Embed Size (px)
Citation preview

Guillain-Barre Syndrome (GBS)
Iman binti Jeffrey0611750

Outline
DefinitionEpidemiologyEtiologyPathogenesis & PathologyClinical featuresInvestigationsDiagnosis Differential diagnosisTreatmentPrognosis

Definition
Postinfectious polyneuropathy involving mainly motor but sometimes also sensory and autonomic nerves
Affects people of all ages and is not hereditary Most patients have a demyelinating neuropathy, but primarily axonal degeneration is documented in some cases. also known as: Acute inflammatory demyelinating polyneuropathy (AIDP)

Epidemiology
usually in children over 4-9 yearsoverall frequency is 1.9 cases per 100,000 populationfollows infection or immunization by 10 daysfollows respiratory tract infection or gastrointestinal infection

Etiology
GIT infectionCampylobacter jejuni (26-41%)Cytomegalovirus (10-22%)Respiratory tract infectionMycoplasma pneumoniae Ebstein-Barr virus (10%)Vaccines Rabies Avian-flu influenza


Pathogenesis
Molecular mimicryCross-reactive immune attack by host Ab & T cell with are directed against the pathogen & nerve components.
Eg: Campylobacter jejuniImmune response directed against capsular LPS producing Ab cross-reacting with myelin to cause demyelination (mimics the gangliosides)

Pathogenesis
Presentation of Ag to naïve T cell → activation↓
Activated T cells attach to venular endothelium of peripheral nerves
↓Migrate through endothelial lining to
perivascular location ↓
Sensitized → contact myelin → segmental demyelination

Pathology
Inflammatory lesions scattered throughout the peripheral nervous systemCircumscribed areas of myelin loss associated with presence of lymphocytes and macrophagesInitial lesion: nodes of RanvierMyelin damage: penetration of macrophages into basement membrane around nerve fibers & strip myelin awaySevere cases: interruption of axon & wallerian degeneration


Clinical Features
Weakness o Onset is gradual and progresses over weekso Lower extremities (unable/refusal to walk) trunks upper limbs
bulbar muscles flaccid tetraplegia = Landry Ascending Paralysiso Proximal and distal muscles are involved relatively symmetrically, but
asymmetry is found in 9% of patient
Muscle tenderness – At the onset
Paraesthesias – in some cases
Areflexia (83%)

Clinical Features
Bulbar involvement (50%)o Dysphagia and facial weakness – signs of impending respiratory failureo Interfere with eating. Increase risk of aspiration
Cranial nerve involvement (50%)o Facial nerve o Oculomotor nerve
Autonomic involvemento Lability of blood pressureo Postural hypotensiono Profound bradycardiao Occasional asystoleo Urinary o retention or incontinence (20% of cases, usually transient)

Clinical Features
Symptoms of viral meningitis / meningoencephalitis
o In young children
CNS involvemento ataxiao papilledema
Miller-Fisher syndromeo External ophtalmoplegiao ataxiao areflexia

Table 1:Clinical features in 49 children with GBS*
Features Prevalence
Age 7.1years (mean)
Male/female ratio 1.2:1
Weakness 73%
Pain 55%
Ataxia 44%
Paraesthesias 18%
Shortness of breath
4%
* Data from unpublished observation of John Sladky. Two patients had consistent findings of Fisher syndrome

Course
Initial phase Gradually increasing involvement lasts 10-30 days
(less than 4 weeks)
Plateau phase Short phase (within 2 weeks) Long plateau phase → poor prognosis
Recovery phase Within months Usually complete Motor sequelae (5-25%) Relapse & late recurrences (3%)

Investigations
Lumbar puncture – cerebrospinal fluid (CSF)o Elevation of CSF protein (more than twice upper limit of
normal)o Cell content of CSF is normal (<10 cells/mm³)o Glucose level normalo Bacterial and viral culture is negative
Electromyographyo Motor nerve conduction velocities are greatly reduced,
and sensory nerve conduction time is often slow o evidence of acute denervation of muscle
Serum Creatine Kinaseo Elevated or normal

Muscle biopsyo appear normal in early stages o show evidence of denervation atrophy in chronic stages
Sural nerve biopsy o segmental demyelination, focal inflammation, and
wallerian degeneration
Serologic testing for Campylobacter infection

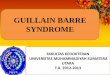
This is a high-power image of an nerve stained with the standard H&E. The GBS is fairly acute, and the nerve contains significant inflammation. The majority of the small round nuclei are those of lymphocytes infiltrating the nerve. Some residual myelinated axons can be seen. The denser pink lines (black arrow) are the axons and the bubbly-appearing pink areas surrounding them are myelin sheaths

This is a mid-power image of a nerve which has been stained with a different myelin stain, which stains the myelin blue. There is patchy myelin loss within the nerve. You an also see some small round lymphocyte nuclei.

Subdivision of GBSSubdivision Clinical manifestation
Sporadic GBS (AIDP)
As mentioned
Acute motor-sensory axonal neuropathy(AMSAN)
Relatively infrequentSevere degeneration of motor and sensory axonsLittle demyelinationFulminant, extensive and severe weakness with delayed and incomplete recovery
Acute motor-axonal neuropathy(AMAN)
Severe pure motor axonal neuropathy Clinical course and recovery is similar to AIDP
Miller-Fisher syndrome
Triad: ophthalmoplegia, ataxia, & areflexia
Chronic IDP(CIDP)
Neurologic symptoms are slower (>4 weeks)

Diagnosis
Required for diagnosis
Progressive motor weakness involving >1 extremitiesAreflexia or marked hyporeflexiaNo more than 50 monocytes or 2 granulocytes per µL CSF
Supportive
Initial absence of feverProgression over days to few weeksOnset of recovery 2-4 weeks after cessation of progressRelatively symmetric weaknessMild sensory signs & symptomsCranial nerve signsElevation of CSF protein after 1 week of symptomSlowed nerve conduction velocityAutonomic dysfunction
From National Institute of Neurologic and Communicative Disorders and Stroke

Differential Diagnosis
Spinal cord compression Transverse myelitis Tick paralysis Poliomyelitis Botulism Diphtheria

Treatment
Patients with early stages of this acute diseaseShould be admitted to the hospital for observation because the ascending paralysis may rapidly involve respiratory muscles during the next 24 hour.
Patients with slow progression:may simply be observed for stabilization and spontaneous remission without treatment.
Patients with rapidly progressive ascending paralysis:o Intravenous immunoglobulin (IVIG), administered for 2, 3, or 5 dayso Plasmapheresis, steroids, and/or immunosuppressive drugs are
alternatives, if IVIG is ineffective o Combined administration of immunoglobulin and interferon is effective
in some patients.
Supportive care, such as respiratory support, prevention of decubiti in children with flaccid tetraplegia, and treatment of secondary bacterial infections, is important

Prognosis
Spontaneous recovery begins within 2–3 weeks.Most regain normal muscular functionTendon reflexes are usually the last function to recover Improvement usually follows a gradient inverse to the direction of involvement.Bulbar and respiratory muscle involvement may lead to death if the syndrome is not recognized and treated 3 clinical features predictive to poor outcome: Cranial nerve involvement Intubation Maximum disability at the time of presentation

References
Menkes & Sarnat: Child Neurology, 6th ed. USA, Lippincott Williams & Wilkins, 2000
Aicardi, Jean: Clinics in Developmental Medicine: Diseases of The Nervous System in Childhood, 2nd ed. London, Mac Keith Press, 1998
Behrman, Kliegman, Jenson: Nelson Textbook of Pediatrics, 17th ed. China, Elsevier Saunders, 2004