Embed Size (px)
Citation preview

6-year-old boy with a swollen kneeBy J. Muse Davis, MD & Sheryl Henderson, MD, PhD
Educational Objectives After reading this article and answering the review questions, the reader will be able to:
1. Recognize common clinical presentations of Lyme disease in children
2. State when laboratory testing is indicated, which tests apply to the particular case, and how to interpret the results
3. Articulate the appropriate treatment regimens for children and adolescentswithdifferentpresentationsofLymedisease
Case A 6-year old boy presents to an urgent care clinic in northern Wisconsin in late December with a swollen, painful right knee. Theswellingstartedfivedaysagoandseemstobegettingbigger. There is no history of recent trauma to the site and he has never had joint complaints before. Physical examination shows a healthy, well-developed boy with a warm, tender swollenknee.Thepatellaismobileandagenerouseffusionisdetectable beneath. There is no erythema of the skin and the rest of his exam is unremarkable. X ray of the knee shows no bonyabnormalities.Theeffusionistappedandhas~21,000leukocytes/ml3, with a predominance of granulocytes.
The patient lives with his parents in Georgia and is visiting family in Wisconsin for the winter holidays. He had previously visited the North Woods of Wisconsin in early August for a family camping vacation.Duringthefirstweekofschoolhedevelopedfeverandmalaisewithbodyaches.Hehadafivedayhistoryofacuriouscircular rash noted on his chest which started as a small red
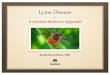
“spot”thatexpandedoverthecourseoffivedays,developingacentralclearing.Itwasflatandred,butnotpainfuloritchy.Hismother brings a picture of the rash (Figure 1). He was treated supportively, and his symptoms resolved within a week.
Lyme disease is rarely found in Georgia, however, his travel to an endemic area and febrile illness with a characteristic rash shortly after his summer visit to Wisconsin raises suspicion for Lyme arthritis. There is no recollection of a tick bite on the patient or his familymembers.ALymeEIA(EnzymeImmunoassay)withreflexWestern blot IgG was sent from his serum, and the knee joint fluidissentforcultureandnucleicacidtesting(PCR)forBorrelia burgdorferi.Heisempiricallyprescribedamoxicillinat50mg/kg/day dividedin3doses/dayfor28days.Thejointfluidbacterialculture and the PCR are negative but the total serum antibody is3.0LIV(positiveisover1.2).Giventhisresult,aserumIgGimmunoblotisperformed,whichispositivefor7ofthe10diagnostic bands. His knee swelling begins to improve within a week of starting treatment.
Diagnosis: Lyme Arthritis—Late Lyme Disease
S U M M E R 2 0 1 4
PathwaysPediatric
A M E R I C A N FA M I LY C H I L D R E N ’ S H O S P I TA L P U B L I C AT I O N F O R P H Y S I C I A N S M A D I S O N , W I S C O N S I N
CME ARTICLE 1: SEE PAGE 7 FOR CME INFORMATION
– continued on page 2
Rash on chest of 6-year-old boy

2
CONTINUED FROM PAGE 1
Introduction Lyme disease is caused by Borrelia burgdorferi, a spirochete transmitted by tick bites from Ixodes tick species. Wisconsin is one of the endemic areas for Lyme disease in the United States. The disease’s myriad presentations are categorized based on the site and timing of appearance after the tick bite (early localized, early disseminated or late disease). The classic and most common presentation of early Lyme disease is erythema migrans (EM), a unique circular rash as seen in this case. A very common presentation of late Lyme disease is arthritis of large joints, most commonly the knee. The arthritis can be monoarticular or oligoarticular. While early Lyme disease with its characteristic rash can often be diagnosed based on history and physical exam alone,lateLymediseasecanbeadifficultdiagnosis.Herewewilloutlinethelifecycleof B. burgdorferi, discuss the major manifestations of early and late Lyme disease, and review the current recommendations for treatment. We will also review the laboratory investigations of Lyme disease and their proper interpretations.
Background Lymediseasewasfirstrecognizedin1975afteranepidemiologicstudyofchildrenin Lyme, Connecticut. Due to its distinct geographic and seasonal characteristics, Lymewasthoughtmostlikelytobeassociatedwithanarthropodvector.In1982,thecausativeagentwasidentifiedasBorrelia burgdorferi, a Treponema-like bacterium discovered in the gastrointestinal tract of Ixodes scapularis (also known as the blacklegged or deer tick). This tick is limited geographically to the coastal northeastandthenorthernMidwest.In2012,Wisconsinwasoneof13USstatestoreportLymedisease.Lymeisourmostcommontickbornediseasewith>23,000documentedcasesinWisconsinfrom1980to2010.Themajorityofcasesoccurduring the summer months when the deer tick is feeding. Practitioners should also be aware that in Wisconsin Ixodes scapularis hosts other human pathogens such as Babesia, Anaplasma phagocytophilum, Ehrlichia sp. and the Powassan virus. It is not uncommon for co-infections to occur.
B. burgdorferi relies on vertebrate (non-human) reservoir hosts as its primary home. In Wisconsin the most common reservoir is the white footed mouse. Reservoir hosts can tolerate relatively high numbers of bacteria without developing symptoms. The tick larva acquires B. burgdorferi by feeding on a reservoir host. It subsequently develops into a nymph. The nymph or adult tick is capable of transmitting B. burgdorferi to humans.
To complete this article, read more about Lyme Disease, and receive CME credit, please go to uwhealth.org/pediatricpathways
J. Muse Davis, MD is a Pediatric Infectious Disease fellow and Sheryl Henderson, MD, PhD is board certified in Pediatric Infectious Disease and an Assistant Professor in the Department of Pediatrics at the University of Wisconsin School of Medicine and Public Health.
Dear Colleagues,
In this issue of Pediatric Pathways,weofferCME articles highlighting a variety of pediatric topics that you may encounterinyourofficethis summer. Our authors give an overview of each topic in a case-based format and provide recommendations regarding relevant evaluation, treatment resources, and referral information online. To access the full articles and receive CME credit, please go to uwhealthkids.org/pediatricpathways
Please contact me at [email protected] if you have any feedback on this publication or suggestions for future topics.
Sincerely,
Michelle Kelly, MD
Michelle Kelly, MD is a Pediatric Hospitalist and Assistant Professor of Pediatrics at the University of Wisconsin School of Medicine and Public Health.
Pediatric Pathways Editorial Staff
Medical Editor: Michelle Kelly, MD
CME Director: Barb Anderson
Editors: Ellen Wald, MD Kristin Knackers, MD
Marketing & Public AffairsEditor: MichaelFelber
Online Editor: Chad Hanson
A Letter from the Medical Editor
Sheryl Henderson, MD, PhD
J. Muse Davis, MD
2
To make a referral to the Pediatric Infectious Disease clinic,call(608)263-0943.

3
CONTINUED FROM PAGE 1
3
Pediatric Office EmergenciesBy Christine Zimmerman, MD
Educational Objectives After reading this article and answering the review questions, the reader will be able to:
1. Identify the most common pediatric emergencies seen in the outpatient setting
2. List the supplies necessary for common pediatric emergencies in this setting
3. Recognize the importance of written emergency protocols and regular mock codes in clinics
4. Identifytheadditionalstepsnecessaryforemergency preparedness for children with special needs
Case You are working in your clinic one sunny summer afternoon when a 2-year-old girl, Madelyn, is brought in by her mother. Madelyn was playing at the park and stung by a bee and experienced an abrupt onset of hives. The mother tells the receptionist that en routetotheoffice,thegirlalsodevelopedswellingofherlipsandface. She vomited once, and her breathing is somewhat labored.
Thereceptionistnotifiesthenurseofthegirl’sconditionandescortsthechildandhermothertotheofficeprocedureroom. The nurse recognizes that the child is experiencing an anaphylactic reaction,instructsthereceptionisttocall911immediately,andthen retrieves you from another patient’s room for help.
When you arrive, you see a toddler who is clearly distressed. She iscoveredinhives,hassignificantangioedemaofthelips,andis tachypneic with wheezing and deep retractions. The nurse goesinsearchofapulseoximeterwhileyouscrambletofindan appropriately sized face mask and an oxygen canister. The medical assistant informs you that her vital signs are as follows: pulse130,respiratoryrate55,temperature99.0,bloodpressure85/62. Once the pulse oximeter is obtained, the oxygen saturation is noted to be 81% on room air. You place the child on oxygen andadminister1:1000epinephrineIM.Youalsoorderanalbuterolnebulizer treatment and a dose of IM benadryl, and ask the nurse toplaceanIV.Atthispoint,thepatientisstartingtolookbetter,andheroxygensaturationhasincreasedto92%.EMSarrivesand you provide a brief summary of the patient’s course while in theoffice,includingtheinterventionsperformedandvitalsigns.The receptionist provides the EMS team with a printed patient summary from the patient’s electronic medical record, and the patient is transported to the nearest hospital.
Ifthischildhadbeenbroughttoyouroffice,wouldshehavereceived the prompt medical attention she needed? Would the
staffhavenotedherillappearanceandnotifiedyouimmediately?Wouldyourofficehavehadthenecessaryemergencymedications and equipment organized, up-to-date, and readily available? Would there have been a written protocol for pediatric anaphylaxis on-hand?
Overview Children requiring urgent or emergent treatment often initially presenttotheirprimarycarephysician.Accordingtothe2012Periodic Survey #27 from the American Academy of Pediatrics (AAP), pediatricians see an average of about 2 patients per week who require emergency treatment.
To complete this article, read more about preparing for office emergencies, and receive CME credit, please go to uwhealth.org/pediatricpathways
ChristineZimmerman,MDisboardcertifiedin Pediatrics and Adolescent Medicine and an Assistant Professor in the Department of Pediatrics at the University of Wisconsin School of Medicine and Public Health.
Christine Zimmerman, MD
CME ARTICLE 2: SEE PAGE 7 FOR CME INFORMATION
To make an appointment with Dr. Zimmerman, call (608)263-3301.

4
Educational Objectives After reading this article and answering the review questions, the reader will be able to:
1. State the risk factors for unsafe sleep in infants
2. Describe best practice recommendations for infant safe sleep
3. Describe strategies to promote a safe sleep environment for infants in the home
Case A 25-year-old African American woman comes into yourofficewithher3-month-oldmaleinfantforawell-child check. She is a single mother with three other children and works thirty hours a week. She had herfirstchildwhenshewas16andher3-month-oldwas born preterm with low birth weight. The mother has tried several times to quit smoking but has been unsuccessful. While she is at work the grandmother takes care of the infant and a couple of other children in her home.
When asking the mother about the sleeping arrangements for her infant, she tells you that she was given a used, older crib and blankets, bumper pads and sheets from a friend. She notes that she places the infant on its back to sleep. The crib is set up in a room across the hall with two younger siblings. The infant wakes up frequently to eat during the night. The mother tells you that she lies down with baby in her bed to breastfeed and is usually too tired to return the infant to his crib.
Overview of infant sleep-related deaths Sudden unexpected infant death (SUID) is the death of a previously healthy infant without an immediately obvious cause prior to investigation. After case investigation, SUIDs can be attributedtosuffocation,asphyxia,entrapment,infection,ingestions, metabolic diseases, cardiac arrhythmias, and trauma (accidental or nonaccidental). These deaths may be further categorized as: 1) SIDS (sudden infant death syndrome), sudden death of an infant younger than 1 year of age that cannot be explained even after a full investigation that includes a complete autopsy, examination of the death scene, and review of the clinicalhistory;2)ASSB(accidentalsuffocationandstrangulationinbed);or3)otherunspecifiedcauses.OnetypeofSUID,ASSBis a cause-of-death code used for vital statistics purposes. This codeisusedtoidentifyinfantdeathscausedbysuffocationorasphyxia in a sleeping environment, for example:
• Suffocationbysoftbedding:Whensoftbedding,apillow,ora waterbed mattress blocks the infant’s airway.
• Overlay: When another person shares the sleep surface with the infant and lays on or rolls on top of or against the infant while sleeping, blocking the infant’s airway.
• Wedging or entrapment: When an infant gets trapped between two objects, such as a mattress and wall, bed frame, or furniture, blocking the infant’s airway.
• Strangulation: When something presses on or wraps around the infant’s head and neck blocking the airway.
TheinfantmortalityrateintheUnitedStatesfor2010was6.15infantdeathsper1,000livebirths.Suddeninfantdeathsyndrome (SIDS) is the 3rd leading cause of infant death for 2010andtheleadingcauseofdeathamonginfantsages1to12months.In2010,therewereatotalof3,610or0.9SUIDsper1,000livebirths,accountingfor15%ofallinfantdeaths.Ofthesedeaths,2,063wereattributedtoSIDS(ICD-10codeR95);918attributedtounknowncause(ICD-10codeR99),and629attributedtoaccidentalsuffocationandstrangulationinbed(ASSB,ICS-10codeW75).
Therehasbeenavastshiftintheclassificationofsuddeninfantdeath that has taken place in the United States over the last 15 years.Since1998,accordingtotheCentersforDiseaseControl
Safe to SleepBy Nan Peterson, RN, MS & Kristin Shadman, MD
CME ARTICLE 3: SEE PAGE 7 FOR CME INFORMATION
– continued on page 5

55
and Prevention (CDC), it appears that medical examiners and coroners are moving away from classifying deaths as SIDSandcallingmoredeathsaccidentalsuffocationorunknown cause. In addition, practices in investigation and cause-of-death determination are inconsistent, thus limiting the ability to monitor national and state trends, ascertain risk factors, and design and evaluate programs to prevent these deaths. CDC’s SUID Initiative is aimed at improving the investigation and reporting practices of SIDS and SUID.
TheSIDSrateremainssignificantlyhigheramongcertainracial and ethnic groups, including non-Hispanic Blacks andAmericanIndian/AlaskaNatives.In2009,theinfantmortalityratefornon-Hispanicblackwomenwas12.40infantdeathsper1,000livebirths,2.8timesgreaterthanthelowestrateof4.40forinfantsofAsianorPacificIslander mothers. Rates were also higher for infants of AmericanIndianorAlaskaNative(8.47)andPuertoRican(7.18) mothers.
A CDC and Wisconsin Department of Health Services sponsored survey (PRAMS) of mothers in Wisconsin reported that:
• 1 out of 5 infants are not put on their back to sleep (1 out of 3 for Black infants)
• Over 1/3 of mothers frequently bed share with their infant (over ½ for Black/Hispanic)
• Only 52% of infants consistently sleep on their backs and in their own sleep space.
To complete this article, read more about the AAP safe sleep recommendation, talking with parents about sleep, and receive CME credit, please go to uwhealth.org/pediatricpathways
Nan Peterson, RN, MS is the program director for Child Health Advocacy at the American Family Children’s Hospital.
Kristin Shadman, MD is a Pediatric Hospitalist board certified in Pediatrics and Adolescent Medicine and an Assistant Professor in the Department of Pediatrics at the University of Wisconsin School of Medicine and Public Health.
New clinic helps with diagnostic dilemmas
A new Pediatric Diagnostic and Consultation clinic at UW Health’s American Family Children’s Hospital, directed by Jonathan Fliegel, MD, provides evaluations for children of all ages with challenging diagnostic and/or management problems.
“Our goal is to work with the primary care provider and UW
Healthpediatricsubspecialiststofindthebestpathfordiagnosis and treatment for children whose symptoms remain puzzling. We see patients whose symptoms do not fall clearly within the scope of another pediatric specialty or when families and their clinicians request a second opinion to have a ‘new set of eyes’ look over a child’s situation,” says Dr. Fliegel, who also is a member of the Division of Hospital Medicine at American Family Children’s Hospital. “In most cases, we expect that only one visit to our clinic will besufficientbeforeanactionplancanbeidentified.”
Common reasons to consider a referral include complex symptoms, such as: poor weight gain or growth, unexplained fevers, persisting pain, fatigue or other problems.
Referring pediatricians or family physicians are asked to provide records of visits, labs and studies before a child is seen in the DiagnosticandConsultationClinic.Afterthefirstappointment,Dr. Fliegel works collaboratively with each patient and family, the child’s regular physician and, when needed, other pediatric specialists at the American Family Children’s Hospital to plan further steps in diagnosis and treatment.
Within several days of the consultation, the Diagnostic and Consultation Clinic will complete and send a full report to the referring physician. Most patients will not require follow-up visits and will be encouraged to work closely with their primary care physician for ongoing care. Dr. Fliegel may also suggest referrals for additional services or specialty evaluations, if necessary.Nan Peterson,
RN, MS
Kristin Shadman, MD
JonathanFliegel, MD
CONTINUED FROM PAGE 4
To refer a patient to the Diagnostic and Consultation Clinic, call the American Family Children’s Hospital’s PediatricSpecialtyClinicat(608)263-6420.PhysicianswithspecificquestionspriortoorafterareferralmaycontactDr.Fliegel’sofficedirectlyat(608)265-5545.

6
Formorethan20years,thePediatricSedation program at UW Health’s American Family Children’s Hospital has been helping alleviate both pain and fear by focusing on each child’s individual needs prior to each medical procedure.
Created by medical director Gregory Hollman, MD, a pediatric critical care physician,theprogramofferssedationsthat take into account the type of
procedure that will be performed, the age, developmental status, and personality type of the child. Thought is always given to how a procedure could be accomplished without medication, through the use of preparation and/or distraction techniques, or using oral medications and avoiding an intravenous line.
“Our Sedation Program has been incredibly well received by literally thousands of patients and families,” says Dr. Hollman. “Parents never want to see their child in distress and, thanks to this program, most children never even remember having the procedureinthefirstplace.”
Typical procedures for which children are sedated include:
• Non-painful procedures that require a child to hold still for a relatively long period of time, such as MRI and CT scans
• Painful procedures such as lumbar punctures, bone marrow aspirates and biopsies and dermatologic procedures
• Distressful procedures such as voiding cystourethrograms and urinary catheter placements
How do we decide if it is safe to sedate a child? We will review a child’s history and do a careful physical examination. We may reschedule the child’s sedation or refer them for general anesthesia if they are acutely ill or have a cardiorespiratory or other illness that places them at high risk for sedation. We may also choose to send a child through general anesthesia if they have a history of a medical condition that may compromise cardiorespiratory function, such as:
• Sleep apnea or central apnea
• Craniofacial abnormalities that distort the airway
• Poorly controlled seizures
• Severegastricrefluxdisease
• Increased intracranial pressure
Whattypesofsedationareoffered?Minimal: The child may stay awake but be more relaxed and less aware of the procedure.
Moderate: The child may be awake but very relaxed with little or no pain or may fall asleep but be easy to awaken.
Deep: The child will fall asleep, have little to no movement, and will not be easy to awaken.
Our Sedation Program does not use breathing tubes. Rather, our goal is to alleviate pain and fear but, at the same time, allow the child to breath spontaneously throughout the procedure.
Gregory Hollman, MD
Patient Emmalyn undergoing sedation
Pediatric Sedation Program reduces anxiety before procedures
To schedule a sedation appointment, call our clinic at(608)262-4402.

7
Upcoming ProgramsFind out more at cpdqi.pediatrics.wisc.edu or email [email protected] to request weekly updates to CME programs.
Pediatrics Grand Rounds EVERY THURSDAY FROM 7:30 A.M. TO 8:30 A.M.UW Health Sciences Learning CenterMadison, WisconsinWatch via live stream at http://live.videos.med.wisc.edu
SAVE THE DATE:
Adolescent Reproductive Health Care Services ConferenceAugust 1, 2014Madison, WIhttp://tinyurl.com/m5cyduv
PALS PlusSeptember 17-18, 2014UW Health Simulation Centerhttp://pals.pediatrics.wisc.edu
SeminarsinPediatrics2014September 18-19, 2014Monona Terrace Community and Convention Center, Madisonhttp://seminars.pediatrics.wisc.edu
Upper Midwest Clinical Genetics ConferenceSeptember 19, 2014Monona Terrace Community and Convention Center, Madison
SeminarsinPediatrics2015October 1-2, 2015Monona Terrace Community and Convention Center, Madison
Past issues of Pediatric Pathways are available at: uwhealth.org/pediatricpathways.
CME Information Release date: July 15, 2014 Expiration date: July 15, 2015
Method of ParticipationThe articles in this document are an introduction to a CME opportunity that is available online. To obtain CME credit, go to uwhealth.org/pediatricpathways, read the complete articles and submit your answers to the reviewquestions.A scoreof80%correctorbetterwill allowyouto claim your credit. Credit letters will be automatically generated if you receive a passing score. Please send an email to [email protected]. Estimatedtimetocompletetheactivity:1.0Hour.
Accreditation StatementThe University of Wisconsin School of Medicine and Public Health is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
Credit Designation StatementThe University of Wisconsin School of Medicine and Public Health designatesthisenduringmaterialforamaximumof1.0 AMA PRA Category 1 Credit™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Questions?Please contact Barb Anderson, at [email protected] or (608)263-8542.
Policy on DisclosureIt is the policy of the University of Wisconsin School of Medicine and Public Health that the faculty, authors, planners, and other persons who may influence content of this CME activity disclose all relevant financialrelationshipswithcommercialinterestsinordertoallowCMEstafftoidentifyand resolveanypotentialconflictsof interest.Facultymustalsodiscloseany planned discussions of unlabeled/unapproved uses of drugs or devices during their presentation(s). For this educational activity all conflicts ofinterests have been resolved and detailed disclosures are listed below:
The followingeditorsandauthors reporthavingnofinancial relationshipswith commercial interests and will not reference unlabeled or unapproved uses of drugs or devices: Barbara Anderson, J. Muse Davis, Michael Felber, Chad Hanson, Sheryl Henderson, Michelle Kelly, Kirstin Knackers, Cathy Means, Nan Peterson, Kristin Shadman, Ellen Wald, Christine Zimmerman.
This activity is a collaboration between the University of Wisconsin School ofMedicineandPublicHealth,DepartmentofPediatricsandtheOfficeofContinuing Professional Development and the American Family Children’s Hospital.
©2014bytheBoardofRegentsoftheUniversityofWisconsinSystem.All rights reserved.
No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by any means, electronic or mechanical, including photocopying or recording, with out the written permission of the Board of Regents of the University of Wisconsin.
Past issues of Pediatric Pathways are available at:
uwhealth.org/pediatricpathways
7

CH12300-0207P
Call the Access CenterThe American Family Children’s Hospital’s AccessCenterisopen24hoursaday,seven days a week to handle all issues surrounding patient admissions and referrals. Referring physicians can use the Access Center to:• Obtain rapid consultations with specialty
staffor• Refer patients on an or inpatient basis or• Request Med Flight or ground transport
(CHETA)Please note: Access Center is for the exclusive use of physicians and other health care providers caring for patients. Patients wishing to schedule appointments may call 1-800-323-8942(OutsideMadison)or (608)263-6420.
Referral informationTo facilitate smooth and timely transfers, we kindly ask physicians to provide the following information:• Patient’s name• Birth date• Patient address and telephone number• UW Hospital patient registration number
(if known)• Insurance information, including the
name of insurance plan or HMO, pre-admission requirements and second surgical opinion guidelines, if appropriate.
Prior authorizationTo assure compliance with payor-based prior authorization requirements, insurance information is necessary at the time of referral.Pleasecall(608)263-8773(orsendafaxto608-263-9422)tocontacttrainedadmissionandinsurancestaff.Ifyourpatient has no health insurance, an advisor maybecontactedat(608)263-8770toreview possible sources of assistance.
Outside Madison: (800) 472-0111 or Greater Madison Area: (608) 263-6796
Referring a patient?CalltheAccessCenter24/7
CH-402
84-14For listings of physicians by specialty, please visit
uwhealthkids.org
Subscribe Online Visit uwhealthkids.org/pediatricpathways and subscribe to this publication electronically. Pediatric Pathways is published quarterly online and semiannually in print.
Earn CME Credit!See inside this issue for more information.
University of Wisconsin Hospital and Clinics 301 S. Westfield Road, Suite 320Madison, WI 53717