Embed Size (px)
Citation preview

Curtis K. Argo, MD
Liver Transplantation Evaluation:
Essential Work-UpEssential Work Up
Curtis K. Argo, MD, MS
VGS/ACG Regional Postgraduate Course
Williamsburg, VA
September 13, 2015
Objectives• Discuss determining readiness for
transplantation – when is the right time to refer for transplantation evaluation?
• Describe the key aspects of liver transplantation medical evaluation
ACG/VGS/ODSGNA Regional Postgraduate Course - Williamsburg Copyright 2015 American College of Gastroenterology
1

Curtis K. Argo, MD
Transplantation Readiness
–Confirm cirrhosis• Clinical diagnosis
– Imaging (nodular liver and/or splenomegaly + presence of varices on EGD or varices/ascites on imaging + thrombocytopenia
Bi• Biopsy-proven– Nice but often not necessary unless mixed
signals
Transplantation Readiness
• Likely to survive without a transplant?– Child’s class/CTP score
CTP class: A = 5-6, B = 7-9, C = 10-15
ACG/VGS/ODSGNA Regional Postgraduate Course - Williamsburg Copyright 2015 American College of Gastroenterology
2

Curtis K. Argo, MD
Transplantation Readiness• Likely to survive without a transplant?
No: Child’s class C = CTP > 10–No: Child s class C = CTP > 10–30-35% mortality in 1 year
–Probably: Child’s class B = CTP 7-9–20% mortality in 5 years
Y Child’ l A CTP 5 6–Yes: Child’s class A = CTP 5-6–90% survival for ≥ 5 years
Transplantation Readiness• Likely to survive without a transplant?
MELD score– MELD score
Wiesner R et al. Gastroenterology 2003.
ACG/VGS/ODSGNA Regional Postgraduate Course - Williamsburg Copyright 2015 American College of Gastroenterology
3

Curtis K. Argo, MD
Transplantation Readiness• Likely to survive long-term without a
transplant?transplant?
–No: MELD > 20– >10% mortality in 3 months
–Unlikely: MELD = 15-195 10% mortality in 3 months–5-10% mortality in 3 months
–Possibly: MELD = 10-12–<5% mortality in 3 months
–Yes: MELD < 10
Transplantation Readiness• Likely to survive without a transplant?
MELD score vs CTP score– MELD score vs. CTP score
MELD appears to bemore sensitive than CTPo e se s t e t a Cin predicting mortality
Wiesner R et al. Gastroenterology 2003.
ACG/VGS/ODSGNA Regional Postgraduate Course - Williamsburg Copyright 2015 American College of Gastroenterology
4

Curtis K. Argo, MD
Transplantation Readiness• Likely to survive without a transplant?
Presence of portal hypertensive– Presence of portal hypertensive complications
• Variceal bleeding
• Ascites without good control
• Hepatic encephalopathy requiring ED/admission
• Spontaneous bacterial peritonitis• Spontaneous bacterial peritonitis – 50-60% 1 year survival
• Hepatorenal syndrome– Median survival = 2 weeks
Andreu M et al. Gastroenterology 1993.
Transplantation Readiness• Better off with a transplant?
1 year survival
Merion RM et al AJT 2005.
ACG/VGS/ODSGNA Regional Postgraduate Course - Williamsburg Copyright 2015 American College of Gastroenterology
5

Curtis K. Argo, MD
Transplantation Readiness• Better off with a transplant?
Transplant benefit appears to occur
Schaubel DE et al AJT 2006
Transplant benefit appears to occuron a 5-year time horizon at MELDof 10
Transplantation Readiness• Appropriate time to refer for transplant
evaluation?evaluation? – MELD score ≥ 15
• Waiting time still a factor with MELD < 20
– CTP ≥ 8
– Life-threatening portal HTN complicationLife threatening portal HTN complication
– Hepatocellular carcinoma
– MELD exception to 22 points in selected cases that meet Milan criteria
AASLD guideline 2005
ACG/VGS/ODSGNA Regional Postgraduate Course - Williamsburg Copyright 2015 American College of Gastroenterology
6

Curtis K. Argo, MD
Transplantation Evaluation• Basic but Important Questions
– Can the patient survive the operation and the p pimmediate postoperative period?
• Nutrition ● Comorbidities
• Functional status ● Age
– Can the patient be expected to comply with the complex post-transplant medical regimen?p p p g
• Past behavior predicts future behavior
• Addiction
– Does the patient have other comorbidities that could severely compromise graft function or patient survival – futile? AASLD guideline 2005
Transplantation Evaluation• Age
– No specific age limitationp g• Patients age >70 have had reduced long-term post-
transplant survival, mainly due to death from malignancies or perioperative complications
• Coronary Artery Disease– RFs: smoker, age>50, DM, personal or FmHx, g , , p
– Increased perioperative mortality in CAD pts
– Stress echo is best studied, but there is no consensus on best risk stratifying test
– Catheterization is indicated in any positive test
ACG/VGS/ODSGNA Regional Postgraduate Course - Williamsburg Copyright 2015 American College of Gastroenterology
7

Curtis K. Argo, MD
Transplantation Evaluation• High risk features for transplant in
NASH/cryptogenic cirrhosisyp g– ≥ 60 years old
– BMI ≥ 30
– Pre-transplant Diabetes +
– Pre-transplant HTN +
Dil 0% 1 li i k i l• Dilemma: 50% 1-year mortality risk in largest retrospective cohort of transplanted NASH cirrhosis pts (n=98) in patients with all 4 of these risk factors (n=18)
Malik SM et al, AJT 2009
Transplantation Evaluation• Substance abuse/addiction – Use vs. Abuse
– Abuse: demonstration of dependence through ti d b t d it ti ff tcontinued substance use despite negative effects
on health, family, job, or legal status
– Use: intermittent use of substance that does not have the above negative ramifications and is remediable with relatively conservative measures
UVA’ li• UVA’s policy– We do not condone use of any illegal, illicit drug in
any transplant candidate
– Alcoholic abstinence of at least 6 consecutive months is required prior to listing for liver transplant
ACG/VGS/ODSGNA Regional Postgraduate Course - Williamsburg Copyright 2015 American College of Gastroenterology
8

Curtis K. Argo, MD
Transplantation Evaluation• Obesity• BMI > 40 is strongly
associated with reducedassociated with reduced 30-day, 1-yr, and 2-yr post-transplant survival
• BMI > 35 is associated with reduced 5-yr survival
• Our cutoff for transplant listing at UVA is BMI ≤ 40listing at UVA is BMI ≤ 40
• Underweight• BMI < 18 is strongly
associated with poor post-transplant outcome
Nair S, et al, Hepatology 2002
Transplantation Evaluation• Extrahepatic Malignancies
– High risk for recurrent disease due to gimmunosuppression
– A waiting period is standard after cure/remission of a malignancy
• Waiting period varies by the type, grade, and extent of the extrahepatic malignancy
– UVA utilizes a cancer consultation service (Israel Penn) to aid in determining appropriate waiting period and risk of recurrence
ACG/VGS/ODSGNA Regional Postgraduate Course - Williamsburg Copyright 2015 American College of Gastroenterology
9

Curtis K. Argo, MD
Transplantation Evaluation• HIV infection
– HIV is a chronic infection thanks to HAART
– Patients can undergo transplant if they have HIV • Control of infection with present HAART is required
with undetectable HIV viral load
• CD4 count > 250
• HCV and renal failure is a relative contraindication
– Significant drug interactions between calcineurin inhibitors (tacrolimus, cyclosporine) and certain protease inhibitors (use integrase inhibitors?)
Transplantation Evaluation• Hepatopulmonary Syndrome (HPS)
– Chronic liver disease, hypoxemia, widespread i l dil iintrapulmonary vasodilation
• Not pathophysiologically compatible to have both HPS and pulmonary HTN (vasoconstriction)
• More likely hypoxemia with pulmonary HTN is portopulmonary HTN
– Workup– Workup• ABG for pO2 – higher MELD if pO2< 60
• Transthoracic echocardiogram with bubble study– Exclude intracardiac shunting and confirm pulm shunting
• Macroaggregated albumin scan to quantify intrapulmonary shunting if pO2 and echo fit
ACG/VGS/ODSGNA Regional Postgraduate Course - Williamsburg Copyright 2015 American College of Gastroenterology
10

Curtis K. Argo, MD
Transplantation Evaluation• Portopulmonary HTN
– Idiopathic pulmonary HTN in cirrhotic patient with p p y pno history of underlying lung disease
– Mild and moderate pulmonary HTN not contraindication to transplantation and pulm HTN usually resolves in 4-6 months
– Severe pulmonary HTN = mean PA pressure ≥ Se e e pu o a y ea p essu e35 mm Hg
• Contraindication to transplantation due to possibility of poor graft function related to passive congestion
• May use vasodilator medications to correct to under this limit
Transplantation Evaluation• Vascular anatomy
– MR angiogram is our study of choice although CT g g y gangiogram can be adequate with careful contrast protocol
– Require suitable portal inflow and hepatic arterial and venous anatomy
– Portal vein thrombosis is not a contraindicationo a e o bos s s o a co a d ca o
– Portal system atrophy/complete occlusion is a CI
• Imaging also helpful in assessing liver volume– General rule: liver mass to be transplanted should
be 1-2% of total body mass of recipient
ACG/VGS/ODSGNA Regional Postgraduate Course - Williamsburg Copyright 2015 American College of Gastroenterology
11

Curtis K. Argo, MD
Transplantation Evaluation
• Hepatocellular carcinoma (HCC or hepatoma)T l t ti i ti i l t d did t– Transplantation is curative in selected candidates
• Can consider resection but need to be free of portal HTN
– IR or Rad Onc supplies valuable services in preventing patients from progressing outside of criteria as well as downstaging to meet criteria
TACE RFA XRT Y 90 i h• TACE, RFA, XRT, Y-90 microspheres
– Sorafenib’s role pre- and post-transplant is unclear
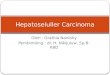
AASLD Guidelines for HCC Diagnosis
2< 1 cm 1 -2 cm > 2cm
If characteristic on 2 dynamic images –arterial enhancement + washout
If characteristic on 1 dynamic imaging
or
Low likelihood of HCCUS q 3 months
No growth in 1 2 yrs enhancement washout(CT, MRI, contrast Enhanced US)
Treat as HCC
If not typical onimaging, biopsy
lesion
AFP > 200 ng/mLTreat as HCC
If not typical onimaging, biopsy
lesion
Bruix J et al. Hepatology 2005;42:1208-1236
No growth in 1-2 yrsResume q 6 month US
False negative30%
ACG/VGS/ODSGNA Regional Postgraduate Course - Williamsburg Copyright 2015 American College of Gastroenterology
12

Curtis K. Argo, MD
Milan Criteria
– No evidence of extrahepatic spread
1 lesion < 5 cm
– Based on pre-transplant imaging
– 4 year survival - 74%
– Recurrence rate -<10%3 lesions, none > 3 cm
– Validated in several studies with > 1000 patients
• 5 yr survival >70%• Recurrence < 15%
Mazzoferro et al N Engl J Med 1996;334(11):693-9
Transplantation Evaluation• Acute liver failure (ALF)
– If the patient is a viable liver transplant candidate from psychosocial perspective, then tertiary referral is recommended for critical care management and urgent evaluation
• Remember King’s criteria in acetaminophen overdose– pH< 7.3, INR > 6.5, Creatinine > 3.4, grade III/IV encephalopathy
• Low phosphorous is good prognostic sign• Low phosphorous is good prognostic sign
• Utilize N-acetylcysteine IV in both acetaminophen and non-acetaminophen ALF
• Aggressively treat encephalopathy and renal failure but there is no role for correcting coagulopathy unless acute bleeding occurring
ACG/VGS/ODSGNA Regional Postgraduate Course - Williamsburg Copyright 2015 American College of Gastroenterology
13

Curtis K. Argo, MD
Thanks for your attention!Curtis Argo, MD, [email protected]
ACG/VGS/ODSGNA Regional Postgraduate Course - Williamsburg Copyright 2015 American College of Gastroenterology
14