Embed Size (px)
Citation preview

1
Stjepan Gamulin Kvantitativne metode kliničkih istraživanja, zadatci za seminare, 2017 Na seminare donesite: 1. zadatke 2. otisnute članke 3. skripta S. Gamulin, Klinička istraživanja, definicije i formule 4. kalkulator (ako niste sigurni u korištenju kalkulatora na računalu) Dijagnoza 1 Keller T, Zeller T, Peetz D, Tzikas S, Roth A, Czyz E, Bickel C, Baldus S, et al. Sensitive troponin I assay in early diagnosis of acute myocardial infarction. N Engl J Med. 2009;361(9):868-77. BACKGROUND: Cardiac troponin testing is central to the diagnosis of acute myocardial infarction. We evaluated a sensitive troponin I assay for the early diagnosis and risk stratification of myocardial infarction. METHODS: In a multicenter study, we determined levels of troponin I as assessed by a sensitive assay, troponin T, and traditional myocardial necrosis markers in 1818 consecutive patients with suspected acute myocardial infarction, on admission and 3 hours and 6 hours after admission. RESULTS: For samples obtained on admission, the diagnostic accuracy was highest with the sensitive troponin I assay (area under the receiver-operating-characteristic curve [AUC], 0.96), as compared with the troponin T assay (AUC, 0.85) and traditional myocardial necrosis markers. With the use of the sensitive troponin I assay (cutoff value, 0.04 ng per milliliter) on admission, the clinical sensitivity was 90.7%, and the specificity was 90.2%. The diagnostic accuracy was virtually identical in baseline and serial samples, regardless of the time of chest-pain onset. In patients presenting within 3 hours after chest-pain onset, a single sensitive troponin I assay had a negative predictive value of 84.1% and a positive predictive value of 86.7%; these findings predicted a 30% rise in the troponin I level within 6 hours. A troponin I level of more than 0.04 ng per milliliter was independently associated with an increased risk of an adverse outcome at 30 days (hazard ratio, 1.96; 95% confidence interval, 1.27 to 3.05; P=0.003). CONCLUSIONS: The use of a sensitive assay for troponin I improves early diagnosis of acute myocardial infarction and risk stratification, regardless of the time of chest-pain onset.

2
Iz podataka u tablici 1 izračunaj dijagnostičke pokazatelje (osjetljivost, specifičnost, LR+, vjerojatnost prije i poslije testa) za troponin T i inverziju T vala za bolesnike s akutnim infarktom miokarda, te zajedničku vjerojatnost nakon testa za troponin T i inverziju T vala.

3
Dijagnoza 2 Bates SM, Kearon C, Crowther M, Linkins L, O'Donnell M, Douketis J, et. al. A diagnostic strategy involving a quantitative latex D-dimer assay reliably excludes deep venous thrombosis. Ann Intern Med. 2003;138(10):787-94. BACKGROUND: Because clinical diagnosis is inaccurate, objective testing is usually considered necessary when patients present with suspected deep venous thrombosis (DVT). OBJECTIVE: To determine whether a negative result on a quantitative latex D dimer assay eliminates the need for further investigation in patients with a low or moderate pretest probability of DVT. DESIGN: Prospective cohort study. SETTING: Three tertiary care hospitals in Canada. PATIENTS: 556 consecutive outpatients with suspected first DVT. INTERVENTION: Patients were categorized as having a low, moderate, or high pretest probability of DVT and then underwent D-dimer testing. Patients with low or moderate pretest probability and a negative D-dimer result had no further diagnostic testing and received no anticoagulant therapy. Serial compression ultrasonography was performed in all other patients. Patients who did not receive a diagnosis of DVT were followed for symptomatic venous thromboembolism. MEASUREMENTS: Objectively confirmed symptomatic venous thromboembolic events during 3 months of follow-up. RESULTS: 283 patients (51%) had low or moderate pretest probability and a negative D-dimer result. One of these patients had DVT during follow-up (negative likelihood ratio, 0.05 [CI, 0.01 to 0.23]). The negative likelihood ratio of the d -dimer test in all patients was 0.03 (CI, 0.01 to 0.16). CONCLUSION: A negative result on a quantitative latex d -dimer assay safely eliminates the need for further testing in patients with low or moderate pretest probability of DVT. Iz tablice izračunaj dijagnostičke pokazatelje za bolesnike s niskom i umjerenom te visokom pretest vjerojatnosti za DVT

4
5
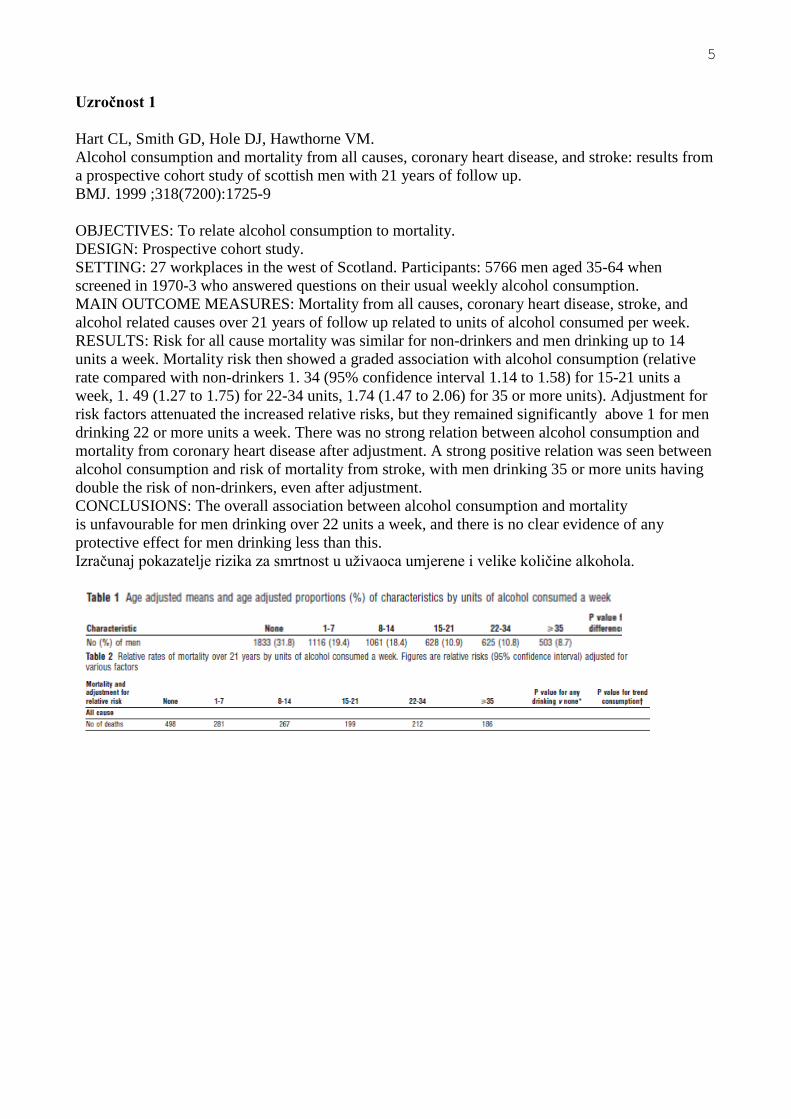
Uzročnost 1 Hart CL, Smith GD, Hole DJ, Hawthorne VM. Alcohol consumption and mortality from all causes, coronary heart disease, and stroke: results from a prospective cohort study of scottish men with 21 years of follow up. BMJ. 1999 ;318(7200):1725-9 OBJECTIVES: To relate alcohol consumption to mortality. DESIGN: Prospective cohort study. SETTING: 27 workplaces in the west of Scotland. Participants: 5766 men aged 35-64 when screened in 1970-3 who answered questions on their usual weekly alcohol consumption. MAIN OUTCOME MEASURES: Mortality from all causes, coronary heart disease, stroke, and alcohol related causes over 21 years of follow up related to units of alcohol consumed per week. RESULTS: Risk for all cause mortality was similar for non-drinkers and men drinking up to 14 units a week. Mortality risk then showed a graded association with alcohol consumption (relative rate compared with non-drinkers 1. 34 (95% confidence interval 1.14 to 1.58) for 15-21 units a week, 1. 49 (1.27 to 1.75) for 22-34 units, 1.74 (1.47 to 2.06) for 35 or more units). Adjustment for risk factors attenuated the increased relative risks, but they remained significantly above 1 for men drinking 22 or more units a week. There was no strong relation between alcohol consumption and mortality from coronary heart disease after adjustment. A strong positive relation was seen between alcohol consumption and risk of mortality from stroke, with men drinking 35 or more units having double the risk of non-drinkers, even after adjustment. CONCLUSIONS: The overall association between alcohol consumption and mortality is unfavourable for men drinking over 22 units a week, and there is no clear evidence of any protective effect for men drinking less than this. Izračunaj pokazatelje rizika za smrtnost u uživaoca umjerene i velike količine alkohola.
6
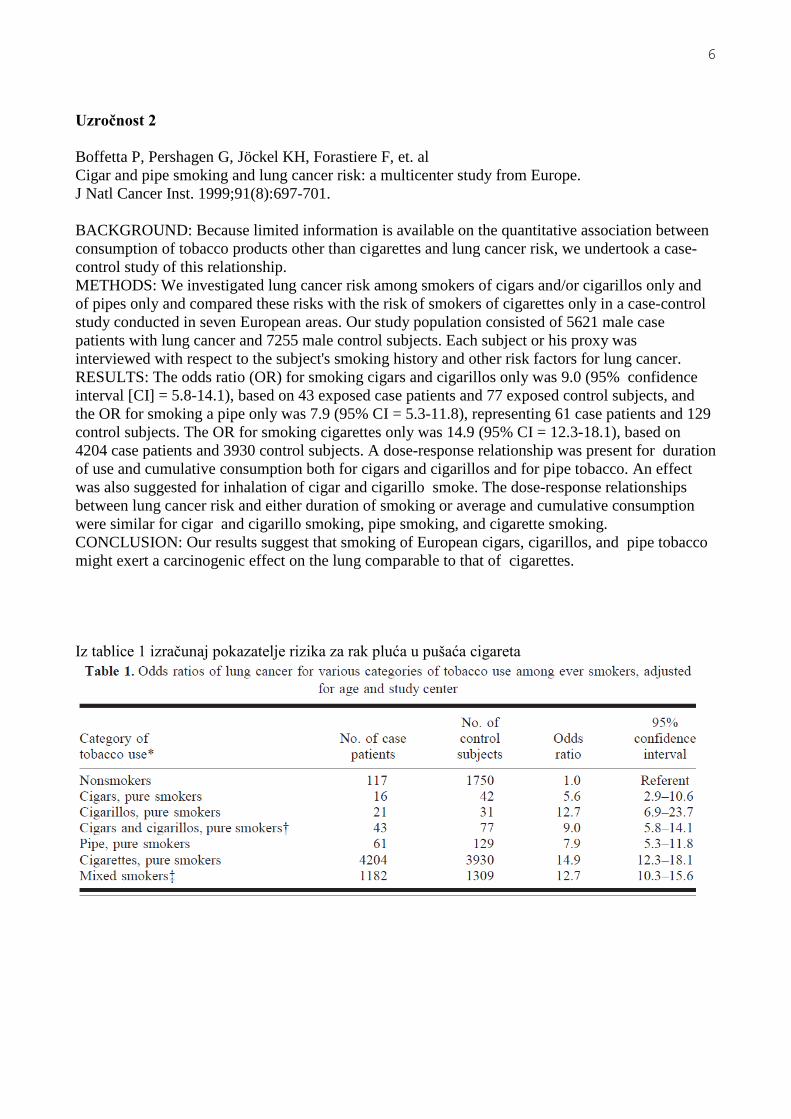
Uzročnost 2 Boffetta P, Pershagen G, Jöckel KH, Forastiere F, et. al Cigar and pipe smoking and lung cancer risk: a multicenter study from Europe. J Natl Cancer Inst. 1999;91(8):697-701. BACKGROUND: Because limited information is available on the quantitative association between consumption of tobacco products other than cigarettes and lung cancer risk, we undertook a case-control study of this relationship. METHODS: We investigated lung cancer risk among smokers of cigars and/or cigarillos only and of pipes only and compared these risks with the risk of smokers of cigarettes only in a case-control study conducted in seven European areas. Our study population consisted of 5621 male case patients with lung cancer and 7255 male control subjects. Each subject or his proxy was interviewed with respect to the subject's smoking history and other risk factors for lung cancer. RESULTS: The odds ratio (OR) for smoking cigars and cigarillos only was 9.0 (95% confidence interval [CI] = 5.8-14.1), based on 43 exposed case patients and 77 exposed control subjects, and the OR for smoking a pipe only was 7.9 (95% CI = 5.3-11.8), representing 61 case patients and 129 control subjects. The OR for smoking cigarettes only was 14.9 (95% CI = 12.3-18.1), based on 4204 case patients and 3930 control subjects. A dose-response relationship was present for duration of use and cumulative consumption both for cigars and cigarillos and for pipe tobacco. An effect was also suggested for inhalation of cigar and cigarillo smoke. The dose-response relationships between lung cancer risk and either duration of smoking or average and cumulative consumption were similar for cigar and cigarillo smoking, pipe smoking, and cigarette smoking. CONCLUSION: Our results suggest that smoking of European cigars, cigarillos, and pipe tobacco might exert a carcinogenic effect on the lung comparable to that of cigarettes. Iz tablice 1 izračunaj pokazatelje rizika za rak pluća u pušaća cigareta

7
Prognoza 1 Vanni S, Polidori G, Vergara R, Pepe G, Nazerian P, Moroni F, Garbelli E, Daviddi F, Grifoni S. Prognostic value of ECG among patients with acute pulmonary embolism and normal blood pressure. Am J Med. 2009;122(3):257-64. OBJECTIVE: To investigate the prognostic value of electrocardiography (ECG) alone or in combination with echocardiography in patients with acute pulmonary embolism and normal blood pressure. METHODS: Consecutive adult patients presenting to the emergency department at Azienda Ospedaliero-Universitaria Careggi with the first episode of pulmonary embolism were included. Patients with systolic blood pressure less than 100 mm Hg were excluded. ECG and echocardiography were performed within 1 hour from diagnosis and evaluated in a blinded fashion. Right ventricular strain was diagnosed in the presence of one or more of the following ECG findings: complete or incomplete right ventricular branch block, S1Q3T3, and negative T wave in V1-V4. The main outcome measurement was clinical deterioration or death during in-hospital stay. The association of variables with the main outcome was evaluated by multivariate Cox survival analysis. RESULTS: A total of 386 patients with proved pulmonary embolism were included in the study; 201 patients (52%) had right ventricular dysfunction according to echocardiography, and 130 patients (34%) showed right ventricular strain. Twenty-three patients (6%) had clinical deterioration or died. At multivariate survival analysis, right ventricular strain was associated with adverse outcome (hazard ratio 2.58; 95% confidence interval, 1.05-6.36) independently of echocardiographic findings. Patients with both right ventricular strain and right ventricular dysfunction (26%) showed an 8-fold elevated risk of adverse outcome (hazard ratio 8.47; 95% confidence interval, 2.43-29.47). CONCLUSION: Right ventricular strain pattern on ECG is associated with adverse short-term outcome and adds incremental prognostic value to echocardiographic evidence of right ventricular dysfunction in patients with acute pulmonary embolism and normal blood pressure. Iz tablice izračunaj prognostičke parametre za kompozitni ishod

8
Prognoza 2 van de Vijver MJ, He YD, van't Veer LJ, Dai H, Hart AA, Voskuil DW, et. al A gene-expression signature as a predictor of survival in breast cancer. N Engl J Med. 2002 ;347(25):1999-2009. BACKGROUND: A more accurate means of prognostication in breast cancer will improve the selection of patients for adjuvant systemic therapy. METHODS: Using microarray analysis to evaluate our previously established 70-gene prognosis profile, we classified a series of 295 consecutive patients with primary breast carcinomas as having a gene-expression signature associated with either a poor prognosis or a good prognosis. All patients had stage I or II breast cancer and were younger than 53 years old; 151 had lymph-node-negative disease, and 144 had lymph-node-positive disease. We evaluated the predictive power of the prognosis profile using univariable and multivariable statistical analyses. RESULTS: Among the 295 patients, 180 had a poor-prognosis signature and 115 had a good-prognosis signature, and the mean (+/-SE) overall 10-year survival rates were 54.6+/-4.4 percent and 94.5+/-2.6 percent, respectively. At 10 years, the probability of remaining free of distant metastases was 50.6+/-4.5 percent in the group with a poor-prognosis signature and 85.2+/-4.3 percent in the group with a good-prognosis signature. The estimated hazard ratio for distant metastases in the group with a poor-prognosis signature, as compared with the group with the good-prognosis signature, was 5.1 (95 percent confidence interval, 2.9 to 9.0; P<0.001). This ratio remained significant when the groups were analyzed according to lymph-node status. Multivariable Cox regression analysis showed that the prognosis profile was a strong independent factor in predicting disease outcome. CONCLUSIONS: The gene-expression profile we studied is a more powerful predictor of the outcome of disease in young patients with breast cancer than standard systems based on clinical and histologic criteria. Iz tablice izračunaj prognostičke pokazatelje za N+ bolesnice

9
Terapija 1 Fisher B, Costantino JP, Wickerham DL, Redmond CK, Kavanah M, Cronin WM, Vogel V, Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst. 1998;90(18):1371-88. BACKGROUND: The finding of a decrease in contralateral breast cancer incidence following tamoxifen administration for adjuvant therapy led to the concept that the drug might play a role in breast cancer prevention. To test this hypothesis, the National Surgical Adjuvant Breast and Bowel Project initiated the Breast Cancer Prevention Trial (P-1) in 1992. METHODS: Women (N=13388) at increased risk for breast cancer because they 1) were 60 years of age or older, 2) were 35-59 years of age with a 5-year predicted risk for breast cancer of at least 1.66%, or 3) had a history of lobular carcinoma in situ were randomly assigned to receive placebo (n=6707) or 20 mg/day tamoxifen (n=6681) for 5 years. Gail's algorithm, based on a multivariate logistic regression model using combinations of risk factors, was used to estimate the probability (risk) of occurrence of breast cancer over time. RESULTS: Tamoxifen reduced the risk of invasive breast cancer by 49% (two-sided P<.00001), with cumulative incidence through 69 months of follow-up of 43.4 versus 22.0 per 1000 women in the placebo and tamoxifen groups, respectively. The decreased risk occurred in women aged 49 years or younger (44%), 50-59 years (51%), and 60 years or older (55%); risk was also reduced in women with a history of lobular carcinoma in situ (56%) or atypical hyperplasia (86%) and in those with any category of predicted 5-year risk. Tamoxifen reduced the risk of noninvasive breast cancer by 50% (two-sided P<.002). Tamoxifen reduced the occurrence of estrogen receptor-positive tumors by 69%, but no difference in the occurrence of estrogen receptor-negative tumors was seen. Tamoxifen administration did not alter the average annual rate of ischemic heart disease; however, a reduction in hip, radius (Colles'), and spine fractures was observed. The rate of endometrial cancer was increased in the tamoxifen group (risk ratio = 2.53; 95% confidence interval = 1.35-4.97); this increased risk occurred predominantly in women aged 50 years or older. All endometrial cancers in the tamoxifen group were stage I (localized disease); no endometrial cancer deaths have occurred in this group. No liver cancers or increase in colon, rectal, ovarian, or other tumors was observed in the tamoxifen group. The rates of stroke, pulmonary embolism, and deep-vein thrombosis were elevated in the tamoxifen group; these events occurred more frequently in women aged 50 years or older. CONCLUSIONS: Tamoxifen decreases the incidence of invasive and noninvasive breast cancer. Despite side effects resulting from administration of tamoxifen, its use as a breast cancer preventive agent is appropriate in many women at increased risk for the disease.

10
Izračunaj pokazatelje koristi i štetnosti preventivne primjene tamoksifena

11
Terapija 2 Holman RR, Farmer AJ, Davies MJ, Levy JC, Darbyshire JL, Keenan JF, Paul SK; Three-year efficacy of complex insulin regimens in type 2 diabetes. N Engl J Med. 2009;361(18):1736-47 BACKGROUND: Evidence supporting the addition of specific insulin regimens to oral therapy in patients with type 2 diabetes mellitus is limited. METHODS: In this 3-year open-label, multicenter trial, we evaluated 708 patients who had suboptimal glycated hemoglobin levels while taking metformin and sulfonylurea therapy. Patients were randomly assigned to receive biphasic insulin aspart twice daily, prandial insulin aspart three times daily, or basal insulin detemir once daily (twice if required). Sulfonylurea therapy was replaced by a second type of insulin if hyperglycemia became unacceptable during the first year of the study or subsequently if glycated hemoglobin levels were more than 6.5%. Outcome measures were glycated hemoglobin levels, the proportion of patients with a glycated hemoglobin level of 6.5% or less, the rate of hypoglycemia, and weight gain. RESULTS: Median glycated hemoglobin levels were similar for patients receiving biphasic (7.1%), prandial (6.8%), and basal (6.9%) insulin-based regimens (P=0.28). However, fewer patients had a level of 6.5% or less in the biphasic group (31.9%) than in the prandial group (44.7%, P=0.006) or in the basal group (43.2%, P=0.03), with 67.7%, 73.6%, and 81.6%, respectively, taking a second type of insulin (P=0.002). [corrected] Median rates of hypoglycemia per patient per year were lowest in the basal group (1.7), higher in the biphasic group (3.0), and highest in the prandial group (5.7) (P<0.001 for the overall comparison). The mean weight gain was higher in the prandial group than in either the biphasic group or the basal group. Other adverse event rates were similar in the three groups. CONCLUSIONS: Patients who added a basal or prandial insulin-based regimen to oral therapy had better glycated hemoglobin control than patients who added a biphasic insulin-based regimen. Fewer hypoglycemic episodes and less weight gain occurred in patients adding basal insulin. Usporedi koristi (Hb1c)i stetnost (hipoglikemija) pri primjeni bazalni i prandijalni inzulinski režim u odnosu na bifazični.

12
Terapija 3 Bolland MJ, Barber PA, Doughty RN, Mason B, Horne A, et. al Vascular events in healthy older women receiving calcium supplementation: randomised controlled trial. BMJ. 2008;336(7638):262-6. OBJECTIVE: To determine the effect of calcium supplementation on myocardial infarction, stroke, and sudden death in healthy postmenopausal women. DESIGN: Randomised, placebo controlled trial. SETTING: Academic medical centre in an urban setting in New Zealand. PARTICIPANTS: 1471 postmenopausal women (mean age 74): 732 were randomised to calcium supplementation and 739 to placebo. MAIN OUTCOME MEASURES: Adverse cardiovascular events over five years: death, sudden death, myocardial infarction, angina, other chest pain, stroke, transient ischaemic attack, and a composite end point of myocardial infarction, stroke, or sudden death. RESULTS: Myocardial infarction was more commonly reported in the calcium group than in the placebo group (45 events in 31 women v 19 events in 14 women, P=0.01). The composite end point of myocardial infarction, stroke, or sudden death was also more common in the calcium group (101 events in 69 women v 54 events in 42 women, P=0.008). After adjudication myocardial infarction remained more common in the calcium group (24 events in 21 women v 10 events in 10 women, relative risk 2.12, 95% confidence interval 1.01 to 4.47). For the composite end point 61 events were verified in 51 women in the calcium group and 36 events in 35 women in the placebo group (relative risk 1.47, 0.97 to 2.23). When unreported events were added from the national database of hospital admissions in New Zealand the relative risk of myocardial infarction was 1.49 (0.86 to 2.57) and that of the composite end point was 1.21 (0.84 to 1.74). The respective rate ratios were 1.67 (95% confidence intervals 0.98 to 2.87) and 1.43 (1.01 to 2.04); event rates: placebo 16.3/1000 person years, calcium 23.3/1000 person years. For stroke (including unreported events) the relative risk was 1.37 (0.83 to 2.28) and the rate ratio was 1.45 (0.88 to 2.49). CONCLUSION: Calcium supplementation in healthy postmenopausal women is associated with upward trends in cardiovascular event rates. This potentially detrimental effect should be balanced against the likely benefits of calcium on bone. Iz tablice izračunaj pokazatelje škodljivosti kalcija za infarkt miokarda i kompozitni ishod

13
Terapija 4 van Nood E(1), Vrieze A, Nieuwdorp M, Fuentes S, et. al. Duodenal infusion of donor feces for recurrent Clostridium difficile. N Engl J Med. 2013;368(5):407-15. BACKGROUND: Recurrent Clostridium difficile infection is difficult to treat, and failure rates for antibiotic therapy are high. We studied the effect of duodenal infusion of donor feces in patients with recurrent C. difficile infection. METHODS: We randomly assigned patients to receive one of three therapies: an initial vancomycin regimen (500 mg orally four times per day for 4 days), followed by bowel lavage and subsequent infusion of a solution of donor feces through a nasoduodenal tube; a standard vancomycin regimen (500 mg orally four times per day for 14 days); or a standard vancomycin regimen with bowel lavage. The primary end point was the resolution of diarrhea associated with C. difficile infection without relapse after 10 weeks. RESULTS: The study was stopped after an interim analysis. Of 16 patients in the infusion group, 13 (81%) had resolution of C. difficile-associated diarrhea after the first infusion. The 3 remaining patients received a second infusion with feces from a different donor, with resolution in 2 patients. Resolution of C. difficile infection occurred in 4 of 13 patients (31%) receiving vancomycin alone and in 3 of 13 patients (23%) receiving vancomycin with bowel lavage (P<0.001 for both comparisons with the infusion group). No significant differences in adverse events among the three study groups were observed except for mild diarrhea and abdominal cramping in the infusion group on the infusion day. After donor-feces infusion, patients showed increased fecal bacterial diversity, similar to that in healthy donors, with an increase in Bacteroidetes species and clostridium clusters IV and XIVa and a decrease in Proteobacteria species. CONCLUSIONS: The infusion of donor feces was significantly more effective for the treatment of recurrent C. difficile infection than the use of vancomycin. Iz rezultata izračunaj učinkovitost fekalne transplantacije u odnosu na vankomicin.





























