-
8/18/2019 Diagnosis and Management of Subarachnoid
Hemorrhage
1/25
Diagnosis andManagement ofSubarachnoidHemorrhage
Jose I. Suarez, MD, FNCS, FANA
ABSTRACT
Purpose of Review: The purposeof this article is to present the
epidemiology, clinicalpresentation, and management of patients with
subarachnoid hemorrhage (SAH). SAHis a neurologic emergency that
carries high morbidity and mortality. Patients with SAHare at risk
for several significant neurologic complications, including
hydrocephalus, ce-rebral edema, delayed cerebral ischemia,
rebleeding, seizures, and neuroendocrine ab-normalities that lead
to impaired body regulation of sodium, water, and glucose.Recent
Findings: The incidence of SAH has remained stable, but
mortality of hos-pitalized patients has significantly declined over
the past 3 decades. Many commontherapies for SAH have created
controversy, and various recent neuroprotective clinicaltrials have
produced negative results. However, the publication of two
consensus guide-lines by theAmerican Heart Association/American
StrokeAssociation and theNeurocriticalCare Society have provided a
clarification for what should constitute best practice forpatients
with SAH. The most important of those recommendations include the
fol-lowing: admission of patients to high-volumecenters(defined as
more than 35 patientswith SAH per year) under the management of a
specialized and multidisciplinary team;
early identification and management of the bleeding source;
evaluation and treatmentdecision for unsecured aneurysms by a
multidisciplinary team made up of cerebrovas-cular neurosurgeons,
endovascular practitioners, and neurointensivists; managementof
patients in the neurocritical care unit with oral nimodipine, blood
pressure control,euvolemia, and frequent monitoring for neurologic
and systemic complications; anddelayed cerebral ischemia secondary
to cerebral vasospasm should be treated withinduced hypertension
and endovascular therapies once confirmed.Summary: SAH is a
devastating neurologic disease. Management of patients with
SAHshould adhere to currently available treatment guidelines.
Several aspects of SAH man-agement remain controversial and need
further studies to clarify their role in improvingpatient
outcome.
Continuum (Minneap Minn) 2015;21(5):1263–1287.
INTRODUCTION
Nontraumatic subarachnoid hemor-rhage (SAH) represents about 3%
of all strokes in the United States.1 The
worldwide incidence of SAH rangesfrom 2 to 16 per 100,000
people andhas not changed in the past 3 decades.2
Most epidemiologic studies have shown
that women are more likely to have SAHcompared to men (1.24:1.0)
and thatminority groups (particularly African
American and Hispanic populations)are more frequently
affected comparedto white Americans.1,2 The incidenceof SAH
increases with age, with a typi-cal mean age of onset of 50 years
or
Address correspondence toDr Jose I. Suarez,
Baylor College of Medicine, OneBaylor Plaza, NB:302,
Houston,TX 77030, [email protected].
Relationship Disclosure:Dr Suarez reports no disclosure.
Unlabeled Use of Products/Investigational Use
Disclosure:Dr Suarez reports no disclosure.
* 2015, American Academy of Neurology.
1263Continuum (Minneap Minn) 2015;21(5):1263–1287
www.ContinuumJournal.com
Review Article
Copyright © American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
mailto:[email protected]:[email protected]
-
8/18/2019 Diagnosis and Management of Subarachnoid
Hemorrhage
2/25
older.2 In about 80% of SAH cases, aruptured cerebral aneurysm
is found.
However, neuroimaging techniquesmay show no source of bleeding
in 15%of SAH cases or show other abnormali-ties (eg, arteriovenous
malformation,
vasculitis) in the remaining 5% of cases.SAH causes
significant morbidity and
mortality. Mortality rates vary widely among studies,
ranging from 8% to 67%(median of 30% in the United States),
with the caveat that most of these studiesdid not account
fully for prehospitaldeaths, which have been estimated to
be between 10% and 15%.
3
However,there has been a significant decrease incase-fatality
rates of SAH across theglobe,3 which has been attributed to
im-proved survival of hospitalized patientsand is most likely owing
to changes inmanagement of patients with SAH, in-cluding
neurocritical care, endovascular therapy, and more refined
microsurgicaltechniques. Nevertheless, it is importantto emphasize
that despite the decreasein case-fatality rates, about half of
survi-
vors experience significant chronic reduc-
tions in health-related quality of life.4,5For example, a large
proportion of survi-
vors do not return to their previous levelof employment,
social independence andinteractions, or personal or family
rela-tionships even 5 years after the event.This reduction in
health-related qual-ity of life may be due to a combinationof
factors, including impaired physicalfunctioning, cognitive deficits
(partic-ularly executive function and memory),mood and emotional
symptoms (eg, an-
xiety, depression, and posttraumaticstress disorder), and
personality changes.Several risk factors for SAH have been
identified ( Table 1-1 ).2,6 Y 10
Whether any of these factors plays a predominantrole in
an individual patient remains un-clear. Genetic and environmental
fac-tors also can increase the risk of SAH,and some of these
factors can interact.For instance, the size at which cerebral
aneurysms rupture may be smaller for those patients with
concomitant hyper-
tension and cigarette smoking than for those with either
factor alone.
SAHremains one of the topneurologicemergencies, and neurologists
must fa-miliarize themselves with this devastatingdisease. This
review discusses the mainfeatures of diagnosis and management
of SAH. The main areas of emphasis whencaring for patients
with SAH should in-clude the following: prompt evaluationand
diagnosis,11 immediate transfer toappropriate centers,2,12
expeditious di-
agnosis and treatment of the bleedingsource,13,14 and overall
good neurocrit-ical care adhering to available treat-ment
guidelines.2,12
CLINICAL PRESENTATION
SAH typically presents with sudden andsevere headache (usually
described as‘‘the worst headache ever’’) accompa-nied by nausea,
vomiting, photophobia,neck pain, and loss of
consciousness( Case 1-1A ).15 Physical
examinationshould include determination of level
of consciousness, funduscopic evalua-tion, determination of
meningeal signs,and presence of focal neurologic defi-cits
( Table 1-2 ). The latter are presentin about 10% of
patients with SAH andare associated with worse prognosis whendue to
the presence of thick subarach-noid clot or parenchymal
hemorrhage.Transient elevation in the intracranialpres-sure (ICP)
causes nausea, vomiting, andsyncope. However, more sustained
andsevere increases in ICP can lead to coma
and brain death. Terson syndrome (vit-reous hemorrhage
associated with SAH)can present in up to 40% of patients
with SAH.16,17 The sudden spike in ICPis thought to lead
to preretinal hemor-rhages, which are associated with moresevere
SAH and increased mortality.
Some patients with SAH can have amore atypical
presentation.11,15 Occasion-ally, patients may present with
seizures,
KEY POINTS
h Subarachnoid hemorrhage
is more frequent in
women than men and
more frequent in
minority populations
compared to
white Americans.
h Case-fatality rates of
hospitalized patients
with subarachnoid
hemorrhage have
decreased with the
advent of neurocriticalcare,
endovascular therapy,
and more refined
microsurgical techniques.
h The most important
points in the management
of patients with
subarachnoid hemorrhage
are prompt evaluation
and diagnosis, immediate
transfer to appropriate
centers, expeditious
diagnosis andtreatment of
the bleeding source, and
overall good neurocritical
care adhering to available
treatment guidelines.
1264 www.ContinuumJournal.com October 2015
Subarachnoid Hemorrhage
Copyright © American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/18/2019 Diagnosis and Management of Subarachnoid
Hemorrhage
3/25
TABLE 1-1 Risk Factors for Subarachnoid Hemorrhage
b Nonmodifiable Risk Factors
Age
Female sex
Prior history of aneurysmal subarachnoid hemorrhage
Family history of subarachnoid hemorrhage
History of aneurysm in first-degree relatives (especially in two
or more relatives)
b Modifiable Risk Factors
Hypertension
Cigarette smoking
Heavy alcohol use
Sympathomimetic drug use (eg, cocaine)
b Other
Certain genetic disorders (eg, autosomal dominant polycystic
kidney disease,type IV Ehlers-Danlos syndrome)
Anterior circulation aneurysms are more likely to rupture in
patients who areyounger than 55 years of age
Posterior circulation aneurysms are more likely to rupture in
men
Significant financial or legal problems within the past 30
days
Cerebral aneurysms of more than 7 mm in diameter
Case 1-1AA 45-year-old right-handed woman presented to a primary
stroke center with sudden onset of severeheadache accompanied by
nausea, vomiting, and syncope, which developed 1 hour prior
topresentation while she was moving furniture at her house. She had
a past history of heavy smokingand cocaine use. Upon arrival to the
emergency department, her blood pressure was 180/100 mm Hg,heart
rate was 105 beats per minute, arterial oxygen saturation (SaO2)
was 97% on room air, andher temperature was 36.5-C (97.7-F). Her
examination revealed a Glasgow Coma Scale score of 15,normal
cranial nerves, and no motor or sensory deficits. Her World
Federation of Neurological SurgeonsScale (WFNSS) score was 1 and
her modified Fisher Scale score was 3. She reported neck
painthroughout the interview. She was treated with 4 mg of IV
morphine sulfate and 10 mg of IV labetalolwithout much response.
She was then started on a nicardipine drip to maintain a systolic
blood pressureless than 160 mm Hg. A noncontrast head CT showed a
subarachnoid hemorrhage (SAH) withpredominance in the anterior
interhemispheric fissure (Figure 1-1A). The patient was
immediatelytransferred by helicopter to a comprehensive stroke
center for further care. Digital subtractionangiography (DSA)
revealed an irregular, multilobed, and wide-neck anterior
communicating arteryaneurysm (Figure 1-1B and 1-1C).
After discussion among the neuroradiologist, the
cerebrovascularneurosurgeon, and neurointensivists, the patient
underwent surgical clipping of the unsecured aneurysm.Following
surgery, the patient was transferred to the neurocritical care
unit, where she received oralnimodipine, pain control, IV
levetiracetam (seizure prophylaxis for 3 days), and fluids to
maintain euvolemia.Nicardipine was discontinued, and she maintained
her systolic blood pressure between 140 and 160 mm Hgspontaneously.
Her neurologic examination remained unchanged and she was mobilized
out of bed.
Continued on page 1266
1265Continuum (Minneap Minn) 2015;21(5):1263–1287
www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/18/2019 Diagnosis and Management of Subarachnoid
Hemorrhage
4/25
Comment. This case delineates the initial management of a
patient with SAH. The key issues toconsider include early
identification, transfer to a high-volume center, admission to a
specializedneurocritical care unit, identification and treatment of
the bleeding source, and multidisciplinarydiscussion to undertake
best treatment for an unsecured aneurysm. In addition, this
patientunderwent blood pressure control prior to aneurysm treatment
to prevent rebleeding, and receivedoral nimodipine, which has been
shown to improve long-term outcomes in patients with SAH.
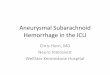
FIGURE 1-1 Initial imaging studies of the patient
in Case 1-1. A, Nonenhanced head CTshows diffuse
subarachnoid hemorrhage with predominance in anterior
interhemisphericfissure without cerebral edema or significant
hydrocephalus. B, A two-dimensional
digital subtraction angiogram shows an anterior communicating
artery aneurysm on a lateralview (arrow ). C , A
three-dimensional rotational digital subtraction angiogram reveals
that theanterior communicating artery aneurysm is irregular and
trilobed and has a wide neck ( arrow ).
Continued from page 1265
1266 www.ContinuumJournal.com October 2015
Subarachnoid Hemorrhage
Copyright © American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/18/2019 Diagnosis and Management of Subarachnoid
Hemorrhage
5/25
acute encephalopathy, and concomitantsubdural hematoma and head
trauma,making the underlying diagnosis of SAH
more elusive. A minority of patients may have a warning
‘‘sentinel’’ headache daysto weeks before an aneurysmal SAH,
which is thought to represent a small an-eurysmal
leak.18,19 Regrettably, this pieceof information is only obtained
retro-spectively as most of the time the head-ache is transient and
head CT scanningis unrevealing in about 50% of cases.
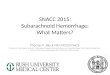
DIAGNOSISHead CT Scan
The most appropriate initial diagnos-tic test for patients
suspected of havingSAH is a noncontrast head CT scan( Figure
1-2 ) ( Case 1-1A ).15 The sen-sitivity of a
CT scan has been reportedto be 98% to 100% for the detectionof
subarachnoid blood within 12 hoursof symptom onset when compared
tolumbar puncture. However, the sensi-tivity of a CT scan decreases
to 93% at
24 hours and 50% at 7 days.20,21 Thecharacteristic appearance of
extravasatedblood in the basal subarachnoid cisterns
is hyperdense ( Figure 1-1 A). Other loca-tions
include the sylvian fissures; inter-hemispheric fissure;
interpeduncular fossa; and suprasellar, ambient,
andquadrigeminal cisterns. CT also can detectintracerebral
hemorrhage, intraventricu-lar hemorrhage, and hydrocephalus.
Although MRI may be as sensitive as CTscan in the first 2
days of SAH presen-tation, it is rarely performed in this sce-nario
because of logistical issues.22,23 MRI
with hemosiderin-sensitive sequences
(gradient echo and susceptibility-weightedimaging) or with
fluid-attenuated inver-sion recovery (FLAIR) sequences is
moresensitive than CT scan when performedseveral days after the
onset of SAH.
Lumbar Puncture
A lumbar puncture is recommended inany patient with
suspected SAH and neg-ative or equivocal results on head CT
KEY POINTS
h In some instances,
diagnosis of
subarachnoid hemorrhagecan be elusive owing to
atypical findings on
presentation such as
seizures at onset, acute
encephalopathy, and
concomitant subdural
hematoma and
head trauma.
h The sensitivity of CT for
detection of subarachnoid
blood may be 98% to
100% when obtained
within 12 hours of onsetof symptoms, compared
to lumbar puncture.
TABLE 1-2 Focal Physical Findings in Patients With
Subarachnoid Hemorrhage
Findings Likely Cause
Third nerve palsy Usually posterior communicating aneurysm; also
posterior cerebralartery and superior cerebellar artery
aneurysms
Sixth nerve palsy Elevated intracranial pressure (false
localizing sign)
Combination of hemiparesis andaphasia or visuospatial
neglect
Middle cerebral artery aneurysm, thick subarachnoid clots,
orparenchymal hematomas
Bilateral leg weakness and abulia Anterior communicating artery
aneurysm
Ophthalmoplegia Internal carotid artery aneurysm impinging upon
the cavernous sinus
Unilateral visual loss or bitemporalhemianopia
Internal carotid artery aneurysm compressing optic nerve or
optic chiasm
Impaired level of consciousness andimpaired upward gaze
Pressure on the dorsal midbrain due to hydrocephalus
Brainstem signs Brainstem compression by basilar artery
aneurysm
Neck stiffness Meningeal irritation by the presence of
subarachnoid blood
Retinal and subhyaloid hemorrhages Sudden increase of
intracranial pressure
Preretinal hemorrhages (Terson syndrome) Vitreous hemorrhage due
to severe elevations of intracranial pressure
1267Continuum (Minneap Minn) 2015;21(5):1263–1287
www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/18/2019 Diagnosis and Management of Subarachnoid
Hemorrhage
6/25
scan ( Figure 1-2 ). CSF should be col-lected four
consecutive tubes, and redblood cell count should be determinedin
tubes one and four.11,15 The diagno-
sis of SAH is supported by the following:elevated opening
pressure, elevated redblood cell count that does not signifi-cantly
decrease from tube one to tubefour, and especially xanthochromia.
Thelatter, which indicates red blood cellbreakdown, can be
determined by visualinspection or by spectrophotometry.
Xanthochromia takes about 12 hours todevelop after SAH,
and spectropho-
tometry seems to be more sensitivethan visual inspection.
However, mosthospitals in the United States use visualinspection,
and no well-conducted clin-
ical studies exist that allow clinicians toknow with certainty
what the false-negative rate for xanthochromia is at var-ious time
intervals from SAH onset.24
Identification of Bleeding Source
All patients with a diagnostic CT scan or with
eitherequivocal or diagnostic lumbar puncture must undergo
further imaging
with CT angiography (CTA) or cerebral
KEY POINT
h The diagnosis of
subarachnoid hemorrhage
is supportedby thefinding
of xanthochromia in CSF.
FIGURE 1-2 Diagnostic algorithm for subarachnoid
hemorrhage.
CT = computed tomography.
Reprinted with permission from Suarez JI,et al,N Eng J
Med.15
B 2006 Massachusetts Medical Society.
www.nejm.org/doi/full/10.1056/
NEJMra052732.
1268 www.ContinuumJournal.com October 2015
Subarachnoid Hemorrhage
Copyright © American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
http://www.nejm.org/doi/full/10.1056/NEJMra052732http://www.nejm.org/doi/full/10.1056/NEJMra052732http://www.nejm.org/doi/full/10.1056/NEJMra052732http://www.nejm.org/doi/full/10.1056/NEJMra052732http://www.nejm.org/doi/full/10.1056/NEJMra052732
-
8/18/2019 Diagnosis and Management of Subarachnoid
Hemorrhage
7/25
digital subtraction angiography (DSA)( Figure
1-1 ).11,15 The latter has tradition-
ally been considered the ‘‘gold stan-dard’’ to elucidate the
source of bleedingin SAH (particularly aneurysmal), butCTA has
become widely available andis being commonly performed as
first-line vascular imaging or even in lieu of DSA in some
centers. CTA has a sensi-tivity and specificity ranging from 90%to
97% and 93% to 100%, respectively,depending on technique
(16-detector rows versus 64-detector rows, slice thick-ness,
and data processing algorithms)and the reader’s experience.25,26
CTA may not be reliable for the detection of smaller (ie,
less than 4 mm) or distal an-eurysms. The decision to perform
CTA or DSA will vary depending on resourceavailability and
institutional practices.However, loss of consciousness at theonset
of SAH may be a strong predictor for the detection of ruptured
cerebralaneurysm on subsequent DSA.27 Thus,in those patients with a
negative CTA,this presentation should still prompt aDSA. In the
author’s institution, a com-
bination of two-dimensional and three-dimensional DSA are
performed as thestandard diagnostic testing for aneurysmdetection
in all SAH cases. Patients witha negative DSA should have a
repeatstudy 7 to 14 days after initial presenta-tion, and if
negative, MRI should be per-formed to uncover a possible
vascular malformation of the brain, brainstem,or spinal
cord.15,23
Misdiagnosis
Misdiagnosis of SAH is still common
because the classic findings may occur inconsistently or
patients may present
with atypical findings. Misdiagnosis isassociated with
significantly increasedmortality and disability (up to fourfold)in
those patients presenting withoutneurologic deficits at their
initial hospital
visit. Fortunately, the frequency of SAHmisdiagnosis has
decreased from morethan 60% in the early 1980s to less than
15% more recently.28,29 Nevertheless, itis important to
emphasize that practi-
tioners should have a high level of sus-picion for any patient
presenting withnew-onset headache and understandthe possible
pitfalls in the diagnosis of SAH ( Table 1-3 ). A
recent study reported100% sensitivity to detect SAH in pa-tients
older than 40 years of age usingclinical decision-making rules that
in-clude any of the following factors: neck pain or stiffness,
witnessed loss of con-sciousness, and symptom onset duringexertion
plus thunderclap headacheand pain on neck flexion.30
Perimesencephalic SubarachnoidHemorrhage
As previously mentioned, in about 15%of patients with SAH,
imaging studiesfail to demonstrate the source of bleed-ing.
Approximately 38% of these patientshave nonaneurysmal
perimesencephalicSAH.31 Most patients with nonaneurys-mal
perimesencephalic SAH (about 54%)are male and have a low risk of
com-plications and better outcomes than pa-
tients with aneurysmal SAH. A correctdiagnosis is important
because of thecatastrophic consequences of missinga ruptured
cerebral aneurysm. Nona-neurysmal perimesencephalic SAH isconfirmed
in the presence of a nega-tive CTA or DSA in patients with
thefollowing head CT scan pattern32: cen-ter of hemorrhage located
immediately anterior to the midbrain, with or withoutextension
of blood to the anterior partof the ambient cistern or to the
basalpart of the sylvian fissures; no completefilling of the
anterior interhemisphericfissure and no extension to the
lateralsylvian fissures, except for minuteamounts of blood; and
absence of frank intraventricular blood ( Figure
1-3 ).
INITIAL EVALUATION
Initial evaluation and managementof patients with SAH should
focus on
KEY POINTS
h All patients with a
diagnostic CT scan or
with either equivocal or
diagnostic lumbar
puncture must undergo
further imaging with CT
angiography or digital
subtraction angiography.
h Any of the following
clinical factors should
prompt a workup for
subarachnoid hemorrhage
in patients older than 40:
neck pain or stiffness,
witnessed loss of
consciousness, andsymptom onset during
exertion plus thunderclap
headache and pain on
neck flexion.
1269Continuum (Minneap Minn) 2015;21(5):1263–1287
www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/18/2019 Diagnosis and Management of Subarachnoid
Hemorrhage
8/25
stabilization of airway, breathing, andcirculation.2,12,15,22,23
Once patientsare deemed stable, a head CT scan mustbe performed.
Patients who are unable toprotect their airway should be
intubatedimmediately. The most common indica-tions for endotracheal
intubation include
coma, hydrocephalus, seizure, and needfor sedation for
significant agitation. Inaddition, extreme blood pressure
valuesshould be avoided. Hypertension controlis predicated on the
premise that it may precipitate rebleeding.33 No data
fromrandomized controlled clinical trials exist,but usual practice
and current recommen-dations are to maintain a mean arterialblood
pressure of less than 110 mm Hg
or a systolic blood pressure of less than160 mm Hg until the
ruptured aneu-rysm is secured, while using premorbidbaseline blood
pressures to refine tar-gets and avoid hypotension. Commonly,pain
control may be sufficient to achieveblood pressure
control;otherwise, admin-
istration of IV labetalol (5 mg to 20 mg),hydralazine (5 mg to
20 mg), or continu-ous infusion of nicardipine (5 mg/h to15 mg/h)
is preferred. Pain control isbest achieved with the
administrationof short-acting opiates ( Case
1-1A ).
Disease Severity Scoring
The severity of neurologic impair-ment and the amount of
subarachnoid
KEY POINT
h Mean arterial blood
pressure should be
maintained at less than
110 mm Hg or systolic
blood pressure at less
than 160 mm Hg until
the ruptured aneurysm
is secured, whileavoiding hypotension.
TABLE 1-3 Reasons for Misdiagnosis of Subarachnoid
Hemorrhagea
b Failure to Recognize Spectrum of Presentation of
Subarachnoid Hemorrhage
Not obtaining complete history from patients with unusual (for
the patient) headaches(Was the onset abrupt? Is the quality
different and severity greater than prior headaches?)
Failure to appreciate that the headache can improve
spontaneously or with non-narcotic analgesics
Focusing on the secondary head injury resulting from syncope and
fall or motor vehicle collision
Focusing on ECG findings
Focusing on elevated blood pressure
Overreliance on the classic presentation
Assuming symptoms may be related to other disorders (eg, viral
syndrome, viral meningitis, migraine,tension-type headache,
sinus-related headache, psychiatric disorder)
b Failure to Understand the Limitations of Head CT
Scanning
Sensitivity decreases with increasing time from onset of
headache
False-negative results with small-volume bleeds
Lack of experience of physician reader
Motion artifacts or lack of thin cuts of posterior fossa
False-negative results due to hematocrit of less than 30%
b Failure to Perform Lumbar Puncture or Interpret the CSF
Findings Correctly
Failure to perform lumbar puncture in patients with negative or
inconclusive CT scans
Failure to distinguish a traumatic tap from true subarachnoid
hemorrhage
Failure to recognize that xanthochromia may be absent very early
(less than 12 hours) and very late(more than 2 weeks)
CSF = cerebrospinal fluid; CT = computed tomography; ECG =
electrocardiogram.a Data from Edlow JA, et al, J Emerg Med.11
www.jem-journal.com/article/S0736-4679(07)00729-9/abstract .
1270 www.ContinuumJournal.com October 2015
Subarachnoid Hemorrhage
Copyright © American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
http://www.jem-journal.com/article/S0736-4679(07)00729-9/abstracthttp://www.jem-journal.com/article/S0736-4679(07)00729-9/abstract
-
8/18/2019 Diagnosis and Management of Subarachnoid
Hemorrhage
9/25
bleeding on admission are the strongestpredictors of neurologic
complicationsand outcome.15,23 Therefore, it isessential that
patients with SAH bescored promptly after arrival and
sta-bilization. There are several scoringsystems available.
However, the World
Federation of Neurological SurgeonsScale (WFNSS) and the
modified Fisher Scale are the most reliable and simple
to perform ( Table 1-415,34,35 ).23
Higher WFNSS and modified Fisher Sca lescores are
associated with worse clin-ical outcome and a higher proportionof
neurologic complications.
Admission to High-Volume
CentersThe next immediate steps are to transfer the patient
to a high-volume center (if not
KEY POINT
h The severity of neurologic
impairment and the
amount of subarachnoid
bleeding on admission are
the strongest predictors
of neurologic complications
and outcome.
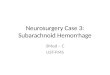
FIGURE 1-3 Noncontrast head CT scan of a patient with
nonaneurysmal perimesencephalic subarachnoid hemorrhage.The center
of the hemorrhage is located immediately anterior to the midbrain
( A and C , arrows) and extendsto the
anterior part of the ambient cistern (B, arrow ).
TABLE 1-4 Clinical and Radiologic Grading Scales for
Subarachnoid Hemorrhagea
World Federation of NeurologicalSurgeons Scale34 Modified Fisher
Scale35
GradeGlasgowComa Scale
NeurologicExamination Grade
SubarachnoidHemorrhage
IntraventricularHemorrhage
1 15 No motor deficit 0 Absent Absent
2 13 Y 14 No motor deficit 1 Minimal Absent in both
lateral ventricles
3 13 Y 14 Motor deficit 2 Minimal Present in both
lateral ventricles
4 7 Y 12 With or withoutmotor deficit
3 Thickb Absent in both lateral ventricles
5 3 Y 6 With or withoutmotor deficit
4 Thickb Present in both lateral ventricles
a Modified with permissionfromSuarezJI, etal, N EnglJ
Med.15 B 2006 Massachusetts Medical Society.
www.nejm.org/doi/full/10.1056/NEJMra052732.b Thick is defined as a
hemorrhage filling one or more cisterns or fissures out of a total
of 10: interhemispheric fissure, the quadrigeminal
cistern, both suprasellar cisterns, both ambient cisterns, both
basal sylvian fissures, and both lateral sylvian fissures.
1271Continuum (Minneap Minn) 2015;21(5):1263–1287
www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
http://www.nejm.org/doi/full/10.1056/NEJMra052732http://www.nejm.org/doi/full/10.1056/NEJMra052732http://www.nejm.org/doi/full/10.1056/NEJMra052732
-
8/18/2019 Diagnosis and Management of Subarachnoid
Hemorrhage
10/25
already in one), admit the patient to adedicatedneurocritical
care unit, and have
the patient undergo a multidisciplinary evaluation for the
management of an un-secured cerebral aneurysm ( Table
1-5 ).2,12
It has been shown that admission of pa-tients with SAH to
low-volume centers
is associated with higher 30-day mor-tality compared to
admission to high-
volume centers. In addition, admission
TABLE 1-5 Summary of Key Recommendations for the
Management of Patients WithSubarachnoid Hemorrhage
TreatmentDecision
American Heart Association/AmericanStroke Association2,a
Neurocritical Care Society12,b
Hospital/systemcharacteristics
Low-volume hospitals (eg, less than10 subarachnoid hemorrhage
[SAH] casesper year) should consider early transfer ofpatients with
SAH to high-volume centers(eg, more than 35 SAH cases per year)
withexperienced cerebrovascular surgeons,endovascular specialists,
andmultidisciplinary neurointensive careservices (Class I, Level
B).
Patients with SAH should be treated athigh-volume centers
(moderate qualityof evidence, strong recommendation).
After discharge, it is reasonable to referpatients with SAH for
a comprehensiveevaluation, including cognitive, behavioral,and
psychosocial assessments(Class IIa, Level B).
High-volume centers should haveappropriate specialty
neurointensivecare units, neurointensivists, vascularneurosurgeons,
and interventionalneuroradiologists to provide theessential
elements of care(moderate quality of evidence,strong
recommendation).
Aneurysm treatment Surgical clipping or endovascular coiling
ofthe ruptured aneurysm should beperformed as early as feasible in
the
majority of patients to reduce the rate ofrebleeding after SAH
(Class I, Level B).
Early aneurysm repair should beundertaken, when possible and
reasonableto prevent rebleeding (high quality of
evidence, strong recommendation).
For patients with ruptured aneurysms judged to be
technically amenable to eitherendovascular coiling and
neurosurgicalclipping, endovascular coiling should beconsidered
(Class I, Level B).
An early, short course of antifibrinolytictherapy prior to early
aneurysm repair(begun at diagnosis and continued up tothe point at
which the aneurysm is securedor at 72 hours post ictus, whichever
isshorter) should be considered (low qualityof evidence, weak
recommendation).
Complete obliteration of the aneurysm isrecommended whenever
possible(Class I, Level B).
Delayed (more than 48 hours after theictus) or prolonged (more
than 3 days)antifibrinolytic therapy exposes patientsto side
effects of therapy when the riskof rebleeding is sharply reduced
andshould be avoided (high quality of
evidence, strong recommendation).
Stenting of a ruptured aneurysm is associatedwith increased
morbidity and mortality(Class III, Level C).
For patients with an unavoidable delay inobliteration of
aneurysm, a significant riskof rebleeding, and no compelling
medicalcontraindications, short-term (less than72 hours) therapy
with tranexamic acid oraminocaproic acid is reasonable to reducethe
risk of early aneurysm rebleeding(Class IIa, Level B).
Continued on page 1273
1272 www.ContinuumJournal.com October 2015
Subarachnoid Hemorrhage
Copyright © American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/18/2019 Diagnosis and Management of Subarachnoid
Hemorrhage
11/25
TABLE 1-5 Summary of Key Recommendations for the
Management of Patients WithSubarachnoid Hemorrhage Continued from
page 1272
TreatmentDecision
American Heart Association/AmericanStroke Association2,a
Neurocritical Care Society12,b
Blood pressure control Between the time of SAH symptom onsetand
aneurysm obliteration, blood pressureshould be controlled with a
titratableagent to balance the risk of stroke,hypertension-related
rebleeding, andmaintenance of cerebral perfusionpressure (Class I,
Level B).
Treat extreme hypertension in patientswith an unsecured,
recently rupturedaneurysm. Modest elevations in bloodpressure (mean
blood pressure of less than110 mm Hg) do not require
therapy.Premorbid baseline blood pressures shouldbe used to refine
targets and hypotensionshould be avoided (low quality of
evidence,strong recommendation).
The magnitude of blood pressure controlto reduce the risk of
rebleeding has notbeen established, but a decrease in systolic
blood pressure to less than 160 mm Hgis reasonable (Class IIa,
Level C).
Intravascularvolume status
Maintenance of euvolemia and normalcirculating blood volume is
recommendedto prevent delayed cerebral ischemia(Class I, Level
B).
Intravascular volume management shouldtarget euvolemia and avoid
prophylactichypervolemic therapy. In contrast, there isevidence for
harm from aggressiveadministration of fluid aimed at
achievinghypervolemia (moderate qualityof evidence, strong
recommendation).
Cardiopulmonarycomplications
No recommendations given. Baseline cardiac assessment with
serialenzymes, ECG, and echocardiography isrecommended, especially
in patientswith evidence of myocardial dysfunction(low quality of
evidence, strong
recommendation).
Monitoring of cardiac output may be usefulin patients with
evidence of hemodynamicinstability or myocardial dysfunction(low
quality of evidence, strongrecommendation).
Seizures The use of prophylactic anticonvulsantsmay be
considered in the immediateposthemorrhagic period (Class IIb, Level
B).
Routine use of anticonvulsant prophylaxiswith phenytoin is not
recommendedafter SAH (low quality of evidence,strong
recommendation).
The routine long-term use of anticonvulsantsis not recommended
(Class III, Level B). If anticonvulsant prophylaxis is used,
a short
course (3 Y 7 days) is recommended (lowquality of
evidence, weak recommendation).
Continuous EEG monitoring should beconsidered in patients with
poor-gradeSAH who fail to improve or who haveneurologic
deterioration of undeterminedetiology (low quality of
evidence,strong recommendation).
Continued on page 1274
1273Continuum (Minneap Minn) 2015;21(5):1263–1287
www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/18/2019 Diagnosis and Management of Subarachnoid
Hemorrhage
12/25
TABLE 1-5 Summary of Key Recommendations for the
Management of Patients WithSubarachnoid Hemorrhage Continued from
page 1273
TreatmentDecision
American Heart Association/AmericanStroke Association2,a
Neurocritical Care Society12,b
Fever treatment Aggressive control of fever to a target
ofnormothermia by use of standard oradvanced temperature-modulating
systemsis reasonable in the acute phase of SAH(Class IIa, Level
B).
During the period of risk for delayed cerebralischemia, control
of fever is desirable;intensity should reflect the
individualpatient’s relative risk of ischemia (lowquality of
evidence, strong recommendation).
Surface cooling or intravascular devicesaremore effective
andshould be employedwhen antipyretics fail in cases where
fevercontrol is highly desirable (high quality ofevidence, strong
recommendation).
Glucose control Careful glucose management with strictavoidance
of hypoglycemia may beconsidered as part of the general
criticalcare management of patients with SAH(Class IIb, Level
B).
Hypoglycemia (serum glucose of less than80 mg/dL) should be
avoided (high qualityof evidence, strong recommendation).
Serum glucose should be maintainedbelow 200 mg/dL (moderate
quality ofevidence, strong recommendation).
Deep venousthrombosisprophylaxis
Heparin-induced thrombocytopenia anddeep venous thrombosis are
relativelyfrequent complications after SAH. Earlyidentification and
targeted treatment arerecommended,but further research is neededto
identify the ideal screening paradigms(Class I, Level B).
Measures to prevent deep venousthrombosis should be employed in
allpatients with SAH (high quality of evidence,strong
recommendation).
The use of unfractionated heparin forprophylaxis could be
started 24 hoursafter undergoing aneurysm obliteration
(moderate quality of evidence,strong recommendation).
Delayed cerebralischemia
Oral nimodipine should be administered toall patients with SAH
(Class I, Level A).
Oral nimodipine (60 mg every 4 hours)should be administered
after SAH fora period of 21 days (high quality ofevidence, strong
recommendation).
Maintenance of euvolemia and normalcirculating blood volume is
recommendedto prevent delayed cerebral ischemia(Class I, Level
B).
The goal should be maintainingeuvolemia, rather than
attemptinghypervolemia (moderate qualityof evidence, strong
recommendation).
Prophylactic hypervolemia or balloonangioplasty before the
development ofangiographic spasm is not recommended(Class III,
Level B).
Transcranial Doppler may be used formonitoring and detection of
large arteryvasospasm with variable sensitivity(moderate quality of
evidence,strong recommendation).
Transcranial Doppler is reasonable tomonitor for the development
of arterialvasospasm (Class IIa, Level B).
Digital subtraction angiography is thegold standard for
detection of largeartery vasospasm (high quality of evidence,strong
recommendation).
Perfusion imaging with CT or MRI can beuseful to identify
regions of potentialbrain ischemia (Class IIa, Level B).
Continued on page 1275
1274 www.ContinuumJournal.com October 2015
Subarachnoid Hemorrhage
Copyright © American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/18/2019 Diagnosis and Management of Subarachnoid
Hemorrhage
13/25
to dedicated neurocritical care units st-affed by dedicated
neurointensivists isassociated with decreased
in-hospitalmortality.36
Treatment of UnsecuredAneurysms
Treatment of unsecured aneurysms has
evolved, and two accepted efficacious
management modalities currently exist:
surgical clipping and endovascular coil-
ing. The choice of treatment depends
on several factors, including the pa-
tient’s age and aneurysm location,
morphology, and relationship to ad-
jacent vessels. Because of the complex-
ity of determining the most appropriate
treatment for individual patients, it
is recommended that a multidisciplin-
ary team made up of cerebrovascular
neurosurgeons, endovascular practi-
tioners, and neurointensivists confer
TABLE 1-5 Summary of Key Recommendations for the
Management of Patients WithSubarachnoid Hemorrhage Continued from
page 1274
TreatmentDecision
American Heart Association/AmericanStroke Association2,a
Neurocritical Care Society12,b
Induction of hypertension is recommendedfor patients with
delayed cerebral ischemiaunless blood pressure is elevated
atbaseline or cardiac status precludes it(Class I, Level B).
Patients clinically suspected of delayedcerebral ischemia should
undergo atrial of induced hypertension(moderate quality of
evidence,strong recommendation).
Cerebral angioplasty and/or selectiveintra-arterial vasodilator
therapy isreasonable in patients with symptomaticvasospasm,
particularly those who arenot responding to hypertensive
therapy
(Class IIa, Level B).
Endovascular treatment usingintra-arterial vasodilators
and/orangioplasty may be considered forvasospasm-related delayed
cerebralischemia (moderate quality of evidence,
strong recommendation).
Anemia andtransfusion
The use of packed red blood celltransfusion to treat anemia
might bereasonable in patients with SAH whoare at risk of cerebral
ischemia. Theoptimal hemoglobin goal is still to bedetermined
(Class IIb, Level B).
Patients should receive packed red bloodcell transfusions to
maintain hemoglobinconcentration above 8 Y 10 g/dL
(moderatequality of evidence, strongrecommendation).
Hyponatremia The use of fludrocortisone acetate andhypertonic
saline solution is reasonablefor preventing and
correctinghyponatremia (Class IIa, Level B).
Fluid restriction should not be used totreat hyponatremia (weak
quality ofevidence, strong recommendation).
Early treatment with hydrocortisoneor fludrocortisone may be
used tolimit natriuresis and hyponatremia
(moderate quality of evidence,weak recommendation).
Mild hypertonic saline solutions can be usedto correct
hyponatremia (very low qualityof evidence, strong
recommendation).
CT = computed tomography; ECG = electrocardiogram; EEG =
electroencephalogram; MRI = magnetic resonance imaging.a American
Heart Association / American Stroke Association
recommendations follow the American Heart Association Stroke
Council’s methods of classifying the level of certainty of the
treatment effect and the class of evidence.b For the Neurocritical
Care Society’s guidelines, the quality of the data was assessed and
recommendations developed using the
Grading of Recommendations, Assessment, Development, and
Evaluation (GRADE) system.
KEY POINT
h Admission of patients
with subarachnoidhemorrhage to
low-volume centers is
associated with higher
30-day mortality
compared to admission
to high-volume centers.
1275Continuum (Minneap Minn) 2015;21(5):1263–1287
www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/18/2019 Diagnosis and Management of Subarachnoid
Hemorrhage
14/25
to reach a consensus.2,12,15,22,23,29 The
International Subarachnoid Aneurysm
Trial (ISAT) was a prospective random-ized controlled clinical
trial that evalu-
ated patients with unsecured aneurysms
who were considered suitable for either
endovascular coiling or surgical clip-
ping.13,14 Patients assigned to the endo-
vascular coiling group had a significantly
higher favorable outcome (defined as
survival free of disability at 1 year)
and lower risk of epilepsy compared
to those assigned to the surgical clip-
ping group. However, the risk of
rebleeding and partial occlusion of aneurysms was lower
with surgical
clipping. Overall, endovascular coil-
ing should be preferred over surgical
clipping whenever possible; however,
many aneurysms are not equally suit-
able for either surgical clipping or endo-
vascular coiling ( Table 1-6 ) ( Case
1-1A ).
Regardless of the treatment modality
chosen, unsecured aneurysms must be
treated as soon as possible to prevent
rebleeding ( Table 1-5 ). In the author’s
institution, the median time for aneu-rysm treatment is 7 hours
from initial
hospital arrival.
INTENSIVE CARE UNITMANAGEMENT
SAH is often accompanied by more se-
vere initial systemic and intracranial re-
sponses than other cerebral insults.37 Y 40
More than 75% of patients with SAH
experience systemic inflammatory re-
sponse syndrome (SIRS), which is likely
related to elevated levels of inflammatory
cytokines. SIRS has been associated with
permanent neurocognitive dysfunction.In addition, patients with
SAH are at risk
for several significant neurologic com-
plications, including hydrocephalus, cere-
bral edema, delayed cerebral ischemia,
rebleeding, seizures, and neuroendo-
crine abnormalities that lead to impaired
body regulation of sodium, water, and
glucose. Furthermore, SAH unleashes
hypothalamic-mediated changes, includ-
ing increased sympathetic and parasym-pathetic drive, that
result in cardiac and
pulmonary complications. For example,
increased circulating catecholamines are
thought to be the cause for several cardiac
manifestations, including ECG changes,
arrhythmias, impaired cardiac contrac-
tility (eg, Takotsubo cardiomyopathy),
troponinemia, and myocardial necrosis.
Pulmonary complications, such as neu-
rogenic pulmonary edema, most likely
have a similar underlying pathophysi-
ologic mechanism. It is important torecognize and treat all
these systemic
complications as they are associated
with increased risk for delayed cerebral
ischemia and poor neurologic outcome
after SAH.
Neurologic Complications
Rebleeding. Rebleeding is a major dis-
abling complication of SAH, which car-
ries high mortality and morbidity. In
the first 24 hours, 4% to 15% of pa-
tients will rebleed, with the highest risk occurring less
than 6 hours from symp-tom onset.33 Rebleeding risk decreasesover
the following 2 weeks. The mainrisk factors associated with
rebleeding
include high systolic blood pressure
(ie, greater than 160 mm Hg), poor neu-
rologic grade, intracerebral or intraven-
tricular hematomas, ruptured posterior
circulation aneurysms, and aneurysms
of greater than 10 mm in size.33
The best measure to reduce the risk
of rebleeding is the early treatment of unsecured aneurysms
( Table 1-5 ).2,12
However, in some instances there may be a delay in surgical
clipping or endo-
vascular coiling of the aneurysm, andshort-term (ie, less
than 72 hours) treat-ment with tranexamic acid or amino-caproic
acid has been recommended if no contraindications exist. The
use of these antifibrinolytic agents is based
KEY POINTS
h Overall, when
considering treatment of
unruptured aneurysms,
endovascular coiling
should be preferred over
surgical clipping
whenever possible.
h Patients with
subarachnoid
hemorrhage are at risk
for several significant
neurologic complications,
including hydrocephalus,
cerebral edema,
delayed cerebral ischemia,
rebleeding, seizures,and neuroendocrine
abnormalities.
h The best measure to
reduce the risk of
rebleeding is the
early treatment of
unsecured aneurysms.
1276 www.ContinuumJournal.com October 2015
Subarachnoid Hemorrhage
Copyright © American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/18/2019 Diagnosis and Management of Subarachnoid
Hemorrhage
15/25
on the premise that early risk for re-bleeding is a consequence
of activatedfibrinolysis and reduced clot stability during the
first 6 hours. In addition,
blood pressure control is also very im-portant to prevent
rebleeding prior toaneurysm obliteration, as
previously mentioned. Patients suspected of re-bleeding should
be evaluated promptly,have a follow-up head CT scan and
DSA (if not already done), and immediately undergo
aneurysm obliteration. Endo-
vascular treatment of ruptured cere-bral aneurysms should
include coilingonly. Stenting of cerebral aneurysms inthe setting
of SAH should be avoidedas it is associated with higher
bleedingcomplications and poor outcome.2
Hydrocephalus. Acute symptomatic
hydrocephalus occurs in about 20% of
patients with SAH, usually within the
first few days after symptom onset.2,15,22
Patients manifestdecreased levels of con-
sciousness and other signs of increasedICP, such as impaired
upward gaze andhypertension. An immediate follow-up
head CT scan is warranted in any patient with suspected
symptomatic hydroceph-alus and must be followed by insertion
of an external ventricular drain (EVD).
Some centers perform lumbar drain in-sertion instead of EVD in
patients withSAH who have communicating hydro-cephalus. Weaning the
patient of an EVD
should begin shortly after aneurysm ob-literation or within 48
hours of insertionif the patient is neurologically stable.
A rapid weaning protocol is preferred.
About 60% of patients with SAH who
undergo EVD insertion will have suc-cessful weaning, and the
others may require chronic ventriculoperitoneal
shunt insertion ( Case 1-1B ).Seizures.
Delineating the true fre-quency of seizures in patients with SAHhas
been difficult and controversial asmany patients (20% to 26%)
present withseizurelike episodes that are not easy tocharacterize
as many of them occur atthe time of symptom
onset.2,12 Y 15 Ingeneral, patients with middle
cerebralartery (MCA) aneurysms, concomitant
KEY POINT
h About 60% of patients
with subarachnoid
hemorrhage who undergo
external ventricular drain
insertion will have
successful weaning and
the others may require
chronic ventriculoperitoneal
shunt insertion.
TABLE 1-6 Preferences for Treatment of Unsecured
Aneurysms
CharacteristicsPreferred TreatmentModality
Advanced age Endovascular coiling
Poor clinical grade Endovascular coiling
Multiple underlying systemic conditions Endovascular coiling
Aneurysms with wide neck-to-body ratio Surgical clipping
Normal arterial branches arising from dome or bodyof
aneurysm
Surgical clipping
Middle cerebral artery aneurysm Surgical clipping
Top-of-the-basilar aneurysm Endovascular coiling
Aneurysm associated with large parenchymal hematoma Surgical
clipping
High surgical risk Endovascular coiling
Patient preference Endovascular coiling
Clinical equipoisea Endovascular coiling
a Unsecured aneurysm is considered equallysuitable for either
endovascular coiling or surgical clipping.
1277Continuum (Minneap Minn) 2015;21(5):1263–1287
www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/18/2019 Diagnosis and Management of Subarachnoid
Hemorrhage
16/25
intraparenchymal hematomas, and poor clinical grade are at
higher risk for sei-
zures, whereas patients treated withendovascular coiling have
lower ratesof seizures. Long-term risk for epilepsy is
low.
The administration of prophylacticanticonvulsants in patients
with SAH wascommon practice; however, anticonvul-sant
administration (particularly phenyt-oin) has been associated with
worseclinical outcome and a high frequency of
medication-related complications.2,12
Current recommendations are to avoidphenytoin, and, if
desirable, short-termanticonvulsant administration for 3 to7 days
could be administered. In addi-tion, concern exists that the
frequency of subclinical seizures may be high inpatients with
poor-grade SAH, and con-tinuous EEG has been recommended inthis
setting.12
Delayed cerebral ischemia. Delayed
cerebral ischemia is one of the most
dreaded complications after SAH and isthe most important factor
impacting func-
tional outcome.39 Y 41 Delayed cerebral
ischemia occurs in about 30% of pa-
tients with SAH, usually between 4 and
14 days after the onset of symptoms.
Delayed cerebral ischemia is defined as
any neurologic deterioration (focal or
global) presumed secondary to cerebral
ischemia that persists for more than 1
hour and cannot be explained by any
other neurologic or systemic condition.
The latter implies an absence of signif-icant hydrocephalus,
sedation, hypox-
emia, seizures, and electrolyte or renal or
hepatic impairment. Thus, delayed cere-
bral ischemia is a diagnosis of exclusion.Several factors have
been impli-
cated in the pathogenesis of delayed
KEY POINTS
h Anticonvulsant
administration
(particularly phenytoin)
has been associated
with worse
clinical outcome.
h Delayed cerebral ischemia
is defined as any
neurologic deterioration
(focal or global) presumed
secondary to cerebral
ischemia that persists for
more than 1 hour and
cannot be explained by
any other neurologic or
systemic condition.
Case 1-1BThe patient discussed in Case 1-1A continued
to evolve satisfactorily with normal mean cerebral bloodflow
velocities by transcranial Doppler (TCD). On postbleed day 6, TCD
revealed an increase in mean
cerebral blood flow velocity in the right middle cerebral artery
(MCA) to 160 cm/s from 80 cm/s onday 5. The next morning, the
patient developed a sudden onset of left hemiparesis and
confusion.A head CT scan revealed no rebleeding, cerebral edema, or
hydrocephalus. She was given anIV bolus of 500 mL of 0.9% saline
and was started on a norepinephrine drip with some improvementof
her left hemiparesis but without complete resolution. The patient’s
electrolytes, blood urea nitrogen,creatinine, and liver function
tests were normal, and her white blood cell count was 14,000
cells/mm 3.A follow-up TCD after neurologic deterioration showed a
further increase in mean cerebral blood flowvelocity of her right
MCA to 220 cm/s and a Lindegaard ratio (MCA/extracranial internal
carotidartery mean blood flow velocities) of 6. Digital subtraction
angiography (DSA) was performed 90 minutesafter symptom onset,
showing severe vasospasm of her right MCA and anterior cerebral
artery (ACA)(Figure 1-4A). She underwent balloon angioplasty of the
right MCA and subsequent intra-arterialinfusion of nicardipine in
both the right MCA and ACA with radiologic and clinical
improvement(Figure 1-4B). The patient’s neurologic examination
normalized, and her systolic blood pressure wasmaintained at
greater than 180 mm Hg for 3 more days. Her TCD showed improvement
in meancerebral blood flow velocities to less than 100 cm/s by day
9, and the patient was slowly weaned offnorepinephrine by day 10.
On day 11 she developed a decreased level of consciousness without
focalneurologic findings except for limited upward gaze. A
follow-up head CT scan showed communicatinghydrocephalus, and an
external ventricular drain (EVD) was inserted (Figure 1-4C).
Several attempts atweaning the patient off the EVD failed and,
therefore, she underwent programmable ventriculoperitonealshunt
placement (Figure 1-4D) on day 15, after which she was transferred
to the regular floor. Thepatient was discharged to home on day 17,
after clearance by physical and occupational therapies,
withinstructions to continue nimodipine for 4 more days and
schedule follow-up in vascular neurology andneurosurgery outpatient
clinics.
Continued on page 1279
1278 www.ContinuumJournal.com October 2015
Subarachnoid Hemorrhage
Copyright © American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/18/2019 Diagnosis and Management of Subarachnoid
Hemorrhage
17/25
-
8/18/2019 Diagnosis and Management of Subarachnoid
Hemorrhage
18/25
cerebral ischemia, including cerebral va-
sospasm, microcirculatory constriction,
microthrombosis, cortical spreadingdepression, and delayed
cellular apo-
ptosis.39 Most likely, the main driver of
all these processes is the release of oxy-
hemoglobin and erythrocyte contents
through hemolysis, which unleashes a
host of inflammatory and proapoptotic
factors. The risk for cerebral vasospasm
increases with the thickness, density,
location, and persistence of the sub-
arachnoid blood. In addition, poor
clinical grade, loss of consciousness at
ictus, cigarette smoking, cocaine use,SIRS, hyperglycemia, and
hydrocepha-
lus also increase the risk of delayed
cerebral ischemia and poor neurologic
outcome.39,40 However, predicting who
will develop delayed cerebral ischemia
has proven very difficult. The latter has
important implications for the reduc-
tion of level of monitoring in patients
with SAH who are at low risk for delayed
cerebral ischemia, thus avoiding poten-
tial adverse effects of aggressive man-
agement and potentially decreasingresource utilization. The best
predic-
tors for patients requiring less frequent
monitoring include older age (more than
65 years), a WFNSS score of 1 to 3, and
a modified Fisher Scale score less than
3 ( Table 1-5 ).39
Prophylaxis. The best studied of theavailable interventions
aimed at prevent-ing delayed cerebral ischemia are calciumchannel
blockers and intravascular vol-ume status. The use of nimodipine
to
decrease the risk of delayed cerebralischemia and poor
functional outcomeis well supported and recommended( Table
1-5 ).2,12,23,39 Nimodipine is ad-ministered by enteral route
at 60 mgevery 4 hours for 21 days. Nimodipineaffords
neuroprotection without decreas-ing the frequency of angiographic
vaso-spasm. The most common adverse effectsof nimodipine include
constipation and
hypotension. The latter could be prob-lematic as it could lead
to hypoperfusion
due to decreased cerebral perfusion pres-sure (CPP). Therefore,
it is important thatsystolic blood pressure not be compro-mised
when administering nimodipine.One solution employed by the author
isto half the nimodipine dose to 30 mgevery 2 hours while
maintaining ade-quate intravascular volume.
Patients with SAH frequently experi-ence decreased intravascular
volume andnegative fluid balance, which have beenassociated with
higher incidence of cere-
bral infarction and poor neurologic out-come. These findings led
to the institutionof prophylactic hypervolemic therapy.However,
this strategy hasnotbeen shownto improve cerebral blood flow (CBF)
or decrease the frequency of cerebral vaso-spasm or delayed
cerebral ischemia, andit increases the frequency of
cardiopul-monary complications. Therefore, pro-phylactic
hypervolemia should not bepursued. Current recommendations areto
maintain euvolemia at all times after SAH.2,12 It is important
to emphasize
that controversy still exists about themethodology to follow to
determineeuvolemia. Many neurointensivists use acombination of
methods, including strictmonitoring of fluid balance, central
venous pressure, echocardiogram, andstroke volume
variation, among others.In practice, maintenance of euvolemiacan
generally be ensured by replacingurine output and even
administeringfludrocortisone or hydrocortisone in pa-tients with
significant diuresis ( Table 1-5 ).
Diagnosis and monitoring. Diagnos-ing delayed cerebral
ischemia is not easy.However, the combination of
neurologicexamination and imaging studies canenhance the chances of
early detectionandmanagement. Patients with SAHmustbe in the
neurocritical care unit wherethey can be examined very
frequently,preferably at least every 2 hours. Delayedcerebral
ischemia must be suspected
KEY POINTS
h Possible underlying
conditions implicated
in the pathogenesis
of delayed cerebral
ischemia include
cerebral vasospasm,
microcirculatory
constriction,
microthrombosis, cortical
spreading depression, and
delayed cellular apoptosis.
h Nimodipine should be
administered to all
patients with
subarachnoid
hemorrhage to decreasethe risk of delayed
cerebral ischemia
and poor
functional outcome.
h Euvolemia should be
maintained at all times,
while prophylactic
hypervolemia should
be avoided.
1280 www.ContinuumJournal.com October 2015
Subarachnoid Hemorrhage
Copyright © American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/18/2019 Diagnosis and Management of Subarachnoid
Hemorrhage
19/25
when patients with SAH develop focalneurologic impairment
or a decrease
of at least 2 points on the Glasgow ComaScale that lasts for
more than 1 hour and cannot be explained by any
other cause. In addition, all patients with SAHshould undergo
head CT or MRI 24 to48 hours after aneurysm occlusion.Therefore,
any new hypodensities onCT imaging after this period not
attri-butable to EVD insertion or intra-parenchymal hematoma should
beregarded as cerebral infarctions fromdelayed cerebral ischemia
regardless of
clinical signs.
41
The general consensus among prac-titioners indicates that
patients with SAHshould undergo additional imaging
and/or physiologic monitoring routinely duringthe risk period
for delayed cerebral isch-emia ( Table 1-5 ).2,12 Such
monitoring isusually multimodal and includes ICP,CPP, CBF, EEG,
transcranial Doppler (TCD), DSA, CTA, CT perfusion (CTP),and
brain tissue oxygenation. TCD hasbeen the longest and best studied
of allthe monitoring modalities. TCD has
adequate sensitivity and specificity todetect delayed cerebral
ischemia sec-ondary to cerebral vasospasm in largearteries compared
to DSA, but is limitedby the operator’s experience and thepatient’s
cranial windows.42 TCD thresh-olds for vasospasm are the
following:mean cerebral blood flow velocities of less than 120
cm/s for absence and morethan 200 cm/s or a Lindegaard ratio
(MCA mean cerebral blood flow velocity/extra-cranial internal
carotid artery mean
cerebral blood flow velocity) of greater than 6 for
presence. In addition, meancerebral blood flow velocity increases
by more than 50 cm/s within 24 to 48 hoursalso have been
associated with delayedcerebral ischemia.
DSA is the gold standard for detectionof large artery
vasospasm.2,12 CTA hasbecome more widely available and
may replace DSA for screening of vasospasm
with a high degree of specificity. CTPfindings of an
elevated mean transit time
(MTT) of greater than 6.4 seconds may be additive to CTA in
predicting delayedcerebral ischemia and has been recom-mended as a
threshold for decreasedcerebral perfusion. Qualitative visual
in-terpretation of CTP can also be useful.Brain tissue oxygenation
and CBF moni-toring can provide additional information
when used in the context of a multimo-dality approach,
bearing in mind their limitations, such as limited tissue
sam-pling and location in relation to pathology.
Continuous EEG offers the advantage of being able to
monitor broad regions of the brain to detect epileptiform
dis-charges noninvasively. Continuous EEGis particularly useful in
patients with poor-grade SAH where neurologic examina-tion is
limited.
Some variability exists regarding the
timing and frequency of use of the var-
ious neuromonitoring techniques men-tioned above. The author’s
institution
follows an algorithm for identifying andtreating subarachnoid
hemorrhage sim-
ilar to the one proposed by Macdonaldas shown in Figure
1-5.39 Patients with
SAH are stratified into low risk (ie, older age, a WFNSS
score of 1 to 2, and a mod-
ified Fisher Scale score of less than 3),
high risk (ie, a WFNSS score of 1 to 3
and a modified Fisher Scale score of 3),and high risk with poor
neurologic
status (ie, clouded examination due tosedation, a WFNSS score of
3 to 5, anda modified Fisher Scale score of 4). Allpatients with
aneurysmal SAH undergo
TCD (daily or every other day) and headCT/CTA/CTP on admission
and on days3 to 5 and days 7 to 10 for screening of decreased
cerebral perfusion or vaso-spasm. DSA also can be performed inlieu
of CTA/CTP. High-risk patients
with poor neurologic status undergoadditional
neuromonitoring, includ-ing EEG, brain tissue oxygenation, andCBF
determination.
KEY POINTS
h Delayed cerebral
ischemia must be
suspected when patients
with subarachnoid
hemorrhage develop
focal neurologic
impairment or a decrease
of at least 2 points on
the Glasgow Coma Scale
that lasts for more than
1 hour and cannot
be explained
by any other cause.
h Any new hypodensities
on CT imaging 24 to
48 hours after aneurysmtreatment should be
regarded as cerebral
infarctions from delayed
cerebral ischemia.
h Transcranial Doppler
thresholds for vasospasm
include mean cerebral
blood flow velocities of
less than 120 cm/s for
absence and more than
200cm/s or a Lindegaard
ratio of greater than
6 for presence.
h Digital subtraction
angiography is the gold
standard for detection of
large artery vasospasm.
h CT perfusion findings of
elevated mean transit
time of greater than
6.4 seconds may be
additive to CT angiography
in predicting delayed
cerebral ischemia and
has been recommended
as a thresholdfor decreasedcerebral perfusion.
1281Continuum (Minneap Minn) 2015;21(5):1263–1287
www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/18/2019 Diagnosis and Management of Subarachnoid
Hemorrhage
20/25
Management. All of the patients withSAH in the author’s
institution are treated
with nimodipine and euvolemia as men-tioned above
( Table 1-5 ) ( Figure 1-5 ).
Low-risk patients whose neurologic ex-
amination remains unchanged along with absence of vasospasm
and hypo-
perfusion on TCD and CTA/CTP are
considered for transfer to a lower level
of care as early as 5 days post ictus.
High-risk patients who have good
neurologic status and whose neurologic
examination remains unchanged along
with normal TCD and CTA/CTP aretransferred out of the
neurocritical care
unit as early as 7 days after symptom
onset. High-risk patients with poor
neurologic status, whose examination
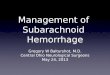
FIGURE 1-5 Management approach to delayed cerebral
ischemia.
BP = blood pressure; CPP = cerebral perfusion pressure; CT =
computed tomography; CTA = computedtomography angiography; CTP =
computed tomography perfusion; DCI = delayed cerebral ischemia;
ICP = intracranial pressure; IVH = intraventricular hemorrhage;
MTT = mean transit time; SAH = subarachnoid hemorrhage;TCD =
transcranial Doppler; WFNSS = World Federation of Neurological
Surgeons Scale.
Reprinted with permission from Macdonald RL, Nat Rev
Neurol.39
B 2014 Macmillan Publishers Limited.
www.nature.com/nrneurol/journal/v10/n1/full/
nrneurol.2013.246.html .
1282 www.ContinuumJournal.com October 2015
Subarachnoid Hemorrhage
Copyright © American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
http://www.nature.com/nrneurol/journal/v10/n1/full/nrneurol.2013.246.htmlhttp://www.nature.com/nrneurol/journal/v10/n1/full/nrneurol.2013.246.htmlhttp://www.nature.com/nrneurol/journal/v10/n1/full/nrneurol.2013.246.htmlhttp://www.nature.com/nrneurol/journal/v10/n1/full/nrneurol.2013.246.htmlhttp://www.nature.com/nrneurol/journal/v10/n1/full/nrneurol.2013.246.html
-
8/18/2019 Diagnosis and Management of Subarachnoid
Hemorrhage
21/25
remains unchanged, and all neuro-
monitoring values remain within normal
limits, are considered for transfer to alower level of care 14
days after SAH. If at any given time low-risk or
high-risk patients develop elevated TCD mean ce-rebral blood
flow velocities or abnormalCTA/CTP, the intensity and frequency
of neurologic monitoring is escalated.
Once patients experience neuro-
logic deterioration suggestive of delayed
cerebral ischemia, rescue therapies are
initiated. Current guidelines indicate
that induced hypertension is indicated
( Table 1-5 ) ( Figure 1-5 ).
2,12
At the au-thor’s institution, typically, an IV fluid
bolus (1 to 2 liters of 0.9% saline) is ad-
ministered and hypertension is induced
with norepinephrine as our drug of
choice. Blood pressure augmentation
progresses in stepwise fashion with fre-
quent assessment of neurologic functionat each 10 mm Hg change
in systolic(up to 200 mm Hg) or mean arterialblood pressures to
determine whether a higher blood pressure target is needed.The
author’s institution reserves the use
of inotropes (dobutamine or milrinone)for those patients with
known poor car-diac function. If neurologic deficits per-sist, then
the patient undergoes CT/CTA/ CTP or DSA with subsequent
endovas-cular therapy once cerebral vasospasmis confirmed.
Endovascular treatmentusing intra-arterial vasodilators
and/or angioplasty is supported by prospectiveand
retrospective observational data andis currently recommended
( Table 1-5 ).2,12
Induced hypertension is maintained
for at least 72 hours or until stability isachieved and is
slowly weaned off after that. We do not perform
prophylacticangioplasty when cerebral vasospasmis discovered during
the screeningCT/CTA/CTP or DSA without neurologicdeterioration
because this practice isassociated with higher
complicationrates.2,12 In high-risk patients with
poor neurologic status, diagnosis and treat-
ment of delayed cerebral ischemia may be somewhat
subjective and mostly
based on neuromonitoring findings.The protocol at the author’s
institu-tion dictates induced hypertensionand CT/CTA/CTP or DSA
when thesepatients experience elevated TCD meancerebral blood flow
velocities indica-tive of vasospasm, abnormal brain tis-sue
oxygenation, or CBF ( Figure 1-5 ).
Medical Complications
Cardiopulmonary. Cardiopulmonary al-
terations are among the most common
systemic complications of SAH and canrange from minor ECG
changes to se-
vere dilated cardiomyopathy and acute
respiratory distress syndrome (ARDS).38
ECG alterations and cardiac enzyme
(troponin T) elevations are quite frequent
after SAH and, depending on their se-
verity, are also significant surrogates for
clinical outcome. ECG changes include
sinus tachycardia, peaked T waves, T-wave
inversions, ST segment depression or
elevation, and QT prolongation. Tro-
ponin elevation can be seen in up to30% of patients. The exact
pathogenesis
behind cardiac abnormalities is not com-
pletely understood but may reflect a
catecholamine-related myocardial injury.
Echocardiogram can help differentiate
patients with diffuse cardiac dysfunction
related to SAH from those with underly-
ing cardiac ischemia showing regional
wall motion abnormalities restricted to
the territory of a coronary vessel. Clin-
ically, patients with SAH can develop sig-
nificant cardiac dysfunction manifestingas left ventricular
failure, with impairedcardiac output, hypotension, and pul-
monary edema. These cardiovascular
dysfunctions can lead to severe hypo-
perfusion, reduced CPP or brain tissue
oxygenation, with added catastrophic
consequences for an already-injured
brain prone to delayed cerebral ische-
mia and poor neurologic outcome.
KEY POINTS
h Once patients experience
neurologic deterioration
suggestive of delayed
cerebral ischemia, rescue
therapies are initiatedwith
induced hypertension as
first-line modality.
h In high-risk patients
with poor neurologic
status, diagnosis and
treatment of delayed
cerebral ischemia may
be somewhat subjective
and mostly based on
neuromonitoring findings.
h Cardiopulmonary
alterations are
among the most
common systemic
complications of
subarachnoidhemorrhage.
1283Continuum (Minneap Minn) 2015;21(5):1263–1287
www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/18/2019 Diagnosis and Management of Subarachnoid
Hemorrhage
22/25
The term stunned myocardium hasbeen applied to patients with SAH
who
present with hypoxemia and cardiogenicshock with pulmonary edema
withinhours of disease onset. Takotsubo cardio-myopathy (typically
characterized by apicalballooning on echocardiogram) can beseen in
those patients with poor neuro-logic status and increases the risk
of
delayed cerebral ischemia.12 Current rec-
ommendations for the treatment of pul-
monary edema or ARDS in patients with
SAH are to avoid excessive fluid intake
and to use diuretics judiciously to target
euvolemia. In addition, standard man-
agement of heart failure is indicated,
keeping in mind that CPP should be main-
tained within normal limits.12 Although
lung-protective mechanical ventilation
should be tried whenever possible, hy-
percarbia should be closely monitored
and managed to avoid ICP elevations.
Cardiopulmonary function should be
supported, even with the insertion of an
intra-aortic balloon pump if necessary,as these abnormalities
usually improve
a few days after onset.
Fever. Fever is the most common non-neurologic complication
of SAH, occur-ring in up to 70% of patients during
their hospitalization.2,12 Fever is more likely to occur
in patients with poor neuro-logic status and higher modified
Fisher Scale scores. Fever in SAH has been as-sociated with
poor clinical outcome andis more likely related to SIRS rather
thaninfectious in origin. There is currently no clear evidence
indicating that fever control is beneficial for patients
with
SAH. However, current recommenda-tions are to monitor body
temperaturefrequently and to seek and treat infec-tious processes.
In addition, during theperiod of risk for delayed cerebral
ische-mia, fever control should be achieved ina stepwise fashion
starting with standardantipyretic medications and escalating
tosurface cooling or intravascular devices
while avoiding shivering.
Thromboembolism. The incidenceof deep venous thrombosis
(DVT) after
SAH ranges from 2% to 20% dependingon the screening methodology
used.12
The risk of DVT is higher in patients withpoor neurologic
status. Because of thehigh incidence of DVT and its
potentiallife-threatening consequences, prophy-laxis should be
administered to allpatients with SAH. Sequential compres-sion
devices are recommended for allpatients with SAH ( Table
1-5 ). The useof unfractionated heparin for prophy-laxis is
indicated after aneurysm obliter-
ation and can be started 24 hours after the
procedure.Glucose abnormalities. Hyperglyce-
mia is a common phenomenon follow-ing SAH. Its real impact is
still unclear,but hyperglycemia has been associated
with the development of delayed cere-bral ischemia and
poor clinical outcome.Hypoglycemia also is associated with
worse clinical outcome. The methods,timing, and
aggressiveness of glucosecontrol are not well studied in
patients
with SAH. Current recommendations
are to maintain a blood glucose between80 mg/dL and 200 mg/dL
pending further investigations ( Table 1-5 ).12
Hyponatremia. Hyponatremia is themost common electrolyte
disorder inSAH and can occur in about 30% of pa-tients.2,12,15
Hyponatremia has been as-sociated with development of
delayedcerebral ischemia and poor clinical out-come. Hyponatremia
can be secondary to cerebral salt wasting or
inappropriatesecretion of antidiuretic hormone. Tra-
ditionally, in patients without SAH, theformer is treated with
volume infusionand the latter with fluid restriction. How-ever,
because determination of fluid statuscan be difficult in the
neurocritical careunit and because hypovolemia is asso-ciated with
poor clinical outcome, fluidrestriction should be avoided in
patients
with SAH. Treatment goals for hypona-tremia in SAH should
be oral free water
KEY POINTS
h Pulmonary edema or
acute respiratory distress
syndrome in patients
with subarachnoid
hemorrhage should be
treated with judicious
use of diuretics and other
standard heart failure
therapies targeting
euvolemia and normal
cerebral perfusion pressure.
h Fever is the most
common non-neurologic
complication in
patients with
subarachnoid hemorrhage.
h Fever in patients with
subarachnoid hemorrhage
has been associated with
poor clinical outcome.
h Deep venous thrombosis
prophylaxis should be
administered to all
patients with
subarachnoidhemorrhage.
1284 www.ContinuumJournal.com October 2015
Subarachnoid Hemorrhage
Copyright © American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/18/2019 Diagnosis and Management of Subarachnoid
Hemorrhage
23/25
restriction while maintaining euvolemia.Patients can be treated
with continuous
infusion of hypertonic saline (1.5% to 3%)and fludrocortisone if
diuresis is activeand impedes maintenance of adequate
fluid balance. It is important to test for
thyroid and adrenal dysfunction, partic-
ularly in those patients with SAH who
require vasopressors to maintain blood
pressure goals.
Hemoglobin. The majority of patients with SAH
experience a drop in hemo-globin during hospitalization, which
couldbe due to several factors, including ex-
cessive blood draws, blood loss for other reasons, or
systemic inflammation.12 Ane-mia has been associated with
delayedcerebral ischemia and poor clinical out-come in patients
with SAH. However,the optimal hemoglobin concentrationin patients
with SAH has not been deter-mined, and whether blood
transfusionimproves clinical outcome remains tobe proven. Current
recommendationsare to minimize blood loss from blooddrawing and to
maintain a hemoglobinconcentration of above 8 g/dL to 10 g/dL
( Table 1-5 ).
CONCLUSION
SAHis a neurologic emergency associated
with high morbidity and mortality. SAHis more frequent in
women than menand more frequent in minority popula-tions compared
to white Americans. Themain areas of emphasis when caring
for
patients with SAH should be the fol-lowing: prompt evaluation
and diagnosis,immediate transfer to appropriate centers,
expeditiousdiagnosis and treatment of thebleeding source, and
overall good neuro-
critical care adhering to available treatmentguidelines. The
main neurologic com-plications of SAH include
hydrocephalus,seizures, cerebraledema, delayed cerebral
ischemia, and neuroendocrine disorders.Patients with SAH
frequently experiencecardiopulmonary complications, whichcan be
life threatening.
REFERENCES1. Go AS, Mozaffarian D, Roger VL, et al. Heart
disease and stroke statistics V 2014 update:a report
from the AmericanHeart Association.
Circulation 2014;129(3):e28 Y e292.
doi:10.1161/01.cir.0000441139.02102.80.
2. Connolly ES Jr, Rabinstein AA, Carhuapoma JR,
et al Guidelines for the management
of aneurysmal subarachnoid hemorrhage: a
guideline for healthcare professionals from
the American Heart Association/American
Stroke Association. Stroke 2012;43(6):1711 Y 1737.
doi:10.1161/STR.0b013e3182587839.
3. Lovelock CE, Rinkel GJ, Rothwell PM. Time
trends in outcome of subarachnoid hemorrhage:
population-based study and systematic review.
Neurology 2010;74(19):1494 Y 1501.
doi:10.1212/
WNL.0b013e3181dd42b3.
4. Tjahjadi M, Heinen C, Konig R, et al.
Health-related quality of life after
spontaneous subarachnoid hemorrhage
measured in a recent patient population.
World Neurosurg 2013;79(2):296 Y 307.
doi:10.1016/j.wneu.2012.10.009.
5. Lo B, Macdonald RL. Health-related quality of
life after aneurysmal subarachnoid hemorrhage:
new data from a large series in Germany.
World Neurosurg 2013;79(2):243 Y 244.
doi:10.1016/j.wneu.2012.12.025.
6. Broderick JP, Brown RD Jr, Sauerbeck L,
et al. Greater rupture risk for familial as
compared to sporadic unruptured intracranial
aneurysms. Stroke 2009;40(6):1952 Y 1957.
doi:10.1161/STROKEAHA.108.542571.
7. Lindner SH, Bor AS, Rinkel GJ. Differences in risk
factors according to the site of intracranial
aneurysms.J Neurol NeurosurgPsychiatry 2010;
81(1):116 Y 118. doi:10.1136/jnnp.2008.163063.
8. Etminan N, Beseoglu K, Steiger HJ, Hanggi D.
The impact of hypertension and nicotine on
the size of ruptured intracranial aneurysms.
J Neurol Neurosurg Psychiatry 2011;82(1):4 Y 7.
doi:10.1136/jnnp.2009.199661.
9. Shiue I, Arima H, Anderson CS; ACROSS
Group. Life events and risk of subarachnoid
hemorrhage: the Australasian Cooperative
Research on Subarachnoid Hemorrhage Study
(ACROSS). Stroke 2010;41(6):1304 Y 1306.
doi:10.1161/STROKEAHA.109.575282.
10. Andreasen TH, Bartek J Jr, Andresen M,
et al. Modifiable risk factors for aneurysmal
subarachnoid hemorrhage. Stroke 2013;
44(12):3607 Y 3612. doi:10.1161/STROKEAHA.
113.001575.
11. Edlow JA, Malek AM, Ogilvy CS. Aneurysmal
subarachnoid hemorrhage: update for
emergency physicians. J Emerg Med 2008;
34(3):237 Y 251. doi:10.1016/j.jemermed.
2007.10.003.
KEY POINTS
h Fluid restriction should
be avoided in patients
with subarachnoid
hemorrhage, and
hyponatremia should be
treated with oral free
water restriction while
maintaining euvolemia.
h Anemia in patients with
subarachnoidhemorrhage
has been associated
with delayed cerebral
ischemia and worse
clinical outcome.
1285Continuum (Minneap Minn) 2015;21(5):1263–1287
www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized
reproduction of this article is prohibited.
-
8/18/2019 Diagnosis and Management of Subarachnoid
Hemorrhage
24/25
12. Diringer MN, Bleck TP, Claude Hemphill J 3rd,
et al. Critical care management of patients
following aneurysmal subarachnoid
hemorrhage: recommendations from theNeurocritical Care Society’s
Multidisciplinary
Consensus Conference. Neurocrit Care
2011;15(2):211 Y 240. doi:10.1007/
s12028-011-9605-9.
13. Molyneux A, Kerr R, Stratton I, et al.
International Subarachnoid Aneurysm Trial
(ISAT) of neurosurgical clipping versus
endovascular coiling in 2143 patients with
ruptured intracranial aneurysms: a randomized
trial. Lancet 2002;360(9342):1267 Y 1274.
doi:10.1016/S0140-6736(02)11314-6.
14. Molyneux AJ, Kerr RS, Yu LM, et al.
International Subarachnoid Aneurysm Trial
(ISAT) of neurosurgical clipping versus
endovascular coiling in 2143 patients withruptured intracranial
aneurysms: a randomised
comparison of effects on survival, dependency,
seizures, rebleeding, subgroups, and
aneurysm occlusion. Lancet 2005;366(9488):
809 Y 817. doi:10.1016/S0140-6736(02)11314-6.
15. Suarez JI, Tarr RW, Selman WR. Aneurysmal
subarachnoid hemorrhage. N Engl J Med
2006;354(4):387 Y 396. doi:10.1056/
NEJMra052732.
16. Hassan A, Lanzino G, Wijdicks EF, et al.
Terson’s syndrome. Neurocrit Care 2011;15(3):
554 Y 558. doi:10.1007/s12028-011-9555-2.
17. McCarron MO, Alberts MJ, McCarron P. A
systematic review of Terson’s syndrome:
frequency and prognosis after subarachnoidhemorrhage. J Neurol
Neurosurg Psychiatry
2004;75(3):491 Y 493. doi:10.1136/
jnnp.2003.016816.
18. Linn FH, Wijdicks EF, van der Graaf Y, et al.
Prospective study of sentinel headache in
aneurysmal subarachnoid haemorrhage.
Lancet 1994;344(8922):590 Y 593.
doi:10.1016/
S0140-6736(94)91970-4.
19. Leblanc R. The minor leak preceding
subarachnoid hemorrhage. J Neurosurg
1987;66(1):35 Y 39.
20. Sames TA, Storrow AB, Finkelstein JA,
Magoon MR. Sensitivity of new-generation
computed tomography in subarachnoid
hemorrhage. Acad Emerg Med
1996;3(1):16 Y 20.doi:10.1111/j.1553-2712.1996.tb03296.x.
21. Boesiger BM, Shiber JR. Subarachnoid
hemorrhage diagnosis by computedtomography
and lumbar puncture: are fifth generation CT
scanners better at identifying subarachnoid
hemorrhage? J Emerg Med 2005;29(1):23 Y 27.
doi:10.1016/j.jemermed.2005.02.002.
22. Raya AK, Diringer MN. Treatment of
subarachnoid hemorrhage. Crit Care Clin 2014;
30(4):719 Y 733. doi:10.1016/j.ccc.2014.06.004.
23. Rabinstein AA, Lanzino G, Wijdicks EF.
Multidisciplinary management and emerging
therapeutic strategies in aneurysmal
subarachnoid haemorrhage. Lancet
Neurol2010;9(5):504 Y 519. doi:10.1016/
S1474-4422(10)70087-9.
24. Perry JJ, Sivilotti ML, Stiell IG, et al. Should
spectrophotometry be used to identify
xanthochromia in the cerebrospinal fluid
of alert patients suspected of having
subarachnoid hemorrhage? Stroke
2006;37(10):2467 Y 2472. doi:10.1161/
01.STR.0000240689.15109.47.
25. McKinney AM, Palmer CS, Truwit CL, et al.
Detection of aneurysms by 64-section
multidetector CT angiography in patients
acutely suspected of having an intracranial
aneurysm and comparison with digital
subtraction and 3D rotational angiography.AJNR Am J Neuroradiol
2008;29(3):594 Y 602.
doi:10.3174/ajnr.A0848.
26. Donmez H, Serifov E, Kahriman G, et al.
Comparison of 16-row multisliceCT angiography
with conventional angiography for detection
and evaluation of intracranial aneurysms.
Eur J Radiol 2011;80(2):455 Y 461.
doi:10.1016/
j.ejrad.2010.07.012.
27. DupontSA, Lanzino G, Wijdicks EF,Rabinstein AA.
The use of clinical and routine imaging data
to differentiate between aneurysmal and
nonaneurysmal subarachnoid hemorrhage
prior to angiography. Clinical article.
J Neurosurg 2010;113(4):790 Y 794.
doi:10.3171/2010.4.JNS091932.
28. Kowalski RG, Claassen J, Kreiter KT, et al.Initial
misdiagnosis and outcome after
subarachnoid hemorrhage. JAMA 2004;291(7):
866 Y 869. doi:10.1001/jama.291.