Embed Size (px)
Citation preview

Lyme Disease: Considerations for Dentistry
GaryM. Heir. DMDAssociate Clinical ProfessorTMD and Orofacjal Pain CenlerUniversity of Medicine and DentistryNew Jersey Dental SchoolNewark, New Jerseyand Private PracticeBayonne, New Jersey
Lesley A, Fein, MD, WIPHCurrently, Pnvate PracticeWest Caldwell, New JerseyFormerly, MemberNew Jersey Task Force on Lyme
DiseaseFormerly, MemberCongressional National Health Care
Reform Task Force
Correspondence to:Dr Gary M. Heir718 BosdwayBayonne, New Jersey 07002
Althongb Lyme disease bas spread rapidly and il is difficult todiagnose, a review of the dental literature does not reveal manyreferences to this illness. Dental practitioners must be aware of thesystemic effects of tbis often multiorgan disorder. Its clinical mani-festations may include facial and dental pain, facial nerve palsy,beadacbe, temporomandibular joint pain, and masticatory musclepain. Tbe effects precipitated when performing dental procedureson a patient witb Lyme disease must also be considered. Tbisstudy discusses tbe epidemiology and diagnosis of Lyme disease.Its prevention, and factors to consider when making a differentialdiagnosis. Dental care of the patient with Lyme disease and cur-rently available treatments also are considered. Three case reportsare presented.J OROFACIAL PAIN 1996;10;74-86.
key words: Lyme disease, orofacial pain, temporomandibular,facial nerve palsy, spriochetal disease, borreliosis
The rapid spread of Lyme disease in the United States hasreached epidemic levels. Symptoms of Lyme disease canmimic hundreds of other disorders and create a diagnostic
dilemma for dentists and physicians.' Despite this, a review of thedental literature finds a paucity of references to this illness.
Lyme disease was first reported in the medical literature in 1977as "a previously unrecognized clinical entity, the epidemiology ofwhich suggest transmission by an arthropod vector."- AlthoughLyme disease was only first described in the late 1970s, there isreason to believe that this condition has been a problem for amuch longer time.- The emergence of Lyme disease m the UnitedStates in this century is thought to have occurred because of éco-logie conditions favorable for deer. The reported national inci-dence of Lyme disease in 1993 was 3.3 per 100,000 population.^From 1982 through February 1995, a total of 69,626 cases occur-ring in 49 states were reported to the Centers for Disease Control(CDC) (information provided by the Lyme Disease Foundation,Hartford, CT, 1995).
Lyme disease is caused by a bacterial infection transmitted bythe bite of certain very small infected ricks. The bacteria is a coiledspirochete, known as Borrelia burgdorferi. It is named for DrWilly Burgdorfer of the US Public Health Services who first identi-fied the spirochete in the bodies of the deer tick that carry it."*
Lyme disease, or Lyme borreliosis, which is caused by threegroups of the spirochete Borrelia burgdorferi, is transmitted inNorth America, Europe, and Asia by ticks of the ¡xodes ricinuscomplex. The most important Lyme infection-carrying tick in the
7 4 Volume 10, Number 1, 1996

Heir/Fe in
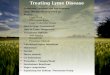
Northeast is the deer tick, or Ixodes dainmini.This tick is very smalls in the tiymph stage it iscomparable in size to a poppy seed (Fig 1). Ticksare active not only in the summer motiths as iscommonly thought, hut also at tetnperatures aslow as 35 °F.
Prevalence
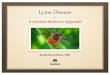
Demographic profiles of those infected withBorrelia burgdorferi, or Lyme disease, indicatethat individuals in suburban and rtjrai areas are athigh risk.' Victims of Lyme disease now number inthe thousands. It has become the most prevalenttick-borne disease in the United States, and its geo-graphic distribution appears to be spreading.''Although more than 60,000 cases have beenreported in this country dtjriog the past decade,health officials acknowledge that this number is agtoss underestimate.''''* The CDC reported that thenumber of Lyme disease cases rose 17% in 1991from those reported the previous year. In 1990,there were 7,943 reported cases; in 1991, 9,344cases were reported.' It is believed that these num-bers reflect only 75% of those individuals actuallyinfected. One county in New Jersey reported anincrease of an amazing 322% in 1993.' In 1994,11,835 cases were reported to the CDC (Fig 2).''
Although Lyme disease has heen found in 49states, it is concentrated in relatively few. Theyare the east coast states of Massachusetts, Con-necticut, Rhode Island, New York, New Jersey,Pennsylvania, Maryland, and Delaware. Otherareas of the country in which this disease has alsobeen reported are the north central and westernstates of Wisconsin, Minnesota, Michigan, andCalifornia, In these states, the bite of the westernblack-legged tick, ¡xodes pacificus, is the source ofmfection"* (Tahle 1¡.
i i I M i I i l l M n IFig 1 Ixadcs ddimnini from nympb to adult stage, com-pared ro tbe head of pin. Tbe tick may vary in size fromapproximately 0.5 mm ro 2.5 mtn.
1982 1983 1984 1985 19a6 1937 1988 19S9 1990 1991 1992 1993 1994
Vear
Fig 2 Increased prevalence of Lyme disease.
Journal of Orofacial Pain 75

Heir/Fein
Table 1 Incidence of Lyme Disease by State"
State
ALAK
AZARCACOCTDE
DCFLGA
HIID
ILIN
lAKSKYLAMEMDMAMlMNMSMOMT
NENVNHNJNMNYNCNDOHOK
ORPARlSOSDTNTXUT
VTVAWAV WWlWY'
Totai
1980
00a0
00
5200010000000001
11060000i0
10070000D130000Q
0000
25
0106226
1982
0
00000
1351
0000000000007
150
22000000
570
170000002
39000010Û
00
580
497
1983
0001
11
073
400
00000000004
131
55000001
700
26710001
020
0011100
00
690
594
1984
0004
24
0483
1
00!0Û01000Ü0
11
330
86020000
1550
46616030
105
201
01
18001
00
1760
1518
1985
0000
700
699
0021002010001
2069
164
010000
1750
123514
0205
294t
304
!72002
00
135
04
2752
1986
10û
0107
000002
0001
10004
15163
094
010007
2190
4626022
103157
301
8107
00
1620
21389
1987
1000
182
0215
601400
634
1300
27
954
9404
0000
257
0377
20
142
196574
321
3300
27
30
3580
22394
1988
100
16200
2362
40
053
0150
150521
66802167
65000
8500
02637
191
3944
306121
\02
131821
2595
246
0
4882
1989
2500
10250
1774
2506
7151
4279
8271521
23
138
12916592
7108
007
3680
53224
6112
99165
626415
183
3082
3
154
3315
762
6
8803
1990
3300
22345
0704
54
57
16121
301516141839
238117134
707
2050024
1074
03244
87
3361311
553101
72
2844
1
11129
3011
3375
7943
1991
1811
29323
11221
72
52331
02
2513222243
69
27429011085
-193
020
7
35852
03357
312
17331
51022
17710
145
1537
2023
44424
9
9344
1992
to00
21231
01760
2133
2423
2
24121331828
71
183212
35201
0150
015
1
49681
2
337065
2
326
131119274
21
3373
69
12314
14525
5
9658
1993
4008
134
01350
1432
3044
12
1932
854163
18180
14823
141
0103
065
15786
2
2818862
30198
1085272
90
2048
212
959
50401
9
8257
1994
6008
831
176278
927
10603
11141714
232
27379256
33
1650
37021
311303
84417
770
7876
01327471
7
01345
3
13129
027
05
11144
2/95
000071010
000000
03000
3090
0000010
24
01330600
11601
000
00104
00
225
Total
99
11
119
19676
9590607
24
1201142
653
218108144141
1572573
15731640
5271244
20364
04325
1536843
17
26589513
2251416991
62872075
74
11190557
2354
795106170
367839
11469626
'Information provided by the Lyme Disease Foundation, iHartford, CT, IStUnknowrt,
76 Volume 10, Number 1, 1996

Heir/Fein
In nature, the Lyme disease hacteria exists in acycle involving ticks and small animals. Deer ticksprefer to live in the woods; dense, mature woodswith a thick undergrowth of shrubs and small treesare their favorite habitat. They also are found, to alesser degree, along the edge of the woods wherethe lawn meets the woods." They are spread inthe wild by animals such as birds, mice, raccoons,and deer, but domestic animals such as cats, dogs,horses, and cows can also carry infected tickscloser to and into the home."' When mice becomeinfected, they remain so for long periods of timewithout any apparent ill effects; however, theyspread the infection to immature ticks that feed onthem. These infected ticks then sptcad the diseaseto other rodents and animals as well as humans.Adult ticks seem to prefer to feed on larger ani-mals, especially deer. Deer are resistant to Lymeinfection and do not directly participate In the lifecycle of the Lyme hacteria except to provide bloodmeals for adult ticks and to potentially carry theticks to regions not previously invaded. More than20 species of birds are known to be infected andhave been theorized to transport the ticks ovetgreat distances, resulting in spread to previouslyunaffected areas,'- Fortunately, Lyme disease doesnot appear to be communicable betweenhumans,'"
Signs and Symptoms
The tick bite is usually painless and may go unno-ticed because the tick injects a local anesthetic atthe site of the hite. Symptoms of Lyme disease mayvary and can appear days or even years after anindividual is hitten by an infected tick. Early symp-toms of Lyme disease may appear within days orweeks of a tick bite and can improve within sev-eral weeks, even without treatment,'-''"^ Delayedsymptoms of untreated Lyme disease can occur atany time of the year and frequently follow monthsof dotmancy during which patienrs are asymp-tomatic. Late symptoms may appear weeks,months, or years later and may improve or comeand go without treatment. In some cases, theremay be no symptoms at all, which makes the dis-ease difficult to diagnose.'^
One of the first symptoms of infection is a char-acteristic red, circular, expanding rash, the borderof which IS raised and warm (Fig 3). This rash isnamed erythema migrans (EM), Estimates suggestthat it may present m less than 50% of tick hites oror may go undetected. Generally painless, it issometimes associated with a mild stinging or itch-
hig 3 Eryrhema migrans rash, (Courtesy of Roberr A,Schwartz, MD; reprinted with permission from Curis1991;47:229.i')
ing. This rash can begin at least 4 days after thebite but might not appear for several weeks. Theappearance of the rash is not always associatedwith other physical signs of illness. In less than10% of reported cases, the rash could appear inseveral places as erythema chronicium migrans, inaddition to the site of the bitc,'^
As will be demonstrated in the following casereports, "An accurate and detailed medical histotyand careful physical examination form the basisrequired for arriving at a correct diagnosis ofLyme disease. Medical history and physical exami-nation are of particular importance in this diseasebecause currently available laboratory tests are lessthan satisfactory.'"'
Symptoms and clinical findings of the variousstages of the disease are listed in Table 2,
Lyme Disease—A Multisystem,Multiorgan Disease
The stages of Lyme disease may be divided intoearly, disseminated, and chronic. Patients havereported a variety of symptoms that have beenassociated with these different stages (Table 3).
Dental Concerns
Dental patients with a history of Lyme diseaserequire special considerations. When practicing inareas hyperendemic for Lyme disease, health statusinterviews or questionnaires must explore the pos-sibility of Lyme disease in the same way a patientwould be interrogated concerning any other perti-
Journal of Orofacisl Pain 77

Heir/Fein
Table 2 Manifestation of Lyme Disease iiy Stage'
Early Infection
Systemt
Skin
Localised stage 1 Disseminated stage 2
Erthyema migrans (EM)
Muscuioskeietal
Neuroiogic
Lymphatic
Heart
Eyes
LiverRespiratory
Kidney
GenitourinaryConstituíional symptoms
Regio na i lymphadenopathy
Minor
Secondary annular lesions
Diffuse erythema or urticanaEvanescent iesionsLymphocytomaMigratory pain in joints,
tendons, bursae. muscle,bone
Brief arthritis attacksMyositis'Osteomyelitis'
Panniculitis'MeningitisGranial neuritis, Beil's paisyMotor or sensoryradicuioneuritis
Subtle encephalitisMononeurilis multiplexMyelitis'Chorea'Cerebeliar ataxia'Regional or generaiized
iymphadenopathySplenomegaiyAV node biockMyoperi carditisPancarditisConjunctivitisiritis'Choroiditis'Retinai hemorrhage or
detachment'Panopthaimitis*Mild or recurrent hepatitisNon exudative sore throatNonproductive coughAduit respiratory distress
syndrome'Microscopic hematüria or
proteinuriaOrchils'Severe malaise and fatigue
Late Infection
Persistent stage 3
Acrodermatitis chronicatrDphicans
Prolonged arthntis attacks
Chronic arthntisPeripherai enthesopathyPenostitis or Joint
EubiuKations beiowacrodermatitis
Subtie mentai disordersAxonai poly neuropath yLeukoencephalitis
EncephaiomyelitisSpastic paraparesisAtaxic gaitDementia'
Cardiomyopathy
Karatitis
Fatigue
The staging system provides a guideiine tor ttie expected timing o( the different maniFestationstThe systems are iisted from ttie most to the ieast commoniy affectedtSince tlie inclusion of this manifestation is based ori one or a lew cases, it shouid he oonsideied possibie but not pidiseases.
iiiess. but this may vary in an individual patient
78 Volume 10, Number 1, 1996

Heir/Fein
Table 3 Patient Complaints
Eariy
EM rash
Disseminated
Early
Joint pains
Body achesNight sweatsSensitivity to light, sound,touch
Migratory painsFatigueBeii's paisy
Heart paipitationsSwoilen giandsStiff neckWorsening of asthmatic
symptomsDisorientadonLyme fog
Conjunctivitis
Sleep disturbances
Late
Severe headache,migraine headache
Crippling arthritis
Swoiien jointsHeart problemsHypersensitivity lo light,sojnd.touch
Cnppling migratory painsSevere fatigueProblems with vision andincreased eyecomplications
SeizuresNose biee elsMemory lossConfusion (Lyme fogJ
Dyslexic reversalsSleep disturbances,nightmares
Reports Or abnormal magneticresonance images, computerizedaxial tomography scans,elect roencephalograms,cerebrospinal fluid
Gaslrointestinal symptoms
Chronic
Migraine headache
Arthntis
Loss of libido
Muscle weaknessFatigueDisequilibrium
Dyslexia
Hearing los
nent medical history.-** It may not be enough tomerely ask the patient if he or she was ever diag-nosed as having Lyme disease. The dental practi-tioner must be suspicious of the patient who pro-vides a diverse medical history with multisystemcomplaints that seem to run in cycles; unexplained,recurrent illnesses require further investigation.-'
Premedication
A percentage of dental patients require prophylac-tic antibiotic therapy for dental procedures. Thismay be because of a history of cardiac disorders,or other issues. However, when providmg antibi-otics for patients who have or have had Lyme dis-ease, special considerations are necessary.
The infectious organism of Lyme disease, B.burgdorferi, can "hide" in tissue and seems to havethe ability to remain dormant for long periods oftime. The administration of antibiotics for any rea-son may result in an untoward effect on thepatient's immune system, causing what is known asa Jarisch-Herxbeimer reaction. Commonly knownas Herxheimer reaction, the patient experiences an
exacerbation of Lyme disease-related symptomsthat may last from a few days to a few weeks. TheJarisch-Herxheimer reaction is a clinical syndromeoccurring soon after the first adequate dose of anantimicrobial drug to treat infectious diseases stichas Lyme disease, syphilis, and relapsing fever. ^This reaction may be misconstrued as an allergicresponse by the patient or treating doctor, but acareful history may find otherwise.^' In fact, theprecipitation of Herxheimer reaction may assist inarriving at a diagnosis where none had been possi-ble in the past.
Possible Effects From Dental Treatment
Exacerbation of Lyme disease-related symptomsmay also arise from dental procedures that involvedisturbance of connective tisstie, such as periodon-tal surgery and endodontia. Spirochetes seem tohave an affinity toward connective tissue. "Whensurgical or invasive procedures are performed, theresultant healing and scar tissue formation mayattract these organisms and result in increasedsymptoms.-'*•-•'
Journal of OrofacisI Pain 79

Heir/Fein
The introduction of an infectious process pro-duces an immune response to its antigens. It hasalso been postulated that this response to Borreliahurgdorferi may trigger the onset of an autoim-mune disease. "However, inflammatory diseasesseem to continue, even when the organism is seem-ingly eliminated. In fact, many inflammatory dis-eases thought to be of an autoimmune nature mayactually be caused hy an immune response directedagainst non viable, but persistent microbial anti-gens present in the target tissues, or ever? againstoccult viable infectious organisms."^'' As with anysimilar disease process, when the patient is physi-cally challenged by trauma, nonrelared illnesses, ordental procedures, a fiare of the autoimmune/Lyme disease—related symptoms may he antici-pated.
Lyme disease rather than the result of primarytemporomandibular disorders.-' Temporo-mandibular disorders symptomology usuallyoccurs early in the course of Lyme disease.- "** Ameticulous clinical evaluation and history are vitalin arriving at a differential diagnosis.
Neuralgia
Neuralgic facial pain. Bell's palsy, pain of the mas-ticatory musculature, and TMJ pain are character-istic of Lyme disease and may cause a patient toseek a dental exatnination, as the following casereports illustrate.^^• ''
Case Reports
Temporomandibular Disorders
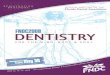
Lyme arthritis has commonly been associated withlarge peripheral |Omts such as the knee. However,the temporomandibular joint {TMJ) is the fourthmost commonly affected joint in Lyme disease.-'"The synovial memhrane becomes hypertrophiewith numerous folds producing villus like struc-tures overlaid by hyperplastic synovial cells.Varying degrees of synovial edema are present.The presence of vasculopathy within the synoviumand extensive fibrin deposits in the stroma are verysuggestive of Lyme arthritis, even in the absence ofclinical history."^^ Arthroscopy of the temporo-mandibular joint of a Lyme disease-infectedpatient, as In other joints so affected, reveals sig-nificant synovial inflammation and swelling(Hoffman D. TMD and Orofacial Pain Center,University of Medicine of New Jersey, unpublisheddata, 1995) (Figs 4a and 4b). Patients may presentwith ear pain, TMJ pain, or claudication of themasticatory musculature, which is secondary to
Case 1
JG is a 49-year-old woman with a 14-month historyof neurologic symptomology. On close questioning,it was concluded that her symptoms probably datefurther back than that. Her chief complaints were:
1. Facial pain2. Facial numbness3. Pain in the left eye4. Numbness of the extremities5. Joint pain6. Difficulty concentrating
The numbness was originally of the left side ofthe face but appeared to spread more inro the leftside of the forehead with time. It was occasionallyassociated with pain in the left eye and bilateralblurred vision. In retrospect, she recalled that shealso had symptoms of extremity paresthesias and|Oint pam as well as cognitive dysfunction. How-ever, she failed to mention these symptoms untilmuch later.
Figs 4a and 4b Artiiroscopic viewsof the temporomandibular joints oftwo patients with confirmed Lymedisease demonstrate significant syn-ovial hypertrophy. Capillary invagi-nation of the synovial plica (left);vascularity of the synovial hyperpla-sia (right). (Courtesy of DavidHuffman, DDS).
8 0 VolLime 10, Number 1. 1996

Heir/Fein
Initial neurologic evaluation revealed hyper-reflexia and extensor plantar responses. A mag-netic resonance itnage (MRI) of the brain was neg-ative, the cervical spine was positive for a stiiallleft C5-6 herniated disc, and the thoracic spinewas positive for a central disc htiige at T6-7, Itwas thought that neither her symptoms nor signswere related to these findings.
By the time symptoms were present for LI fullyear, she had undergone extensive dental tteattuetit,which included restorations, endodontia, and anapicoectomy, with no resolution of her facial painand numbness. Her neurologic examination wasunchanged, A spinal tap was performed, revealingthe presence of oligoclonal bands, Serologie testingrevealed a Lyme disease titer that was positive, aswas a Western Blot, Spinal fluid was analyzed andwas borderline positive on enzyme-linked immuno-sorbent assay (ELISA) testing, although no WesternBlot or Polymerase Chain Reaction test was per-formed. Following the spinal tap, the patient devel-oped Ittmbosacral pain that has persisted, with anew onset of palpitations. A lumbar spine MRI re-vealed early degenerative joint disease without dischern i a ti on.
The patient was finally treated for Lyme diseaseafter approximately 2 years from the date of onsetof her complaints. The treating physician immedi-ately initiated therapy with oral amoxicillin.During the first week of therapy, the patient expe-rienced severe exacerbation of her palpitations andhad an abnormal electrocardiogram suggestive ofmyocarditis. This is consistent with a Herxheimerreaction, which is well known in Lyme disease,and strongly supports the diagnosis. This reactionalso should be perceived as supportive evidencethat in fact, she does have cardiac involvement,even in the absence of a positive echocardio-gram.'-"- ''
The patient was admitted to the hospital withina few days of initiation of treatment. Intravenousceitriaxone sodium (Rocephin, Roche Laborator)',Nutley, NJ) was administered for prestjmptiveLyme carditis. The patient was continued on thismedication for S weeks. She reported an initialflare of symptoms, followed hy improvement last-ing for several weeks, then another flareiip severalweeks later, which slowly resolved. This is fairlycommon in patients with Lyme disease becausethey enter cyclical phases during treatment. At anexamination performed several months into treat-ment, the patient reported feeling considerably bet-ter but was still quite symptomatic. Of most con-cern was her significant cognitive dysfunction.Although she is a mathematician, she no longer
teaches. She noticed that she would either forgetwhat she was writing on the blackhoard or wotddput something down other than what she hadintended. She became disoriented and confused,and she developed short-term memory loss. Shewas also clearly depressed despite taking fluoxe-tlne hydrochloride (Prozac, Dista Products,Indianapolis, IN),
The most recent Western Blot performed waspositive for IgG proteins consistent with Lyme dis-ease. Her most recent electrocardiogram was unre-markable and her examination revealed a hlankfacial expression that could be mild paresis or sim-ply a reflection of her depressed affect. She does nothave complete facial palsies; however, incompletefacial palsy, which has heen seen clinically in patientswith Lyme disease, improves with treatment.
Case 2
CC is a 28-year-old woman who was referred for afacial pain evaluation. Her chief complaints were:
1, Stabbing pain in the left TMJ2, Bilateral facial pain during chewing, which
was descrihed as jaw muscle fatigue thatincreases with continued function
3, Migraine headache (diagnosed by the physician)4, Neck pain5, Upper body numbness6, Visual problems—persistent blurred vision
The patient also stated that she felt "deptessed andhandicapped." While her history was reviewed,she stared that she had been healthy until approxi-mately 1990, when she had several episodes of"big," swollen knees, which were treated by non-steroidal anti-inflammatories with apparent suc-cess. The knee problem resolved but left her withwhat she described as a "mild arthritis," Since thattime, she has experienced what was diagnosed asepisodes of chtonic sinusitis and sinus infection.There was occasional shortness of hreath. She wasgiven antibiotic therapy in June 1993, for approxi-mately 1 month. In July 1993, she experienced anacute migraine attack with "strokelike" symptoms,which included a left-side facial nerve palsy;numbness in her face; slurred speech; a tinglingsensation in her face, arms and hands; and blurredvision. The blurred vision persisted for 11 weeks.She also described possible claudication of legmuscles. She experienced additional episodes ofheadache, which were described as bilateral andarising from the shoulders and neck with radiatingpain into the forehead. Neck stiffness accompaniedthese headaches. The headaches were described as
Journal of Orofacial Pain 8 1

Heir/Fein
debilitating and were preceded by the blurredvision. The headaches would last several days orweeks. She also described episodes of stahhingpain in her face, which resulted in "facial droopi-ness" that for lasted several hours.
During the time prior to the episodes of swollenknees, she was quite active and enjoyed hikingalong tbe Appalachian Trail. During the past fewyears, however, she has felt more and more dis-abled. She stated that she no longer has felt confi-dent about driving. She added, "1 feel as thoughI've lost my independence due to the illness andconstant pain." She does not recall a tick hite.
This patient has been evaluated by many physi-cians, including neurologists and otolaryngologyspecialists. She had been given a variety of medica-tions with little effect. They include nonsteroidalanti-inflammatory drugs, subclinical doses of pro-pranolol hydrochloride ¡Inderal, Wyeth-AyerstLaboratories, St David, PA], and tricyclic antide-pressants, A brain MRI showed areas of plaque orenhancing lesions, hut this was not deemed clini-cally significant at the time.
An evaluation of the patient's TMJs and masti-catory musculature found that she had a normalmandibular range of motion, with slight crepita-tion of the left joint. Both joints wete moderatelytender to palpation, and the masticatory muscula-ture was also moderately to severely tender.Although the clinical presentation might haveaccounted for some of the facial pain andheadache complaints, it was believed to be respon-sible for only a small portion of her problems,
A palpatory evaluation of the cervical and upperback muscles was remarkable for multiple tenderareas. A cranial nerve screening evaluation waspositive for asymmetry of peripheral vision, whichwas less on the right (cranial nerve II), hyperalge-sia of the right cheek and forehead (cranial nerveV, divisions 1 and 2), ie, pain is produced by lighttouch, and a slight weakness of the left lip duringgrimace or smiling [cranial nerve Vtl).
The differential diagnoses were:
1. Capsulitis/synovitis of the TMJs, bilaterally2. Associated myalgia of the masticatory muscu-
lature3. Ruhng out of Lyme disease prior to accepting
the diagnosis of migraine4. Ruling out of fibromyalgia (characterized by
multiple, nonreferring tender points in muscles)5. Consideration of a demyelinating process such
as multiple sclerosis
Treatment options were discussed with thepatient regarding potential temporomandibular
disorders. She was also advised tbat local therapiesmight not be productive if other systemic condi-tions were present. She was referred for serologtctesting for Lyme disease, and the results were posi-tive. The patient is currently receiving antibiotictherapy and is improving. Since treatment began,she has not experienced any additional episodes ofTMJ pain, facial pain, or Bell's palsy.
Case 3
JN, a ,)4-year-old woman, presented for a facialpain evaluation with chief complaints of:
1, Pain of the right cheek2, Pain of the forehead and chin3, Paralysis of the lower half of the right side of
her face
Coincident with her pregnancy in 1993, thepatient developed a dental infection of the maxil-lary right first premolar. This tooth had priorendodontic therapy in 1991, and che dentistelected to petform an apicoectomy, which wasdone in July 1993. The patient described this pro-cedure as difficult and recalled that the woundrequired resuturing on four occasions. Eventuallyit was allowed to granulate in. She recalled thatsoon after this procedure, she began to experiencea sense of numbness associated with the surgicalsite as well as a dull aching sensation on the rightside of her face. She also became aware of "electri-cal jabs deep in the uppet jaw." She attrihuted thisdiscomfort to the "healing process" and antici-pated recovery. The discomfort seemed to persist,and there was point tenderness over the surgicallocation.
On the morning of January 28, 1994, she awokewith a partial palsy of the right side of her face.She was aware of an inahility to purse her lips.During the course of the day, the condition wots-ened until she was not able to close her eye, con-tain liquids in her mouth, or smile. She called herdentist who referred her to an oral surgeon. Onexamination, according to the patient, the surgeonoffered only two treatment options. They wereeither to repeat the apicoectomy or to remove theinvolved tooth. The tooth was subsequentlyextracted, hut as might have been anticipated, norelief of the Bell's palsy ensued.
The patient next contacted her obstetrician/gynecologist, who referred her to a neurologist.Facial nerve palsy was diagnosed. Diagnostic test-ing confirmed a lower motor neuron disorder.Because the patient was pregnant, medicationswere not considered.
82 Volume 10, Number 1,

Heir/Fein
Since onset, iacial muscle fnnction has returnedto approximately 80% ot" normal, but the patientcontinncs to experience n dull, aching, right, ortugging pain in her face extending from above theright eye, through her cheek and intu her maxillaryand mandibular right jaw.
A clmical exammatton fonnd no dental etiologyfor any facial pain cotnplaint. An evaluation of theTMJs and jaw function was unremarkable.However, a palpatory examination of the mastica-tory musculature did disclose multiple tender areasof these structures, particularly on the right.
A crantai nerve evaluation was positive forweakness of the facial nerve, particularly of themuscles of the lower half of facial expression. Thepatient was able to fully close both eyes. The righteye could be forced open, bnt not as easily asreported earlier by the patient's neurologist.
Although It was unlikely that any dental pathol-ogy or any of the dental procedures performed forthis patient were tn any way involved in the onsetof ßell's palsy, dental pathology was considered tobe the primary etiology hy her treating dentists.
Although the Bell's palsy seems to have evolvedcoincidentally with various dental surgeries, thereis no support for any connection between the con-dition and procedures. The onset of the paralysiswas remote from the dental surgeries. Initially, themedical history was unremarkable except for areport of asthma and minor allergies. However,after a series of sérologie tests, the patient testedpositive for Lyme disease.
Testing, Treatment, and Other Concerns
Laboratory Testing for Lyme Disease
The issue of laboratory resting for Lyme disease isone fraught with controversy.^^-^' The standardtest performed by most commercial laboratories isthe ELISA. Although this test has been studiedextensively, there are numerous test kits, many ofwhtch are unreliable. Several studies have demon-strated that the same tube of blood sent to differ-ent laboratories yield markedly disparate results.Certain autoimmune diseases are thought to causea false positive result, a factor further confusingthe issue. Very few laboratories in the country areconsistently accurate.
The Western Blot is a highly sophisticatedmethod of testing for Lyme disease. The patient'sblood is cross-reacted with a series of antigens thatare derivatives of the proteins of Borreiia burgdor-feri. This method is highly specific, since certain
fragments of these proteins are unique to thisorganism. As with other tests, the commercial kitsare variable in their sensitivity. Reagents need to bemaintained and purified under strictly controlledcircumstances. Again, there are only a handful ofspecialized laboratories with the advanced technol-ogy necessary to provide consistent results. Incon-sistencies havL- been observed between and withincommercial laboratories. Overall, combining all thestudies, the sensitivity and specificity of both testsare equal. When interpreting these tests, referral tothe recommendations of the CDC for standardiza-tion and interpretation of Lyme disease WesternBlot testing is suggested.
The Western Blot should be performed on ailpositive or equivocal ELISA specimens. In additionto the CDC recommendations, it must be pointedout that other proteins not included in the CDCrecommendations are now recognized as veryspecies specific for BorreUa burgdorferi and mustbe included in any study of any patient suspectedof having Lyme disease. An analysis of confirmedLyme disease in patients concluded that tests thatincluded these species-specific proteins not in-cluded in the CDC recommendations were 27.7%more specific than those that did not include them(Tilton RC, North American Analytic LaboratoryCroup, New Britain, CT, 1994).
Many immunologists disagree with the strainrestrictions and patient restriction. Based on 5,034positive specimens, it has been found that proteinsnot included in the CDC recommendations are sig-nificant and must be included in the criteria. ^ Byincluding these bands, the sensitivity of the resultsis increased from 74% to S7,2% (Tilton RC,North American Analytic Laboratory Croup, NewBritain, CT, 1994). Therefore, these proteins mustbe included despite the CDC recommendations.
In addition to the aforementioned commentsregarding CDC criteria, many clinicians disagreewith the CDC recommendations about performingWestern Blots only to confirm equivocal or positiveLLISA tests. An ongoing study that has analyzed20,000 cases reveals that a significant percentage ofpatients have positive Western Blots in tbe absenceof any findings on ELISA testing (Tilton RC,unpublished study. North American AnalyticLaboratory Group, New Britain, CT, 1995),
Both tbe IgM and the IgG Western Blots shouldbe used in the serodiagnosis of early Lyme disease.The specificity of the positive IgM blot critetiadecreases after this time, and positive IgM results inpatients with late symptoms must be viewed cau-tiously. Prior antibiotic therapy may invalidate theresults.'^ In any case, these are only recommenda-
Jojrnal of Orofacial Pain 83

Heir/Feir
tions, .ind the diagnosis remains one that is primarilyclinical. The laboratory should be used as a sec-ondary source for support for or against a diagnosis.
Two laboratories currently perform anothersérologie test called the enzyme capture assay,which is very specific for recent infection. In pre-liminary studies, this test has a 60% probability ofdetecting early cases.
Several laboratories are now doing thePolymerase Chain Reaction, which is a test inwhich specific genetic fragments of the bacteria aredetected in the blood, urine, spinal fluid, and syn-ovial fluid. The yield on this test is yet to be deter-mined. A urine test of great value is the LymeUrine Antigen test. This test is also a method ofdetecting the breakdown products of tbe Lymebacteria.
An additional blood test performed in only onelaboratory in the country is the Gunderson test.This test is for the detection of "killer" antibodiesin a patient's serum; ie, the ability of the antibodyto kill live bacteria in a laboratory setting. If posi-tive, this is a definite indication of infection.
Treatment
"Because infection rates in ticks are high, primarycare physicians are faced with the dilemma ofwhether to treat patients bitten by these ticksimmediately or to wait and treat them only if thesymptoms of Lyme disease develop.'"'" The LymeDisease Foundation currently advocates immediatepreventive antibiotic therapy at the first sign of atick bite in endemic areas.'" It is generally agreedthat early treatment is important.''^ Currentlyaccepted treatment includes antibiotic therapy. Insome cases, oral antibiotics are the treatment ofchoice. In more chronic cases, intravenous antibi-otic therapy is required."'•'"''' *
have these ticks where you don't have deer. Heand other experts have made the following sugges-tions'*'"''" to avoid Lyme disease for people whospend time in areas infested with Ixodes dammini,the tick that carries Borrelia hurgdorferi:
1. When in the woods, brush, or tall grass, socksand shoes should be worn, pants should havebottoms tucked into sboes, and shirts sbould betuckeci in with a snug collar, long sleeves, andcuffs. Brush and leaf litter should be avoided.
2. An insect repellent containing dietbyltolu-amide (DEET) should he applied and reap-plied as necessary to exposed skin, socks,lower pant legs, sleeve cuffs, and collars. Forchildren, repellent should be apphed to cloth-ing, not to skin.
3. After an outing, a shower should be taken towash iiway unattached ticks. A daily full-bodyexam should be performed on people andpets, keeping in mind that nymphs are the sizeof a pin head before feeding.
4. All ticks should be removed promptly withfine-pointed tweezers placed on the mouthparts, not the head or body, as close to theskin as possible. The area the tick came fromshould be washed and swabbed with alcohol.The tick should not be handled.
5. Individuals can make their yards inhospitahleto ticks by removing leaf litter and keepingsoil relatively dry. Borders should be cleanedup, and an insecticide should be used to treatthe yard edge and a little way into adjacentwooded areas.
6. Individuals should watch for the bull's-eyelesion: red with a clearing in the center thatmay follow infection. If an infection is sus-pected, medical help should be soughtpromptly.
Prevention
The control of Lyme disease is a difficult problem.Investigations continue to lead to a better under-standing of the complicated ecology of Lyme dis-ease, identifying areas where ticks commonly carrythe Lyme bacterium. Recent research has studiedmethods to make such endemic areas safer, includ-ing application of insecticides and the use of deerfences. Future methods may include host-targetedinsecticides, environmental alteration, and biologiccontrol."'
According to Fish,""- a medical entomologistfrom New York Medical College, "The big prob-lem is the suburbs, or the woodburbs. You don't
Research and Prognosis
With an increase in public awareness of Lyme dis-ease, research in treatment and prevention of Lymedisease has intensified. This research has takenthree distinctive avenues of investigation.
Currently there are very few reliable tests for thediagnosis of Lyme disease. At this time, the clinicalexpertise of the physician performing the examina-tion remains the key. Investigators are seeking newand reliable tests to confirm the presence of aBorrelia burgdorferi infection.
Although antihiotic therapy is the best treat-ment available for Lyme infection, the medica-tions used are not always 100% effective in all
84 Volume 10, Number 1, 1996

Heir/Fein
cases. The majority of patients do respond favor-ably; however, more specific antibiotics are beingdeveloped, which will hopefully result in motepredictable results. Ancillary treatment modalitiesinclude analgesia, antidepressants, acetazolamide(Diamox, Lederle Laboratories, St David, PA),nutritional supplements, and physical therapy.
A vaccine against Lyme disease is already avail-able for vetermary use. However, it is not yetavailable for use m humans, although experimen-tal versions are now being tested."* •"'" The efficacyhas not yet been determined. Unfortunately, rhereate substantial flaws in the study design that mayintetfere with the interpretation of results.''**- '
Summary
Lyme disease, a debilitating infection that maycause a variety of mild to crippling symptoms, hasbeen confounding patients and physicians formany years. Through diagnostic failure, mistreat-ment, and overtreatment, the cost to the publicand the physical and psychologic toll taken onthose suffering with this disease has been exorbi-tant. ' It is to be hoped that the spread of this dis-ease can be controlled with heightened public andprofessional awareness; dedicated physicians, den-tists, and health care providers; and advances inresearch. The public and health care professionsmust remain diligent in their pursuit of a solution.
Acknowledgment
The authors would like ro rbank Lori Heir for her assisraiicewith the researcli for this srudy.
References
1. Lukasik S, Wojtowicz A, Bctkowski A. OddzialuOwlatyngologicinego Szpitala Wojewodzkiegu Nr 1,Rzeszowie. Wiad Lek 1993;46:S06-510.
2. Steere AC, Malawista SE. Snydman DH, Shope RE,Andiman "WA, Ross MR, Steele FM. Lytne artbritis: Anepidemic of oligoarticular arthritis in cbildren and aduitsin three Cotinecticut communities. Arthritic Rheum1977;20:7-17.
3. Orloski K, Bailey R, Campbell G, Dennis D, Herrington J.Nanonal Surveillance for Lyme Disease—USA [pamphlet].Fort Collins, CO: Centers for Disease Control and Pre-vention National Center fot Infectious Diseases, DivisionofVector-Bornc Infectious Diseases, 1995.
4 Craft JE Scboen RT. Lyme Disease. Crotón, CT: PfiïerCentral Research. 1593.
5. Clinical Briefs. Am Fam Physician 1993;4B:155.
6. Diagnosis and treatment nf Lyme disease. NationalInstitute State of rbe Art Conference. In: Clinical Courier¡newsletter uf the National Insrirute of Arthriris andMusculoskeletal and Skin Dibcabes and National Instituteof Allergy and Infectious Disiabcl. l9SJ|;m.S).
7. Taylor GC. Lyme disease: An oi erview of its public healthbiynili^aiice. J Environ Health l991;.S4i2')-27.
a. ThaclcL-r SB, Kecwhan C. Brachman PS. The siirreiilanceof infectious diseases. JAMA I983;249|9):l 181-11 S.!.
9. Brandes J. Lymt disease in Hunterdon increases 322%.Star-Ledger 1993 Nov 4:.îO.
10. Centers for Disease Control and Prevention (CDC). Infor-mation .Service, Atlanta, 1994.
I I. Sniith-Fiola, Porcellini. Am Nurseryman 1991. Circd in:Prevent Tick Bircs: Prevent Lyme Disease. Rutgers Co-operativL Extension of Ocean Gounry, 1992.
12. Masters EJ, Donnel H, Fobbs M. Missouri Lyme Disease:1989-1992. J Spirocbetal Tick-Borne Disease Dis1994;H1).
13. Steere AC. Lyme disease—1993. Bull Rheum Dis 1993;42(61:4-7.
14. Sreere AC. Lyme disease. Proc Narl Acad Sei USA 1994;91(71:2378-2383.
15. Barbour AG, Fiih D. The biological and social phenomenonof Lyme dibease. Science 1993a6ü(Sll4¡:161O-lél6.
16. Burrascano JJ Jr. Managing Lyme Disease: DiagnosticHints and Treatmenr Guidelines fot Lyme Borteliosis, ed10. EastHamptom, NY, 199.Î.
17. Schutzer SE, Schwartz RA. Diagnosing Lyme disease.Often simple, often difficult. Cutis 1991;47:229-232.
IS. Steere AG. Lyme disease. N EngI J Med 1589;32]:586-596.
19. Land D, DeSilva DM. Coping With Lyme Disease. NewYork: Henry Holt, 1993.
20. Steere AC. Lyme disease: A growing threat to urban popu-lations. Proc Narl Acad Sei USA 1 994;91:2378-23 83,
21 Goldfarb D, Sataloft RT. Lymo disease: A review for tbeotolaryngologist. Ear Nose Throat J1994;73i824-829.
22. Negussie Y, Remick DG, DeForge LE, Kunkel SL, Eynon A,Griffin GE, Derection of plasma tumor necrosis factor, inter-leukins 6, and S during the Jarisch-Her>¡heimer Reaction ofrelapsing fever. J Exp Med 1992;]75:1207-1212.
23 Hurley JC. Anribiotic-mduced release of endotoxin: Areappraisal. Clin Infect Dis 1992;1S:84O-8.S4.
24. Georgilis K, Peacocke M, Klempner MS. Fibroblasts pro-tect rhe Lyme disease spirocbete, Borrelia ijurgdorferi,from ceftriaxone in vitto. J Infect Dis 1992;166:440-t44.
25. Klempner MS, Noring R, Roger RA. Invasion of humanskin fibroblasts by the Lyme disease spirocbete. BoneliabiAi-sdorf^n. J Infect Dis 1993;167ilO74-IOSl.
26. Bebar S. Porcelli SA. Mechanisms of autoimmune diseaseinduction. Artbritis Rheum i 995;3 8:458-476.
27 Steere AC, Dwyer E. Winchester R]. Association ofchronic Lyme arthritis with HLA-DR4 and HLA-DR2alíeles. NEiiglJ Med |99Ü;323:219-223.
28. Duray PH. Histoparhology of human borroliosis. In:Coyle PK (ed], Lyme Disease. Chicagot Mosby Yearbook,1992:49-58.
29. Kelsey JH. Lyme disease: An important consideration mthe differential diagnosis of TMD. ,] Mich Dent Assoc1990;72:209-210.
30. Fallón BA, Nields J. Lyme disease: A neuropsychiatrie ill-ness. Am J Psychiatry 1994;151:1571-1583.
31. Eppes SC, Klein JD. Caputo GM, Rose CD, Physicianbeliefs, attitudes, and approacbes toward Lyme disease inan endemic area. Clin Pediatr (Phila) 1994i33i 130-134.
Journal of Orofacial Pain 8 5

He ir/Fein
32. Lesniak OM, LirinaQ .W, Antiiifev VF. Heart disurders iLyme disease, Klin Mt-J [Mosk] 1 994;72;45^7,
33 Joksiinovic Z, Siiranuvic-Kuljic M, Lazartvie-Milanovic N,Jankovic-Nikolic A, Pavlovic-Nikolic S, Lyme carditis—Casereport, Glas Srp Akad Naiika [Med] 1993;43:237-239,
34, Woolf PK, A 12 year old with fever and rash, Pediatr O r e1994; I0T24 9-250,
35, Sieeie AC, Bacsfcird P, Weinberg M, Alexander J, BergerHJ, Wolfion S, Malawista SE. Lyme carditis: Cardinaljbnormaliries of Lyme disease. Ann Intern Med 1980;93:ÍÍ-1É,
36, Fung RP. McHugli GL, Leong JM. Sreere AC, Humoralimmune response to outer surface proreiti C of Borreliaburgdorfeii in Lyme diseaset Role of the lmmiinoglobulinM reîponse in the serodiagnosis of early infection, ItifectImmunol I994;62:3213-322I,
37, Sat; N, Immunologj' and diagnostic test }-e5u)ts in Lyme bor-rehosis, Schweiz Med Wochenschr 1992;122:]779-179J,
38, Dressier F, Whalcn JA, Reinhardt BN, Steere AC, "Westernblottmg in the serodiagnosii of Lyme disease. J Infect Dis1993;167:392-400.
39, Golightly MG, Laborite for the Diagnosis of LymeDisease, Stony Brook, NY: Stony Brook University Hos-pital, Decl994,Costello CM, Steere AC, Pinkerton RE, Eeder HM, Aprospective study of tick bites in an endemic area forLyme disease, J Infec Dis I989a59:136-I39,Rationale for antibiotic prophylaxis upon tick bite. LymeDisease Foundation Newsletter, Hartford, CT: LymeDiieaBc Foundation, 1994.
42. Massoraotti EM, Luget SW. Treatment of early Lyme dis-ease- Am I Med 1992;92:396-i03,
40.
41
50
51
43, Rahn DW, Malawista SE. Lymt disease: Recom-mendations for diagnosis and treatment. Ann Intern Med
45
46.
44, Wolf SR, Heininger U. Schneider W, Wen?-el D, Currentaspects in diagnosis and therapy of pédiatrie facial paraly-sis, HNO 1994;42:íi24-628.f-ish D, Environmental risk and prevention of Lyme dis-ease. Am J Med 1995;24:98:2S-8S,Rutz DA, Recommendations for Control of Ticks in NewYork State, Milbrook, NY: Cornell Cooperative Ex-tension, Farm and Home Center Inewsletrcr], Jiily 1990,
47, Chang YH, Appel MJ, Jacobson RH, Shin SJ, HarpendingP, ,Stiaubinger R, et al. Recombinant ObpA protects dogsagainst infection and disease caused by Botrelia hurgdor-feri. Infect Immun ] 995i63i3543-354S,
48, Telford SR HI, Kantor FS, Lobet Y, Barthold SW,Spielman A, Flavell RA, Fikrig E, Efficacy of human Lymedisease vaccine formulations in a mouse model- J InfectDis 1995;17I:136S-]37O,
49, Fikrig E, Telford SR ill, Wallich R, Chen M, Lohet Y,Matuschka FR, et al. Vaccination against Lyme diseasecaused by diverse Bondia biirgdorferi. ] Exp Med 1995j181:215-221,Marconi RT, Konkei ME, Garon CF, Variability of ospgenes and gene products among species of Lyme diseasespirochctes. Infect Immun 1993i61:2611-2617,Wilske B, Preac-Mursic V, Jauris S, Hofmann A, Pradel I,Soutschek E, et al, Inimunological and molecular poly-morphisms of OspC, an immunodominant major outersurface protein of Borrdia biirgdorferi. Infect Immun1993;61i2182-2191,
52, Barbour AG, Biological and social determinants of theLyme disease problem. Infect Agents Dis 1992;1:5O-S1,
Resumen Zusammenfassung
Enfermedad de Lyme: Consideraciones Odontológicas
Aunque la enfermedad de Lyme se ha expandido rápidamente yes difícil de diagnosticar, la revisión de la literatura odontológicano revela muchas referencias sobre esta enfermedad. Los prac-ticantes de odontología deben esíar al tanto de los efectossistémioos de este desorden que es a menudo mulíiorgánico.Sus manifestaciones clinícas pueden incluir dolor dental y facial.parálisis del nervio facial, cefalea, doior de la articulación tem-poromandibular, y dolor muscular masticatono. Los efectos queson precipitados c jan do se realizan procedimientos dentales enun paciente con enfermedad de Lyme, también deben ser con-siderados. Este estudio discute la epidemiología y diagnósticode la enfermedad de Lyme, su prevención, y factores para con,siderar cuando se hace un diagnóstico diferencial. También seconsiderarán el cuidado dental del paciente con enfermedad deLyme y los tratamientos disponibles actualmente. Se presentantres casos.
Lyme-Atthritis: Überlegungen für die Zahnmedizin
Obwohi sich die Lyme-Arthritis sdinall verbreitet hat undschwierig zu diagnostizieren ist, sind in der zahnarztlichenLiteratur nur wenige Hinweise auf diese Erkrankung zu finden.Zahnärzte soliten die mogiichen kiinischen Manifestationen ken-nen: Gesichtsschmerzen, Zahnschmerzen. Fazialisparese.Kopfschmerzen, Kiefergelenk- und Kaumuskelschmerzen. Esmüssen auch mögliche Auswirkungen von zahnärztlicherTätigkeit bei solchen Patienten erwogen werden. Diese Studiediskutiert die Epidemiologie und Diagnose der Lyme-Arthritis.ihre Prävention und Faktoren, welche bei der Differential-diagnose ÎU berucksichtigeri sind. Die zahnärztliche Betreuungdieser Patienten, sowie momentan mögliche Behandlungen wer-den auch besprochen. Es werden drei Fallbeispiele geschildert.
86 Volume 10, Number 1, 1996