Embed Size (px)
Citation preview
Trust Guideline for the Management of Gastroschisis A clinical guideline recommended
For use in:Children’s ServicesFoetal Medicine
By:Children’s healthcare providers in the above areas (All staff in the named area)
For: Neonatal period
Division responsible for document: Division 3 – Women and Children’s
Key words:Gastroschisis, Assessment, Management, Closure, Neonates, Antenatal, Postnatal
Names of document authors: Miss Alexandra Scarlett, Dr Florence Walston
Job titles of document authors:Specialty Registrar in Paediatric Surgery, Neonatology Consultant
Name of document author’s Line Manager:
Mr Ashish Minocha
Job title of document author’s Line Manager:
Consultant Paediatric Surgeon
Supported by:Consultant Paediatric and Neonatal SurgeonsNeonatology Consultants, Paediatric Anaesthetic Consultants
Assessed and approved by:
Clinical Guidelines Assessment Panel (CGAP)
If approved by committee or Governance Lead Chair’s Action; tick here
Date of approval: 09/03/2021
Ratified by or reported as approvedto (if applicable):
Clinical Safety and Effectiveness Sub-Board
To be reviewed before:This document remains current after this date but will be under review
09/03/2024
To be reviewed by: AuthorsReference and / orTrustdocs ID No:
14521
Version No: 1.1Description of changes: N/A as new documentCompliance links: (is there any NICE related to guidance)
None
If Yes – does the strategy/policy deviate from the recommendations of NICE?If so, why?
N/A
This guideline has been approved by the Trust's Clinical Guidelines Assessment Panel as an aid to the diagnosis and management of relevant patients and clinical circumstances. Not every patient or situation fits neatly into a standard guideline scenario and the guideline must be interpreted and applied in practice in the light of prevailing clinical circumstances, the diagnostic and treatment options available and the professional judgement, knowledge and expertise of relevant clinicians. It is advised that the rationale for any departure from relevant guidance should be documented in the patient's case notes. The Trust's guidelines are made publicly available as part of the collective endeavour to continuously improve the quality of healthcare through sharing medical experience and knowledge. The Trust accepts no responsibility for any misunderstanding or misapplication of this document.
Clinical Guideline for: Management of Gastroschisis Author/s: A Scarlett, F Walston Author/s title: SpR Paediatric Surgery, Neonatology ConsultantApproved by: CGAP Date approved: 09/03/2021 Review date: 09/03/2024 Available via Trust Docs Version: 1.1 Trust Docs ID: 14521 Page 1 of 16
Trust Guideline for the Management of Gastroschisis
Version and Document Control:
VersionNumber
Date ofUpdate
Change Description Author
1.1 09/03/2021Reviewed but no clinical changes made
Miss Alexandra Scarlett, Dr Florence Walston
This is a Controlled Document
Printed copies of this document may not be up to date. Please check the hospitalintranet for the latest version and destroy all previous versions.
Clinical Guideline for: Management of Gastroschisis Author/s: A Scarlett, F Walston Author/s title: SpR Paediatric Surgery, Neonatology ConsultantApproved by: CGAP Date approved: 09/03/2021 Review date: 09/03/2024 Available via Trust Docs Version: 1.1 Trust Docs ID: 14521 Page 2 of 16
Trust Guideline for the Management of Gastroschisis
Quick reference
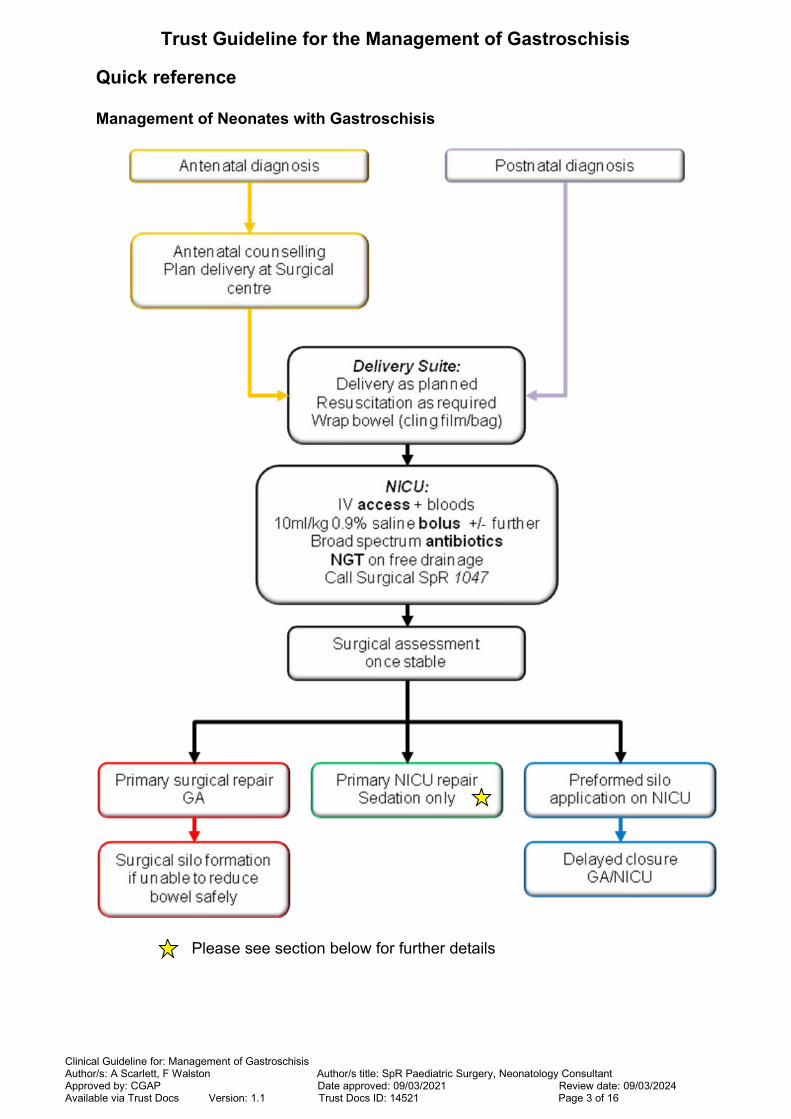
Management of Neonates with Gastroschisis
Please see section below for further details
Clinical Guideline for: Management of Gastroschisis Author/s: A Scarlett, F Walston Author/s title: SpR Paediatric Surgery, Neonatology ConsultantApproved by: CGAP Date approved: 09/03/2021 Review date: 09/03/2024 Available via Trust Docs Version: 1.1 Trust Docs ID: 14521 Page 3 of 16
Trust Guideline for the Management of Gastroschisis
Glossary and abbreviations
CPAP Continuous positive airway pressure
CXR Chest X-ray
ETT Endotracheal tube
FBC Full blood count (haematology blood test)
IV Intravenous
GA General anaesthetic
MDT Multidisciplinary team
NEC Necrotising enterocolitis
NICU Neonatal intensive care unit
NGT Nasogastric tube
PIP Peak inspiratory pressure
SALT Speech and language team
Silo Plastic construction (either ‘homemade’ by the surgeon or ‘pre-made’) to protect bowel whilst allowing it to return into abdomen over time using gravity = staged closure
SMOF Lipid emulsion form of parenteral nutrition (Soybean oil, Medium chain
triglycerides, Olive oil, Fish oil)
TPN Total parenteral nutrition
USS Ultrasound scan
U+ E Urea and electrolytes (biochemistry blood test)
UAC Umbilical arterial catheter
UVC Umbilical venous catheter
Clinical Guideline for: Management of Gastroschisis Author/s: A Scarlett, F Walston Author/s title: SpR Paediatric Surgery, Neonatology ConsultantApproved by: CGAP Date approved: 09/03/2021 Review date: 09/03/2024 Available via Trust Docs Version: 1.1 Trust Docs ID: 14521 Page 4 of 16
Trust Guideline for the Management of Gastroschisis
Objective
The various methods for surgical management of gastroschisis are well established with a solid evidence base. The NNUH Trust Guideline aims to standardise pre-operative care across the department; with a focus on the MDT optimising infants in an efficient and structured fashion; allowing a timely and safe surgical repair.
Background
Gastroschisis represents one of the more common congenital anterior abdominalwall defects and its incidence has increased in the past 10 years (now 1 in 2000-5000). This trend is partially due to improved antenatal detection which allows for MDT planning and counselling. This, normally right sided, ventral defect has an unknown, but suspected complex aetiology. Visceral herniation involves the midgut and possibly the bladder, liver, stomach and reproductive organs in females. A simple gastroschisis is associated with uncomplicated closure and speedy achievement of full enteral feeds. A complex case may be associated with intestinal atresias (~10% patients), perforation, necrosis and a loss of bowel length (leading to short bowel syndrome). These complex patients are more likely to develop long-term complications with gut dysmotility, malabsorption and intestinal failure.
Although gastroschisis repair was first reported in 1940’s, the mortality remained above 90% until a combination of a staged reduction, described by Schuster et alin 1967, and the subsequent advent of parenteral nutrition. Since then outcomeshave continued to dramatically improve, up to the current expectations of >90% survival rate.
Differential diagnoses include an omphalocoele, hernia of the cord, urachal remnant or patent vitellointestinal duct or bladder exstrophy. (Please see Appendix 3 for differences between omphalocoele and gastroschisis)
Rationale
There is variation in pre-operative management across the department leading tosome confusion throughout the extended medical team. This guideline strives to streamLine the preparation of a neonate prior to the time sensitive closure of the abdominal defect.
Key points
1) Antenatal counselling where possible and delivery at surgical centre with serial USS to reduce risk of bowel compromise
2) Prevent loss of heat and fluid from bowel with cling-film/plastic bag
3) Resuscitation with IV access and fluid bolus and broad spectrum antibiotics
4) Assess bowel to plan closure technique
Antenatal management
Clinical Guideline for: Management of Gastroschisis Author/s: A Scarlett, F Walston Author/s title: SpR Paediatric Surgery, Neonatology ConsultantApproved by: CGAP Date approved: 09/03/2021 Review date: 09/03/2024 Available via Trust Docs Version: 1.1 Trust Docs ID: 14521 Page 5 of 16
Trust Guideline for the Management of Gastroschisis
If a gastroschisis diagnosis is suspected antenatally there should be:
Parental counselling by an appropriate member of the Paediatric Surgical, NICU and Foetal medicine teams.
Close liaison between the teams regarding timing of delivery.
Plan to deliver in NNUH or another Surgical centre.
Gastroschisis should not dictate mode of delivery which can be determined by obstetric factors.
The vast majority of gastroschisis cases are diagnosed antenatally and subsequently undergo serial USS with the Foetal Medicine Unit. Evidence has suggested the fascial defect narrows in the third trimester, causing congestion in any incarcerated bowel loops; ultimately this can compromise the bowel vascularity or the defect close completely. Serial USS allows close monitoring of the defect and the herniated viscera, with signs of bowel dilatation used as an indication for earlier induction of labour.
Once delivery is imminent the On-call Paediatric Surgery registrar (#1047) shouldbe informed who will contact the On-call Paediatric Surgery Consultant.
Initial postnatal management
The principles of managing an infant with gastroschisis have not significantly changed since it was first described: resuscitation of the neonate, minimise losses (both heat and fluid) and prompt surgical management of the eviscerated bowel.
Pre-operative management can be divided into three portions:
On delivery suite:
Routine resuscitation of the infant, as required, by a Tier 2 Neonatal practitioner.
Visual inspection of eviscerated bowel (colour, inflammation, any obvious atresia) and document findings.
Minimise heat and fluid loss from exposed viscera by wrapping baby in cling film whilst warming baby on the Resuscitaire® or incubator.
The bowel should be wrapped in such a way that it is supported on the anterior abdominal wall avoiding torsion or tension on the vascular pedicle (See Appendix 4).
Stabilise baby +/- intubation if required – avoiding CPAP and high-flow O2
where possible.
If there is any doubt regarding viscera (black/dusky) call Surgical SpR asap.
Place an 8Fr NGT (or as large as possible), aspirate and leave on free drainage.
Clinical Guideline for: Management of Gastroschisis Author/s: A Scarlett, F Walston Author/s title: SpR Paediatric Surgery, Neonatology ConsultantApproved by: CGAP Date approved: 09/03/2021 Review date: 09/03/2024 Available via Trust Docs Version: 1.1 Trust Docs ID: 14521 Page 6 of 16
Trust Guideline for the Management of Gastroschisis
On arrival in NICU:
Made nil by mouth (and may continue for a significant period post-operatively).
Peripheral IV line should be inserted to allow blood tests (FBC, U+E, clotting screen and crossmatch).
Consider need for 10mL/kg bolus of 0.9% saline.
Most infants born with gastroschisis are in a significant (>25%) fluiddeficit at birth and may require a further 10mL/kg bolus.
Maintenance fluids should be established at a suitable volume for gestation.
Broad spectrum antibiotics (eg. Benzylpenicillin, metronidazole and gentamicin) should be commenced to reduce risk from bacterial translocation.
When baby is stable, the Paediatric Surgical SpR (#1047) should be informed of the patient’s arrival on the unit.
Due to likely prolonged period of bowel rest required post-operatively, these patients will need TPN with SMOF lipid when central venous access is achieved (not for UAC/UVC).
Surgical assessment on NICU
may require 1-2 extra hands to manoeuvre baby/bowel
The basic principles remain; therefore this examination should occur within a humidified, warm incubator. The viscera should be inspected for inflammation, general condition and atresias. The defect should be assessed (including internal margin) and measured and the abdominal cavity size considered, especially in small for gestational age or premature infants. Once the examination is complete the viscera should be re-wrapped within cling-film in a stable and supported position to optimise good perfusion.
After discussion with the On-call Paediatric Surgical consultant, there are three possible courses of action (to be used as per Surgeon’s preference):
PRIMARY SURGICAL REPAIR under GA
Aim to return viscera to abdomen if possible and close defect or form asurgical silo if bowel not reducible
Majority of repairs use this method; especially with a small defect, significant peel/matting or small sized abdomen
PRIMARY ‘SUTURELESS’ REPAIR ON NICU
Bowel replaced in abdomen on NICU and defect closed with umbilical cord and SteriStrips®
Clinical Guideline for: Management of Gastroschisis Author/s: A Scarlett, F Walston Author/s title: SpR Paediatric Surgery, Neonatology ConsultantApproved by: CGAP Date approved: 09/03/2021 Review date: 09/03/2024 Available via Trust Docs Version: 1.1 Trust Docs ID: 14521 Page 7 of 16
Trust Guideline for the Management of Gastroschisis
Considered if good sized abdomen in a stable baby, with moderately healthy bowel
PRE-FORMED SILO APPLICATION ON NICU
Bowel placed in a commercially available ‘silo’, commonly Medicina (see Appendix 2), bowel passively returns into abdominal cavity; followed by either ‘sutureless’ or surgical closed at later date (normally 3-5 days later).
Consider if significant healthy bowel eviscerated
Due to the potential need for urgent laparotomy following a trial of closure on NICU, the Emergency theatre team should be alerted prior to any attempt and consider discussing with the On-Call Paediatric Anaesthetic consultant. The closure of the defect should occur promptly after the decision to operate. Pre-operative bloods should be checked and parents fully consented.Surgical closure
The standard procedure is grossly similar whether in theatre or on NICU and involves the following steps:
Full paralysis if under GA
Assess viscera and decompress upper gastrointestinal tract via NGT. Consider bowel washout if marked distension of colon or distal small bowel. Divide any mesenteric bands attached to defect rim
Gentle reduction of viscera without compromising blood supply
Respiratory effort to be carefully monitored with early intervention if any deterioration
Closure of defect
Documentation of:
o Herniated viscera
o Size of defect
o Type of closure
o Clear post-operative plan regarding ventilation, antibiotic duration, monitoring for bowel compromise or compartment syndrome
Post-operative recovery often slow
o Prolonged PN use
o Intestinal dysmotility and potential subsequent failure
o Increased risk of NEC
o Prolonged length of stay
Further considerations for NICU bedside reduction
Clinical Guideline for: Management of Gastroschisis Author/s: A Scarlett, F Walston Author/s title: SpR Paediatric Surgery, Neonatology ConsultantApproved by: CGAP Date approved: 09/03/2021 Review date: 09/03/2024 Available via Trust Docs Version: 1.1 Trust Docs ID: 14521 Page 8 of 16

Trust Guideline for the Management of Gastroschisis
Due to the risk of a failed bedside reduction and possible need for urgent laparotomy or bedside application of a preformed silo, the parents should also beconsented for these alternative strategies. Please consider informing the On-call Paediatric Anaesthetic consultant if high suspicion of need for laparotomy. Assess baby for need for low flow oxygen during reduction.
Prior to commencing reduction the following team members should be available:
2x members of surgical team
1-2x assistants (to hold baby and to aspirate the NGT)
An allocated NICU nursing member to monitor baby +/- NICU staff as ‘runner’ for any additional equipment
NICU medical team on stand-by in anticipation of potential problems
A team brief should confirm that all team members are available. They should be confident in their roles and aware of steps involved. A list of equipment required for a bedside reduction can be found in Appendix 1. Commence LocSSIP documentation (Trustdocs ID: 14520) prior to starting procedure.
The following should also be considered prior to beginning attempt:
Appropriate monitoring on baby
Good light source available and correctly positioned
Wide bore NGT in situ and on free drainage
Antibiotics given
IV paracetamol given - consider using sucrose for comfort
Need for opiates or sedation prior to procedure (IV morphine 50mcg/kg or buccal midazolam)
Need for rectal washout
Baby stable prior to attempting reduction
Factors to consider converting to GA reduction:
Any difficulty in reducing bowel
Any compromise bowel or defects previously not seen
Any respiratory or cardiac embarrassment
Any tension in abdomen on closing defect
Post closure progress
Post-operative plans will vary depending on surgical findings and procedure performed. Enteral feeds may be considered once NG aspirates have reduced, this may take weeks requiring prolonged use of PN. Babies should be fed on the
Clinical Guideline for: Management of Gastroschisis Author/s: A Scarlett, F Walston Author/s title: SpR Paediatric Surgery, Neonatology ConsultantApproved by: CGAP Date approved: 09/03/2021 Review date: 09/03/2024 Available via Trust Docs Version: 1.1 Trust Docs ID: 14521 Page 9 of 16
Trust Guideline for the Management of Gastroschisis
high risk feeding regimen with close monitoring due to increased risk of NEC witha low threshold for Surgical assessment +/- conservative management.
Wound care post closure
The care of post-operative gastroschisis wounds can be difficult as can have increased risk of infection. Any erythema noted should be reviewed closely, including for possible NEC. Dressings will depend on type of closure. ‘Sutureless’closure dressings will normally consist of SteriStrips® and occlusive dressings and should remain in situ for 7 days (unless otherwise specified); care for surgical closure wounds should be as per the operative note.
Antibiotic use post reduction of bowel This may vary in individual cases.
Primary surgical closure – 5 days unless specified differently on operative note
‘Sutureless’ closure – 5 days and review
Pre-formed silo reduction – continue until 24hrs post removal of silo
Management of babies after pre-formed Silo application
Assess appropriate use of pain relief
Consider low flow oxygen as required
Change and weigh gauze around silo regularly and replace losses appropriately
Regularly assess bowel perfusion (notably any colour change) – please call Paediatric Surgery SpR (#1047) if concerned and consider releasing ‘slip knot’
Ensure umbilical cord remains moist
Ensure silo remains vertical at all times
Factors for discharge
Feeding established (NGT/bottle/breast) and parents trained (i.e. NGT feeds)
Adequate growth on current feeding plan
Dietician plan in place
Contact with local paediatrician / Health visitor / Social worker as required
Audit of Guideline – to be performed in 24-36 months (prior to guideline review)
1. Surgical antenatal counselling[100%]
Clinical Guideline for: Management of Gastroschisis Author/s: A Scarlett, F Walston Author/s title: SpR Paediatric Surgery, Neonatology ConsultantApproved by: CGAP Date approved: 09/03/2021 Review date: 09/03/2024 Available via Trust Docs Version: 1.1 Trust Docs ID: 14521 Page 10 of 16
Trust Guideline for the Management of Gastroschisis
2. Time to surgical intervention[100%]
Silo or primary closure within 6hrs for in-house patients
3. Operative documentation[100%]
The audit results will be sent to the department Audit Lead, who will ensure that these are discussed at relevant governance meetings to review the results and make recommendations for further action.
Development and consultation process undertaken before registration and dissemination
The authors listed above drafted this document on behalf of NICU/Paediatric Surgery Consultants who has agreed the final content.
This version has been endorsed by the Clinical Guidelines Assessment Panel Committee(s).
Distribution List
Trust intranet
Children’s services
NICU
Foetal Medicine
References
1. Gamba P, Midrio P. Abdominal wall defects: prenatal diagnosis, newborn management, and long-term outcomes. Semin Pediatr Surg. 2014 Oct;23(5):283-90.
2. Lansdale N, Hill R, Gull-Zamir S et al. Staged reduction of gastroschisis using preformed silos: practicalities and problems. J Pediatr Surg. 2009 Nov;44(11):2126-9
3. Long AM, Court J, Morabito A, Gillham JC. Antenatal diagnosis of bowel dilatation in gastroschisis is predictive of poor postnatal outcome. J Pediatr Surg. 2011 Jun;46(6):1070-5.
4. Spitz L and Coran AG. Operative Pediatric Surgery. 6e 2006 CRC Press, USA; Chapter 31 – Gastroschisis, pages 267-277
5. Weinsheimer RL, Yanchar NL, Bouchard SB et al; Canadian Pediatric Surgery Network. Gastroschisis closure--does method really matter? J Pediatr Surg. 2008 May;43(5):874-8
Clinical Guideline for: Management of Gastroschisis Author/s: A Scarlett, F Walston Author/s title: SpR Paediatric Surgery, Neonatology ConsultantApproved by: CGAP Date approved: 09/03/2021 Review date: 09/03/2024 Available via Trust Docs Version: 1.1 Trust Docs ID: 14521 Page 11 of 16

Trust Guideline for the Management of Gastroschisis
6. Preformed Silo Application: Guideline for Application, Daily Care, Sequential Bowel Reduction and Defect Closure for the Management of Gastroschisis. J Bell. Sheffield Children’s NHS Foundation Trust (to be submitted for approval 2017)
Clinical Guideline for: Management of Gastroschisis Author/s: A Scarlett, F Walston Author/s title: SpR Paediatric Surgery, Neonatology ConsultantApproved by: CGAP Date approved: 09/03/2021 Review date: 09/03/2024 Available via Trust Docs Version: 1.1 Trust Docs ID: 14521 Page 12 of 16
Trust Guideline for the Management of Gastroschisis
Appendix 1 - Equipment required for bedside gastroschisis reduction or Silo application
Beside reduction
Extra umbilical clamp
Suture (eg. 2/0 PDS, 3/0 vicryl ties)
Scissors
Aqueous chlorhexidine 2% or betadine solution
Disposable blade
Saline ampoules
½” and ¼“ SteriStrips®
Occulsive dressing (eg Tegaderm™)
Inco sheets
Cling film
Preformed silos available
Rectal washout
Jacques catheter 14/16Fr
Warm saline (20mL/kg)
60mL bladder syringe
Silo applicationAbove +:
Preformed silos in multiple sizes (found in Theatre 12 store cupboard) – see Appendix 2
Cavilon™ Spray
Dressing pack including multiple gauze swabs
Small Tegaderm™ dressings – multiple required
Large Jelonet™ dressing for wrapping cord
Clinical Guideline for: Management of Gastroschisis Author/s: A Scarlett, F Walston Author/s title: SpR Paediatric Surgery, Neonatology ConsultantApproved by: CGAP Date approved: 09/03/2021 Review date: 09/03/2024 Available via Trust Docs Version: 1.1 Trust Docs ID: 14521 Page 13 of 16

Trust Guideline for the Management of Gastroschisis
Appendix 2 – Pre-formed silos
A ‘silo’, whether surgically constructed or ‘preformed’ are commonly used in a staged repair of gastroschisis. Sterile plastic/silicone is fashioned into watertight container for the bowel and secured to the abdominal wall (with a dressing or suture). The column of bowel loops then returns to the abdominal cavity over time under the pressure of gravity and some gentle compression. Closure of the residual defect then occurs, either on NICU (sutureless) or in theatre under GA.
Figure 1 – Pre-formed silo
Figure 2 – Pre-formed silo insitu undergoing gentle reductions
Update August 2017
Currently the Medicina Preformed silos are unavailable pending update of their CE Mark following a manufacturing fault. Whilst these are unavailable most babies will require operative primary closure. Application of a silo in situations where primary closure cannot be achieved will require nonstandard techniques and products.
Clinical Guideline for: Management of Gastroschisis Author/s: A Scarlett, F Walston Author/s title: SpR Paediatric Surgery, Neonatology ConsultantApproved by: CGAP Date approved: 09/03/2021 Review date: 09/03/2024 Available via Trust Docs Version: 1.1 Trust Docs ID: 14521 Page 14 of 16
Trust Guideline for the Management of Gastroschisis
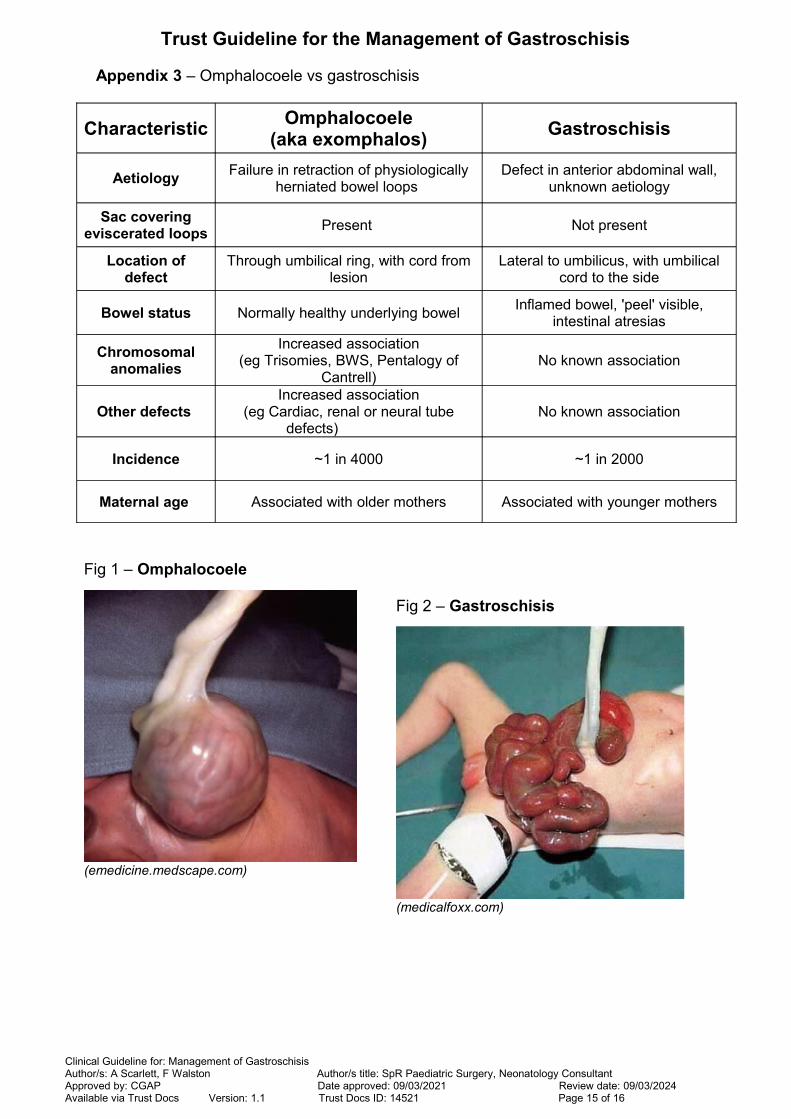
Appendix 3 – Omphalocoele vs gastroschisis
CharacteristicOmphalocoele
(aka exomphalos)Gastroschisis
AetiologyFailure in retraction of physiologically
herniated bowel loops Defect in anterior abdominal wall,
unknown aetiology
Sac coveringeviscerated loops
Present Not present
Location ofdefect
Through umbilical ring, with cord fromlesion
Lateral to umbilicus, with umbilicalcord to the side
Bowel status Normally healthy underlying bowelInflamed bowel, 'peel' visible,
intestinal atresias
Chromosomalanomalies
Increased association(eg Trisomies, BWS, Pentalogy of
Cantrell)No known association
Other defects Increased association
(eg Cardiac, renal or neural tubedefects)
No known association
Incidence ~1 in 4000 ~1 in 2000
Maternal age Associated with older mothers Associated with younger mothers
Fig 1 – Omphalocoele
(emedicine.medscape.com)
Fig 2 – Gastroschisis
(medicalfoxx.com)
Clinical Guideline for: Management of Gastroschisis Author/s: A Scarlett, F Walston Author/s title: SpR Paediatric Surgery, Neonatology ConsultantApproved by: CGAP Date approved: 09/03/2021 Review date: 09/03/2024 Available via Trust Docs Version: 1.1 Trust Docs ID: 14521 Page 15 of 16

Trust Guideline for the Management of Gastroschisis
Appendix 4 – Suggestion for wrapping of the bowel in cling film
Cling film covering all eviscerated bowel – without compressing bowel
Bowel remains well perfused in central position on anterior abdominal wall
‘Bolsters’ (in red on diagram) can be used either side to support bowel (eg usingrolled IncoSheets)
Umbilical cord should be kept moist with Jelonet™
Clinical Guideline for: Management of Gastroschisis Author/s: A Scarlett, F Walston Author/s title: SpR Paediatric Surgery, Neonatology ConsultantApproved by: CGAP Date approved: 09/03/2021 Review date: 09/03/2024 Available via Trust Docs Version: 1.1 Trust Docs ID: 14521 Page 16 of 16
![Cloacal exstrophy associated with gastroschisis: Case ...gastroschisis, omphalocele, bladder exstrophy, and cloacal exs-trophy [1,2]. Gastroschisis is a defect of the anterior abdominal](https://img.dokumen.tips/doc/110x75/5f82b6822991d932fc2027c1/cloacal-exstrophy-associated-with-gastroschisis-case-gastroschisis-omphalocele.jpg)