Embed Size (px)
Citation preview

1507
Perimesencephalic Subarachnoid HemorrhageAdditional Perspectives From Four Cases
Wouter I. Schievink, MD; Eelco F.M. Wijdicks, MD; David G. Piepgras, MD;Douglas A. Nichols, MD; Michael J. Ebersold, MD
Background Nonaneurysmal perimesencephalic hemor-rhage, a distinct form of subarachnoid hemorrhage, is arecently described variant of intracranial hemorrhage. Wedescribe two patients who presented with unusual features ofthis type of subarachnoid hemorrhage and also two patientswho had a perimesencephalic pattern of hemorrhage due to aruptured posterior circulation aneurysm.
Case Descriptions The first patient, a 41-year-old womanwith perimesencephalic hemorrhage, underwent an explor-atory craniotomy because angiography had suggested ananomaly of the basilar tip. No source of hemorrhage could beidentified at the time of surgery. The second patient was a3-year-old boy who presented with opisthotonos and who wasfound to have a perimesencephalic hemorrhage. Angiographyrevealed no source for the hemorrhage. The third patient, a54-year-old man, had a perimesencephalic pattern of sub-arachnoid hemorrhage from a vertebrobasilar junction aneu-
In approximately 15% of patients with spontaneoussubarachnoid hemorrhage (SAH) the cause of thehemorrhage cannot be detected despite detailed
imaging studies.14 It has repeatedly been shown thatSAH of unknown origin is associated with a much betteroutcome than aneurysmal SAH, although recurrentbleeding and delayed cerebral ischemia do occur.15
Recently, van Gijn and colleagues58 described a benignvariant of SAH, the so-called perimesencephalic non-aneurysmal hemorrhage. This type of SAH is charac-terized radiographically by a pattern of hemorrhagerestricted to the perimesencephalic or prepontine cis-terns in combination with a normal angiogram andclinically by an invariably excellent prognosis.23-5"Since its original description, it has subsequently beenshown that the good prognosis of SAH of unknownetiology can be largely explained by the high prevalenceof perimesencephalic nonaneurysmal hemorrhage inseries of patients with SAH and a negative angiogram.5
Thus, when perimesencephalic-type hemorrhages areexcluded from series of patients with SAH and anegative angiogram, outcome is much less favorable.Despite the increasing number of reports of series ofpatients with nonaneurysmal perimesencephalic hemor-
Received February 3, 1994; final revision received April 12,1994; accepted April 12, 1994.
From the Departments of Neurologic Surgery (W.I.S., D.G.P.,M.J.E.), Neurology (E.F.M.W.), and Diagnostic Radiology(D.A.N.), Mayo Clinic, Rochester, Minn.
Correspondence to Dr Wouter I. Schievink, Department ofNeurologic Surgery, Mayo Clinic, 200 First St SW, Rochester, MN55905.
© 1994 American Heart Association, Inc.
rysm associated with a fenestration that was missed on theinitial angiographic study. The fourth patient, a 43-year-oldman, suffered a perimesencephalic pattern of subarachnoidhemorrhage from a small posterior cerebral artery aneurysm,which had not been recognized on two angiograms.
Conclusions These patients elaborate on the clinical spec-trum of subarachnoid hemorrhage with a perimesencephalicpattern. First, a negative exploratory craniotomy suggests thatthe source of nonaneurysmal perimesencephalic hemorrhagemay not be arterial. Second, nonaneurysmal perimesence-phalic hemorrhage may also occur in children. Finally, theindex of suspicion for a posterior circulation aneurysm shouldremain high in patients who present with a perimesencephalicpattern of subarachnoid hemorrhage, and these aneurysmsmay rise from unusual locations. (Stroke. 1994^5:1507-1511.)
Key Words • angiography • subarachnoid hemorrhage •cerebral aneurysm
Triage,2-3-5"11 many uncertainties remain regarding thisdistinct type of SAH, especially relating to their etiol-ogy and evaluation. In this communication we describefour patients who manifest some unusual aspects ofperimesencephalic SAH. Two patients had a nonaneu-rysmal perimesencephalic hemorrhage, and two had aperimesencephalic hemorrhage due to a ruptured pos-terior circulation aneurysm.
Case ReportsPatient 1
A 41-year-old woman developed the acute onset of asevere headache associated with nausea and vomiting.A computed tomography (CT) scan, obtained 2 hoursafter the ictus, showed an SAH limited to the interpe-duncular and prepontine cisterns with minimal exten-sion into both sylvian fissures. She was transferred toour institution.
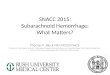
On admission, examination only showed moderatenuchal rigidity. Four-vessel cerebral angiographyshowed a small domelike dilatation of the basilar tip butwas otherwise normal (Fig 1). Magnetic resonanceimaging (MRI) only showed residual blood in theinterpeduncular cistern. Angiography was repeated 7days later and was unchanged. Subsequently, through aright frontotemporal craniotomy, the upper basilar ar-tery was explored, and a small bulbous dilatation wasidentified posteriorly at the basilar tip. There was noevidence that this dilatation had ever ruptured orleaked, and no other suspicious areas could be identi-fied. The patient recovered well from her surgery andhas remained asymptomatic during 1 year of follow-up.
by guest on April 17, 2018
http://stroke.ahajournals.org/D
ownloaded from

1508 Stroke Vol 25, No 7 July 1994
FIG 1. Patient 1. Left vertebral angiogram (anteroposteriorprojection), obtained 24 hours after the ictus, reveals a smalldomelike protuberance of the basilar tip.
Patient 2A 3-year-old white boy developed the acute onset of
a severe headache accompanied by nausea and vomit-ing. Twenty-four hours later marked neck stiffness wasnoted by his parents. Lumbar puncture revealed grosslyhemorrhagic cerebrospinal fluid, and examination ofthe supernatant revealed xanthochromia. He was trans-ferred to our institution.
The patient was a product of an uncomplicated full-term pregnancy. There was no history of trauma orevidence of child abuse.
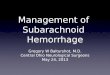
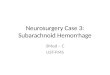
On admission, examination was remarkable only formarked nuchal rigidity and opisthotonos. Laboratoryexaminations, including complete blood count, serumelectrolytes, liver function tests, coagulation studies,and drug screen, were all within normal limits. Reviewof the outside CT scan revealed a localized hemorrhagewithin the suprasellar and prepontine cisterns (Fig 2).MRI revealed the area of acute hemorrhage within theprepontine cistern extending rostrally into the interpe-duncular and suprasellar cisterns, separate from thebasilar artery (Fig 3). Four-vessel cerebral angiographyonly revealed narrowing of the basilar artery, consistentwith vasospasm secondary to the SAH. An MRI exam-ination of the entire spine was normal. A secondfour-vessel cerebral angiogram 10 days later was nor-mal, with resolution of the vasospasm. Neuropsycholog-
FIG 2. Patient 2. Axial computed tomographic scan, obtained36 hours after the ictus, reveals a hemorrhage in the suprasellarcistern.
ical evaluation was normal. The patient was dischargedhome in excellent condition 2 weeks after admission.
The patient has continued to do well during 10months of follow-up. A second MRI of the head withgadolinium administration was unremarkable (Fig 3).
Patient 3This 54-year-old man developed a sudden severe
headache associated with nausea and vomiting. CT
FIG 3. Patient 2. Sagittal T,-weighted magnetic resonanceimaging. The image on the left, obtained 4 days after the ictus,reveals an area of hemorrhage within the prepontine, interpe-duncular, and suprasellar cisterns. The image on the right,obtained 3 months later, reveals resolution of the hemorrhage.
by guest on April 17, 2018
http://stroke.ahajournals.org/D
ownloaded from

Schievink et al Perimesencephalic Hemorrhage 1509
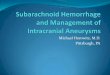
FIG 4. Patient 3. Axial computed tomographic scan, obtained 6hours after the ictus, reveals a subarachnoid hemorrhage limitedto the interpeduncular and right ambient cisterns. The leaves ofthe tentorium may be more dense than normal, Indicating thepresence of a thin layer of subarachnoid blood.
examination showed a localized hemorrhage in theprepontine and interpeduncular cisterns with no exten-sion into the frontal interhemispheric or sylvian fissures(Fig 4). No intraventricular or parenchymal hemorrhagewas noted. The patient was transferred to ourinstitution.
Examination was remarkable only for moderatenuchal rigidity. A four-vessel cerebral angiogram wasinterpreted as normal (Fig 5 A). MRI examination of thecervical spine was normal. One week later, a secondangiography revealed a 3-mm aneurysm rising betweentwo limbs of a fenestration of the proximal basilar trunk(Fig 5B). In retrospect, the aneurysm was present onthe initial study. The aneurysm was successfully treatedwith a single Guglielmi detachable coil measuring 3mmx4 cm.
Patient 4This 43-year-old man suddenly developed a severe
headache after an orgasm. CT examination, performed3 hours after the onset of symptoms, showed an SAFfcentered within the right ambient cistern with no exten-sion into the frontal interhemispheric or sylvian fissures(Fig 6). No intraventricular or parenchymal hemorrhagewas seen. Two cerebral angiograms were reported asnormal. The patient was transferred to our institution.
Examination showed mild nuchal rigidity only. Onreview of the angiograms, a 2-mm right posterior cere-bral artery aneurysm (P2 segment) was noted (Fig 7).Through a right frontotemporal craniotomy a very
FIG 5. Patient 3. A, Left vertebral angiogram (anteroposterior view), obtained 24 hours after the ictus, was interpreted as normal. B, Leftvertebral angiogram (anteroposterior view), obtained 1 week later, shows a 3-mm aneurysm rising between the two limbs of afenestration of the proximal basilar trunk.
by guest on April 17, 2018
http://stroke.ahajournals.org/D
ownloaded from

1510 Stroke Vol 25, No 7 July 1994
FIG 6. Patient 4. Axial computed tomographic scan, obtained 3hours after the ictus, reveals blood in the right ambient andinterpeduncular cisterns.
thin-walled aneurysm was encountered, which rose atthe P2 segment along with the origin of a circummes-encephalic branch. There was clear evidence of recentrupture, and the aneurysm was clipped. The patientrecovered well from his surgery and has not had recur-rent problems.
DiscussionNonaneurysmal perimesencephalic hemorrhage has
become well recognized as a distinct type of SAH2-3-5"11
and may account for up to two thirds of all SAHs ofunknown cause.3-5 Patients with a typical clinical pictureof perimesencephalic SAH are adults with the acuteonset of headache without loss of consciousness or focalneurological symptoms.2J-511 Neurological examinationis normal, and often only meningeal irritation isfound.2-3-5-11 The clinical course is without secondarydeterioration from delayed cerebral ischemia or recur-rent bleeding, and the long-term prognosis is invariablyexcellent.2-3-5-11 Perimesencephalic SAH is diagnosed onthe basis of CT or MRI examination, which demon-strates a localized area of hemorrhage centered withinthe perimesencephalic or prepontine cisterns withoutintracerebral or intraventricular extension.57 After theterm "perimesencephalic hemorrhage" was coined in1985,6 it has become apparent that a number of thesehemorrhages are centered around the prepontine cis-tern and that some also extend into the suprasellarcistern.7 With the advent of MRI, blood may also bedemonstrated anterior to the medulla oblongata.7
Angiography in perimesencephalic hemorrhagerarely reveals an intracranial aneurysm or other sourceof bleeding.57 However, full cerebral angiography re-mains mandatory in all patients with perimesencephalic
FIG 7. Patient 4. Right vertebral angiogram (anteroposteriorview), obtained 12 hours after the ictus, shows a 2-mm aneu-rysm (arrowhead) of the right posterior cerebral artery (P2segment).
SAH because a ruptured basilar artery aneurysm mayproduce a similar pattern of hemorrhage on imagingstudies.7 Repeated angiography after a negative studyhas not demonstrated an aneurysm or other source ofhemorrhage in previously reported series2-3-5"11 but spo-radically has resulted in cerebral infarction.4-5 There-fore, it has been suggested that it is reasonable to limitangiography to a single examination.5-6-12-13 However, in2% to 16% of patients with a pattern of perimesence-phalic hemorrhage, a posterior circulation aneurysm isfound.5-7101114 Furthermore, it is well known that angi-ography may not demonstrate a ruptured aneurysm inall cases of aneurysmal SAH on the initial examination.The posterior circulation aneurysms in our patients 3and 4 were difficult to recognize on the initial angio-grams. This failure to identify a posterior circulationaneurysm highlights the concerns in clinical practicewhen a patient with a perimesencephalic pattern ofSAH is encountered. Possibly, physicians who recognizea perimesencephalic pattern of SAH on CT may biastheir expectations for a negative angiogram. Althoughour case material does not support a second angio-graphic study in patients with perimesencephalic hem-orrhage, it does underscore the need for a high index ofsuspicion for a ruptured aneurysm of the posteriorcirculation. Moreover, a perimesencephalic pattern ofSAH may be caused not only by a ruptured aneurysm ofthe basilar top but also by those in more unusual
by guest on April 17, 2018
http://stroke.ahajournals.org/D
ownloaded from

Schievink et al Perimesencephalic Hemorrhage 1511
locations, such as the distal posterior cerebral artery orvertebrobasilar artery junction.
Nonaneurysmal perimesencephalic hemorrhage hasnot been described in childhood or adolescence. Theyoungest reported patient with nonaneurysmal perimes-encephalic hemon-hage was 22 years.7 The clinical andradiographic characteristics of our 3-year-old patientwith SAH were consistent with nonaneurysmal peri-mesencephalic hemorrhage. Other causes of SAH inthis age group,1516 eg, arteriovenous malformation, an-eurysm, blood dyscrasia, brain tumor, intracranial arte-rial dissection, sickle cell disease, or structural spinaldisorders, were excluded in our patient. Battery couldpossibly have created a similar pattern of hemorrhage,but there was no evidence of child abuse in our patient.Moreover, isolated SAH in the absence of retinalhemorrhages or subdural hematoma is rare in thebattered child syndrome. Furthermore, if SAH due tobattery is identified it is often in the interhemisphericfissure.17 Recognition of nonaneurysmal perimesence-phalic hemorrhage is important in the pediatric as wellas the adult population, especially in view of its benignnature. Restrictions of activities or other adjustments inlifestyle do not need to be instituted in patients withnonaneurysmal perimesencephalic SAH,5-12 certainly apertinent point for an active young child. Whether thelong-term clinical course in children is as favorable asthat in adults, however, remains to be determined, butthere are no compelling arguments to believe otherwise.
The clinical entity of nonaneurysmal perimesence-phalic hemorrhage has not been defined by a patholog-ical substrate, but a venous or capillary source ofbleeding has been implicated.58 An exploratory cra-niotomy in one of our patients failed to disclose a sourceof hemorrhage despite the presence of an irregularbasilar tip. Likewise, others have described patientswith nonaneurysmal perimesencephalic hemorrhagewho underwent an exploratory craniotomy without elu-cidating the cause of the hemorrhage.18'19 These nega-tive exploratory craniotomies suggest that the source ofthe hemorrhage is probably not arterial.
The patients described in this report demonstrateseveral unusual aspects of perimesencephalic hemor-rhage and suggest that the clinical spectrum of this typeof SAH needs further refinement. The index of suspi-cion for a posterior circulation aneurysm should remainhigh in patients who present with a perimesencephalicpattern of SAH. The diagnosis of nonaneurysmal peri-mesencephalic hemorrhage is one of exclusion.
References1. Alexander MSM, Dias PS, Uttley D. Spontaneous subarachnoid
hemorrhage and negative cerebral panangiography: review of 140cases. J Neumsurg. 1986;64:537-542.
2. Iwanaga H, Wakai S, Ohiai C, Narita J, Inoh S, Nagai M. Rupturedcerebral aneurysms missed by initial angiographic study. Neuro-surgery. 1990^27:45-51.
3. Ferbert A, Hubo I, Biniek R. Non-traumatic subarachnoid hem-orrhage with normal angiogram: long-terra follow-up and CT pre-dictors of complications. J Neurol ScL 1992;107:14-18.
4. Ronkainen A, Hernesniemi J. Subarachnoid hemorrhage ofunknown etiology. Acta Neurochir (Wien). 1992;119:29-34.
5. Rinkel GJE, Wijdicks EFM, Hasan D, Kienstra GEM, Franke CL,Hageman LM, Vermeulen M, van Gijn J. Outcome in patients withsubarachnoid haemorrhage and negative angiography according topattern of haemorrhage on computed tomography. Lancet. 1991;338:964-968.
6. van Gijn J, van Dongen KJ, Vermeulen M, Hijdra A. Perimesen-cephalic hemorrhage: a nonaneurysmal and benign form of sub-arachnoid hemorrhage. Neurology. 1985^5:493-497.
7. Rinkel GJE, Wijdicks EFM, Vermeulen M, Ramos LMP, TangheHLJ, Hasan D, Meiners LC, van Gijn J. Nonaneurysmal perimes-encephalic subarachnoid hemorrhage: CT and MR patterns thatdiffer from aneurysmal rupture. AJNR Am J NeuroradioL 1991;12:829-834.
8. Rinkel GJE, Wijdicks EFM, Vermeulen M, Hasan D, BrouwersPJAM, van Gijn J. The clinical course of perimesencephalic non-aneurysmal subarachnoid hemorrhage. Ann Neurol. 1991 ;29:463-468.
9. Goergen SK, Barrie D, Sacharias N, Waugh JR. Perimesence-phalic subarachnoid haemorrhage: negative angiography andfavourable prognosis. Australas RadioL 1993;37:156-160.
10. Kitahara T, Ohwada T, Tokiwa K, Kurata A, Miyasaka Y, Yada K,Kan S. Qinical study in patients with perimesencephalic sub-arachnoid hemorrhage of unknown etiology [in Japanese]. NoShinkei Geka. 1993;21:903-908.
11. van Calenbergh F, Plets C, Goffin J, Velghe L. Nonaneurysmalsubarachnoid hemorrhage: prevalence of perimesencephalic hem-orrhage in a consecutive series. Surg Neurol. 1993;39:320-323.
12. Adams HP Jr, Gordon DL. Nonaneurysmal subarachnoid hem-orrhage. Ann NeuroL 1991;29:461-462.
13. van Gijn J. Subarachnoid haemorrhage. Lancet. 1992;339:652-655.14. Pinto AN, Ferro JM, Canhao P, Campos J. How often is a peri-
mesencephalic haemorrhage CT pattern caused by rupturedaneurysms? Acta Neurochir (Wien). 1993;124:79-81.
15. Hourihan MD, Gates PC, McAllister VL. Subarachnoid hem-orrhage in childhood and adolescence. J Newosurg. 1984;60:1163-1166.
16. Pasqualin A, Mazza C, Cavazzani P, Scienza R, DaPian R. Intra-cranial aneurysms and subarachnoid hemorrhage in children andadolescents. Chiids Nerv Syst. 1986;2:185-190.
17. Duhaime AC, Gennarelli TA, Thibault LE, Bruce DA, MarguelisSS, Wiser R. The shaken baby syndrome: a clinical, pathological,and biomechanical study. J Neuroiurg. 1987;66:4O9-415.
18. Rinkel GJE. Perimesencephalic Nonaneurysmal Hemorrhage.Utrecht, the Netherlands: University of Utrecht; 1991. Thesis.
19. Jafar JJ, Weiner HL. Surgery for angiographicalry occult cerebralaneurysms. J Neumsurg. 1993;79:674-679.
by guest on April 17, 2018
http://stroke.ahajournals.org/D
ownloaded from

W I Schievink, E F Wijdicks, D G Piepgras, D A Nichols and M J EbersoldPerimesencephalic subarachnoid hemorrhage. Additional perspectives from four cases.
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1994 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.25.7.1507
1994;25:1507-1511Stroke.
http://stroke.ahajournals.org/content/25/7/1507World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Stroke Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on April 17, 2018
http://stroke.ahajournals.org/D
ownloaded from