-
8/4/2019 malunion colles
1/12
Journ al of the American Academ y of Ortho paedic Surgeon
s270
Malunion is a recognized cause of
suboptimal function after distal
r ad ius fr ac tu re . The ob jec t ive
find ings and subjective comp laints
of a symptomatic malunion have
come to be better appreciated as
patients of all ages have demand-
ed h igh levels of fun ction after th iscommon injury . Furtherm
ore, ad-
vances in the u nderstand ing of the
biomechanics of the hand-wrist-
forearm u nit have led to imp rove-
ments in surgical techniques for
r e s t or i n g t h e n o r m a l a n a t o m i c
relationships, resulting in better
function for patients with a mal-
union.
Anatomy
The distal radius includ es the radi-
al metaphysis, with its thin dorsal
cortex and the rich trabecular net-
work sup porting the radiocarpal
and distal radioulnar articular sur-
faces . This h igh ly specia l ized
platform perm its execution of
the complex motions demanded by
a vast a rray of activities.
The distal articular su rface of the
radius is contoured an d spatially
oriented to direct the motions of
the carpa l bones. The art icular
margin of the distal radius is the
point of attachment for the radio-scaphocapitate,
radiolunotrique-
tral, radioscapholunate, and dorsal
radiotriquetral ligaments, which
provide stability to an d guide force
transmission about the radiocarpal
articulation.
An equally important articula-
t ion, the dis ta l radiou lnar jo int
(DRUJ), is composed of the sig-
moid notch, or fossa, of the radius
and the ulnar head. The portion
of the ulnar head that articulates
with the sigmoid notch is calledt h e u l n a r s e a t ; t h e
p o r t i o n
und er the triangular fibrocartilage
is considered the ulnar pole .
The relat ionship of the concave
s i g m o i d n o t c h , w i t h i t s l a r g e r
r a d i u s o f c u r v a t u r e , a n d t h e
s m a l l e r u l n a r s e a t p e r m i t s a
un ique combinat ion of ro ta t ion
and t rans la t ion.1 However , the
area of art icular contact is rela-
tively small and has little inherent
stability imparted by the osseous
structure.
M ot ion a t t he D R U J i s con-
trolled by stabilizing soft tissues
about the distal ulna, including
the volar and d orsa l radioulnar
ligaments, the articular disk of the
triangular fibrocartilage complex
(TFCC), the DRUJ cap sule , th e
extensor sheaths of the fifth and
s i x t h c o m p a r t m e n t s , a n d t h e
pronator quadratu s . The radio-
carpal unit translates dorsally and
distal ly about the stable ulna in
supination, delivering the ulnar
head volarward. In pronation, theradiocarpal un it translates
volarly
and p rox im a l ly , de l ive r ing th e
ulnar seat dorsally.
Dr. Graham is Attending Surgeon, Section of
Hand and Upper Extremity Surgery, Depart-
ment of Orthopaedic Surgery, Cleveland Clinic
Foundation, Cleveland, and Assistant Clinical
Professor of Orthopaedic Surgery, Ohio State
University, Columbus.
Reprint requests: Dr. Graham, Section ofHand and Upper Extremity
Surgery, Depart-
ment of Orthopaedic Surgery, Cleveland Clinic
Foundation, 9500 Euclid Avenue - A51,
Cleveland, OH 44195.
Copyright 1997 by the American Academy of
Orthopaedic Su rgeons.
Abstract
Malunion of a distal radius fracture may result in functional
limitation and
pain. Reestablishing the geometry of the metaphysis and the
alignment of the
articular surface, restoring the relationship at the distal
radioulnar joint, and
respecting the soft-tissue envelope are elements of a successful
reconstruction.
The author describes a systematic approach to evaluation and t
reatment, includ-
ing the indications for surgical correction, techniques of
reconstruction, and
potential complications. Salient aspects of postsurgical
rehabilitation and sal-
vage procedures are discussed.
J Am Acad Orthop Surg 1997;5:270-281
Surgical Correction of Malunited Fractures
of the Distal Radius
Thomas J. Graham, MD
-
8/4/2019 malunion colles
2/12
Thomas J. Graham, MD
Vol 5, No 5, September/October 1997 271
Radiographic Evaluation
Five familiar measurements can be
used to evaluate the distal end of
the radius: rad ial inclination, rad ial
length, ulnar variance, radial tilt,
and radial shift.
On a posteroanterior (PA) radio-graph, the inclination of the
radial
platform is the angle between a line
draw n from the t ip of the radial
s ty loid to th e most d is ta l u lnar
aspect of the lunate facet and a line
perpend icular to the longitudinal
axis of the rad ius (Fig. 1, A). The
average ra dia l inc l inat ion i s 22
degrees.2
Radial length is measured on a
PA film by determining the longi-
tud inal difference between a line
perp endicular to the long axis of
the radius drawn at the radial sty-
loid and another line tangential to
the distal articular surface of the
ulna (Fig. 1, B).2 With this method,the normal rad ial length is
app roxi-
mately 11 mm . I do not favor this
method, as it does not truly assess
the DRUJ, where length inequity
has its greatest imp act. Instead, I
p re fe r t o r ecord u lna r va r i ance
(Hultens variance), or radioulnar
length.3,4 Both methods reflect the
relationship of the articular sur-
faces of the radius and ulna at the
DRUJ, and both are useful because
they take into account the anatomic
and mechanical impact a fracture
wi th med ia l fragment d isplace-
ment may have on wrist and fore-
arm function. A PA view of the
normal wrist should also be taken,because there can be
differences in
the d istal radioulnar relationship
among individuals.
Ulnar variance, or radioulnar
length, can be calculated in a variety
of ways, all of which yield similar
results.3 This variable is determined
by draw ing a line perpendicular to
the long axis of the radius at the sig-
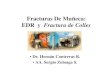
Fig. 1 Calculation of radiographic measurem ents of the distal
radius. A, On a PA radiograph, the radial inclination (RI) is the
angle sub-tended by a p erpendicular to the long axis of the rad
ius and a line reflecting the articular surface of the radius. B,
On a PA film, the radiallength (RL) is the d istance between
tangents draw n at th e radial styloid and the ulnar pole, perpend
icular to their shaft axes. C, The ulnarvariance, or radioulnar
length, also measured on a PA film, reflects the axial relationship
between the ulnar pole and the ulnarm ost aspectof the distal
radius. In the drawing on the left, the radioulnar length is
neutral. The drawing on the right d emonstrates a prominent ulnaat
the DRUJ. D, On a lateral radiograph, the radial tilt (RT) is the
angle between the articular surface and a line p erpendicular to
the rad ialshaft. E, On a PA film, the radial shift (RS), or radial
width, is a comparison measurement made between the malunited
radius and thenoninjured radius. It is the distance between p
arallel lines draw n tangent to the radial styloid an d the long
axis of the radius.
A B C
D
RT
RL
RI
E
Volar Dorsal
RSRS
-
8/4/2019 malunion colles
3/12
Malunited Distal Radius Fractures
Journ al of the American Academ y of Ortho paedic Surgeon
s272
moid notch and then measur ing
how much of the ulnar head is dis-
tal to that line (Fig. 1, C).
Ulnar variance has important
pr ognostic imp lications. Aro and
Koivunen4 classified three types of
r ad iou lna r r e l a t ionsh ips a t t he
DRUJ after distal radius fractures.Axial shortening of the
radius by
less than 3 mm, d esignated grade 0,
was considered acceptable. Grade
1 includ ed fractures w ith 3 to 5 mm
of shortening. A fracture with more
than 5 mm of radia l shor tening
at the DRUJ was termed grade 2.
Good or excellent functional results
occurred in 96% of their patients
with a grade 0 radioulnar relation-
ship. Functional impairment was
reported in the other two groups,
which correlated directly with the
length disparity. When dorsal or
radial malalignment or displace-
ment of the distal articular surface
of the radius was combined w ith
radial shortening, the result was an
even greater decrement in clinical
outcome.
The radial tilt is measured on a
latera l film (Fig. 1, D). The norm al
pa lm arw ard o r i en ta t ion o f t he
articular surface, or platform, is
m easured by com par ing a l i nedrawn through the volar and
dor-
sa l margins of the dis ta l radius
wi th th e long axis of the rad ia l
shaft. The normal radial tilt is ap-
proximately 11 deg rees. Mann et
al5 have shown that d orsal tilting is
not found in the noninjured adult
wrist, and that women generally
have slightly more palmar tilt than
men.
The radial shift, or radial width,6
is the distance between the longitu-
dinal axis of the radius and a linedrawn tangential to the
radial sty-
loid. This measu rement reflects the
shor t en ing and r ad ia l co l l apse
often seen in comminuted distal
radius fractures and is related to
radial inclination, rad ial length,
and ulnar variance. In preopera-
tive planning, the radial shift of the
malunion i s compared wi th the
relationship in the non injured con-
tralateral wrist (Fig. 1, E).
When evaluating posttraumatic
radial d eformity, it is also imp or-
tant to assess fracture location and
adequacy of reduction, particularlyintra-articular displacement
at the
rad ioca rpa l jo in t ,7 t he s igm oid
fossa, and the u lnar head.
Biomechanics
Changes in the osseous architec-
tur e affect the mechan ics of the
rad iocarpal joint, th e DRUJ, and
the forearm axis. For examp le, do r-
sal tilting of the radial platform
shifts axial loading through the
w r i s t do r sa l ly and u lna r ly and
decreases the joint contact area .8
Dorsal tilting may also produce a
carpal collapse pattern similar to
that seen in dorsal intercalated seg-
ment instability (DISI) but without
interosseous ligament disruption9
or secondary midcarpal instabili-
ty10 (Fig. 2).
The relationship between radial
malunion and kinematic alteration
at the DRUJ and anatomic distor-tion of the TFCC has been
studied
by Adams,11 who observed that the
greatest change in kinematics at the
DRUJ accompanies r adial shor ten-
ing. Loss of rad ial inclination and
dorsal tilting of the platform in the
s a g i t t a l p l a n e h a d a m o d e r a t e
effect. Dorsal disp lacement of the
d i s t a l f r agm ent caused l i t t l e
change. Radial shorten ing created
the greatest strain in th e articular
disk and in the volar and dorsal
radioulnar ligaments of the TFCC.
Fur the rm ore , he obse rved tha t
deformity of the radius alone in the
presence of an intact TFCC did not
perm it dislocation of the DRUJ.
Fig. 2 A, Radiograph of a m alunited d istal radius fracture w
ith dorsal tilting of the plat-form in the sagittal plane. Note the
dorsal posture of the lunate and the increases in thescapholunate
angle and the capitolunate angle. B, Normal rad iocarpal and
intercarpalalignment in the sagittal plane. C, The collapse pattern
often seen with distal radialmalunion w ithout intercarpal ligament
disruption.
A B C
Normal Malunion
-
8/4/2019 malunion colles
4/12
Thomas J. Graham, MD
Vol 5, No 5, September/October 1997 273
Clinical Presentation
The symptom complex that f re-
quently accompanies radial mal-
union includes pain, motion loss,
and weakness. The location of the
pain can be variable and multifo-
cal. Causes of pain include gener-alized synovitis,
osteocartilaginous
damage due to the initial injury or
resulting from altered mechanics or
ulnocarpal abutment, a TFCC tear,
and arthrosis at the wrist joint or
the DRUJ. It is important to differ-
entiate mechanical pain from dys-
t roph ic sym ptom s . Loca l i z ing
symptoms to the radial side or the
u lna r s ide o f t he w r i s t has an
impact on treatment, particularly
with respect to surgical manage-
ment of the d istal ulna.
Although decreased motion can
be observed in any plane of wrist
motion or forearm rotation, radio-
carpal flexion is typically dimin-
ished d ue to d orsal angulation of
the distal radius. Sup ination loss is
a p redictable complaint and clinical
finding; pronation is usually dimin-
ished to a lesser extent. The combi-
nation of al tered m echanics and
pain resul t s in decreased gr ip
strength. Recording of wrist andforearm m otion in all planes
and
gr ip-s t rength measurements i s
important.
PreoperativeConsiderations
Indications
Not all malunited distal radius
fractures require surgical treat-
ment . The decis ion to proceed
with a rad ial osteotomy or an ulnaros teoplas ty , or both ,
should be
based on a combination of factors,
including the location and intensity
of pain, the functional impact of
mot ion loss and d ecreased gr ip
strength, and the radiologic find-
ings . Of these fac tors , c l in ica l
symptoms and functional losses are
most imp ortant.
Fernandez12 observed a patho-
logic displacement of the flexion-
extension arc with a change in rad i-
al tilt greater than 25 degrees. He
also found that less severe deformi-
ties (10 to 15 degrees of dorsal tilt-ing f rom norm al) may
resul t in
midcarpal instabil i ty in patients
w i th p reex i s t ing w r i s t l ax i ty .
Fourr ier e t a l13 conclud ed f rom
their study of 64 radial malunions
t h a t s y m p t o m s a n d f u n c ti on a l
impairment resulted from a loss of
sagittal tilt of 10 to 20 degrees and
that a 20- to 30-degree loss of radial
inclination h ad a severe effect on
function.
Laboratory studies support the
concep t t ha t m a lu n ion im pa i r s
function and may be an accelera-
tor of arthrosis.8,11,14 Dorsal tilt in
the ran ge of 20 to 30 degrees alters
the forces on the radial articular
cartilage and thus m ay cause de-
generative change.8,14 On the basis
of laboratory studies and clinical
surveys, Graham and Hastings15
suggested four radiographic crite-
ria for assessing h ealing of a distal
rad ius f rac ture . These cr i ter ia
focus on the position of the radialplatform, the status of the
DRUJ,
and the congruity of the articular
surface a t the radiocarpal jo int
(Table 1).
How ever, these criteria are not
absolute. Individ ual variations in
normal anatomy and the clinical
impact of the malunion must be
t aken in to cons ide ra t ion . The
greatest variability appears to be in
the patients response to a change
in rad ial tilt. Many patients willtolerate a dorsal tilt in the
range of
10 to 15 degrees (approximately 25
degrees of deviation from normal);
pa t i en t s w i th dor sa l t i l t i ng in
excess of 20 degrees have a greater
r i sk o f deve lop ing sym ptom s .
Pred ic t ab ly , shor t en ing o f t he
radius, with the accompanying d is-
turbance a t the rad iocarpal and
radioulnar joints, seems to have the
most direct correlation with devel-
opment an d intensity of symptoms.
There are no well-established
criteria for articular incongruity a t
the DRUJ. There is relatively little
articular contact between the u lnar
seat and the sigmoid fossa; maxi-
mum contact at neutral rotation is
about 60%, and contact is as little
as 10% at the extremes of prono-
sup ination. It is conceivable that
intra-articular malunion could be
tolerated. How ever, personal ex-
perience indicates that step-offs of
1 to 2 mm at the DRUJ can causesymptoms.
G r a h a m a n d H a s t i n g s15 d e-
scribed four clinical groups based
on the above-m ent ioned r ad io -
Table 1
Radiographic Criteria for Acceptable Healing of a Distal Radial
Fracture
Radiographic Criterion Acceptable Measurement
Radiou lnar length Radia l shor ten ing of
-
8/4/2019 malunion colles
5/12
Journ al of the American Academ y of Ortho paedic Surgeon
s274
graphic criteria and developed a
systematic approach to the surgical
treatment of symptomatic distal
rad ial ma lun ions (Table 2). Pro-
cedures selected on the basis of
these guidelines resulted in im-
provements in wrist motion, pro-
nosupination, and grip strength.In groups I, II, and III, the
DRUJ
was salvaged . Reconstru ction of
the DRUJ with or without realign-
ment of the radial platform with
respect to the radiocarpal joint uni-
formly resulted in subjective im-
provement and enhancement of
wrist and forearm function. Pa-
tients who underwent DRUJ abla-
tion had a higher comp lication rate
due to instability and radioulnar
impingement. However, group IV
pa t i en t s a l so dem ons t r a t ed the
grea t e s t im provem ent i n g r ip
strength, with elimination of pain-
ful ulnocarpal abutment or DRUJ
arthrosis.
These f ind ings ind ica t e t ha t
restoration of DRUJ alignment is
technically feasible and is clinically
indicated even when the primary
pain seems to emanate from the
DRUJ. Distal ulna r ablation should
be reserved for arthritic joints and
incongruous joints that cannot berealigned.
Al though complaints about a
p rom inen t u lna a re f r equen t i n
patients with a m alunion, cosmetic
improvement alone is not an indi-
cation for surgical interven tion.
Preoperative discussions should
emphasize that the goals are pain
relief and anatomic restoration.A gray area in clinical
decision
making is the situation in which a
young patient (aged less than 40
years) has a radial malunion that is
considered un acceptable on the
basis of radiographic criteria yet is
only minimally symp tomatic. The
natural history of long-standing
radial malunion is unknown, and
the results of biomechanical studies
are only suggestive of an increased
risk of arthrosis. Anatom ic derange-
ment, motion, pain, and the desired
level of activity must be the key
determining fac tors . Operat ive
treatment of asymptomatic patients
and those with minor impairment is
seldom ap propriate.
The degree of funct ional im-
provem ent varies. In the series of
Graham and Hastings,15 wrist flex-
ion improved to a slightly greater
degree than wrist extension. Sup i-
na t ion w as the m os t im proved ;
however, pron ation also increased.In a l l group s , gr ip s t
rength im-
proved to ap proximately two thirds
of that on the contralateral side.
Timing of Distal Radial
Osteotomy
The optimal timing for osteotomy
continues to be debated. Postponing
the osteotomy until fracture consoli-dation, recovery of motion,
and
reversal of osteopenia have occurred
is appealing; however, in cases of
severe deformity, impaired function,
and pain, earlier intervention may
be ind icated. An early, or nascent,
distal radial osteotomy can be per-
formed in the first 4 to 8 weeks after
fracture. If a fracture originally
treated by closed method s shows
increasing collapse, takedown of the
callus and anatomic reconstruction
with a bone graft and internal fixa-
tion will redu ce the rehabilitation
time. There is also a potential bene-
fit to rebalancing the soft tissues and
preventing contracture.
Jupiter and Ring16 compared the
results of early and late reconstruc-
tion of the malunited distal radius.
(Early reconstruction was defined as
that performed an average of 8 weeks
after injury; late osteotomies were
performed on average at 40 weeks.)
The results were comparable andslightly favored early
reconstruction.
Thomas J. Graham, MD
Table 2
Criteria for Patient Grouping and Treatment Recommendations in
Study by Graham and Hasting s15
Group Radial Radioulnar DRUJ Reducible by Acceptable DRUJ
Reconstruction
Assignment Measurements Length Radial Osteotomy Articular
Surfaces Indicated
Group I Unacceptable Unacceptable Yes Yes Distal radial
osteotomy
Group II Acceptable Unacceptable NA
*
Yes Ulnar shorteningGroup III Unacceptable Unacceptable No Yes
Distal radial osteotomy
and ulnar shortening
Group IV Unacceptable Unacceptable No No Distal radial
osteotomy
and distal ulnar ablation
*N A = not app licable to this group because no distal radial
osteotomy was p erformed in group II patients.
-
8/4/2019 malunion colles
6/12
Thomas J. Graham, MD
Vol 5, No 5, September/October 1997 275
These investigators conclud ed that
the osteotomy was technically easier
and the overall period of disability
was shor ter with early correction.
Contraindications
If the radiocarpal or intercarpal
joints exhibit advan ced d egenera-tive arthrosis, a radial
osteotomy
wil l provide l i t t le symp tomat ic
relief. The quality of the bone stock
is important; severe osteoporosis is
a re la t ive cont ra indicat ion, but
advanced age alone is not. If non-
mechanical symptoms or sympa-
thetically m ediated p ain dom inates
the p resen ta t ion , t he op e ra t ion
should be postponed.
Preoperative Planning
The success of radial osteotomy is
dependent on jud icious patient selec-
tion, meticulous preoperative plan-
ning, and careful surgical execution.
At a minimum, a full set of radio-
graphs of the injured and the con-
tralateral, noninjured w rist should be
obtained. These stud ies are usually
adequate for the necessary calcula-
tions and template preparation.17,18
Computed tomography is helpful in
assessing the articular surfaces. In
patients with complex intra-articularinvolvement, preoperative
wrist
arthroscopy may be useful.
More sophisticated methods of
planning, includ ing trigonometric
calculations, have emerged. Nom o-
gram s have been deve loped to
facilitate prediction of the size and
shape of the graft that is required
for the correction.19 C om pute r -
generated mod els have also been
developed to assist the surgeon in
cases of comp lex deformity.20
A thorough und ers tanding of the steps of the operation (Fig.
3)
will facilitate intraoperative prepa-
ration. The possible need for pro-
visional external fixation,21 lamina
spreaders, power equipment, fluo-
roscopy, and var iable f ixat ion
devices should be anticipated.
Surgical Techniques
Extra-articular Radial Malunion
Most radial malunions present
with sh ortening , loss of radial incli-
nation, and dorsal t i l t ing of the
rad ius. The goal of reconstru ction
is to restore the alignment of the
radiocarpal joint and the DRUJ by
performing an osteotomy through
the site of the original fracture and
supp or t ing the d i s t a l f r agm ent
with a corticocancellous bone graft
and intern al fixation. My preferred
A B
D E
C
Fig. 3 Steps in performance of a distal radial osteotomy. A, The
location of the incision ismarked. B, Position of guid e pins. Pin
A is an intra-articular or juxta-articular p in used to
jud ge the orientation of the rad ial articular sur face. Pin B
diverge s from being pa rallel topin A in an an gle that will
eventually be the amou nt of correction yielded by the osteoto-my
(hatched line represents level of osteotomy); it is placed at the
eventual site of the mid-dle hole of the plate and can be used to
secure the intraoperative external fixator. Pin C isan optional pin
that can be used to judge the recovery of radial inclination; it
divergesfrom being par allel to the joint in the angle of eventu al
correction. Pin D is placed d orsallyperpend icular to the axis of
the radius and will be parallel to pin B when the correction iscomp
lete; it can be a half-pin used to erect the intraop erative
external fixator. Pin E is the
companion pin to pin C if correction of inclination is to be
monitored; it is perpendicular tothe axis of the rad ius in the
radial-to-ulnar direction. A second external fixator based onpins C
and E can be used, but I prefer to simply place smooth wires in
these positions todiminish the hole size. C, The geometry of the
radius has been restored through theosteotomy site, and an external
fixator m aintains the correction held by the lamina spread-ers.
Note th at all pin pa irs (i.e., B and D, C and E) are par allel
after correction. D, Harvestof the bicortical graft from th e iliac
crest. The graft is usu ally taken from the sup erior crestand the
outer table, although the inner-table contour may be more su itable
in some cases.E, Plate fixation stabilizes the osteotomy
construct.
Angle of
inclination
correction
Angle of
sagittal
correction
Line parallel
to joint
Line parallel
to joint
A
A
B
B
C
C
D
D
E
E
-
8/4/2019 malunion colles
7/12
Journ al of the American Academ y of Ortho paedic Surgeon
s276
surgical approach to reconstruction
of a typical radial malunion is sum-
marized in Figure 3.
A dorsally angulated malun ion is
exposed by a longitudinal or slight-
ly curved dorsal incision extending
from the midcarpal level to the radi-
al metadiaphysis (Figs. 3, A; 4, A).Skin flaps are raised by
dissecting
the areolar suprafascial plane. The
third dorsal compartment is then
incised. The extensor pollicis lon-
gus is retracted rad ially and left
transposed at the end of the proce-
dure.
Subperiosteal dissection of the
second and fourth dorsal compart-
ments is performed to fully expose
the malun ited radiu s. A smooth
wire is inserted into th e radiocarpal
joint or parallel to it just proximal
to the subchond ral bone (Fig. 3, B).
This wire is the locator for the joint
and will be a guide to appropriate
positioning of the distal fragment
after osteotomy.
I r em ove the p rom inence o f
Listers tubercle, find the center of
what will become the distal frag-
ment, and then p lace a part ial ly
threaded Schanz pin that will be
used for intraoperative construc-
tion of a small external fixator. The
pin has a thread diameter of 2.0 or
3.0 mm . The hole created by the
pin will become the central screw
hole for the fixation plate. The pini s p l aced such tha t t he
ang le
between the partially threaded pin
and the smooth wire is the angle
needed to correct the volar tilt.
A second partially threaded pin
is placed p erpend icular to the long
axis of the radius in a proximal
location. This pin has a du al pu r-
pose; it will be the proximal anchor
for the intraoperative fixator and
will also be the standard by which
the distal fragment orientation will
be judged for sagittal correction.
When the correct volar t i l t i s
gained (as predetermined from the
contralateral radius), the proximal
and distal pins should be parallel;
thus , the f ixator and the rad ius
make a perfect quadr ilateral (Fig. 3,
C) . Fluoroscopy is help ful for
intraoperative confirmation of pin
placements and alignmen t correc-
tion.
Smooth 0.045-inch wires can
also be inserted from th e lateral
aspect of the radius to guide the
correction of rad ial inclination, if
desired (Fig. 3, A). The proximal
pin is placed 90 degrees to the longaxis of the rad ius. The
distal pin is
placed at an angle divergent from
the articular surface such that it
will be parallel to the proximal pin
when the desired angle of correc-
tion is achieved .
The os teotomy is car r ied ou t
with an oscillating saw or osteo-
tomes and must be proximal to the
sigmoid notch of the radius. The
usual level of the os teotomy is
about 2.5 cm proximal to the radio-
carpal joint, near the proximal base
of Listers tubercle, which is typi-
cally at the level of the fracture
deformity. I tend to make the os-
teotomy perpendicular to the long
axis of the radius in the PA plane,
rather than parallel to the joint ,
a l t hough the l a t t e r i s pe r f ec t ly
acceptable an d creates less volar
Thomas J. Graham, MD
A B C D
Fig. 4 Distal radial osteotomy. A, Incision and dissection down
to the level of the fascia, incision of the third dorsal
compartment, andtransposition of the extensor pollicis longus (in
retractor). B, Lamina spread ers are u sed to establish orientation
of the d istal fragment.External fixator is in place to maintain
correction before graft insertion. C, Graft placement. (Because
distraction was released while har-vesting the graft, the void size
does not m atch graft dimensions.) D, Graft in place (with fixator
on) before remo val of external fixator an dplate application.
-
8/4/2019 malunion colles
8/12
Thomas J. Graham, MD
Vol 5, No 5, September/October 1997 277
displacement of the d is ta l frag-
ment. Among the reasons for my
preference is that it establishes a
relatively flat proximal base for the
corticocancellous graft, creates a
less severe slope from radial to
ulnar at th e distal edge of the graft,
and provides more bone about therad ial styloid for p otential
fixation.
In the sagittal plane, I typically
create the osteotomy parallel to the
malunited joint. It mu st be recalled
that the spatial relationships about
the ar t icular surface have been
changed; articular penetration by
the saw or os t eo tom e m us t be
avoided.
Limi ted volar re lease of the
prona to r quadra tus can be pe r -
formed through the osteotomy site
to better mobilize the distal frag-
ment . Use of small lamina spread -
ers will facilitate positioning of the
distal fragment and will stabilize
the relationship if an external fixa-
tor is ap plied (Figs. 3, C; 4, B). The
void created by p ositioning the dis-
tal fragment in the d esired orienta-
tion is the best guide to the amou nt
of bone that will have to be har-
vested from the iliac crest, althou gh
the dimensions should be close to
the calculations performed in pre-operative planning.
Before deciding on the f inal
graft dimensions, the provisionally
s tabi l ized const ruct i s taken
through the range of motion. The
wrist flexion-extension arc should
be imp roved. I have not found it
necessary to perform a limited d or-
sal radiocarpal capsulotomy, but it
can be considered . A provisional
check of pronosupination will dic-
tate whether adjunctive DRUJ cap-
sulectomy wi l l be necessary ,depend ing on the d egree of
resid-
ual pronation or supination con-
tracture.
A t t h i s po in t , t he a l ignm ent
shou ld be checked w i th f luo -
roscopy or radiography. A trape-
zoidal bicortical graft, taken from
the ou te r t ab l e o f t he i l ium , i s
placed such that its cortical mar-
gins are on the dorsoradial aspect
of the rad ius (Figs. 3, D; 4, C). Only
in f r equen t ly i s t he i l i um th in
enough to yield a tricortical graft
that can be intercalated in the void.
It is the superior aspect of the iliacwing that will become the
radial
aspect of the graft, with the cortical
bone from the inner or outer table
fo rm ing the dor sa l s t ru t o f t he
graft. Therefore, the sup erior por-
t ion of the i l iac wing should be
inspected to d etermine whether the
osseous architecture of the inner or,
more commonly, the outer table
better suits the p atients anatomy.
The goal is an intercalated graft
well stabilized between the radial
fragments. Placing it in the void
w hi l e t he cons t ruc t i s s l i gh t ly
overdistracted by the fixator and
lamina spreaders and then careful-
ly releasing the distraction is ad-
vised (Fig. 4, D). Fixation of the
graft can be d one by any of several
meth ods (Fig. 3, E). I pr efer plate
fixation with an oblique T plate
(Fig . 5) , but I have used mini
condylar blade plates in patients
with thin rad ii (Fig. 6). Kirschner
wires can also be used to fix the
graft in place.
Two other alternatives for per-
forming an osteotomy of the dor-
sally t i l ted rad ial platform h ave
been described. The first is the
trapezoidal osteotomy, wherein abone graft of specific
proportion is
taken from the malunited d orsal
radius itself (Fig. 7).22 After radial
os t eotom y th r ough the l eve l o f
deformity, the corticocancellous
trapezoidal graft is rotated into th e
void for support of the distal frag-
ment. This procedu re observes the
basic principles already described
but has the theoretical advantage
that pelvic donor-site morbidity is
avoided. It should be reserved for
the patient with a wide rad ius in
the radioulnar dimension and the
patient with a strong aversion to
il iac-crest harvest or some con-
traindication, such as prior har-
vests.
The second alternative is a closing-
w edge os t eo tom y o f t he d i s t a l
radius.23 Radial platform correc-
tion may be effected with this tech-
nique, but it requires both resection
Fig. 5 PA (A) and lateral (B) views of the wrist of a p atient
with a d orsally tilted, short-ened radial articular surface. C an
d D, Reconstruction w ith an opening-wedge osteotomyand fixation
with an oblique T plate restored near-anatomic relationships at the
radio-carpa l joint and th e DRUJ. Care mu st be exercised to avoid
intra-articular penetr ation withthe screws in the d istal
fragment.
A B C D
-
8/4/2019 malunion colles
9/12
Malunited Distal Radius Fractures
Journ al of the American Academ y of Ortho paedic Surgeon
s278
of a l a rge por t ion o f t he r ad ia l
metap hysis and sacr i fice of the
DRUJ. There is little role for this
reconstruction, as more desirable
alternatives exist, except perhaps
for very low-demand patients with
poor bone stock.
If the radial platform demon-
strates excessive volar tilt in the
sagittal plane, the app roach taken is
opposi te to that for dorsa l t i l t .
Exposure can be performed throu gh
the distal aspect of Henrys flexorcarpi radialisradial artery
interval
for a straightforward malunion or
through a more generous approach
in which the carpal canal is released
and the skin is incised on the ulnar
side of the volar aspect of the fore-
arm. The la t ter app roach is re-
served for pat ients wi th severe
deformity, those with medial-side
int ra-ar t icular malunion of the
radius, and those with concomitant
median or ulnar neuropathy. The
radius is then exposed by entering
the interval between the ulnar neuro-
vascular bundle and the flexor digi-
to rum pro fund us t endons . The
pronator quadratus is elevated from
the la tera l s ide of the rad ius ineither exposure.
An opening-wedge osteotomy
from the volar aspect should ac-
complish the correction. A precon-
toured T plate can be used to fix the
distal fragment and intercalary graft
and thereby restore the integrity of
the volar rad ius (Fig. 8). Typically,
there is minimal shortening in volar
malun ions, and anatomic correction
will require only an osteotomy and
plate stabilization, with a minimum
of grafting. If surg ery is requiredon the ulnar side, the
options for
exposure of the ulna include addi-
tional deep dissection through the
same dorsal approach used to per-
form the osteotomy and/ or addi-
tional incision from the volar side or
the subcutaneous border.
Intra-articular Malun ion
Correction of an intra-articular
malunion is more challenging than
reconstruction of an extra-articular
m a lun ion . M any pa t i en t s have
both an intra-articular and an extra-
ar t icular m alunion of the dis ta l
radius. Cross-sectional imaging isgenerally necessary to
characterize
the location an d extent of d eformity.
Wrist arthroscopy may have a role
in preoperative and intraoperative
assessment.
Saffar described alternatives for
the surgical management of intra-
articular malunions based on the
location of the incongruity.24 His
recommendations are summarized
in Table 3.
Saffar d oes not p ropose rad io-
scaphoid fusion and radioscapholu-
nate fusion as alternatives for treat-
ment of some intra-articular malu-
nions, but these procedures should
be considered . There are as yet no
outcome studies that establish the
efficacy of intra-articular corrective
osteotomies. A long-standing intra-
articular malunion is a technical
challenge, and there is a high likeli-
hood that wrist arthrodesis may
eventually be required . If the mal-
union is intra-articular with respectto the DRUJ, an ablation
procedure
may be preferable to a diff icult
reconstruction and lengthy rehabili-
tation.
Surgical Handlin g of the Ulnar
Side o f the Wrist
I prefer reconstruction of the
DRUJ relationship by radial osteot-
o m y a n d / o r u l n a r o st e o p la s t y ,
wh en possible. In some cases, non-
ana tom ic hea l ing o f t he d i s t a l
radius w ill be noted, but the radio-graphic measurements of the
plat-
form will still be acceptable with
the except ion of the rad ioulnar
length . In th is s i tua t ion, u lnar
shortening may restore the DRUJ
and p rov ide pa in r e l i e f a s t he
apposing articular surfaces of the
Fig. 6 PA (A) and lateral (B) views of the wrist of a p atient
with a d orsally tilted, short-ened articular su rface. C an d D, A
dorsal opening-wed ge osteotomy was used. Becausethe radius was
extremely narrow, minicondylar blade plates were used to secure
thegraft.
A B C D
Fig. 7 Schematic of a trapezoidal osteot-omy. The
corticocancellous graft used tocorrect the m alunion is harvested
from th edorsal surface of the radius.
-
8/4/2019 malunion colles
10/12
Thomas J. Graham, MD
Vol 5, No 5, September/October 1997 279
radius and ulnar are adequate ly
redu ced. Of course, the articular
cartilage must be of good quality.
Preoperative planning should min-
imize the need to perform ulnar
shortening when a radial osteoto-
my is done, but occasionally it is
needed.
If the DRUJ is not reducible byradia l os teotomy or i f a r
thros is
exists on the ulnar or radial aspect
of the joint, some type of ablation is
indicated. How ever, ablation of
the ulna potentially compromises
the axial load ing chara cterist ics
about the wrist and may result in
decreased strength and stability.25
The opt ions for abla t ion of the
DRUJ fall into three general cate-
gor ies 26-28: (1) complete d is ta l
ulnar excision (Darrach resection
and its variations), (2) partial distalu lnar excis ion (e .g .
, Bowers
hemiresection interposition tech-
nique, Watsons matched resec-
t ion ), and (3) d i s t a l r ad iou lna r
arthrodesis with creation of a prox-
imal ulnar p seudarthrosis (Sauv-
Kapandji procedu re).
The decision to do an ulnar-side
procedure often comes after recon-
struction of the radius. In most
cases , a wel l -p lanned and wel l -
executed radial osteotomy will re-
store the DRUJ and lead to recovery
of forearm rotation, obviating the
need for surgery on the ulnar side. Ibelieve there is little
difference in
outcome between the various types
of ulnar resections performed in
conjunction w ith rad ial osteotomy,
provided one adheres to recom-
mended indications and techniques.
Excessive distal ulnar excision with-
out stabilization, performance of the
hemiresection interposition tech-
nique when there is an incompetent
TFCC, or ulnar surgery when there
is global forearm -axis instability
(e.g., after an Essex-LoPresti injury)
can lead to suboptimal results. If
the situation calls for DRUJ ablation,
the Darrach resection or th e hemire-
section interposition technique is
genera lly effective.
Postoperative Care andRehabilitation
A sugar-tong splint is applied at
the conclusion of the operation,
which is changed to a short-arm
cast 10 to 14 days later. A remov-
able orthosis is substituted at 4 to 6
weeks , and gent le wr is t mot ion
and forearm rotation are begun.
When tenderness at the fracture
site diminishes or when definitive
signs of healing are identified rad io-graph ically, the
orthosis is d iscon-
tinued. A systematic, but not overly
rigorous, regimen of rehabilitation is
used to restore motion and strength.
A concentrated effort is made to
restore forearm rotation, especially
supination.
Com plications and SalvageProcedures
Complications after distal radial
os t eo tom y inc lude f a i lu re to
ach ieve the d es ir ed a l ignm en t ,
ne rve dam age , nonun ion a t t he
os t eo tom y s i t e , and ins t ab i li t y
about the ulnar stump after resec-
tion. One par ticular comp lication
is l imitat ion of pron osup ination
due to DRUJ capsular contracture.
In a subset of patients, the radial
platform and the DRUJ are ana-
tomically realigned by rad ial os-
t eo tom y, bu t fo rea rm ro t a t ion
A B
Fig. 8 A, Malunion after a volar marginfracture. B, Anatomic
restoration after avolar opening-wedge osteotomy, bonegrafting, and
plate ap plication.
Table 3
Surgical Options for Treatment of Intra-articular Malunion,
According to
Saffar24
Description of Malunion Surgical Options
Scaphoid facet m alunion Intra-articular osteotom y
Radial styloidectomy
Proximal row carpectomy
Lunate facet m alunion Osteotom y for posterom ed ial fragm
ent
Radiolunate fusion for global
involvement
Global w rist involvem ent Early in tra-articu lar osteotom
y
Wrist denervation
Total w rist fusion
Anterior or posterior rim malunion Simple bone resection
-
8/4/2019 malunion colles
11/12
Malunited Distal Radius Fractures
Journ al of the American Academ y of Ortho paedic Surgeon
s280
r em ains lim i t ed . I f pa th o log ic
changes a t o ther locat ions have
been excluded, a contracted DRUJ
capsule may be the cause of prono-
supination loss, necessitating surgi-
cal treatment.
The DRUJ capsule, a structure
distinct from the TFCC, is particu-larly suited for its role in
accomm o-
dating the ulnar seat during fore-
arm rotation.29 Its volar and dorsal
components, continuou s with th e
stout proximal portion of the cap-
sule, are thin and capacious, allow-
ing motion at the DRUJ. In the
pathologic state, the capsule loses
its compliant nature and becomes
thick and scarred. This contracture
a lone has been show n to l im i t
DRUJ mot ion. A DRUJ capsulecto-
my is an effective way to restore
pron osupination. The TFCC mu st
be preserved w hen excis ing the
capsule.
Due to the nature of DRUJ rela-
t ionships du r ing rota t ion, volar
capsulectomy restores supination,
and dorsal capsulectomy restores
pronation; a combination is some-
times necessary. Volar capsu lecto-
my is performed through the inter-
val between the flexor carpi ulnaris
and the ulnar neurovascular bun-dle and then p erforming an
exci-
sion of the scarred capsule, protect-
ing the volar rad ioulnar ligament.
Dorsal capsulectomy is similarly
performed; the fifth dorsal com-
partment is incised, and the exten-
sor digiti minimi is transposed to
allow access directly to th e capsu le.
This operation can be combined
with radial osteotomy when intra-
ope ra t ive l im i t a t ion o f p rono-
supination is noted after successful
anatom ic correction.
For seve re o r l ong- s t and ingdeformities, additional
procedures
may be necessary. Release of the
pronator quad ratus may be n eces-
sary to achieve optimal improve-
ment. Staged lengthening by dis-
traction method s can be used in the
t r ea tm en t o f d i s t a l r ad ia l m a l -
unions resulting from trau ma in an
a d u l t p a t i e n t o r d u e t o g r o w t h
arrest in the distal radial physis.30
This is technically difficult to plan
and execute but is one of the few
motion-sparing procedures avail-
ab le fo r t he t r ea tm en t o f som e
severe deformities.
Some salvage procedures were
previously mentioned in the sec-
tion on intra-articular malunions
(Table 3). Comp lete fusion of the
wrist is the u lt imate salvage for
g loba l de fo rm i ty o r a r th r i t i s .
Partial fusions (radioscaphoid or
radioscapholunate) may have a
role in relieving pain and provid-
ing s tabi l ity . The pat ient mustaccept a d ecrease in m
otion or even
elimination of motion as the trade-
off for pain relief and sta bility. A
distal ulnar resection can be con-
sidered if only the ulnar column is
pro blematic. H owever , persistent
instability of the radiocarpal unit
about the distal ulnar stump may
necessitate further surgery.
Summary
The planning and execution of sur-gical reconstruction of a
malunited
distal radius fracture p resent a clin-
ical and techn ical challenge. The
surgeon shou ld establish his or her
own person al criteria for acceptab le
hea l ing and func t ion based on
available data and clinical experi-
ence, bearing in mind that not all
radiographic malunions are symp-
toma tic. Surgical han dling of the
distal ulna requires an understand-
ing of the anatomy and mechanics
of the DRUJ, as well as flexibility in
choosing w hether to reconstruct or
ablate the articulation. Preoper-
ative planning is critical to ultimate
success. Distal rad ial osteotomy is
among several procedures used as
salvage techniques after subopti-
mal healing of the original fracture;
the best results follow a natomic
res to ra t ion o f t he in i t i a l r ad ia l
injury.
Acknowledgments: I should like to thank
my friends and mentors Hill Hastings II,
MD, and William B. Kleinman, MD, for
their support and assistance in developing
many of these concepts, as well as for case
materials.
References
1. af Ekenstam F, Hager t CG: Anatom -
ical studies on the geometry and stabil-
ity of the distal radioulnar joint. Scand
J Plast Reconstr Surg 1985;19:17-25.
2. Friberg S, Lund strm B: Radiogra phic
measurem ents of the r adio-carpal joint
in normal adults. Acta Radiol [Diagn]
(Stockh) 1976;17:249-256.
3. Palmer AK, Glisson RR, Werner FW:
Ulnar variance determ ination. J Hand
Surg [Am] 1982;7:376-379.
4. Aro HT, Koivunen T: Minor axial
shortening of the radius affects out-
come of Colles fracture treatment. J
Hand Surg [Am] 1991;16:392-398.
5. Mann FA, Kang SW, Gilula LA: Nor -
mal palmar tilt: Is dorsal tilting really
normal ? J Hand Surg [Br] 1992;17:
315-317.
6. van d er Lind en W, Ericson R: Colles
fracture: How should its displacement
be measured and how should i t be
immobilized? J Bone Joint Surg Am
1981;63:1285-1288.
7. Knirk JL, Jupiter JB: Intra-art icular
fractures of the distal end of the ra dius
in young adults. J Bone Joint Surg Am
1986;68:647-659.
8. Short WH, Palmer AK, Werner FW,
Murph y DJ: A biomechanical study of
distal radial fractures. J Hand Surg
[Am] 1987;12:529-534.
9. Linscheid RL, Dobyns JH, Beabout JW,
http://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=4023639&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=4023639&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=4023639&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=4023639&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=4023639&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=4023639&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1274658&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1274658&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1274658&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1274658&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1274658&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1274658&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=7119397&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=7119397&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=7119397&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=7119397&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=7119397&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1861016&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1861016&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1861016&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1861016&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1861016&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1861016&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1624865&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1624865&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1624865&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1624865&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1624865&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1624865&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=7287798&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=7287798&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=7287798&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=7287798&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=7287798&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=7287798&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3722221&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3722221&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3722221&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3722221&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3722221&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3611649&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3611649&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3611649&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3611649&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3611649&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3611649&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=4653642&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=4653642&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3611649&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3722221&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=7287798&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=7287798&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1624865&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1861016&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=7119397&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1274658&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=4023639&Dopt=r
-
8/4/2019 malunion colles
12/12
Thomas J. Graham, MD
Vol 5, No 5, September/October 1997 281
Bryan RS: Traum atic instability of the
wrist: Diagnosis, classification, and
pathomechanics. J Bone Joint S urg A m
1972;54:1612-1632.
10. Taleisnik J, Watson HK: Midcarp al
instability caused by ma lunited frac-
tures of the distal radius. J Hand Surg
[Am] 1984;9:350-357.
11. Ada ms BD: Effects of rad ial deformityon d istal radioulnar
joint m echanics. J
Hand Surg [Am] 1993;18:492-498.
12. Fernandez DL: Corrective osteotomy
for extra-articular malunion of the dis-
tal radius, in Saffar P, Cooney WP III
(eds): Fractures of the Distal Radius.
London: Martin Dunitz, 1995, pp 104-
117.
13. Fourrier P, Bardy A, Roche G, Cisterne
JP, Chambon A: Approche dune dfi-
nition du cal vicieux du poignet. Int
Orthop 1981;4:299-305.
14. Pogue DJ, Viegas SF, Patterson RM, et
al: Effects of distal radius fracture
malunion on wrist joint mechanics. J
Hand Surg [Am] 1990;15:721-727.
15. Graham T, Hastings H: Management
of the distal radio-ulnar joint in post-
traumatic deformity of the rad ius, in
Vastamki M, Vilkki S, Gransson H,
Jaroma H, Raatikainen T, Viljakka T
(eds): 6th Congress of International
Federation of Societies for Surgery of
the Hand (IFSSH ). Bologna, I taly :
Monduzzi, 1995, pp 571-574.
16. Jup iter JB, Ring D: A compa rison of
early and late reconstruction of mal-
united fractures of the distal end of the
radius. J Bone Joint Surg Am 1996;78:
739-748.
17. Fernand ez DL: Radial osteotomy and
Bowers ar throplasty for ma luni ted
fractures of the distal end of the radius.
J Bone Joint Surg Am 1988;70:1538-1551.
18. Fernand ez DL: Correction of post-
trauma tic wrist deformity in adu lts byosteotomy,
bone-grafting, and internal
fixation. J Bone Joint Surg A m 1982;64:
1164-1178.
19. H a u c k R , Ka h l e r S, M a n d e r s E :
Trigonometric preoperative planning
fo r d i s t a l r ad i us o s t eo t omy , i n
Vastamki M, Vilkki S, Gransson H,
Jaroma H, Raatikainen T, Viljakka T
(eds): 6th Congress of International
Federation of Societies for Surgery of
the Hand (IFSSH ). Bologna, I taly :
Monduzzi, 1995, pp 161-164.
20. Jupi ter JB, Ruder J , Roth DA:
Computer-generated bone models in
the planning of osteotomy of multi-
directional distal radius m alunions.
J Hand Surg [Am] 1992;17:406-415.
21. Haga n HJ, Hoop er WE: Provisional
fixation of distal radial osteotomies
using the AO small external fixator. J
Hand Surg [Br] 1993;18:343-345.
22. Watson HK, Castle TH Jr: Trapez oidal
os t eo t omy o f t he d i s t a l r ad i us fo r
unacceptable articular angu lation after
Colles fractur e. J Hand Surg [Am]
1988;13:837-843.
23. Posner MA, Ambr ose L: Malunited
Colles fractures: Correction with a
biplanar closing wedge osteotomy. J
Hand Surg [Am] 1991;16:1017-1026.
24. Saffar P: Treatment of distal radial
i n t r a -ar t i cu l ar mal un i ons , i n
Vastamki M, Vilkki S, Raatikainen T,
Viljakka T (eds): Current Trends in
Hand Su rgery: Proceedings of t he 6th
Congress of the International Federation ofSocieties for Surgery
of the Hand (IFSSH),
Helsinki, 37 July 1995. Amsterdam:
Elsevier Science, 1995, pp 249-258.
25. Petersen MS, Ada ms BD: Biomechan -
ical evaluation of distal radioulnar
reconst ruct ions. J Hand Surg [Am]
1993;18:328-334.
26. Bowers WH: Distal radioulnar joint
arthroplasty: The hemiresection-inter-
position technique. J Hand Surg [Am]
1985;10:169-178.
27. Watson HK, Ryu J , Burgess RC:
Matched d istal ulnar resection. J Hand
Surg [Am] 1986;11:812-817.
28. Taleisnik J: The Sauv-Kap and ji pro -
cedure. Clin Orthop 1992;275:110-123.
29. Kleinman WB, Graham TJ: The DRUJ
capsule: Clinical anatomy and role in
post-traumatic limitation of forearm
rotation. Presented at the 50th Annual
Meeting of the American Society for
Surgery of the Hand, San Francisco,
Septem ber 1316, 1995.
30. Burge ss RC: Use of the Ilizarov tech-
nique to treat radial nonunion with
physea l a r r es t . J Hand Su rg [Am]
1991;16:928-931.
http://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=4653642&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=4653642&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=4653642&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=4653642&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=4653642&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=6725893&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=6725893&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=6725893&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=6725893&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=6725893&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=6725893&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=8515022&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=8515022&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=8515022&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=8515022&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=8515022&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=7228467&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=7228467&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=7228467&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=7228467&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=7228467&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=7228467&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=2229966&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=2229966&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=2229966&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=2229966&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=2229966&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=2229966&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=8642031&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=8642031&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=8642031&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=8642031&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=8642031&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=8642031&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=8642031&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3198679&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3198679&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3198679&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3198679&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3198679&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=6752150&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=6752150&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=6752150&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=6752150&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=6752150&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=6752150&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=6752150&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1613212&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1613212&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1613212&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1613212&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1613212&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1613212&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=8345264&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=8345264&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=8345264&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=8345264&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=8345264&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=8345264&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3271005&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3271005&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3271005&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3271005&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3271005&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3271005&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1748745&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1748745&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1748745&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1748745&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1748745&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1748745&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=8463602&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=8463602&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=8463602&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=8463602&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=8463602&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3980927&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3980927&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3980927&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3980927&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3980927&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3794235&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3794235&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3794235&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3794235&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3794235&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1735199&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1735199&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1735199&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1735199&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1940176&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1940176&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1940176&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1940176&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1940176&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1940176&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1735199&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3794235&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3980927&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=8463602&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1748745&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1748745&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3271005&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=8345264&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=1613212&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=6752150&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=3198679&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=8642031&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=8642031&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=2229966&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=7228467&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=8515022&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=6725893&Dopt=rhttp://www.ncbi.nlm.nih.gov/cgi-bin/Entrez/referer?/htbin-post/Entrez/query%3fdb=m&form=6&uid=4653642&Dopt=r