Embed Size (px)
Citation preview
Sept 2012 NZSTM: Malaria Prevention Slide 1
Malaria Prevention
Alan J. Magill MD, FACP, FIDSA, FASTMH
Emeritus, Division of Experimental Therapeutics
Walter Reed Army Institute of Research
Sept 2012 NZSTM: Malaria Prevention Slide 2
Disclaimer
• The opinions presented in this lecture are
those of the author and do not reflect the
official views of WRAIR or the US
Department of Defense.
• COL Magill has no financial conflict of
interests to declare.
• Use of FDA approved drugs for a non
approved indication will be discussed:
– primaquine
Sept 2012 NZSTM: Malaria Prevention Slide 3
Sept 2012 NZSTM: Malaria Prevention Slide 4
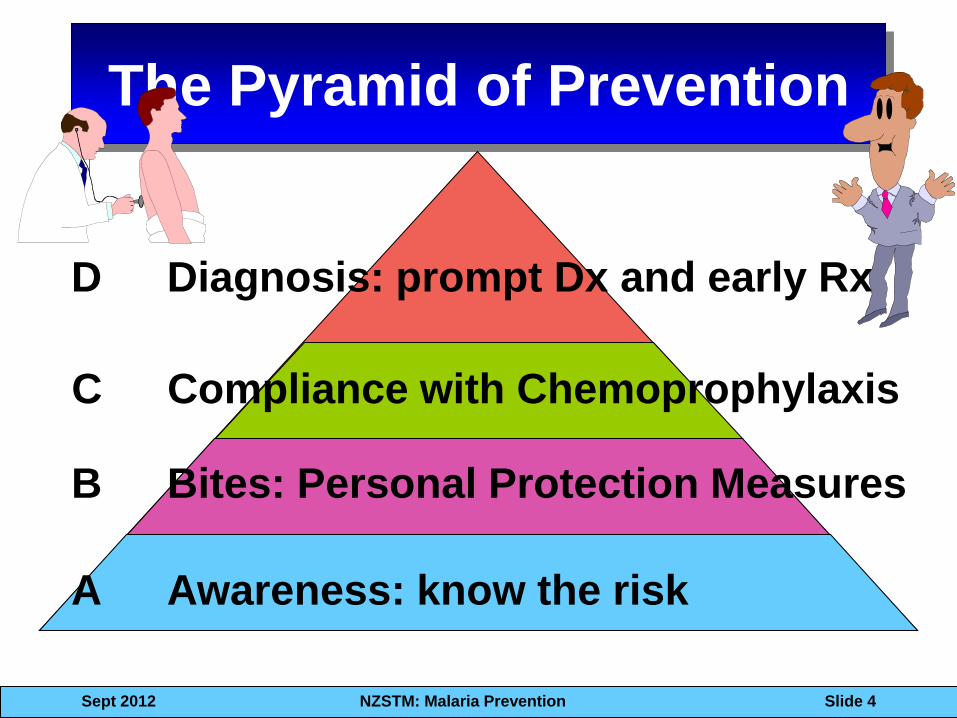
The Pyramid of Prevention
B Bites: Personal Protection Measures
A Awareness: know the risk
C Compliance with Chemoprophylaxis
D Diagnosis: prompt Dx and early Rx
Sept 2012 NZSTM: Malaria Prevention Slide 5
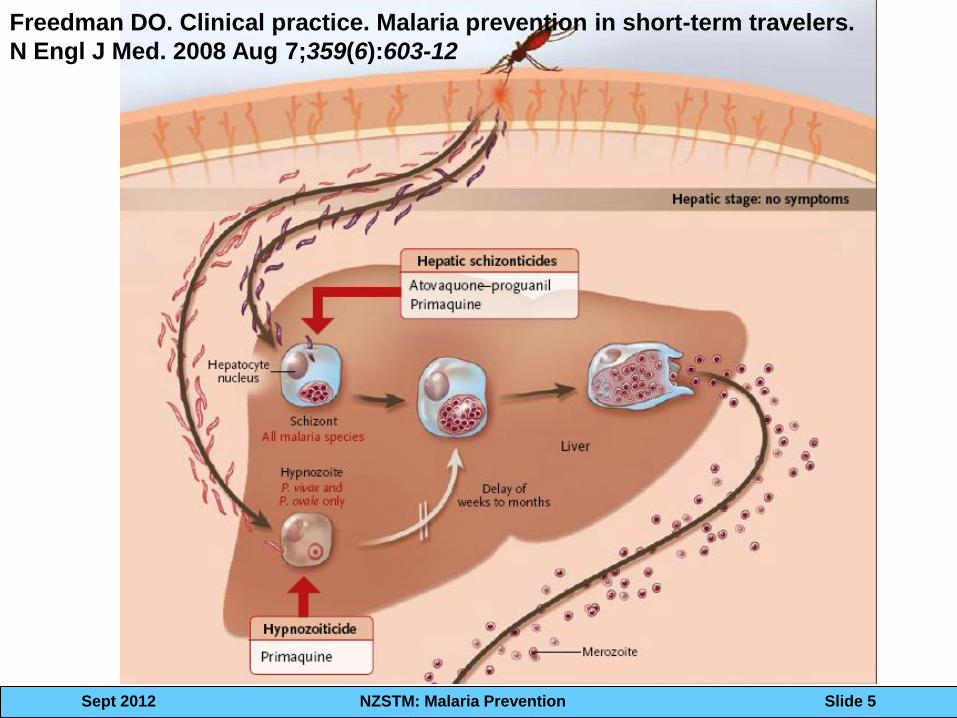
Freedman DO. Clinical practice. Malaria prevention in short-term travelers.
N Engl J Med. 2008 Aug 7;359(6):603-12
Sept 2012 NZSTM: Malaria Prevention Slide 6
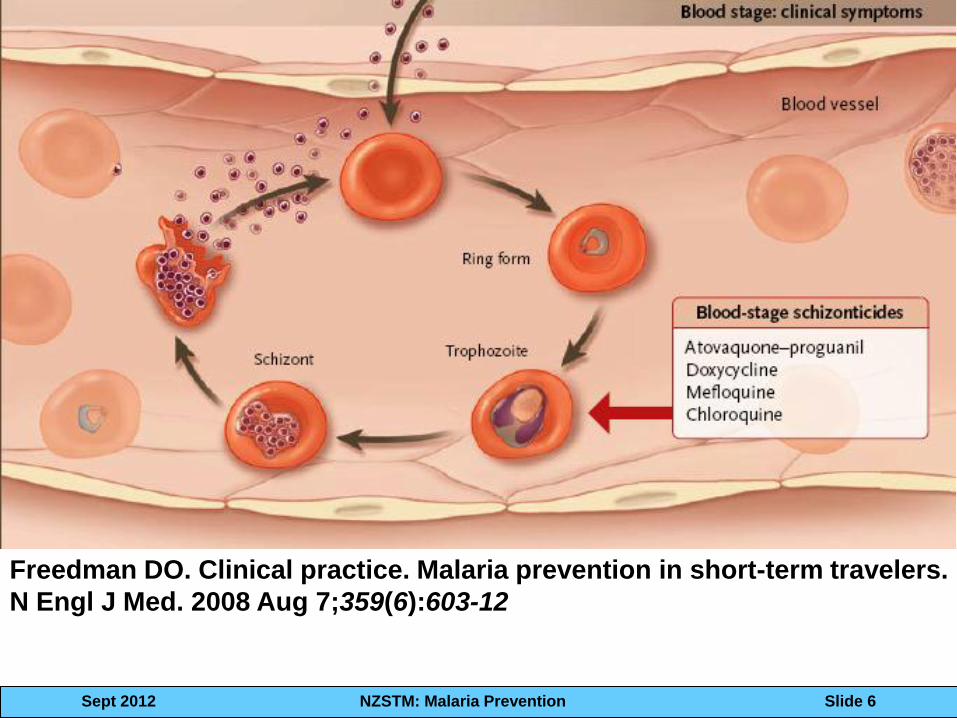
Freedman DO. Clinical practice. Malaria prevention in short-term travelers.
N Engl J Med. 2008 Aug 7;359(6):603-12
Sept 2012 NZSTM: Malaria Prevention Slide 7
What is the best way to
prevent infection?
Don’t get bitten!!
Sept 2012 NZSTM: Malaria Prevention Slide 8
Sept 2012 NZSTM: Malaria Prevention
The mercurial malariologist, Sir Ronald Ross:
“I myself have been
infected with malaria
only once in spite of
nineteen years service
in India and thirteen
subsequent malaria
expeditions to warm
climates; I attribute this
good fortune to my
scrupulous use of the
bed net”
Ross R. Memoirs with a full account of the great malaria problem and its
solution. London: Murray, 1923.
Slide 9
Sept 2012 NZSTM: Malaria Prevention Slide 10
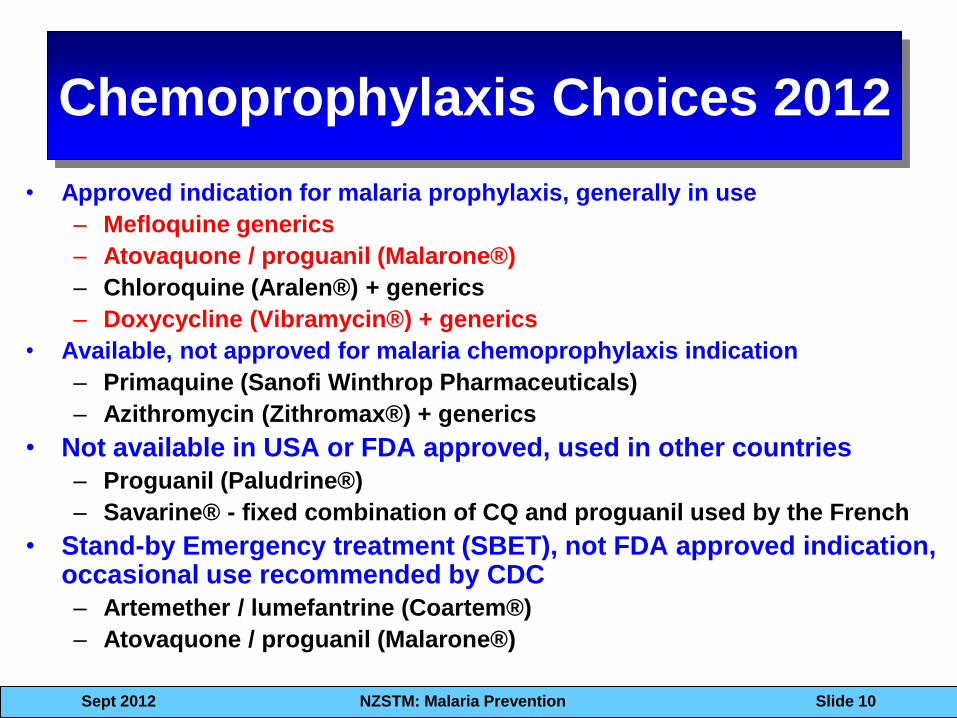
Chemoprophylaxis Choices 2012
• Approved indication for malaria prophylaxis, generally in use
– Mefloquine generics
– Atovaquone / proguanil (Malarone®)
– Chloroquine (Aralen®) + generics
– Doxycycline (Vibramycin®) + generics
• Available, not approved for malaria chemoprophylaxis indication
– Primaquine (Sanofi Winthrop Pharmaceuticals)
– Azithromycin (Zithromax®) + generics
• Not available in USA or FDA approved, used in other countries
– Proguanil (Paludrine®)
– Savarine® - fixed combination of CQ and proguanil used by the French
• Stand-by Emergency treatment (SBET), not FDA approved indication, occasional use recommended by CDC
– Artemether / lumefantrine (Coartem®)
– Atovaquone / proguanil (Malarone®)
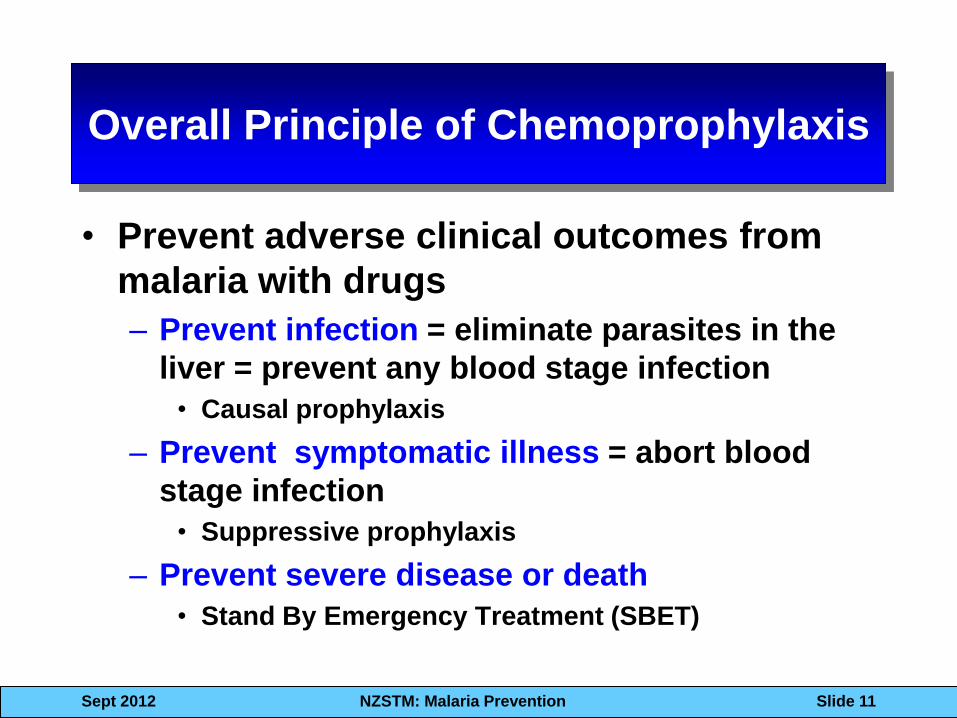
Overall Principle of Chemoprophylaxis
• Prevent adverse clinical outcomes from
malaria with drugs
– Prevent infection = eliminate parasites in the
liver = prevent any blood stage infection
• Causal prophylaxis
– Prevent symptomatic illness = abort blood
stage infection
• Suppressive prophylaxis
– Prevent severe disease or death
• Stand By Emergency Treatment (SBET)
Sept 2012 NZSTM: Malaria Prevention Slide 11
Sept 2012 NZSTM: Malaria Prevention Slide 12
Causal Prophylaxis
• Causal drugs do not need to be given more than 7 days after last exposure
• Atovaquone-proguanil
• primaquine Atovaquone- Proguanil
Primaquine
Liver Schizont
Sept 2012 NZSTM: Malaria Prevention Slide 13
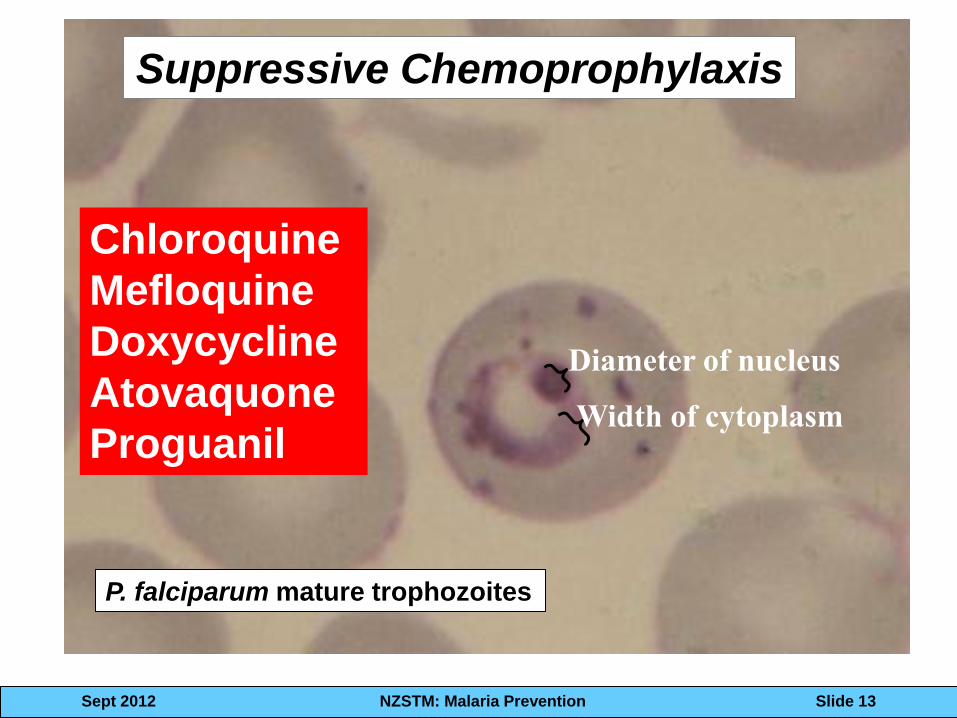
P. falciparum mature trophozoites
Chloroquine
Mefloquine
Doxycycline
Atovaquone
Proguanil
Suppressive Chemoprophylaxis
Width of cytoplasm
Diameter of nucleus
Sept 2012 NZSTM: Malaria Prevention Slide 14
Suppressive
Chemoprophylaxsis
• Doxy and mefloquine need to be
taken for 28 days after last exposure.
– 28 pills of doxy, once daily
– 4 pills of MQ once weekly
– Absent DOT, it won’t happen
Sept 2012 NZSTM: Malaria Prevention Slide 16
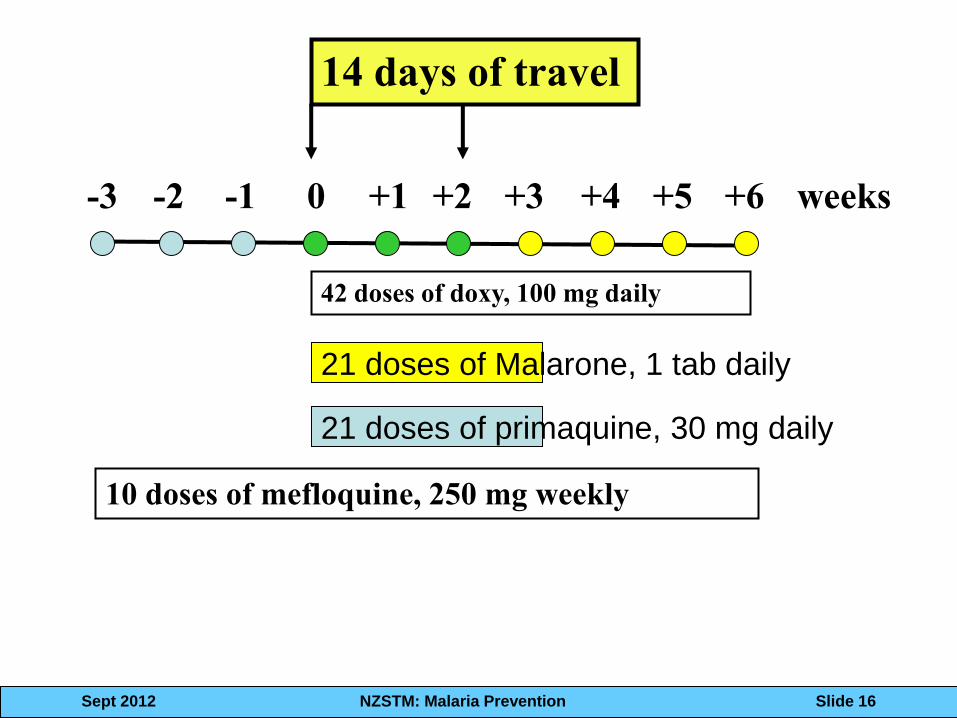
-2 -1 +1 0 +2 +3 +4 weeks
42 doses of doxy, 100 mg daily
14 days of travel
-3 +5 +6
10 doses of mefloquine, 250 mg weekly
21 doses of primaquine, 30 mg daily
21 doses of Malarone, 1 tab daily
1st question: Does this traveler
need to take malaria prophylaxis?
• Yes or No
• Most of us default this
decision to “guidelines”
– CDC Yellow Book
– Commercial services (e.g.
Travex®)
– WHO green book
– CATMAT
• Guidelines differ! Sept 2012 NZSTM: Malaria Prevention Slide 16
Sept 2012 NZSTM: Malaria Prevention Slide 17
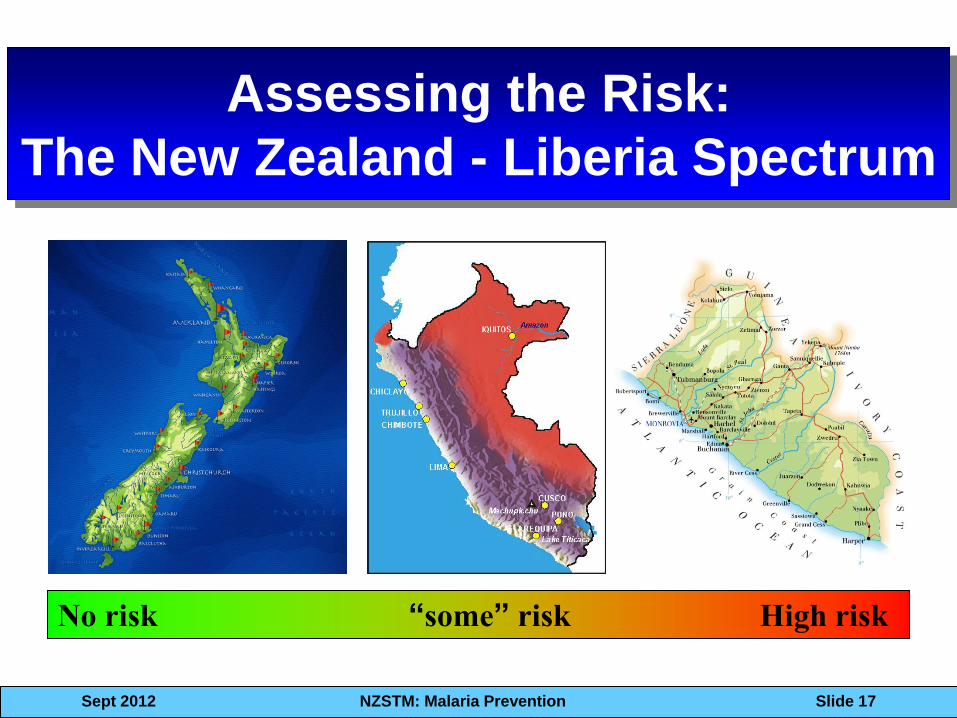
Assessing the Risk:
The New Zealand - Liberia Spectrum
No risk “some” risk High risk
Sept 2012 NZSTM: Malaria Prevention Slide 18
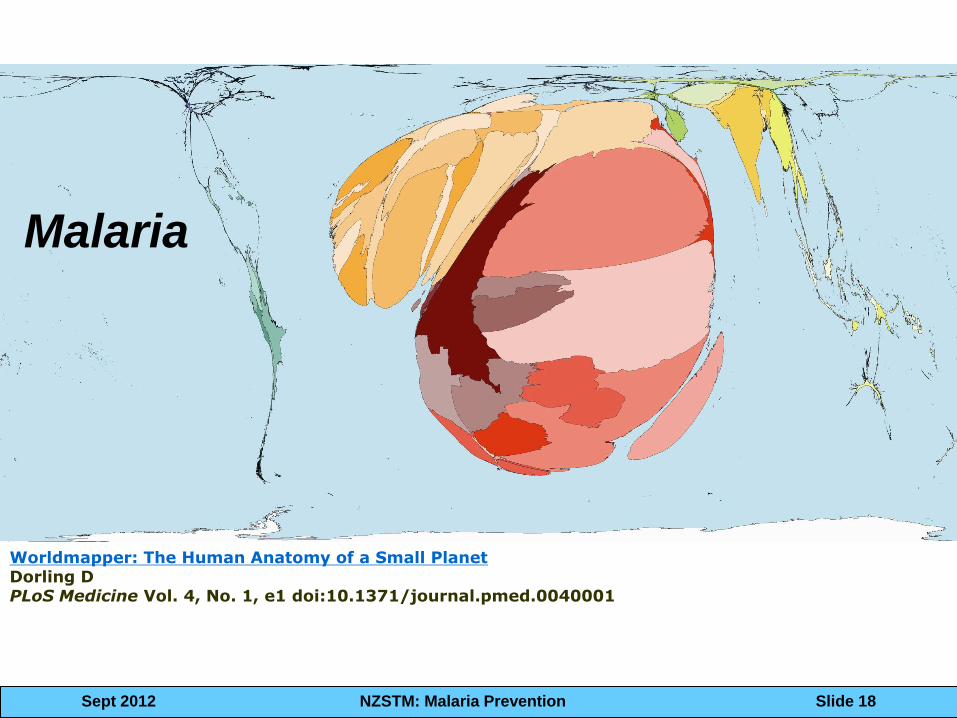
Worldmapper: The Human Anatomy of a Small Planet Dorling D PLoS Medicine Vol. 4, No. 1, e1 doi:10.1371/journal.pmed.0040001
Malaria
Sept 2012 NZSTM: Malaria Prevention Slide 19
Malarious Places
• High risk, all or most of the time
– West Africa
• Seasonal risk
– Mali, Peru
• Very low risk, but not zero risk
– Latin America
Sept 2012 NZSTM: Malaria Prevention Slide 20
Malarious Places
• Unpredictable, very focal risk
• Wide range of “data” and “facts”
• Non-expert cannot know what is
truth
• We default to recommending
prophylaxis because we cannot
assess individual risk
Sept 2012 NZSTM: Malaria Prevention Slide 21
What is the risk of malaria for
the individual traveler?
Destination
Sleeping Activities
Behaviors
Sept 2012 NZSTM: Malaria Prevention Slide 22
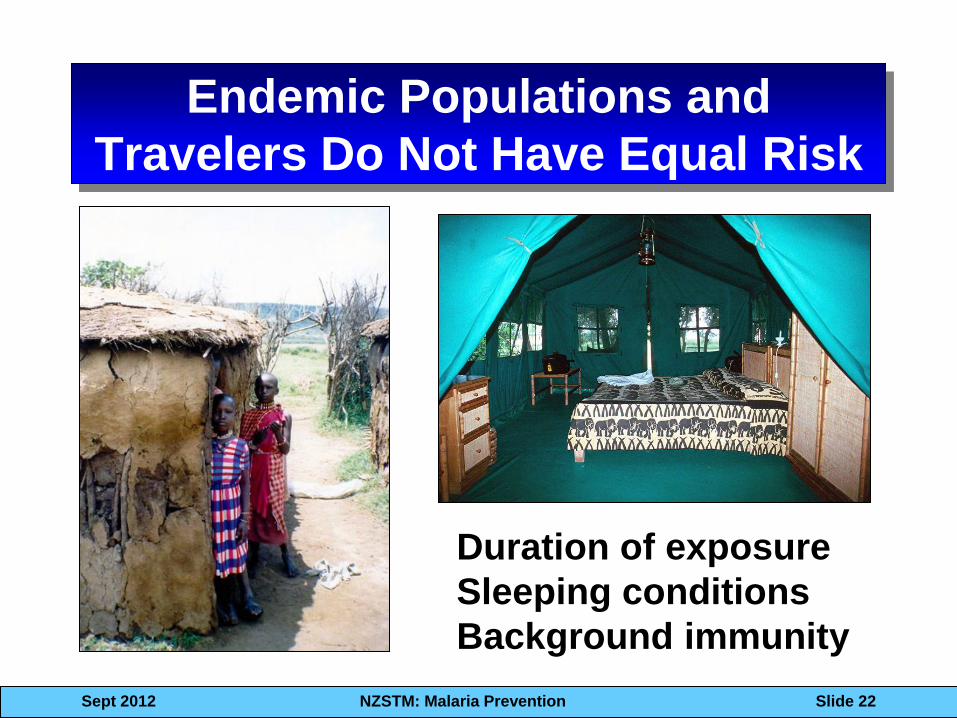
Endemic Populations and
Travelers Do Not Have Equal Risk
Duration of exposure
Sleeping conditions
Background immunity
Sept 2012 NZSTM: Malaria Prevention Slide 23
Risk of Malaria in Travelers
Two surveillance
networks specifically
focused on travelers
http://www.tropnet.net/
http://www.istm.org/geosentinel/main.html
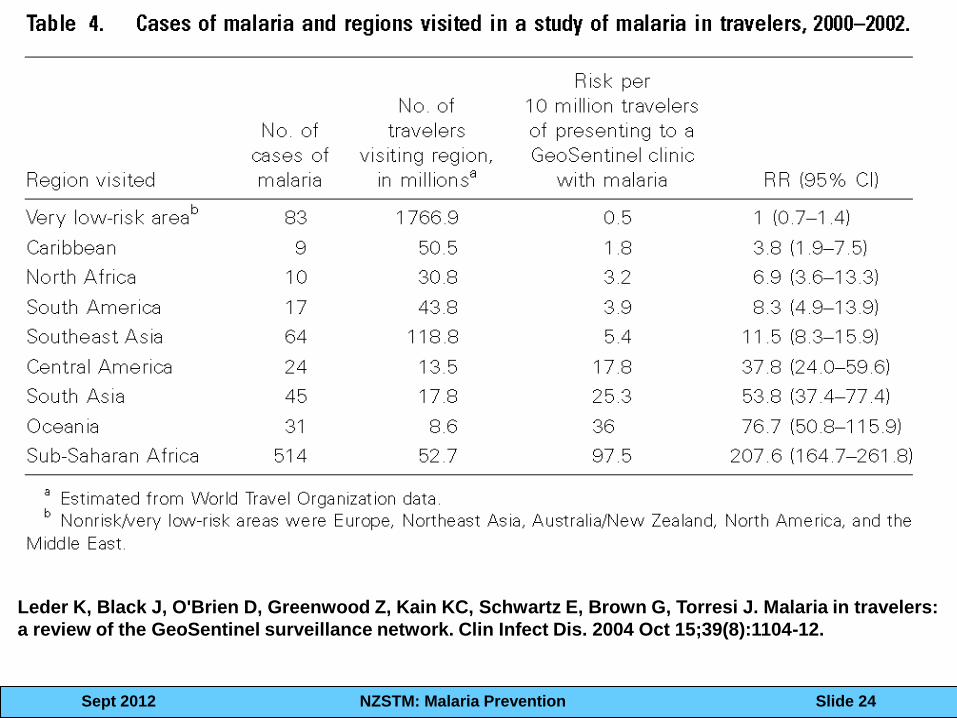
Sept 2012 NZSTM: Malaria Prevention Slide 24
Leder K, Black J, O'Brien D, Greenwood Z, Kain KC, Schwartz E, Brown G, Torresi J. Malaria in travelers:
a review of the GeoSentinel surveillance network. Clin Infect Dis. 2004 Oct 15;39(8):1104-12.
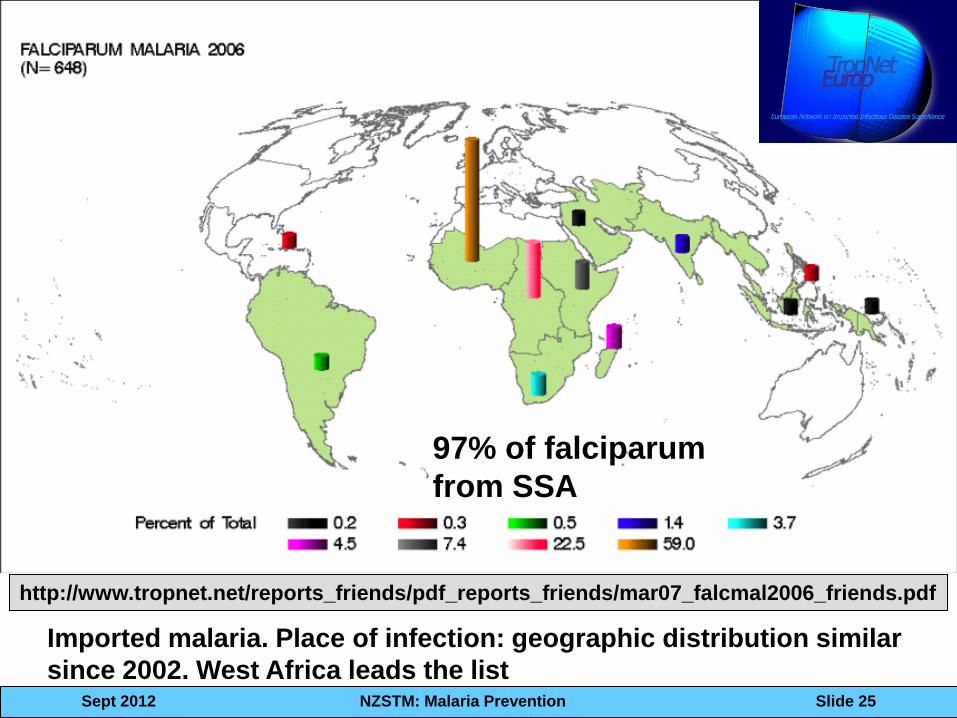
Sept 2012 NZSTM: Malaria Prevention Slide 25
http://www.tropnet.net/reports_friends/pdf_reports_friends/mar07_falcmal2006_friends.pdf
Imported malaria. Place of infection: geographic distribution similar
since 2002. West Africa leads the list
97% of falciparum
from SSA
Sept 2012 NZSTM: Malaria Prevention Slide 69
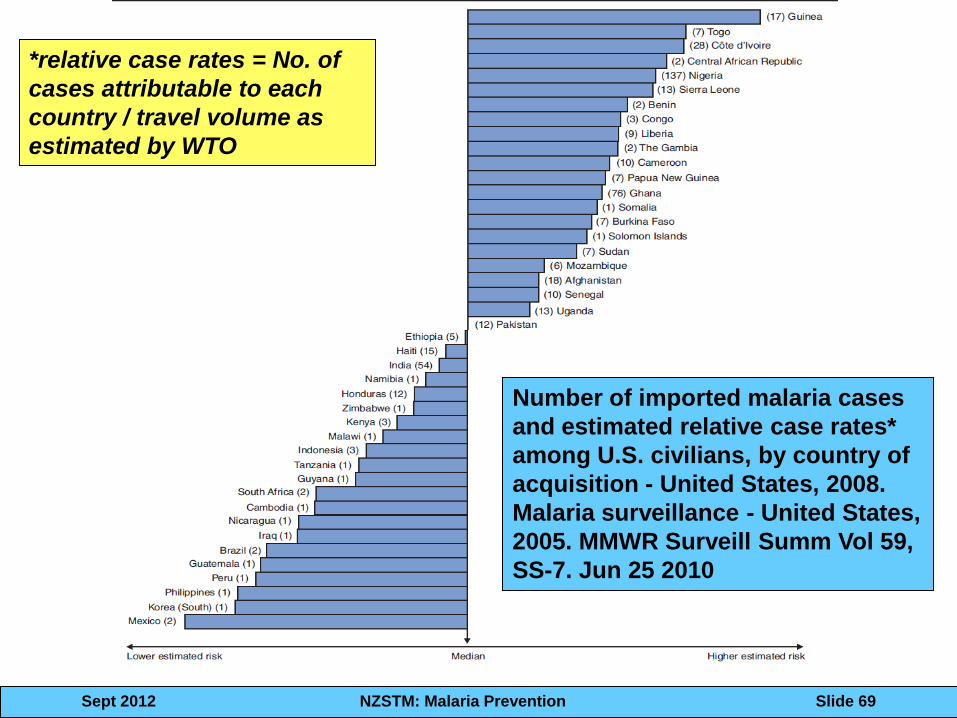
Number of imported malaria cases
and estimated relative case rates*
among U.S. civilians, by country of
acquisition - United States, 2008.
Malaria surveillance - United States,
2005. MMWR Surveill Summ Vol 59,
SS-7. Jun 25 2010
*relative case rates = No. of
cases attributable to each
country / travel volume as
estimated by WTO
Sept 2012 NZSTM: Malaria Prevention Slide 27
Chemoprophylaxis: The Big 3
Mefloquine Doxycycline Atovaquone-
proguanil
Sept 2012 NZSTM: Malaria Prevention Slide 28
How do we choose
Chemoprophylaxis Drugs?
For CQ resistant P. falciparum destinations…
3 choices of: Malarone®, mefloquine and
doxycycline • Listed alphabetically • All considered efficacious • Choice based on tolerability
Sept 2012 NZSTM: Malaria Prevention Slide 29
How do we choose
Chemoprophylaxis Drugs?
http://www.cdc.gov/travel/yb/ http://www.who.int/ith/en/
Sept 2012 NZSTM: Malaria Prevention Slide 30
Remember!
Your patient is asymptomatic
This is a trip of a lifetime
They are spending a lot of money
When choosing a chemoprophylaxis drug…….
Sept 2012 NZSTM: Malaria Prevention Slide 31
Mefloquine
• Lariam® is very efficacious
• Not tolerated by some
• Neurotoxicity concerns
• Screen patients
– Have taken MQ before w/o problems
– Careful education, consider options
• Risk / benefit
Mefloquine: facts and fiction
Sept 2012 NZSTM: Malaria Prevention Slide 32
The Lariam® Controversy

Sept 2012 NZSTM: Malaria Prevention Slide 33
Sept 2012 NZSTM: Malaria Prevention Slide 34
Does MQ cause neuro-
psychiatric adverse events?
• Unknown biologic mechanism
• Women at higher risk
• Low body weight / BMI
• Polymorphisms in MDR1 / ABCB1
transporters in endothelial cells
• Active area of research needed
Sept 2012 NZSTM: Malaria Prevention Slide 35
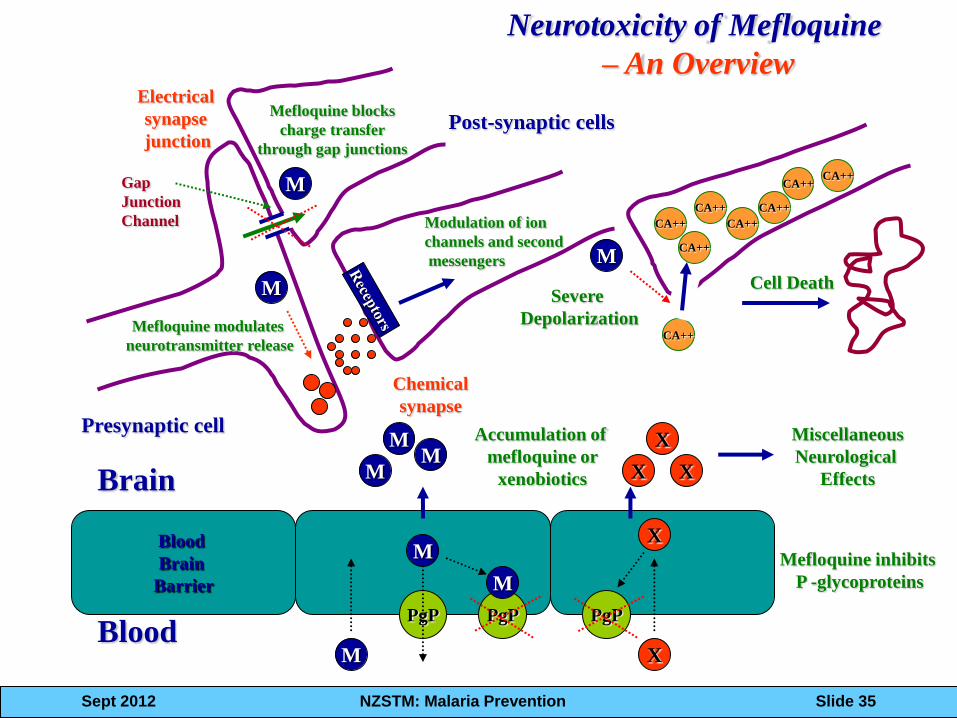
Neurotoxicity of Mefloquine
– An Overview
Presynaptic cell
Post-synaptic cells
Electrical
synapse
junction
Brain
Blood X
Blood
Brain
Barrier
PgP
M
PgP
M
M M
M
M
M
Chemical
synapse
CA++
CA++
CA++
CA++
CA++
CA++ CA++
CA++
X
X X
X
PgP
Miscellaneous
Neurological
Effects
Cell Death
Accumulation of
mefloquine or
xenobiotics
M
Severe
Depolarization
Gap
Junction
Channel
M
Mefloquine blocks
charge transfer
through gap junctions
Mefloquine modulates
neurotransmitter release
Modulation of ion
channels and second
messengers
Mefloquine inhibits
P -glycoproteins
Sept 2012 NZSTM: Malaria Prevention Slide 36
Other Adverse Reactions with
MQ • Gastrointestinal - N/V/D/Abd pain
• Dizziness / vertigo
• Sleep disturbances – Intense and vivid dreams
– Insomnia
• May be difficult or impossible to distinguish mefloquine AEs from travel related symptoms of jet lag, new experiences, etc.
Sept 2012 NZSTM: Malaria Prevention Slide 37
Lariam Medication Guide
Sept 2012 NZSTM: Malaria Prevention Slide 38
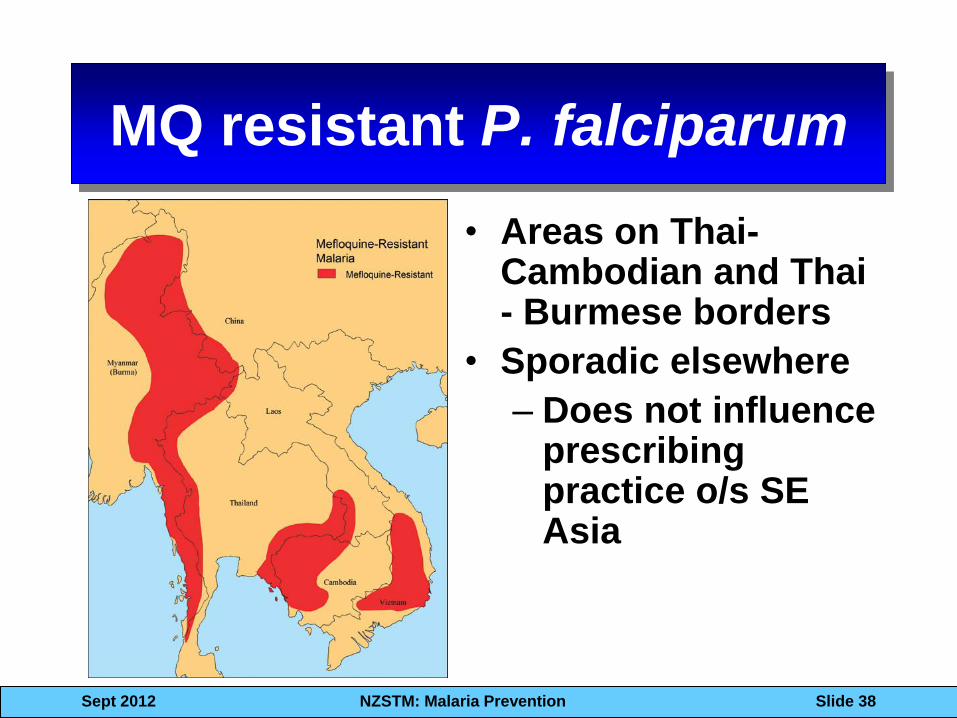
MQ resistant P. falciparum
• Areas on Thai-Cambodian and Thai - Burmese borders
• Sporadic elsewhere
– Does not influence prescribing practice o/s SE Asia
Sept 2012 NZSTM: Malaria Prevention Slide 39
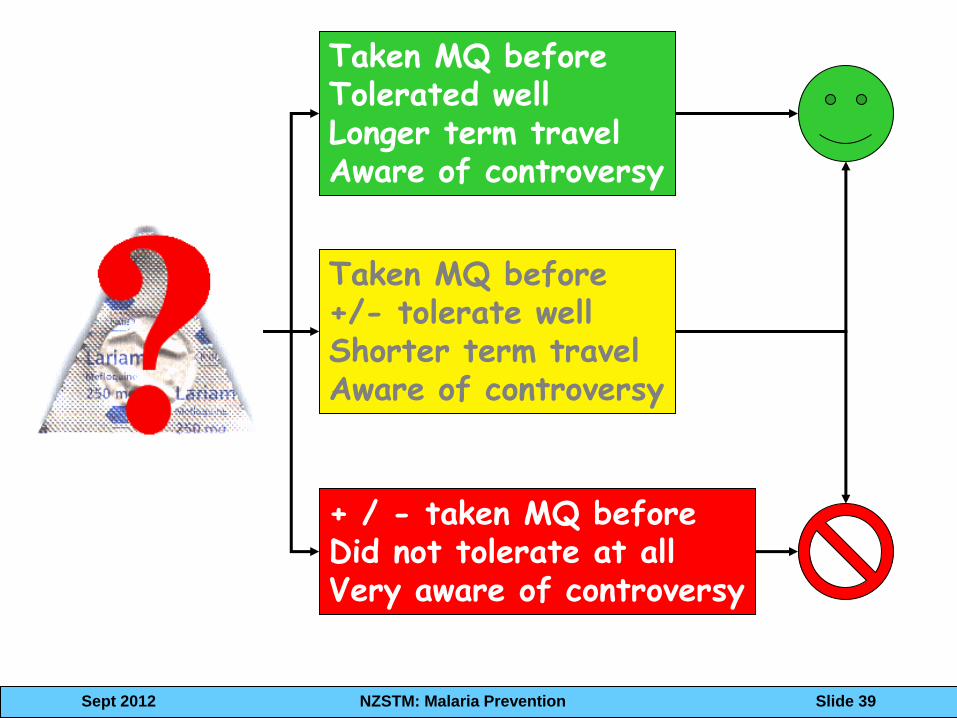
Taken MQ before Tolerated well Longer term travel Aware of controversy
Taken MQ before +/- tolerate well Shorter term travel Aware of controversy
+ / - taken MQ before Did not tolerate at all Very aware of controversy
Sept 2012 NZSTM: Malaria Prevention Slide 40
Malarone®
• Well tolerated combination
• Very efficacious combination
• Causal activity
– 7 days post-travel
• No geographic considerations for resistance (yet)
• Optimal choice for short term (2-3 weeks) travel
Sept 2012 NZSTM: Malaria Prevention Slide 41
• Fixed combination tabs – 100 mg PRO + 250 mg
ATQ (adult)
– 25 mg PRO + 62.5 mg ATQ (peds)
– 4 tabs once daily X 3 days
• > 98% efficacious in licensure trials – Semi-immunes in
Thailand, Gabon, Peru, Philippines
Am J Trop Med Hyg 1999 Apr;60(4):533-41
Sept 2012 NZSTM: Malaria Prevention Slide 42
Adverse Events with Malarone ®
• Both components of combination have very good safety records
• Gastrointestinal symptoms uncommon with prophylaxis daily dose
• Few drug-related adverse events when used for prophylaxis
• Occasional dermatological SAEs – Stevens Johnsons syndrome
• Better tolerated in RDBPC trials when compared to MQ, doxy, CQ/proguanil
Sept 2012 NZSTM: Malaria Prevention Slide 43
What Malarone® does not do
• Does not prevent hypnozoite relapse
in relapsing malarias (vivax and
ovale)
• Expensive, cost prevents use in
longer term travel for many
• Daily administration not ideal for
some
Primaquine for Prophylaxis
• In 2012 CDC
Yellow Book
primaquine is
recommended for
destinations in
Latin America with
> 90-95% vivax
malaria
Sept 2012 NZSTM: Malaria Prevention Slide 44
Primaquine for Prophylaxis
• 30 mg (base) daily starting a day
before travel, daily during travel, and
7 days after return
• G6PD normal
• Take with food
• Do not use for Sub-Saharan Africa
• Limited data to support indication
Sept 2012 NZSTM: Malaria Prevention Slide 45
Sept 2012 NZSTM: Malaria Prevention Slide 46
Why do travelers get malaria?
• Do not use any PPMs
• Do not take any prophylaxis
• Do not take the correct drugs
• Do not adhere prescribed regimens
Sept 2012 NZSTM: Malaria Prevention Slide 47
Outstanding Issues in Malaria
Chemoprophylaxis • Long stay traveler
– Safety of long term drug use
– Pre-Iicensure trials won’t include long durations
• Short stay, frequent visits, low risk (airline
personnel, oil field workers)
• New drug development
– No big pharma involvement
• Novel systems / delivery
– IM injection
– New way of using drugs we have: e.g. pre-exposure
prophylaxis
Sept 2012 NZSTM: Malaria Prevention Slide 48
Outstanding Issues in Malaria
Chemoprophylaxis • Drug – drug interactions
• Dueling guidelines and different
recommendations leading to traveler confusion
• Do we really know the right dose and regimen for
doxycycline?
• Current malaria control activities are making big
changes in the epidemiology of falciparum
malaria in Sub-Saharan Africa – when will our
recommendations change?
Sept 2012 NZSTM: Malaria Prevention Slide 49
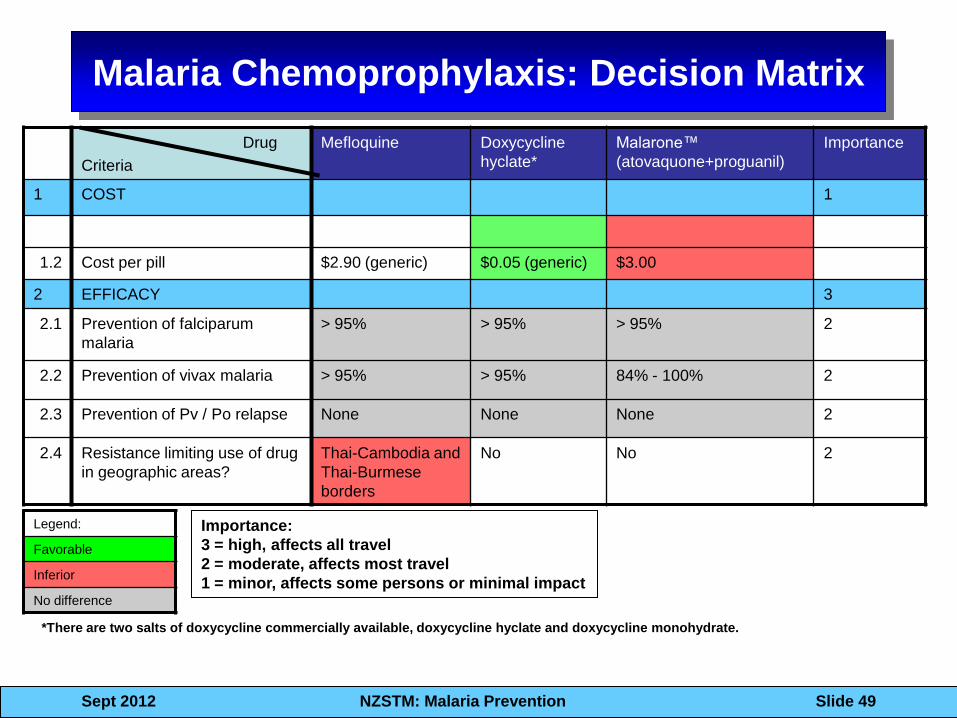
Malaria Chemoprophylaxis: Decision Matrix
Drug
Criteria
Mefloquine Doxycycline
hyclate*
Malarone™
(atovaquone+proguanil)
Importance
1 COST 1
1.2 Cost per pill $2.90 (generic) $0.05 (generic) $3.00
2 EFFICACY 3
2.1 Prevention of falciparum
malaria
> 95% > 95% > 95%
2
2.2 Prevention of vivax malaria > 95% > 95% 84% - 100% 2
2.3 Prevention of Pv / Po relapse None None None 2
2.4 Resistance limiting use of drug
in geographic areas?
Thai-Cambodia and
Thai-Burmese
borders
No No 2
*There are two salts of doxycycline commercially available, doxycycline hyclate and doxycycline monohydrate.
Importance:
3 = high, affects all travel
2 = moderate, affects most travel
1 = minor, affects some persons or minimal impact
Legend:
Favorable
Inferior
No difference
Sept 2012 NZSTM: Malaria Prevention Slide 50
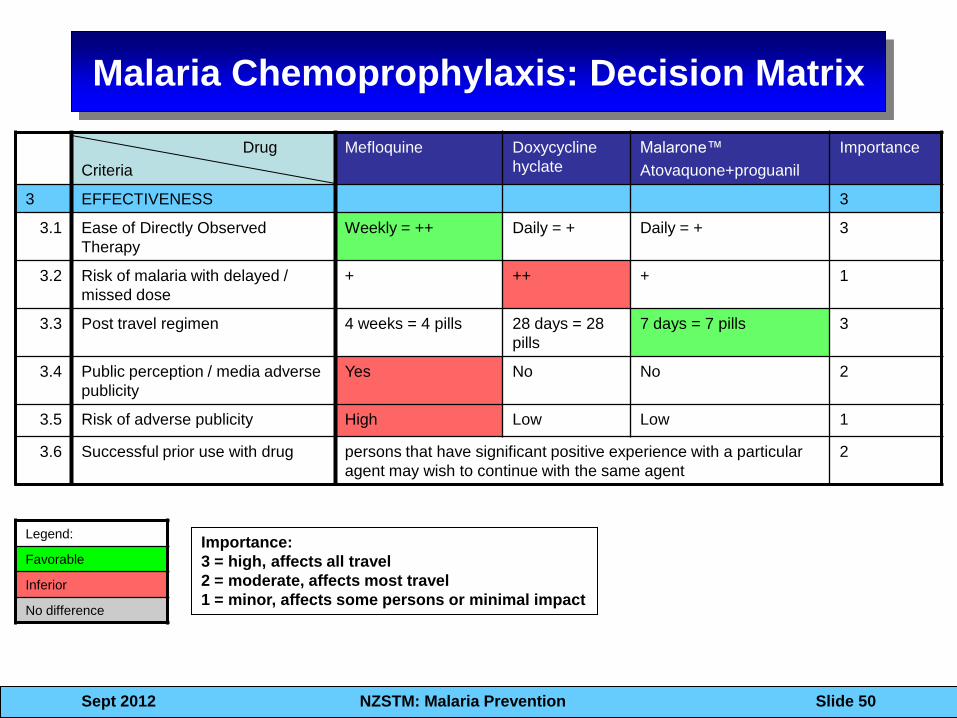
Malaria Chemoprophylaxis: Decision Matrix
Drug
Criteria
Mefloquine Doxycycline
hyclate
Malarone™
Atovaquone+proguanil
Importance
3 EFFECTIVENESS 3
3.1 Ease of Directly Observed
Therapy
Weekly = ++ Daily = + Daily = + 3
3.2 Risk of malaria with delayed /
missed dose
+ ++ + 1
3.3 Post travel regimen 4 weeks = 4 pills 28 days = 28
pills
7 days = 7 pills 3
3.4 Public perception / media adverse
publicity
Yes No No 2
3.5 Risk of adverse publicity High Low Low 1
3.6 Successful prior use with drug persons that have significant positive experience with a particular
agent may wish to continue with the same agent
2
Legend:
Favorable
Inferior
No difference
Importance:
3 = high, affects all travel
2 = moderate, affects most travel
1 = minor, affects some persons or minimal impact
Sept 2012 NZSTM: Malaria Prevention Slide 51
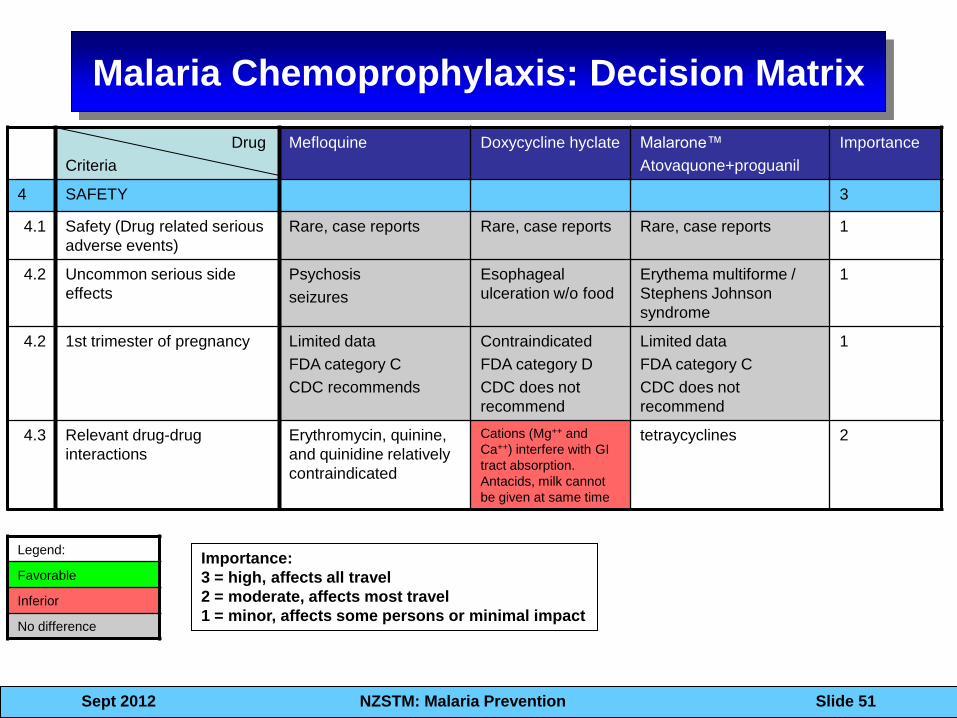
Malaria Chemoprophylaxis: Decision Matrix
Drug
Criteria
Mefloquine Doxycycline hyclate Malarone™
Atovaquone+proguanil
Importance
4 SAFETY 3
4.1 Safety (Drug related serious
adverse events)
Rare, case reports Rare, case reports Rare, case reports 1
4.2 Uncommon serious side
effects
Psychosis
seizures
Esophageal
ulceration w/o food
Erythema multiforme /
Stephens Johnson
syndrome
1
4.2 1st trimester of pregnancy Limited data
FDA category C
CDC recommends
Contraindicated
FDA category D
CDC does not
recommend
Limited data
FDA category C
CDC does not
recommend
1
4.3 Relevant drug-drug
interactions
Erythromycin, quinine,
and quinidine relatively
contraindicated
Cations (Mg++ and
Ca++) interfere with GI
tract absorption.
Antacids, milk cannot
be given at same time
tetraycyclines 2
Legend:
Favorable
Inferior
No difference
Importance:
3 = high, affects all travel
2 = moderate, affects most travel
1 = minor, affects some persons or minimal impact
Sept 2012 NZSTM: Malaria Prevention Slide 52
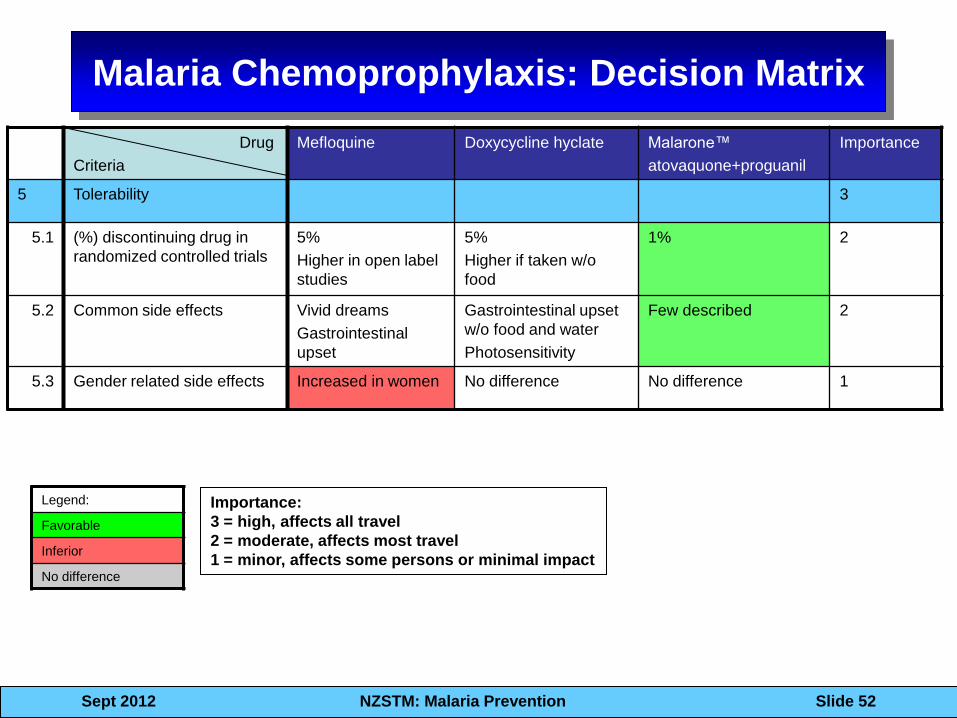
Malaria Chemoprophylaxis: Decision Matrix
Drug
Criteria
Mefloquine Doxycycline hyclate Malarone™
atovaquone+proguanil
Importance
5 Tolerability 3
5.1 (%) discontinuing drug in
randomized controlled trials
5%
Higher in open label
studies
5%
Higher if taken w/o
food
1% 2
5.2 Common side effects Vivid dreams
Gastrointestinal
upset
Gastrointestinal upset
w/o food and water
Photosensitivity
Few described 2
5.3 Gender related side effects Increased in women No difference No difference 1
Legend:
Favorable
Inferior
No difference
Importance:
3 = high, affects all travel
2 = moderate, affects most travel
1 = minor, affects some persons or minimal impact
Sept 2012 NZSTM: Malaria Prevention Slide 53
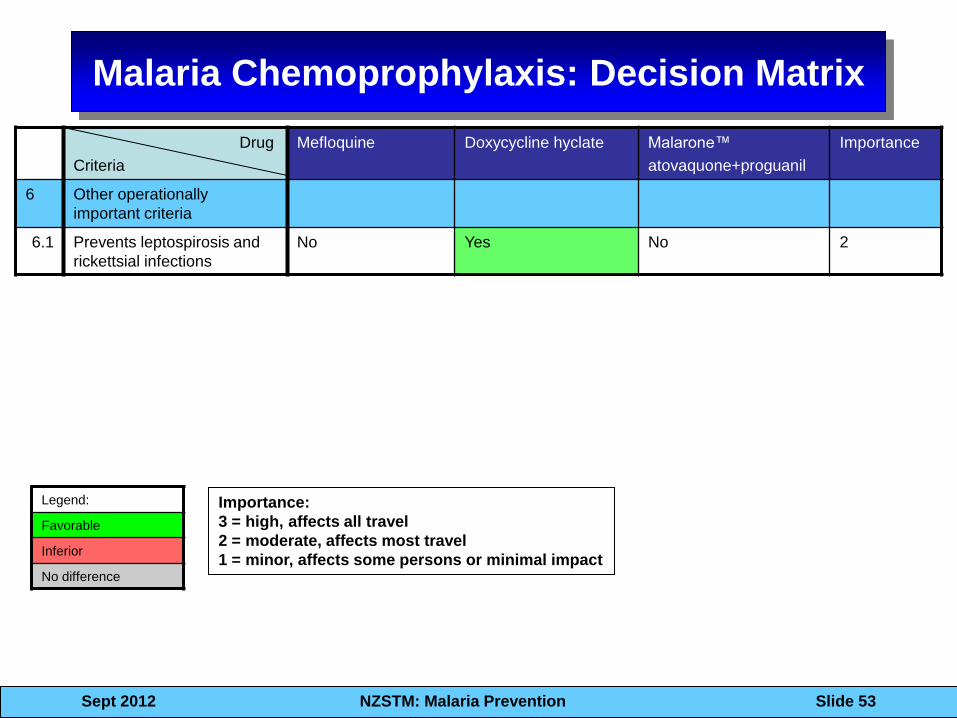
Malaria Chemoprophylaxis: Decision Matrix
Drug
Criteria
Mefloquine Doxycycline hyclate Malarone™
atovaquone+proguanil
Importance
6 Other operationally
important criteria
6.1 Prevents leptospirosis and
rickettsial infections
No Yes No 2
Legend:
Favorable
Inferior
No difference
Importance:
3 = high, affects all travel
2 = moderate, affects most travel
1 = minor, affects some persons or minimal impact
Sept 2012 NZSTM: Malaria Prevention Slide 54
Chemoprophylaxis !!!
• Malaria prophylaxis
with quinine first
used by British
Royal Navy
• The bitter taste of
quinine was
masked by gin
• Tonic water today
still has quinine!
Sept 2012 NZSTM: Malaria Prevention Slide 55
• In the United States, the Food and Drug
Administration limits the quinine content in
tonic water to 83 ppm (83 mg per liter)
• 500 – 1000 ml of tonic water (58.3 mg / l)
ingested in 15 minutes by N = 6 volunteers
• Mean quinine plasma levels of 0.62 mg/l
(0.4 – 0.77 mg/l) at 1-32 hours after ingestion
• At low end of quinine MICs
• Meyer CG, Marks F, May J.Editorial: Gin tonic
revisited. Trop Med Int Health. 2004 Dec;9(12):1239-40
• At a 1 part gin / 2 parts tonic mix, it may
require up to 1 - 2 liters of gin and tonic to
have sufficient levels of quinine.
•More research is clearly needed!!
Sept 2012 NZSTM: Malaria Prevention Slide 56
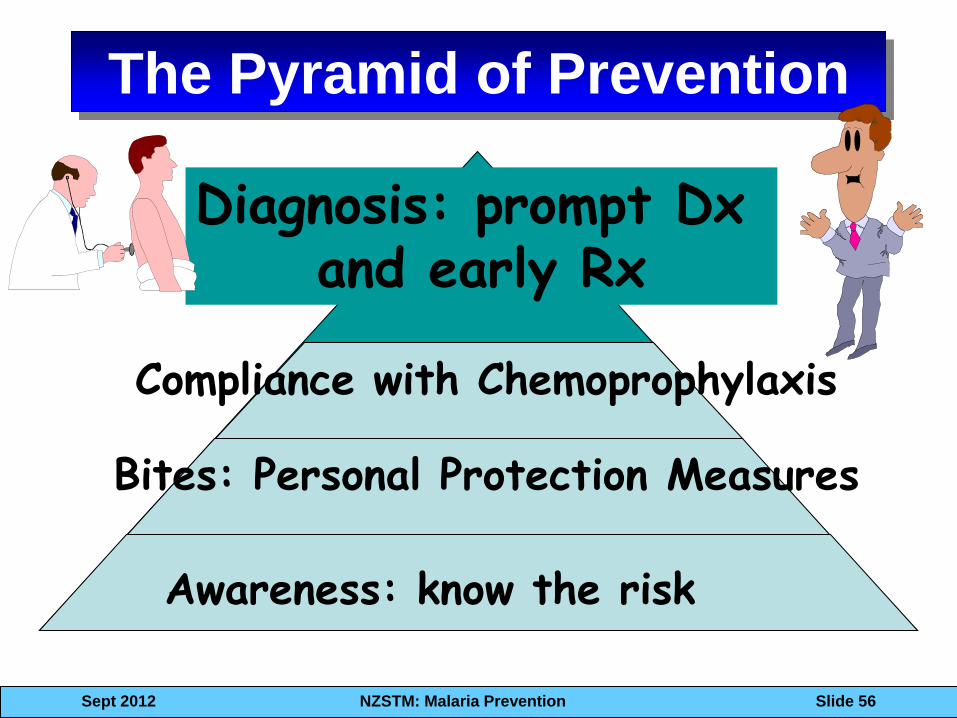
The Pyramid of Prevention
Bites: Personal Protection Measures
Awareness: know the risk
Compliance with Chemoprophylaxis
Diagnosis: prompt Dx and early Rx
Sept 2012 NZSTM: Malaria Prevention Slide 57
Alan J. Magill MD, MACP, FIDSA, FASTMH
COL / MC US Army (retired)
Emeritus, WRAIR
Associate Professor, Uniformed Services
University of the Health Sciences
Thank you!