Embed Size (px)
DESCRIPTION
•Background•Pathophysiology•Frequency•Mortality/Morbidity•Clinical Examinination•Differential Diagnoses•Treatment Modalities•Prognosis•Jordanian Perspective
Citation preview

Wilms’ TumorNephroblastoma
AbdulQadir J. Nashwan

Road Map

Max Wilms, MD
To know more about Max Wilms

Background
Wilms’ tumor, or nephroblastoma, is the most common childhood abdominal malignancy
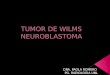
at present5o years ago
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Survival Rates in Children with Wilm's Tumor
(Coppes & Pritchard-Jones, 2000)

Frequency
• Wilms’ tumor affects approximately 10 children and
adolescents per 1 million before the age of 15 years.
• Accounts for 6-7% of all childhood cancers in North America.
• About 450-500 new cases are diagnosed each year
(ACS, 2010)

Facts
• In 7% of children with Wilms’ tumor, both kidneys are involved at diagnosis.
• In only 1% of the children who have a kidney removed due to Wilms’ tumor, does the cancer re-appear later in the other kidney.
• Possible causable factors in the environment of parents or their child that might lead to Wilms’ tumor have not been determined.
• There is a family history of the disease in only 1% of cases.
(NWTSG)

Race
6-9 cases per million
3-4 cases per million
10 cases per million
(Breslow, Olshan, Beckwith & Green, 1993)

Gender
10.6
:
(Breslow, Olshan, Beckwith & Green, 1993)

Age
The median age at diagnosis is
approximately 3.5 years
(Breslow, Olshan, Beckwith & Green, 1993)

Wilms’ Tumor Experience at King Hussein Medical Center
Saudi Journal of Kidney Disease and Transplantation
2000
Isam Haddadin, Pediatric Oncologist
Issa Hazza, Pediatric Nephrologist


Overgrowth Abnormalities
hemihypertrophyBeckwith-
Wiedemann Syndrome
Omphalocele
Associated Signs & Syndromes

The WAGR Syndrome
Wilms’ Tumor
Aniridia
Genito-urinary Malformations
Mental Retardation

Wilms’ Tumor

Clinical Features
Abdominal mass 80%
Abdominal pain or Hematuria 25%
UTI and varicocele are less common findings
Hypertension, gross hematuria, and fever 5-30%

Diagnoses
Laboratory Studies
Imaging Studies
Histological Findings
Staging

Diagnoses
Laboratory Studies
CBC countChemistry
profile
(KFT & LFT)Urinalysis Coagulation
studies
Cytogenetics studies
(WT1 gene)

Diagnoses
Imaging Studies
Renal ultrasonography CT scanning MRI scanning

Diagnoses
Histological Findings
Nephrogenic rests (NRs)
believed to represent precursor lesions.

Stage I.• The tumor is limited to the kidney, is encapsulated, and can
be completely removed surgically.Stage II.
• The tumor extends beyond the kidney but is completely removed.
Stage III.• The tumor is not completely removed surgically, but
disease is still limited to the abdomen.Stage IV.
• The disease has spread to the lung, liver, bone, brain, or to lymph nodes outside the pelvic region.
Stage V.• Both kidneys contain tumor at diagnosis.
Staging
(NWTSG)

Treatment & MedicationStage and Histology Surgery Chemotherapy Radiation Therapy*
Stage I or II favorable histology without LOH 1p
and 16q Nephrectomy Vincristine, dactinomycin No
Stage I or II favorable histology with LOH 1p and
16qNephrectomy
Vincristine, dactinomycin, doxorubicin
No
Stage III and IV favorable histology without LOH 1p
and 16qNephrectomy
Vincristine, dactinomycin, doxorubicin
Yes
Stage III and IV favorable histology with LOH 1p and
16qNephrectomy
Vincristine, dactinomycin, doxorubicin,
cyclophosphamide, etoposide
Yes
(Dome, et al 2006)
Table 1. Current Approach to Favorable Histology Wilms Tumo by Stage

References1. Coppes MJ, Pritchard-Jones K. Principles of Wilms' tumor biology. Urol
Clin North Am. Aug 2000;27(3):423-33, viii.
2. Breslow N, Olshan A, Beckwith JB, Green DM. Epidemiology of Wilms tumor. Med Pediatr Oncol. 1993;21(3):172-81
3. Dome JS, Cotton CA, Perlman EJ, et al. Treatment of anaplastic histology Wilms' tumor: results from the fifth National Wilms' Tumor Study. J Clin Oncol. May 20 2006;24(15):2352-8.
4. Coppes MJ, Arnold M, Beckwith JB, et al. Factors affecting the risk of contralateral Wilms tumor development: a report from the National Wilms Tumor Study Group. Cancer. Apr 1 1999;85(7):1616-25.