH patients. Prior to our study there were only 3 prospective RCT studies regarding usage of anticoagulant in the prevention of VTE in spontaneous ICH patients. The biggest and most recent was by Orken et al (Orken et al., 2009). They randomized 75 ICH patients to receive either LMWH (enoxaparin 40mg/d) 48h after ictus or only receive long compression stockings. As our own study concluded, they also found a relatively low incidence of VTE as only four DVT occurred. There was no significant difference between the two groups with regard to VTE and hemorrhagic enlargement. Dickmann et al randomized 46 patients to receive heparin either 4 days or 10 days after ICH. Thrombotic events were more frequent in their study as eighteen patients had evidence of VTE and fourteen patients had PE (Dickmann et al., 1988). No significant difference was found in hematoma enlargement between the two groups. Boeer et al used the same data as Dickman but added 22 patients to receive heparin 2 days after ICH (Boeer et al., 1991). Again, the risk of hematoma enlargement was not significantly associated with the timing of the anticoagulant. However, patients receiving heparin 2 days after ICH showed significantly less PE (5%) compared to patients receiving heparin 4 (22%) and 10 days (39%) after ICH. The scientific value of these studies suffers from their significantly smaller sample size compared to our study. Also, both Dickman and Boeer studies included AVM, aneurysm and cerebral infarction patients. Usage of long compression socks or IPC was unclear.
There are some retrospective studies regarding the safety and efficiency of antithrombotic medication in ICH patients. Tetri et al found 3% VT events in patients with enoxaparin 20mg administered once a day 1-4 days after ictus (Tetri et al., 2008). We had a slightly lower rate of VTE, probably due to higher enoxaparin dosage (20mg x 2 /d). Asymptomatic DVT could have been missed in their data since they did not routinely perform compression ultrasonography on

80
all patients as we did. Hematoma enlargement was also not sufficiently evaluated as they did not rigorously obtain a follow up head CT. Another retrospective study by Keindies et al found 0,8% thrombotic events in ICH patients (Kleindienst et al., 2003). However, their patient inclusion criteria was not as strict as ours as they included patients with AVM, aneurysm and cerebral infarction. Also, whether patients had hemiparesis or hemiplegia was unclear.
Lacking sufficient RCT, no strong recommendation could be made in both AHA/ASA or European guidelines. Based on 3 small RCT, mentioned above, recent AHA/ASA guidelines (2015) concluded that administering LMWH 1-4 days after ICH onset does not seem to increase the incidence of recurrent hemorrhage (Hemphill et al., 2015). The ESO guidelines do not make any kind of recommendation regarding this issue due to lack of a large RCT (Steiner et al., 2014). It is alarming that in the absence of any strong recommendations, only 16.5% of ICH patients receive any kind of thrombosis prophylaxis according to a recent publication (Prabhakaran et al., 2015). It is clear that lacking sufficient thrombosis prophylaxis, patients are at risk of thrombotic events which result in higher morbidity and mortality from the already morbid disease of ICH. This study has shed valuable light to the subject that administering LMWH early is both safe and efficient for prevention of VTE.
The strength of our study lies in its prospective double-blinded randomization setting. Inclusion criteria was strict as we excluded patients with secondary causes of ICH and excessive risk factors for later thrombosis formation. Weakness of our study is that only one out of twenty three deceased patient was conducted autopsy. Thus, majority of cause of death could not be determined. However there were no significant differences in mortality rate between groups (18% placebo group vs 15 % enoxaparin group). Another limitation in our study was that pulmonary CTA was not routinely performed on all patients to screen for asymptomatic PE. However, we did not see the need to obtain pulmonary CT for asymptomatic patients as it was unnecessary to expose patients to excessive radiation. We did, however, routinely perform compression ultrasonography on all patients as it has no risk of additional radiation exposure. Strict inclusion criteria and double-blinded randomized setting does mean that our results add significant value to the available data regarding this topic.

81
7 Summary and conclusions
- High CRP level at admission is an independent risk factor for poor outcome in ICH patients. This effect is present after excluding other known predictors for poor outcome in ICH patients. The prediction value of high CRP cannot be explained by infectious diseases and it remained an independent risk factor even after excluding infectious diseases. We postulate that a high CRP level can be a sign of severe neuronal injury in the absence of aspiration.
- Our results are in line with other research as the subcortical location of ICH is a strong predictive factor of all types of epileptic seizure in ICH patients, whereas young age is a risk factor for immediate and late seizures only. A low GCS score increases the risk of immediate seizures, which can partly be explained by non-convulsive seizure. Surgery has been found to be associated with late seizures. This can be explained by the invasive nature of cortectomy that erupts neuronal tissues.
- Although 49% of patients who had immediate seizures died within 3 months, epileptic seizures did not increase overall mortality rate in ICH patients. Patient with immediate seizures has increased risk for infectious diseases such as aspiration pneumonia. Patients in early and late seizure groups had better functional outcome. Thromboembolic events were more common in immediate and late seizure groups.
- Administering early (1 day after onset) enoxaparin does not increase the risk of ICH enlargement compared to starting anticoagulant at a later stage (3 days after onset).
- There are no significant differences in the occurrence of thromboembolic complications whether anticoagulant is administered 1 or 3 days after ICH.

82

83
References Adams, R.E., Diringer, M.N. (1998). Response to external ventricular drainage in
spontaneous intracerebral hemorrhage with hydrocephalus. Neurology, 50(2), 519-23.
Ahmadian, A., Mizzi, A., Banasiak, M., Downes, K., Camporesi, E. M., Thompson Sullebarger, J., . . . Agazzi, S. (2013). Cardiac manifestations of subarachnoid hemorrhage. Heart, Lung and Vessels, 5(3), 168-178.
Alexandrova, M. L., & Danovska, M. P. (2011). Serum C-reactive protein and lipid hydroperoxides in predicting short-term clinical outcome after spontaneous intracerebral hemorrhage. Journal of Clinical Neuroscience: Official Journal of the Neurosurgical Society of Australasia, 18(2), 247-252. doi:10.1016/j.jocn.2010.07.125
Alqahtani, F., Aljohani, S., Tarabishy, A., Busu, T., Adcock, A., & Alkhouli, M. (2017). Incidence and outcomes of myocardial infarction in patients admitted with acute ischemic stroke. Stroke, 48(11), 2931-2938. doi:10.1161/STROKEAHA.117.018408
Al-Shahi Salman, R., Frantzias, J., Lee, R. J., Lyden, P. D., Battey, T. W. K., Ayres, A. M., . . . Rosand, J. (2018). Absolute risk and predictors of the growth of acute spontaneous intracerebral haemorrhage: A systematic review and meta-analysis of individual patient data. The Lancet. Neurology, 17(10), 885-894. doi:10.1016/S1474-4422(18)30253-9
Andaluz, N., & Zuccarello, M. (2009). Recent trends in the treatment of spontaneous intracerebral hemorrhage: Analysis of a nationwide inpatient database. Journal of Neurosurgery, 110(3), 403-410. doi:10.3171/2008.5.17559
Anderson, C. S., Heeley, E., Huang, Y., Wang, J., Stapf, C., Delcourt, C., . . . Chalmers, J. (2013). Rapid blood-pressure lowering in patients with acute intracerebral hemorrhage. The New England Journal of Medicine, 368(25), 2355-2365. doi:10.1056/NEJMoa1214609
Anderson, C. S., Huang, Y., Wang, J. G., Arima, H., Neal, B., Peng, B., . . . Chalmers, J. (2008). Intensive blood pressure reduction in acute cerebral haemorrhage trial (INTERACT): A randomised pilot trial. The Lancet. Neurology, 7(5), 391-399. doi:10.1016/S1474-4422(08)70069-3
Arabi, Y. M., Khedr, M., Dara, S. I., Dhar, G. S., Bhat, S. A., Tamim, H. M., & Afesh, L. Y. (2013). Use of intermittent pneumatic compression and not graduated compression stockings is associated with lower incident VTE in critically ill patients: A multiple propensity scores adjusted analysis. Chest, 144(1), 152-159. doi:10.1378/chest.12-2028
Arntz, R., Rutten-Jacobs, L., Maaijwee, N., Schoonderwaldt, H., Dorresteijn, L., van Dijk, E., & de Leeuw, F. (2013). Post-stroke epilepsy in young adults: A long-term follow-up study. PloS One, 8(2), e55498. doi:10.1371/journal.pone.0055498
Baharoglu, M. I., Cordonnier, C., Salman, R. A., de Gans, K., Koopman, M. M., Brand, A., . . . Roos, Y. B. (2016). Platelet transfusion versus standard care

84
after acute stroke due to spontaneous cerebral haemorrhage associated with antiplatelet therapy (PATCH): A randomised, open-label, phase 3 trial. Lancet (London, England), 387(10038), 2605-2613. doi:10.1016/S0140-6736(16)30392-0
Balami, J. S., & Buchan, A. M. (2012). Complications of intracerebral haemorrhage. The Lancet. Neurology, 11(1), 101-118. doi:10.1016/S1474-4422(11)70264-2
Basaldella, L., Marton, E., Fiorindi, A., Scarpa, B., Badreddine, H., & Longatti, P. (2012). External ventricular drainage alone versus endoscopic surgery for severe intraventricular hemorrhage: A comparative retrospective analysis on outcome and shunt dependency. Neurosurgical Focus, 32(4), E4. doi:10.3171/2012.1.FOCUS11349
Becattini, C., Sembolini, A., & Paciaroni, M. (2016). Resuming anticoagulant therapy after intracerebral bleeding. Vascular Pharmacology, 84, 15-24. doi:10.1016/j.vph.2016.05.012
Bercault, N., & Boulain, T. (2001). Mortality rate attributable to ventilator-associated nosocomial pneumonia in an adult intensive care unit: A prospective case-control study. Critical Care Medicine, 29(12), 2303-2309. doi:10.1097/00003246-200112000-00012
Bhattathiri, P. S., Gregson, B., Prasad, K. S. M., & Mendelow, A. D. (2006). Intraventricular hemorrhage and hydrocephalus after spontaneous intracerebral hemorrhage: Results from the STICH trial. Acta Neurochirurgica. Supplement, 96, 65-68.
Bladin, C. F., Alexandrov, A. V., Bellavance, A., Bornstein, N., Chambers, B., Coté, R., . . . Norris, J. W. (2000). Seizures after stroke: A prospective multicenter study. Archives of Neurology, 57(11), 1617-1622. doi:10.1001/archneur.57.11.1617
Boeer, A., Voth, E., Henze, T., & Prange, H. W. (1991). Early heparin therapy in patients with spontaneous intracerebral haemorrhage. Journal of Neurology, Neurosurgery, and Psychiatry, 54(5), 466-467.
Bråthen, G., Brodtkorb, E., Helde, G., Sand, T., & Bovim, G. (1999). The diversity of seizures related to alcohol use. A study of consecutive patients. European Journal of Neurology, 6(6), 697-703.
Brogi E, Corbella D, Coccolini F, Gamberini E, Russo E, Agnoletti V, Forfori F. (2020). The role of platelet transfusions after intracranial hemorrhage in patients on antiplatelet agents: a systematic review and meta-analysis. World neurosurgery,4(11).S1878-8750(20)30687-2.doi. 10.1016/j.wneu.2020.03.216. [Epub ahead of print]
Brott, T., Broderick, J., Kothari, R., Barsan, W., Tomsick, T., Sauerbeck, L., . . . Khoury, J. (1997). Early hemorrhage growth in patients with intracerebral hemorrhage. Stroke, 28(1), 1-5. doi:10.1161/01.str.28.1.1
Brouwers, H. B., Biffi, A., McNamara, K. A., Ayres, A. M., Valant, V., Schwab, K., . . . Goldstein, J. N. (2012). Apolipoprotein E genotype is associated with CT angiography spot sign in lobar intracerebral hemorrhage. Stroke, 43(8), 2120-2125. doi:10.1161/STROKEAHA.112.659094

85
Brouwers, H. B., Falcone, G. J., McNamara, K. A., Ayres, A. M., Oleinik, A., Schwab, K., . . . Goldstein, J. N. (2012). CTA spot sign predicts hematoma expansion in patients with delayed presentation after intracerebral hemorrhage. Neurocritical Care, 17(3), 421-428. doi:10.1007/s12028-012-9765-2
Brouwers, H. B., & Greenberg, S. M. (2013). Hematoma expansion following acute intracerebral hemorrhage. Cerebrovascular Diseases (Basel, Switzerland), 35(3), 195-201. doi:10.1159/000346599
Bu, Y., Chen, M., Gao, T., Wang, X., Li, X., & Gao, F. (2016). Mechanisms of hydrocephalus after intraventricular haemorrhage in adults. Stroke and Vascular Neurology, 1(1), 23-27. doi:10.1136/svn-2015-000003
Castaño Ávila, S., Corral Lozano, E., Vallejo De La Cueva, A., Maynar Moliner, J., Martín López, A., Fonseca San Miguel, F., . . . Manzano Ramírez, A. (2013). Intraventricular hemorrhage treated with intraventricular fibrinolysis. A 10-year experience. Medicina Intensiva, 37(2), 61-66. doi:10.1016/j.medin.2012.02.011
Cervoni, L., Artico, M., Salvati, M., Bristot, R., Franco, C., & Delfini, R. (1994). Epileptic seizures in intracerebral hemorrhage: A clinical and prognostic study of 55 cases. Neurosurgical Review, 17(3), 185-188.
Chen, C., Liu, C., Tung, Y., Lee, H., Chuang, H., Lin, S., & Cho, D. (2011). Endoscopic surgery for intraventricular hemorrhage (IVH) caused by thalamic hemorrhage: Comparisons of endoscopic surgery and external ventricular drainage (EVD) surgery. World Neurosurgery, 75(2), 264-268. doi:10.1016/j.wneu.2010.07.041
Claessens, D., Bekelaar, K., Schreuder, Floris H. B. M., de Greef, Bianca T. A., Vlooswijk, M. C. G., Staals, J., . . . Rouhl, R. P. W. (2017). Mortality after primary intracerebral hemorrhage in relation to post-stroke seizures. Journal of Neurology, 264(9), 1885-1891. doi:10.1007/s00415-017-8573-1
Clagett, G. P., Anderson, F. A., Levine, M. N., Salzman, E. W., & Wheeler, H. B. (1992). Prevention of venous thromboembolism. Chest, 102(4 Suppl), 391S-407S.
Curtis, R., Schweitzer, A., & van Vlymen, J. (2015). Reversal of warfarin anticoagulation for urgent surgical procedures. Canadian Journal of Anaesthesia = Journal Canadien D'Anesthesie, 62(6), 634-649. doi:10.1007/s12630-015-0366-3
Davis, S. M., Broderick, J., Hennerici, M., Brun, N. C., Diringer, M. N., Mayer, S. A., . . . Steiner, T. (2006). Hematoma growth is a determinant of mortality and poor outcome after intracerebral hemorrhage. Neurology, 66(8), 1175-1181. doi:10.1212/01.wnl.0000208408.98482.99
De Herdt, V., Dumont, F., Hénon, H., Derambure, P., Vonck, K., Leys, D., & Cordonnier, C. (2011). Early seizures in intracerebral hemorrhage: Incidence, associated factors, and outcome. Neurology, 77(20), 1794-1800. doi:10.1212/WNL.0b013e31823648a6
De Reuck, J. (2009). Management of stroke-related seizures. Acta Neurologica Belgica, 109(4), 271-276.

86
De Reuck, J., Hemelsoet, D., & Van Maele, G. (2007). Seizures and epilepsy in patients with a spontaneous intracerebral haematoma. Clinical Neurology and Neurosurgery, 109(6), 501-504. doi:10.1016/j.clineuro.2007.04.001
Delcourt, C., Huang, Y., Wang, J., Heeley, E., Lindley, R., Stapf, C., . . . Anderson, C. (2010). The second (main) phase of an open, randomised, multicentre study to investigate the effectiveness of an intensive blood pressure reduction in acute cerebral haemorrhage trial (INTERACT2). International Journal of Stroke: Official Journal of the International Stroke Society, 5(2), 110-116. doi:10.1111/j.1747-4949.2010.00415.x
Delgado Almandoz, J. E., Yoo, A. J., Stone, M. J., Schaefer, P. W., Goldstein, J. N., Rosand, J., . . . Romero, J. M. (2009). Systematic characterization of the computed tomography angiography spot sign in primary intracerebral hemorrhage identifies patients at highest risk for hematoma expansion: The spot sign score. Stroke, 40(9), 2994-3000. doi:10.1161/STROKEAHA.109.554667
Demchuk, A. M., Dowlatshahi, D., Rodriguez-Luna, D., Molina, C. A., Blas, Y. S., Dzialowski, I., . . . Aviv, R. I. (2012). Prediction of haematoma growth and outcome in patients with intracerebral haemorrhage using the CT-angiography spot sign (PREDICT): A prospective observational study. The Lancet. Neurology, 11(4), 307-314. doi:10.1016/S1474-4422(12)70038-8
Dennis, M., Sandercock, P., Reid, J., Graham, C., Forbes, J., & Murray, G. (2013). Effectiveness of intermittent pneumatic compression in reduction of risk of deep vein thrombosis in patients who have had a stroke (CLOTS 3): A multicentre randomised controlled trial. Lancet (London, England), 382(9891), 516-524. doi:10.1016/S0140-6736(13)61050-8
Di Napoli, M., Godoy, D. A., Campi, V., del Valle, M., Piñero, G., Mirofsky, M., . . . Rabinstein, A. A. (2011). C-reactive protein level measurement improves mortality prediction when added to the spontaneous intracerebral hemorrhage score. Stroke, 42(5), 1230-1236. doi:10.1161/STROKEAHA.110.604983
Di Napoli, M., Godoy, D. A., Campi, V., Masotti, L., Smith, C. J., Parry Jones, A. R., . . . Popa Wagner, A. (2012). C-reactive protein in intracerebral hemorrhage: Time course, tissue localization, and prognosis. Neurology, 79(7), 690-699. doi:10.1212/WNL.0b013e318264e3be
Di Nisio, M., van Es, N., & Büller, H. R. (2016). Deep vein thrombosis and pulmonary embolism. Lancet (London, England), 388(10063), 3060-3073. doi:10.1016/S0140-6736(16)30514-1
Dickmann, U., Voth, E., Schicha, H., Henze, T., Prange, H., & Emrich, D. (1988). Heparin therapy, deep-vein thrombosis and pulmonary embolism after intracerebral hemorrhage. Klinische Wochenschrift, 66(23), 1182-1183.
Diedler, J., Sykora, M., Hahn, P., Rupp, A., Rocco, A., Herweh, C., & Steiner, T. (2009). C-reactive-protein levels associated with infection predict short- and long-term outcome after supratentorial intracerebral hemorrhage. Cerebrovascular Diseases (Basel, Switzerland), 27(3), 272-279. doi:10.1159/000199465

87
Diringer, M. N., Edwards, D. F., & Zazulia, A. R. (1998a). Hydrocephalus: A previously unrecognized predictor of poor outcome from supratentorial intracerebral hemorrhage. Stroke, 29(7), 1352-1357. doi:10.1161/01.str.29.7.1352
Diringer, M. N., Edwards, D. F., & Zazulia, A. R. (1998b). Hydrocephalus: A previously unrecognized predictor of poor outcome from supratentorial intracerebral hemorrhage. Stroke, 29(7), 1352-1357. doi:10.1161/01.str.29.7.1352
Divani, A. A., Hevesi, M., Pulivarthi, S., Luo, X., Souslian, F., Suarez, J. I., & Bershad, E. M. (2015). Predictors of nosocomial pneumonia in intracerebral hemorrhage patients: A multi-center observational study. Neurocritical Care, 22(2), 234-242. doi:10.1007/s12028-014-0065-x
Dizon, M. A. M., & De Leon, J. M. (2018). Effectiveness of initiating deep vein thrombosis prophylaxis in patients with stroke: An integrative review. The Journal of Neuroscience Nursing: Journal of the American Association of Neuroscience Nurses, 50(5), 308-312. doi:10.1097/JNN.0000000000000385
Dunatov, S., Antoncic, I., Bralic, M., & Jurjevic, A. (2011). Intraventricular thrombolysis with rt-PA in patients with intraventricular hemorrhage. Acta Neurologica Scandinavica, 124(5), 343-348. doi:10.1111/j.1600-0404.2010.01481.x
Dziedzic, T., Slowik, A., Pera, J., & Szczudlik, A. (2007). Beta-blockers reduce the risk of early death in ischemic stroke. Journal of the Neurological Sciences, 252(1), 53-56. doi:10.1016/j.jns.2006.10.007
Elkind, M. S. V., Luna, J. M., Moon, Y. P., Liu, K. M., Spitalnik, S. L., Paik, M. C., & Sacco, R. L. (2009). High-sensitivity C-reactive protein predicts mortality but not stroke: The northern manhattan study. Neurology, 73(16), 1300-1307. doi:10.1212/WNL.0b013e3181bd10bc
Engelhard, H. H., Andrews, C. O., Slavin, K. V., & Charbel, F. T. (2003). Current management of intraventricular hemorrhage. Surgical Neurology, 60(1), 15-22. doi:10.1016/s0090-3019(03)00144-7
Fang, H. -., Lin, C. -., & Ko, W. -. (2005). Hematology and coagulation parameters predict outcome in taiwanese patients with spontaneous intracerebral hemorrhage. European Journal of Neurology, 12(3), 226-232. doi:10.1111/j.1468-1331.2004.01018.x
Faught, E., Peters, D., Bartolucci, A., Moore, L., & Miller, P. C. (1989). Seizures after primary intracerebral hemorrhage. Neurology, 39(8), 1089-1093.
Fayos-Vidal, F., Arzamendi-Aizpurua, D., Millán-Álvarez, X., Guisado-Alonso, D., Camps-Renom, P., Prats-Sánchez, L., . . . Martí-Fàbregas, J. (2017). Left atrial appendage closure in patients with intracranial haemorrhage and atrial fibrillation. Neurologia (Barcelona, Spain), doi:10.1016/j.nrl.2017.05.013
Feigin, V. L., Lawes, C. M. M., Bennett, D. A., Barker-Collo, S. L., & Parag, V. (2009). Worldwide stroke incidence and early case fatality reported in 56 population-based studies: A systematic review. The Lancet. Neurology, 8(4), 355-369. doi:10.1016/S1474-4422(09)70025-0
Firsching, R., Huber, M., & Frowein, R. A. (1991). Cerebellar haemorrhage: Management and prognosis. Neurosurgical Review, 14(3), 191-194.

88
Fisher, C. M. (1971). Pathological observations in hypertensive cerebral hemorrhage. Journal of Neuropathology and Experimental Neurology, 30(3), 536-550. doi:10.1097/00005072-197107000-00015
Fisher, R. S., Acevedo, C., Arzimanoglou, A., Bogacz, A., Cross, J. H., Elger, C. E., . . . Wiebe, S. (2014). ILAE official report: A practical clinical definition of epilepsy. Epilepsia, 55(4), 475-482. doi:10.1111/epi.12550
Fogelholm, R., Nuutila, M., & Vuorela, A. L. (1992). Primary intracerebral haemorrhage in the jyväskylä region, central finland, 1985-89: Incidence, case fatality rate, and functional outcome. Journal of Neurology, Neurosurgery, and Psychiatry, 55(7), 546-552.
Fountas, K. N., Kapsalaki, E. Z., Parish, D. C., Smith, B., Smisson, H. F., Johnston, K. W., & Robinson, J. S. (2005). Intraventricular administration of rt-PA in patients with intraventricular hemorrhage. Southern Medical Journal, 98(8), 767-773. doi:10.1097/01.smj.0000170732.24324.ea
Gaberel, T., Magheru, C., & Emery, E. (2012). Management of non-traumatic intraventricular hemorrhage. Neurosurgical Review, 35(4), 485-495. doi:10.1007/s10143-012-0399-9
Garrett, M. C., Komotar, R. J., Starke, R. M., Doshi, D., Otten, M. L., & Connolly, E. S. (2010). Elevated troponin levels are predictive of mortality in surgical intracerebral hemorrhage patients. Neurocritical Care, 12(2), 199-203. doi:10.1007/s12028-009-9245-5
Garrett, M. C., Komotar, R. J., Starke, R. M., Merkow, M. B., Otten, M. L., & Connolly, E. S. (2009). Predictors of seizure onset after intracerebral hemorrhage and the role of long-term antiepileptic therapy. Journal of Critical Care, 24(3), 335-339. doi:10.1016/j.jcrc.2008.10.015
Gattringer, T., Niederkorn, K., Seyfang, L., Seifert-Held, T., Simmet, N., Ferrari, J., . . . Enzinger, C. (2014). Myocardial infarction as a complication in acute stroke: Results from the austrian stroke unit registry. Cerebrovascular Diseases (Basel, Switzerland), 37(2), 147-152. doi:10.1159/000357799
Gilad, R., Boaz, M., Dabby, R., Sadeh, M., & Lampl, Y. (2011). Are post intracerebral hemorrhage seizures prevented by anti-epileptic treatment? Epilepsy Research, 95(3), 227-231. doi:10.1016/j.eplepsyres.2011.04.002
Gilmore, E., Choi, H. A., Hirsch, L. J., & Claassen, J. (2010). Seizures and CNS hemorrhage: Spontaneous intracerebral and aneurysmal subarachnoid hemorrhage. The Neurologist, 16(3), 165-175. doi:10.1097/NRL.0b013e3181c7cd0b
Goldhaber, S. Z. (2004). Pulmonary embolism. Lancet (London, England), 363(9417), 1295-1305. doi:10.1016/S0140-6736(04)16004-2
Goldhaber, S. Z., & Bounameaux, H. (2012). Pulmonary embolism and deep vein thrombosis. Lancet (London, England), 379(9828), 1835-1846. doi:10.1016/S0140-6736(11)61904-1
Goldstein, J. N., Fazen, L. E., Snider, R., Schwab, K., Greenberg, S. M., Smith, E. E., . . . Rosand, J. (2007). Contrast extravasation on CT angiography predicts hematoma expansion in intracerebral hemorrhage. Neurology, 68(12), 889-894. doi:10.1212/01.wnl.0000257087.22852.21

89
Goldstein, J. N., Fazen, L. E., Wendell, L., Chang, Y., Rost, N. S., Snider, R., . . . Rosand, J. (2009). Risk of thromboembolism following acute intracerebral hemorrhage. Neurocritical Care, 10(1), 28-34. doi:10.1007/s12028-008-9134-3
Goswami, R. P., Karmakar, P. S., & Ghosh, A. (2012). Early seizures in first-ever acute stroke patients in india: Incidence, predictive factors and impact on early outcome. European Journal of Neurology, 19(10), 1361-1366. doi:10.1111/j.1468-1331.2012.03782.x
Greenberg, S. M., Vonsattel, J. P., Segal, A. Z., Chiu, R. I., Clatworthy, A. E., Liao, A., . . . Rebeck, G. W. (1998). Association of apolipoprotein E epsilon2 and vasculopathy in cerebral amyloid angiopathy. Neurology, 50(4), 961-965. doi:10.1212/wnl.50.4.961
Grill, M. F., & Maganti, R. K. (2011). Neurotoxic effects associated with antibiotic use: Management considerations. British Journal of Clinical Pharmacology, 72(3), 381-393. doi:10.1111/j.1365-2125.2011.03991.x
Griselli, M., Herbert, J., Hutchinson, W. L., Taylor, K. M., Sohail, M., Krausz, T., & Pepys, M. B. (1999). C-reactive protein and complement are important mediators of tissue damage in acute myocardial infarction. The Journal of Experimental Medicine, 190(12), 1733-1740. doi:10.1084/jem.190.12.1733
Guglin, M., & Novotorova, I. (2011). Neurogenic stunned myocardium and takotsubo cardiomyopathy are the same syndrome: A pooled analysis. Congestive Heart Failure (Greenwich, Conn.), 17(3), 127-132. doi:10.1111/j.1751-7133.2011.00210.x
Hallevi, H., Albright, K. C., Aronowski, J., Barreto, A. D., Martin-Schild, S., Khaja, A. M., . . . Grotta, J. C. (2008). Intraventricular hemorrhage: Anatomic relationships and clinical implications. Neurology, 70(11), 848-852. doi:10.1212/01.wnl.0000304930.47751.75
Hallevi, H., Dar, NS., Barreto, A.D., Morales, M. M., Martin-Schild, S., Abraham, A. T., Walker, K. C., Gonzales, N.r., Illoh, K., Grotta, J.C., Savitz, S. I. (2009). The IVH score: a novel tool for estimating intraventricular hemorrhage volume: clinical and research implications. Crit care med, 37(3), 969-74
Hanley, D. F. (2009). Intraventricular hemorrhage: Severity factor and treatment target in spontaneous intracerebral hemorrhage. Stroke, 40(4), 1533-1538. doi:10.1161/STROKEAHA.108.535419
Hanley, D. F., Thompson, R. E., Muschelli, J., Rosenblum, M., McBee, N., Lane, K., . . . Zuccarello, M. (2016). Safety and efficacy of minimally invasive surgery plus alteplase in intracerebral haemorrhage evacuation (MISTIE): A randomised, controlled, open-label, phase 2 trial. The Lancet. Neurology, 15(12), 1228-1237. doi:10.1016/S1474-4422(16)30234-4
Hanley DF, Lane K, McBee N, Ziai W, Tuhrim S, Lees KR, Dawson J, Gandhi D, Ullman N, Mould WA, Mayo SW, Mendelow AD, Gregson B, Butcher K, Vespa P, Wright DW, Kase CS, Carhuapoma JR, Keyl PM, Diener-West M, Muschelli J, Betz JF, Thompson CB, Sugar EA, Yenokyan G, Janis S, John S, Harnof S, Lopez GA, Aldrich EF, Harrigan MR, Ansari S, Jallo J, Caron JL, LeDoux D, Adeoye O, Zuccarello M, Adams HP Jr, Rosenblum M,

90
Thompson RE, Awad IA24. (2017). Thrombolytic removal of intraventricular haemorrhage in treatment of severe stroke: results of the randomised, multicentre, multiregion, placebo-controlled CLEAR III trial. Lancet, 389(10069):603-611. doi: 10.1016/S0140-6736(16)32410-2. Epub 2017 Jan 10.
Hanley, D. F., Thompson, R. E., Rosenblum, M., Yenokyan, G., Lane, K., McBee, N., . . . Awad, I. A. (2019). Efficacy and safety of minimally invasive surgery with thrombolysis in intracerebral haemorrhage evacuation (MISTIE III): A randomised, controlled, open-label, blinded endpoint phase 3 trial. Lancet (London, England), 393(10175), 1021-1032. doi:10.1016/S0140-6736(19)30195-3
Harms, H., Prass, K., Meisel, C., Klehmet, J., Rogge, W., Drenckhahn, C., . . . Meisel, A. (2008). Preventive antibacterial therapy in acute ischemic stroke: A randomized controlled trial. PloS One, 3(5), e2158. doi:10.1371/journal.pone.0002158
Hasegawa, K., Fix, M.L., Wendell, L., Schwab, K., Ay, H., Smith, E.E., Greenberg, S.M., Rosand, J., Goldstein, J.n., Brown, D.F. (2012). Ischemic-appearing electrocardiographic changes predict myocardial injury in patients with intracerebral hemorrhage. Am J Emerg Med., 30(4), 545-52. doi: 10.1016/j.ajem.2011.02.007.
Hays, A., & Diringer, M. N. (2006). Elevated troponin levels are associated with higher mortality following intracerebral hemorrhage. Neurology, 66(9), 1330-1334. doi:10.1212/01.wnl.0000210523.22944.9b
Hemphill, J. C., Bonovich, D. C., Besmertis, L., Manley, G. T., & Johnston, S. C. (2001a). The ICH score: A simple, reliable grading scale for intracerebral hemorrhage. Stroke, 32(4), 891-897. doi:10.1161/01.str.32.4.891
Hemphill, J. C., Bonovich, D. C., Besmertis, L., Manley, G. T., & Johnston, S. C. (2001b). The ICH score: A simple, reliable grading scale for intracerebral hemorrhage. Stroke, 32(4), 891-897. doi:10.1161/01.str.32.4.891
Hemphill, J. C., Greenberg, S. M., Anderson, C. S., Becker, K., Bendok, B. R., Cushman, M., . . . Woo, D. (2015). Guidelines for the management of spontaneous intracerebral hemorrhage: A guideline for healthcare professionals from the american heart association/american stroke association. Stroke, 46(7), 2032-2060. doi:10.1161/STR.0000000000000069
Hillbom, M. E. (1980). Occurrence of cerebral seizures provoked by alcohol abuse. Epilepsia, 21(5), 459-466. doi:10.1111/j.1528-1157.1980.tb04296.x
Hinson, H. E., Hanley, D. F., & Ziai, W. C. (2010). Management of intraventricular hemorrhage. Current Neurology and Neuroscience Reports, 10(2), 73-82. doi:10.1007/s11910-010-0086-6
Horstmann, S., Rizos, T., Jenetzky, E., Gumbinger, C., Hacke, W., & Veltkamp, R. (2014). Prevalence of atrial fibrillation in intracerebral hemorrhage. European Journal of Neurology, 21(4), 570-576. doi:10.1111/ene.12215
Horstmann, S., Zugck, C., Krumsdorf, U., Rizos, T., Rauch, G., Geis, N., . . . Veltkamp, R. (2014). Left atrial appendage occlusion in atrial fibrillation after intracranial hemorrhage. Neurology, 82(2), 135-138. doi:10.1212/WNL.0000000000000022

91
Hu, X., Lee, J. S., Pianosi, P. T., & Ryu, J. H. (2015). Aspiration-related pulmonary syndromes. Chest, 147(3), 815-823. doi:10.1378/chest.14-1049
Hwang, B. Y., Bruce, S. S., Appelboom, G., Piazza, M. A., Carpenter, A. M., Gigante, P. R., . . . Connolly, E. S. (2012). Evaluation of intraventricular hemorrhage assessment methods for predicting outcome following intracerebral hemorrhage. Journal of Neurosurgery, 116(1), 185-192. doi:10.3171/2011.9.JNS10850
Hylek, E. M., Evans-Molina, C., Shea, C., Henault, L. E., & Regan, S. (2007). Major hemorrhage and tolerability of warfarin in the first year of therapy among elderly patients with atrial fibrillation. Circulation, 115(21), 2689-2696. doi:10.1161/CIRCULATIONAHA.106.653048
Idicula, T. T., Brogger, J., Naess, H., Waje-Andreassen, U., & Thomassen, L. (2009). Admission C-reactive protein after acute ischemic stroke is associated with stroke severity and mortality: The 'bergen stroke study'. BMC Neurology, 9, 18. doi:10.1186/1471-2377-9-18
Ionita, C. C., Siddiqui, A. H., Levy, E. I., Hopkins, L. N., Snyder, K. V., & Gibbons, K. J. (2011). Acute ischemic stroke and infections. Journal of Stroke and Cerebrovascular Diseases: The Official Journal of National Stroke Association, 20(1), 1-9. doi:10.1016/j.jstrokecerebrovasdis.2009.09.011
Isaacs, A. M., Bezchlibnyk, Y. B., Yong, H., Koshy, D., Urbaneja, G., Hader, W. J., & Hamilton, M. G. (2016). Endoscopic third ventriculostomy for treatment of adult hydrocephalus: Long-term follow-up of 163 patients. Neurosurgical Focus, 41(3), E3. doi:10.3171/2016.6.FOCUS16193
Jennett B, Bond M. (1975). Assessment of outcome after severe brain damage. Lancet, 1, 480-484
Juvela, S. (1996). Prevalence of risk factors in spontaneous intracerebral hemorrhage and aneurysmal subarachnoid hemorrhage. Archives of Neurology, 53(8), 734-740.
Juvela, S., Hillbom, M., & Palomäki, H. (1995). Risk factors for spontaneous intracerebral hemorrhage. Stroke, 26(9), 1558-1564.
Juvela, S., Kuhmonen, J., & Siironen, J. (2012). C-reactive protein as predictor for poor outcome after aneurysmal subarachnoid haemorrhage. Acta Neurochirurgica, 154(3), 397-404. doi:10.1007/s00701-011-1243-7
Kase, C. S., Williams, J. P., Wyatt, D. A., & Mohr, J. P. (1982). Lobar intracerebral hematomas: Clinical and CT analysis of 22 cases. Neurology, 32(10), 1146-1150.
Kerro, A., Woods, T., & Chang, J. J. (2017). Neurogenic stunned myocardium in subarachnoid hemorrhage. Journal of Critical Care, 38, 27-34. doi:10.1016/j.jcrc.2016.10.010
Kim, J., Smith, A., Hemphill, J. C., Smith, W. S., Lu, Y., Dillon, W. P., & Wintermark, M. (2008). Contrast extravasation on CT predicts mortality in primary intracerebral hemorrhage. AJNR. American Journal of Neuroradiology, 29(3), 520-525. doi:10.3174/ajnr.A0859
King, N. K. K., Lai, J. L., Tan, L. B., Lee, K. K., Pang, B. C., Ng, I., & Wang, E. (2012). A randomized, placebo-controlled pilot study of patients with

92
spontaneous intraventricular haemorrhage treated with intraventricular thrombolysis. Journal of Clinical Neuroscience: Official Journal of the Neurosurgical Society of Australasia, 19(7), 961-964. doi:10.1016/j.jocn.2011.09.030
Kiphuth, I. C., Köhrmann, M., Huttner, H. B., & Schellinger, P. D. (2009). The safety and usefulness of low molecular weight heparins and unfractionated heparins in patients with acute stroke. Expert Opinion on Drug Safety, 8(5), 585-597. doi:10.1517/14740330903150157
Klehmet, J., Harms, H., Richter, M., Prass, K., Volk, H. D., Dirnagl, U., . . . Meisel, C. (2009). Stroke-induced immunodepression and post-stroke infections: Lessons from the preventive antibacterial therapy in stroke trial. Neuroscience, 158(3), 1184-1193. doi:10.1016/j.neuroscience.2008.07.044
Kleindienst, A., Harvey, H. B., Mater, E., Bronst, J., Flack, J., Herenz, K., . . . Schön, R. (2003). Early antithrombotic prophylaxis with low molecular weight heparin in neurosurgery. Acta Neurochirurgica, 145(12), 1085-1091. doi:10.1007/s00701-003-0142-y
Knudsen, K. A., Rosand, J., Karluk, D., & Greenberg, S. M. (2001). Clinical diagnosis of cerebral amyloid angiopathy: Validation of the boston criteria. Neurology, 56(4), 537-539.
Kothari RU, Brott T, Broderick JP, Barsan WG, Sauerbeck LR, Zuccarello M. (1996). The ABCs of measuring intracerebral hemorrhage volumes. Stroke 27, 1304-1305
Kuo, L,T., Lu, H. Y., Tsai, J.C., Tu, Y. K. (2018). Prediction of shunt dependency after intracerebral hemorrhage and intraventricular hemorrhage. Neurocritical care, 29(2), 233-240. doi: 10.1007/s12028-018-0532-x.
Kuramatsu, J. B., Biffi, A., Gerner, S. T., Sembill, J. A., Sprügel, M. I., Leasure, A., . . . Huttner, H. B. (2019). Association of surgical hematoma evacuation vs conservative treatment with functional outcome in patients with cerebellar intracerebral hemorrhage. Jama, 322(14), 1392-1403. doi:10.1001/jama.2019.13014
Kuramatsu, J. B., Gerner, S. T., Schellinger, P. D., Glahn, J., Endres, M., Sobesky, J., . . . Huttner, H. B. (2015a). Anticoagulant reversal, blood pressure levels, and anticoagulant resumption in patients with anticoagulation-related intracerebral hemorrhage. Jama, 313(8), 824-836. doi:10.1001/jama.2015.0846
Kuramatsu, J. B., Gerner, S. T., Schellinger, P. D., Glahn, J., Endres, M., Sobesky, J., . . . Huttner, H. B. (2015b). Anticoagulant reversal, blood pressure levels, and anticoagulant resumption in patients with anticoagulation-related intracerebral hemorrhage. Jama, 313(8), 824-836. doi:10.1001/jama.2015.0846
Lacut, K., Bressollette, L., Le Gal, G., Etienne, E., De Tinteniac, A., Renault, A., . . . Oger, E. (2005). Prevention of venous thrombosis in patients with acute intracerebral hemorrhage. Neurology, 65(6), 865-869. doi:10.1212/01.wnl.0000176073.80532.a2

93
Lamy, C., Domigo, V., Semah, F., Arquizan, C., Trystram, D., Coste, J., & Mas, J. L. (2003). Early and late seizures after cryptogenic ischemic stroke in young adults. Neurology, 60(3), 400-404. doi:10.1212/wnl.60.3.400
Lapointe, M., & Haines, S. (2002). Fibrinolytic therapy for intraventricular hemorrhage in adults. The Cochrane Database of Systematic Reviews, (3), CD003692. doi:10.1002/14651858.CD003692
Lewis, C. E., Antoine, J., Mueller, C., Talbot, W. A., Swaroop, R., & Edwards, W. S. (1976). Elastic compression in the prevention of venous stasis. A critical reevaluation. American Journal of Surgery, 132(6), 739-743. doi:10.1016/0002-9610(76)90447-5
Li, Q., Liu, Q., Yang, W., Wang, X., Zhao, L., Xiong, X., . . . Xie, P. (2017). Island sign: An imaging predictor for early hematoma expansion and poor outcome in patients with intracerebral hemorrhage. Stroke, 48(11), 3019-3025. doi:10.1161/STROKEAHA.117.017985
Li, X., Wen, S., Li, S., Bai, R., Liu, N., Feng, L., . . . Ma, C. (2016). Over 1-year efficacy and safety of left atrial appendage occlusion versus novel oral anticoagulants for stroke prevention in atrial fibrillation: A systematic review and meta-analysis of randomized controlled trials and observational studies. Heart Rhythm, 13(6), 1203-1214. doi:10.1016/j.hrthm.2015.12.037
Li, Z., Zhao, X., Wang, Y., Wang, C., Liu, L., Shao, X., . . . Wang, Y. (2015). Association between seizures and outcomes among intracerebral hemorrhage patients: The china national stroke registry. Journal of Stroke and Cerebrovascular Diseases: The Official Journal of National Stroke Association, 24(2), 455-464. doi:10.1016/j.jstrokecerebrovasdis.2014.09.021
Line, B. R. (2001). Pathophysiology and diagnosis of deep venous thrombosis. Seminars in Nuclear Medicine, 31(2), 90-101.
Lipton, R. B., Berger, A. R., Lesser, M. L., Lantos, G., & Portenoy, R. K. (1987). Lobar vs thalamic and basal ganglion hemorrhage: Clinical and radiographic features. Journal of Neurology, 234(2), 86-90.
Löppönen, P., Tetri, S., Juvela, S., Huhtakangas, J., Saloheimo, P., Bode, M. K., . . . Hillbom, M. (2013a). A population based study of outcomes after evacuation of primary supratentorial intracerebral hemorrhage. Clinical Neurology and Neurosurgery, 115(8), 1350-1355. doi:10.1016/j.clineuro.2012.12.022
Löppönen, P., Tetri, S., Juvela, S., Huhtakangas, J., Saloheimo, P., Bode, M. K., . . . Hillbom, M. (2013b). A population based study of outcomes after evacuation of primary supratentorial intracerebral hemorrhage. Clinical Neurology and Neurosurgery, 115(8), 1350-1355. doi:10.1016/j.clineuro.2012.12.022
Lord, A. S., Langefeld, C. D., Sekar, P., Moomaw, C. J., Badjatia, N., Vashkevich, A., . . . Elkind, M. S. V. (2014). Infection after intracerebral hemorrhage: Risk factors and association with outcomes in the ethnic/racial variations of intracerebral hemorrhage study. Stroke, 45(12), 3535-3542. doi:10.1161/STROKEAHA.114.006435
Lossius, M. I., Rønning, O. M., Slapø, G. D., Mowinckel, P., & Gjerstad, L. (2005). Poststroke epilepsy: Occurrence and predictors--a long-term

94
prospective controlled study (akershus stroke study). Epilepsia, 46(8), 1246-1251. doi:10.1111/j.1528-1167.2005.57904.x
Lowe, G. D. O., Sweetnam, P. M., Yarnell, J. W. G., Rumley, A., Rumley, C., Bainton, D., & Ben-Shlomo, Y. (2004). C-reactive protein, fibrin D-dimer, and risk of ischemic heart disease: The caerphilly and speedwell studies. Arteriosclerosis, Thrombosis, and Vascular Biology, 24(10), 1957-1962. doi:10.1161/01.ATV.0000141842.27810.a9
Madžar, D., Kuramatsu, J. B., Gollwitzer, S., Lücking, H., Kloska, S. P., Hamer, H. M., . . . Huttner, H. B. (2014). Seizures among long-term survivors of conservatively treated ICH patients: Incidence, risk factors, and impact on functional outcome. Neurocritical Care, 21(2), 211-219. doi:10.1007/s12028-014-9968-9
Manning, L., Hirakawa, Y., Arima, H., Anderson, C, S. (2014). Blood pressure variability and outcome after acute intracerebral haemorrhage: a post-hoc analysis of INTERACT2, a randomised controlled trial. Lancet Neurol, 13(4), 364-73. doi: 10.1016/S1474-4422(14)70018-3. Epub 2014 Feb 13.
Manno, E. M., Atkinson, J. L. D., Fulgham, J. R., & Wijdicks, E. F. M. (2005). Emerging medical and surgical management strategies in the evaluation and treatment of intracerebral hemorrhage. Mayo Clinic Proceedings, 80(3), 420-433. doi:10.4065/80.3.420
Martí-Fàbregas, J., Martínez-Ramírez, S., Martínez-Corral, M., Díaz-Manera, J., Querol, L., Suárez-Calvet, M., . . . Martí-Vilalta, J. -. (2008). Blood pressure is not associated with haematoma enlargement in acute intracerebral haemorrhage. European Journal of Neurology, 15(10), 1085-1090. doi:10.1111/j.1468-1331.2008.02254.x
Masiero, S., Pierobon, R., Previato, C., & Gomiero, E. (2008). Pneumonia in stroke patients with oropharyngeal dysphagia: A six-month follow-up study. Neurological Sciences: Official Journal of the Italian Neurological Society and of the Italian Society of Clinical Neurophysiology, 29(3), 139-145. doi:10.1007/s10072-008-0925-2
Mayer, S. A., Brun, N. C., Begtrup, K., Broderick, J., Davis, S., Diringer, M. N., . . . Steiner, T. (2005). Recombinant activated factor VII for acute intracerebral hemorrhage. The New England Journal of Medicine, 352(8), 777-785. doi:10.1056/NEJMoa042991
Mayer, S. A., Brun, N. C., Begtrup, K., Broderick, J., Davis, S., Diringer, M. N., . . . Steiner, T. (2008). Efficacy and safety of recombinant activated factor VII for acute intracerebral hemorrhage. The New England Journal of Medicine, 358(20), 2127-2137. doi:10.1056/NEJMoa0707534
McCarron, M. O., Nicoll, J. A., Stewart, J., Ironside, J. W., Mann, D. M., Love, S., . . . Dewar, D. (1999). The apolipoprotein E epsilon2 allele and the pathological features in cerebral amyloid angiopathy-related hemorrhage. Journal of Neuropathology and Experimental Neurology, 58(7), 711-718. doi:10.1097/00005072-199907000-00005
McCarthy, S. T., Turner, J. J., Robertson, D., Hawkey, C. J., & Macey, D. J. (1977). Low-dose heparin as a prophylaxis against deep-vein thrombosis after acute stroke. Lancet (London, England), 2(8042), 800-801.

95
Meisel, C., Schwab, J. M., Prass, K., Meisel, A., & Dirnagl, U. (2005). Central nervous system injury-induced immune deficiency syndrome. Nature Reviews. Neuroscience, 6(10), 775-786. doi:10.1038/nrn1765
Mendelow, A. D., Gregson, B. A., Fernandes, H. M., Murray, G. D., Teasdale, G. M., Hope, D. T., . . . Barer, D. H. (2005). Early surgery versus initial conservative treatment in patients with spontaneous supratentorial intracerebral haematomas in the international surgical trial in intracerebral haemorrhage (STICH): A randomised trial. Lancet (London, England), 365(9457), 387-397. doi:10.1016/S0140-6736(05)17826-X
Mendelow, A. D., Gregson, B. A., Rowan, E. N., Murray, G. D., Gholkar, A., & Mitchell, P. M. (2013). Early surgery versus initial conservative treatment in patients with spontaneous supratentorial lobar intracerebral haematomas (STICH II): A randomised trial. Lancet (London, England), 382(9890), 397-408. doi:10.1016/S0140-6736(13)60986-1
Messé, S. R., Sansing, L. H., Cucchiara, B. L., Herman, S. T., Lyden, P. D., & Kasner, S. E. (2009a). Prophylactic antiepileptic drug use is associated with poor outcome following ICH. Neurocritical Care, 11(1), 38-44. doi:10.1007/s12028-009-9207-y
Messé, S. R., Sansing, L. H., Cucchiara, B. L., Herman, S. T., Lyden, P. D., & Kasner, S. E. (2009b). Prophylactic antiepileptic drug use is associated with poor outcome following ICH. Neurocritical Care, 11(1), 38-44. doi:10.1007/s12028-009-9207-y
Mullen, M. T., Kasner, S. E., & Messé, S. R. (2013). Seizures do not increase in-hospital mortality after intracerebral hemorrhage in the nationwide inpatient sample. Neurocritical Care, 19(1), 19-24. doi:10.1007/s12028-012-9791-0
Murai, Y., Ikeda, Y., Teramoto, A., & Tsuji, Y. (1998). Magnetic resonance imaging-documented extravasation as an indicator of acute hypertensive intracerebral hemorrhage. Journal of Neurosurgery, 88(4), 650-655. doi:10.3171/jns.1998.88.4.0650
Murthy, S. B., Awad, I., Harnof, S., Aldrich, F., Harrigan, M., Jallo, J., . . . Ziai, W. C. (2017). Permanent CSF shunting after intraventricular hemorrhage in the CLEAR III trial. Neurology, 89(4), 355-362. doi:10.1212/WNL.0000000000004155
Murthy, S. B., Gupta, A., Merkler, A. E., Navi, B. B., Mandava, P., Iadecola, C., . . . Kamel, H. (2017). Restarting anticoagulant therapy after intracranial hemorrhage: A systematic review and meta-analysis. Stroke, 48(6), 1594-1600. doi:10.1161/STROKEAHA.116.016327
Murthy, S. B., Moradiya, Y., Shah, J., Merkler, A. E., Mangat, H. S., Iadacola, C., . . . Ziai, W. C. (2016). Nosocomial infections and outcomes after intracerebral hemorrhage: A population-based study. Neurocritical Care, 25(2), 178-184. doi:10.1007/s12028-016-0282-6
Naff, N. J., Hanley, D. F., Keyl, P. M., Tuhrim, S., Kraut, M., Bederson, J., . . . Schmutzhard, E. (2004). Intraventricular thrombolysis speeds blood clot resolution: Results of a pilot, prospective, randomized, double-blind, controlled trial. Neurosurgery, 54(3), 577-584. doi:10.1227/01.neu.0000108422.10842.60

96
Naff, N, Williams, M. A., Keyl, P. M., Tuhrim, S., Bullock, M. R., Mayer, S. A., Coplin, W., Narayan, R., Haines, S., Cruz-Flores, S., Zuccarello, M., Brock, D., Awad, I., Ziai, W. C., Marmarou, A., Rhoney, D., McBee, N., Lane, K., Hanley, D. F. Jr. (2011). Low-dose recombinant tissue-type plasminogen activator enhances clot resolution in brain hemorrhage: the intraventricular hemorrhage thrombolysis trial. Stroke, 42(11):3009-16. doi: 10.1161/STROKEAHA.110.610949. Epub 2011 Aug 25.
Nagasaka, T., Inao, S., & Wakabayashi, T. (2013). What does the CT angiography "spot sign" of intracerebral hemorrhage mean in modern neurosurgical settings with minimally invasive endoscopic techniques? Neurosurgical Review, 36(3), 341-348. doi:10.1007/s10143-012-0437-7
Naidech, A. M., Garg, R. K., Liebling, S., Levasseur, K., Macken, M. P., Schuele, S. U., & Batjer, H. H. (2009). Anticonvulsant use and outcomes after intracerebral hemorrhage. Stroke, 40(12), 3810-3815. doi:10.1161/STROKEAHA.109.559948
Naidech, A. M., Liebling, S. M., Rosenberg, N. F., Lindholm, P. F., Bernstein, R. A., Batjer, H. H., . . . Kwaan, H. C. (2012). Early platelet transfusion improves platelet activity and may improve outcomes after intracerebral hemorrhage. Neurocritical Care, 16(1), 82-87. doi:10.1007/s12028-011-9619-3
Neshige, S., Kuriyama, M., Yoshimoto, T., Takeshima, S., Himeno, T., Takamatsu, K., . . . Ota, S. (2015a). Seizures after intracerebral hemorrhage; risk factor, recurrence, efficacy of antiepileptic drug. Journal of the Neurological Sciences, 359(1-2), 318-322. doi:10.1016/j.jns.2015.09.358
Neshige, S., Kuriyama, M., Yoshimoto, T., Takeshima, S., Himeno, T., Takamatsu, K., . . . Ota, S. (2015b). Seizures after intracerebral hemorrhage; risk factor, recurrence, efficacy of antiepileptic drug. Journal of the Neurological Sciences, 359(1-2), 318-322. doi:10.1016/j.jns.2015.09.358
Newell, D. W., Shah, M. M., Wilcox, R., Hansmann, D. R., Melnychuk, E., Muschelli, J., & Hanley, D. F. (2011). Minimally invasive evacuation of spontaneous intracerebral hemorrhage using sonothrombolysis. Journal of Neurosurgery, 115(3), 592-601. doi:10.3171/2011.5.JNS10505
Nielsen, P. B., Larsen, T. B., Skjøth, F., Gorst-Rasmussen, A., Rasmussen, L. H., & Lip, G. Y. H. (2015). Restarting anticoagulant treatment after intracranial hemorrhage in patients with atrial fibrillation and the impact on recurrent stroke, mortality, and bleeding: A nationwide cohort study. Circulation, 132(6), 517-525. doi:10.1161/CIRCULATIONAHA.115.015735
Nielsen-Kudsk, J. E., Johnsen, S. P., Wester, P., Damgaard, D., Airaksinen, J., Lund, J., . . . Krieger, D. W. (2017). Left atrial appendage occlusion versus standard medical care in patients with atrial fibrillation and intracerebral haemorrhage: A propensity score-matched follow-up study. EuroIntervention: Journal of EuroPCR in Collaboration with the Working Group on Interventional Cardiology of the European Society of Cardiology, 13(3), 371-378. doi:10.4244/EIJ-D-17-00201
Nieuwkamp, D. J., de Gans, K., Rinkel, G. J., & Algra, A. (2000). Treatment and outcome of severe intraventricular extension in patients with subarachnoid

97
or intracerebral hemorrhage: A systematic review of the literature. Journal of Neurology, 247(2), 117-121. doi:10.1007/pl00007792
Nilsson, O. G., Lindgren, A., Brandt, L., & Säveland, H. (2002). Prediction of death in patients with primary intracerebral hemorrhage: A prospective study of a defined population. Journal of Neurosurgery, 97(3), 531-536. doi:10.3171/jns.2002.97.3.0531
Nordestgaard, B. G., & Zacho, J. (2009). Lipids, atherosclerosis and CVD risk: Is CRP an innocent bystander? Nutrition, Metabolism, and Cardiovascular Diseases: NMCD, 19(8), 521-524. doi:10.1016/j.numecd.2009.07.005
Oddo, M., Carrera, E., Claassen, J., Mayer, S. A., & Hirsch, L. J. (2009). Continuous electroencephalography in the medical intensive care unit. Critical Care Medicine, 37(6), 2051-2056. doi:10.1097/CCM.0b013e3181a00604
Ohwaki, K., Yano, E., Nagashima, H., Nakagomi, T., & Tamura, A. (2008). Impact of infection on length of intensive care unit stay after intracerebral hemorrhage. Neurocritical Care, 8(2), 271-275. doi:10.1007/s12028-007-9007-1
Orken, D. N., Kenangil, G., Ozkurt, H., Guner, C., Gundogdu, L., Basak, M., & Forta, H. (2009). Prevention of deep venous thrombosis and pulmonary embolism in patients with acute intracerebral hemorrhage. The Neurologist, 15(6), 329-331. doi:10.1097/NRL.0b013e3181a93bac
Ostábal, M. I., Sanz-Sebastián, C., Suárez-Pinilla, M. A., & del Río-Ligorit, A. (1996). [Study of electrocardiographic alterations during the acute phase of intracerebral hemorrhage and their prognostic implications]. Revista De Neurologia, 24(134), 1229-1232.
Pang, D., Sclabassi, R. J., & Horton, J. A. (1986). Lysis of intraventricular blood clot with urokinase in a canine model: Part 3. effects of intraventricular urokinase on clot lysis and posthemorrhagic hydrocephalus. Neurosurgery, 19(4), 553-572. doi:10.1227/00006123-198610000-00010
Passero, S., Rocchi, R., Rossi, S., Ulivelli, M., & Vatti, G. (2002). Seizures after spontaneous supratentorial intracerebral hemorrhage. Epilepsia, 43(10), 1175-1180.
Poli, D., Antonucci, E., Marcucci, R., Fatini, C., Alterini, B., Mannini, L., . . . Prisco, D. (2007). Risk of bleeding in very old atrial fibrillation patients on warfarin: Relationship with ageing and CHADS2 score. Thrombosis Research, 121(3), 347-352. doi:10.1016/j.thromres.2007.05.014
Prabhakaran, S., Herbers, P., Khoury, J., Adeoye, O., Khatri, P., Ferioli, S., & Kleindorfer, D. O. (2015). Is prophylactic anticoagulation for deep venous thrombosis common practice after intracerebral hemorrhage? Stroke, 46(2), 369-375. doi:10.1161/STROKEAHA.114.008006
Prass, K., Meisel, C., Höflich, C., Braun, J., Halle, E., Wolf, T., . . . Meisel, A. (2003). Stroke-induced immunodeficiency promotes spontaneous bacterial infections and is mediated by sympathetic activation reversal by poststroke T helper cell type 1-like immunostimulation. The Journal of Experimental Medicine, 198(5), 725-736. doi:10.1084/jem.20021098

98
Qureshi, A. I., & Palesch, Y. Y. (2011). Antihypertensive treatment of acute cerebral hemorrhage (ATACH) II: Design, methods, and rationale. Neurocritical Care, 15(3), 559-576. doi:10.1007/s12028-011-9538-3
Rasool, A. H. G., Rahman, A. R. A., Choudhury, S. R., & Singh, R. B. (2004). Blood pressure in acute intracerebral haemorrhage. Journal of Human Hypertension, 18(3), 187-192. doi:10.1038/sj.jhh.1001647
Reddig, R. T., Nixdorf, K. E., & Jensen, M. B. (2011). The prophylactic use of an antiepileptic drug in intracerebral hemorrhage. Clinical Neurology and Neurosurgery, 113(10), 895-897. doi:10.1016/j.clineuro.2011.07.008
Renou, P., Thambo, J., Iriart, X., Nicot, S., Kabore, N., Jalal, Z., . . . Sibon, I. (2017). Left atrial appendage closure in patients with atrial fibrillation and previous intracerebral hemorrhage. Journal of Stroke and Cerebrovascular Diseases: The Official Journal of National Stroke Association, 26(3), 545-551. doi:10.1016/j.jstrokecerebrovasdis.2016.11.126
Rief, P., Raggam, R. B., Hafner, F., Avian, A., Hackl, G., Cvirn, G., . . . Gary, T. (2018). Calculation of HAS-BLED score is useful for early identification of venous thromboembolism patients at high risk for major bleeding events: A prospective outpatients cohort study. Seminars in Thrombosis and Hemostasis, 44(4), 348-352. doi:10.1055/s-0037-1607433
Robertson, J. S., Maraqa, M. I., & Jennett, B. (1973). Ventriculoperitoneal shunting for hydrocephalus. British Medical Journal, 2(5861), 289-292. doi:10.1136/bmj.2.5861.289
Roldán, V., Marín, F., Manzano-Fernández, S., Gallego, P., Vílchez, J. A., Valdés, M., . . . Lip, G. Y. H. (2013). The HAS-BLED score has better prediction accuracy for major bleeding than CHADS2 or CHA2DS2-VASc scores in anticoagulated patients with atrial fibrillation. Journal of the American College of Cardiology, 62(23), 2199-2204. doi:10.1016/j.jacc.2013.08.1623
Rosand, J., Eckman, M. H., Knudsen, K. A., Singer, D. E., & Greenberg, S. M. (2004). The effect of warfarin and intensity of anticoagulation on outcome of intracerebral hemorrhage. Archives of Internal Medicine, 164(8), 880-884. doi:10.1001/archinte.164.8.880
Rossi, C., De Herdt, V., Dequatre-Ponchelle, N., Hénon, H., Leys, D., & Cordonnier, C. (2013). Incidence and predictors of late seizures in intracerebral hemorrhages. Stroke, 44(6), 1723-1725. doi:10.1161/STROKEAHA.111.000232
Sahay, S., Nombela-Franco, L., Rodes-Cabau, J., Jimenez-Quevedo, P., Salinas, P., Biagioni, C., . . . Macaya, C. (2017). Efficacy and safety of left atrial appendage closure versus medical treatment in atrial fibrillation: A network meta-analysis from randomised trials. Heart (British Cardiac Society), 103(2), 139-147. doi:10.1136/heartjnl-2016-309782
Saloheimo, P., Ahonen, M., Juvela, S., Pyhtinen, J., Savolainen, E., & Hillbom, M. (2006). Regular aspirin-use preceding the onset of primary intracerebral hemorrhage is an independent predictor for death. Stroke, 37(1), 129-133. doi:10.1161/01.STR.0000196991.03618.31
Saloheimo, P., Lapp, T., Juvela, S., & Hillbom, M. (2006). The impact of functional status at three months on long-term survival after spontaneous

99
intracerebral hemorrhage. Stroke, 37(2), 487-491. doi:10.1161/01.STR.0000198868.78546.fc
Sato, S., Arima, H., Hirakawa, Y., Heeley, E., Delcourt, C., Beer, R., . . . Anderson, C. S. (2014). The speed of ultraearly hematoma growth in acute intracerebral hemorrhage. Neurology, 83(24), 2232-2238. doi:10.1212/WNL.0000000000001076
Scaggiante, J., Zhang, X., Mocco, J., & Kellner, C. P. (2018). Minimally invasive surgery for intracerebral hemorrhage. Stroke, 49(11), 2612-2620. doi:10.1161/STROKEAHA.118.020688
Skaf, E., Stein, P. D., Beemath, A., Sanchez, J., Bustamante, M. A., & Olson, R. E. (2005). Venous thromboembolism in patients with ischemic and hemorrhagic stroke. The American Journal of Cardiology, 96(12), 1731-1733. doi:10.1016/j.amjcard.2005.07.097
Sproston, N. R., & Ashworth, J. J. (2018). Role of C-reactive protein at sites of inflammation and infection. Frontiers in Immunology, 9, 754. doi:10.3389/fimmu.2018.00754
Staykov, D., Huttner, H. B., Struffert, T., Ganslandt, O., Doerfler, A., Schwab, S., & Bardutzky, J. (2009). Intraventricular fibrinolysis and lumbar drainage for ventricular hemorrhage. Stroke, 40(10), 3275-3280. doi:10.1161/STROKEAHA.109.551945
Stein, M., Luecke, M., Preuss, M., Boeker, D., Joedicke, A., & Oertel, M. F. (2010). Spontaneous intracerebral hemorrhage with ventricular extension and the grading of obstructive hydrocephalus: The prediction of outcome of a special life-threatening entity. Neurosurgery, 67(5), 1243-1251; discussion 1252. doi:10.1227/NEU.0b013e3181ef25de
Stein, P. D., Goldhaber, S. Z., & Henry, J. W. (1995). Alveolar-arterial oxygen gradient in the assessment of acute pulmonary embolism. Chest, 107(1), 139-143. doi:10.1378/chest.107.1.139
Steiner, T., Al-Shahi Salman, R., Beer, R., Christensen, H., Cordonnier, C., Csiba, L., . . . Wagner, M. (2014). European stroke organisation (ESO) guidelines for the management of spontaneous intracerebral hemorrhage. International Journal of Stroke: Official Journal of the International Stroke Society, 9(7), 840-855. doi:10.1111/ijs.12309
Sung, C. Y., & Chu, N. S. (1989). Epileptic seizures in intracerebral haemorrhage. Journal of Neurology, Neurosurgery, and Psychiatry, 52(11), 1273-1276. doi:10.1136/jnnp.52.11.1273
Sykora, M., Diedler, J., Poli, S., Rizos, T., Turcani, P., Veltkamp, R., & Steiner, T. (2011). Autonomic shift and increased susceptibility to infections after acute intracerebral hemorrhage. Stroke, 42(5), 1218-1223. doi:10.1161/STROKEAHA.110.604637
Szaflarski, J. P., Rackley, A. Y., Kleindorfer, D. O., Khoury, J., Woo, D., Miller, R., . . . Kissela, B. M. (2008). Incidence of seizures in the acute phase of stroke: A population-based study. Epilepsia, 49(6), 974-981. doi:10.1111/j.1528-1167.2007.01513.x
Takahashi, H., Urano, T., Nagai, N., Takada, Y., & Takada, A. (1998). Progressive expansion of hypertensive intracerebral hemorrhage by coagulopathy.

100
American Journal of Hematology, 59(2), 110-114. doi:10.1002/(sici)1096-8652(199810)59:23.0.co;2-0
Temes, R. E., Tessitore, E., Schmidt, J. M., Naidech, A. M., Fernandez, A., Ostapkovich, N. D., . . . Parra, A. (2010). Left ventricular dysfunction and cerebral infarction from vasospasm after subarachnoid hemorrhage. Neurocritical Care, 13(3), 359-365. doi:10.1007/s12028-010-9447-x
Tetri, S., Hakala, J., Juvela, S., Saloheimo, P., Pyhtinen, J., Rusanen, H., . . . Hillbom, M. (2008). Safety of low-dose subcutaneous enoxaparin for the prevention of venous thromboembolism after primary intracerebral haemorrhage. Thrombosis Research, 123(2), 206-212. doi:10.1016/j.thromres.2008.01.018
Tetri, S., Juvela, S., Saloheimo, P., Pyhtinen, J., & Hillbom, M. (2009). Hypertension and diabetes as predictors of early death after spontaneous intracerebral hemorrhage. Journal of Neurosurgery, 110(3), 411-417. doi:10.3171/2008.8.JNS08445
Tetri, S., Mäntymäki, L., Juvela, S., Saloheimo, P., Pyhtinen, J., Rusanen, H., & Hillbom, M. (2008). Impact of ischemic heart disease and atrial fibrillation on survival after spontaneous intracerebral hemorrhage. Journal of Neurosurgery, 108(6), 1172-1177. doi:10.3171/JNS/2008/108/6/1172
Trinka, E., & Kälviäinen, R. (2017). 25 years of advances in the definition, classification and treatment of status epilepticus. Seizure, 44, 65-73. doi:10.1016/j.seizure.2016.11.001
Urra, X., Cervera, A., Obach, V., Climent, N., Planas, A. M., & Chamorro, A. (2009). Monocytes are major players in the prognosis and risk of infection after acute stroke. Stroke, 40(4), 1262-1268. doi:10.1161/STROKEAHA.108.532085
van Asch, C. J., Luitse, M. J., Rinkel, G. J., van der Tweel, I., Algra, A., & Klijn, C. J. (2010). Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: A systematic review and meta-analysis. The Lancet. Neurology, 9(2), 167-176. doi:10.1016/S1474-4422(09)70340-0
Vespa, P. M., O'Phelan, K., Shah, M., Mirabelli, J., Starkman, S., Kidwell, C., . . . Martin, N. A. (2003). Acute seizures after intracerebral hemorrhage: A factor in progressive midline shift and outcome. Neurology, 60(9), 1441-1446. doi:10.1212/01.wnl.0000063316.47591.b4
Vespa P, Hanley D, Betz J, Hoffer A, Engh J, Carter R, Nakaji P, Ogilvy C, Jallo J, Selman W, Bistran-Hall A, Lane K, McBee N, Saver J, Thompson RE, Martin N. (2016). ICES (Intraoperative Stereotactic Computed Tomography-Guided Endoscopic Surgery) for Brain Hemorrhage: A Multicenter Randomized Controlled Trial. Stroke, 47(11):2749-2755.
Wang, J., & Doré, S. (2007). Inflammation after intracerebral hemorrhage. Journal of Cerebral Blood Flow and Metabolism: Official Journal of the International Society of Cerebral Blood Flow and Metabolism, 27(5), 894-908. doi:10.1038/sj.jcbfm.9600403
Waqar, M., Ellenbogen, J. R., Stovell, M. G., Al-Mahfoudh, R., Mallucci, C., & Jenkinson, M. D. (2016). Long-term outcomes of endoscopic third

101
ventriculostomy in adults. World Neurosurgery, 94, 386-393. doi:10.1016/j.wneu.2016.07.028
Warlow, C., Ogston, D., & Douglas, A. S. (1976). Deep venous thrombosis of the legs after strokes: Part 2-natural history. British Medical Journal, 1(6019), 1181-1183.
Wartenberg, K. E., & Mayer, S. A. (2007). Reducing the risk of ICH enlargement. Journal of the Neurological Sciences, 261(1-2), 99-107. doi:10.1016/j.jns.2007.04.044
Webb, A. J. S., Ullman, N. L., Mann, S., Muschelli, J., Awad, I. A., & Hanley, D. F. (2012). Resolution of intraventricular hemorrhage varies by ventricular region and dose of intraventricular thrombolytic: The clot lysis: Evaluating accelerated resolution of IVH (CLEAR IVH) program. Stroke, 43(6), 1666-1668. doi:10.1161/STROKEAHA.112.650523
Weinstein, R., Ess, K., Sirdar, B., Song, S., & Cutting, S. (2017). Primary intraventricular hemorrhage: Clinical characteristics and outcomes. Journal of Stroke and Cerebrovascular Diseases: The Official Journal of National Stroke Association, 26(5), 995-999. doi:10.1016/j.jstrokecerebrovasdis.2016.11.114
Weisberg, L. A., Shamsnia, M., & Elliott, D. (1991). Seizures caused by nontraumatic parenchymal brain hemorrhages. Neurology, 41(8), 1197-1199.
Westendorp, W. F., Nederkoorn, P. J., Vermeij, J., Dijkgraaf, M. G., & van de Beek, D. (2011). Post-stroke infection: A systematic review and meta-analysis. BMC Neurology, 11, 110. doi:10.1186/1471-2377-11-110
Whitworth JA. World Health organization, International society of hypertension writing group. (2003). WHO/International society of hypertension statement on management of hypertension. J hypertens, 21, 1983-1992.
Witt, D. M., Clark, N. P., Martinez, K., Schroeder, A., Garcia, D., Crowther, M. A., . . . Delate, T. (2015). Risk of thromboembolism, recurrent hemorrhage, and death after warfarin therapy interruption for intracranial hemorrhage. Thrombosis Research, 136(5), 1040-1044. doi:10.1016/j.thromres.2015.10.002
Woo, D., Haverbusch, M., Sekar, P., Kissela, B., Khoury, J., Schneider, A., . . . Broderick, J. (2004). Effect of untreated hypertension on hemorrhagic stroke. Stroke, 35(7), 1703-1708. doi:10.1161/01.STR.0000130855.70683.c8
Woo, D., Sauerbeck, L. R., Kissela, B. M., Khoury, J. C., Szaflarski, J. P., Gebel, J., . . . Broderick, J. P. (2002). Genetic and environmental risk factors for intracerebral hemorrhage: Preliminary results of a population-based study. Stroke, 33(5), 1190-1195. doi:10.1161/01.str.0000014774.88027.22
Woo, K., Yang, S., & Cho, K. (2012). Seizures after spontaneous intracerebral hemorrhage. Journal of Korean Neurosurgical Society, 52(4), 312-319. doi:10.3340/jkns.2012.52.4.312
Yang, T., Lin, W., Chang, W., Ho, J., Wang, H., Tsai, N., . . . Lu, C. (2009a). Predictors and outcome of seizures after spontaneous intracerebral hemorrhage. clinical article. Journal of Neurosurgery, 111(1), 87-93. doi:10.3171/2009.2.JNS081622

102
Yang, T., Lin, W., Chang, W., Ho, J., Wang, H., Tsai, N., . . . Lu, C. (2009b). Predictors and outcome of seizures after spontaneous intracerebral hemorrhage. clinical article. Journal of Neurosurgery, 111(1), 87-93. doi:10.3171/2009.2.JNS081622
Zacharia, B. E., Vaughan, K. A., Hickman, Z. L., Bruce, S. S., Carpenter, A. M., Petersen, N. H., . . . Connolly, E. S. (2012). Predictors of long-term shunt-dependent hydrocephalus in patients with intracerebral hemorrhage requiring emergency cerebrospinal fluid diversion. Neurosurgical Focus, 32(4), E5. doi:10.3171/2012.2.FOCUS11372
Zeng, Z., Hu, Z., & Zhang, J. (2015). Venous thromboembolism prevention during the acute phase of intracerebral hemorrhage. Journal of the Neurological Sciences, 358(1-2), 3-8. doi:10.1016/j.jns.2015.08.026
Zhang, D., Li, F., Li, X., & Du, G. (2018). Effect of intermittent pneumatic compression on preventing deep vein thrombosis among stroke patients: A systematic review and meta-analysis. Worldviews on Evidence-Based Nursing, 15(3), 189-196. doi:10.1111/wvn.12288
Zhang, Z., Li, X., Liu, Y., Shao, Y., Xu, S., & Yang, Y. (2007). Application of neuroendoscopy in the treatment of intraventricular hemorrhage. Cerebrovascular Diseases (Basel, Switzerland), 24(1), 91-96. doi:10.1159/000103122
Zhao, J., Liu, Y., & Li, H. (2015). Aspiration-related acute respiratory distress syndrome in acute stroke patient. PloS One, 10(3), e0118682. doi:10.1371/journal.pone.0118682
Zhou, X., Chen, J., Li, Q., Ren, G., Yao, G., Liu, M., . . . Xie, P. (2012). Minimally invasive surgery for spontaneous supratentorial intracerebral hemorrhage: A meta-analysis of randomized controlled trials. Stroke, 43(11), 2923-2930. doi:10.1161/STROKEAHA.112.667535
Ziai, W. C., Tuhrim, S., Lane, K., McBee, N., Lees, K., Dawson, J., . . . Hanley, D. F. (2014). A multicenter, randomized, double-blinded, placebo-controlled phase III study of clot lysis evaluation of accelerated resolution of intraventricular hemorrhage (CLEAR III). International Journal of Stroke: Official Journal of the International Stroke Society, 9(4), 536-542. doi:10.1111/ijs.12097

103
Original publications I Löppönen P, Qian C, Tetri S, Juvela S, Huhtakangas J, Bode MK, Hillbom M.
(2014). Predictive value of C-reactive protein for the outcome after primary intracerebral hemorrhage. Journal of neurosurgery, 121(6), 1374-9. II Immediate, early and late seizures after primary intracerebral hemorrhage.
Qian C, Löppönen P, Tetri S, Huhtakangas J, Juvela S, Turtiainen HM, Bode MK, Hillbom. (2014). Immediate, early and late seizures after primary intracerebral hemorrhage. Epilepsy Res.108(4):732-9.
III Qian C., Huhtakangas J., Juvela S., Bode M., Tatlisumak T., Numminen H., Ollikainen J., Luostarinen L., Kupila L., Tetri S. Early vs. late enoxaparin for prevention of venous thromboembolism in patients with ICH. Manuscript.
Reprinted with permission from the American association of neurological surgeons (I), Elsevier ltd. (II).
Original publications are not included in the electronic version of the dissertation.

103

I


J Neurosurg 121:1374–1379, 2014
1374 J Neurosurg / Volume 121 / December 2014
©AANS, 2014
Primary intracerebral hemorrhage (ICH) is the most devastating form of stroke, with high case fatality and morbidity. The outcome remains difficult to
predict, and an erroneous decision regarding treatment limitations can further impair the outcome.23 It is never-theless important to try to predict the outcome soon after admission. Well-known factors affecting the outcome in-clude the clinical and radiological severity of the bleed-ing, older age, infection,9 and the use of anticoagulants.6,15 The predictive values of laboratory parameters have been poorly investigated.
Elevated levels of C-reactive protein (CRP), a nonspe-cific inflammatory marker of tissue trauma and infection, have been shown to be associated with a poor outcome and an increased risk of death after ischemic stroke10 and aneurysmal subarachnoid hemorrhage,13 but both insig-nificant and significant associations between an elevated CRP concentration on admission and 30-day mortality have been reported among patients with primary ICH.1,7 On the other hand, low CRP levels seem to be associ-ated with a good outcome for patients with primary ICH.4 Poor outcomes have been reported to be associated with elevated CRP levels in infected patients,9 and CRP levels measured more than 48 hours after the onset of bleeding seem to predict mortality and a poor outcome better than values measured at admission.8
Predictive value of C-reactive protein for the outcome after primary intracerebral hemorrhage
Clinical articlePekka LöPPönen, M.D.,1 Cheng Qian, M.D.,1 SaMi TeTri, M.D., Ph.D.,1 SePPo JuveLa, M.D., Ph.D.,4 Juha huhTakangaS, M.D., Ph.D.,2 MiChaeLa k. BoDe, M.D., Ph.D.,3 anD MaTTi hiLLBoM, M.D., Ph.D.2
Departments of 1Neurosurgery, 2Neurology, and 3Diagnostic Radiology, Oulu University Hospital, Oulu; and 4Clinical Neurosciences, University of Helsinki, Finland
Object. Primary intracerebral hemorrhage (ICH) carries high morbidity and mortality rates. Several factors have been suggested as predicting the outcome. The value of C-reactive protein (CRP) levels in predicting a poor outcome is unclear, and findings have been contradictory. In their population-based cohort, the authors tested whether, inde-pendent of confounding factors, elevated CRP levels on admission (< 24 hours after ictus) are associated with an unfavorable outcome.
Methods. The authors identified all patients who suffered primary ICH between 1993 and 2008 among the popu-lation of Northern Ostrobothnia, Finland, and from the laboratory records they extracted the CRP values at admission. Independent predictors of an unfavorable outcome (moderate disability or worse according to the Glasgow Outcome Scale at 3 months) were tested by unconditional logistic regression in a model including all the well-established con-founding factors and CRP on admission.
Results. Of 961 patients, 807 (84%) had CRP values available within 24 hours of admission, and multivariable analysis showed elevated CRP at that point to be associated with an unfavorable outcome (OR 1.41 per 10 mg/L [95% CI 1.09–1.81], p < 0.01), together with diabetes mellitus (OR 1.99 [95% CI 1.09–3.64], p < 0.05), age (1.06 per year [95% CI 1.04–1.08], p < 0.001), low Glasgow Coma Scale score (0.75 per unit [95% CI 0.67–0.84], p < 0.001), hematoma size (1.05 per ml [95% CI 1.03–1.07], p < 0.001), and the presence of an intraventricular hemorrhage (2.70 [95% CI 1.66–4.38], p < 0.001). Subcortical location predicted a favorable outcome (0.33 [95% CI 0.20–0.54], p < 0.001).
Conclusions. Elevated CRP on admission is an independent predictor of an unfavorable outcome and is only slightly associated with the clinical and radiological severity of the bleeding.(http://thejns.org/doi/abs/10.3171/2014.7.JNS132678)
key WorDS • intracerebral hemorrhage • C-reactive protein • outcome • predictive value • vascular disorders
Abbreviations used in this paper: CRP = C-reactive protein; GCS = Glasgow Coma Scale; GOS = Glasgow Outcome Scale; ICH = intracerebral hemorrhage; IVH = intraventricular hemorrhage.

J Neurosurg / Volume 121 / December 2014
CRP as a predictor of outcome after ICH
1375
Since the available data do not prove convincingly that elevated CRP, if observed soon after the onset of bleeding and in the absence of infection, is also predic-tive of a poor outcome among patients with primary ICH, we set out to test the hypothesis that elevated CRP on admission is associated with the severity of primary ICH and thereby predict an unfavorable outcome.
MethodsThe protocol was approved by the ethics committee
of the Northern Ostrobothnia Hospital District.
Patient PopulationWe conducted a survey, identifying all patients among
the population of Northern Ostrobothnia, Finland, who were treated for primary ICH at Oulu University Hospital from January 1, 1993, to December 31, 2008. The hospital is the only one serving acute stroke patients in this area (population of 356,026 in 1993 and 389,671 in 2008). We excluded patients not living in the hospital’s catchment area and those who had a brain tumor, aneurysm, vascu-lar malformation, hematological malignancy, hemophilia, or head trauma. Six patients died before reaching the hos-pital, the diagnoses for whom were confirmed by autopsy. Altogether, 961 patients with first-ever primary ICH were identified. We then excluded patients whose CRP values were obtained more than 24 hours after the onset of the stroke, leaving a series of 813 patients with CRP values taken within 24 hours of ictus. The series included 114 patients who underwent surgery. The CRP values of 6 of these patients were obtained only after the operation (but still within 24 hours of ictus); these patients were also ex-cluded. Thus, a total of 807 patients (84%) were included in the final analysis.
Neuroradiological MethodsPrimary ICH was verified with a CT scan on admis-
sion by experienced neuroradiologists. The locations and volumes of primary ICHs were determined, and the pres-ence of intraventricular hemorrhage was recorded. As in our previous work,11 measurement of ICH volumes was performed as either with a sum of individual slice vol-umes2 or with an easier ABC/2 method.14 Presence of in-traventricular hemorrhage (IVH) was dichotomized (yes/no). If aneurysms or arteriovenous malformations were suspected as a cause for the hemorrhage, CT, MR, or digi-tal subtraction angiography was performed immediately. Survivors were checked for other structural abnormali-ties by performing follow-up imaging (CT or MRI) 2–3 months after the hemorrhage.
Clinical DataThe patient’s clinical condition on admission at the
emergency department was assessed in terms of the Glasgow Coma Scale (GCS) score.18 Scores were miss-ing in 7 cases. Information on previous diseases, blood pressure history, and the use of anticoagulants and oth-er medications was extracted from the hospital records. The patients were considered to be hypertensive if their
blood pressure readings preceding the index stroke had repeatedly exceeded 160/90 mm Hg, in accordance with the WHO/ISH (World Health Organization/International Society of Hypertension) statement,22 or if they were tak-ing antihypertensive medication. Patients were recorded as having diabetes mellitus if they were taking oral hy-poglycemic agents or insulin. Cardiac disease included myocardial infarction, coronary artery disease, heart failure, and/or atrial fibrillation. Blood samples for CRP analysis were obtained in the emergency department or on the ward the next morning. C-reactive protein values were recorded on a daily basis, and CRP was analyzed using a turbidimetric method (normal values < 10 mg/L, coefficient of variation < 6%; Siemens Activa).
Outcome MeasurementsDeath records were obtained from the Causes of
Death Register and were checked for the entire patient series. Patients were followed up for 3 months at our out-patient clinic or on the hospital’s rehabilitation ward, with the exception of some who showed exceptionally good recovery on discharge and were assumed to have main-tained this state for at least 3 months unless they were readmitted. All patients who experienced deterioration or rebleeding were readmitted to our hospital. The outcome was assessed according to the Glasgow Outcome Scale (GOS);12 patients with a score of 5 (good recovery) were considered to have a favorable outcome, whereas patients with scores of 1–4 (death, persistent vegetative state, or severe or moderate disability) were considered to have an unfavorable outcome.
ManagementImmediately after admission the physician on duty
chose the most appropriate treatment for the patient ac-cording to the hospital’s treatment protocols at that time. Standard care, reversal of the warfarin effect, and throm-boprophylaxis were performed according to institutional protocols. Hematomas were evacuated by standard crani-otomy or through a bur hole in 114 cases.
Statistical AnalysisData were analyzed using IBM SPSS Statistics for
Windows (version 20.0, IBM Corp.). Categorical vari-ables were compared by conventional statistical methods including Pearson’s chi-square test and Fisher’s exact test, and continuous variables were compared by t-tests, the Mann-Whitney U-test, a 1-way ANOVA, and/or the Kruskal-Wallis test for nonparametric ANOVA. Uni-variate associations between continuous variables were tested using Spearman rank correlation coefficients (rs). Predictors of an unfavorable outcome 3 months after pri-mary ICH were searched for using unconditional logis-tic regression. Maximum-likelihood forward elimination procedures were used, with the variables selected on the basis of their probability values (p < 0.05). The following variables were tested: sex, age, presence of cardiac dis-ease, presence of diabetes mellitus, hematoma size (per ml), GCS score (per unit), IVH, subcortical hematoma location, hematoma evacuation, use of warfarin, and CRP

P. Löppönen et al.
1376 J Neurosurg / Volume 121 / December 2014
level (per 10 mg/L) on admission. All significant predic-tors found in stepwise logistic regression were included in the final model. A 2-tailed p value < 0.05 was considered statistically significant.
ResultsThe baseline and clinical characteristics of the pa-
tients according to outcome are shown in Table 1. One hundred ninety-two patients (24%) had a favorable out-come and 615 (76%) had an unfavorable outcome within 3 months. The patients with unfavorable outcome were significantly more often women and older than those with a favorable outcome. These patients also significantly more often had diabetes mellitus, cardiac disease, warfa-rin medication, a higher CRP value on admission, a lower GCS score, a larger hematoma, intraventricular bleeding, an evacuated hematoma, and infectious complications (Table 1). Infectious complications were observed in 216 patients and included urinary tract infections in 8 (4%) of 192 patients with a favorable outcome and 80 (13%) of 615 patients with an unfavorable outcome (p < 0.001) and pneumonia in 3 (2%) of 192 patients with a favorable out-come and 125 (20%) of 615 patients with an unfavorable outcome (p < 0.001).
C-reactive protein values on admission were ana-lyzed according to characteristics and outcome (Table 2). Due to the skewed distributions of the CRP values, nonparametric statistical methods were used. C-reactive protein values on admission were significantly higher in patients with cardiac disease, diabetes mellitus, warfarin treatment, and impaired outcome at 3 months. There was
a threshold in CRP values between good recovery and unfavorable outcome. The size of the hematoma correlat-ed with admission CRP levels (rs = 0.084, p = 0.018), but admission GCS score correlated significantly with CRP levels only more than 24 hours after primary ICH (at ad-mission: rs = 0.067, p = 0.060; after 24 hours: rs = 0.237, p < 0.001). Admission CRP levels did not differ clearly in terms of later diagnoses of infections, but later CRP levels did show such a pattern (data not shown, p < 0.01).
The predictors of an unfavorable outcome are shown in Table 3. In multivariable analysis the significant predic-tors of an unfavorable outcome were older age, diabetes mellitus, a low GCS score on admission, a large hemato-ma, the presence of intraventricular bleeding, nonsubcor-tical location, and elevated CRP value on admission. The risk of an unfavorable outcome increased 1.4-fold in the multivariable analysis for every 10-mg/L increase in CRP on admission (Table 3).
The patients who developed pneumonia later (n = 128) had very high CRP values after ictus relative to those without pneumonia (47.9 ± 68.0 vs 21.5 ± 35.8 within 48 hours and 67.3 ± 59.1 vs 25.5 ± 42.5 within 96 hours, p < 0.001 for both). We then excluded the patients with pneu-monia and repeated multivariable analysis for an unfavor-able/favorable outcome, but the results were unchanged: high CRP on admission still predicted an unfavorable outcome (OR 1.45 per 10 mg/L [95% CI 1.10–1.90], p < 0.01).
DiscussionOur results demonstrate that an elevated CRP value,
TABLE 1: Baseline and clinical characteristics of the patients with primary ICH, according to outcome*
VariableFavorable Outcome
(n = 192)Unfavorable Outcome
(n = 615) Total (n = 807) p Value
mean age in yrs 64 ± 11 71 ± 12 69 ± 12 <0.001men 116 (60) 320 (52) 436 (54) 0.042previous diseases hypertension 124 (65) 390 (63) 514 (64) 0.769 diabetes 20 (10) 125 (20) 145 (18) 0.002 cardiac disease 52 (27) 257 (42) 309 (38) <0.001warfarin medication 19 (10) 128 (21) 147 (18) <0.001mean INR on arrival in units 1.2 ± 0.6 1.6 ± 1.1 1.5 ± 1.0 <0.001mean CRP value per mg/L 7.3 ± 5.5 12.6 ± 26.0 11.3 ± 23.0 0.005median GCS score (25th, 75th percentiles) 15 (14, 15) 13 (6, 15) 14 (10, 15) <0.001mean hematoma vol in ml 12 ± 16 41 ± 45 34 ± 42 <0.001intraventricular hemorrhage 31 (16) 339 (55) 370 (46) <0.001subcortical hematoma 64 (33) 173 (28) 237 (29) 0.167hematoma evacuation 11 (6) 98 (16) 109 (14) <0.001infectious complications urinary tract infection 8 (4) 80 (13) 88 (11) <0.001 pneumonia 3 (2) 125 (20) 128 (16) <0.001dead w/in 3 mos 0 (0) 280 (46) 280 (35) <0.001
* Values are number of patients (%) unless noted otherwise. Mean values are presented as the mean ± SD. INR = international normalized ratio.

J Neurosurg / Volume 121 / December 2014
CRP as a predictor of outcome after ICH
1377
if observed on admission within 24 hours after ictus, in-dependent of confounding factors predicts an unfavorable outcome following primary ICH. The effect of elevated CRP on admission cannot be explained by preexisting heart disease, diabetes mellitus, and severity of the bleed-ing or infections.
The mechanisms behind hemorrhage-induced brain damage and the development of perihematomal edema are not clear, but inflammation is believed to be one im-portant factor involved in the process.1,21 Castillo et al. hypothesized that certain regulatory pathways activated after primary ICH can prevent secondary brain dam-age in cases of small hematomas but can produce the opposite effect when larger hematomas are concerned.5 In addition, high levels of CRP were found around the hemorrhagic clot in patients with large hematomas who died within 48 hours of primary ICH.8 C-reactive protein, mainly produced in the hepatocytes in response to cyto-kines, is a sensitive nonspecific marker of inflammation and infection. Mildly elevated levels have been found in patients with hypertension, diabetes, heart disease, and smoking.10 Hypertension and diabetes are also impor-tant risk factors for primary ICH.3,17 In our series cardiac disease and diabetes mellitus, but not hypertension, were significantly associated with elevated CRP. Cardiac dis-ease and diabetes have also been found as predictors of death after ICH.19,20 In the present multivariable analy-sis, however, cardiac disease was not a predictor of an unfavorable outcome, suggesting that primary ICH itself influences CRP more than does cardiac disease.
A slightly elevated CRP level on admission was found in many of the patients who later developed pneumonia. These patients showed a poor clinical condition soon af-ter the onset of stroke. Aspiration leads to pneumonia, and it may be aspiration that could explain the high CRP on admission. However, CRP can increase up to 1000-fold within a few hours after the onset of other inflammatory stimuli such as tissue necrosis and trauma.16 The response reaches a peak at 48 hours after the initial stimulus and falls to baseline levels within 7–12 days once the inflam-matory stimulus is over.16
In our series the predictive value of elevated CRP for an unfavorable outcome persisted even after exclusion of the patients who later developed pneumonia, imply-ing that aspiration and subsequent clinical pneumonia did not explain the association between elevated CRP on admission and an unfavorable outcome. We assume that the severity of the brain trauma is independently associ-ated with high CRP on admission and thereby also with a poor outcome. This cannot be confirmed in our series, however, and the reason for the independent role of CRP on admission in predicting a poor outcome remains to be elucidated.
Serial CRP measurements taken on consecutive days could predict the outcome after primary ICH better than a single CRP taken at admission.13 This was evident in our series, where not only the patients who already had elevat-ed CRP on admission but also those who had an appre-ciable increase in CRP within 3 days had an unfavorable outcome. Such an increase in CRP after admission was fre-quently associated with pneumonia. Patients who are in a
TABLE 2: C-reactive protein values of patients with primary ICH on admission, according to patient characteristics and outcomes*
VariableNo. of
PatientsMean Admission
CRP Value per mg/L† p Value‡
all patients 807 11.3 ± 23.0sex NS men 436 12.7 ± 28.6 women 371 9.7 ± 13.6hypertonia NS yes 514 10.1 ± 20.2 no 293 13.4 ± 27.1diabetes mellitus 0.049 yes 145 12.9 ± 20.5 no 662 10.9 ± 23.5cardiac disease 0.002 yes 309 12.9 ± 25.8 no 498 10.3 ± 21.0warfarin 0.020 yes 147 13.1 ± 20.8 no 660 10.9 ± 23.4hematoma size NS <30 ml 511 9.7 ± 14.7 ≥30 ml 295 14.1 ± 32.5IVH NS yes 370 13.0 ± 29.6 no 436 9.9 ± 15.2subcortical location NS yes 237 13.6 ± 33.1 no 570 10.3 ± 17.0urinary tract infection 0.038 yes 88 13.4 ± 20.7 no 715 11.1 ± 23.3pneumonia NS yes 128 17.1 ± 37.7 no 675 10.2 ± 18.8hematoma evacuation NS yes 109 14.6 ± 41.6 no 698 10.8 ± 18.4GCS score NS 3–8 172 13.4 ± 23.3 9–12 140 11.3 ± 21.6 13–15 489 10.0 ± 19.2GOS score 0.004 5 192 7.3 ± 5.5 4 143 10.6 ± 17.6 3 189 9.9 ± 14.7 2 6 6.8 ± 3.4 1 277 15.5 ± 34.4
* NS = not significant.† Presented as ± SD.‡ Mann-Whitney, except for GCS and GOS scores, where Kruskal-Wallis ANOVA was used.

P. Löppönen et al.
1378 J Neurosurg / Volume 121 / December 2014
poorer clinical condition and have infections a few days af-ter the ictus do show a less favorable outcome than others.
The strengths of this study lie in the strict inclusion criteria, the relatively large, homogeneous patient series, and the population-based design. The radiological analy-ses were performed carefully, and those responsible were blinded to the case histories. We were also able to take into account all of the well-known potential risk factors for the outcome following primary ICH and adjust for them in the analyses. One limitation was that we had to exclude 16% of the original patients because of a lack of admission CRP data. These patients who were excluded had the same mean hematoma size as those enrolled in the study, so we believe that this did not cause any notable selection bias. Another limitation was the retrospective, observational study design. Our patient population was nevertheless large enough to obtain the necessary statisti-cal power to show a significant independent association between CRP levels on admission and the outcome fol-lowing primary ICH. The result did not change even after excluding the patients who later developed pneumonia. Even so, some patients with a poor outcome may have had unnoticed aspirations on admission to the hospital that increased the admission CRP value.
ConclusionsAn elevated CRP level on admission is an inde-
pendent risk factor for an unfavorable outcome among patients with ICH and cannot be explained by preexist-ing heart disease, diabetes, or infections and severity of bleeding. Elevated CRP on admission can be a sign of unnoticed aspiration among patients with a poor clinical condition on admission, or in the absence of aspiration, it may suggest the presence of a severe brain trauma.
Disclosure
The authors report no conflict of interest concerning the mate-rials or methods used in this study or the findings specified in this paper.
Author contributions to the study and manuscript preparation
include the following. Conception and design: Löppönen, Qian, Tetri, Juvela, Hillbom. Acquisition of data: all authors. Analysis and interpretation of data: all authors. Drafting the article: all authors. Critically revising the article: all authors. Reviewed submitted ver-sion of manuscript: all authors. Approved the final version of the manuscript on behalf of all authors: Löppönen. Statistical analysis: Löppönen, Tetri, Juvela, Hillbom. Study supervision: Tetri, Juvela, Hillbom.
References
1. Alexandrova ML, Danovska MP: Serum C-reactive protein and lipid hydroperoxides in predicting short-term clinical outcome after spontaneous intracerebral hemorrhage. J Clin Neurosci 18:247–252, 2011
2. Broderick JP, Brott TG, Duldner JE, Tomsick T, Huster G: Volume of intracerebral hemorrhage. A powerful and easy-to-use predictor of 30-day mortality. Stroke 24:987–993, 1993
3. Brott T, Thalinger K, Hertzberg V: Hypertension as a risk fac-tor for spontaneous intracerebral hemorrhage. Stroke 17:1078–1083, 1986
4. Castellanos M, Leira R, Tejada J, Gil-Peralta A, Dávalos A, Castillo J: Predictors of good outcome in medium to large spontaneous supratentorial intracerebral haemorrhages. J Neurol Neurosurg Psychiatry 76:691–695, 2005
5. Castillo J, Dávalos A, Alvarez-Sabín J, Pumar JM, Leira R, Silva Y, et al: Molecular signatures of brain injury after intra-cerebral hemorrhage. Neurology 58:624–629, 2002
6. Cucchiara B, Messe S, Sansing L, Kasner S, Lyden P: Hema-toma growth in oral anticoagulant related intracerebral hem-orrhage. Stroke 39:2993–2996, 2008
7. Di Napoli M, Godoy DA, Campi V, del Valle M, Piñero G, Mirofsky M, et al: C-reactive protein level measurement im-proves mortality prediction when added to the spontaneous intracerebral hemorrhage score. Stroke 42:1230–1236, 2011
8. Di Napoli M, Godoy DA, Campi V, Masotti L, Smith CJ, Par-ry Jones AR, et al: C-reactive protein in intracerebral hemor-rhage: time course, tissue localization, and prognosis. Neurol-ogy 79:690–699, 2012
9. Diedler J, Sykora M, Hahn P, Rupp A, Rocco A, Herweh C, et al: C-reactive-protein levels associated with infection predict short- and long-term outcome after supratentorial intracere-bral hemorrhage. Cerebrovasc Dis 27:272–279, 2009
10. Elkind MS, Luna JM, Moon YP, Liu KM, Spitalnik SL, Paik MC, et al: High-sensitivity C-reactive protein predicts mortal-ity but not stroke: the Northern Manhattan Study. Neurology 73:1300–1307, 2009
TABLE 3: Predictors of an unfavorable outcome after primary ICH*
Variable Univariable OR (95% CI) Multivariable OR (95% CI)†
age (per yr) 1.05 (1.04–1.06)‡ 1.06 (1.04–1.08)‡cardiac disease 1.93 (1.35–2.76)‡ 0.96 (0.60–1.53)diabetes mellitus 2.19 (1.33–3.63)§ 1.99 (1.09–3.64)§GCS (per unit) 0.65 (0.58–0.73)‡ 0.75 (0.67–0.84)‡hematoma size (per ml) 1.05 (1.04–1.07)‡ 1.05 (1.03–1.07)‡presence of intraventricular hemorrhage 6.40 (4.22–9.71)‡ 2.70 (1.66–4.38)‡subcortical hematoma location 0.78 (0.55–1.11) 0.33 (0.20–0.54)‡CRP on admission (per 10 mg/L) 1.37 (1.10–1.70)¶ 1.41 (1.09–1.81)¶
* Unfavorable outcome denotes moderate disability or worse outcome according to the GOS. † The ORs in the multivariate analysis were also adjusted for sex.‡ p < 0.001.§ p < 0.05.¶ p < 0.01.

J Neurosurg / Volume 121 / December 2014
CRP as a predictor of outcome after ICH
1379
11. Huhtakangas J, Tetri S, Juvela S, Saloheimo P, Bode MK, Hill-bom M: Effect of increased warfarin use on warfarin-related cerebral hemorrhage: a longitudinal population-based study. Stroke 42:2431–2435, 2011
12. Jennett B, Bond M: Assessment of outcome after severe brain damage. Lancet 1:480–484, 1975
13. Juvela S, Kuhmonen J, Siironen J: C-reactive protein as pre-dictor for poor outcome after aneurysmal subarachnoid haem-orrhage. Acta Neurochir (Wien) 154:397–404, 2012
14. Kothari RU, Brott T, Broderick JP, Barsan WG, Sauerbeck LR, Zuccarello M, et al: The ABCs of measuring intracerebral hemorrhage volumes. Stroke 27:1304–1305, 1996
15. Leira R, Dávalos A, Silva Y, Gil-Peralta A, Tejada J, Garcia M, et al: Early neurologic deterioration in intracerebral hemor-rhage: predictors and associated factors. Neurology 63:461–467, 2004
16. Nordestgaard BG, Zacho J: Lipids, atherosclerosis and CVD risk: is CRP an innocent bystander? Nutr Metab Cardiovasc Dis 19:521–524, 2009
17. Sacco RL: Identifying patient populations at high risk for stroke. Neurology 51 (3 Suppl 3):S27–S30, 1998
18. Teasdale G, Jennett B: Assessment of coma and impaired con-sciousness. A practical scale. Lancet 2:81–84, 1974
19. Tetri S, Juvela S, Saloheimo P, Pyhtinen J, Hillbom M: Hyper-tension and diabetes as predictors of early death after spon-taneous intracerebral hemorrhage. Clinical article. J Neuro-surg 110:411–417, 2009
20. Tetri S, Mäntymäki L, Juvela S, Saloheimo P, Pyhtinen J, Ru-sanen H, et al: Impact of ischemic heart disease and atrial fibrillation on survival after spontaneous intracerebral hemor-rhage. J Neurosurg 108:1172–1177, 2008
21. Wang J, Doré S: Inflammation after intracerebral hemorrhage. J Cereb Blood Flow Metab 27:894–908, 2007
22. Whitworth JA, World Health Organization, International Society of Hypertension Writing Group: 2003 World Health Organization (WHO)/International Society of Hypertension (ISH) statement on management of hypertension. J Hyper-tens 21:1983–1992, 2003
23. Zahuranec DB, Brown DL, Lisabeth LD, Gonzales NR, Lon-gwell PJ, Smith MA, et al: Early care limitations independent-ly predict mortality after intracerebral hemorrhage. Neurol-ogy 68:1651–1657, 2007
Manuscript submitted December 4, 2013.Accepted July 2, 2014.Please include this information when citing this paper: pub-
lished online August 29, 2014; DOI: 10.3171/2014.7.JNS132678.Address correspondence to: Pekka Löppönen, M.D., Department
of Neurosurgery, Oulu University Hospital, Box 20, 90029 OYS, Finland. email: [email protected].

II


E
Ip
CJHM
a
b
c
d
RA
h0
pilepsy Research (2014) 108, 732—739
j ourna l h om epa ge: www.elsev ier .com/ locate /ep i lepsyres
mmediate, early and late seizures afterrimary intracerebral hemorrhage
heng Qiana,∗, Pekka Löppönena, Sami Tetri a,uha Huhtakangasb, Seppo Juvelad,anna-Maria E. Turtiainena, Michaela K. Bodec,atti Hillbomb
Department of Neurosurgery, Oulu University Hospital, Oulu, FinlandDepartment of Neurology, Oulu University Hospital, Oulu, FinlandDepartment of Diagnostic Radiology, Oulu University Hospital, Oulu, FinlandDepartment of Clinical Neurosciences, University of Helsinki, Helsinki, Finland
eceived 23 October 2013; received in revised form 21 January 2014; accepted 28 February 2014vailable online 12 March 2014
KEYWORDSSeizures;Primary intracerebralhemorrhage;Epilepsy;Infection;Subcorticalhematoma
SummaryBackground: Seizures after primary intracerebral hemorrhage (PICH) are significant and treat-able complications, but the factors predicting immediate, early and late seizures are poorlyknown. We investigated characteristics and outcome with special reference to occurrence andtiming of a first seizure among consecutive subjects with PICH.Methods: A population-based study was conducted in Northern Ostrobothnia, Finland, in1993—2008 that included all patients with a first-ever primary ICH without any prior diagnosisof epilepsy. Immediate (<24 h after admission), early (1—14 days) and late (>2 weeks) seizureswere considered separately.
Results: Out of a total of 935 ICH patients, 51 had immediate, 21 early and 58 lateseizures. The patients with seizures were significantly younger than the others andmore often had a subcortical hematoma location (p < 0.05). Lifestyle factors did notdiffer between the groups. The risk factors for immediate seizures in multivariableanalysis were a low Glasgow coma scale score (GCS) on admission, subcortical loca- tion and age inversely (p < 0.01). The only independent risk factor for early seizures∗ Corresponding author at: Department of Neurosurgery, Oulu University Hospital, Box 25, 90029 OYS, Finland. Tel.: +358 83152665.E-mail addresses: [email protected], [email protected] (C. Qian).
ttp://dx.doi.org/10.1016/j.eplepsyres.2014.02.020920-1211/© 2014 Published by Elsevier B.V.

Seizures after primary intracerebral hemorrhage 733
was subcortical location (p < 0.001), whereas subcortical location (p < 0.001), age inversely(p < 0.01) and hematoma evacuation (p < 0.05) independently predicted late seizures. Immediateand early seizures predicted infectious complications (p < 0.05).Conclusions: Patients with subcortical hematoma and of younger age are at risk for immediateseizures after primary ICH irrespective of hematoma size. Patients with immediate and earlyseizures more often had infectious complications. Surgery increases the risk of a late seizureafter ICH.© 2014 Published by Elsevier B.V.
S
Wtuttlilojhtbuas2
N
Pcumpa2fAiaspwo
C
TuJennett, 1974). Data on previous diseases, blood pressurevalues and the use of anticoagulants were obtained fromhospital records. Data were obtained from the forensic
Introduction
Seizures are common complications after ICH, the reportedincidence being approximately 10% (Passero et al., 2002).The incidence of seizures after primary ICH (PICH) has notbeen reported, but the incidence after spontaneous ICH(SICH) has been reported to vary between 2.8 and 18.7%(Kase et al., 1982; Lipton et al., 1987; Arboix et al., 1997;Berger et al., 1988; Cheung et al., 2003; De et al., 2007).Authors have usually classified seizures by the time of onset,as early or late, but the definitions for the time frame dif-fer widely (Gilmore et al., 2010), although the cut-off pointhas generally been 2 weeks after the onset of the stroke(Jennett, 1974). Seizures after a stroke have not been foundto affect the outcome and are therefore considered to bea relatively harmless complication (De, 2009). Only a smallminority of patients with ICH later develop epilepsy (Bladinet al., 2000), although prolonged seizures and/or statusepilepticus could damage the brain and cause secondarybrain injury (Treiman et al., 1998). In a study including 1402patients, 3-month mortality rates were reported to be 34%for those having early seizures after ICH and 13% for thosehaving late seizures (Sung and Chu, 1989).
Earlier studies dealing with ischemic or hemorrhagicstroke-related seizures and the few studies of seizures afterSICH have reported conflicting results (De et al., 2007;Bladin et al., 2000; Burn et al., 1997; Sung and Chu, 1989).A number of investigations with continuous EEG (cEEG)monitoring in intensive care units (ICUs) have shown themajority of seizures to be non-convulsive in nature, butnon-convulsive seizures cannot be recognized without cEEG(Gilmore et al., 2010).
Some previous reports have demonstrated the effect ofseizures on the outcome with small patient populations(Cervoni et al., 1994; Kase et al., 1982; Lipton et al., 1987),but the significance of seizures for the outcome, their pre-vention and their association with other complications werematters that remained unclear. In addition, the benefits ofprophylactic anticonvulsant medication remained uncertain(Morgenstern et al., 2010).
The aim here was to clarify which factors predict imme-diate, early and late seizures among patients with PICH ina large population-based cohort and to assess the effects ofthese seizure categories on the outcome and the occurrenceof infectious and thromboembolic complications.
Methods
The protocol was approved by the Ethics Committee of theNorthern Ostrobothnia Hospital District.
aPpe
ubjects
e identified all subjects with PICH among the popula-ion of Northern Ostrobothnia, Finland, from January 1993ntil January 2008. The series included all patients admit-ed to Oulu University Hospital, which is the only hospitalreating acute stroke patients in its catchment area (popu-ation in 1993—2008: 356,026—389,671). Patients not livingn the area and those with a brain tumor, aneurysm, vascu-ar malformation, head trauma, hematological malignancyr hemophilia were excluded. We also identified six sub-ects who had died of PICH without being admitted to ourospital by collecting data from the Causes of Death Regis-er (Statistics Finland). The diagnoses of these patients hadeen confirmed by autopsy, and the data also included these of anticoagulants at the time of death. Data on use ofntiepileptic drugs (AEDs) and occurrence of first epilepticeizures were collected for all patients up to December 31,008.
euroradiological methods
ICH was verified by a head CT scan on admission in allases. CT scans were analyzed and the locations and vol-mes of the hematomas measured by neuroradiologists. Theethod for measuring hematoma volume has been describedreviously (Huhtakangas et al., 2011). Secondary structuralbnormalities were searched for by follow-up brain imaging—3 months after the hematoma. Angiography was per-ormed immediately if aneurysmal bleeding was suspected.ll the surviving surgically treated patients and the major-
ty of the conservatively treated patients were followed upt least once with CT or MRI. Locations were classified asubcortical, thalamic, ganglionic (including extensions of autaminal hematoma into the thalamus and/or subcorticalhite matter), infratentorial (cerebellum and/or pons) andther hematomas (primary intraventricular, multiple, etc.).
linical data
he patient’s clinical condition on admission was assessedsing the Glasgow coma scale score (GCS) (Teasdale and
utopsy charts of those who had succumbed on the scene.atients were considered to be hypertensive if their bloodressure readings preceding the index stroke had repeatedlyxceeded 160/90 mmHg in accordance with the WHO/ISH

7 C. Qian et al.
sthCahltafdmPowohatbrs
P
SbphHtppn
O
DifttcsoS(h1w
S
CCacpfit
25 Patients had
epilepsy before
PICH
935 Patients d id no t
have epilepsy before
PICH
130 Patients had seizures
after PICH 805 Patients did not have
seizures af ter PICH
51 Patients had
immedi ate seizur es after
PICH
21 Patients had earl y
seizures af ter PICH
58 Patients had la te
seizures af ter PICH
982 patients with PICH in
1993-2008 a mong the
population of Northern
Ostrobothnia
960 Patients
with f irst- ever
PICH
Fs
iafiG(dt(fvRwapwantswofhs
R
Ttw
34
tatement (Whitworth and Chalmers, 2004), or if they wereaking antihypertensive medication. Persons taking an oralypoglycemic agent or insulin were recorded as diabetics.ardiac disease included myocardial infarction, coronaryrtery disease, heart failure and atrial fibrillation. Recenteavy drinking was defined as the weekly ingestion of ateast 300 g of ethanol during the month preceding the stroke,he data having been obtained by interviewing the patientsnd/or their relatives. Alcohol intake data were missingor 9% of the patients, however. Warfarin medication wasouble-checked from the national register of prescribededicines kept by the Social Insurance Institution of Finland.
atients were recorded to having seizures if they devel-ped seizures and a need for sedatives or AEDs, and theseere categorized into three groups according to the timingf the seizures (Hemphill et al., 2001): immediate if theyad a seizure within 24 h of admission, early if they had
seizure >24 h but <2 weeks after admission, and late ifhey had seizures >2 weeks after admission. The use of AEDsefore and after seizures was ascertained from the hospitalecords. Patients were categorized according to her/his firsteizure.
atient management
tandard care, reversal of the warfarin effect and throm-oprophylaxis were performed according to institutionalrotocols. The methods adopted for thromboprophylaxisave been described earlier (Huhtakangas et al., 2011).ematomas were evacuated by standard craniotomy orhrough a burr hole. No patients were treated with decom-ressive craniectomy or neuroendoscopic surgery during theeriod concerned. Data were collected on the additionaleed for external ventricular drainage (EVD).
utcome measurements
eath records were obtained from the Causes of Death Reg-ster and checked for the study population. Patients wereollowed up at our outpatient clinic or in the rehabilita-ion ward of our hospital for 3 months after the ICH, withhe exception of those who showed good recovery at dis-harge. The latter were assumed to have maintained thistate for 3 months unless they had been readmitted. Theutcome was assessed according to the Glasgow Outcomecale (GOS) (De et al., 2011). Patients with scores of 4—5moderate disability or good recovery) were considered toave a favorable outcome, whereas patients with scores of—3 (death, persistent vegetative state or severe disability)ere considered to have a poor outcome.
tatistical methods
ategorical variables were compared using the Pearsonhi-square test. Univariable associations of continuous vari-bles were tested by reference to Spearman rank (rs)
orrelation coefficients. Logistic regression analyses wereerformed to determine odds ratios (OR) and 95% con-dence intervals (CI) for the variables associated withhe appearance of seizures (separately for factors whichy2wi
igure 1 Flow chart showing the composition of the patienteries.
ndependently predicted immediate, early and late seizures)nd infectious complications. The following variables wererst tested by the forward stepwise method: sex, age,CS score, hematoma size, intraventricular hemorrhage
IVH), hematoma location, prior ischemic stroke and heavyrinking. The subsequent analysis included also hyper-ension, diabetes, cardiac disease, cardiac complicationsincluding myocardial infarction, arrhythmias and/or heartailure), thromboembolic complications (including deepenous and/or pulmonary embolism), and use of warfarin.isk factors (hazard ratios [HR] with 95%CIs) for case fatalityithin 3 months were tested with Cox proportional haz-rd regression models, employing age, sex, hematoma size,resence of intraventricular hemorrhage, GCS on admission,arfarin treatment, infectious complications and immedi-te seizures as the covariates. Early and late seizures wereot included, because most deaths occurred within the firstwo days of onset of bleeding. All the variables that had aignificant (p < 0.05) association in the univariable analysisere included in the multivariable analysis. The assumptionf the proportionality of variables was checked. The testor significance was based on changes in log (partial) likeli-ood. A two-tailed p value of less than 0.05 was consideredtatistically significant.
esults
he distribution of patients included in the series is shown inhe flow chart (Fig. 1). There were altogether 982 patientsith PICH in Northern Ostrobothnia during the period of 16
ears, for 960 of whom this was the first-ever PICH, including5 patients who had epilepsy. Thus the number of patientsith a first-ever PICH and without epilepsy who could bencluded in the eventual series was 935 (Fig. 1).

Seizures after primary intracerebral hemorrhage 735
Table 1 Baseline characteristics of subjects with new-onset seizures.
Subjects withoutseizures (n = 805)
Subjects with seizures Total (n = 935)
Immediate (n = 51) Early (n = 21) Late (n = 58)
Mean age, yr ± SD* 70 ± 12 64 ± 16 73 ± 11 63 ± 10 69 ± 12Men, n (%) 431 (54) 25 (49) 13 (62) 32 (55) 501 (54)Previous diseases, n (%)
Diabetes* 145 (18) 6 (12) 9 (43) 8 (14) 168 (18)Ischemic stroke 167 (21) 10 (20) 7 (33) 12 (21) 196 (21)Hypertension 510 (63) 32 (63) 13 (62) 22 (38) 587 (63)Cardiac disease 325 (40) 15 (29) 10 (48) 19 (33) 369 (39)
Lifestyle factors, n (%)Current smoking 68 (8) 8 (16) 1 (5) 4 (7) 81 (9)Heavy drinking 94 (12) 8 (16) 0 (0) 5 (9) 107 (11)Warfarin medication 158 (20) 6 (12) 5 (24) 5 (9) 174 (19)
isht
C
Tdo2tdC(isa(co
O
Taorbec
ahwm
* Significant heterogeneity between the groups, p < 0.05.
Of the 935 patients, 130 had seizures after PICH and805 did not. The former included 51 cases of immediateseizures (<24 h after ICH), 21 with early seizures (>24 h to2 weeks after ICH) and 58 with late seizures. The base-line characteristics of these patients are shown in Table 1.There was significant heterogeneity between the seizuregroups in terms of age, the patients with immediate and lateseizures being significantly younger than those with earlyseizures (p < 0.05). Diabetes was found significantly moreoften among the patients with early seizures than amongthose with immediate and late seizures.
The clinical, radiological and outcome variables areshown in Table 2. The patients with immediate seizureshad significantly lower GCS scores on admission than theother groups (p < 0.001) and those with early seizures hadsmaller hematomas than the others (p < 0.01). A subcor-tical location of the hematoma was more common in thepatients with than without seizures (p < 0.001), while throm-boembolic complications were more common in the patientswith immediate and late seizures (p < 0.05). Pneumonia wasfound more often in the patients with immediate or earlyseizures than in the others (p < 0.05), while the patients whodeveloped late seizures more often had surgery for theirhematoma (p < 0.001).
The use of a prophylactic AED turned out to be rare amongthe population of our area, and its rates of use among thepatients with immediate, early and late seizures were 1/51(2%), 1/21 (5%), and 11/58 (19%), respectively. The inci-dence of late epilepsy after a first-ever ICH was 7% (Table 2)among subjects without epilepsy as a preceding disease.
Predictors of seizures
The univariable and multivariable risk factors for imme-diate, early and late seizures after ICH are presented inTable 3. The independent risk factors for immediate seizuresin the multivariable analysis were a low GCS score on admis-
sion, subcortical location of the hematoma and age inversely(p < 0.01 for each). Small hematoma size seemed also tobe associated with immediate seizures after adjustment formore significant factors. Subcortical location was the onlyao
a
ndependent risk factor for early seizures (p < 0.001), whileubcortical location (p < 0.001), age inversely (p < 0.01) andematoma evacuation (p < 0.05) were independently predic-ive of late seizures.
ase fatality
hree hundred and thirteen out of the 935 patients (33%)ied within 3 months of ICH, the highest fatality rate beingbserved among the patients with immediate seizures, since5 out of the 51 (49%) died within 3 months whereas none ofhose with late seizures died within that time. The indepen-ent predictors of death (within 3 months) as determined byox regression survival analysis were large hematoma sizeadjusted HR 1.06 per 10 ml, 95%CI 1.03—1.08), presence ofntraventricular blood (2.13, 95%CI 1.62—2.81), a low GCScore on admission (0.83 per unit, 95%CI 0.81—0.86), higherge (1.03 per year, 95%CI 1.03—1.05) and warfarin treatment2.40, 95%CI 1.86—3.09). Immediate seizures and infectiousomplications were not found to be significantly predictivef early death after ICH.
utcome
he outcomes differed between the patients with immedi-te, early and late seizures and those without seizures, poorutcomes being recorded in 63%, 48%, 36% and 58% of cases,espectively (Table 2). There was significant heterogeneityetween the groups in terms of outcome, with the patientsxperiencing late seizures having the most favorable out-ome status (p < 0.001).
A large hematoma size (p < 0.001), a low GCS score ondmission (p < 0.001), infectious complications (p < 0.001),igh age (p < 0.001), IVH (p < 0.001) and diabetes (p < 0.02)ere independent risk factors for a poor outcome in theultivariable analysis. Seizures occurring more than 48 h
fter ICH were independently associated with a favorableutcome (Table 4).
Infectious complications, especially pneumonia, weressociated with a poor outcome after ICH. Logistic

736 C. Qian et al.
Table 2 Clinical characteristics and outcome of ICH subjects, by time of onset of new-onset seizures after the index stroke.
Without seizures(n = 805)
With seizures Total (n = 935)
Immediate (n = 51) Early (n = 21) Late (n = 58)
Median GCS, (25and 75%percentiles)
14 (10, 15) 10 (5, 14)† 13 (12, 15) 14 (12, 15) 14 (10, 15)
Mean hematomavolume, ml ± SD
34 ± 43 32 ± 41 19 ± 19‡ 30 ± 28 33 ± 42
Intraventricularhemorrhage, n(%)
366 (46) 25 (49) 6 (29) 19 (33) 416 (45)
Subcorticallocation*
209 (26) 24 (47) 13 (62) 32 (55) 278 (30)
Complications, n (%)Cardiac 58 (7) 6 (12) 4 (19) 2 (3) 70 (7)
Thromboembolic**16 (2) 3 (6) 0 4 (7) 23 (2)
Infection* 192 (24) 19 (37) 13 (62) 14 (24) 238 (25)Urinary tractinfection
77 (10) 8 (16) 4 (19) 10 (17) 99 (11)
Pneumonia* 111 (14) 12 (24) 9 (43) 7 (12) 139 (15)Hematoma
evacuation, n(%)*
97 (12) 9 (18) 1 (5) 18 (31) 125 (13)
Prophylactic AED N/A 1 (2) 1 (5) 11 (19) N/AEpilepsy after
PICH0/0 11 (22) 8 (38) 49 (84) 68 (7)
Glasgow Outcome Scale, n (%)**
Favorable 338 (42) 19 (37) 11 (52) 37 (64) 405 (43)Poor 463 (58) 32 (63) 10 (48) 21 (36) 526 (56)
Dead within 3months, n (%)*
283 (35) 25 (49) 5 (24) 0 (0) 313 (33)
AED = antiepileptic drug.* Significant heterogeneity between groups, p < 0.001.
** Significant heterogeneity between groups, p < 0.05.† Lower mean GCS than in other groups (p < 0.001).
ual v
r11ppo
D
WsPmmtld
luCc(1fboOilh
‡ Smaller volume than in subjects without seizures (p = 0.003 eq
egression analysis showed immediate seizures (OR.96, 95%CI 1.05—3.66, p < 0.05), early seizures (4.47,.79—11.18, p < 0.01), thromboembolism (2.83, 1.21—6.67,
< 0.05), and cardiac complications (2.37, 1.39—4.03, < 0.01) to be independently associated with the occurrencef an infectious complication.
iscussion
e found that 5.5% of the patients had had immediateeizures, altogether 8% had had seizures within 2 weeks ofICH and 7% had developed epilepsy requiring drug treat-ent later on. The patients with immediate seizures had had
ore infectious complications and showed higher mortalityhan the others. Hematoma evacuation was a predictor ofate seizures, suggesting possibly a need for antiepilepticrug treatment for those who have been operated on.
biso
ariances not assumed).
We found a subcortical location of the hematoma, aow GCS score on admission and a small hematoma vol-me to significantly predict immediate seizures after PICH.onflicting observations have been reported previously con-erning the role of hematoma size, however, as both smallPassero et al., 2002; Faught et al., 1989; Weisberg et al.,991) and large hematomas (Yang et al., 2009) have beenound to increase the risk of seizures, and there have eveneen reports of no significant effect of hematoma volumen the seizure risk (Woo et al., 2012; De et al., 2011).ur result supports the findings of those former studies as
mmediate seizures were less common among patients witharge hematomas when adjusted for clinical condition andematoma location.
Immediate, early and late seizures have not previously
een studied separately. Our observations suggest thatmmediate seizures are frequently associated with a low GCScore and younger age. Impaired consciousness was foundn admission in many patients with immediate seizures,
Seizures after primary intracerebral hemorrhage 737
Table 3 Predictors of immediate, early and late seizures after PICH.
Variable Univariate OR (95%CI) Multivariate OR (95%CL)
Immediate seizureHematoma size (per ml) 1.00 (0.99—1.01) 0.99 (0.97—1.00)‡
GCS on admission (per unit) 0.88 (0.83—0.93)* 0.83 (0.77—0.89)*
Subcortical location 2.21 (1.25—3.89)# 2.93 (1.6—5.39)*
Age (per year) 0.97 (0.95—0.99)# 0.97 (0.95—1.00)#
Early seizureHematoma size (per ml) 0.99 (0.97—1.00) 0.99 (0.96—1.00)GCS on admission (per unit) 1.09 (0.96—1.25) 1.01 (0.87—1.18)Subcortical location 3.98 (1.63—9.71)# 5.42 (2.15—13.62)*
Age (per year) 1.03 (0.99—1.07) 1.03 (0.99—1.07)Hematoma evacuation 0.32 (0.04—2.40) 0.41 (0.04—3.71)
Late seizureHematoma size (per ml) 1.00 (0.99—1.01) 1.00 (0.99—1.00)GCS on admission (per unit) 1.07 (0.99—1.15) 1.09 (0.99—1.20)Subcortical location 3.16 (1.84—5.41)* 2.90 (1.60—5.29)*
Age (per year) 0.96 (0.94—0.98)* 0.96 (0.94—1.00)#
Hematoma evacuation 3.24 (1.79—5.85)* 2.47 (1.12—5.45)†
Odds ratios in the multivariate analysis have been adjusted for sex and the variables listed in the table. OR, odds ratio; CI, confidenceinterval.
* p < 0.001.# p < 0.01.‡ p < 0.02.† p < 0.05.
but it remained unclear whether this was due to a non-convulsive status epilepticus in some patients, as we did notuse cEEG monitoring. Although immediate seizures were notsignificant predictors of death in the multivariable analy-sis, patients having them showed a statistically significantlyhigher case fatality rate than those who had late seizures.Also, immediate seizures were not predictive of death or
Table 4 Predictors of a poor outcome after ICH.
Variable Multivariate OR (95%CI)
Hematoma size (perml)
1.03 (1.02—1.04)*
Presence of IVH 2.63 (1.79—3.86)*
GCS on admission(per unit)
0.75 (0.69—0.81)*
Age (per year) 1.05 (1.04—1.07)*
Warfarin treatment 1.36 (0.82—2.25)Immediate seizures 0.67 (0.29—1.54)Early seizures 0.34 (0.12—0.97)†
Late seizures 0.47 (0.23—0.96)†
Cardiac disease 1.23 (0.81—1.86)Hypertension 0.80 (0.54—1.17)Diabetes 1.79 (1.10—2.93)†
Post-PICH infections 2.93 (1.95—4.41)*
Thromboemboliccomplication
1.34 (0.46—3.85)
Odds ratios in the multivariate analysis have been adjusted forsex and the variables listed in the table. OR, odds ratio; CI,confidence interval; IVH, intraventricular hemorrhage.
* p < 0.001.† p < 0.05.
atfiipabSli
poskF2becftebttbgsanrt
poor outcome in the multivariate analysis likely becauseheir lower GCS scores as compared with others. One newnding was our observation of an association between
mmediate seizures and infectious complications, especiallyneumonia. It seems to be that patients with immedi-te seizures are prone to develop pneumonia, probablyecause of aspiration due to their impaired consciousness.ince immediate seizures are frequently associated with aow GCS, impairment of consciousness could be a factornvolved.
Subcortical location of the hematoma was the only inde-endent predictor of early seizures, while the predictorsf late seizures were subcortical location, younger age andurgery for the hematoma. Subcortical location is a well-nown risk factor for seizures after ICH (Passero et al., 2002;aught et al., 1989; Weisberg et al., 1991; Rossi et al.,013), and young age has also been found previously toe a risk factor for seizures (Passero et al., 2002; Reddigt al., 2011; Yang et al., 2009), whereas the increased riskaused by hematoma evacuation is a less-known effect. Weound earlier that surgery reduced mortality but increasedhe number of patients with a poor outcome (Löppönent al., 2013), which may in turn have increased the num-er of patients with late seizures. Surgery causes additionalrauma to the subcortical matter, leading to loss of func-ional components. Another reason for this observation maye that survivors remaining in a poor condition have under-one more frequently life-saving hematoma evacuation, i.e.urgery may be a proxy of prolonged impaired condition
fter PICH. Thus, prolonged impaired condition, which can-ot be measured by admission GCS score, may be also aeason for late seizures. These may in our opinion increasehe risk of late seizures. Our observations confirmed that
7
df2
tsadth
mosph1
sfpheTwacsdspApepAcss
eaaiaTinuiPnsdgapcCtis
C
•
•
•
••
D
Wica
R
A
B
B
B
C
C
D
D
D
F
G
38
eath after PICH is predicted by the well-known prognosticactors for ICH described in the literature (Hemphill et al.,001).
The occurrence of early and late seizures predicted a bet-er outcome than did immediate seizures or the absence ofeizures. In fact, early and late seizures were predictors of
favorable outcome, even though many of these patientseveloped epilepsy later on. This is explained by the defini-ion of the seizure types; those who survive beyond 48 h willave a better outcome.
We found the incidence of epilepsy calling for drug treat-ent was high (84%) among those having a late occurrence
f the first seizure and low among those with immediateeizures (22%). It must be borne in mind, however, thatatients with an acute symptomatic status epilepticus mayave a high risk of a recurrence of seizures (Hesdorffer et al.,998).
Prophylactic AEDs are not recommended, except forelected cases with lobar ICH (Steiner et al., 2006). Veryew patients in our hospital were given intravenous pro-hylactic AEDs, although such treatment is reported toave been given to 28—89% of patients elsewhere (Passerot al., 2002; Woo et al., 2012; Reddig et al., 2011).his may explain why we had a large number of patientsith immediate seizures in our study. It was found in
recent prospective, randomized, double-blind, placebo-ontrolled trial that the use of valproic acid reduced earlyeizures (Gilad et al., 2011). Patients treated with thisrug also showed an improved outcome, and the authorsuggested that the medicine may have had some neuro-rotective effects. In another study, however, prophylacticED treatment was associated with a poor outcome inde-endently of other established outcome predictors (Messet al., 2009). Most of the patients in that cohort receivedhenytoin, however. Our results suggest that prophylacticED should perhaps be given to all patients with sub-ortical hematomas, and particularly to those obtainingurgery, as these patients run the highest risk of lateeizures.
The long follow-up time in the present investigationnabled us to recognize the occurrence of late seizuresnd to ascertain definite diagnoses of epilepsy after PICHs accurately as possible. Other strengths of our studynclude the careful radiological analysis of the hematomasnd the population-based design, avoiding selection bias.here are still some limitations, however. The use of cEEG
n our ICU was sporadic, so that we probably missed someon-convulsive early seizures. Also, a variety of AEDs weresed to treat the seizures, and the cases were treatedndividually as regards the duration of AED medication.rophylactic AEDs were rarely used, however, providing aatural result for the incidence of immediate and earlyeizures after PICH. Due to the study design we lack detailedata of seizures types. It was possible to identify a sub-roup of patients who run a risk of immediate seizuresnd complications related to them, but the effect of pro-hylactic medication remains to be proved in prospectiveontrolled trials. Only a few subjects had a second head
T scan to verify rapid enlargement of the hematoma, andherefore the whole question of rapid hematoma volumencrease and its association with immediate seizures remainspeculative.G
C. Qian et al.
onclusions
Relatively young patients with subcortical hematomas runa risk of immediate seizures irrespective of hematomasize and are more prone to infectious and other compli-cations.
Subjects with immediate seizures show the highest casefatality rate.
Subjects with early seizures are older, have smallerhematomas and have diabetes more frequently than thosewith immediate and/or late seizures.
Surgery may increase the risk of late seizures after PICH. Evacuation of subcortical hematoma could perhaps be
considered an indication for prophylactic treatment withAEDs.
isclosure
e confirm that we have read the Journal’s position on issuesnvolved in ethical publication and affirm that this report isonsistent with those guidelines. None of the authors hasny conflict of interest to disclose.
eferences
rboix, A., Garcia-Eroles, L., Massons, J.B., Oliveres, M., Comes,E., 1997. Predictive factors of early seizures after acute cere-brovascular disease. Stroke 28, 1590—1594.
erger, A.R., Lipton, R.B., Lesser, M.L., Lantos, G., Portenoy, R.K.,1988. Early seizures following intracerebral hemorrhage: impli-cations for therapy. Neurology 38, 1363—1365.
ladin, C.F., Alexandrov, A.V., Bellavance, A., Bornstein, N., Cham-bers, B., Cote, R., Lebrun, L., Pirisi, A., Norris, J.W., 2000.Seizures after stroke: a prospective multicenter study. Arch.Neurol. 57, 1617—1622.
urn, J., Dennis, M., Bamford, J., Sandercock, P., Wade, D., Warlow,C., 1997. Epileptic seizures after a first stroke: the OxfordshireCommunity Stroke Project. BMJ 315, 1582—1587.
ervoni, L., Artico, M., Salvati, M., Bristot, R., Franco, C., Delfini,R., 1994. Epileptic seizures in intracerebral hemorrhage: aclinical and prognostic study of 55 cases. Neurosurg. Rev. 17,185—188.
heung, C.M., Tsoi, T.H., Au-Yeung, M., Tang, A.S., 2003. Epilep-tic seizure after stroke in Chinese patients. J. Neurol. 250,839—843.
e, R.J., Hemelsoet, D., Van, M.G., 2007. Seizures and epilepsyin patients with a spontaneous intracerebral haematoma. Clin.Neurol. Neurosurg. 109, 501—504.
e, R.J., 2009. Management of stroke-related seizures. Acta Neurol.Belg. 109, 271—276.
e, H.V., Dumont, F., Henon, H., Derambure, P., Vonck, K., Leys,D., Cordonnier, C., 2011. Early seizures in intracerebral hemor-rhage: incidence, associated factors, and outcome. Neurology77, 1794—1800.
aught, E., Peters, D., Bartolucci, A., Moore, L., Miller, P.C., 1989.Seizures after primary intracerebral hemorrhage. Neurology 39,1089—1093.
ilad, R., Boaz, M., Dabby, R., Sadeh, M., Lampl, Y., 2011. Are postintracerebral hemorrhage seizures prevented by anti-epileptic
treatment? Epilepsy Res. 95, 227—231.ilmore, E., Choi, H.A., Hirsch, L.J., Claassen, J., 2010. Seizuresand CNS hemorrhage: spontaneous intracerebral and aneurysmalsubarachnoid hemorrhage. Neurologist 16, 165—175.

R
R
S
S
T
T
W
W
W
Seizures after primary intracerebral hemorrhage
Hemphill III, J.C., Bonovich, D.C., Besmertis, L., Manley, G.T., John-ston, S.C., 2001. The ICH score: a simple, reliable grading scalefor intracerebral hemorrhage. Stroke 32, 891—897.
Hesdorffer, D.C., Logroscino, G., Cascino, G., Annegers, J.F.,Hauser, W.A., 1998. Risk of unprovoked seizure after acute symp-tomatic seizure: effect of status epilepticus. Ann. Neurol. 44,908—912.
Huhtakangas, J., Tetri, S., Juvela, S., Saloheimo, P., Bode, M.K.,Hillbom, M., 2011. Effect of increased warfarin use on warfarin-related cerebral hemorrhage: a longitudinal population-basedstudy. Stroke 42, 2431—2435.
Jennett, B., 1974. Early traumatic epilepsy. Incidence and signifi-cance after nonmissile injuries. Arch. Neurol. 30, 394—398.
Kase, C.S., Williams, J.P., Wyatt, D.A., Mohr, J.P., 1982. Lobarintracerebral hematomas: clinical and CT analysis of 22 cases.Neurology 32, 1146—1150.
Lipton, R.B., Berger, A.R., Lesser, M.L., Lantos, G., Portenoy, R.K.,1987. Lobar vs thalamic and basal ganglion hemorrhage: clinicaland radiographic features. J. Neurol. 234, 86—90.
Löppönen, P., Tetri, S., Juvela, S., Huhtakangas, J., Saloheimo, P.,Bode, M.K., Koivukangas, J., Hillbom, M., 2013. A populationbased study of outcomes after evacuation of primary supraten-torial intracerebral hemorrhage. Clin. Neurol. Neurosurg. 115,1350—1355.
Messe, S.R., Sansing, L.H., Cucchiara, B.L., Herman, S.T., Lyden,P.D., Kasner, S.E., 2009. Prophylactic antiepileptic drug use isassociated with poor outcome following ICH. Neurocrit. Care 11,38—44.
Morgenstern, L.B., Hemphill III, J.C., Anderson, C., Becker, K., Brod-erick, J.P., Connolly Jr., E.S., Greenberg, S.M., Huang, J.N.,MacDonald, R.L., Messe, S.R., Mitchell, P.H., Selim, M., Tamargo,R.J., 2010. Guidelines for the management of spontaneous intra-cerebral hemorrhage: a guideline for healthcare professionalsfrom the American Heart Association/American Stroke Associa-
tion. Stroke 41, 2108—2129.Passero, S., Rocchi, R., Rossi, S., Ulivelli, M., Vatti, G., 2002.Seizures after spontaneous supratentorial intracerebral hemor-rhage. Epilepsia 43, 1175—1180.
Y
739
eddig, R.T., Nixdorf, K.E., Jensen, M.B., 2011. The prophylacticuse of an antiepileptic drug in intracerebral hemorrhage. Clin.Neurol. Neurosurg. 113, 895—897.
ossi, C., De, H.V., Quatre-Ponchelle, N., Henon, H., Leys, D., Cor-donnier, C., 2013. Incidence and predictors of late seizures inintracerebral hemorrhages. Stroke 44, 1723—1725.
teiner, T., Kaste, M., Forsting, M., Mendelow, D., Kwiecinski,H., Szikora, I., Juvela, S., Marchel, A., Chapot, R., Cognard,C., Unterberg, A., Hacke, W., 2006. Recommendations for themanagement of intracranial haemorrhage. Part I: Spontaneousintracerebral haemorrhage. The European Stroke Initiative Writ-ing Committee and the Writing Committee for the EUSI ExecutiveCommittee. Cerebrovasc. Dis. 22, 294—316.
ung, C.Y., Chu, N.S., 1989. Epileptic seizures in intrace-rebral haemorrhage. J. Neurol. Neurosurg. Psychiatry 52,1273—1276.
easdale, G., Jennett, B., 1974. Assessment of coma and impairedconsciousness. A practical scale. Lancet 13 (2), 81—84.
reiman, D.M., Meyers, P.D., Walton, N.Y., Collins, J.F., Colling, C.,Rowan, A.J., Handforth, A., Faught, E., Calabrese, V.P., Uthman,B.M., Ramsay, R.E., Mamdani, M.B., 1998. A comparison of fourtreatments for generalized convulsive status epilepticus, Veter-ans Affairs Status Epilepticus Cooperative Study Group. N. Engl.J. Med. 339, 792—798.
eisberg, L.A., Shamsnia, M., Elliott, D., 1991. Seizures causedby nontraumatic parenchymal brain hemorrhages. Neurology 41,1197—1199.
hitworth, J.A., Chalmers, J., 2004. World HealthOrganisation—International Society of Hypertension(WHO/ISH) hypertension guidelines. Clin. Exp. Hypertens. 26,747—752.
oo, K.M., Yang, S.Y., Cho, K.T., 2012. Seizures after sponta-neous intracerebral hemorrhage. J. Korean Neurosurg. Soc. 52,312—319.
ang, T.M., Lin, W.C., Chang, W.N., Ho, J.T., Wang, H.C., Tsai, N.W.,Shih, Y.T., Lu, C.H., 2009. Predictors and outcome of seizuresafter spontaneous intracerebral hemorrhage. Clinical article. J.Neurosurg. 111, 87—93.

III


Runningtitle:PreventionofVTEinpatientswithICHEarlyvs.lateenoxaparinforthepreventionofvenousthromboembolisminpatientswithICHQianC,MD;HuhtakangasJ,MD,PhD;JuvelaS,MD,PhD;BodeM,MD,PhD;TatlisumakT,MD,PhD;SavolainenM,MD,PhD;NumminenH,MD,PhD;OllikainenJ,MD,PhD;LuostarinenL;MD,PhD;KupilaL,MD,PhDandTetriS,MD,PhD.DepartmentofNeurosurgery,OuluUniversityHospital,Oulu,Finland(QC,TS)DepartmentofNeurology,OuluUniversityHospital,Oulu,Finland(HJ)DepartmentofClinicalNeurosciences,UniversityofHelsinki,Helsinki,Finland(JS,SM)DepartmentofRadiology,OuluUniversityHospital,Oulu,Finland(BM)DepartmentofNeurology,HelsinkiUniversityCentralHospital,Helsinki,Finland(TT)DepartmentofNeurology,SouthKarelianCentralHospital,Lappeenranta,Finland(SM)DepartmentofNeurology,SahlgrenskaUniversityHospital,Gothenburg,Sweden(TT)DepartmentofNeurology,TampereUniversityHospital(NH,OJ)DepartmentofNeurology,Päijät-HämeCentralHospital(LL,KL)DepartmentofClinicalNeuroscience,InstituteofNeuroscienceandPhysiology,SahlgrenskaAcademyatUniversityofGothenburg,Gothenburg,Sweden(TT)Addressforcorrespondence:SamiTetri,MD,PhD,OuluUniversityHospitalBox25,90029Oulu,[email protected]+35883152623StatisticalanalysisofthisstudywasconductedbySeppoJuvela,MD,PhD.Tables:3Figures:1References:19Keywords:intracerebralhemorrhage,deepvenousthrombosis,thrombosisprophylaxis,lowmolecularweightheparin,safety,Wordcount:Title:91(charactersandspaces)Abstract:247(words)Article:4397(words)

ABSTRACTBackroundVenoustromboembolism(VTE)afterprimaryintracerebralhemorrhage(ICH)worsenspatientprognosis.Administeringlow-molecularweightheparins(LMWH)forthrombosisprophlaxisearly(24h)mayincreasetheriskofhematomaenlargement,whereasadministeringlate(72h)afteronsetmaydecreaseitseffectonthrombosisprevention.TheauthorsinvestigatewhenitissafeandeffectivetostartLMWHinICHpatients.MethodsInthesettingofdoubleblindedrandomization,patients>18yearsofagewithpareticlowerextremity,andadmittedtotheemergencyroomwithin12hoftheonsetofICH,wererandomizedintotwogroups.Patientsintheenoxaparingroupreceived40mg/daily24hours(early)aftertheonsetofICHandintheplacebogroup72hours(late)afteronsetrespectively.BothgroupsimmediatelyreceivedintermittentpneumaticcompressionstockingsattheER.PatientswereprospectivelyandroutinelyscreenedforVTEandhemorrhagiccomplications1dayafteronsetandbeforedischarge.Results139patientswereincludedforrandomizationinthisstudy.Only3patientsdevelopedVTE,2intheearlyenoxaparingroupandoneinthelateenoxaparingroup.NopatientsdevelopedPE.Thromboembolicevents(p=0.901),riskofhematomaenlargement(p=0.927)andoveralloutcome(P=0.904)didnotdiffersignificantlybetweenthegroups.ConclusionAdministering40mg/dLMWHforthrombosisprophylaxistoaspontaneousICHpatientissaferegardlessofwhetheritisstarted24hours(early)or72hours(late)afterthehemorrhage.RiskofhemorrhageenlargementisnotassociatedwithearlyLMWHtreatment.AdministeringLMWHlatedidnotincreasethromboembolicevents.

IntroductionPatientssufferingaprimary intracerebralhemorrhage(ICH)haveasubstantialrisk of venous thromboembolism (VTE). Early studies showed that withoutprevention, deep venous thrombosis (DVT) occurs in about half of all strokepatients (47-53%) and 3-16% of them succumb to pulmonary embolism (PE)[1,2].Inparticular,thosewhohavehemiparesis/hemiplegiarunaveryhighriskofVTE(75%)[3,4].ThedevelopmentofVTE inapatientwith ICHadds furtherdetrimental complications to an already lethal disease,with a one-month casefatalityrateof35%to52%[5].Based on multiple RCTs [6,7]in both American (class 1 Evidence B) andEuropean (strong recommendation) guidelines, intermittent pneumaticcompression (ICP) is recommended together with long graduatedcompression/elasticstockingsand lowmolecularweightheparins (LMWHs)asprophylaxisforVTEinpatientswithacuteICH[8,9].Theseguidelinesaremostlybasedontrialsemployingasmallsamplesizeandheterogeneousapproachestostroke diagnosis, not limited to ICH. Even today, however, the role ofmedicalthrombosisprophylaxisinthetreatmentofpatientswithICHremainsunclear.Weconductedamulticenterdoubleblindrandomizedcontrolledstudytoclarifythe safetyandefficacyofLMWHuse forVTEprophylaxis inpatientswith ICH.Enoxaparin 40mg/day subcutaneously was started for paralyzed ICH patientseither 24 or 72 hours after the onset of the stroke. The ICP device andcompressionstockingswereadoptedatoncewhenthepatientwasadmittedtotheemergencyroom.Thesafetyandefficacyofbothalternativeswereanalyzed.

MethodsStandardprotocolapprovals,registration,andpatientconcentTheprotocolwasapprovedbytheethicalcommitteesofallthehospitaldistrictsconcerned.(statementnumber128/2007).Writtenconseptinformingthestudyprotocolwasobtainedtoallparticiantsortheirrelativesandparticipants.Thosewillingtotakeaparttoastudysignedaproof.Anypersontakingpartofthisstudycannotberecognizeontheinformationpublishedinthisstudy.NochangestomethodsweremadeduringthestudyafteritscommencementBeforestartingthisstudy,thestudyprotocolwasregistered(ClinicalTrialsGovIdentifier/NTC00699465andEudract2007-006206-24).TrialdesignThismulticenterstudywascarriedoutjointlyatOuluUniversityHospital,HelsinkiUniversityCentralHospital,TampereUniversityHospital,andLahtiCentralHospital,Finland,asanationalmulticenterstudy.Whenalikelyeligiblepatientarrived,investigatorswerealertedandoneoftheprimaryinvestigatorscheckedthepatient’seligibility.AlleligiblepatientsreceivedanIPCdeviceandcompressionstockingsassoonaspossibleintheemergencyroom,andwerethenrandomizedintotwogroups.ParticipantsAllsubjectswithprimaryICHadmittedtothestrokeunitsoftheabove-mentionedhospitalsbetween2008and2015werescreenedbyheadCTorMRscan.Thoseagedatleast18yearswereeligibleiftheywereunabletowalkunassistedduetomotorimpairment,withascore>2ofthepareticlowerextremityontheNationalInstitutesofHealthStrokeScale(NIHSS),andifadmittedtotheemergencyroomwithin12hoftheonsetofICH.Patientswhohadbeenreceivingoralanticoagulants,SSRIdrugs,clopidogrel,aspirinandotherNSAIDswereincluded.ThesedrugswerenaturallydiscontinuedatadmissionandtheeffectofwarfarinwasreversedimmediatelyintheemergencyroomwithVitaminKand/orprothrombincomplexconcentrate.Alleligiblepatientswereaskedtoparticipateinthetrialandinformedconsentwasobtained.Ifthepatientcouldnotgiveinformedconsentarelativewasapproached.AcombinationofCT,MRI,CTAand/ordigitalsubtractionangiographywasusedto exclude patients with secondary ICH related to aneurysm, arteriovenous

malformation, trauma or tumor. Patients who needed immediate hematomaevacuationorsomeotherformofneurosurgicalinterventionwereexcluded.Patients who were comatose (Glasgow Coma Scale (GCS) <8), had no or onlymildlimbparesis(NIHSS<2),orhadbeenseverelydisabledpriortothestroke(ModifiedRankin Scale (mRS)>2), or had the onset of the stroke>12hbeforeadmittancetohospitalwereexcluded.InterventionsSubcutaneousinjectionsofenoxaparinortheplacebowerestarted24haftertheonset of ICH and repeated twice daily, i.e. at 12h intervals. Each injectioncontained20mg(2000 IU)ofenoxaparin, implyingadailydoseof40mg.Theplacebogroupreceivedsalineinjectionsaccordingtothesameregime,andthiswasreplacedwithenoxaparin72haftertheonsetofthestroke.Theenoxaparintreatmentwasstoppedoncethepatientwasabletowalkindependently,orifasevererecurrenceofbleedingwasobserved.All thepatientshadacranial computed tomography (CT)scanonadmission,acontrol CT scan 24 hours after admittance, and a further CT scan before thepatient was transferred to another hospital. In addition, a head CT wasperformedwheneverapatient’sconditiondeteriorated.DVTduplexandcompressionultrasonographywereperformeddirectly ifsignsor symptoms of DVT appeared and for all patients before discharge fromhospital.OutcomesThe primary endpointwas the occurrence of a confirmed VTE, defined as thecomposite of symptomatic or asymptomatic DVT, or symptomatic or fatal PE(death related to VTE) occurring during the treatment period (up to 90 daysaftertheonsetofthestroke).Secondary endpoints included significantly increased ICH volume (>33%)observed in a head CT or autopsy, including recurrent bleeding, other severebleeding complications, cardiovascular death or death due to any causeoccurringwithinthetreatmentperiod.Inthecaseofdeathfromanycausewhilestill in hospital an autopsy was performed. If death occurred later in thetreatmentperiodandoutsidehospital,anautopsywasrecommended.All therecruitedpatientswere followedup for threemonths fromtheonsetofthebleeding.AheadCTwasperformedonallpatientsduringacontrolvisit tohospital. GOS and RANKIN scale examinations were performed during thefollow-upinacontrolvisitorinsomecasesbytelephonetoeitherthepatientora relative. Good or poor outcome was measured according to modified GOS:1=normal, 2=minimal disability, 3=moderate disability, 4=severe disability,5=vegetative state, and 6=dead.With this scale 1-3was considered as a goodoutcomeand4-6asapooroutcome.

SamplesizeThedesiredsamplesizewascalculatedon thebasisofa fifteenpercent (15%)expectedincidenceoftheprimaryendpointinthelateenoxaparingroupandafivepercent(5%)incidenceintheearlyenoxaparingroup.Alternatively, a similar sample size would be needed to reveal a significantdifferenceifbleedingcomplicationsweretooccurinfifteenpercent(15%)oftheearlyenoxaparingroupandfivepercent(5%)ofthelateenoxaparingroup.Approximately320patients(160ineachgroup)wouldbeneededtodetectthesedifferencesbyamarginoftenpercent(10%)ataalevelof0.05(two-tailed)anda b level of 0.2. After recruiting the first 80 patients an independent safetycommittee analysed the observations. Non-significant differencewas observedbetween the enoxaparin and placebo groups and the safety committee gavepermissiontocontinuepatientrecruitment.RandomizationSubcutaneousinjectionswereobtainedfromthehospitalpharmacy.Therewerealways 2-3 sets of injections ready for all eligible study patients be theyenoxaparin or placebo. All the injection sets looked exactly the samewhetherthey include enoxaparin or saline. The investigator randomly chose one of theinjectionsetsandthecodefortheinjectionsetwasplacedinthesealedenvelopetogetherwith the patient study number. The same informationwas sealed fortheemergencyenvelope.Envelopeswereopenedafterthestudy.Oneemergencyenvelopewasopenedduring thestudydue toseverere-bleeding36hafter theonset, and in that case thepatienthad received theplacebo.Thepatient studycodeand IDweresealed inanotherenvelopewhichwasopenedonlyafter thestudy. Thismethod of preparing the studymedicine in the hospital pharmacyensuredthattherewouldbenofinancialconflictofinterest.BlindingThe envelopes containing patient study code and the injection set code wereopenedduringawitnessedmeetingonlyaftertheendofthestudy.Thismethodensuredthatboththeinvestigatorsandthedoctorsondutywereblindedastotheassignmentofthepatienttoaparticulargroup(treatmentorplacebo).RadiologicalmethodsThesitesofthehematomasweredividedintothefollowinggroups:subcortical,putaminal, thalamic, combined (extension of a putaminal hematoma into thethalamusand/orextensivelyintothesubcorticalwhitematter),caudatenucleus,cerebellar or pontine. Hematoma volumes were calculated from the CT scansusingthefollowingformulaforanellipsoid:volumeABC/2[10](whereA,BandCrepresenttheradiiinthreedimensions).Oneoftheseradiiwasmeasuredfromthe largestdiameteron theCT imagewith the largestareaof ICHand the two

remaining radii were measured perpendicularly to the largest diameter. Thedegreeof intraventricularhemorrhage(IVH)wasclassifiedas follows:grade0,noIVH;grade1,asmallamountofbloodintheoccipitalhornsorinthethirdorfourthventricle;grade2,bloodoccupyingmostofone lateralventriclewithorwithoutbloodinthethirdorfourthventricle;andgrade3,majorIVHwithbloodfilling all ventricles and frequently distending the ventricular system[11]. Anincreaseinhematomasize>33%wasconsideredasignificantenlargementandled to cessation of the placebo/ enoxaparinmedication. All the CT scanswereexamined and the hematoma volumes measured by the same experiencedneurosurgeon (SJ), who was blinded with respect to the patient records andmodesoftreatment.Compression ultrasonography of both legs or, alternatively, bilateral contrastvenography, was performed according to a standardized protocol. PE wasconfirmed by available methods, i.e., ventilation perfusion (VQ) or thoracichelicalTscan,pulmonaryangiography,orautopsy.StatisticalmethodsCategorical variableswere compared using the Fisher exact or two-tailed test.Continuous variables were compared between groups by using the Mann–Whitney U-test or Student t-tests. A probability value less than 0.05 wasconsideredsignificant.DataavailabilitystatementAuthorsstatethatanonymizeddatawillbesharedbyrequestfromanyqualifiedinvestigator,pleasecontactthecorrespondingauthor.ResultsTheparticipant flowdiagramisshowninFigure1.149patientswereenrolledfor the study. Inninepatients theexact timeofonsetof strokewasuncertainand these patients were excluded. One patient refused to take a part in thisstudy.After initial checkingof theexclusioncriteria,a totalof139consecutivepatientswereenrolledinthestudy.Completefollowupdataexistedforall139patients.ThebaselinecharacteristicsofthepatientsareshowninTable1.Therewere68whohadreceivedearlyenoxaparin(24h)and71whostartedenoxaparin lateron(72h).ThereweresignificantlymorepreviousNSAIDusers(non-ASA)intheplacebogroupthanintheenoxaparingroup(9vs.0,p<0.005).TheclinicalcharacteristicsandoutcomesofthepatientsareshowninTable2.One patient in the placebo group (1%) and 2 in the enoxaparin group (3%)developedDVT,anoverallrateof2%,butnonedevelopedPE.Accordingly,therewasnosignificantdifferencebetweenthetwogroupsregardingtheoccurrenceofVTE.Sixteenofthepatients(12%)hadsignificant(>33%)enlargementofthehematomaobservableinrepeatedheadCTscans,eightinbothgroups(p=0.927).

No statistically significant difference in outcome was observed between theenoxaparinandplacebogroupsas29patientsinthefirstand31patientsinthelattergrouphadagoodoutcome(GOS1-3,p=0.904).Anon-significantdifferenceinmortalityrateswasobservedbetweenthegroups,as12patients(18%)diedwithin3monthsintheenoxaparingroupcomparedto11patients(15%)intheplacebogroup,p=0.733.OnlyonepatientwasautopsiedandnoVTEnorPEwasfound.Clinicaldataforthe3patientswhodevelopedDVTcanbeseeninTable3.Allofthem had been taking aspirin as a regularmedication before the onset of thebleeding.Nonehadbeenonanticoagulationbeforetheictus,andallthreehadapooroutcome(GOS4-6).DiscussionThe aim of this work was to evaluate the safety and efficacy of early onsetenoxaparintreatmentforthepreventionofVTEamongpatientswithICH.Inthetreatmentgroupenoxaparin(anLMWHdrug)wasadministeredatadoseof40mgdailystarting24haftertheonsetofICHandcomparedwithaplaceboforthefirst three days. Thereafter, i.e. from the 4th day onwards, all the patientsreceivedenoxaparinsubcutaneouslyuntiltheywereabletowalkorweremovedtoanotherhospital.Wefoundthattheearlytreatmentwasaseffectiveandsafeas the treatment started 72h after the onset of ICH. Thosewho received earlyenoxaparin showed neither enlargement of the hematoma nor had a pooroutcomeanddeathanymorethanthosewhofirstreceivedenoxaparinlateron.There are only three published prospective randomized studies regardingphrophylacticuseofLMWH for thepreventionofvenous thromboembolism inICHpatients[12-14].IntheearlystudybyDickmann[12]etal46patientswererandomizedintotwogroups.Thefirstgroup(n=23)receivedheparin(3x5000units/day)4daysafterICHandthesecondgroup(n=23)10daysaftertheonsetof ICH. Eighteen patients had evidence of VTE, and 14 patients had PE. Nosignificant differences were found between the groups and heparin did notincrease the risk of re-bleeding. Orken [14] prospectively randomized 75 ICHpatients into twogroups,oneofwhich (n=39)receivedLMWH(enoxaparin40mg/ds.c.)48hoursaftertheonsetofICHwhiletheothergroup(n=36)receivedonly long compression stockings. Four symptomaticDVTswere observed, 3 ofthem (4%) in the LMWHgroup.No hematoma growthwas observed in eithergroup, and the authors concluded that LMVH prophylaxis should be used inpatients with ICH. Boeer [13] randomized 68 ICH patients into three groups,receiving low-doseheparins(3x5000units/days.c.)2(n=22),4(n=23)or10(n=23)daysafterICH.Againtherewerenodifferencesinrecurrenthemorrhagerates between the groups, but the early treatment group (2 days) showedsignificantly less PE (n=1, 5%) comparedwith the others (n=5, 22% and n=9,39%).Theseotherstudies,however,hadsignificantlysmallersamplesizesthanthis study, which also employed more specific criteria for the prospectiveanalysis of hematoma enlargement, and also started LMWH treatment earlier(only24hafteronset).

Other studieson this issuehavebeen retrospectiveonesand the timingof theinitiationoftreatmentvarieswidely.Tetrietal.[15]foundintheirseriesof407patientsthattherateofclinicalVTeventsinthosewhoreceivedenoxaparin20mgonceadaywas3%.AslightlylowerVTErateoccurredinthepresentstudyand the number of events did not increase if the LMWHdrugwas introducedlater(onthe4thday).PEdidnotoccuratall,butitshouldberememberedthatthe authors did not routinely perform embolic CT scans on asymptomaticpatients.Elsewhere,Kleindiestetal. [16]reportedDVTandPEin0.4%oftheirpatients. That study, however, was retrospective in nature and also includedarteriovenous malformation, SAH and cerebral infarction patients, for whomonly limited information was available as to whether they hadhemiparesis/hemiplegia.All thepresent patients had lower limbparalysis andwere unable to walk when enrolled for this study. In the case of theseretrospective studies no straightforward conclusions can be drawn as towhetheritissafetouseanticoagulantsforICHpatients,andifso,whenitissafetocommencetreatmentandthemostappropriatedosestoutilize.IntherecentAHA/ASAguideline[17]andanESOguideline[18]itisconcludedthat the evidence for when to recommend LMWH for ICH patients is weak.AHA/ASArecommendsLMWHforICHpatients1to4daysafteronset,andstatesthatcurrentdatasuggeststhatadministeringLMWHdoesnotseemtoincreasethe incidence of recurrent hemorrhage. This is based on the two smallrandomizedstudiesmentionedabove,namelyDickman1988(with46patients)andBoeer1991(withanadditional22patients).Unfortunately,theseseriesalsoincludedangiomas,aneurysmsandembolicstrokepatients(n=12).Besidesthesmall sample size, it is also unclear whether ES or IPC was applied. The ESOguidelinedoesnotmakeanyrecommendationinthismatterduetothelackofalargeRCT.Intheabsenceofproperrecommendations,cliniciansarereluctanttoadminister LMWH to ICH patients for fear of hemorrhagic complications. It issignificantthatinthepaperpublishedbyPrabhakaranetal.[19],only16.5%ofthe ICH patients received any medical thrombosis prophylactics during theirhospitalstayand44.8%ofthesebegantoreceive itonday2. It isclearthat inthe current situation a large number of ICH patients do not have properthrombosisprophylaxis.Three patients in the present series (2%) developed DVT, one in the placebogroupandtwointheenoxaparingroup,whenfollowingtheguidelinesstrictlyina prospective setting. However, no PE events occurred, even though routinepulmonary CT was not performed and only one patient who died during thefollow-up period was autopsied, revealing neither PE nor DVT. The patients’outcomesdidnotdifferbetweenthetwogroups:42%intheplacebogroupand44%intheenoxaparingrouphadagoodoutcome(GOS1-3)and58%and56%,respectively, a poorer outcome (GOS 4-6). It seems that if the guidelines arefollowedstrictlyandifLMWHtreatmentisactuallystartedatanearlystageafterICH,VTEeventswillbecomeveryrareeveninpatientshavingmajorriskfactorsforthese.

This is the largestrandomizeddouble-blindedstudytodate thathasevaluatedthesafetyandefficacyofadministeringananticoagulanttoprimaryICHpatients.Our goalwas to collect320patients (160 in eachgroup), butdue to the strictinclusioncriteriaoflowerextremitieparesis,wecouldonlyachieve136patientsin the stipulated 10-year period, in spite of the national multicenter setting.Therefore,anadequatesamplesizewasnotreached.Additionalrecruitmentofseveralhundredmorepatientsforseveraladditionalyearswouldbeneededtoeven showa trend for associationbetween lowerVTEoccurrencewith earlieradministrationofenoxaparin.Therecruitmentofpatientswasthereforeended.Nevertheless,thestrictinclusioncriteriaandthedouble-blindedrandomizationproceduredomeanthat theresultsaddvaluable information to thepreviouslylimited data available in this field. In this study, bilateral ultrasound wasperformedroutinelyoneverypatientinthehospitalperiod.ThelimitationsarethatpulmonaryCTwasonlycarriedoutforsymptomaticpatients(notroutinely)andonlyoneofthedeceasedpatientswasautopsiedtodetectVTE.ConclusionsThromboemboliccomplicationsareveryrareinparalyzedICHpatientsifIPCisused together with compression stockings and early LMWH. The data in thisstudysuggeststhatadministeringananticoagulanttoaspontaneousICHpatientissaferegardlessofwhetheritisstarted24hours(early)or72hours(late)afterthe hemorrhage. No risk of hematoma enlargement is associated withadministering20mgof anticoagulant LMWH twice aday at an early stage, nordoeslateadministrationofLMWHentailanadditionalriskofVTE.OtherinformationConflictofinterest:None.Funding:TTreceivedacademicgrantsforICHresearchfromHelsinkiUniversityCentralHospital,UniversityofGothenburg,SahlgrenskaUniversityHospital,andSigridJuseliusFoundation.STreceivedacademicgrantsfromFinnishMedicalFoundations.Registration:TrialRegistrationNumberNTC00699465,EudraCTnumber2007-006206-24

Reference List
(1) Warlow C, Ogston D, Douglas AS. Deep venous thrombosis of the legs after strokes: Part 2-Natural history. Br Med J 1976;1:1181-1183.
(2) Clagett GP, Anderson FA, Jr., Levine MN, Salzman EW, Wheeler HB. Prevention of venous thromboembolism. Chest;102:391S-407S.
(3) McCarthy ST, Turner JJ, Robertson D, Hawkey CJ, Macey DJ. Low-dose heparin as a prophylaxis against deep-vein thrombosis after acute stroke. Lancet 1977;2:800-801.
(4) Kelly J, Rudd A, Lewis R, Hunt BJ. Venous thromboembolism after acute stroke. Stroke 2001;32(1):262-267.
(5) Broderick J, Connolly S, Feldmann E, Hanley D, Kase C, Krieger D, Mayberg M, Morgenstern L, Ogilvy CS, Vespa P, Zuccarello M. Guidelines for the management of spontaneous intracerebral hemorrhage in adults: 2007 update: a guideline from the American Heart Association/American Stroke Association Stroke Council, High Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdisciplinary Working Group. Circulation 2007;116:391-413.
(6) Dennis M, Sandercock PA, Reid J, Graham C, Murray G, Venables G, Rudd A, Bowler G. Effectiveness of thigh-length graduated compression stockings to reduce the risk of deep vein thrombosis after stroke (CLOTS trial 1): a multicentre, randomised controlled trial. Lancet 2009;373:1958-1965.
(7) Dennis M, Sandercock P, Reid J, Graham C, Murray G, Venables G, Rudd A, Bowler G. The effect of graduated compression stockings on long-term outcomes after stroke: the CLOTS trials 1 and 2. Stroke 2013;44:1075-1079.
(8) Hemphill JC, III, Greenberg SM, Anderson CS, Becker K, Bendok BR, Cushman M, Fung GL, Goldstein JN, Macdonald RL, Mitchell PH, Scott PA, Selim MH, Woo D. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2015;46:2032-2060.
(9) Steiner T, Kaste M, Forsting M, Mendelow D, Kwiecinski H, Szikora I, Juvela S, Marchel A, Chapot R, Cognard C, Unterberg A, Hacke W. Recommendations for the management of intracranial haemorrhage - part I: spontaneous intracerebral haemorrhage. The European Stroke Initiative Writing Committee and the Writing Committee for the EUSI Executive Committee. Cerebrovasc Dis 2006;22:294-316.
(10) Kothari RU, Brott T, Broderick JP, Barsan WG, Sauerbeck LR, Zuccarello M, Khoury J. The ABCs of measuring intracerebral hemorrhage volumes. Stroke 1996;27(8):1304-1305.
(11) Juvela S. Risk factors for impaired outcome after spontaneous intracerebral hemorrhage. Arch Neurol 1995;52:1193-1200.
(12) Dickmann U, Voth E, Schicha H, Henze T, Prange H, Emrich D. Heparin therapy, deep-vein thrombosis and pulmonary embolism after intracerebral hemorrhage. Klin Wochenschr 1988;66:1182-3.
(13) Boeer A, Voth E, Henze T, Prange HW. Early heparin therapy in patients with spontaneous intracerebral haemorrhage. J Neurol Neurosurg Psychiatry 1991;54:466-467.

(14) Orken DN, Kenangil G, Ozkurt H, Guner C, Gundogdu L, Basak M, Forta H. Prevention of deep venous thrombosis and pulmonary embolism in patients with acute intracerebral hemorrhage. Neurologist 2009;15:329-331.
(15) Tetri S, Hakala J, Juvela S, Saloheimo P, Pyhtinen J, Rusanen H, Savolainen ER, Hillbom M. Safety of low-dose subcutaneous enoxaparin for the prevention of venous thromboembolism after primary intracerebral haemorrhage. Thromb Res 2008;123:206-212.
(16) Kleindienst A, Harvey HB, Mater E, Bronst J, Flack J, Herenz K, Haupt WF, Schon R. Early antithrombotic prophylaxis with low molecular weight heparin in neurosurgery. Acta Neurochir (Wien ) 2003;145:1085-1090.
(17) Hemphill JC 3rd, Greenberg SM, Anderson CS, Becker K, Bendok BR, Cushman M, Fung GL, Goldstein JN, Macdonald RL, Mitchell PH, Scott PA, Selim MH, Woo D; American Heart Association Stroke Council; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2015;46:2032-60
(18) Steiner T, Al-Shahi SR, Beer R, Christensen H, Cordonnier C, Csiba L, Forsting M, Harnof S, Klijn CJ, Krieger D, Mendelow AD, Molina C, Montaner J, Overgaard K, Petersson J, Roine RO, Schmutzhard E, Schwerdtfeger K, Stapf C, Tatlisumak T, Thomas BM, Toni D, Unterberg A, Wagner M. European Stroke Organisation (ESO) guidelines for the management of spontaneous intracerebral hemorrhage. Int J Stroke 2014;9:840-855.
(19) Prabhakaran S, Herbers P, Khoury J, Adeoye O, Khatri P, Ferioli S, Kleindorfer DO. Is prophylactic anticoagulation for deep venous thrombosis common practice after intracerebral hemorrhage? Stroke 2015;46:369-75

Table 1. Baseline Characteristics of 139 patients with spontaneous ICH Placebo
n=68 Enoxaparin
n=71 Total
n=139 Male n(%) 36 (53) 36 (51) 72 (52) Mean age, y(±SD) 68±6 66±19 67±11 Previous diseases n(%)
Hypertension 54 (79) 52 (73) 106 (76) Cardiac disease 18 (26) 14 (20) 32 (23) Atrial Fibrillation 12 (18) 6 (8) 18 (13) Diabetes 9 (13) 16 (23) 25 (18) Cancer 2 (3) 5 (7) 7 (5) Brain infarction/TIA 11 (16) 11 (15) 22 (16) Epilepsy 2 (3) 2 (3) 4 (3)
Heavy drinking n(%) 4 (6) 2 (3) 6 (4) VTE in history n(%)* 0 (0) 4 (6) 4 (3) Previous medications n(%)
anticoagulants 11 (16) 11 (15) 22 (16) aspirin 19 (28) 29 (41) 48 (35) clopidogrel 2 (3) 4 (6) 6 (4) dipyridamol 1 (1) 3 (4) 4 (3) SSRI 5 (7) 4 (6) 9 (6) NSAID* 9 (13) 0 (0) 9 (6)
*p <0.005

Table 2. Clinical Characteristics and Outcome of 139 patients with spontaneous ICH Placebo
n=68 Enoxaparin
n=71 Total
n=139 Hematoma volume, ml (±SD) 21±23 28±31 24±27 Location of hematoma, n(%)
Subcortex 10 (15) 21 (30) 31 (22) Putamen 26 (38) 21 (30) 47 (34) Thalamus 19 (28) 14 (20) 33 (24) Basal ganglia 5 (7) 9 (13) 14 (10) Combined 6 (9) 5 (7) 11 (8) Other 2 (3) 1 (1) 3 (2)
Intraventricular haemorrhage, n(%) 45 (66) 53 (75) 98 (71) Later hematoma evacuation, n(%) 2 (3) 3 (4) 5 (4) Mean ICH Score, (±SD) 1.4±1.0 1.4±1.1 1.4±1.0 Mean GCS score, (±SD) 14±2 13±3 13±2 Complications, n(%)
hematoma enlargement 33% 8 (12) 8 (11) 16 (12) GI-bleeding 0 (0) 0 (0) 0 (0) Seizure 4 (6) 3 (4) 7 (5) DVT 1 (1) 2 (3) 3 (2) PE 0 (0) 0 (0) 0 (0)
Outcome GOS 1-3 (good) 29 (42) 31 (44) 60 (43) GOS 4-6 (poor) 39 (57) 40 (56) 79 (57) Death within 3 mo 12 (18) 11 (15) 23 (17) GCS=Glasgow Coma Scale, DVT=Deep venous thrombosis, PE=Pulmonary embolism, GI=gastrointestinal, GOS=Glasgow Outcome Scale, BP=Blood pressure

Table 3. Baseline, Clinical characteristics and outcome of 3 DVT patients Patient 1 Patient 2 Patient 3 Age (yr.) 66 95 71 ICH volume, ml 49 50 45 ICH Score 1 1 1 GCS 11 14 15 Hematoma location subcortical putaminal basal ganglia Previous diseases
Cardiac disease no yes yes Atrial fibrillation no yes no Diabetes yes no yes
Previous medications Antigoaculants no no no ASA yes yes yes
Complications Hematoma enlargement no no no Pneumonia no yes no
Outcome NIHSS 22 21 8 GOS 6 5 4 Dead within 3 mo yes no no NIHSS=, GOS=Glascow Outcome Scale

Figure 1. Consort flow diagram of progress through phases of the trial.
Assessed for eligibility (n=149 )
Excluded (n=10)
Not meeting inclusion criteria (n=9)
Declined to participate (n=1)
Analysed (n=68 )
Excluded from analysis (n=0 )
Lost to follow-up (n=0)
Follow up included CT within 24 hours after
admission, both legs duplex ultrasound beforedischarge and outcome 3 months after the
onset
Placebo group (n=68 )
Received late enoxaparin (n=68 )
Lost to follow-up (n=0 )
Follow up included CT within 24 hours after
admission, both legs duplex ultrasoundbefore discharge and outcome 3 months after
the onset
Allocated to intervention (n=71 )
Received early enoxaparin (n=71 )
Analysed (n=71 )
Excluded from analysis (n=0)
Allocation
Analysis
Follow-Up
Randomized (n=139 )
Enrollment