Embed Size (px)
Citation preview

Diagnostic and Interventional Imaging (2015) 96, 657—666
CONTINUING EDUCATION PROGRAM: FOCUS. . .
Subarachnoid hemorrhage in ten questions
M. Edjlali a,b,∗, C. Rodriguez-Régenta, J. Hodelb,R. Aboukaisc, D. Trystrama, J.-P. Pruvob, J.-F. Medera,C. Oppenheima, J.-P. Lejeunec, X. Leclercb,O. Naggaraa
a Inserm UMR 894, Department of Neuroradiolgy, Faculty of Medicine Paris DescartesUniversity, Pyschiatry and Neurosciences Centers, Sainte-Anne Hospital, Sorbonne Paris Cité,1, rue Cabanis, 75014 Paris, Franceb Department of Neuroradiology, Lille Nord de France University, Roger Salengro Hospital,Lille University Hospitals, avenue Émile-Laine, 59037 Lille cedex, Francec Department of Neurosurgery, Lille Nord de France University, Roger Salengro Hospital, LilleUniversity Hospitals, avenue Émile-Laine, 59037 Lille cedex, France
KEYWORDSHemorrhage;Intracranialaneurysm;CT;MRI
Abstract Traumatic subarachnoid hemorrhage (SAH) has an annual incidence of 9 per 100 000people. It is a rare but serious event, with an estimated mortality rate of 40% within thefirst 48 hours. In 85% of cases, it is due to rupture of an intracranial aneurysm. In the earlyphase, during the first 24 hours, cerebral CT, combined with intracranial CT angiography isrecommended to make a positive diagnosis of SAH, to identify the cause and to investigatefor an intracranial aneurysm. Cerebral MRI may be proposed if the patient’s clinical conditionallows it. FLAIR imaging is more sensitive than CT to demonstrate a subarachnoid hemorrhageand offers greater degrees of sensitivity for the diagnosis of restricted subarachnoid hemorrhagein cortical sulcus. A lumbar puncture should be performed if these investigations are normalwhile clinical suspicion is high.
© 2015 Éditions francaises de radiologie. Published by Elsevier Masson SAS. All rights reserved.
Subarachnoid hemorrhage (SAH) is defined as blood in the cerebrospinal fluid contained
in the basal cisternae and the sub-arachnoid space of the cerebral hemispheres, containedbetween the arachnoid mater and the pia mater.The most common cause is head injury. Apart from this cause, SAH accounts for 5 to10% of cerebrovascular accidents and has a high mortality rate, which is estimated to be
∗ Corresponding author. Inserm UMR 894, Department of Neuroradiolgy, Faculty of Medicine Paris Descartes University, Pyschiatry andNeurosciences Centers, Sainte-Anne Hospital, Sorbonne Paris Cité, 1, rue Cabanis, 75014 Paris, France.
E-mail address: [email protected] (M. Edjlali).
http://dx.doi.org/10.1016/j.diii.2015.06.0032211-5684/© 2015 Éditions francaises de radiologie. Published by Elsevier Masson SAS. All rights reserved.
6
bo(
fc
tr
Wsa
Uho(i
Aodcsehua2ChtAi
C
Fc(et
ho
rarlf
amv
ahtwaoo
As
N
Ahstatomartery.
On the other hand, features of pyramidal irritation and
58
etween 40 and 50% [1,2]. By far the most common causef SAH apart from trauma is intracranial aneurysm rupture85% of non-traumatic causes) [3].
If SAH is suspected, cerebral imaging should be per-ormed urgently to confirm the diagnosis, identify anyomplications and investigate its cause.
We propose you here to develop the theme of SAH throughen questions. We will not consider the complications ofebleeding and vasospasm in this article.
hen a patient presents with audden-onset headache, is CT anppropriate investigation?
nenhanced cerebral CT is recommended for acuteeadaches (less than 24 hours old), which are sudden innset, to investigate for a subarachnoid hemorrhage (SAH)grade A guideline, guide to the correct use of medical imag-ng examinations).
The clinical features of the headache are fundamental. SAH should be suspected in the case of a sudden-nset headache of maximum intensity from the outset andescribed as a ‘‘thunderclap in a clear sky’’. This may beombined with meningism without fever or reduced con-ciousness level. An urgent CT should be performed andnables a diagnosis of SAH to be made if an unenhancedyperdensity is present in the subarachnoid spaces, whichsually involves the basal cisternae, inter-hemispheric sulcind lateral sulci [4]. When it is performed during the first4 hours, CT has a sensitivity of 95% [5]. The sensitivity ofT depends mostly on the extent of the SAH but also onemoglobin concentration and falls with the time betweenhe initial headache and time when the scan is performed.fter 7 days, therefore, CT is positive in only 50% of cases
n SAH.
Apart from a positive diagnosis of SAH, the initialT examination can detect the early complications of
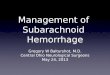
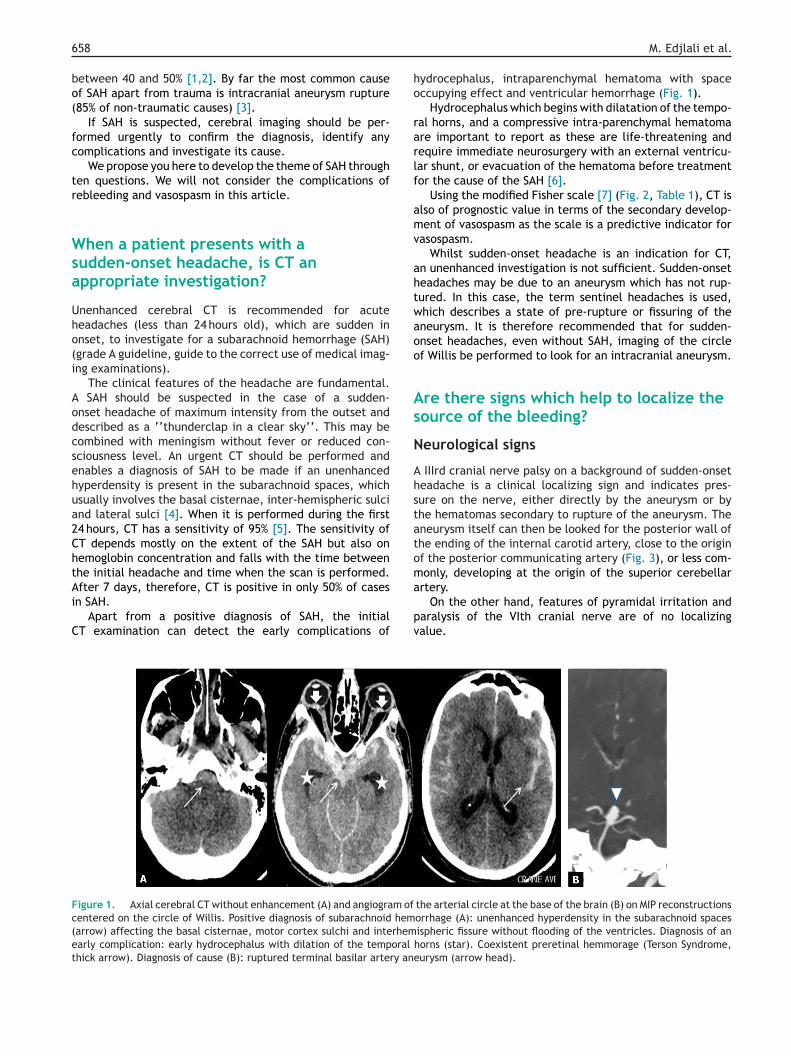
igure 1. Axial cerebral CT without enhancement (A) and angiogram ofentered on the circle of Willis. Positive diagnosis of subarachnoid hemarrow) affecting the basal cisternae, motor cortex sulchi and interhemarly complication: early hydrocephalus with dilation of the temporal
hick arrow). Diagnosis of cause (B): ruptured terminal basilar artery an
pv
M. Edjlali et al.
ydrocephalus, intraparenchymal hematoma with spaceccupying effect and ventricular hemorrhage (Fig. 1).
Hydrocephalus which begins with dilatation of the tempo-al horns, and a compressive intra-parenchymal hematomare important to report as these are life-threatening andequire immediate neurosurgery with an external ventricu-ar shunt, or evacuation of the hematoma before treatmentor the cause of the SAH [6].
Using the modified Fisher scale [7] (Fig. 2, Table 1), CT islso of prognostic value in terms of the secondary develop-ent of vasospasm as the scale is a predictive indicator for
asospasm.Whilst sudden-onset headache is an indication for CT,
n unenhanced investigation is not sufficient. Sudden-onseteadaches may be due to an aneurysm which has not rup-ured. In this case, the term sentinel headaches is used,hich describes a state of pre-rupture or fissuring of theneurysm. It is therefore recommended that for sudden-nset headaches, even without SAH, imaging of the circlef Willis be performed to look for an intracranial aneurysm.
re there signs which help to localize theource of the bleeding?
eurological signs
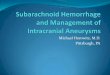
IIIrd cranial nerve palsy on a background of sudden-onseteadache is a clinical localizing sign and indicates pres-ure on the nerve, either directly by the aneurysm or byhe hematomas secondary to rupture of the aneurysm. Theneurysm itself can then be looked for the posterior wall ofhe ending of the internal carotid artery, close to the originf the posterior communicating artery (Fig. 3), or less com-only, developing at the origin of the superior cerebellar
the arterial circle at the base of the brain (B) on MIP reconstructionsorrhage (A): unenhanced hyperdensity in the subarachnoid spacesispheric fissure without flooding of the ventricles. Diagnosis of anhorns (star). Coexistent preretinal hemmorage (Terson Syndrome,eurysm (arrow head).
aralysis of the VIth cranial nerve are of no localizingalue.
Subarachnoid hemorrhage in ten questions 659
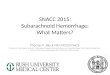
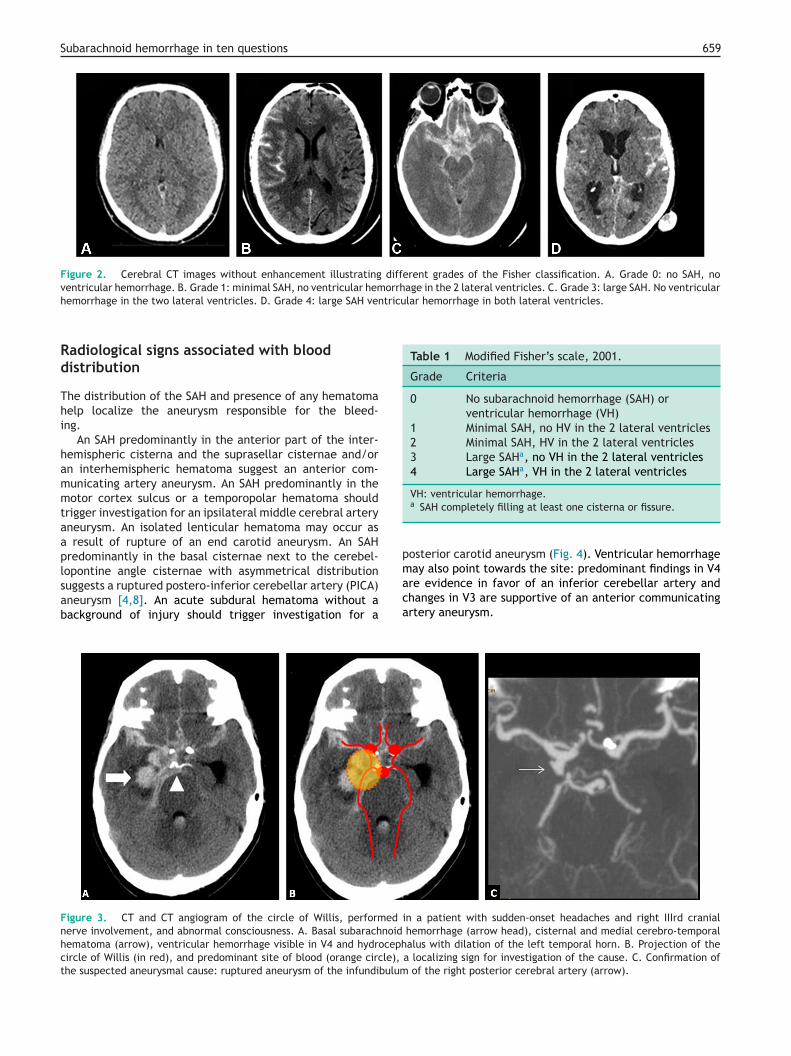
Figure 2. Cerebral CT images without enhancement illustrating different grades of the Fisher classification. A. Grade 0: no SAH, noventricular hemorrhage. B. Grade 1: minimal SAH, no ventricular hemorrhage in the 2 lateral ventricles. C. Grade 3: large SAH. No ventricular
tricular hemorrhage in both lateral ventricles.
Table 1 Modified Fisher’s scale, 2001.
Grade Criteria
0 No subarachnoid hemorrhage (SAH) orventricular hemorrhage (VH)
1 Minimal SAH, no HV in the 2 lateral ventricles2 Minimal SAH, HV in the 2 lateral ventricles3 Large SAHa, no VH in the 2 lateral ventricles4 Large SAHa, VH in the 2 lateral ventricles
VH: ventricular hemorrhage.
p
hemorrhage in the two lateral ventricles. D. Grade 4: large SAH ven
Radiological signs associated with blooddistribution
The distribution of the SAH and presence of any hematomahelp localize the aneurysm responsible for the bleed-ing.
An SAH predominantly in the anterior part of the inter-hemispheric cisterna and the suprasellar cisternae and/oran interhemispheric hematoma suggest an anterior com-municating artery aneurysm. An SAH predominantly in themotor cortex sulcus or a temporopolar hematoma shouldtrigger investigation for an ipsilateral middle cerebral arteryaneurysm. An isolated lenticular hematoma may occur asa result of rupture of an end carotid aneurysm. An SAHpredominantly in the basal cisternae next to the cerebel-
lopontine angle cisternae with asymmetrical distributionsuggests a ruptured postero-inferior cerebellar artery (PICA)aneurysm [4,8]. An acute subdural hematoma without abackground of injury should trigger investigation for amaca
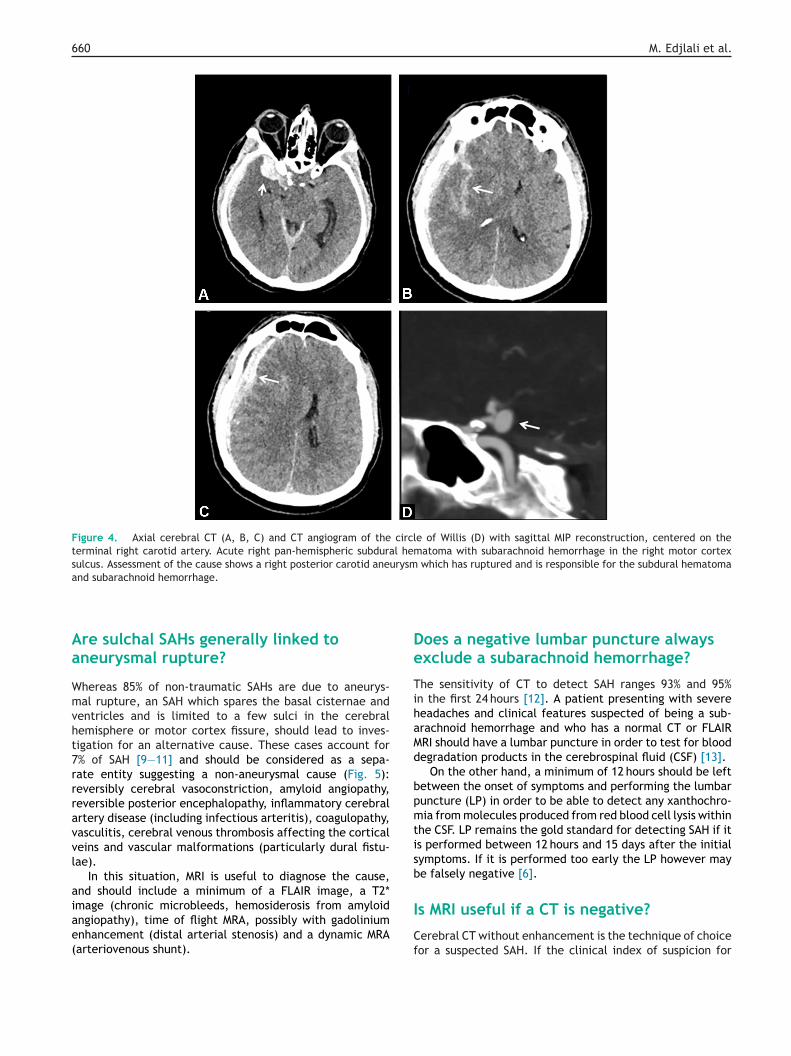
Figure 3. CT and CT angiogram of the circle of Willis, performed inerve involvement, and abnormal consciousness. A. Basal subarachnoid
hematoma (arrow), ventricular hemorrhage visible in V4 and hydrocephcircle of Willis (in red), and predominant site of blood (orange circle),
the suspected aneurysmal cause: ruptured aneurysm of the infundibulum
a SAH completely filling at least one cisterna or fissure.
osterior carotid aneurysm (Fig. 4). Ventricular hemorrhageay also point towards the site: predominant findings in V4
re evidence in favor of an inferior cerebellar artery andhanges in V3 are supportive of an anterior communicatingrtery aneurysm.
n a patient with sudden-onset headaches and right IIIrd cranialhemorrhage (arrow head), cisternal and medial cerebro-temporalalus with dilation of the left temporal horn. B. Projection of the
a localizing sign for investigation of the cause. C. Confirmation of of the right posterior cerebral artery (arrow).
660 M. Edjlali et al.
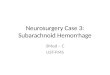
Figure 4. Axial cerebral CT (A, B, C) and CT angiogram of the circle of Willis (D) with sagittal MIP reconstruction, centered on theterminal right carotid artery. Acute right pan-hemispheric subdural hematoma with subarachnoid hemorrhage in the right motor cortexsulcus. Assessment of the cause shows a right posterior carotid aneurysm which has ruptured and is responsible for the subdural hematomaand subarachnoid hemorrhage.
Aa
Wmvht7rrravvl
aiae(
De
TihaMd
bpmtisb
Is MRI useful if a CT is negative?
re sulchal SAHs generally linked toneurysmal rupture?
hereas 85% of non-traumatic SAHs are due to aneurys-al rupture, an SAH which spares the basal cisternae and
entricles and is limited to a few sulci in the cerebralemisphere or motor cortex fissure, should lead to inves-igation for an alternative cause. These cases account for% of SAH [9—11] and should be considered as a sepa-ate entity suggesting a non-aneurysmal cause (Fig. 5):eversibly cerebral vasoconstriction, amyloid angiopathy,eversible posterior encephalopathy, inflammatory cerebralrtery disease (including infectious arteritis), coagulopathy,asculitis, cerebral venous thrombosis affecting the corticaleins and vascular malformations (particularly dural fistu-ae).
In this situation, MRI is useful to diagnose the cause,nd should include a minimum of a FLAIR image, a T2*mage (chronic microbleeds, hemosiderosis from amyloid
ngiopathy), time of flight MRA, possibly with gadoliniumnhancement (distal arterial stenosis) and a dynamic MRAarteriovenous shunt).Cf
oes a negative lumbar puncture alwaysxclude a subarachnoid hemorrhage?
he sensitivity of CT to detect SAH ranges 93% and 95%n the first 24 hours [12]. A patient presenting with severeeadaches and clinical features suspected of being a sub-rachnoid hemorrhage and who has a normal CT or FLAIRRI should have a lumbar puncture in order to test for bloodegradation products in the cerebrospinal fluid (CSF) [13].
On the other hand, a minimum of 12 hours should be leftetween the onset of symptoms and performing the lumbaruncture (LP) in order to be able to detect any xanthochro-ia from molecules produced from red blood cell lysis within
he CSF. LP remains the gold standard for detecting SAH if its performed between 12 hours and 15 days after the initialymptoms. If it is performed too early the LP however maye falsely negative [6].
erebral CT without enhancement is the technique of choiceor a suspected SAH. If the clinical index of suspicion for

Subarachnoid hemorrhage in ten questions 661
Figure 5. Causes of subarachnoid sulcal hemorrhage. Subarachnoid sulcal hemorrhages (A, orange box) are investigated by comparisonwith subarachnoid hemorrhages affecting the basal cisternae (A, white box), specific causes and other circle of Willis aneurysms. SulcalFLAIR hyperintensity showing subarachnoid hemorrhage (A). The different causes which may be looked for: a mycotic aneurysm (B), primary
metertinte
•
•
a•
•
Da
angiitis (C), or secondary angiitis in view of the irregularities in diaencephalopathy, in view of the bilateral parenchymal FLAIR hypecortical venous thrombosis (G).
an SAH is high when a CT is negative, it is recommendedthat:• a CT angiogram of the circle of Willis be performed in
order to investigate for an intracranial aneurysm;• a LP be performed;• a MRI may be indicated.
FLAIR imaging is more sensitive than CT to detect anSAH, particularly if it is small and carried out immediatelyafter the onset of headache, but particularly within the first48 hours [14,15]. The sensitivity of FLAIR in detecting SAHwithin 48 hours is 99%, dropping to 33% beyond 5 days. Onthe other hand, combining FLAIR with T2*-weighted imagingcan achieve a sensitivity of 99% in the first 15 days after theonset of symptoms. More recently, double inversion recov-ery (DAR) 3D sequences have detected SAH 15 days after theinitial symptoms [16].
Do all FLAIR hyperintensities in thesubarachnoid spaces represent blood?
A FLAIR hyperintensity in the subarachnoid spaces doesnot always represent blood. The other possible causes are(Fig. 6):
• intubated and ventilated patients: if oxygen saturation isclose to 100% a FLAIR hyperintensity may be seen in thecortical sulchi and basal cisternae [17];
• leptomeningeal disease (infectious or carcinomatousmeningitis): the rich cell content makes it impossible toachieve effective CSF saturation on FLAIR imaging;
aC9o[
r of the arterial branches, a Dural fistula (D), reversible posteriornsities, predominantly posterior (E), amyloid angiopathy (F) and
breach of the blood-brain barrier in ischemic disease ora reperfusion syndromes after treatment of tight carotidstenoses [18];gadolinium-chelate or iodinated contrast material injec-tion within 24 hours before the MRI [19]: diffuse FLAIRhyperintensities are due to contrast medium spreadinginto the cerebrospinal fluid.
Artefacts can also produce a hyperintensity in the sub-rachnoid spaces:CSF flow artefacts: 2D FLAIR images are sensitive to CSFpulsatility artefacts, showing hyperintensities on FLAIRimages usually located in the prepontine areas. Defectiveannulation of the fluid image is due to movement spins.Optimized 2D FLAIR images and particularly now, 3D FLAIRimages, can circumvent these artefacts [20,21];metal artefacts: artefacts present on both 2D and 3Dimages due to metal materials (dental materials, etc.)may cause hypertintensities on FLAIR images, particularlyin the posterior fossa. Although usually these artefacts donot raise any diagnostic problem, they may hinder inter-pretation as they mask important areas of cerebrospinalcirculation.
oes a normal CT angiogram (or MRIngiogram) exclude an intracranialneurysm?
T angiography of the circle of Willis has a sensitivity of8% to detect intracranial aneurysms, particularly becausef its excellent spatial resolution, which is less than 1 mm22—25].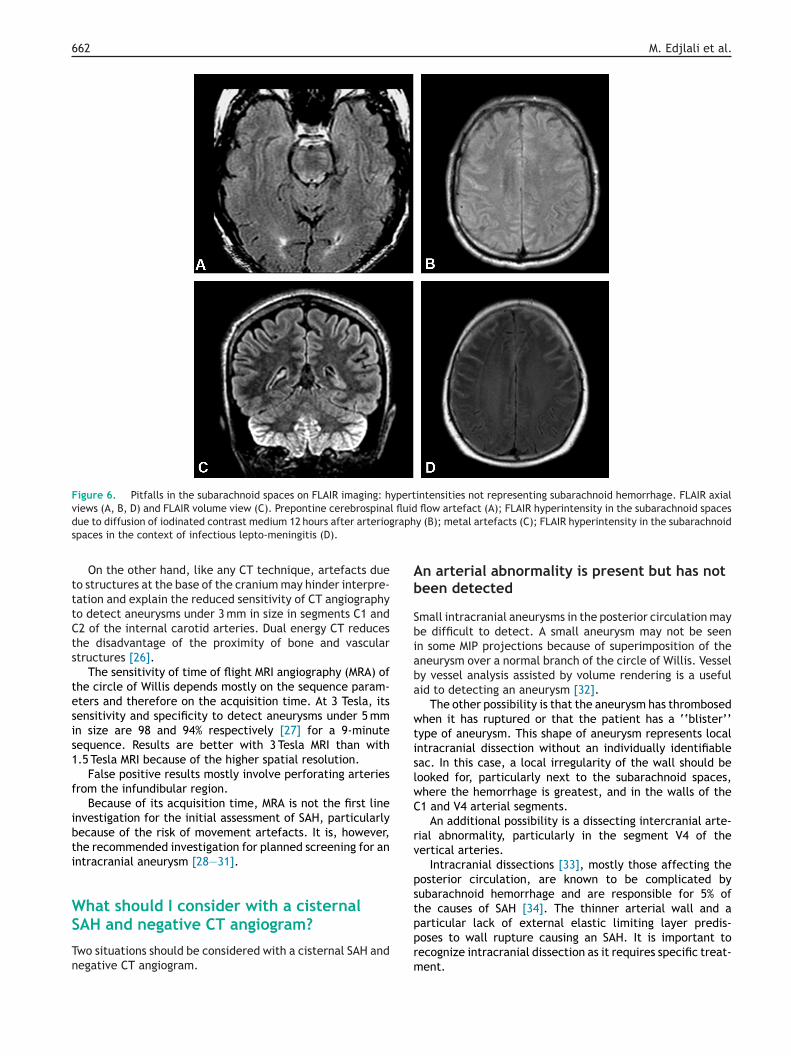
662 M. Edjlali et al.
Figure 6. Pitfalls in the subarachnoid spaces on FLAIR imaging: hypertintensities not representing subarachnoid hemorrhage. FLAIR axialviews (A, B, D) and FLAIR volume view (C). Prepontine cerebrospinal fluid flow artefact (A); FLAIR hyperintensity in the subarachnoid spacesd raphs
tttCts
tesis1
f
ibti
WS
Tn
Ab
Sbiaba
wtislwC
rv
pst
ue to diffusion of iodinated contrast medium 12 hours after arteriogpaces in the context of infectious lepto-meningitis (D).
On the other hand, like any CT technique, artefacts dueo structures at the base of the cranium may hinder interpre-ation and explain the reduced sensitivity of CT angiographyo detect aneurysms under 3 mm in size in segments C1 and2 of the internal carotid arteries. Dual energy CT reduceshe disadvantage of the proximity of bone and vasculartructures [26].
The sensitivity of time of flight MRI angiography (MRA) ofhe circle of Willis depends mostly on the sequence param-ters and therefore on the acquisition time. At 3 Tesla, itsensitivity and specificity to detect aneurysms under 5 mmn size are 98 and 94% respectively [27] for a 9-minuteequence. Results are better with 3 Tesla MRI than with.5 Tesla MRI because of the higher spatial resolution.
False positive results mostly involve perforating arteriesrom the infundibular region.
Because of its acquisition time, MRA is not the first linenvestigation for the initial assessment of SAH, particularlyecause of the risk of movement artefacts. It is, however,he recommended investigation for planned screening for anntracranial aneurysm [28—31].
hat should I consider with a cisternal
AH and negative CT angiogram?wo situations should be considered with a cisternal SAH andegative CT angiogram.
pprm
y (B); metal artefacts (C); FLAIR hyperintensity in the subarachnoid
n arterial abnormality is present but has noteen detected
mall intracranial aneurysms in the posterior circulation maye difficult to detect. A small aneurysm may not be seenn some MIP projections because of superimposition of theneurysm over a normal branch of the circle of Willis. Vessely vessel analysis assisted by volume rendering is a usefulid to detecting an aneurysm [32].
The other possibility is that the aneurysm has thrombosedhen it has ruptured or that the patient has a ‘‘blister’’
ype of aneurysm. This shape of aneurysm represents localntracranial dissection without an individually identifiableac. In this case, a local irregularity of the wall should beooked for, particularly next to the subarachnoid spaces,here the hemorrhage is greatest, and in the walls of the1 and V4 arterial segments.
An additional possibility is a dissecting intercranial arte-ial abnormality, particularly in the segment V4 of theertical arteries.
Intracranial dissections [33], mostly those affecting theosterior circulation, are known to be complicated byubarachnoid hemorrhage and are responsible for 5% ofhe causes of SAH [34]. The thinner arterial wall and a
articular lack of external elastic limiting layer predis-oses to wall rupture causing an SAH. It is important toecognize intracranial dissection as it requires specific treat-ent.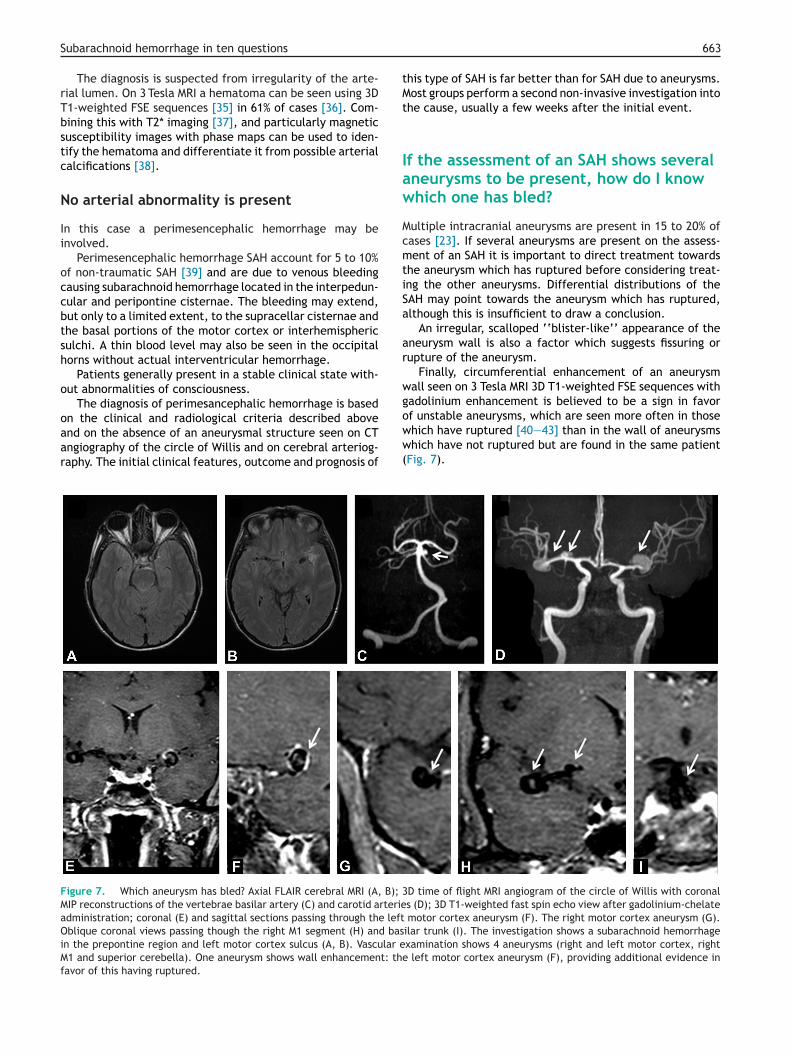
tMt
Iaw
McmtiSa
ar
wg
Subarachnoid hemorrhage in ten questions
The diagnosis is suspected from irregularity of the arte-rial lumen. On 3 Tesla MRI a hematoma can be seen using 3DT1-weighted FSE sequences [35] in 61% of cases [36]. Com-bining this with T2* imaging [37], and particularly magneticsusceptibility images with phase maps can be used to iden-tify the hematoma and differentiate it from possible arterialcalcifications [38].
No arterial abnormality is present
In this case a perimesencephalic hemorrhage may beinvolved.
Perimesencephalic hemorrhage SAH account for 5 to 10%of non-traumatic SAH [39] and are due to venous bleedingcausing subarachnoid hemorrhage located in the interpedun-cular and peripontine cisternae. The bleeding may extend,but only to a limited extent, to the supracellar cisternae andthe basal portions of the motor cortex or interhemisphericsulchi. A thin blood level may also be seen in the occipitalhorns without actual interventricular hemorrhage.
Patients generally present in a stable clinical state with-out abnormalities of consciousness.
The diagnosis of perimesancephalic hemorrhage is based
on the clinical and radiological criteria described aboveand on the absence of an aneurysmal structure seen on CTangiography of the circle of Willis and on cerebral arteriog-raphy. The initial clinical features, outcome and prognosis ofoww(
Figure 7. Which aneurysm has bled? Axial FLAIR cerebral MRI (A, B); 3MIP reconstructions of the vertebrae basilar artery (C) and carotid arterieadministration; coronal (E) and sagittal sections passing through the leftOblique coronal views passing though the right M1 segment (H) and basin the prepontine region and left motor cortex sulcus (A, B). Vascular eM1 and superior cerebella). One aneurysm shows wall enhancement: thefavor of this having ruptured.
663
his type of SAH is far better than for SAH due to aneurysms.ost groups perform a second non-invasive investigation into
he cause, usually a few weeks after the initial event.
f the assessment of an SAH shows severalneurysms to be present, how do I knowhich one has bled?
ultiple intracranial aneurysms are present in 15 to 20% ofases [23]. If several aneurysms are present on the assess-ent of an SAH it is important to direct treatment towards
he aneurysm which has ruptured before considering treat-ng the other aneurysms. Differential distributions of theAH may point towards the aneurysm which has ruptured,lthough this is insufficient to draw a conclusion.
An irregular, scalloped ‘‘blister-like’’ appearance of theneurysm wall is also a factor which suggests fissuring orupture of the aneurysm.
Finally, circumferential enhancement of an aneurysmall seen on 3 Tesla MRI 3D T1-weighted FSE sequences withadolinium enhancement is believed to be a sign in favor
f unstable aneurysms, which are seen more often in thosehich have ruptured [40—43] than in the wall of aneurysmshich have not ruptured but are found in the same patientFig. 7).
D time of flight MRI angiogram of the circle of Willis with coronals (D); 3D T1-weighted fast spin echo view after gadolinium-chelate
motor cortex aneurysm (F). The right motor cortex aneurysm (G).ilar trunk (I). The investigation shows a subarachnoid hemorrhagexamination shows 4 aneurysms (right and left motor cortex, right
left motor cortex aneurysm (F), providing additional evidence in
6 M. Edjlali et al.
Wcw
Wudtb
t
oit
aaic
C
Ahnot
Q
A
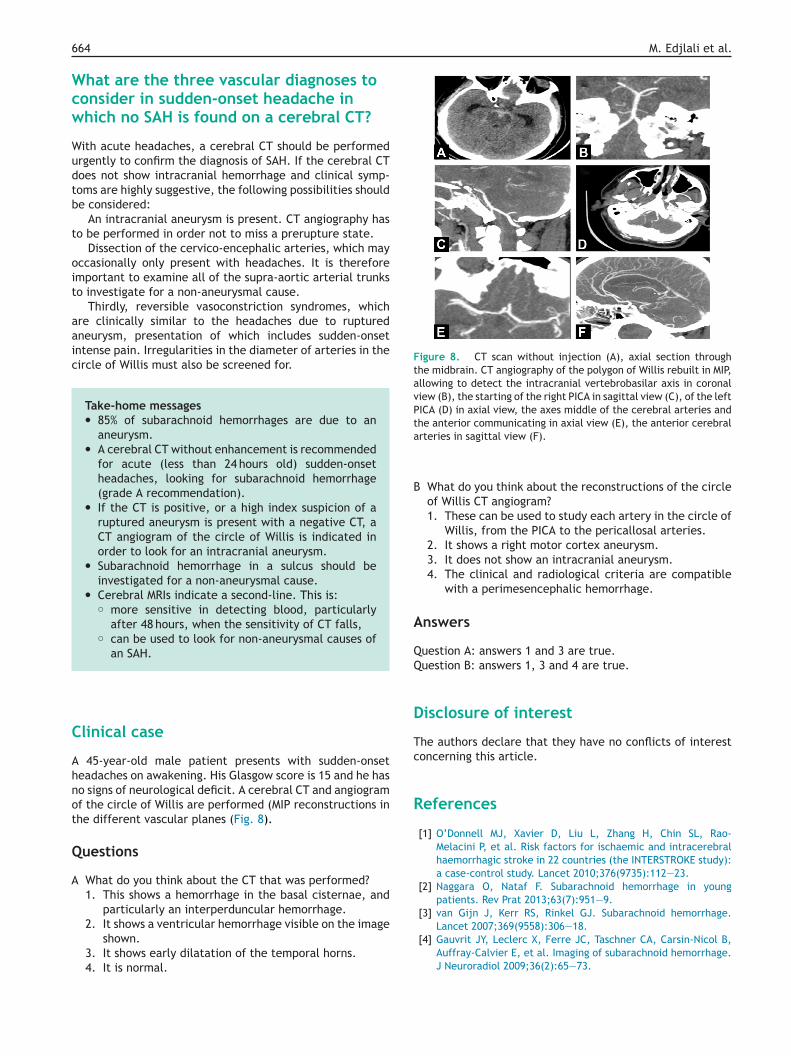
Figure 8. CT scan without injection (A), axial section throughthe midbrain. CT angiography of the polygon of Willis rebuilt in MIP,allowing to detect the intracranial vertebrobasilar axis in coronalview (B), the starting of the right PICA in sagittal view (C), of the leftPICA (D) in axial view, the axes middle of the cerebral arteries andthe anterior communicating in axial view (E), the anterior cerebrala
B
A
D
Tc
R
64
hat are the three vascular diagnoses toonsider in sudden-onset headache inhich no SAH is found on a cerebral CT?
ith acute headaches, a cerebral CT should be performedrgently to confirm the diagnosis of SAH. If the cerebral CToes not show intracranial hemorrhage and clinical symp-oms are highly suggestive, the following possibilities shoulde considered:
An intracranial aneurysm is present. CT angiography haso be performed in order not to miss a prerupture state.
Dissection of the cervico-encephalic arteries, which mayccasionally only present with headaches. It is thereforemportant to examine all of the supra-aortic arterial trunkso investigate for a non-aneurysmal cause.
Thirdly, reversible vasoconstriction syndromes, whichre clinically similar to the headaches due to rupturedneurysm, presentation of which includes sudden-onsetntense pain. Irregularities in the diameter of arteries in theircle of Willis must also be screened for.
Take-home messages• 85% of subarachnoid hemorrhages are due to an
aneurysm.• A cerebral CT without enhancement is recommended
for acute (less than 24 hours old) sudden-onsetheadaches, looking for subarachnoid hemorrhage(grade A recommendation).
• If the CT is positive, or a high index suspicion of aruptured aneurysm is present with a negative CT, aCT angiogram of the circle of Willis is indicated inorder to look for an intracranial aneurysm.
• Subarachnoid hemorrhage in a sulcus should beinvestigated for a non-aneurysmal cause.
• Cerebral MRIs indicate a second-line. This is:◦ more sensitive in detecting blood, particularly
after 48 hours, when the sensitivity of CT falls,◦ can be used to look for non-aneurysmal causes of
an SAH.
linical case
45-year-old male patient presents with sudden-onseteadaches on awakening. His Glasgow score is 15 and he haso signs of neurological deficit. A cerebral CT and angiogramf the circle of Willis are performed (MIP reconstructions inhe different vascular planes (Fig. 8).
uestions
What do you think about the CT that was performed?1. This shows a hemorrhage in the basal cisternae, and
particularly an interperduncular hemorrhage.
2. It shows a ventricular hemorrhage visible on the imageshown.3. It shows early dilatation of the temporal horns.4. It is normal.
rteries in sagittal view (F).
What do you think about the reconstructions of the circleof Willis CT angiogram?1. These can be used to study each artery in the circle of
Willis, from the PICA to the pericallosal arteries.2. It shows a right motor cortex aneurysm.3. It does not show an intracranial aneurysm.4. The clinical and radiological criteria are compatible
with a perimesencephalic hemorrhage.
nswers
uestion A: answers 1 and 3 are true.uestion B: answers 1, 3 and 4 are true.
isclosure of interest
he authors declare that they have no conflicts of interestoncerning this article.
eferences
[1] O’Donnell MJ, Xavier D, Liu L, Zhang H, Chin SL, Rao-Melacini P, et al. Risk factors for ischaemic and intracerebralhaemorrhagic stroke in 22 countries (the INTERSTROKE study):a case-control study. Lancet 2010;376(9735):112—23.
[2] Naggara O, Nataf F. Subarachnoid hemorrhage in youngpatients. Rev Prat 2013;63(7):951—9.
[3] van Gijn J, Kerr RS, Rinkel GJ. Subarachnoid hemorrhage.
Lancet 2007;369(9558):306—18.[4] Gauvrit JY, Leclerc X, Ferre JC, Taschner CA, Carsin-Nicol B,Auffray-Calvier E, et al. Imaging of subarachnoid hemorrhage.J Neuroradiol 2009;36(2):65—73.
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
Subarachnoid hemorrhage in ten questions
[5] Boesiger BM, Shiber JR. Subarachnoid hemorrhage diagno-sis by computed tomography and lumbar puncture: are fifthgeneration CT scanners better at identifying subarachnoidhemorrhage? J Emerg Med 2005;29(1):23—7.
[6] van Gijn J, Rinkel GJ. Subarachnoid haemorrhage: diagnosis,causes and management. Brain 2001;124(Pt 2):249—78.
[7] Claassen J, Bernardini GL, Kreiter K, Bates J, Du YE, CopelandD, et al. Effect of cisternal and ventricular blood on risk ofdelayed cerebral ischemia after subarachnoid hemorrhage: theFisher scale revisited. Stroke 2001;32(9):2012—20.
[8] Pierot L, Boulin A, Castaings L, Rey A, Moret J. The endovas-cular approach in the management of patients with multipleintracranial aneurysms. Neuroradiology 1997;39(5):361—6.
[9] Brunot S, Fromont A, Ricolfi F, Moreau T, Giroud M. [Focalsubarachnoid hemorrhage and cerebral amyloid angiopathy:a non-fortuitous association]. Rev Neurol (Paris) 2010;166(1):83—9.
[10] Cuvinciuc V, Viguier A, Bonneville F. Cerebral amyloid angiopa-thy: a forgotten cause of sub-arachnoid hemorrhage. JNeuroradiol 2009;36(4):245—6.
[11] Spitzer C, Mull M, Rohde V, Kosinski CM. Non-traumatic corticalsubarachnoid haemorrhage: diagnostic work-up and aetiolog-ical background. Neuroradiology 2005;47(7):525—31.
[12] Evans RW. Diagnostic testing for the evaluation of headaches.Neurol Clin 1996;14(1):1—26.
[13] Beetham R, Fahie-Wilson MN, Park D. What is the role of CSFspectrophotometry in the diagnosis of subarachnoid haemor-rhage? Ann Clin Biochem 1998;35(Pt 1):1—4.
[14] da Rocha AJ, da Silva CJ, Gama HP, Baccin CE, BragaFT, Cesare Fde A, et al. Comparison of magnetic reso-nance imaging sequences with computed tomography todetect low-grade subarachnoid hemorrhage: Role of fluid-attenuated inversion recovery sequence. J Comput AssistTomogr 2006;30(2):295—303.
[15] Mohamed M, Heasly DC, Yagmurlu B, Yousem DM. Fluid-attenuated inversion recovery MR imaging and subarachnoidhemorrhage: not a panacea. AJNR Am J Neuroradiol2004;25(4):545—50.
[16] Hodel J, Aboukais R, Dutouquet B, Kalsoum E, Benadjaoud MA,Chechin D, et al. Double inversion recovery MR sequence forthe detection of subacute subarachnoid hemorrhage. AJNR AmJ Neuroradiol 2015;36(2):251—8.
[17] Deliganis AV, Fisher DJ, Lam AM, Maravilla KR. Cerebrospinalfluid signal intensity increase on FLAIR MR images in patientsunder general anesthesia: the role of supplemental O2. Radi-ology 2001;218(1):152—6.
[18] Dechambre SD, Duprez T, Grandin CB, Lecouvet FE, PeetersA, Cosnard G. High signal in cerebrospinal fluid mimick-ing subarachnoid haemorrhage on FLAIR following acutestroke and intravenous contrast medium. Neuroradiology2000;42(8):608—11.
[19] Morris JM, Miller GM. Increased signal in the subarachnoid spaceon fluid-attenuated inversion recovery imaging associatedwith the clearance dynamics of gadolinium chelate: a poten-tial diagnostic pitfall. AJNR Am J Neuroradiol 2007;28(10):1964—7.
[20] Lummel N, Schoepf V, Burke M, Brueckmann H, Linn J. 3D fluid-attenuated inversion recovery imaging: reduced CSF artifactsand enhanced sensitivity and specificity for subarachnoid hem-orrhage. AJNR Am J Neuroradiol 2011;32(11):2054—60.
[21] Naganawa S. The technical and clinical features of 3D-FLAIR inneuroimaging. Magn Reson Med Sci 2015;14(2):93—106.
[22] Papke K, Kuhl CK, Fruth M, Haupt C, Schlunz-Hendann M,Sauner D, et al. Intracranial aneurysms: role of multidetectorCT angiography in diagnosis and endovascular therapy plan-
ning. Radiology 2007;244(2):532—40.[23] Pozzi-Mucelli F, Bruni S, Doddi M, Calgaro A, Braini M,Cova M. Detection of intracranial aneurysms with 64 channel
665
multidetector row computed tomography: comparison withdigital subtraction angiography. Eur J Radiol 2007;64(1):15—26.
24] Taschner CA, Thines L, Lernout M, Lejeune JP, Leclerc X. Treat-ment decision in ruptured intracranial aneurysms: comparisonbetween multi-detector row CT angiography and digital sub-traction angiography. J Neuroradiol 2007;34(4):243—9.
25] Westerlaan HE, van Dijk JM, Jansen-van der Weide MC, de GrootJC, Groen RJ, Mooij JJ, et al. Intracranial aneurysms in patientswith subarachnoid hemorrhage: CT angiography as a primaryexamination tool for diagnosis — systematic review and meta-analysis. Radiology 2011;258(1):134—45.
26] Postma AA, Das M, Stadler AA, Wildberger JE. Dual-energyCT: what the neuroradiologist should know. Curr Radiol Rep2015;3(5):16.
27] Li MH, Li YD, Gu BX, Cheng YS, Wang W, Tan HQ, et al. Accuratediagnosis of small cerebral aneurysms ≤ 5 mm in diameter with3.0-T MR angiography. Radiology 2014;271(2):553—60.
28] Adams WM, Laitt RD, Jackson A. The role of MR angiography inthe pretreatment assessment of intracranial aneurysms: a com-parative study. AJNR Am J Neuroradiol 2000;21(9):1618—28.
29] Ferre JC, Carsin-Nicol B, Morandi X, Carsin M, de Kersaint-GillyA, Gauvrit JY, et al. Time-of-flight MR angiography at 3 T ver-sus digital subtraction angiography in the imaging follow-upof 51 intracranial aneurysms treated with coils. Eur J Radiol2009;72(3):365—9.
30] Rodriguez-Regent C, Edjlali-Goujon M, Trystram D, BoulouisG, Ben Hassen W, Godon-Hardy S, et al. Non-invasivediagnosis of intracranial aneurysms. Diagn Interv Imaging2014;95(12):1163—74.
31] Sailer AM, Wagemans BA, Nelemans PJ, de Graaf R,van Zwam WH. Diagnosing intracranial aneurysms with MRangiography: systematic review and meta-analysis. Stroke2014;45(1):119—26.
32] Li H, Yan L, Li MH, Li YD, Tan HQ, Gu BX, et al. Evaluationof intracranial aneurysms with high-resolution MR angiographyusing single-artery highlighting technique: correlation with dig-ital subtraction angiography. Radiol Med 2013;118(8):1379—87.
33] Debette S, Compter A, Labeyrie MA, Uyttenboogaart M, MetsoTM, Majersik JJ, et al. Epidemiology, pathophysiology, diagno-sis, and management of intracranial artery dissection. LancetNeurol 2015;14(6):640—54.
34] Sasaki O, Ogawa H, Koike T, Koizumi T, Tanaka R. A clinico-pathological study of dissecting aneurysms of the intracranialvertebral artery. J Neurosurg 1991;75(6):874—82.
35] Edjlali M, Roca P, Rabrait C, Naggara O, Oppenheim C. 3Dfast spin-echo T1 black-blood imaging for the diagnosis of cer-vical artery dissection. AJNR Am J Neuroradiol 2012;34(9):E103—6.
36] Wang Y, Lou X, Li Y, Sui B, Sun S, Li C, et al. Imaginginvestigation of intracranial arterial dissecting aneurysms byusing 3 T high-resolution MRI and DSA: from the interventionalneuroradiologists’ view. Acta Neurochir (Wien) 2014;156(3):515—25.
37] Naggara O, Oppenheim C, Louillet F, Touze E, Mas JL, LeclercX, et al. Traumatic intracranial dissection: mural hematoma onhigh-resolution MRI. J Neuroradiol 2010;37(2):136—7.
38] Kim TW, Choi HS, Koo J, Jung SL, Ahn KJ, Kim BS, et al. Intra-mural hematoma detection by susceptibility-weighted imagingin intracranial vertebral artery dissection. Cerebrovasc Dis2013;36(4):292—8.
39] Flaherty ML, Haverbusch M, Kissela B, Kleindorfer D, SchneiderA, Sekar P, et al. Perimesencephalic subarachnoid hemorrhage:incidence, risk factors, and outcome. J Stroke Cerebrovasc Dis2005;14(6):267—71.
40] Edjlali M, Gentric JC, Regent-Rodriguez C, Trystram D, Hassen
WB, Lion S, et al. Does aneurysmal wall enhancement on vesselwall MRI help to distinguish stable from unstable intracranialaneurysms? Stroke 2014;45(12):3704—6.
6
[
[
[Regent C, Nataf F, et al. Advanced technologies applied
66
41] Matouk CC, Mandell DM, Gunel M, Bulsara KR, Malhotra A,Hebert R, et al. Vessel wall magnetic resonance imaging iden-tifies the site of rupture in patients with multiple intracranialaneurysms: proof of principle. Neurosurgery 2013;72(3):492—6[discussion 6].
42] Nagahata S, Nagahata M, Obara M, Kondo R, MinagawaN, Sato S, et al. Wall enhancement of the intracranialaneurysms revealed by magnetic resonance vessel wall imag-ing using three-dimensional turbo spin-echo sequence with
M. Edjlali et al.
motion-sensitized driven-equilibrium: a sign of rupturedaneurysm? Clin Neuroradiol 2014, http://dx.doi.org/10.1007/s00062-014-0353-z.
43] Edjlali M, Roca P, Gentric JC, Trystram D, Rodriguez-
to physiopathological analysis of central nervous systemaneurysms and vascular malformations. Diagn Interv Imaging2014;95(12):1187—93.