Embed Size (px)
Citation preview

EVIDENCE-BASED DIAGNOSTICS
Spontaneous Subarachnoid Hemorrhage:A Systematic Review and Meta-analysisDescribing the Diagnostic Accuracy of History,Physical Examination, Imaging, and LumbarPuncture With an Exploration of TestThresholdsChristopher R. Carpenter, MD, MSc, Adnan M. Hussain, MD, Michael J. Ward, MD, MBA,Gregory J. Zipfel, MD, Susan Fowler, Jesse M. Pines, MD, MBA, MSCE, andMarco L. A. Sivilotti, MD, MSc
AbstractBackground: Spontaneous subarachnoid hemorrhage (SAH) is a rare, but serious etiology of headache.The diagnosis of SAH is especially challenging in alert, neurologically intact patients, as missed ordelayed diagnosis can be catastrophic.
Objectives: The objective was to perform a diagnostic accuracy systematic review and meta-analysis ofhistory, physical examination, cerebrospinal fluid (CSF) tests, computed tomography (CT), and clinicaldecision rules for spontaneous SAH. A secondary objective was to delineate probability of diseasethresholds for imaging and lumbar puncture (LP).
Methods: PubMed, Embase, Scopus, and research meeting abstracts were searched up to June 2015 forstudies of emergency department patients with acute headache clinically concerning for spontaneousSAH. QUADAS-2 was used to assess study quality and, when appropriate, meta-analysis was conductedusing random effects models. Outcomes were sensitivity, specificity, and positive (LR+) and negative(LR�) likelihood ratios. To identify test and treatment thresholds, we employed the Pauker-Kassirermethod with Bernstein test indication curves using the summary estimates of diagnostic accuracy.
Results: A total of 5,022 publications were identified, of which 122 underwent full-text review; 22 studieswere included (average SAH prevalence = 7.5%). Diagnostic studies differed in assessment of history andphysical examination findings, CT technology, analytical techniques used to identify xanthochromia, andcriterion standards for SAH. Study quality by QUADAS-2 was variable; however, most had a relativelylow risk of biases. A history of neck pain (LR+ = 4.1; 95% confidence interval [CI] = 2.2 to 7.6) and neckstiffness on physical examination (LR+ = 6.6; 95% CI = 4.0 to 11.0) were the individual findings moststrongly associated with SAH. Combinations of findings may rule out SAH, yet promising clinicaldecision rules await external validation. Noncontrast cranial CT within 6 hours of headache onsetaccurately ruled in (LR+ = 230; 95% CI = 6 to 8,700) and ruled out SAH (LR� = 0.01; 95% CI = 0 to 0.04);CT beyond 6 hours had a LR� of 0.07 (95% CI = 0.01 to 0.61). CSF analyses had lower diagnostic
From the Division of Emergency Medicine, Washington University in St. Louis School of Medicine (CRC), St. Louis, MO; theDepartment of Emergency Medicine, Northwestern University Feinberg School of Medicine (AMH), Chicago, IL; the Departmentof Emergency Medicine, Vanderbilt University (MJW), Nashville, TN; the Department of Neurosurgery, Washington University inSt. Louis (GJZ), St. Louis, MO; Becker Medical Library, Washington University School of Medicine in St. Louis (SF), St. Louis, MO;the Department of Emergency Medicine and Center for Practice Innovation, George Washington University (JMP), Washington,DC; and the Department of Emergency Medicine and Department of Biomedical & Molecular Sciences, Queen’s University,Kingston, Ontario, Canada.Received January 22, 2016; revision received March 31, 2016; accepted April 2, 2016.Portions of this manuscript were presented at the American College of Emergency Physicians annual meeting, Seattle, WA,October 2013.The authors have no relevant financial information or potential conflicts to disclose.Supervising Editor: Shahriar Zehtabchi, MD.Address for correspondence: Christopher Carpenter, MD, MSc; e-mail: [email protected]. Reprints will not be available.A related article appears on page 1077.
© 2016 by the Society for Academic Emergency Medicine ISSN 1069-6563 963
PII ISSN 1069-6563583 963doi: 10.1111/acem.12984

accuracy, whether using red blood cell (RBC) count or xanthochromia. At a threshold RBC count of1,000 9 106/L, the LR+ was 5.7 (95% CI = 1.4 to 23) and LR� was 0.21 (95% CI = 0.03 to 1.7). Using thepooled estimates of diagnostic accuracy and testing risks and benefits, we estimate that LP only benefitsCT-negative patients when the pre-LP probability of SAH is on the order of 5%, which corresponds to apre-CT probability greater than 20%.
Conclusions: Less than one in 10 headache patients concerning for SAH are ultimately diagnosed withSAH in recent studies. While certain symptoms and signs increase or decrease the likelihood of SAH, nosingle characteristic is sufficient to rule in or rule out SAH. Within 6 hours of symptom onset,noncontrast cranial CT is highly accurate, while a negative CT beyond 6 hours substantially reduces thelikelihood of SAH. LP appears to benefit relatively few patients within a narrow pretest probability range.With improvements in CT technology and an expanding body of evidence, test thresholds for LP maybecome more precise, obviating the need for a post-CT LP in more acute headache patients. ExistingSAH clinical decision rules await external validation, but offer the potential to identify subsets most likelyto benefit from post-CT LP, angiography, or no further testing.
ACADEMIC EMERGENCY MEDICINE 2016;23:963–1003 © 2016 by the Society for Academic EmergencyMedicine
Headache is a common presenting complaint tothe emergency department (ED) and representsapproximately 2% of ED visits annually in the
United States.1 While most headaches are self-limiting,the possibility of spontaneous subarachnoid hemor-rhage (SAH) is an important diagnostic consideration inpatients presenting with a sudden, severe headache.These sudden-onset headaches include the classic“thunderclap headache” that instantaneously peaks atheadache onset, as well as headaches that reach maxi-mal severity within seconds to 1 hour of onset. Sudden-onset headaches include a wide spectrum of possiblediagnoses, including SAH (approximately 1% of acuteheadaches), benign postcoital headache, exertional head-ache, intracranial cysts or tumors, intracerebral hemor-rhage, hypophyseal apoplexy, sphenoid sinusitis, sinusthrombosis, cough-related headache, vascular dissection,cerebral vasospasm, and migraine headaches.2–10
Migraine and other more benign headaches mimic SAHand are estimated to be at least 50 times more commonthan SAH.11 Moreover, while SAH is often caused by aruptured cerebral aneurysm and represents a neurosur-gical emergency, a variety of other SAH etiologies rangefrom the benign, low-pressure perimesencephalic hem-orrhage, which can be treated conservatively,12,13 to vas-cular malformations, arterial dissection, and vasculitis,which require time-sensitive interventions (Table 1).14
Thus, the diagnostic approach to acute headacheepitomizes the practice of emergency medicine with ahigh-stakes condition without a clear-cut presentationlurking within a high-volume complaint, and ultimatelymost patients do not have a serious diagnosis.
Between 1960 and 1995, the 6-month mortality ofaneurysmal SAH decreased by 15%,15 but mortalityremains 27%–44% with substantial regional variabil-ity.16 Up to 25% of patients die within 24 hours, and the3-month mortality rate can be as high as 50% withoutearly definitive treatment.17 In addition, one-third ofSAH survivors suffer neurologic deficits affecting theirdaily lives15 and up to 50% never return to work.18
Early detection and treatment can significantly reducemorbidity and mortality.11,19 However, SAH can be achallenging diagnosis to make, particularly in alert, neu-rologically intact adults.20 Missed diagnosis is the
primary reason for delayed treatment and case seriessuggest that 12%–53% of SAH cases are misdiagnosedon their initial presentation in a variety of settings,including the ED.21 Patients with misdiagnosed or undi-agnosed warning bleeds that subsequently rebleed havea 70% mortality.22–25 ED providers miss the diagnosis ofSAH in about 5% of cases, primarily those with loweracuity at presentation and misdiagnosis is estimated tobe more likely in nonteaching hospitals.26,27 Most emer-gency medicine and neurosurgery textbooks providelimited guidance on the diagnostic accuracy and utilityof history, physical examination, cerebrospinal fluid(CSF) analysis, or computed tomography (CT) forthe diagnosis of SAH.28,29 Indeed, given the serious nat-ure of the condition, few have proposed a sensiblethreshold below which testing is not necessary, whichcontributes to overtesting and the unintended conse-quences that include incidental findings with prolongedpatient uncertainty.30
Unenhanced cranial CT is usually the first-line diag-nostic test to evaluate for suspected SAH. Becauseearly-generation CTs did not detect up to 5% of SAHs,traditional teaching has emphasized the need to per-form lumbar puncture (LP) to exclude SAH to reducethe probability of error. Yet many patients fear havingan LP because an LP is painful and invasive and canlead to a post-LP headache in 6%–30% of patients
Table 1Potential Etiologies of Spontaneous SAH
Cerebral aneurysmPerimesencephalicIsolated convexityVascular malformations (arteriovenous malformations/AVF)Arterial dissectionCerebral amyloid angiopathyMoyamoyaVasculitis (PRES, RCVS, lupus)Coagulopathy (thrombocytopenia, anticoagulation)Sickle cell diseaseHypertensionSympathomimetic drugs
SAH = subarachnoid hemorrhage.
964 Carpenter et al. • SUBARACHNOID HEMORRHAGE EVIDENCE-BASED DIAGNOSTICS

depending on the gauge of the LP needle.31 Additionalclinician-level barriers to LP testing include the timeneeded to perform32 and low diagnostic yield.20,33–36 Inaddition, LP may be contraindicated if a patient has ableeding disorder or increased intracranial pressure orsimply does not consent to the procedure.37 Despitedogma, LP is not always performed after CT and multi-center observational studies report that fewer than halfof acute headache patients undergo LP following a neg-ative CT to “rule out” SAH. Even in these studies lessthan one in 100 LPs are ultimately deemed “true posi-tives” after negative CT using a third-generation scan-ner.38,39 Additionally, the specificity of LP is reduced by“traumatic taps” in which bleeding from the procedurecontaminates the CSF being collected, estimated tooccur in about one in six LPs.40 Identifying xanthochro-mia due to the breakdown of hemoglobin in CSF is con-sidered to be pathognomonic for SAH, yetxanthochromia requires up to 12 hours to develop andis prone to false positives due to ex vivo hemolysis orhyperbilirubinemia.21,41 National guidelines in the Uni-ted Kingdom advocate using spectrophotometry toidentify xanthochromia, yet nearly all North Americanhospitals rely on visual inspection alone.42 A recent sys-tematic review comparing visual inspection to spec-trophotometry to detect CSF xanthochromia was unableto draw a conclusion due to significant heterogeneity inthe underlying studies.43
To our knowledge, there are no prior systematicreviews assessing the diagnostic accuracy of history,physical examination, and imaging studies for SAH inthe setting of acute-onset headache patients in the ED.Therefore, we set out to collect and summarize theavailable published literature regarding these charac-teristics as well as LP findings and clinical decisionrules for spontaneous (nontraumatic) SAH. Since recentsystematic reviews have evaluated CT angiography(CTA)44 and magnetic resonance angiography (MRA),45
we did not repeat these meta-analyses. However,additional studies exploring visible xanthochromiadiagnostic accuracy have been published since the 2014systematic review by Chu et al.43 so we report anupdated meta-analysis of visible xanthochromia. Wealso used these diagnostic accuracy estimates to delin-eate an optimal diagnostic strategy using the test–treat-ment threshold approach of Pauker and Kassirer.46,47
In particular, we used the graphical Bayesian approachof test indication curves first proposed by Bernstein48
to identify the a priori likelihood of disease in patientsfor whom LP would be rational despite a negativecranial CT.
METHODS
Study DesignWe conducted a systematic review and meta-analysis oforiginal research studies that reported data on the diag-nosis of SAH in ED patients with acute headache. Thedesign and manuscript structure conform to the recom-mendations from the Preferred Reporting Items for Sys-tematic Reviews and Meta-Analyses (PRISMA)49 andthe Meta-analysis of Observational Studies (MOOSE)criteria.50 Studies were included if they described adult
patients (14 years or older) seen in an ED with acuteheadache or other symptoms or signs (such as syncope,acute mental status change, or otherwise unexplainednausea) and in whom SAH was a diagnostic considera-tion. In addition, studies had to report sufficient detailon the diagnostic test and criterion standard to be ableto construct two-by-two tables. We elected to define“disease positive” as being an acute SAH includingnonaneurysmal SAH (e.g., perimesencepahlic hemor-rhage) as most original studies did not distinguishbetween SAH subtypes. We recognized that CT findingsof subarachnoid blood were therefore incorporated intothis definition, thereby inflating CT sensitivity, speci-ficity, positive likelihood ratio (LR+), and negative likeli-hood ratio (LR�; incorporation bias), but report theseestimates for completeness.51 Recognizing the absenceof an accepted definition for a positive LP, we analyzedseparately an erythrocyte count above 1,000 9 106/L inthe final tube as well as either visible or spectrophoto-metric xanthochromia. Patients with negative imagingin whom LP was not performed were deemed as “dis-ease negative” only when the authors reported effort atfollow-up after hospital discharge. We excluded studiesthat solely reported data on patients with SAH (i.e.,where only sensitivity could be calculated), precludingan estimate of specificity or LRs.
Search StrategyWe searched the published literature using strategiescreated for the concepts of emergency department,headache, subarachnoid hemorrhage, physical exam,and diagnostic accuracy. Search strategies were estab-lished using a combination of standardized terms andkeywords and were implemented in PubMed 1946–,Embase 1947–, and Scopus 1823–. All searches werecompleted in June 2015 and limited to English usingdatabase supplied limits. Full search strategies forPubMed and Embase are provided in the Data Supple-ment S1 (available as supporting information in theonline version of this paper). One author (AMH) inde-pendently reviewed the titles and abstracts to identifypotentially relevant articles. Where there were questionsabout inclusion, this was discussed with a secondauthor (JMP) and a consensus decision was made aboutwhether the article should be included for full-textreview. Studies deemed not to contain clear inclusion orexclusion criteria were evaluated by a second author(JMP) before final inclusion or exclusion.
Data from each study were independently abstractedby two authors (AMH, CRC). Information abstractedincluded the individual study setting, inclusion criteria,exclusion criteria, specific CT (machine, slice number,and type of CT image), definition of disease, criteria fora positive LP, follow-up description, and whether or notthere was neurosurgical intervention. The abstracteddata were constructed into tables, which were con-firmed by a second author (CRC); any uncertainty wasdiscussed between the two authors and a consensusdecision was made. In addition, the references for eachfull-text article were reviewed to assess whether addi-tional studies could be included in the review, whichwere then assessed by full-text review. The authors con-ducted bibliographic searches of research abstracts
ACADEMIC EMERGENCY MEDICINE • September 2016, Vol. 23, No. 9 • www.aemj.org 965

presented at scientific meetings published in AcademicEmergency Medicine, Annals of Emergency Medicine,Stroke, Neurology, and Neurosurgery, from 2002through October 2015.
Individual Evidence Quality AppraisalTwo authors (AMH, MJW) independently used theQuality Assessment Tool for Diagnostic AccuracyStudies (QUADAS-2)52 for systematic reviews to evalu-ate the quality of evidence for the studies identified.These two authors used several a priori conditions toevaluate an individual study’s risk of bias and degree ofapplicability.
• In the assessment of “inappropriate exclusions”reviewers assessed whether a study’s inclusion andexclusion criteria led investigators to evaluate sus-pected SAH patients who were more or less acutelyill than those typically evaluated in ED settings,which could introduce spectrum bias51 or spectrumeffect53 and skew observed estimates of sensitivity(with sicker populations) or specificity (with less sickpopulations) upward.
• If the study setting was anything other than an ED(for example, a neurosurgery clinic) then the resultswere assessed as “low applicability.”
• In the assessment of continuous data like CSF redblood cells (RBCs), if the authors predefined athreshold for abnormal (example, CSFRBC > 5 9 106 cells/L in the last tube is “abnormal”)then the study results were assessed as “low risk” ofbias.
• If the conduct of the index test differed from routinecare (example, xanthochromia assessed using onlyspectrophotometry), then the results were assessedas “low applicability.”
• No widely accepted criterion standard for SAH yetexists, so we accepted the criterion standard of sub-arachnoid blood on unenhanced CT of the head,CSF xanthochromia, or CSF RBCs > 5 9 106/L in thefinal sample of CSF when any of these findingsincluded an aneurysm or arteriovenous malformationevident on cerebral angiography, as previouslyestablished by a consensus panel of emergencyphysicians and a neurosurgeon.39,54 If less than100% of a study’s subjects underwent cerebralangiography, a surrogate outcome of medical recordreview and structured telephone follow-up of at least6-months were necessary.20 Any other criterion stan-dard was assessed as “high risk” for bias.
• Assessing whether the target condition is identifiedis challenging in SAH diagnostic research. The idealpatient-centric diagnostic test would identify SAHpatients with a lesion amenable to surgical orendovascular intervention rendering measurablebenefit in mortality and morbidity.55 Since perimes-encephalic bleeds cause about 10% of SAH cases yetrequire no intervention other than symptom control,diagnostic studies that report aneurysmal SAH sepa-rately from perimesencephalic SAH would provide ahigher level of evidence by which to associate testingwith patient benefit. Unfortunately, few SAH studiesreport aneurysmal versus nonaneurysmal SAH
separately, so the decision was made that any SAHidentified using an acceptable criterion standard asdefined above would be assessed as “high applicabil-ity.”
• In assessing the uniformity of the criterion standardreported, if all patients with nondiagnostic CT andLP had either subsequent advanced imaging (angiog-raphy) or post-ED follow-up, then the risk of differ-ential verification bias was assessed as being“low.”51
• If a substantial number of patients were reported lostto follow-up and no sensitivity analysis assumingworst-case scenario (lost to follow-up = false-nega-tive SAH index test), then the risk of bias wasassessed to be “high.”
Inter-rater QUADAS-2 reliability was assessed usingprevalence-adjusted, bias-adjusted kappa values toadjust for unique biases between reviewers and the dis-tribution of responses across categories.56 Discrepan-cies were then resolved by consensus.
Data CollectionWe abstracted the study setting, study inclusion criteria,the criterion standard employed to diagnose SAH, CTtechnology, CSF analysis, follow-up procedures inpatients who did not undergo both CT and LP, diseaseprevalence, and every variable on history, physical, ortesting for which a 2 9 2 diagnostic accuracy tablecould be constructed. When reconstructed 2 9 2 contin-gency tables differed from the original investigators’reports of sensitivity and specificity, we contacted theauthors for clarity.
Data AnalysisMeta-analysis estimates were computed by one author(CRC) when ≥1 studies assessed the same finding onhistory or physical examination or index testing. Wechose to combine unenhanced cranial CT studies with-out distinguishing specific generations of technologysince the detector number or geometry and the thick-ness of slices were frequently not specified. We gener-ated combined estimates for diagnostic accuracy usinga random-effects model (Meta-DiSc Version 1.4,Hospital Universitario Ram�on y Cajal).57,58 Interstudyheterogeneity was assessed using the Der-Simonian-Laird random effects model and the index of inconsis-tency (I2).59,60 Pooled estimates of dichotomous LR+and LR� are also reported from the random-effectsmodel. Publication bias was not assessed because thisis not an accepted approach in diagnostic meta-ana-lyses due to the small number of studies generallyidentified.61
The added value of LRs over positive and negativepredictive values is that likelihood ratios are indepen-dent of disease prevalence.62 In addition, LRs can beused on an individual patient to estimate posttest proba-bilities, unlike sensitivity and specificity.63 Larger LR+increase the posttest probability of a disease more thansmaller values of LR+; similarly, smaller LR� decreasethe posttest probability of a disease more than largervalues of LR�. Note that a LR of 1 does not change theposttest probability at all. One rule of thumb is that
966 Carpenter et al. • SUBARACHNOID HEMORRHAGE EVIDENCE-BASED DIAGNOSTICS

LR+ > 10 and LR� < 0.1 provide considerable diagnosticvalue.64
Test–Treatment ThresholdWe used the Pauker-Kassirer method to estimatethresholds for further testing or treatment.47 Thistechnique is based on the diagnostic accuracy of atest, as well as the estimated risks of testing and oftreatment, and the anticipated benefit of treatment.We performed a separate analysis for each of the twoprimary tests in question, namely, cranial CT (strati-fied by time post–headache onset) and LP (usingeither CSF RBC or visible xanthochromia to define“positive LP”). We used the pooled estimates from themeta-analysis for test sensitivity and specificity andour collective clinical experience and selected refer-ences to estimate risks and benefits. We extended thetest indication curve method first proposed by Bern-stein48 to visually represent this analysis. Specifically,the curves display how the information conveyed by apositive or negative test result affects a given patient’sposttest probability of disease relative to the treatmentthreshold. These test indication curves were originallydeveloped to illustrate the pretest probability at whichtesting is no longer indicated based only on the netutilities of treating or not treating patients with andwithout disease.46 We extended this graphicalapproach to incorporate the nonzero risks of testing,which necessarily narrow the range of probabilitiesfor which testing remains rational.47,65 Because theprecise utilities of both testing and treatment are diffi-cult to estimate on a common scale, we performedsensitivity analyses by doubling and halving the calcu-lated treatment threshold (i.e., the ratio of risks oftreatment to the sum of risks and benefits)48 and alsoby reducing the risk of testing by half and
recalculating the test thresholds. Recognizing thatthese estimates are nevertheless somewhat arbitrary,we also provide an interactive calculator to permitreaders to recompute thresholds using different esti-mates of test performance or anticipated risks andbenefits that may be more applicable to the end-users’patient populations and clinical environments (DataSupplement S3, available as supporting information inthe online version of this paper).
In developing the test–treatment threshold, we weremost interested in the common clinical dilemma ofwhether to perform LP after a negative cranial CT orto forgo LP and proceed directly to angiography.Because CT-positive or LP-positive patients do notimmediately undergo neurosurgical clipping orendovascular coiling, the next step being contemplatedis usually angiography, typically by CT or MRA (andsometimes by digital subtraction fluoroscopy), followedby intervention when a culprit aneurysm is identified.Therefore, for Pauker-Kassirer modeling we desig-nated the “test” of interest as being either the unen-hanced CT or the LP and the “treatment” as beingangiography. Furthermore, because an LP is usuallydone after a negative CT, we considered how a nega-tive unenhanced cranial CT would affect the post-CT(i.e., pre-LP) probability of still having a SAH acrossthe range of pre-CT probabilities.
RESULTS
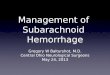
A total of 5,022 citations were identified through asearch of PubMed, Embase, and Scopus. From thissearch, 399 duplicate citations were removed. A total of122 studies underwent full-text review; of these, 22 stud-ies were included in the current analysis (Figure 1 andTable 2). Although most studies enrolled only awake
PUBMED search iden�fied 367 ar�cles
22 primary studies included in this systema�c review
EMBASE search iden�fied 3454 ar�cles
5022 manuscripts and abstracts iden�fied
100 ar�cles excluded • SAH only (28)• No original data (27)• Inability to reconstruct 2x2 tables
(21)• Editorial (18)• Not SAH (4)• Duplicate pa�ents (2)
SCOPUS search iden�fied 1200 ar�cles
122 full manuscripts reviewed
4487 excluded a�er reviewing �tles/abstracts
Hand search of scien�fic assemblies iden�fied 1
abstract
399 duplicates removed and 14 manuscripts unavailable
Figure 1. Study selection process. SAH = subarachnoid hemorrhage.
ACADEMIC EMERGENCY MEDICINE • September 2016, Vol. 23, No. 9 • www.aemj.org 967

Table
2Summary
ofIncludedStudies
Study
Loca
tion
Setting
No.
Patients
Mean
Age
(y)*
InclusionCriteria
StudyDesign
SAH
Criterion
Standard
SAH
Prevalence
%VariablesAss
ess
ed
Follow-up
Back
es2012
University
Medical
Center,
Utrech
t,the
Netherlands,
2005–2
012
ED
250
48*
Age>16y,
clinical
susp
icionof
acu
teonse
tSAH,GCS15
Two
prosp
ective
database
s.First
database
conse
cutive
patients
with
confirm
ed
SAH.Seco
nd
allLPpatients
withSPT.
Notexplicitly
defined.
42.0
Sen/SpecCTat<6
and>6hforSAH.
None
Bo2008
Ake
rshus
University
Hosp
ital,
Norw
ay,
1998–2
002
ED
433
44
Age>14y,acu
te-
onse
tworst
headach
eoflife
Prosp
ective
obse
rvational
conse
cutive
sampling
cohort.
Conse
nsu
sbetw
een
twoneurologists,
butnotexplicitly
defined.
16.4
Sen/Specof
elements
of
history
including
activityatonse
tandpeakintensity
forSAH.
None
Boesiger
2005
PittCounty
Memorial
Hosp
ital,
Greenville
SC,2002
ED
177
NR
Adultswith
headach
eworkup
includingCT
andLP
Retrosp
ective
chart
review.
SAH
obse
rvedonCT
or≥4
00RBCsin
CSFtube1thatdid
notclearby10-fold.
3.4
Sen/SpecofCTfor
SAH.
Phonef/uat1y
if≥4
00RBCsin
CSFtube1that
did
notclearby
10-fold.
Brunell2013
Uppsa
laUniversity
Hosp
ital,
Uppsa
laSweden,
2009–2
011
Hosp
ital
453
NR
Age>10ywith
LPto
exclude
SAH
Lab
inform
ation
system
review.
CSFhemoglobin
detectionvia
SPT
using415-nm
wavelength
orCSF
bilirubin
detection
via
automatic
analyzer.
1.1
Sen/specofCSF
RBC
forSAH.
None
Carstairs
2006
NavalMedical
Center,San
Diego,CA,
Jul2002–J
ul
2004
ED
116
39
Age>18ywith
eitherworst
headach
eoflife
oronse
t<60s
orassociated
neuro
deficit
Prosp
ective
obse
rvational
conse
cutive
sampling
cohort.
SAH
obse
rvedonCT
orRBCsin
CSF
tube1thatdid
not
clearby>25%
intube4orprese
nce
ofxanthoonvisual
insp
ectionbylab.
4.3
Sen/SpecofCTA
andelements
of
history
including
stiffneck
,blurred
vision,andaltered
mentalstatus.
None
Czu
czman
2013
Unsp
ecified
urban
tertiary
care
hosp
ital,
2001–2
009
ED
220
44
Adultswith
headach
es
billedforLPs,
≥5RBCsin
final
CSFtube,and
eitherCT
angiogram
or
magnetic
reso
nance
angiogram
within
2wk
Retrosp
ective
case
series.
Either1)prese
nce
of
SAH
onim
aging;2)
xanthowith
aneurysm
orAVM
>2mm;3)xantho
andcu
lture-or
PCR-negative
meningitis.
11.8
Sen/Specof
elements
of
history
including
suddenonse
theadach
e,worst
headach
e,and
onse
twith
exertion;CSFRBC
iLRs.
None
(Continued)
968 Carpenter et al. • SUBARACHNOID HEMORRHAGE EVIDENCE-BASED DIAGNOSTICS

Table
2(continued)
Study
Loca
tion
Setting
No.
Patients
Mean
Age
(y)*
InclusionCriteria
StudyDesign
SAH
Criterion
Standard
SAH
Prevalence
%VariablesAss
ess
ed
Follow-up
Dupont2008
St.Mary’s
Hosp
ital,
Roch
ester,
MN,1998–
2007
ED
117
45
Age>18ywith
headach
eonse
t<2wkpriorwith
both
nonco
ntrast
CT
fordetectionof
bloodandLP
Retrosp
ective
chart
review.
Notsp
ecified.
12.0
Sen/Specvisual
xanthofor
aneurysm
.
None
Gangloff
2015
Hopitalde
l’Enfant-
J� esu
s,Quebec,
Canada,2003
–2009
ED
706
41
Age>14ywith
acu
teheadach
esu
spiciousfor
SAH,GCS
15,
andinitialhead
CTnegativefor
SAH
with
subse
quentLP
Retrosp
ective
case
series.
Prese
nce
ofany
aneurysm
and
prese
nce
ofeither
visualxanthoor
>59
106RBCs/Lin
last
CSFtube.
0.7
Sen/Specvisual
xantho,iterative
SPT,orU.K.
NEQUA
SPT.
None
Hann2015
Royal
Brisb
ane&
Women’s
Hosp
ital,Jun
2005–J
ul
2012
ED
409
38
Adults
disch
argedwith
headach
eafter
CSFevaluation
forxantho
Retrosp
ective
case
series.
Prese
nce
ofvasc
ular
aneurysm
on
angiogram
within
30dofheadach
eor
norepeatED
visit
orSAH
death
in30
d.
1.5
Sen/Specvisual
xanthovia
visual
insp
ection.
Review
of
Queensland
death
registry
Landtblom
2002
University
Hosp
ital,
Link€ oping,
Sweden,
over
unsp
ecified
31-m
onth
period
ED
137
42*
Age>18y
prese
nting
within
10dof
headach
eonse
twithabrupt
onse
t(<10s)
headach
e,
examinedby
on-call
neurologist
Prosp
ective
obse
rvational
cohort.
Notsp
ecified.
11.3
Sen/Specof
elements
of
history
including
suddenonse
theadach
e,worst
headach
e,and
nause
a.
Phoneat2-
4days,
7-
9days,
and1-,
3-,6-,and12-
monthsfor90
subjectswithout
SAH
Linn1998
Utrech
tUniversity
Hosp
ital,
Utrech
t,the
Netherlands,
Jan1992–O
ct1994
ED
102
48
Alert
adult
patients
without
foca
lneuro
deficitreferred
toED
by
general
practitionerwith
conce
rnfor
SAH
withCT
andLP
Prosp
ective
obse
rvational
cohort.
Notsp
ecified.
41.2
Sen/Specof
elements
of
history
including
activityatonse
tandacu
ityof
onse
t.
None
(Continued)
ACADEMIC EMERGENCY MEDICINE • September 2016, Vol. 23, No. 9 • www.aemj.org 969

Table
2(continued)
Study
Loca
tion
Setting
No.
Patients
Mean
Age
(y)*
InclusionCriteria
StudyDesign
SAH
Criterion
Standard
SAH
Prevalence
%VariablesAss
ess
ed
Follow-up
Morgenstern
1998
Herm
ann
Hosp
ital,
Houston,TX,
Mar1995–
Jun1996
ED
97
39
Adultpatients
with10/10
worstheadach
eoflife
Prosp
ective
obse
rvational
cohort.
Either1)prese
nce
of
SAH
onim
agingor
2)CSFRBCs>
1,000with<25%
decrementfrom
firstto
last
tube
witheithervisual
xantho,SPT
xantho,orelevated
D-dim
er.
18.6
Sen/Specof
elements
of
history
and
physica
lexamination
includingnause
a,
stiffneck
,and
lethargy.
Phonef/uat
mean
24months
O’N
eill2005
Unsp
ecified
hosp
italover
unsp
ecified
1-yearperiod
ED
116
NR
Acu
teheadach
e<24h,clinical
susp
icionSAH,
referredforCT
from
ED
Retrosp
ective
chart
review.
Notsp
ecified.
16.4
Sen/SpecofCTfor
SAH.
None
Perry2006
Six
Canadian
tertiary
care
EDs,
Jul
2002–J
an
2004
ED
220
42
Age>15ywith
acu
te,
spontaneous
headach
ewith
orwithout
synco
pe
Preplanned
substudyof
prosp
ective,
conse
cutive
patientco
hort
study.
Anyoneofthe
following:
subarach
noid
blood
onCT,>59
106/L
RBCsin
3rd
or4th
tubeofCSF,or
visible
xantho+
aneurysm
on
cerebral
angiography.
0.9
Sen/Specofvisual
insp
ectionfor
xanthoandfour
SPTmethodsfor
xanthoforSAH.
Phonef/uat1-
month
forCT-,
LP-patients;
chart
review
at
1-m
onth
forall
patients
Perry2010
Six
Canadian
tertiary
care
EDs,
Nov
2000–N
ov
2005
ED
1,999
43
Age≥16ywith
spontaneous
headach
epeakingwithin
1horsy
nco
pe
associatedwith
aheadach
e
Prosp
ective
cohort
study.
Anyoneofthe
following:
subarach
noid
blood
onCT,visual
xantho,>59
106/L
RBCsin
thefinal
tubeofCSFwithan
aneurysm
orAVM
once
rebral
angiography.
6.5
Sen/Specof
elements
of
history
including
activityatonse
t,neck
stiffness
,and
arrivalmode.
Also,derivationof
threeCDRs.
Phonef/uat1-
and6-m
onths
forallpatients
withoutCTor
LP;ch
art
review
&Ontario
registryreview
atstudyendfor
samepatients
Perry2011
11Canadian
tertiary
care
EDs,
Nov
2000–D
ec
2009
ED
3,132
45
Age>15ywith
acu
te,
spontaneous
headach
ewith
orwithout
synco
pe
Prosp
ective
cohort
study.
Anyoneofthe
following:
subarach
noid
blood
onCT,visual
xantho,>59
106/L
RBCsin
thefinal
tubeofCSFwithan
aneurysm
orAVM
once
rebral
angiography.
7.7
Sen/SpecCTat<6
and>6hforSAH.
Phonef/uat1-
and6-m
onths
forallpatients
withoutCTor
LP;ch
art
review
&provincial
coroner’s
reco
rdsatstudy
endforsa
me
patients
(Continued)
970 Carpenter et al. • SUBARACHNOID HEMORRHAGE EVIDENCE-BASED DIAGNOSTICS

Table
2(continued)
Study
Loca
tion
Setting
No.
Patients
Mean
Age
(y)*
InclusionCriteria
StudyDesign
SAH
Criterion
Standard
SAH
Prevalence
%VariablesAss
ess
ed
Follow-up
Perry2013
10Canadian
tertiary
care
EDs,
Nov
2000–D
ec
2009
ED
2,131
44
Age≥16ywith
spontaneous
headach
epeakingwithin
1horsy
nco
pe
ass
ociatedwith
aheadach
e
Prosp
ective
cohort
study.
Anyoneofthe
following:
subarach
noid
blood
onCT,visual
xantho,>59
106/L
RBCsin
thefinal
tubeofCSFwithan
aneurysm
orAVM
once
rebral
angiography.
6.2
Sen/Specof
elements
of
history
and
physica
lexamination
includingactivity
atonse
t,neck
stiffness
,and
arrivalmode.
Also,derivationof
fourSAH
CDRs.
Phonef/uat1-
and6-m
onths
forallpatients
withoutCTor
LP;ch
art
review
&provincial
coroner’s
reco
rdsatstudy
endforsa
me
patients
Perry2015
12Canadian
tertiary
care
EDs,
Apr
2006–J
ul
2010
ED
1,7391,098
norm
al
LP641
abnorm
al
LP
44
Age>15ywith
acu
te,
spontaneous
headach
ewith
orwithout
synco
pewithLP
toevaluate
potentialSAH
Preplanned
substudyof
prosp
ective,
conse
cutive
patientco
hort
study.
Aneurysm
alSAH
ifsu
barach
noid
blood
onCT,visual
xantho,orany
RBCsin
thefinal
tubeofCSFwithan
aneurysm
on
cerebral
angiography.
2.3
Sen/Specof
<20009
106/L
RBCsin
CSF+no
xanthofor
diagnosis
aneurysm
alSAH.
Phonef/uat1-
and6-m
onths
forallpatients
withoutCTor
LP;ch
art
review
&provincial
coroner’s
reco
rdsatstudy
endforsa
me
patients
VanderW
ee
1995
University
hosp
itals
inUtrech
tand
Rotterdam
the
Netherlands,
1989–1
993
NR
175
NR
Acu
teheadach
ewithout
confusionor
foca
ldeficit
withCTwithin
12h
Unclear
whether
retrosp
ective
orprosp
ective
“co
nse
cutive”
case
series.
Notsp
ecified.
68
Sen/SpecCTat<12
hforSAH.
None
Wood2015
Prince
ssAlexandra
Hosp
ital,
Brisb
ane,
Queensland,
Australia,
Jan2000–
Apr2003
NR
240
NR
Acu
teor
unusu
ally
severe
headach
ewith
LPaftera
norm
alcranial
CTforposs
ible
diagnosisof
SAH
Retrosp
ective
chart
review.
Uniform
CSFblood
stainingacross
serialsa
mpleswith
visualxanthoand
“positive”
angiography.
0.8
Sen/SpecofCSF
SPT(X
I>0.080).
None
AVM
=arteriovenousmalform
ations;
CDR
=clinicaldecisionrule;CSF=ce
rebrosp
inalfluid;CT=co
mputedtomography;f/u=follow-up;GCS
=Glasg
ow
ComaSca
le;iLRs=in-
tervallike
lihood
ratios;
LP=lumbarpuncture;NR
=notreported;SAH
=su
barach
noid
hemorrhage;Sen/Spec=se
nsitivity/specificity;SPT=sp
ectrophotometry;xantho=xan-
thoch
romia;XI=xanthoch
romic
index.
*Median.
ACADEMIC EMERGENCY MEDICINE • September 2016, Vol. 23, No. 9 • www.aemj.org 971

Table
3Overview
ofQuality
Ass
ess
mentofIncludedStudies
Study
Sample
AvoidedInap-
propriate
Exclusions?
Patients
andSet-
tingsMatch
Study
Question?
BlindedInter-
pretationof
IndexTest?
Acc
eptable
IndexTest
Applica
tion?
Acc
eptable
Reference
(Criterion)
Standard?
Outcomes
Ass
ess
ed
byBlinded
Ass
ess
or?
Ass
ess
ed
Outcomes
Pertinent?
Appropriate
IntervalBetw
een
IndexTest
and
Reference
Stan-
dard?
SameRefer-
ence
(Crite-
rion)Stan-
dard
forAll
Patients?
AllPatients
Analyzed?
Back
es2012
Conse
cutive
YES
YES
NO
YES
NO
NO
NO
YES
YES
YES
Bo2008
Conse
cutive
YES
YES
NO
NO
NO
NO
NO
YES
YES
YES
Boesiger
2005
Conse
cutive
YES
YES
NO
YES
YES
YES
NO
YES
YES
YES
Brunell2013
Conse
cutive
YES
YES
YES
NO
NO
YES
NO
YES
YES
YES
Carstairs
2006
Conse
cutive
YES
YES
YES
YES
YES
YES
YES
YES
YES
YES
Czu
czman
2013
Conse
cutive
YES
NO
YES
YES
YES
NO
YES
YES
YES
YES
Dupont2008
Conse
cutive
NO
YES
NO
YES
YES
NO
YES
YES
NO
YES
Gangloff
2015
Conse
cutive
YES
YES
NO
NO
YES
NO
YES
YES
NO
NO
Hann2014
Conse
cutive
NO
NO
NO
NO
YES
NO
YES
YES
YES
YES
Landtblom
2002
Conse
cutive
YES
YES
NO
NO
YES
NO
YES
YES
YES
YES
Linn1998
Conse
cutive
YES
YES
NO
YES
NO
NO
YES
YES
NO
YES
Morgenstern
1998
Conse
cutive
YES
YES
YES
NO
NO
YES
NO
YES
YES
NO
O’N
eill2005
Conse
cutive
YES
YES
YES
YES
NO
YES
YES
YES
YES
NO
Perry2006
Conse
cutive
NO
YES
YES
YES
YES
NO
YES
YES
YES
YES
Perry2010
Conse
cutive
YES
YES
YES
YES
YES
NO
YES
YES
YES
NO
Perry2011
Conse
cutive
YES
YES
YES
YES
YES
YES
YES
YES
YES
NO
Perry2013
Conse
cutive
YES
YES
YES
YES
YES
YES
YES
YES
YES
YES
Perry2015
Conse
cutive
YES
YES
YES
YES
YES
NO
YES
YES
YES
YES
vanderW
ee
1995
Conse
cutive
NO
NO
NO
NO
NO
NO
NO
YES
YES
YES
Wood2005
Conse
cutive
NO
NO
NO
NO
NO
NO
YES
NO
YES
YES
Kappa*
1.00
0.33
0.52
0.05
0.14
0.05
0.05
0.43
0.52
0.62
0.33
*Prevalence
-adjusted,bias-adjustedka
ppaasdefinedbyByrt
etal.56
972 Carpenter et al. • SUBARACHNOID HEMORRHAGE EVIDENCE-BASED DIAGNOSTICS

Table 4Single-study Predictors of SAH from History and Physical Examination Available
Risk Factor Sensitivity, % (95% CI) Specificity, % (95% CI) LR+ (95% CI) LR� (95% CI)
DiplopiaLandtblom 2002 0 (0–15) 98 (94–100) 0.96 (0.05–19.33) 1.00 (0.94–1.07)
Family history cerebral aneurysmCzuczman 2013 0 (0–13) 92 (87–95) 0.22 (0.01–3.54) 1.07 (1.00–1.15)
LethargyMorgenstern 1998 39 (17–64) 82 (72–90) 2.19 (1.04–4.64) 0.74 (0.51–1.09)
Onset < 1 minLinn 1998 50 (34–66) 45 (32–58) 0.91 (0.62–1.33) 1.11 (0.74–1.68)
Onset 1–5 minLinn 1998 24 (12–39) 87 (75–94) 1.79 (0.77–4.14) 0.88 (0.72–1.07)
Onset < 1 hBo 2008 100 (95–100) 12 (9–16) 1.13 (1.09–1.19) 0.06 (0–0.95)
PMH of chronic headacheCzuczman 2013 19 (7–39) 79 (73–85) 0.93 (0.40–2.91) 1.02 (0.83–1.24)
PMH of hypertensionCzuczman 2013 31 (14–52) 80 (74–85) 1.53 (0.81–2.91) 0.87 (0.66–1.13)
ScotomataLandtblom 2002 0 (0–15) 93 (87–97) 0.28 (0.02–4.72) 1.06 (0.98–1.14)
Similar headache in pastLinn 1998 19 (9–34) 90 (79–96) 1.90 (0.71–5.09) 0.90 (0.76–1.07)
LR+ = positive likelihood ratio; LR� = negative likelihood ratio; PMH = past medical history; SAH = subarachnoid hemorrhage.
Ambulance Arrival
Figure 2. Forest plots for diagnostic elements of history for SAH. LR = likelihood ratio; SAH = subarachnoid hemorrhage.
ACADEMIC EMERGENCY MEDICINE • September 2016, Vol. 23, No. 9 • www.aemj.org 973

and alert patients with a Glasgow Coma Scale scoreof 15, some also included those with decreased levelof consciousness, which could introduce spectrumeffect into observed estimates of diagnostic accuracy.All studies were conducted in North American orEuropean countries. Each study included the presenceof subarachnoid blood on unenhanced cranial CT asrepresenting “disease positive.” Descriptors of thespecific technology utilized for CT scanners and spec-trophotometric assessment for CSF xanthochromiawere inconsistent. Definitions of xanthochromia ran-ged from direct visual inspection to spectrophotomet-ric analysis. When using spectrophotometry, studiesvaried with regards to wavelengths sampled andspecific algorithms used to adjust for interference byoxyhemoglobin, protein, and other corrections. Clinicalfollow-up proportion varied considerably, ranging
from no follow-up to complete follow-up with cross-checking of coroner records to ensure no misseddeaths. Assessment of studies by QUADAS-2 (Table 3)showed significant heterogeneity in reference stan-dards used, blinding of index test interpreters to thereference standard, and vice versa. Agreementbetween reviewers was fair for all QUADAS-2 ele-ments except for index and reference standard blind-ing, reference standard appropriateness, andacceptable application of index test in which cases theagreement was poor.66 However, most studies had arelatively low risk of biases overall.
PrevalenceThe overall prevalence of SAH in these studies rangedfrom 0.91% to 68%. In prospective studies within thepast 10 years, the prevalence ranged from 0.91% to
Awoke from Sleep
Figure 2. Continued.
974 Carpenter et al. • SUBARACHNOID HEMORRHAGE EVIDENCE-BASED DIAGNOSTICS

17% with a weighted average of 7.5%. Two of the stud-ies with the lowest prevalence enrolled patients under-going LP following a negative CT.67,68
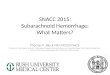
History and Physical ExaminationEight studies described the diagnostic accuracy for 22components of history2,17,33,38,39,69–71 (Table 4 andFigure 2) and six studies described the diagnostic accu-racy for four physical examination tests2,17,69,70 (Table 4and Figure 3) for SAH. Within these studies there wassignificant heterogeneity in the manner in which historyand physical characteristics were obtained and defined.For example, Perry et al.39 defined limited neck flexionon physical examination as “inability to touch chin tochest or raise the head 8 cm off the bed if supine,”whereas Carstairs et al.17 provided no descriptor of how“nuchal rigidity” was objectively assessed on physicalexamination. Perry et al.39 reported the interphysician
reliability of elements of the history and physical exami-nation, with kappa (j) values ranging from 0.44 to 1.00.The least reliable findings were thunderclap headache(j = 0.49) and limited neck flexion (j = 0.44).
No single element of history had a very high pooledLR+. The findings on history that increased the proba-bility of SAH the most included subjective neck stiffness(LR+ = 4.12, 95% CI = 2.24 to 7.59), while the absence of“worst headache of life” (LR� = 0.36, 95% CI = 0.01 to14.22) or onset of headache over more than 1 hour(LR� = 0.06, 95% CI = 0 to 0.95) each reduced the prob-ability of SAH.
On physical examination, neck stiffness (LR+ = 6.59,95% CI = 3.95–11.00) was strongly associated with SAHas reported in three studies, but no single physicalexamination finding had a LR� less than 0.74. Most ele-ments of history and physical examination demon-strated significant statistical heterogeneity.
Blurred Vision
Figure 2. Continued.
ACADEMIC EMERGENCY MEDICINE • September 2016, Vol. 23, No. 9 • www.aemj.org 975

Clinical Decision RulesFour related SAH clinical decision rules have beendescribed, three of which were prospectively validatedin a subsequent study by the same investigator group togenerate the final refined Ottawa SAH Rule. Since morethan one study is needed to perform a meta-analysis,we were unable to pool diagnostic accuracy results forSAH Clinical Decision Rules. The component elements
of each decision rule, along with their combined accu-racy and reliability are available in Data Supplement S2(available as supporting information in the online ver-sion of this paper). Rule 1 appears sufficient to rule outSAH (LR� = 0.06, 95% CI = 0.01–0.22), was uncomfort-able to use for only 18% of surveyed emergency physi-cians, was misinterpreted in 4.7% of cases, and wouldtheoretically decrease CT and/or LP testing rates from
Burst or Explode at Onset
Figure 2. Continued.
976 Carpenter et al. • SUBARACHNOID HEMORRHAGE EVIDENCE-BASED DIAGNOSTICS

84% to 74%. On the other hand, the Ottawa SAH Rulemore accurately rules out SAH (LR� = 0.02, 95%CI = 0.00–0.39), but could increase CT and/or LP testingrates if strictly applied.39
Advanced ImagingFive studies examined the diagnostic accuracy of non-contrast CT (Figure 4).20,72–75 The pooled estimate forsensitivity was 94% (95% CI - 91% to 96%, I2 = 74%)and LR� was 0.07 (95% CI = 0.03 to 0.17, I2 = 78%). vander Wee et al.72 assessed CT accuracy at 12 hours, butdid not provide sufficient data to reconstruct 2 9 2tables stratified by that time threshold. Three otherstudies reported diagnostic accuracy stratified by thetime interval since symptom onset, but only tworeported the threshold of less than 6 hours.20,70,75
Pooled sensitivity within the first 6 hours of symptomonset was 100% (95% CI = 98% to 100%, I2 = 0%) andLR� was 0.01 (95% CI = 0 to 0.04, I2 = 0%). Beyond
6 hours the pooled sensitivity of CT was 89% (95%CI = 83% to 93%, I2 = 89%) and LR� was 0.07 (95%CI = 0.01 to 0.61, I2 = 63%).
CSF Erythrocytes and XanthochromiaSix studies examined diagnostic accuracy of xan-throchromia on CSF analysis, but investigators usedvariable methods to assess xanthochromia ranging fromvisible inspection33,67,68,76 to multiple different spec-trophotometric assays (Table 5, Figure 5).34,67,68,77 Forvisible xanthochromia the pooled meta-analysis resultswere as follows: sensitivity was 85% (95% CI = 66% to96%, I2 = 0%), specificity as 97% (95% CI = 96% to98%, I2 = 13%), LR+ was 24.67 (95% CI = 12.13 to 50.14,I2 = 64%), and LR� was 0.22 (95% CI = 0.09 to 0.54,I2 = 13%). Both Perry and Gangloff evaluated spec-trophotometric bilirubin using the U.K. National Exter-nal Quality Assessment Service (U.K. NEQAS)algorithm78 with pooled sensitivity of 100% (95%
ED Transfer
Figure 2. Continued.
ACADEMIC EMERGENCY MEDICINE • September 2016, Vol. 23, No. 9 • www.aemj.org 977

CI = 59% to 100%, I2 = 0%), specificity of 95% (95%CI = 93% to 96%, I2 = 98%), LR+ of 15.23 (95% CI = 1.58to 146.73, I2 = 96%), and LR� of 0.13 (95% CI = 0.02 to0.83, I2 = 0%).67,68 The diagnostic accuracies of otherspectrophotometric methods to evaluate for CSF biliru-bin are also summarized in Table 5.
Two studies evaluated CSF erythrocyte counts to dis-tinguish a traumatic LP from an aneurysmal SAH. Perryet al.79 noted a sensitivity of 93% (95% CI = 68% to100%), specificity of 91% (95% CI = 88% to 93%), LR+
of 10.25 (95% CI = 7.7 to 13.6), and LR� of 0.07 (95%CI = 0.01 to 0.49) at a threshold CSF RBC < 2,000 9 106/L in the final tube of CSF collected. Czuczman et al.33
reported interval likelihood ratios (iLR)80 for CSF RBCcounts in the final tube collected (using units of cells/lL): iLR<100 = 0, iLR100–10,000 = 1.6, iLR>10,000 = 6.3. Usingraw data from these two studies to evaluate the sum-mary diagnostic accuracy for CSF RBC in the final tubeat an arbitrarily selected new threshold of 1,000 9 106/L, the pooled sensitivity was 76% (95% CI = 60% to
Exertion at Onset
Figure 2. Continued.
978 Carpenter et al. • SUBARACHNOID HEMORRHAGE EVIDENCE-BASED DIAGNOSTICS

88%, I2 = 79%), specificity was 88% (95% CI = 86% to90%, I2 = 95%), LR+ was 5.7 (95% CI = 1.4 to 23,I2 = 97%), and LR� was 0.21 (95% CI = 0.03 to 1.66I2 = 78%). The diagnostic accuracy of CT and LP, andspecifically how the test results affect the posttest prob-ability of disease in a Bayesian fashion, are representedin Figure 6.
Test–Treatment ThresholdThe risks of treatment (designated Rrx by Pauker andKassirer47) were primarily those ascribed to angiogra-phy itself and not those of eventual neurosurgical inter-vention. These risks included additional exposure toionizing radiation and to contrast, the risks of vascularaccess and allergic reactions, and the remote risk of
Female
Figure 2. Continued.
ACADEMIC EMERGENCY MEDICINE • September 2016, Vol. 23, No. 9 • www.aemj.org 979

stroke or other end-organ damage. The lifetime risk ofmalignancy secondary to exposure to ionizing radiationis a function of dose and age; an adult is typicallyexposed to 20 mGy radiation during cranial CT. Usingan average lifetime cancer risk attributable to such anexposure of almost 1%,81 we deemed the total risksrelated to angiography to be relatively low at 0.02.
When considering the benefits of treatment (Brx), weconsidered primarily the benefits of treating ananeurysmal SAH. Overall, SAH has 12% mortality priorto arrival in the ED and 40% in-hospital mortality at1 month despite treatment. In addition, one-third of sur-vivors suffer a severe neurologic deficit.82,83
Neurosurgical and interventional radiology treatmentoptions include clipping and coiling the culprit aneur-ysm when present, with several large randomized trialsreporting long-term poor outcomes in up to 35% oftreated subjects.84–86 The long-term benefits of earlydiagnosis and treatment in the subset of patients whopresent awake and neurologically intact are not wellcharacterized but presumably somewhat better, so weassigned an optimistic overall treatment benefit (Brx) of0.8 with immediate diagnosis.
For LP we considered the common morbidity of apostdural puncture headache, discomfort, and remoterisks of infection and assigned a test risk (Rt) of 0.01.
IIntercourse at Onset
Figure 2. Continued.
980 Carpenter et al. • SUBARACHNOID HEMORRHAGE EVIDENCE-BASED DIAGNOSTICS

The testing thresholds from these estimates of potentialrisk and potential benefit are depicted in Figure 7. Thethresholds bracketing indifference between LP versuseither no further testing (Ttest) or angiography (Ttreat)were very narrow, suggesting that LP should only beconsidered for patients with a pre-LP probabilitybetween 2 and 7% (when using visible xanthochromia)or between 2 and 4% (when using CSF erythrocytecount). Lower-risk patients need no further testing andavoid LP, while higher-risk patients benefit fromangiography and again avoid LP.
Of note, these rather narrow pre-LP probabilitybands correspond to the post-CT disease probability,not the original estimate based on history and physicalexamination (i.e., not the pre-CT estimate). In otherwords, one should take the pre-CT probability estimateand incorporate the information gained from a nega-tive CT in a Bayesian fashion. The impact of a negativeCT on the post-CT (i.e., pre-LP) probability is alsoshown in Figure 7, depending on the interval betweenheadache onset and imaging. Thus, a pre-LP probabil-ity of 2% to 7% represents a pre-CT prior probability
Loss of Consciousness
Figure 2. Continued.
ACADEMIC EMERGENCY MEDICINE • September 2016, Vol. 23, No. 9 • www.aemj.org 981

of over 70% (based on history and physical) for a CTobtained within 6 hours and over 20% for a CTobtained beyond 6 hours. The sensitivity analysesshowed that these estimates were stable across arange of utilities and were primarily influenced by thediagnostic accuracy of the tests being considered, asillustrated in the figures. When the risks of testing (LP)were allowed to approach the risks of treatment (an-giography), then LP was no longer indicated at anypretest probability. Table 6 provides an example illus-trating how to use test indication curves for diagnosticdecision-making.
DISCUSSION
The results of this systematic review demonstrate thatneither the presence nor the absence of commonly citedSAH risk factors from history and physical examinationaccurately rule in or rule out this potentially lethal diag-nosis. Specifically, no single history or physical exami-nation finding significantly increases (LR+ > 10) ordecreases (LR� < 0.1) the posttest probability of SAHfor severe headaches that peak within 1 hour of onset.In addition, many elements of history and physicalexamination for SAH have only fair to good
Male
Figure 2. Continued.
982 Carpenter et al. • SUBARACHNOID HEMORRHAGE EVIDENCE-BASED DIAGNOSTICS

interphysician reliability, with the characterization ofthe headache as “thunderclap” being one of the leastreproducible findings.39 Nonetheless, many physicianswould prefer to never miss a SAH, and missed SAHremains an important cause of litigation in emergencymedicine.23,87
Lacking accurate features on clinical presentation andrecognizing the tension between malpractice risk and agrowing imperative to preserve limited healthcareresources, to adhere to Choosing Wisely
recommendations,23,87,88 and to avoid the unintendedharms of overdiagnosis,30 clinical researchers haveendeavored to develop more efficient prediction instru-ments. Yet the development of highly sensitive instru-ments requires both large data sets and rigorousadherence to methodologic standards. To illustrate, a ret-rospective validation of Rule 1 using medical recordreview in Northern California reported a LR� of 0.13(95% CI = 0.03 to 0.61) and reportedly missed 11 cases(20%) of SAH cases despite cranial CT within 6 hours.89
Nausea
Figure 2. Continued.
ACADEMIC EMERGENCY MEDICINE • September 2016, Vol. 23, No. 9 • www.aemj.org 983

Another retrospective study of aneurysmal SAH patientsdemonstrated 100% sensitivity (95% CI = 97.6% to100%) using the combination of negative cranial CT andall negative responses on the Ottawa SAH Rule.90 How-ever, validating a clinical decision rule retrospectively issuboptimal since all components of the rule may not berecorded in the medical records and whether to code
missing variables as unknown or not present is fre-quently a question.91 In the retrospective validation ofRule 1, the “onset during exertion” variable was missingin one-third of patients.92 Therefore, these instrumentsshould ideally undergo prospective validation in differentsettings before widespread adoption (J. J. Perry et al.,manuscript submitted for publication).91
Neck stiffness, subjective
Figure 2. Continued.
984 Carpenter et al. • SUBARACHNOID HEMORRHAGE EVIDENCE-BASED DIAGNOSTICS

Unenhanced CT remains the first-line imaging test inED headache patients with suspected spontaneousSAH. Within 6 hours of headache onset, CT demon-strates sufficient accuracy to rule in or to rule out SAH,notwithstanding the heterogeneity of the estimatedspecificity and LR+ of the two studies identified. Beyond6 hours the estimated LR� (95% CI = 0.01 to 0.61) andsensitivity (95% CI = 83% to 93%) become less preciseand concerns regarding heterogeneity (I2 = 89% andI2 = 63%, respectively) allow the interpretation that theaccuracy of cranial CT to rule out SAH could rangefrom very good (LR� = 0.01) to unhelpful (LR� = 0.61)taking the extremes of the 95% CI. Therefore, the timing
of CT relative to symptom onset has remained animportant qualifier when estimating the diagnosticaccuracy of the CT. Of course, CT can identify othercauses of headache or other abnormalities and similarlycan miss SAH due to cervical arteriovenous malforma-tions.75 Some researchers in the field stipulate that theCT should be interpreted by an experienced neuroradi-ologist, although recent research indicates that radiolo-gists at nonacademic centers may be equally adept.35
Despite advances in CT imaging, substantial debatepersists surrounding the necessity of LP following anegative head CT, particularly within the first 6 hoursafter onset of headache.93–97 While CSF can provide
Photophobia
Figure 2. Continued.
ACADEMIC EMERGENCY MEDICINE • September 2016, Vol. 23, No. 9 • www.aemj.org 985

crucial diagnostic information for alternative etiologiesof headache like meningitis, it remains an imperfect testfor SAH. Traumatic (blood-contaminated) LPs occur inone of six cases.40 Xanthochromia takes many hours todevelop and is variably defined. In addition, post-LPheadaches are common31,98 despite increasing use ofsmaller-gauge, atraumatic spinal needles and reinsert-ing the stylet before needle removal.32 Other potential
complications include low back pain, brainstem hernia-tion, iatrogenic infection, epidural nerve injury, andspinal hemorrhage.99,100 These factors combined withpatients’ negative bias against the procedure and thephysician time needed help explain emergency physi-cians’ reluctance to pursue LP despite a long-held beliefthat this procedure was mandatory in the setting of sus-pected SAH.101–104 Our analysis provides new insight
Vomiting
Figure 2. Continued.
986 Carpenter et al. • SUBARACHNOID HEMORRHAGE EVIDENCE-BASED DIAGNOSTICS

into the limited utility of performing LP to rule out SAHafter a negative CT. We found that, by incorporatingthe risks and benefits of both testing and continuedinvestigation into the decision analysis, the benefits ofLP are unlikely to outweigh the harm across a widerange of reasonable estimates of pretest disease preva-lence and given the limited diagnostic accuracy of theCSF analysis.
Brunell et al.34 noted that LP provided an alternativediagnosis in 3% of suspected SAH cases, but onlyaltered subsequent management in 0.44% of individualswho had an LP. This equates to 227 LPs (1/0.0044) toidentify one central nervous system infection requiringantibiotics in suspected SAH patients. In addition, usingspectrophotometry, Brunell et al. noted five additionalcases of SAH representing 1.1% of LPs and a number
needed to LP (NNLP) of 91 (1/0.011) to identify one addi-tional SAH. Of note, none of these additional cases of“SAH” were aneurysmal, and none underwent subse-quent surgery; thus the NNLP approaches infinity fordetecting SAH that might benefit from intervention.Perry et al. reported 17/1546 false-negative CTs (withpostheadache onset imaging delays ranging from8 hours to 8 days) that were identified by LP obtainedat the discretion of the attending emergency physi-cian.20 However, only six of these individuals underwentneurosurgical intervention (ventricular drain, aneurysmcoiling, or clipping), which equates to a NNLP = 258 (6/1546 = 0.38%, 1/0.0038 = 258) to identify one aneurysmamenable to neurosurgical intervention following a neg-ative cranial CT. Sayer et al.36 reported NNLP = 250 toidentify one additional aneurysmal SAH. Blok et al.35
Worst Headache of Life
Figure 2. Continued.
ACADEMIC EMERGENCY MEDICINE • September 2016, Vol. 23, No. 9 • www.aemj.org 987

identified one perimesencephalic bleed among 760 CT-negative patients with suspected aneurysmal SAH,which they extrapolated to NNLP = 15,200 to identifyone additional aneurysmal SAH given that one in 20perimesencephalic bleeds are ultimately linked to ananeurysm (760 9 20 = 15,200).105–107
Another approach to more definitively rule out SAHafter a nondiagnostic, noncontrast CT is to proceed toCTA without an LP, an approach that 75% of patientsfavored in one survey108,109 and supporting a role forshared decision-making in evaluation of suspected
SAH.110 Some physicians have even advocated for pre-discharge CTA after a nondiagnostic CT and LP. Car-stairs et al.17 examined CTA in addition to traditionalnoncontrast CT. Patients who were CT negative and LPnegative underwent CTA to more definitively identifyeither SAH or cerebral aneurysm. After evaluating 103CT-negative/LP-negative patients, they detected twocerebral aneurysms, which equates to a number neededto CTA (NNCTA) = 52 to detect one cerebral aneurysmthat might or might not be the cause of the presentingheadache (2/103 = 1.9%, 1/0.019 = 52). Contemplating
Altered Mental Status
Figure 3. Forest plots for diagnostic elements of physical examination for SAH. LR = likelihood ratio; SAH = subarachnoid hemor-rhage.
988 Carpenter et al. • SUBARACHNOID HEMORRHAGE EVIDENCE-BASED DIAGNOSTICS

the NNCTA is essential because CTA is neither com-pletely safe, nor always clinically meaningful. CTA com-plication rates range from 0.25% to 1.8%.111,112
Carstairs et al. interpreted the presence of cerebralaneurysm by CTA to be equivalent to being disease pos-itive for SAH, despite being unable to establish whetherthe aneurysm was the etiology of the patient’s headacheor an incidental finding.
Indeed, intracranial saccular or berry aneurysms arecommon, occurring in 1%–2% of the population.113
Linking a nonruptured aneurysm detected via CTA to
an individual patient’s headache is problematic. The dis-covery of an aneurysm in the context of headache isoften considered to be a symptomatic aneurysm, andneurosurgical intervention may be advised dependingon aneurysm size, location, and specific patient charac-teristics.114 However, the relative risk of rupture forcerebral aneurysms detected in symptomatic individualsis eightfold higher than the rupture rate in asymp-tomatic individuals with incidentally noted cerebralaneurysms.115 Based on one recent meta-analysis of 50studies, the pooled sensitivity and specificity for CTA to
Focal Neuro Deficit
Figure 3. continued.
ACADEMIC EMERGENCY MEDICINE • September 2016, Vol. 23, No. 9 • www.aemj.org 989

detect aneurysms are 98 and 100%, respectively.44 MRAcan also be utilized to detect intracranial aneurysm, withpooled sensitivity and specificity of 95 and 89%, respec-tively. Although MRA is more time-consuming and gen-erally less available from the ED, it may be useful incircumstances where radiation exposure is to beavoided or a patient has an iodine contrast dyeallergy.45
Given the risks of overinvestigation and incidentalfindings, it is important to scrutinize the testing thresh-olds for CT, LP, and angiography. We found that only
patients with a pre-CT likelihood of SAH well above20% were likely to benefit from an LP after a negativeunenhanced CT. Such pre-CT probabilities are excep-tionally high and are far higher than the average diag-nostic yield of around 5% for SAH on initial CT. Thelimited ability of any feature on history or physicalexamination to identify SAH also renders such highpre-CT probabilities unlikely, except for severe caseslikely to have extensive bleeding visible on CT. More-over, patients with only slightly higher pre-CT probabil-ities benefit more from angiography than LP, given the
Neck stiffness, objective
Figure 3. continued.
990 Carpenter et al. • SUBARACHNOID HEMORRHAGE EVIDENCE-BASED DIAGNOSTICS

limitations of CSF analysis. Accordingly, this analysissuggests that LP after a negative CT to “rule out” SAHno longer seems rational for the large majority ofpatients.
The utilitarian approach to decision-making testthresholds is considered by some too arbitrary or artifi-cial, yet it is critically important to recognize how toapply these analyses at the bedside. The separationbetween the test-positive and test-negative curves are avisual representation of the diagnostic performance ofthe test and thus illustrate the summary findings fromthis meta-analysis. The vertical location of the horizontalline that is used to calculate the test thresholds where itintersects each curve is determined by the ratio
between benefits and risks of further treatment and caneasily be shifted up or down to visually estimate newthresholds on the graph. We used a 40:1 ratio of thebenefits:risk of angiography, but allowed this to rangefrom 20:1 to 80:1 in a sensitivity analysis and obtainedsimilar findings. We extended this graphical approachto include the nonzero risks of testing, as illustrated bya narrowing of the range of pretest probabilities forwhich the test is beneficial. We selected a test:treatmentrisk of 1:4 for CT and 1:2 for LP compared to angiogra-phy, but reduced the risk by half in another sensitivityanalysis with again similar findings.
Yet the most compelling argument in support of thisanalysis is that the findings are strikingly similar to
CT Anytime
Figure 4. Forest plots for diagnostic accuracy of CT for SAH. CT = computed tomography; LR = likelihood ratio; SAH = subarach-noid hemorrhage.
ACADEMIC EMERGENCY MEDICINE • September 2016, Vol. 23, No. 9 • www.aemj.org 991

experienced clinicians’ own practice. Initial unenhancedCT is rational across a wide range of pretest probabili-ties, as low as 1%. This 1 in 100 miss rate is consistentwith surveys of emergency physicians and a thresholdused in clinical decision rule construction for SAH andother serious conditions.38,103 On the other hand, after anegative CT, the low LR� coupled with a low pre-CTprobability for SAH renders the post-CT probability solow that the only moderately accurate LP is rarely war-ranted. As such, the observed practice of forgoing LPafter a negative CT, long considered to be a pitfall inthe management of these patients, is easily justified onBayesian grounds, as represented graphically on thetest indication curves.
The test indication curves also help clinicians avoidthe common fallacy sometimes invoked to persuadeheadache patients that an LP is advisable. Manyexplain a “95% sensitivity” of CT by counseling thepatient that “there is still a 1 in 20 (i.e., 100% –95% = 5%) chance that you have a ruptured aneur-ysm.” This is only true if the patient were certain tohave a SAH prior to the test being ordered (pretest
probability = 100%). It is implausible that even themost skilled clinician can predict SAH prior to anytesting in more than one in five awake and alertpatients, the very patient in whom an informed con-sent discussion is needed prior to LP. Our meta-analy-sis confirms that there are few findings on history orphysical examination with a sufficiently strong associa-tion with SAH, and clinical decision rules suffer frommodest to poor specificity precisely because of this dif-ficulty identifying disease positive patients prior to test-ing. Arguably, if one’s own diagnostic yield for SAHon initial CT approaches 20% in awake headachepatients, one might expect one’s miss rate may beunacceptably high. Moreover, such high-risk patientsbenefit from proceeding directly to CTA especially ifthe unenhanced CT cannot be done within 6 hours ofheadache onset, also as indicated on the test thresholdcurves. On the other hand, using a more reasonablepre-CT probability of 1 in 10 (still higher than the 7%prevalence in prospective studies of emergencypatients with headache), a test with 95% sensitivityand perfect specificity implies that the patient being
CT Over 6-hours
Figure 4. continued.
992 Carpenter et al. • SUBARACHNOID HEMORRHAGE EVIDENCE-BASED DIAGNOSTICS

CT Under 6-hours
Figure 4. continued.
Table 5Diagnostic Accuracy of CSF Erythrocytes and Xanthochromia for SAH
Risk Factor Sensitivity, % (95% CI) Specificity, % (95% CI) LR+ (95% CI) LR (95% CI)
CSF RBC > 1000Czuczman 2013 65 (44–83) 79 (72–84) 3.09 (2.09–4.57) 0.44 (0.26–0.75)Perry 2015 93 (68–100) 91 (88–93) 10.25 (7.73–13.59) 0.07 (0.01–0.49)Pooled accuracy 76 (60–88) 88 (86–90) 5.66 (1.38–23.27) 0.21 (0.03–1.66)
Xanthochromia—U.K. NEQASPerry 2006 100 (16–100) 83 (77–88) 4.87 (2.71–8.73) 0.20 (0.02–2.53)Gangloff 2015 100 (48–100) 98 (97–99) 47.67 (26.67–85.20) 0.08 (0.01–1.21)Pooled accuracy 100 (59–100) 95 (93–96) 15.23 (1.58–146.73) 0.13 (0.02–0.83)
Xanthochromia—visualPerry 2006 50 (1–99) 97 (93–99) 15.57 (3.25–74.54) 0.52 (0.13–2.07)Dupont 2008 93 (66–100) 95 (89–98) 19.13 (8.04–45.45) 0.08 (0.01–0.50)Gangloff 2015 80 (28–99) 99 (98–99) 62.31 (28.47–136.37) 0.20 (0.04–1.17)Pooled accuracy 31 (21–41) 98 (97–99) 28.79 (9.77–84.80) 0.22 (0.06–0.80)
Xanthochromia—traditionalPerry 2006 100 (16–100) 29 (23–35) 1.17 (0.70–1.96) 0.57 (0.05–7.28)
Xanthochromia—Chalmers/KileyPerry 2006 0 (0–84) 89 (84–93) 1.49 (0.12–19.23) 0.94 (0.56–1.56)
Xanthochromia—Chalmers revisedPerry 2006 100 (16–100) 29 (23–35) 1.17 (0.70–1.96) 0.57 (0.05–7.28)
CSF = cerebrospinal fluid; LR+ = positive likelihood ratio; LR� = negative likelihood ratio; NEQAS = National External QualityAssessment Service; RBCs = red blood cells; SAH = subarachnoid hemorrhage.
ACADEMIC EMERGENCY MEDICINE • September 2016, Vol. 23, No. 9 • www.aemj.org 993

counseled actually has only a 1 in 180 chance of a rup-tured aneurysm (posttest odds = pre-test odds 9
LR� = 1:9 9 0.05).A cost-effectiveness analysis comparing CT-only, CT/
CTA, CT/LP, and CT/MRA as diagnostic modalitiesfound that CT-only and CT/LP are the preferred strate-gies of diagnosing ED patients with suspected SAH.116
The CT/LP strategy was slightly more costly, but moreeffective due to the LP reducing the possibility of amissed diagnosis and subsequent harm. However, since
the results of this meta-analysis indicate a much lowerthreshold for LP than used in the sensitivity analyses ofthe cost-effectiveness analysis, an updated cost-effec-tiveness analysis would likely shift the preferencetoward a CT-only strategy by decreasing the effective-ness of the CT/LP strategy. Further, this cost-effective-ness analysis did not consider crowding in the ED orphysician and patient reluctance toward LP, which arepractical barriers to the implementation of a CT/LPstrategy.
CSF RBC >1000 x 10 6/L
Figure 5. Forest plots for diagnostic accuracy of CSF analysis for SAH. CSF = cerebrospinal fluid; LR = likelihood ratio; SAH = sub-arachnoid hemorrhage.
994 Carpenter et al. • SUBARACHNOID HEMORRHAGE EVIDENCE-BASED DIAGNOSTICS

Implications for Future ResearchLP has long been considered to be the criterion stan-dard for diagnosing SAH as it may detect smallamounts of xanthochromia or blood in the CSF missedby CT. Due to the advancement of multislice CT, sensi-tivity to detect SAH has increased substantially. The pri-mary clinical question for emergency physiciansremains whether LP is indicated to rule out SAH if headCT is negative. Recent literature suggests within6 hours of symptom onset sensitivity of CT approaches100%. Additional studies in heterogeneous settings (ru-ral, non-North American, community hospitals) areneeded to confirm this diagnostic accuracy.
The significant interstudy heterogeneity observed inour meta-analysis indicates that more research is neededto quantify the diagnostic accuracy of history and physi-cal examination, as well as visible or spectrophotometricassessment of xanthochromia for the diagnosis of SAH.Unfortunately, few SAH studies adhere to the Standardsfor Reporting of Diagnostic Accuracy (STARD) reporting
guidelines.117 Failure to use reporting standards makesdiagnostic studies more difficult for clinicians, research-ers, and guideline developers to locate, interpret, andcompare.118 This is reflected in the poor inter-rater relia-bility results observed in our QUADAS-2 assessments ofblinding and appropriately reproducible conduct of theindex tests. In addition, studies that do not use theSTARD criteria are less likely to report key details neces-sary for clinicians to understand the risk of bias andexpected skew of observed point estimates. Future diag-nostic studies should adhere to the STARD reportingstandards117 and history/physical examination studiesshould follow the STARD criteria recommended for suchstudies.119
Spectrophotometric assessment of xanthochromiashould be standardized in terms of conduct andreporting.78 Most studies did not obtain an LP in allpatients or report any standard follow-up protocol tocapture false-negatives. Opening pressures were onlyobtained in 2% of suspected SAH cases34 and no
LP--UK Spectrophometric Xanthochromia
Figure 5. continued.
ACADEMIC EMERGENCY MEDICINE • September 2016, Vol. 23, No. 9 • www.aemj.org 995

studies evaluated the diagnostic accuracy of openingpressures. Future studies reporting the diagnosticaccuracy of CT should uniformly report the resolutionand timing of imaging, while incorporating post-EDfollow-up at reasonable intervals including review ofdeath registries for detection of false-negative results.In addition, the volume of CSF blood and rapidity ofaneurysmal bleeding probably influence both CT andLP test accuracy, threatening test independence implicitin Bayesian analyses, and therefore merits assessment
for interactions. Future diagnostic researchers shouldalso evaluate test performance stratified by age sinceaneurysmal SAH are rare in young patients. Further-more, the skew of observed sensitivities and specifici-ties as a result of spectrum bias, partial verificationbias, differential verification bias, and imperfect crite-rion standard bias should be contemplated in futurestudies.51
A planned secondary outcome of this systematicreview was to examine clinically significant SAH cases,
LP--Visible Xanthochromia
Figure 5. continued.
996 Carpenter et al. • SUBARACHNOID HEMORRHAGE EVIDENCE-BASED DIAGNOSTICS

defined as requiring neurosurgical intervention. Thestudies in this systematic review did not report ade-quately to be able to assess these outcomes. Specifically,perimesencephalic hemorrhage is traditionally consid-ered to be “true-positive” in SAH diagnostic research,but has a benign clinical course without specificinterventions to alter the natural course of diseaseother than analgesic symptom control. However,
perimesencephalic SAH can recur120 and some neuro-surgeons recommend catheter angiography in sus-pected SAH patients with xanthochromia after anondiagnostic CTA since a culprit aneurysm will beidentified in 8.3% of these cases.121 In clinical practiceSAH is deemed perimesencephalic if two-catheterangiography studies 7 days apart demonstrate no cere-bral aneurysm, since a single-catheter angiogram and
A CT Within 6 Hours of Headache Onset
B CT Beyond 6 Hours of Headache Onset
C LP Using RBC Counts in the Final Tube
D LP Using Visible Xanthochromia
Figure 6. Bernstein test indication curves for CT and LP. Test indication curves with 95% CI natural scale in A–D. Diagnostic accu-racy of CT or lumbar puncture for SAH. Raw test indication curves as proposed by Bernstein are shown, providing a graphical rep-resentation of the Bayesian posttest probability (y-axis) based on either a positive (upper curved black line, with 95% CIs in gray) ora negative (lower curved lines) test result as a function of the pretest probability (x-axis). The graphs use the same principle as theFagan nomogram, but provide more intuitive representations of the diagnostic accuracy of a test. The four tests considered are cra-nial CT obtained within 6 hours (A) or later (B) from headache onset or LP with more than 1,000 9 106/L RBCs (C) or visible xan-thochromia (D). The distances of the curves from the main diagonal of zero diagnostic information provide a visual representationof the information gained from the test result. CT = computed tomography; LP = lumbar puncture; SAH = subarachnoid hemor-rhage; RBCs = red blood cells.
ACADEMIC EMERGENCY MEDICINE • September 2016, Vol. 23, No. 9 • www.aemj.org 997

CTA can miss 4.2% of aneurysms.122 None of the diag-nostic studies included in this meta-analysis reporteduniform CT or catheter angiograms in all patients,
let alone repeat catheter angiograms in those with ini-tially “negative” or nondiagnostic advanced imaging.Future studies examining SAH should distinguish
A CT Within 6 Hours of Headache Onset
B CT Beyond 6 Hours of Headache Onset
C LP Using RBC Counts in the Final Tube
D LP Using Visible Xanthochromia
Figure 7. Testing thresholds. Test indication curves illustrating when benefits of testing outweigh the risks for SAH. The completetest indication curves as proposed by Bernstein are shown which incorporate the Pauker-Kassirer threshold approach to decidingwhether to perform the test in question. This technique compares the risks versus benefits for treatment (in this case proceeding toCT or formal angiography) and calculates the corresponding treatment threshold (shown as horizontal dashed lines, with the pointestimate in black and the upper and lower bands of the sensitivity analysis in gray). The vertical dashed line (or rightmost linewhen two are visible) therefore represents the pretest probability range below which the diagnostic test might be appropriate,assuming that the test in question had neither risks nor costs; when the pretest probability is higher, empirical treatment is recom-mended since the posttest probability exceeds this threshold even if the test is negative. Because tests have a nonzero risk, theactual pretest range for which performing the test is rational is narrower and is shown by the thick line between the arrowheads.The thinner solid line extending beyond the arrows illustrates the effect of reducing the test risk by half. At pretest probabilities tothe left of this range, no further testing is indicated. For example, this approach suggests proceeding directly to angiography whenthe pre-CT probability exceeds 10% (B), unless the unenhanced CT can be obtained within 6 hours (A) in which case a pretest prob-ability of nearly 70% seems appropriate before proceeding directly to angiography. On the other hand, the use of CT is warrantedeven in very-low-risk patients, down to perhaps 0.7% pretest probability as determined primarily by the risks of the CT itself. TheLP curves, however, illustrate that the pre-LP probabilities that justify performing LP are very narrow, ranging from 2% to 4% in C
and 2% to 7% in D. Moreover, these pre-LP probabilities in turn can only arise after an implausibly high pre-CT probability (>>20%).CT = computed tomography; LP = lumbar puncture; SAH = subarachnoid hemorrhage; RBCs = red blood cells.
998 Carpenter et al. • SUBARACHNOID HEMORRHAGE EVIDENCE-BASED DIAGNOSTICS

aneurysmal SAH from perimesencephalic hemorrhageto better examine SAH that merits surgical intervention.
LIMITATIONS
Identification of studies for this meta-analysis used onlyone individual with adjudication of uncertainty of inclu-sion/exclusion criteria by a second author, which couldintroduce a bias in study selection. In addition, weexcluded non-English studies which could have limitedthe scope of our findings and yield biased summaryestimates, although review of interventional meta-ana-lyses do not suggest significant differences when non-English studies are excluded.123 Of the 22 studies thatprovided sufficient detail to be able to reconstruct 2 9 2tables, there was significant heterogeneity in the man-ner in which data were collected and reported. Forexample, when examining sensitivity and specificity ofnoncontrast head CT, not all studies reported the speci-fic technology utilized. When technology utilized wasreported, it was done so in an inconsistent mannermaking it unclear which generation (how many slice)CT scanner was used. Variation in technology undoubt-edly affects diagnostic test performance, and standard-ized reporting of the particular technology used shouldbe encouraged in all future studies.117
Significant variation existed in mechanisms of follow-up for patients that were deemed SAH-negative. Somestudies did not conduct any follow-up, while others hadstructured telephone questionnaires and examinedcoroner records and public death certificates to ensurethat patients deemed disease free did not later turn outto have SAH. Without follow-up for patients that were
deemed SAH negative it is impossible to know that thepatient truly did not have a small CT-undetectable SAHor cerebral aneurysm when they were discharged fromthe ED. Finally, because some of the studies includedpatients who were unconscious or had neurologic defi-cits, the observed estimates of sensitivity and specificitymay be influenced by the spectrum of disease severity.53
There was also significant variation in definition ofdisease, particularly in the incorporation of CSF find-ings into the definition of being SAH-positive. Definitionof disease-positive ranged from number of RBCs in thefinal tube via LP to xanthochromia of CSF. Number ofRBCs was not standardized. Xanthochromia wasdefined by visual inspection in some studies and spec-trophotometry in others. Xanthochromia via spec-trophotometry had substantial variation in theabsorption spectrum used to define a positive LP. Otherstudies used spectrophotometry to detect bilirubin andoxyhemoglobin as indicating a patient with SAH.
CONCLUSIONS
This meta-analysis identified a 7.5% weighted preva-lence of subarachnoid hemorrhage in ED patients withconcerning headache. Although the available high-qual-ity diagnostic evidence is limited, there is no singlecharacteristic on history or physical examination that isadequate to rule in or rule out subarachnoid hemor-rhage in ED settings. Using a threshold of 1,000 9 106/Lred blood cells in the final tube has a summary positivelikelihood ratio of 5.7 and negative likelihood ratio of0.21. Within 6 hours of symptom onset, noncontrastcranial computed tomography accurately both rules inand rules out subarachnoid hemorrhage. Given therisks and benefits of further testing and the limiteddiagnostic accuracy of cerebrospinal fluid erythrocytecounts and of various xanthochromia definitions, lum-bar puncture is likely to benefit only patients within anarrow band of pre–lumbar puncture probabilities,around 2% to 7%. Given the accuracy of computedtomography, even several hours after headache onset,such pre–lumbar puncture probabilities correspond topre–computed tomography probabilities of 20% orhigher. While many still consider computed tomogra-phy followed by lumbar puncture to be the criterionstandard for the diagnosis of subarachnoid hemor-rhage, few studies use this criterion standard givenpractice patterns evolving away from routine lumbarpuncture. The role of lumbar puncture may well wanefurther with improving multislice computed tomogra-phy and increasing evidence to refute the utility of lum-bar puncture. Validation of subarachnoid hemorrhageclinical decision rules offers the opportunity to moreaccurately risk stratify ED headache patients to identifysubsets most likely to benefit from post–computedtomography lumbar puncture, computed tomographyangiography, or no further testing.
References
1. Edlow JA, Panagos PD, Godwin SA, Thomas TL,Decker WW; American College of EmergencyPhysicians. Clinical policy: critical issues in the
Table 6Using Test Indication Curves
You have just seen a 48-year-old housewife who presentsto the ED by private vehicle 8 hours after the onset of asevere headache that peaked within 10 minutes of onset.She is nauseated and complains of neck stiffness but herneurologic examination is intact and she is able to fullyflex her neck. You assign a pretest probability of 10% forSAH and await the final read by the neuroradiologist onduty even though the imaging study appears to beunremarkable to you and to the CT technician. The test–treatment curves can be used like the Fagan nomogram tocalculate the posttest probability of disease. Therefore, youcan estimate that the posttest probability will be around0.8% should the study prove negative (Figure 7B). You canalso estimate that, if you had performed an LP rather thanCT, the posttest likelihood would be around 2% if fewerthan 1,000 9 106/L RBCs were present in the final tube ofCSF (Figure 7C), and similarly 2% if there were no visiblexanthochromia. But you can also “chain” sequential testresults, with the usual caveat that the tests may not beperfectly independent. Thus, after the neuroradiologistconfirms that there are no signs of SAH on the CT, thesame patient would have her probability of diseaselowered from 0.8% pre-LP to about 0.1% after an LPnegative for xanthochromia (Figure 7D). Moreover,decision analysis would suggest that, for this patient, therisks of LP outweigh the potential benefits, since thepretest probability of 0.8% is already below the rangewhen LP is beneficial whether one uses erythrocyte countor xanthochromia, as indicated by the horizontal arrows onthe test indication curves.
ACADEMIC EMERGENCY MEDICINE • September 2016, Vol. 23, No. 9 • www.aemj.org 999

evaluation and management of adult patients pre-senting to the emergency department with acuteheadache. Ann Emerg Med 2008;52:407–36.
2. Landtblom AM, Fridriksson S, Boivie J, Hillman J,Johansson G, Johansson I. Sudden onset headache:a prospective study of features, incidence andcauses. Cephalagia 2002;22:354–60.
3. Delasobera BE, Osborn SR, Davis JE. Thunderclapheadache with orgasm: a case of basilar artery dis-section associated with sexual intercourse. J EmergMed 2012;43:e43–7.
4. Imperato J, Burstein J, Edlow JA. Benign exertionalheadache. Ann Emerg Med 2003;41:98–103.
5. Dodick DW, Wijdicks EF. Pituitary apoplexy pre-senting as a thunderclap headache. Neurology1998;50:1510–1.
6. de Bruijn SF, Stam J, Kappelle LJ. Thunderclapheadache as first symptom of cerebral venous sinusthrombosis. CVST Study Group. Lancet1996;348:1623–5.
7. Pascual J, Iglesias F, Oterino A, Vasquez-BarqueroA, Berciano J. Cough, exertional, and sexual head-aches: an analysis of 72 benign and symptomaticcases. Neurology 1996;46:1520–4.
8. Cordenier A, De Hertogh W, De Keyser J, VersijptJ. Headache associated with cough: a review. JHeadache Pain 2013;14:42.
9. Dodick DW, Brown RD Jr, Britton JW, Huston J3rd. Nonaneurysmal thunderclap headache withdiffuse, multifocal, segmental, and reversible vasos-pasm. Cephalagia 1999;19:118–23.
10. Day JW, Raskin NH. Thunderclap headache: symp-tom of unruptured cerebral aneurysm. Lancet1986;2:1247–8.
11. Edlow JA. Diagnosis of subarachnoid hemorrhagein the emergency department. Emerg Med ClinNorth Am 2003;21:73–87.
12. Canneti B, Mosqueira AJ, Nombela F, Gilo F,Vivancos J. Spontaneous subarachnoid hemor-rhage with negative angiography managed in astroke unit: clinical and prognostic characteristics.J Stroke Cerebrovasc Dis 2015;24:2484–90.
13. Elhadi AM, Zabramski JM, Almefty KK, et al.Spontaneous subarachnoid hemorrhage ofunknown origin: hospital course and long-termclinical and angiographic follow-up. J Neurosurg2015;122:663–70.
14. Wang QT, Tuhrim S. Etiologies of intracere-bral hematomas. Curr Atherscler Rep 2012;14:314–21.
15. Hop JW, Rinkel GJ, Algra A, van Gijn J. Case-fatal-ity rates and functional outcome after subarach-noid hemorrhage: a systematic review. Stroke1997;28:660–4.
16. Nieuwkamp DJ, Setz LE, Algra A, Linn FH, deRooij NK, Rinkel GJ. Changes in case fatality ofaneurysmal subarachnoid haemorrhage over time,according to age, sex, and region: a meta-analysis.Lancet Neurol 2009;8:635–42.
17. Carstairs SD, Tanen DA, Duncan TD, et al. Com-puted tomographic angiography for the evaluationof aneurysmal subarachnoid hemorrhage. AcadEmerg Med 2006;13:486–92.
18. Powell J, Kitchen N, Heslin J, Greenwood R. Psy-chosocial outcomes at 18 months after good neuro-logical recovery from aneurysmal subarachnoidhaemorrhage. J Neurol Neurosurg Psychiatry2004;75:1119–24.
19. Hillman J, Saveland H, Jakobsson KE, et al. Overallmanagement outcome of ruptured posterior fossaaneurysms. J Neurosurg 1996;85:33–8.
20. Perry JJ, Stiell IG, Sivilotti ML, et al. Sensitivity ofcomputed tomography performed within six hoursof onset of headache for diagnosis of subarachnoidhaemorrhage: prospective cohort study. BMJ2011;343:d4277.
21. Edlow JA, Caplan LR. Avoiding pitfalls in the diag-nosis of subarachnoid hemorrhage. N Engl J Med2000;342:29–36.
22. Leblanc R. The minor leak preceding subarachnoidhemorrhage. J Neurosurg 1987;66:35–9.
23. Johansson A, Lagerstedt K, Asplund K. Mishaps inthe management of stroke: a review of 214 com-plaints to a medical responsibility board. Cere-brovasc Dis 2004;18:16–21.
24. Duffy GP. The “warning leak” in spontaneous sub-arachnoid haemorrhage. Med J Aust 1983;1:514–6.
25. Verweij RD, Wijdicks EF, van Gijn J. Warningheadache in aneurysmal subarachnoid hemor-rhage. A case-control study. Arch Neurol1988;45:1019–20.
26. Vermeulen MJ, Schull MJ. Missed diagnosis ofsubarachnoid hemorrhage in the emergencydepartment. Stroke 2007;38:1216–21.
27. Robbert M, Hoogmoed J, van Straaten HA, CoertBA, Peter-Vandertop W, Verbaan D. Time intervalsfrom aneurysmal subarachnoid hemorrhage totreatment and factors contributing to delay. J Neu-rol 2014;261:473–9.
28. Kwiatkowski T, Alagappan K. Headache. in: MarxJA, Hockberger RS, Walls RM, et al., eds. Rosen’sEmergency Medicine: Concepts and Clinical Prac-tice, 2nd ed. Philadelphia: Mosby-Elsevier,2010:1356–66.
29. Hackman JL, Johnson MD, Ma OJ. Spontaneoussubarachnoid and intracerebral hemorrhage. in:Tintinalli JE, Stapczynski JS, Ma OJ, Cline DM,Cydulka RK, Meckler GD, eds. Tintinalli’s Emer-gency Medicine: A Comprehensive Study Guide,7th ed. New York City, NY: McGraw-Hill,2011:1118–22.
30. Carpenter CR, Raja AS, Brown MD. Overtestingand the downstream consequences of overtreat-ment: implications of “preventing overdiagnosis”for emergency medicine. Acad Emerg Med2015;22:1484–92.
31. Seupaul RA, Somerville GG, Viscusi C, ShepardAJ, Hauter WE. Prevalence of postdural punctureheadache after ED performed lumbar puncture.Am J Emerg Med 2005;23:913–5.
32. Straus SE, Thorpe KE, Holroyd-Leduc J. How do Iperform a lumbar puncture and analyze the resultsto diagnose bacterial meningitis? JAMA2006;296:2012–22.
33. Czuczman AD, Thomas LE, Boulanger AB, et al.Interpreting red blood cells in lumbar puncture:
1000 Carpenter et al. • SUBARACHNOID HEMORRHAGE EVIDENCE-BASED DIAGNOSTICS

distinguishing true subarachnoid hemorrhage fromtraumatic tap. Acad Emerg Med 2013;20:247–56.
34. Brunell A, Ridefelt P, Zelano J. Differential diag-nostic yield of lumbar puncture in investigation ofsuspected subarachnoid haemorrhage: a retrospec-tive study. J Neurol 2013;260:1631–6.
35. Blok KM, Rinkel GJ, Majoie CB, et al. CT within6 hours of headache onset to rule out subarach-noid hemorrhage in nonacademic hospitals. Neu-rology 2015;84:1927–32.
36. Sayer D, Bloom B, Fernando K, et al. An observa-tional study of 2,248 patients presenting with head-ache, suggestive of subarachnoid hemorrhage,who received lumbar punctures following normalcomputed tomography of the head. Acad EmergMed 2015;22:1267–73.
37. Euerle BD. Spinal puncture and cerebral spinalfluid examination. in: Roberts JR, Hedges JR, Cus-talow CB, Chanmugam AS, Chudnofsky CR,McManus J, eds. Clinical Procedures in EmergencyMedicine, 5th ed. Philadelphia, PA: Saunders-Else-vier, 2010:1107–27.
38. Perry JJ, Stiell IG, Sivilotti ML, et al. High risk clini-cal characteristics for subarachnoid haemorrhagein patients with acute headache: prospective cohortstudy. BMJ 2010;341:c5204.
39. Perry JJ, Stiell IG, Sivilotti ML, et al. Clinical deci-sion rules to rule out subarachnoid hemorrhagefor acute headache. JAMA 2013;310:1248–55.
40. Shah KH, Richard KM, Nicholas S, Edlow JA. Inci-dence of traumatic lumbar puncture. Acad EmergMed 2003;10:151–4.
41. Roost KT, Pimstone NR, Diamond I, Schmid R. Theformation of cerebrospinal fluid xanthochromiaafter subarachnoid hemorrhage. Enzymatic conver-sion of hemoglobin to bilirubin by the arachnoidand choroid plexus. Neurology 1972;22:973–7.
42. Edlow JA, Bruner KS, Horowitz GL. Xanthochro-mia. Arch Pathol Lab Med 2002;126:413–5.
43. Chu K, Hann A, Greenslade J, Williams J, BrownA. Spectrophotometry or visual inspection to mostreliably detect xanthochromia in subarachnoidhemorrhage: systematic review. Ann Emerg Med2014;64:256–64.e255.
44. Westerlaan HE, van Dijk JM, Jansen-van derWeide MC, et al. Intracranial aneurysms in patientswith subarachnoid hemorrhage: CT angiographyas a primary examination tool for diagnosis–sys-tematic review and meta-analysis. Radiology2011;258:134–45.
45. Sailer AM, Wagemans BA, Nelemans PJ, de GraafR, van Zwam WH. Diagnosing intracranial aneur-ysms with MR angiography: systematic review andmeta-analysis. Stroke 2014;45:119–26.
46. Pauker SG, Kassirer JP. Therapeutic decision mak-ing: a cost-benefit analysis. N Engl J Med 1975;293:229–34.
47. Pauker SG, Kassirer JP. The threshold approach toclinical decision making. N Engl J Med1980;302:1109–17.
48. Bernstein J. Test-indication curves. Med DecisMaking 1997;17:103–6.
49. Liberati A, Altman DG, Tetzlaff J, et al. ThePRISMA statement for reporting systematicreviews and meta-analyses of studies that evaluatehealthcare interventions: explanation and elabora-tion. BMJ 2009;339:b2700.
50. Stroup DF, Berlin JA, Morton SC, et al. Meta-ana-lysis of observational studies in epidemiology: aproposal for reporting. Meta-analysis Of Observa-tional Studies in Epidemiology (MOOSE) group.JAMA 2000;283:2008–12.
51. Kohn MA, Carpenter CR, Newman TB. Under-standing the direction of bias in studies of diag-nostic test accuracy. Acad Emerg Med 2013;20:1194–206.
52. Whiting PF, Rutjes AW, Westwood ME, et al.QUADAS-2: a revised tool for the quality assess-ment of diagnostic accuracy studies. Ann InternMed 2011;155:529–36.
53. Mulherin SA, Miller WC. Spectrum bias or spec-trum effect? Subgroup variation in diagnostic testevaluation. Ann Intern Med 2002;137:598–602.
54. Tsementzis SA, Hitchcock ER, DeCothi A, Gill JS.Comparative studies of the diagnostic value ofcerebrospinal fluid spectrophotometry and com-puted tomographic scanning in subarachnoid hem-orrhage. Neurosurgery 1985;17:908–12.
55. Kanzaria HK, McCabe AM, Meisel ZM, et al.Advancing patient-centered outcomes in emer-gency diagnostic imaging: a research agenda. AcadEmerg Med 2015;22:1435–46.
56. Byrt T, Bishop J, Carlin JB. Bias, prevalence andkappa. J Clin Epidemiol 1993;46:423–9.
57. Macaskill PG, Deeks JJ, Harbord RM, Takwoingi Y.Cochrane Handbook for Systematic Reviews ofDiagnostic Test Accuracy. Version 0.9.0. London:The Cochrane Collaboration, 2010.
58. Zamora J, Abraira V, Muriel A, Khan K, Coomara-samy A. Meta-DiSc: a software for meta-analysis oftest accuracy data. BMC Med Res Methodol2006;6:31.
59. DerSimonian R, Laird N. Meta-analysis in clinicaltrials. Control Clin Trials 1986;7:177–88.
60. DerSimonian R, Kacker R. Random-effects modelfor meta-analysis of clinical trials: an update. Con-temp Clin Trials 2007;28:105–114.
61. Deeks JJ, Macaskill P, Irwig L. The performance oftests of publication bias and other sample sizeeffects in systematic reviews of diagnostic testaccuracy was assessed. J Clin Epidemiol2005;58:882–93.
62. Grimes DA, Schulz KF. Refining clinical diagnosiswith likelihood ratios. Lancet 2005;365:1500–5.
63. Gallagher EJ. Clinical utility of likelihood ratios.Ann Emerg Med 1998;31:391–7.
64. Hayden SR, Brown MD. Likelihood ratio: a power-ful tool for incorporating the results of a diagnostictest into clinical decisionmaking. Ann Emerg Med1999;33:575–80.
65. Glasziou P. Threshold analysis via the Bayes’nomogram. Med Decis Making 1991;11:61–2.
66. Byrt T. How good is that agreement? Epidemiology1996;7:561.
ACADEMIC EMERGENCY MEDICINE • September 2016, Vol. 23, No. 9 • www.aemj.org 1001

67. Perry JJ, Sivilotti ML, Stiell IG, et al. Should spec-trophotometry be used to identify xanthochromiain the cerebrospinal fluid of alert patients sus-pected of having subarachnoid hemorrhage?Stroke 2006;37:2467–72.
68. Gangloff A, Nadeau L, Perry JJ, Baril P, Emond M.Ruptured aneurysmal subarachnoid hemorrhage inthe emergency department: clinical outcome ofpatients having a lumbar puncture for red bloodcell count, visual and spectrophotometric xan-thochromia after a negative computed tomography.Clin Biochem 2015;48:634–9.
69. Linn FH, Rinkel GJ, Algra A, van Gijn J. Headachecharacteristics in subarachnoid haemorrhage andbenign thunderclap headache. J Neurol NeurosurgPsychiatry 1998;65:791–3.
70. Morgenstern LB, Luna-Gonzales H, Huber JC,et al. Worst headache and subarachnoid hemor-rhage: prospective, modern computed tomographyand spinal fluid analysis. Ann Emerg Med 1998;32(3 Pt 1):297–304.
71. Bø SH, Davidsen EM, Gulbrandsen P, Dietrichs E.Acute headache: a prospective diagnostic work-upof patients admitted to a general hospital. Eur JNeurol 2008;15:1293–9.
72. van der Wee N, Rinkel GJ, Hasan D, van Gijn J.Detection of subarachnoid haemorrhage on earlyCT: is lumbar puncture still needed after a negativescan? J Neurol Neurosurg Psychiatry 1995;58:357–9.
73. Boesiger BM, Shiber JR. Subarachnoid hemor-rhage diagnosis by computed tomography andlumbar puncture: are fifth generation CT scannersbetter at identifying subarachnoid hemorrhage? JEmerg Med 2005;29:23–7.
74. O’Neill J, McLaggan S, Gibson R. Acute headacheand subarachnoid haemorrhage: a retrospectivereview of CT and lumbar puncture findings. ScottMed J 2005;50:151–3.
75. Backes D, Rinkel GJ, Kemperman H, Linn FH, Ver-gouwen MD. Time-dependent test characteristicsof head computed tomography in patients sus-pected of nontraumatic subarachnoid hemorrhage.Stroke 2012;43:2115–9.
76. Dupont SA, Wijdicks EF, Manno EM, RabinsteinAA. Thunderclap headache and normal computedtomographic results: value of cerebrospinal fluidanalysis. Mayo Clinic Proc 2008;83:1326–31.
77. Hann A, Chu K, Greenslade J, Williams J, BrownA. Benefit of cerebrospinal fluid spectrophotometryin the assessment of CT scan negative suspectedsubarachnoid haemorrhage: a diagnostic accuracystudy. J Clin Neurosci 2015;22:173–9.
78. Cruickshank A, Auld P, Beetham R, et al. Revisednational guidelines for analysis of cerebrospinalfluid for bilirubin in suspected subarachnoid haem-orrhage. Ann Clin Biochem 2008;45(Pt 3):238–44.
79. Perry JJ, Alyahya B, Sivilotti ML, et al. Differentia-tion between traumatic tap and aneurysmal sub-arachnoid hemorrhage: prospective cohort study.BMJ 2015;350:h568.
80. Brown MD, Reeves MJ. Evidence-based emergencymedicine skills for evidence-based emergency care.Interval likelihood ratios: another advantage for
the evidence-based diagnostician. Ann Emerg Med2003;42:292–7.
81. Hall EJ, Brenner DJ. Cancer risks from diagnosticradiology. Br J Radiol 2008;81:362–78.
82. Schievink WI. Intracranial aneurysms. N Engl JMed 1997;336:28–40.
83. Burrows AM, Korumilli R, Lanzino G. How we doit: acute management of subarachnoid hemor-rhage. Neurol Res 2013;35:111–6.
84. McDougall CG, Spetzler RF, Zabramski JM, et al.The Barrow Ruptured Aneurysm Trial. J Neuro-surg 2012;116:135–44.
85. Spetzler RF, McDougall CG, Albuquerque FC, et al.The Barrow Ruptured Aneurysm Trial: 3-yearresults. J Neurosurg 2013;119:146–57.
86. Molyneux AJ, Kerr RS, Yu LM, et al. Internationalsubarachnoid aneurysm trial (ISAT) of neurosurgi-cal clipping versus endovascular coiling in 2143patients with ruptured intracranial aneurysms: arandomised comparison of effects on survival,dependency, seizures, rebleeding, subgroups, andaneurysm occlusion. Lancet 2005;366:809–17.
87. McNeill A. Neurological negligence claims in the NHSfrom 1995 to 2005. Eur J Neurol 2007;14:399–402.
88. Choosing Wisely: American College of EmergencyPhysicians. 2014. Available at: http://www.choos-ingwisely.org/societies/american-college-of-emer-gency-physicians/. Accessed Oct 16, 2015.
89. Mark DG, Hung YY, Offerman SR, et al. Nontrau-matic subarachnoid hemorrhage in the setting ofnegative cranial computed tomography results:external validation of a clinical and imaging predic-tion rule. Ann Emerg Med 2013;62:1–10.
90. Mark DG, KeneMV, Udaltsova N, Vinson DR, BallardDW. Sensitivity of a clinical decision rule and earlycomputed tomography in aneurysmal subarachnoidhemorrhage. West J EmergMed 2015;16:671–6.
91. Hunter BR, Carpenter CR. The development ofclinical prediction rules. in: Wilson MP, GulumaKZ, Hayden SR, eds. Doing Research in Emergency& Acute Care: Making Order Out of Chaos.Oxford, UK: Wiley-Blackwell, 2015:139–47.
92. Perry JJ, Sivilotti ML, Stiell IG. Pragmatic interpre-tation of the study of nontraumatic subarachnoidhemorrhage in the setting of negative cranial com-puted tomography results: external validation of aclinical and imaging prediction rule. Ann EmergMed 2013;62:435–6.
93. Coats TJ, Loffhagen R. Diagnosis of subarachnoidhaemorrhage following a negative computedtomography for acute headache: a Bayesian analy-sis. Eur J Emerg Med 2006;13:80–3.
94. Coats TJ. Subarachnoid haemorrhage: lumbar punc-ture for every negative scan? BMJ 2006;333:396–7.
95. Gee C, Dawson M, Bledsoe J, et al. Sensitivity ofnewer-generation computed tomography scannersfor subarachnoid hemorrhage: a Bayesian analysis.J Emerg Med 2012;43:13–8.
96. Malabarey MA, Barbic D. Can the combination ofa negative computed tomography result and a neg-ative lumbar puncture safely exclude the diagnosisof subarachnoid hemorrhage in patients with thun-derclap headache? CJEM 2013;15:113–5.
1002 Carpenter et al. • SUBARACHNOID HEMORRHAGE EVIDENCE-BASED DIAGNOSTICS

97. Farzad A, Radin B, Oh JS, et al. Emergency diag-nosis of subarachnoid hemorrhage: an evidence-based debate. J Emerg Med 2013;44:1045–53.
98. Kuntz KM, Kokmen E, Stevens JC, Miller P, OffordKP, Ho MM. Post-lumbar puncture headaches:experience in 501 consecutive procedures. Neurol-ogy 1992;42:1884–7.
99. Abouleish E, Vega S, Blendinger I, Tio TO. Long-term follow-up of epidural blood patch. AnesthAnalg 1975;54:459–63.
100. Evans RW. Complications of lumbar puncture.Neurol Clin 1998;16:83–105.
101. Muhammed O, Teubner D, Jones DN, Slavotinek JP.Retrospective audit of the investigation of patientswith suspected acute subarachnoid haemorrhage. JMed Imaging Radiat Oncol 2010;54:339–46.
102. Mehrotra P, Sookhoo S, Kolla S, Halbert H, LavellK, England S. Investigation of subarachnoid haem-orrhage: does the buck stop with CT? J Med Life2010;3:338–42.
103. Perry JJ, Stiell IG, Wells GA, et al. Attitudes andjudgment of emergency physicians in the manage-ment of patients with acute headache. Acad EmergMed 2005;12:33–7.
104. Perry JJ, Stiell IG, Wells GA, Spacek A. Diagnostictest utilization in the emergency department foralert headache patients with possible subarachnoidhemorrhage. CJEM 2002;4:333–7.
105. Rinkel GJ, Wijdicks EF, Vermeulen MJ, et al.Nonaneurysmal perimesencephalic subarachnoidhemorrhage: CT and MR patterns that differ fromaneurysmal rupture. AJNR Am J Neuroradiol1991;12:829–34.
106. Topcuoglu MA, Ogilvy CS, Carter BS, BuonannoFS, Koroshetz WJ, Singhal AB. Subarachnoidhemorrhage without evident cause on initialangiography studies: diagnostic yield of subse-quent angiography and other neuroimaging tests.J Neurosurg 2003;98:1235–40.
107. Kalra VB, Wu X, Matouk CC, Malhotra A. Use offollow-up imaging in isolated perimesencephalicsubarachnoid hemorrhage: a meta-analysis. Stroke2015;46:401–6.
108. Youssef NA, Gordon AJ, Moon TH, et al. Emer-gency department patient knowledge, opinions,and risk tolerance regarding computed tomogra-phy scan radiation. J Emerg Med 2014;46:208–14.
109. McCormack RF, Hutson A. Can computed tomogra-phy angiography of the brain replace lumbar punc-ture in the evaluation of acute-onset headache aftera negative noncontrast cranial computed tomogra-phy scan? Acad Emerg Med 2010;17:444–51.
110. Hess EP, Grudzen CR, Thomson R, Raja AS, Carpen-ter CR. Shared decision-making in the emergencydepartment: respecting patient autonomy when sec-onds count. Acad EmergMed 2015;22:856–64.
111. Linn FH, Wijdicks EF, vander Graaf Y, Weerdes-teyn-van Vliet FA, Bartelds AI, van Gijn J.Prospective study of sentinel headache in aneurys-mal subarachnoid haemorrhage. Lancet 1994;344:590–3.
112. Cloft HJ, Joseph GJ, Dion JE. Risk of cerebralangiography in patients with subarachnoid hemor-rhage, cerebral aneurysm, and arteriovenous mal-formation: a meta-analysis. Stroke 1999;30:317–20.
113. Brown RD Jr, Broderick JP. Unruptured intracra-nial aneurysms: epidemiology, natural history,management options, and familial screening. Lan-cet Neurol 2014;13:393–404.
114. Brennan JW, Schwartz ML. Unruptured intracra-nial aneurysms: appraisal of the literature and sug-gested recommendations for surgery, usingevidence-based medicine criteria. Neurosurgery2000;47:1359–71; discussion 1371–2.
115. Rinkel GJ, Djibuti M, Algra A, van Gijn J. Preva-lence and risk of rupture of intracranial aneur-ysms: a systematic review. Stroke 1998;29:251–6.
116. Ward MJ, Bonomo JB, Adeoye O, Raja AS, PinesJM. Cost-effectiveness of diagnostic strategies forevaluation of suspected subarachnoid hemorrhagein the emergency department. Acad Emerg Med2012;19:1134–44.
117. Bossuyt PM, Reitsma JB, Bruns DE, et al. TheSTARD statement for reporting studies of diagnos-tic accuracy: explanation and elaboration. AnnIntern Med 2003;138:W1–W12.
118. Smidt N, Rutjes AW, van der Windt DA, et al. Thequality of diagnostic accuracy studies since theSTARD statement: has it improved? Neurology2006;67:792–7.
119. Simel DL, Rennie D, Bossuyt PM. The STARDstatement for reporting diagnostic accuracy stud-ies: application to the history and physical exami-nation. J Gen Intern Med 2008;23:768–74.
120. Reynolds MR, Blackburn SL, Zipfel GJ. Recurrentidiopathic perimesencephalic subarachnoid hemor-rhage. J Neurosurg 2011;115:612–6.
121. Wallace AN, Dines JN, Zipfel GJ, Derdeyn CP. Yieldof catheter angiography after computed tomogra-phy negative, lumbar puncture positive subarach-noid hemorrhage. Stroke 2013;44:1729–31.
122. Delgado-Almandoz JE, Jagadeesan BD, Refai D,et al. Diagnostic yield of repeat catheter angiogra-phy in patients with catheter and computedtomography angiography negative subarachnoidhemorrhage. Neurosurgery 2012;70:1135–42.
123. Morrison A, Polisena J, Husereau D, et al. Theeffect of English-language restriction on systematicreview-based meta-analyses: a systematic reviewof empirical studies. Int J Technol Assess HealthCare 2012;28:138–44.
Supporting Information
The following supporting information is available in theonline version of this paper:
Data Supplement S1. Full search strategies forPubMed and Embase.
Data Supplement S2. Synopsis of SAH clinical deci-sion rule components and diagnostic accuracy.
Data Supplement S3. Test–treatment calculator.
ACADEMIC EMERGENCY MEDICINE • September 2016, Vol. 23, No. 9 • www.aemj.org 1003