Embed Size (px)
Citation preview

BRAIN INJURY, 1999, VOL. 13, NO. 4, 281 ± 290
Aerodynamic, acoustic, and perceptual measures
of nasality following traumatic brain injury
M O N I C A A . M C HE N RY
Galveston Institute of Human Communication, The Transitional Learning Community,
Galveston, TX, USA
(Received 10 October 1998; accepted 26 November 1998 )
Data were obtained from 31 subjects who had incurred a traumatic brain injury (TBI). Two expert
listeners judged nasality using direct magnitude estimation with a referent. They rated samples of the
first sentence of the Rainbow Passage, played backwards, with all pauses removed. Sensitivity was
good for nasalance, velopharyngeal airway resistance, and velopharyngeal orifice area, indicating that
these measures would accurately identify an individual as nasal. Specificity was reduced, and was
adequate only for nasalance. The reduced specificity was due to a high number of false positives,
i.e. perceived nasality in the absence of objective corroboration. Analysis of the false positives revealed
that a slow speaking rate could mislead a listener’s perception of nasality. Overall, for individuals with
dysarthria following TBI, the measure of nasalance may most accurately reflect listener perception of
nasality.
Introduction
There are a number of instrumentation based techniques to measure nasality. ² Little
data are available, however, regarding the degree to which the measures relate to
perceived nasality, particularly following traumatic brain injury (TBI). Dysarthria
following TBI is characterized by a multiplicity of deficits across the speech produc-
tion system. There is considerable variability from person to person, due to the
diffuse nature of the injury. This inherent complexity often makes it difficult to
judge nasality following TBI. Further, the frequency of nasality in dysarthric speak-
ers following TBI is high [1, 2]. The present work addresses the relationship among
commonly used assessment procedures and perceived nasality following TBI.
The correlation of nasalance, an acoustic measure of nasality, and perceived
nasality was initially addressed by Fletcher [3]. Nasalance is defined as the ratio of
nasal energy/(nasal+oral energy). Subjects in Fletcher’s work were children with
repaired cleft palates whose nasality was judged by university students in speech
classes. Although the correlation between grouped listener judgements and nasa-
lance scores was quite good (0.91), Fletcher recognized that the perception of
speech as acceptably or excessively nasal would depend upon the experiential frame-
work and values of the individual listener.
Brain Injury ISSN 0269± 9052 print/ISSN 1362± 301X online Ñ 1999 Taylor & Francis Ltd
http://www.tandf.co.uk/JNLS/bin.htm
http://www.taylorandfrancis.com/JNLS/bin.htm
Correspondence to: Monica A. McHenry, Galveston Institute of Human Communication,
The Transitional Learning Community, 1528 Postoffice St., Galveston, TX 77550, USA. e-mail:
[email protected]² In this work, the term nasality will be used synonymously with hypernasality.
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
ufts
Uni
vers
ity o
n 11
/04/
14Fo
r pe
rson
al u
se o
nly.

Other investigators have explored the relationship between clinical ratings of
nasality and nasalance scores. The majority have focused on establishing nasalance
norms to determine the presence or absence of nasality [4, 5], acknowledging that
these must vary according to language and regional dialect [5, 6]. Dalston and
Warren [7] assessed 124 individuals with cleft palate or craniofacial anomalies.
The ratings by three experienced judges corresponded reasonably well with nasa-
lance (0.76). In a later study [4], the good relationship (0.82) between nasalance
scores and clinical judgement was again supported. Finally, Hardin et al. [5] found
that 82% of nasalance scores reflected listener judgements of the presence or absence
of nasality. These authors, as well as other investigators [8], found a poor relation-
ship between nasalance scores and listener perception for individuals with pharyn-
geal flaps.
The lack of ideal correspondence between nasalance scores and perceived nas-
ality was addressed in recent work [9, 10]. Both studies concluded that nasal air
emission may impact the relationship between nasalance and listener judgements,
because the Nasometer (Kay Elemetrics, Pine Brook, NJ), an instrument based on
Fletcher’ s work, cannot distinguish between aerodynamic and acoustic energy.
Further, although nasal air emission increases the nasalance score, it may not con-
tribute to the perception of nasality.
Delorey et al. [11] conducted the only known study relating to nasalance with
perceived nasality in a neurogenic population. Their subjects were 27 individuals
with amyotrophic lateral sclerosis (ALS). Ten trained listeners rated nasality on a
seven point scale for /i/ and a sentence from the non-nasal `Zoo Passage’ [12]. The
investigators reported that nasalance was highly predictive of nasality ratings of /i/.
Nasalance has also been related to physiological variables. The majority of
physiological data has been obtained from speakers with cleft palate using the press-
ure-flow technique to calculate velopharyngeal orifice area [13]. This method uses a
modified hydraulic equation to calculate velopharyngeal orifice area. The calcula-
tion is based on nasal airflow and differential pressure. Dalston et al. [4] found a poor
correlation between velopharyngeal orifice area and nasalance, but the correlation
between a trained clinician’s judgement and nasalance was 0.82.
There are limitations to the studies reviewed above. They typically have studied
individuals with cleft palate or craniofacial anomalies, who present a much more
isolated problem than do individuals with traumatic brain injury (TBI), and they
employed interval scales for the rating of nasality.
Regarding the second limitation, sporadic research over the years has questioned
the use of interval scales to judge nasality. Historically, clinicians are inclined to use
them because they are easily and quickly administered, but they may not be an
appropriate way to judge nasality. The determination of appropriateness rests on
whether the phenomenon to be perceived is metathetic or prothetic. Metathetic
continua, such as pitch, are discrete and lend themselves to equal partitioning.
Prothetic continua, such as loudness, are additive and do not [14]. Many aspects
of speech production have been found to exist as prothetic continual [15± 17],
therefore, making judgements with interval scaling invalid.
Given these findings, it seems plausible that nasality too is perceived as a pro-
thetic, or additive phenomenon, thus requiring rating with something other than
interval scales. The most appropriate strategy for rating prothetic phenomena is
magnitude estimation, employed in the present work.
282 M. A. McHenryB
rain
Inj
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Tuf
ts U
nive
rsity
on
11/0
4/14
For
pers
onal
use
onl
y.

Methods
Subjects
Subjects were 31 individuals, 20 males and 11 females who incurred a traumatic
brain injury and were participating in a residential community re-entry programme.
Ages ranged from 13 to 45 years old (X = 25; SD = 7). Months post-injury ranged
from 2 to 288 (X = 47, SD = 73).
Procedures
All subjects underwent a comprehensive motor speech evaluation upon admission
to the rehabilitation programme. As part of this evaluation, individuals completed
tasks to assess velopharyngeal airway resistance and nasalance. First, velopharyngeal
airway resistance data were obtained. Individuals were then assessed with the
Nasometer. Finally, individuals were audio tape recorded to provide a sample for
perceptual rating.
To obtain the velopharyngeal airway resistance, subjects wore, over the nose, a
tight-fitting mask (Respironics, Norcross, GA) which was attached to a pneu-
motachograph (Hans Rudolph 4719, Kansas City, MO) and differential pressure
transducer (Honeywell 163PC01D36, Minneapolis, MN). Intraoral pressure was
measured just inside the lips using a polyethylene catheter (2 mm ID) attached to
a pressure transducer (162PC016). The catheter was positioned behind the incisors
so that its distal open tip was perpendicular to airflow and was not occluded by the
tongue. Aerodynamic data were low-pass filtered at 20 Hz (Biocommunications,
Madison, WI) and digitized at 3571 Hz.
The calculation of velopharyngeal airway resistance has been described else-
where in detail [18]. Briefly, velopharyngeal airway resistance was calculated by
dividing the peak intraoral air pressure during /p/ production by the corresponding
nasal airflow, and then subtracting nasal cavity resistance (including factors such as
congestion) at the same nasal airflow [19]. Because nasal cavity resistance is sub-
tracted in the calculation, the velopharyngeal airway resistance value reflects velo-
pharyngeal port function, rather than being a composite indicator of nasal airway
resistance. The pressure-flow technique developed by Warren and DuBois [13]
estimates velopharyngeal orifice area. It is widely accepted as an indicator of velo-
pharyngeal adequacy, but is somewhat invasive, requiring occlusion of the nares,
which perturbs the anterior vocal tract. Velopharyngeal airway resistance calculation
was performed in the present study because the subjects easily tolerated the pro-
cedure.
At a typical pitch and loudness, subjects produced tasks to determine nasal cavity
resistance. These tasks included three trials each of quiet and deep breathing, sus-
tained /m/, and /ma/ syllable trains. Subjects then produced /pi/ syllable trains at
approximately 1.5± 3 syllables/s. The subjects were instructed before each syllable
train to `Take a big breath’. The tasks were modelled and the subjects were pro-
vided with practice trials. Trials which did not meet the criteria of increased pre-
phonatory inspiration and smooth and connected syllable pulsing were re-run.
Before acquiring nasalance data, the Nasometer was calibrated according to the
manufacturer’ s instructions and the headgear fitted to the subject. For acoustic
assessment using the Nasometer, subjects repeated the non-nasal `Zoo Passage’ .
Measures of nasality following TBI 283B
rain
Inj
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Tuf
ts U
nive
rsity
on
11/0
4/14
For
pers
onal
use
onl
y.

During acquisition, nasal and oral acoustic waveforms were isolated by a sound
separator and then filtered with a 300-Hz band-pass filter with a centre frequency
at 500 Hz. Nasalance was determined using Nasometer software, which calculated
the ratio of nasal to nasal-plus-oral acoustic energy. The nasalance score was this
ratio multiplied by 100.
Audio data were obtained in a sound-proof booth using a microphone
(Sennheiser MD421, Old Lyme, CT), amplification (Symetrix SX202, Lynnwood,
WA), and digital audio tape (TASCAM DA-30, Montebello, CA). To provide
material for perceptual judgements, subjects read the `Rainbow Passage’ [20].
Velopharyngeal airway resistance data were analysed using automated software
[21] (RC Electronics, Santa Barbara, CA). Resistance values beyond 500 cm
H2O/ LPS were not calculated and were considered infinite.
As in previous work [22], the velopharyngeal airway resistance data were used to
calculate the velopharyngeal orifice area using the hydrokinetic orifice equation
originally reported by Warren and DuBois [13]. Zajac [23] describes the rationale
and details of the calculation. Velopharyngeal orifice area was calculated because
many clinicians and researchers employ this assessment technique.
Listening tapes were prepared as follows. The first sentence of the previously
recorded `Rainbow Passage’ was digitized at 51 200 samples per second. Pauses were
edited out to reduce overall speaking time and increase similarity across samples.
The sentence was then reversed (i.e. played backwards). A referent sentence (not
included in the samples to be judged) was chosen to represent moderate nasality.
The referent sentence was also reversed, and was recorded before each sample to be
rated. Each reversed sample (with referent) was recorded five times in completely
random order, for a total of 160 samples.
Judging was completed using direct magnitude estimation scaling [24]. The
judges were instructed to rate nasality based on a constant referent which was played
before each sample. If the nasality of the sample was perceived to be greater than the
referent, the judge drew a line proportionally longer than the referent line.
Conversely, if the sample was perceived to be less nasal than the referent, the
judge drew a proportionally shorter line. Two expert listeners judged the tapes.
Each listener had about 18 years experience in working with people with resonance
disorders.
The judges’ lines were manually measured. A ratio was calculated comparing the
length of the judge’s line with the referent line. The geometric mean of the 10
judgements for each sample (five listening opportunities two judges) was deter-
mined.
Inter- and intrajudge reliability were calculated according to Ebel [25].
Intrajudge reliability for judges 1 and 2 was 0.85 and 0.75 respectively.
Interjudge reliability was 0.80.
Results
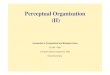
Perceived nasality ratings compared with the referent sample ranged from 0.64
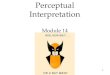
(roughly half as nasal) to 2.82 (roughly three times as nasal). Figures 1, 2, and 3
respectively illustrate perceived nasality compared with nasalance, with velophar-
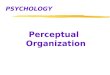
yngeal airway resistance, and with velopharyngeal orifice area. As expected, when
contrasting figures 2 and 3, high velopharyngeal airway resistance corresponded to
low velopharyngeal orifice area.
284 M. A. McHenryB
rain
Inj
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Tuf
ts U
nive
rsity
on
11/0
4/14
For
pers
onal
use
onl
y.

Results and calculated indices are summarized in tables 1, 2, and 3. For nasalance
(table 1), the sensitivity and specificity were 0.86 and 0.70, respectively, with an
overall accuracy of 0.77. The Kappa [26] value was 0.44, indicating a fair corre-
spondence between nasalance and perceived nasality. In particular, these results
suggest that individuals who were perceived to be more nasal than the referent,
were usually found to have increased nasalance as measured by the Nasometer. By
Measures of nasality following TBI 285
Figure 1. The relationship between nasalance and perceived nasality. Perceived nasality is compared with a
referent at 1.
Figure 2. The relationship between velopharyngeal airway resistance and perceived nasality. Perceived nasality is
compared with a referent at 1.
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
ufts
Uni
vers
ity o
n 11
/04/
14Fo
r pe
rson
al u
se o
nly.

contrast, although sensitivity was good for velopharyngeal resistance (table 2) and
estimated velopharyngeal orifice area (table 3), specificity was poor and the Kappa
values were low. In examining the tables, it is apparent that the decreased specificity
and reduced accuracy was due to a high number of false positives, i.e. the judges
perceived increased nasality when it was not present according to objective meas-
ures.
286 M. A. McHenry
Figure 3. The relationship between velopharyngeal orifice area and perceived nasality. Perceived nasality is
compared with a referent at 1.
Table 1. Decision data and calculated indices for nasalance
Nasalance
Perceived nasality Increased nasalance Decreased nasalance Total
More nasal 12 5 17
Less nasal 2 12 14
Total 14 17 31
Total cases, 31; sensitivity = 0.86; specificity = 0.70; accuracy = 0.77.
Table 2. Decision data and calculated indices for velopharyngeal airway resistance (Rvp )
Rvp
Perceived nasality Increased Rvp Decreased Rvp Total
More nasal 8 9 17
Less nasal 1 13 14
Total 9 22 31
Total cases, 31; sensitivity = 0.89; specificity = 0.59; accuracy = 0.68.
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
ufts
Uni
vers
ity o
n 11
/04/
14Fo
r pe
rson
al u
se o
nly.

The high number of false positives that occurred even with the nasalance meas-
ure was of interest. These erroneous perceptions could cause a clinician to perform
unnecessary assessment procedures. Therefore, several potential contributors to
perceived nasality in the absence of objective corroboration were explored. These
were speaking rate, intelligibility, and laryngeal airway resistance (as an indicator of
breathiness). For speaking rate, the number of words spoken per minute was cal-
culated without pauses for the first sentence of the `Rainbow Passage’ . Intelligibility
was based on a single naive judge’ s transcription of the CAIDS [27] sentence test.
Laryngeal airway resistance was obtained from 21 of the 31 subjects, using pre-
viously described standard procedures [28]. Kendall Tau correlations [29] were
calculated to determine the relationship between perceived nasality and each of
these measures obtained at the time of the evaluation. This non-parametric statistic
was used because the distribution of the variables precluded parametric analyses.
Perceived nasality was significantly associated with speaking rate
(Ktau = 0.3380 p < 0.008) and with intelligibility (Ktau = 0.4844, p < 0.000).
These findings indicate that there was a tendency to associate a slow speaking rate
and reduced intelligibility with perceived nasality. The relationship between nasa-
lance and both speaking rate and intelligibility was, therefore, explored. There was
no significant relationship between nasalance and speaking rate (Ktau = 0.0306,
p < 0.811). This implies that an individual could be erroneously perceived as
excessively nasal if their speaking rate was slow. The relationship between nasalance
and intelligibility was significant (Ktau = 0.2633, p < 0.05). Therefore, if a listener
perceived increased nasality in someone with reduced intelligibility, it was likely to
be present. Finally, there was no relationship between laryngeal airway resistance
and perceived nasality for the 21 subjects for whom this measure was obtained. This
indicates that breathiness, present in 71% of the sample, did not contribute to the
perception of nasality.
D iscuss ion
Of clinical interest is the high number of false positives that occurred in all three
analyses. Several avenues were pursued to determine factors which may have con-
tributed to the perception of increased nasality when it was not present in objective
tests. Although perceived nasality was associated with reduced intelligibility and
reduced speaking rate, it is only the reduced speaking rate that could potentially
mislead a clinician. It is possible that, because individuals with slow speaking rates
often present with significant dysarthria, listeners associate slowed rate with deficits
Measures of nasality following TBI 287
Table 3. Decision data compared to referent and calculated indices for estimated velopharyngeal orifice area
Orifice area
Perceived nasality Increased orifice area Decreased orifice area Total
More nasal 9 8 17
Less nasal 2 12 14
Total 11 20 31
Total cases, 31; sensitivity = 0.82; specificity = 0.40; accuracy = 0.68.
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y T
ufts
Uni
vers
ity o
n 11
/04/
14Fo
r pe
rson
al u
se o
nly.

across the speech systems. If the timing of velopharyngeal closure were slow as well,
the nasalance score would also have been associated with reduced speaking rate.
It was considered possible that reduced laryngeal airway resistance, manifested as
breathiness, would be associated with an increased perception of nasality.
Incomplete vocal fold closure increases the average air flow, compared with the
time varying air flow valved by the vocal folds [30]. This alters the spectrum of the
laryngeal signal due to a reduction in the signal-to-noise ratio. An open velophar-
yngeal port on the other hand, dampens the entire acoustic signal, as well as intro-
ducing antiformants which further reduce signal energy [31]. It appears that listeners
in this study were able to discriminate between the two types of signal reduction.
There are limitations to the present investigation. First, only two expert listeners
judged the samples. Secondly, the samples were played backwards, which affected
the ability to use consonant cues to judge nasality [32]. The strategy of playing the
samples backwards in the present study was employed to minimize the differential
effects of widely varying intelligibility upon perceived nasality.
Despite these limitations, the results suggest that nasalance data most closely
reflects expert listener judgements of nasality. This finding corresponds well with
Dalston et al. [4], who found a poor correlation between velopharyngeal orifice size
and listener judgement. It also supports the only other known study of perceived
nasality in individuals with neurogenic, rather than structural deficits [11]. It appears
that when there are concomitant deficits due to dysarthria across the speech pro-
duction mechanism, the nasalance value may provide the most useful basis for
judgements of nasality. This is particularly encouraging given the inherent difficul-
ties in assessing individuals with TBI. The respiratory and articulatory demands of
producing syllable trains for velopharyngeal airway resistance assessment are often
challenging. By contrast, phrasing and articulatory precision are not critical to
accurate nasalance assessment with the Nasometer. Further, procedures required
for aerodynamic assessment are more cumbersome. The nasal pressure sensing
catheter is often perceived by subjects to be invasive, and the oral pressure sensing
catheter becomes clogged frequently in individuals with saliva management diffi-
culties. Thus, the measure of nasalance may provide an efficient and representative
indicator of perceived nasality for individuals with TBI.
Authors who have studied individuals with cleft-palate and cranio-facial anom-
alities [5, 7] encouraged the use of multiple measures to determine the clinical
significance of nasality. Following TBI, however, it may be more important to
assess the relative contribution of nasality to the overall speech production deficit.
Other aspects of dysarthria may or may not be exacerbated by the presence of a
velopharyngeal valving deficit. While nasality may be clinically significant in isola-
tion, relative to an individual’ s cognitive and physical deficits, it may have minimal
impact on their daily activities or quality of life.
Acknowledgem ents
This work was supported by Grant #96-3 by the Moody Foundation of Galveston,
TX. The paper was presented at the American Speech, Hearing, and Language
Association annual convention in Seattle, WA, November 1996. The author grate-
fully acknowledges the expertise of John Palmer, Ph.D. and Rita Gillis, Ph.D., as
well as the technical support of John Minton and Lois Patterson.
288 M. A. McHenryB
rain
Inj
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Tuf
ts U
nive
rsity
on
11/0
4/14
For
pers
onal
use
onl
y.

References
1. THEODOROS, D., MURDOCH, B. E., STOKES, P. D. et al.: Hypernasality in dysarthric speakers
following severe closed head injury: a perceptual and instrumental analysis. Brain Injury, 7: 59± 69,
1993.
2. MCHENRY, M. A.: Velopharyngeal airway resistance disorders following traumatic brain injury.
Archives of Physical Medicine and Rehabilitation, 79: 545± 549, 1998.
3. FLETCHER, S. G.: Contingencies for bioelectronic modification of nasality. Journal of Speech and
Hearing Disorders, 37: 329± 346, 1976.
4. DALSTON, R. M., WARREN, D. W. and DALSTON, E. T.: Use of nasometry as a diagnostic tool
for identifying patients with velopharyngeal impairment. Cleft Palate-Craniofacial Journal, 28: 184±
189, 1991.
5. HARDIN, M. A., VAN DEMARK, D. R., MORRIS, H. L. et al.: Correspondence between nasalance
scores and listener judgments of hypernasality and hyponasality. Cleft Palate-Craniofacial Journal,
29: 346± 351, 1992.
6. SEAVER, E. J., DALSTON, R. M., LEEPER, H. A. et al.: A study of nasometric values for normal
nasal resonance. Journal of Speech and Hearing Research, 34: 715± 721, 1991.
7. DALSTON, R. M. and WARREN, D. W.: Comparison of Tonar II, pressure-flow, and listener
judgments of hypernasality in the assessment of velopharyngeal function. Cleft Palate Journal, 23:
108± 115, 1986.
8. NELLIS, J. L.,NEIMAN, G. S. andLEHMAN, J. A.: Comparison of nasometer and listener judgments
of nasality in the assessment of velopharyngeal function after pharyngeal flap surgery. Cleft Palate-
Craniofacial Journal, 29: 157± 163.
9. KARNELL, M. P.: Nasometric discrimination of hypernasality and turbulent nasal airflow. Cleft
Palate-Craniofacial Journal, 32: 145± 148, 1995.
10. WATTERSON, T., MCFARLANE, S. C. and WRIGHT, D. S.: The relationship between nasalance
and nasality in children with cleft palate. Journal of Communication Disorders, 26: 13± 28, 1993.
11. DELOREY, R. M., LEEPER, H. A. and HUDSON, A. J.: Aerodynamic and acoustic descriptions of
velopharyngeal closure in ALS. Paper presented at the American Speech-Language-Hearing
Association, Anaheim, CA, 1993.
12. FLETCHER, S. G.: Diagnosing Speech Disorders from Cleft Palate (Grune and Stratton), 1978.
13. WARREN, D. W. and DUBOIS, A. B.: A pressure-flow technique for measuring velopharyngeal
orifice area during continuous speech. Cleft Palate Journal, 1: 52± 71, 1964.
14. SNODGRAS, J. G.: Psychophysics. In B. Scharf and G. S. Reynolds (editors) Experimental Sensory
Psychology (Dallas: Scott, Foresman and Company), pp. 18± 67, 1975.
15. BERRY, R. C. and SILVERMAN, F. H.: Equality of intervals on the Lewis-Sherman Scale of
Stuttering Severity. Journal of Speech and Hearing Research, 15: 185± 188, 1972.
16. SCHIAVETTI, N., METZ, D. E. and SITLER, R. W.: Construct validity of direct magnitude estima-
tion and interval scaling of speech intelligibility: Evidence from a study of the hearing impaired.
Journal of Speech and Hearing Research, 24: 441± 445, 1981.
17. SOUTHWOOD, M. H.: Direct magnitude estimation and interval scaling of naturalness and bizare-
ness of the dysarthria associated with amyotrophic lateral sclerosis. Journal of Medical Speech±
Language Pathology, 4: 13± 25, 1996.
18. MCHENRY, M.: Velopharyngeal airway resistance disorders after traumatic brain injury. Archives of
Physical Medicine and Rehabilitation, 79: 545 ± 549, 1998.
19. BARLOW, S. M. and SUING, G.: Aerospeech: Automated digital signal analysis of speech aero-
dynamics. Journal for Computer Users in Speech and Hearing, 7: 211± 227, 1991.
20. FAIRBANKS, G.: Voice and Articulation Drillbook (New York: Harper and Brothers), 1960.
21. BARLOW, S. M., SUING, G., GROSSMAN, A. et al.: A high-speed data acquisition and protocol
control system for vocal tract physiology. Journal of Voice, 3: 283± 293, 1989.
22. MCHENRY, M. A.: The effect of increased vocal effort on estimated velopharyngeal orifice area.
American Journal of Speech-Language Pathology, 6: 55± 61, 1997.
23. ZAJ AC, D. J.: Comment on McHenry (1997). American Journal of Speech-Language Pathology, 7: 95,
1998.
24. ENGEN, T.: Psychophysics: II. Scaling Methods. In J. W. Kling and L. A. Riggs (editors)
Woodworth & Schlosberg’ s Experimental Psychology (New York: Holt, Rinehart and Winston,
Inc.), pp. 47± 86, 1971.
25. EBEL, R. L.: Estimation of the reliability of ratings. Psychometrika, 16: 407± 424, 1951.
Measures of nasality following TBI 289B
rain
Inj
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Tuf
ts U
nive
rsity
on
11/0
4/14
For
pers
onal
use
onl
y.

26. COHEN, J.: A coefficient of agreement for nominal scales. Educational Psychological Assessment, 20:
37± 46, 1960.
27. YORKSTON, K., BEUKELMAN, D. and TRAYNOR, D.: Computerized assessment of intelligibility of
dysarthric speech (Tigard, OR: C.C. Publication Inc), 1984.
28. MCHENRY, M. A.: Laryngeal airway resistance following traumatic brain injury. In D. A. Robin,
K. Yorkston and D. R. Beukelman (editors) Disorders of Motor Speech: Assessment, Treatment, and
Clinical Characterization (Baltimore: Paul H. Brookes Publishing Company), pp. 229± 240, 1996.
29. SPSS for Windows. Release 6.1 (444 N. Michigan Ave, Chicago, ILL 60611: SPSS Inc.), 1994.
30. TITZE, I. R. Principles of Voice Production (Englewood Cliffs, NJ: Prentice Hall), 1994.
31. KENT, R. D. and READ, C.: The Acoustic Analysis of Speech (San Diego, CA: Singular Publishing
Group, Inc.), 1992.
32. COUNIHAN, D. T. and CULLINAN, W. L.: Reliability and dispersion of nasality ratings. Cleft Palate
Journal, 7: 261± 270, 1970.
290 Measures of nasality following TBIB
rain
Inj
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Tuf
ts U
nive
rsity
on
11/0
4/14
For
pers
onal
use
onl
y.