Embed Size (px)
Citation preview
RESTLESS LEGS SYNDROME(RLS)
Symptom Derived Treatment
Philip M. Becker, M.D.
Medical Director, Sleep Medicine Institute, Presbyterian Hospital
Clinical Professor, Dept. of Psychiatry, UT Southwestern Medical Center
Dallas, Texas
Patients describe RLS in a multitude of colorful ways
A compelling sensation occurring at rest that creates URGE to move.
Described, often with difficulty or in dramatic terms, as:
"creepy, crawly, jumpy""heebie jeebies""jerky or jittery"
"ants or worms crawling inside""agitation, anxious" but just in the limbs
(unless very severe)"hurts deep inside but it isn't really pain"

IRLSSG Diagnostic CriteriaFour Core Symptoms are required
“U R G E”U = Urge to move the limb(s)
R = Rest worsens the sensation
G = Get up & Go is Good (temporary relief with movement)
E = Evening / night worsening

Current Hypothesis on Etiology
• Dopaminergic Mechanism in RLS – Success of dopaminergic therapy supposes a mechanism of
action.
– Four studies have identified small reductions (10-20%) in striatal dopamine activity.
• Iron Dysregulation in the CNS– Conner et al. found reduced iron transporter in nigral neurons of
RLS patients compared to control brains.
– Serum ferritin less than 30 increases the likelihood of improvement with iron.
– CSF ferritin reductions correlate with RLS severity.
– Iron stores in the substantia nigra of RLS patients are lower on fMRI.

Epidemiology of RLS
PrevalencePre-1970 2 - 5% (3 studies)Since 19949 - 15%(5 studies)
ProgressionOnset: 43% develop RLS before age 20Increase incidence up to age 69 (& older)In children who have parents with RLS, PLMD found more commonly than RLS.
PLMS noted in 80% of RLS patients on NPSG#1 (and +7.6% on NPSG #2).

Primary Restless Legs Syndrome presents generally before age 30.
Etiology of primary RLS is unknown.
About 50% of primary patients have a positive family history for RLS.
Genetics: • Trenkwalder: probable autosomal dominant inheritance with high penetrance and variable expressivity.• Desaulters: Chromosome 12q in French-Canadians
There must be no medical or substances to accountfor the symptoms.

Secondary RLS arises more commonly after age 30.
It arises in or from other conditions such as:
Uremia 23 - 30% report RLSPregnancy17% report RLS
Neuro Disorders: spinocerebellar ataxia, CMT 2, Small fiber neuropathy, DM, lumbar radiculopathyMetabolic Deficiency: IRON, folate, B12,
thyroid, othersRheumatoid Arthritis
Treatment focuses upon correction of the medical disorder.

Management Strategies for RLS
Behavioral InterventionsSecondary Disorders require active correction and treatment.Pharmacologic Therapies
Target Symptoms for RLS Therapy
Dysesthesia reduce to the lowest level possible throughout the 24 hours.Sleep: Normalize sleep onset, sleep maintenance, and daytime alertness.Periodic Leg Movements: Reduce to an asymptomatic level for patient and bedpartner.Timing of treatment before significant onset of symptoms.Side Effects should be minimized.
Behavior Modification for RLS
Avoid caffeine, chocolate, and MSG.Aerobic exercise, but before 7:00 p.m.Limit use of centrally active stimulant agents: Decongestants, antihistamines, nicotine, appetite suppressants, etc.Avoid SSRI anti-depressants, unless only effective treatment (Possibly better: buproprion or nefazodone).Counter stimuli: socks, stretching, hot bath or shower, ice pack, others.

Pharmacologic Treatment Experience for RLS
• Opiates 300 + years• Benzodiazepines 25 + years
• Clonazepam & others
• Levodopa 15 + years• Dopamine Agonists 5-10 years
• Ropinirole, pramipexole, others
• Anti-convulsants 5 + years• Gabapentin
• Others (iron, mg, calcium, B vitamins, magnets, etc.)
Complex RLS Case
• 54 y/o W/M man with 20+ year hx of RLS.
• Renal disease with creatinine of 2.1, stable.
• Hospitalized for major depression 4 yrs ago; currently taking fluoxetine at 40 mg/d.
• “My legs are driving me nuts. Inside they crawl and hurt. I just have to move them.”
• “I can’t live this way any longer. I would be better off dead.”
• Taking carbidopa/levodopa ER 50/200 qid for 8 months. Relief of 1-2 hours, otherwise 24-hour RLS.

Treatment Planning for WM
Did anything help you? “I slept with Percodan (taken for 3 days after dental work).
Sinemet CR “helped for 2 months and then it won’t last. I took more.”
Do you have a plan to take your life? “No, I love my kids. It wouldn’t be fair to them.”
Recheck creatinine, hemoglobin and hematocrit, B12, folate, and Ferritin. No changes were found.
WM hasAugmentation to Levodopa
• Augmentation: shift of RLS symptoms by two or more hours to an earlier onset compared to the patient’s baseline.
• Levodopa produces augmentation in 30-85% of RLS patients (Ave onset: 1-3 months).
• Dopamine agonists (DA) estimated to produce augmentation in 15-35% of patients (Onset >6 mos).
• Management Options: • For levodopa, taper off then switch to DA.• If DA, consider earlier dosing. Observe for further
augmentation.• In the severe patient, shift to high potency opiate.• Consider gabapentin, clonazepam or other therapy.
Initial Treatment Plan for WM
Taper carbidopa/levodopa ER 50/200 by one tablet every 2 days, beginning at h.s., to prevent augmentation.
To reduce augmentation, substitute ropinirole 0.25 mg for each of the c/l dopa ER tablets every 2 days.
Oxycodone 5 mg p.o. h.s. for acute symptom relief and to improve sleep.
Emphasized complexity, need for daily contact and possible need to hospitalize.
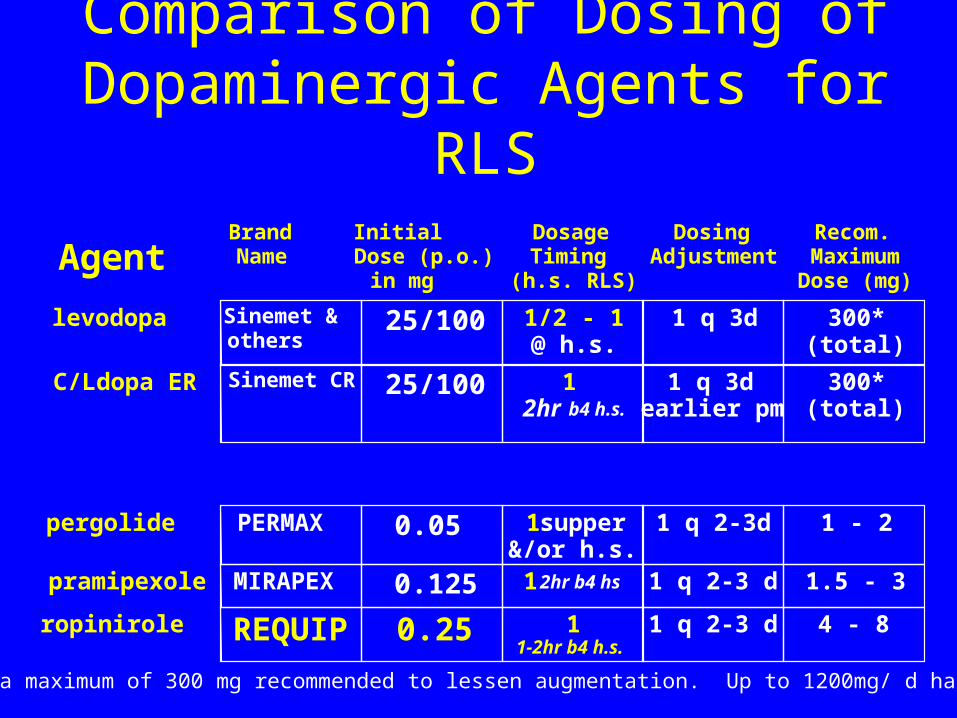
Comparison of Dosing of Dopaminergic Agents for RLS
AgentBrand Name
Initial Dose (p.o.) in mg
Dosage Timing
(h.s. RLS)
Dosing Adjustment
Recom.MaximumDose (mg)
levodopa Sinemet & others
25/100 1/2 - 1@ h.s.
1 q 3d 300*(total)
C/Ldopa ER Sinemet CR 25/100 1 2hr b4 h.s.
1 q 3d earlier pm
300*(total)
pergolide PERMAX 0.05 1 supper &/or h.s.
1 q 2-3d 1 - 2
pramipexole MIRAPEX 0.125 12hr b4 hs 1 q 2-3 d 1.5 - 3
ropinirole REQUIP 0.25 1 1-2hr b4 h.s.
1 q 2-3 d 4 - 8
*Levodopa maximum of 300 mg recommended to lessen augmentation. Up to 1200mg/ d has been used.
WM Treatment Course Day 1-10
Day 1: “I slept 5 hours.”Day 6: “The legs are 30% better, but I’m
only sleeping 4 hours or so.”Response: INCREASE ROPINIROLE
DOSES #3&4 to 0.50 mg.Day 10: “My legs are OK until about 11:00
and then they act up. The medicine makes me really sick (nauseated).”Response: Nausea should get better. (I wish
domperidone was available in U.S.) INCREASE ROPINIROLE at noon to 0.5 mg.

Limitations to Therapeutic Benefit
Side effectsDopamine agonists: nausea, edema, myalgia,
sleepiness, insomnia, augmentationOpioids: sleepiness (? SDB), insomnia,
constipation, nausea, “fear of addiction” Loss of efficacy
Consider anemia/iron deficiency.Need for dose adjustmentIs it augmentation?

WM Treatment Course Day 11-14
Day 11: “I’m sick all day. I didn’t sleep.”Response: Discontinue a.m. ropinirole.
Day 12: “You got to do something.”Response: Reduce ropinirole to 0.25 mg noon
& 6:00 pm, continue 0.5 mg at 10:00 pm.Day 14: “I’m not as sick but my legs are
worse. Is this ever going to get better?”Response: Add oxycodone 5 mg at 6:00 p.m.
(and h.s.). Reduce ropinirole to 0.25 mg TID.

WM Treatment Course Day 21-24
Day 21: “I’m 50 % better. I even slept 6 hours one night.” RL starts at about noon.Response: Increase ropinirole to 0.5 mg
with lunch.Day 24 “That stuff makes me sick. I
decreased it (back to 0.25 mg at noon). My legs were getting puffy.”Response: Checked chemistries and renal
function. No acute changes.
WM Treatment Course Day 26-35
Day 26: “Doc, I think the dope works the best. The fluid was making my legs hurt.”Response:
Stopped ropiniroleChanged oxycodone to METHADONE 5 mg at
6:00 p.m. and 10:00 p.m.
Day 35: “Doc, it’s amazing. I don’t feel my legs jumping and I slept for five nights straight.” Edema resolved.

Efficacy of Different Opioidsin Treatment of RLS in 18 Severe Patients
0
5
10
15
20
25
30
35
8.5 8.7511.17
14.31
18.43
26.67
IRLSS Rating
levorphanol pramipexole hydromorphonehydrocodone propoxyphene Base
ScoringV. Sev.=31-40Severe=21-30Mod. =11-20Mild = 1- 10

WM Treatment CourseDay 35 +
• Depression remained moderate with low energy & motivation; moderate sadness.
• WM’s personal doctor agreed to my request to discontinue Prozac.
• Wellbutrin SR 150 mg was started and increased to a.m. and noon one week later.
• Four weeks later, clonazepam 0.5 mg h.s. was added due to “feeling a bit nervous.”
• At eight weeks, he slept >6 hours nightly and said “I feel pretty good.” He has remained so for 3+ years on methadone, buproprion XL and clonazepam.
Treatment Considerationsfor Restless Legs Syndrome
• Treat symptoms identified as problems by patient.• Dopamine agonists are the first line, presuming a
ferritin > 30. Target therapy before RL onset.Target therapy before RL onset.• C/L dopa causes augmentation. Best used prn.
[Arbitrary limit:300 mg/week ( 3 tabs of 25/100)]
• Opiates restore severe patients. High potency agents preferred (methadone, levorphanol, hydromorphone) but caution for EDS and SDB.
• Gabapentin is variably effective. Best with “pain”.• Depression and anxiety are common and require
treatment when present. Buproprion preferred.