Embed Size (px)
Citation preview

Int. J. Radiation Oncology Biol. Phys., Vol. 78, No. 1, pp. 72–78, 2010Copyright � 2010 Elsevier Inc.
Printed in the USA. All rights reserved0360-3016/$–see front matter
robp.2009.07.1729
doi:10.1016/j.ijCLINICAL INVESTIGATION Brain
PROGNOSTIC FACTORS AFTER EXTRANEURAL METASTASIS OFMEDULLOBLASTOMA
ALI MAZLOOM, M.D.,* AZY H. ZANGENEH, M.P.H.,y AND ARNOLD C. PAULINO, M.D.*z
*Department of Radiology, Section of Radiation Oncology, The Methodist Hospital, Houston, Texas; yDivision of Health Promotionand Behavioral Sciences, The University of Texas School of Public Health, Houston, Texas; and zDepartment of Radiation Oncology,
The Methodist Hospital, Houston, Texas
ReprinHospital,DB1-077441-4493
Present
Purpose: To review the existing literature regarding the characteristics, prognostic factors, treatment, and survivalof patients with medulloblastoma, who develop extraneural metastasis (ENM).Methods and Materials: A PubMed search of English language articles from 1961 to 2007 was performed, yielding47 articles reporting on 119 patients. Factors analyzed included age, time interval to development of ENM, ENMlocation, central nervous system (CNS) involvement, treatment, and outcome.Results: Sites of ENM included bone in 84% of patients, bone marrow in 27% of patients, lymph nodes in 15% ofpatients, lung in 6% of patients, and liver in 6% of patients. Median survival was 8 months after diagnosis of ENM.The 1-, 2-, and 5-year overall survival (OS) rates after diagnosis of ENM were 41.9%, 31.0%, and 26.0%, respec-tively. The 1-, 2-, and 5-year progression-free survival (PFS) rates after diagnosis of ENM were 34.5%, 23.2%, and13.4%, respectively. For patients without CNS involvement at the time of ENM diagnosis, the 1-, 2-, and 5-year OSrates for those treated with and without radiotherapy (RT) were 82.4%, 64.8%, and 64.8% vs. 51.0%, 36.6%, and30.5%, respectively (p = 0.03, log-rank test). RT did not significantly improve OS or PFS rates for those with CNSinvolvement. Concurrent CNS involvement, ENM in the lung or liver, a time interval of <18 months to developmentof ENM, and a patient age of <16 years at ENM diagnosis were found to be negative prognostic factors for both OSand PFS.Conclusions: Several prognostic factors were identified for patients with ENM from medulloblastoma. Patientswithout concurrent CNS involvement, who received RTafter ENM diagnosis had an OS and PFS benefit comparedto those who did not receive RT. � 2010 Elsevier Inc.
Medulloblastoma, Extraneural, Extracranial, Metastasis, Radiotherapy.
INTRODUCTION
Medulloblastoma is the most common brain tumor in chil-
dren and accounts for 15 to 20% of cases (1). Of all the
pediatric brain tumors, medulloblastoma has one of the high-
est rates of metastasis outside the central nervous system
(CNS) (2–5), with 7 to 10% of cases developing extraneural
metastasis (ENM) (6–10). In 1936, Nelson (11) reported the
first case of medulloblastoma that had metastasized outside
of the CNS. Subsequently, a number of case series or reports
of ENM of medulloblastoma have been published (12–29).
Patients diagnosed with ENM have traditionally been treated
with different chemotherapeutic agents including vincristine,
cisplatin, carboplatin, and cyclophosphamide (4, 30); how-
ever, despite treatment, ENM has historically been associated
with a poor prognosis (30). In addition, the relative rarity of
this disease has made systematic study difficult. The purpose
of this study was to perform a comprehensive literature
t requests to: Arnold C. Paulino, M.D., The MethodistDepartment of Radiation Oncology, 6565 Fannin St.,
, Houston, TX 77030. Tel: (713)-441-4820; Fax: (713)-; E-mail: [email protected] in part at the 45th Annual Meeting of the American
72
review and analysis of reported cases to identify the charac-
teristics, prognostic factors, and survival of these patients.
METHODS AND MATERIALS
MEDLINE/PubMed searches of English language articles per-
taining to ENM from medulloblastoma were performed using
a combination of key words: extraneural, metastasis, metastatic,
extracranial, and medulloblastoma. Eligibility for inclusion in the
study included diagnosis of medulloblastoma with ENM prior to
death. Patients who were diagnosed with ENM at autopsy were ex-
cluded from this study. We found 47 articles reporting 119 patients,
published from 1961 to 2007, that met the above-described criteria
(2, 4, 6–10, 12, 20, 21, 23, 24, 26, 30–63). Articles were reviewed
carefully to ensure that the same patient was not counted more
than once in the study (47, 64). Table 1 lists the published reports,
the year of publication, and the number of cases of patients with
ENM from medulloblastoma.
Society of Clinical Oncology, Orlando, FL, May 29 – June 2, 2009.Conflict of interest: none.Received April 8, 2009, and in revised form July 8, 2009.
Accepted for publication July 16, 2009.

Table 1. Studies reporting cases of extraneural metastasisfrom medulloblastoma
Study (reference)Year of
publicationNo. ofcases
Chan et al. (39) 2000 8Miyake et al. (53) 1964 1Booher and Shmidtknecht (9) 1977 1Leo et al. (30) 1997 1Nathanson and Kovacs (54) 1978 2Krouwer et al. (46) 1991 1Lassman (47) 1976 4Donner (41) 2005 1Das and Dalby (21) 1977 3Paterson (12) 1961 7Friedman et al. (4) 1986 4Lewis et al. (10) 1973 1Bates (8) 1973 1Brutschin and Culver (36) 1973 3Rochkind et al. (6) 1991 1Stolzenberg et al. (59) 1970 1Lowery et al. (49) 1982 6Mahoney et al. (51) 1986 1Duffner and Cohen (42) 1981 2Varan et al. (2) 2006 6Wendland et al. (63) 2006 1McComb et al. (26) 1981 6Watterson et al. (62) 1993 1Black and Keats (35) 1964 3Cottu et al. (7) 1994 1Allen and Helson (33) 1981 2Millot et al. (52) 1999 2Paulino (56) 2003 7Brown et al. (20) 1977 1Raimondi and Tomita (24) 1979 3Brydon and Carey (37) 1991 1Spencer et al. (58) 1984 4Akyuz et al. (32) 1999 1Ramsay et al. (57) 1995 1Eberhart et al. (43) 2003 7Vieco et al. (61) 1989 4Bach et al. (34) 1968 1Ahmad et al. (31) 2002 1Parkinson et al. (55) 1974 2Jackson and Graham (23) 1978 1Lefkowitz et al. (48) 1990 1Corrin and Meadows (40) 1967 1Vanneste (60) 1983 1Kleinman et al. (45) 1981 2Kessler et al. (44) 1975 1Chamberlain et al. (38) 1988 7Lundberg et al. (50) 1992 1
Fig. 1. Time interval from diagnosis of primary tumor to ENM ofmedulloblastoma.
Extraneural medulloblastoma d A. MAZLOOM et al. 73
Factors analyzed for each patient included gender, age at diagno-
sis of medulloblastoma, time interval from medulloblastoma diag-
nosis to development of ENM (<18 or >18 months), involvement
of the CNS at the time of ENM, location of ENM, treatment, pro-
gression, and survival. A chi-square test was used to compare the
dichotomous and categorical variables. Estimates of progression-
free survival (PFS) and overall survival (OS) were performed using
the Kaplan-Meier method and were calculated from the time of
ENM (65). For comparisons of survival curves according to site
of metastasis, time interval to metastasis, CNS involvement at
the time of ENM, and treatment parameters, the log-rank test
was used.
RESULTS
Patient characteristicsWe identified 119 patients with ENM from medulloblas-
toma. Of these 119 patients, 63 (52.9%) patients were male
and 37 (31.1%) patients were female; the gender was not
reported for 19 (16.0%) patients. The median age at initial
diagnosis of medulloblastoma was 14 years (range, 0.33–
66 years).
Tumor characteristicsThe time interval from initial diagnosis to extraneural re-
lapse was known in 107 patients. Three (2.8%) patients had
ENM at initial diagnosis of medulloblastoma. The median
time to develop ENM was 16 months (range, 0–164 months).
The time intervals to develop ENM are displayed in Fig. 1. Ap-
proximately 80% of cases occurred by 36 months. Tissue diag-
nosis of ENM was available for 98 of 111 (88.3%) cases, where
the method of diagnosis of ENM was mentioned. In 13 (11.7%)
cases, ENM was diagnosed radiographically; in 8 of the 13
(61.5%) cases, there was concomitant CNS involvement.
The sites of ENM were available for 109 patients. Bone
was the most common site of ENM, as seen in 92 (84.4%)
cases. Of the 92 patients with bone metastasis, 22 (23.9%) pa-
tients had solitary bone involvement. ENM was found in the
bone marrow in 29 (26.9%) patients, the lymph nodes in 16
(14.7%) patients, the lung in 7 (6.4%) patients, the liver in 7
(6.4%) patients, and in other sites in 14 (12.8%) patients, in-
cluding pancreas, retroperitoneum, pleura, paranasal sinuses,
skin, oral cavity, and connective tissue. Of the 29 patients
with bone marrow involvement, 22 (75.9%) patients also
had radiographic evidence of bone metastasis.
Treatment characteristicsInformation about the treatment of ENM was available for
108 patients. Treatment regimens administered included che-
motherapy combined with radiotherapy (RT) in 20 (18%) pa-
tients, chemotherapy alone in 50 (46%) patients, and
RT alone in 18 (17%) patients. Seven patients underwent sur-
gical resection, alone in 1 (1%), followed by chemotherapy in

Fig. 2. OS for patients with extraneural relapse of medulloblastomawith (solid line) and without (dotted line) CNS involvement at thetime of extraneural relapse; p < 0.0001, log rank test.
74 I. J. Radiation Oncology d Biology d Physics Volume 78, Number 1, 2010
2 (2%), followed by RT in 3 (3%) or followed by surgery and
chemotherapy in 1 (1%). No treatment was administered in
the case of 14 (13%) patients. Of the 23 patients for whom
data were available regarding the location of RT after diagno-
sis of ENM, 19 (83%) patients received RT to sites of ENM,
while 4 (17%) patients received RT to the CNS alone. For the
19 patients who received RT to sites of ENM, 15 (78.9%)
patients received RT to bone. Survival outcome was reported
for 112 of 119 patients. The median follow-up for these
patients after the diagnosis of ENM was 7 months (range,
0–300 months). The median follow-up for surviving patients
after the diagnosis of ENM was 24 months (range, 1–300
months). At last follow-up, 16 of 119 (13.4%) patients had
no evidence of disease, 73 (61.3%) patients had died of dis-
ease, and 19 (16.0%) patients were alive with disease. The
median survival for patients with ENM from medulloblas-
toma was 8 months. The 1-, 2-, and 5-year OS rates after
the diagnosis of ENM were 41.9%, 31.0%, and 26.0%,
respectively. The 1-, 2-, and 5-year PFS rates after the diag-
nosis of ENM of medulloblastoma were 34.5%, 23.2%,
13.4%, respectively.
For the 104 patients with available data regarding the type
of treatment and survival, 40 patients underwent RT and
64 did not. The median survival times for patients who re-
ceived RT and for those who did not were 24 and 8 months,
respectively. For patients who received RT, the 1-, 2-, and
5-year OS rates were 58.3%, 44.4%, and 44.4%, respectively,
whereas for those who did not receive RT, the rates were
35.2%, 24.8%, and 12.4%, respectively (p = 0.019, log-
rank test). The 1-, 2-, and 5-year PFS rates for patients who
received RT were 47.5%, 32.1%, and 24.1%, respectively,
whereas for those who did not receive RT, the rates were
29.0%, 18.8%, and 5.2%, respectively (p = 0.025, log-rank
test). For patients who received chemotherapy, the 1-, 2-,
and 5-year OS rates were 49.3%, 33.6%, and 23.7%, respec-
tively, whereas for those who did not receive chemotherapy,
the rates were 34.5%, 30.7%, and 30.7%, respectively
(p = 0.12, log rank test). The 1-, 2-, and 5-year PFS rates for
patients who received chemotherapy were 40.9%, 25.4%,
and 8.1%, respectively, whereas for those who did not receive
chemotherapy, the rates were 26.5%, 20.6%, and 20.6%, re-
spectively (p = 0.39, log rank test). There was no statistical
difference between OS or PFS according to whether or not
the patients underwent surgery as treatment for ENM of
medulloblastoma.
CNS involvementCNS involvement was present at the time of extraneural re-
lapse in 55 of 112 (49.1%) patients with available data; CNS
involvement was not reported for 7 patients. Median survival
times for patients with and without CNS involvement at the
time of extraneural relapse of medulloblastoma were 5 and
24 months, respectively. For patients with CNS involvement,
the 1-, 2-, and 5-year OS rates were 12.8%, 9.6%, and 6.4%,
respectively, whereas for those without CNS involvement,
the rates were 64.2%, 48.2%, and 45.1%, respectively (p <
0.0001, log rank test) (Fig. 2). The 1-, 2-, and 5-year PFS
rates for those with CNS involvement were 8.2%, 6.2%,
and 0%, respectively, whereas for those without CNS in-
volvement, they were 55.4%, 36.7%, and 25.6%, respec-
tively (p < 0.0001, log rank test). For patients with CNS
involvement at the time of extraneural relapse of medullo-
blastoma, the 1-, 2-, and 5-year OS rates for patients treated
with RT were 22.8%,15.2%, and 15.2%, respectively,
whereas for those who were not treated with RT, rates were
10.0%, 10.0%, and 0%, respectively (p = 0.56, log rank
test). The 1-, 2-, and 5-year PFS rates for patients with
CNS involvement treated with RT were 17.6%, 11.8%, and
0%, whereas for those who were not treated with RT, the
rates were 4.0%, 4.0%, and 0%, respectively (p = 0.5, log
rank test). For patients without CNS involvement at the
time of extraneural relapse of medulloblastoma, the 1-, 2-,
and 5-year OS rates for patients treated with RT were
82.4%, 64.8%, and 64.8%, respectively, whereas for those
who did not receive RT, the rates were 51.0%, 36.6%, and
30.5%, respectively (p = 0.03, log rank test) (Fig. 3). The
1-, 2-, and 5-year PFS rates for patients without CNS involve-
ment who were treated with RT were 69.6%, 47.4%, and
42.7%, whereas for those who did not receive RT, the rates
were 45.5%, 29.4%, and 11.2%, respectively (p = 0.04, log
rank test). Cause of death was reported for 59 cases. For pa-
tients with concomitant CNS involvement, the CNS was the
predominant cause of death as seen in 25 of 33 (75.6%) cases.
For patients without concomitant CNS involvement at the
time of diagnosis of ENM, the predominant cause of death
was ENM as seen in 21 of 26 (80.8%) cases.
Site of ENMThe median survival for patients with ENM to the lungs or
liver was 2 months. The OS (p = 0.002, log rank test) and PFS
(p < 0.0001, log rank test) of these patients were lower than
those with ENM to other locations. A total of 75% of patients
with lung or liver involvement had CNS involvement at the

Fig. 3. OS for patients with extraneural relapse of medulloblastomaand without concurrent CNS involvement treated with (solid line[n = 23]) and without (dotted line [n = 33]) radiotherapy; p = 0.03,log rank test.
Extraneural medulloblastoma d A. MAZLOOM et al. 75
time of extraneural relapse, while only 46.7% of patients
without lung or liver ENM had CNS involvement at this
time (p = 0.065). The frequency of concomitant CNS in-
volvement in the different ENM sites is presented in Table 2.
Patient age at ENMFor the 100 patients for whom data were available regard-
ing age at the time of ENM diagnosis, 48 patients were
<16 years old, and 52 patients were $16 years old. Median
survival time for patients of <16 years at the time of extraneu-
ral relapse was 6 months, while for those who were $16 years
old, it was 22 months. For patients younger than 16 years at
the time of ENM, the 1-, 2-, and 5-year OS rates were 26.3%,
18.4%, and 15.3%, respectively, whereas for patients older
than 16 years, the rates were 56.1%, 38.1%, and 27.4%, re-
spectively (p = 0.002, log rank test). The 1-, 2-, and 5-year
PFS rates for those younger than 16 years at the time of
ENM were 21.9%, 15.4%, and 7.7%, respectively, whereas
for those who were $16 years, the rates were 44.2%,
25.5%, and 10.6%, respectively (p = 0.023, log rank test). Pa-
tients who were younger than 16 years of age had a shorter
duration to ENM development. Sixty-seven percent of those
younger than 16 years old had a duration to metastasis of <18
months, whereas 38% of those who were 16 years old or older
had a duration to metastasis of <18 months (p = 0.003).
Table 2. Frequency of concomitant CNS in
Involvement
No. of c
Bone Bone marrow
Concomitant CNS involvement 41 (44.6) 12 (41.3)No concomitant CNS involvement 46 (50.0) 13 (44.8)Unknown 5 (5.4) 4 (13.8)Total 92 (100) 29 (100)
Time interval to development of ENMFor the 100 patients for whom data were available regarding
the time interval from initial diagnosis of medulloblastoma to
ENM development and survival outcome, 53 patients had a du-
ration to relapse of <18 months, and 47 patients had a duration
to relapse of $18 months. For patients with a time interval to
ENM of <18 months the 1-, 2-, and 5-year OS rates were
25.4%, 13.4%, and 13.4, respectively, whereas for those
with a time interval to metastasis of $18 months, rates were
60.6%, 48.0%, and 34.3%, respectively (p = 0.001, log rank
test) (Fig. 4). For patients with a time interval to ENM of
<18 months, the 1-, 2-, and 5-year PFS rates were 21.6%,
9.8%, and 2.0%, respectively, whereas for those with a time
interval to metastasis of $18 months, the rates were 46.8%,
33.2%, and 15.4%, respectively (p = 0.003, log rank test). Pa-
tients with a time interval of <18 months were less likely to be
treated with RT after diagnosis of ENM (27.3%) than those
with a time interval of $18 months (45.6%, p = 0.05).
Time era of publicationPatients in articles published before 1980 were reported to
have a worse PFS (p = 0.0003) than patients in articles
published from 1980 and beyond. There were no differences
in OS rates (p = 0.14). The 5-year OS and PFS rates for pa-
tients reported in articles published prior to 1980 were
11.6% and 2.7%, while the rates were 32.2% and 19.0%, re-
spectively, for patients reported in articles published from
1980 and beyond.
DISCUSSION
Medulloblastoma is a highly malignant tumor that has
been reported to spread both within and outside the CNS.
Liwnicz and Rubinstein (66) reported that glioblastomas
are the most common CNS tumors to spread extraneurally,
but as a proportion of their primary tumor, medulloblastomas
are the most likely to have ENM. Despite the propensity for
extraneural spread, the majority of reports in the literature are
limited to case reports or series, and to our knowledge, very
limited data exist for the prognosis of patients with ENM
from medulloblastoma. We therefore conducted the current
review in order to compile the existing literature data on
this topic and to help determine the prognostic factors and
treatment modalities that affect the outcome of patients
with ENM from medulloblastoma.
In our review of the literature, we concur with previous re-
ports that medulloblastoma patients who develop ENM have
volvement according to site of ENM
ases (% of total) with CNS involvement at:
Lung Liver Lymph nodes Other sites
5 (71.4) 6 (85.7) 6 (37.5) 9 (62.5)2 (28.6) 1 (14.3) 10 (62.5) 5 (37.5)0 (0) 0 (0) 0 (0) 0 (0)7 (100) 7 (100) 16 (100) 14 (100)
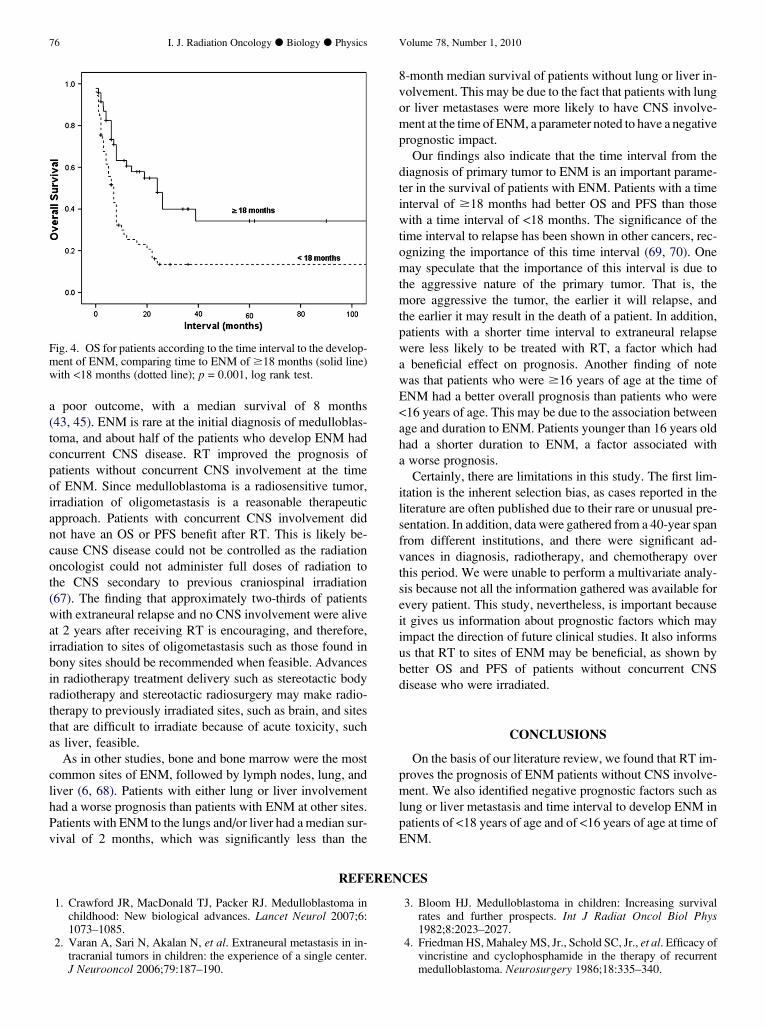
Fig. 4. OS for patients according to the time interval to the develop-ment of ENM, comparing time to ENM of $18 months (solid line)with <18 months (dotted line); p = 0.001, log rank test.
76 I. J. Radiation Oncology d Biology d Physics Volume 78, Number 1, 2010
a poor outcome, with a median survival of 8 months
(43, 45). ENM is rare at the initial diagnosis of medulloblas-
toma, and about half of the patients who develop ENM had
concurrent CNS disease. RT improved the prognosis of
patients without concurrent CNS involvement at the time
of ENM. Since medulloblastoma is a radiosensitive tumor,
irradiation of oligometastasis is a reasonable therapeutic
approach. Patients with concurrent CNS involvement did
not have an OS or PFS benefit after RT. This is likely be-
cause CNS disease could not be controlled as the radiation
oncologist could not administer full doses of radiation to
the CNS secondary to previous craniospinal irradiation
(67). The finding that approximately two-thirds of patients
with extraneural relapse and no CNS involvement were alive
at 2 years after receiving RT is encouraging, and therefore,
irradiation to sites of oligometastasis such as those found in
bony sites should be recommended when feasible. Advances
in radiotherapy treatment delivery such as stereotactic body
radiotherapy and stereotactic radiosurgery may make radio-
therapy to previously irradiated sites, such as brain, and sites
that are difficult to irradiate because of acute toxicity, such
as liver, feasible.
As in other studies, bone and bone marrow were the most
common sites of ENM, followed by lymph nodes, lung, and
liver (6, 68). Patients with either lung or liver involvement
had a worse prognosis than patients with ENM at other sites.
Patients with ENM to the lungs and/or liver had a median sur-
vival of 2 months, which was significantly less than the
8-month median survival of patients without lung or liver in-
volvement. This may be due to the fact that patients with lung
or liver metastases were more likely to have CNS involve-
ment at the time of ENM, a parameter noted to have a negative
prognostic impact.
Our findings also indicate that the time interval from the
diagnosis of primary tumor to ENM is an important parame-
ter in the survival of patients with ENM. Patients with a time
interval of $18 months had better OS and PFS than those
with a time interval of <18 months. The significance of the
time interval to relapse has been shown in other cancers, rec-
ognizing the importance of this time interval (69, 70). One
may speculate that the importance of this interval is due to
the aggressive nature of the primary tumor. That is, the
more aggressive the tumor, the earlier it will relapse, and
the earlier it may result in the death of a patient. In addition,
patients with a shorter time interval to extraneural relapse
were less likely to be treated with RT, a factor which had
a beneficial effect on prognosis. Another finding of note
was that patients who were $16 years of age at the time of
ENM had a better overall prognosis than patients who were
<16 years of age. This may be due to the association between
age and duration to ENM. Patients younger than 16 years old
had a shorter duration to ENM, a factor associated with
a worse prognosis.
Certainly, there are limitations in this study. The first lim-
itation is the inherent selection bias, as cases reported in the
literature are often published due to their rare or unusual pre-
sentation. In addition, data were gathered from a 40-year span
from different institutions, and there were significant ad-
vances in diagnosis, radiotherapy, and chemotherapy over
this period. We were unable to perform a multivariate analy-
sis because not all the information gathered was available for
every patient. This study, nevertheless, is important because
it gives us information about prognostic factors which may
impact the direction of future clinical studies. It also informs
us that RT to sites of ENM may be beneficial, as shown by
better OS and PFS of patients without concurrent CNS
disease who were irradiated.
CONCLUSIONS
On the basis of our literature review, we found that RT im-
proves the prognosis of ENM patients without CNS involve-
ment. We also identified negative prognostic factors such as
lung or liver metastasis and time interval to develop ENM in
patients of <18 years of age and of <16 years of age at time of
ENM.
REFERENCES
1. Crawford JR, MacDonald TJ, Packer RJ. Medulloblastoma inchildhood: New biological advances. Lancet Neurol 2007;6:1073–1085.
2. Varan A, Sari N, Akalan N, et al. Extraneural metastasis in in-tracranial tumors in children: the experience of a single center.J Neurooncol 2006;79:187–190.
3. Bloom HJ. Medulloblastoma in children: Increasing survivalrates and further prospects. Int J Radiat Oncol Biol Phys1982;8:2023–2027.
4. Friedman HS, Mahaley MS, Jr., Schold SC, Jr., et al. Efficacy ofvincristine and cyclophosphamide in the therapy of recurrentmedulloblastoma. Neurosurgery 1986;18:335–340.

Extraneural medulloblastoma d A. MAZLOOM et al. 77
5. Friedman HS, Schold SC, Jr., Rational approaches to the che-motherapy of medulloblastoma. Neurol Clin 1985;3:843–853.
6. Rochkind S, Blatt I, Sadeh M, et al. Extracranial metastases ofmedulloblastoma in adults: Literature review. J Neurol Neuro-surg Psychiatry 1991;54:80–86.
7. Cottu PH, Giacchetti S, Mignot L, et al. High dose chemother-apy with stem-cell transplantation in a metastatic medulloblas-toma in an adult: A case report and review of the literature. JNeurooncol 1994;18:19–23.
8. Bates T. Extracranial metastases from a cerebellar medulloblas-toma. Proc R Soc Med 1973;66:652–654.
9. Booher KR, Jr., Schmidtknecht TM. Cerebellar medulloblas-toma with skeletal metastases: Case report and review of the lit-erature. J Bone Joint Surg Am 1977;59:684–686.
10. Lewis MB, Nunes LB, Powell DE, et al. Extra-axial spread ofmedulloblastoma. Cancer 1973;31:1287–1297.
11. Nelson A. Metastases of intracranial tumor. American Journalof Cancer 1936;28:1–12.
12. Paterson E. Distant metastases from medulloblastoma of thecerebellum. Brain 1961;84:301–309.
13. Friborsky V. Medulloblastoma of the cerebellum. Extracranialmetastases and diagnostical difficulties. Neoplasma 1963;10:427–440.
14. Dexter D, Howell DA. Medulloblastomas and arachnoidal sar-comas. Brain 1965;88:367–374.
15. Bloom HJ, Wallace EN, Henk JM. The treatment and prognosisof medulloblastoma in children. A study of 82 verified cases.Am J Roentgenol Radium Ther Nucl Med 1969;105:43–62.
16. Aron BS. Twenty years’ experience with radiation therapy ofmedulloblastoma. Am J Roentgenol Radium Ther Nucl Med1969;105:37–42.
17. Chatty EM, Earle KM. Medulloblastoma. A report of 201 caseswith emphasis on the relationship of histologic variants to sur-vival. Cancer 1971;28:977–983.
18. Smith CE, Long DM, Jones TK, Jr., et al. Experiences in treat-ing medulloblastoma at the University of Minnesota hospitals.Radiology 1973;109:179–182.
19. Hoffman HJ, Hendrick EB, Humphreys RP. Metastasis via ven-triculoperitoneal shunt in patients with medulloblastoma. J Neu-rosurg 1976;44:562–566.
20. Brown RC, Gunderson L, Plenk HP. Medulloblastoma. A re-view of the LDS hospital experience. Cancer 1977;40:56–60.
21. Das S, Dalby JE. Distant metastases from medulloblastoma.Acta Radiol Ther Phys Biol 1977;16:117–123.
22. Schnitzler ER, Richards MJ, Chun RW. Cerebellar medullo-blastoma. An analysis of four cases of extraneural metastasis.Am J Dis Child 1978;132:1004–1008.
23. Jackson AM, Graham DI. Remote metastases from intracranialtumours. J Clin Pathol 1978;31:794–802.
24. Raimondi AJ, Tomita T. Medulloblastoma in childhood. ActaNeurochir (Wien) 1979;50:127–138.
25. Paillas JE, Hassoun J, Torres-Garcia P, et al. Adult medulloblas-tomas. Clinical, anatomical and therapeutic study of seventeencases (J.E. Paillas, trans). Arch Anat Cytol Pathol 1979;27:78–84.
26. McComb JG, Davis RL, Isaacs H, Jr., Extraneural metastaticmedulloblastoma during childhood. Neurosurgery 1981;9:548–551.
27. Campbell AN, Chan HS, Becker LE, et al. Extracranial metas-tases in childhood primary intracranial tumors. A report of 21cases and review of the literature. Cancer 1984;53:974–981.
28. Kasantikul V, Shuangshoti S. Cerebellar medulloblastomas: Astudy of 35 cases with particular reference to cellular differenti-ation. Surg Neurol 1986;26:532–541.
29. Farwell JR, Flannery JT. Adult occurrence of medulloblastoma.Acta Neurochir (Wien) 1987;86:1–5.
30. Leo E, Schlegel PG, Lindemann A. Chemotherapeutic induc-tion of long-term remission in metastatic medulloblastoma.J Neurooncol 1997;32:149–154.
31. Ahmad S, Roberts GJ, Lucas VS, et al. Metastatic infiltration ofthe dental pulp by medulloblastoma. J Oral Pathol Med 2002;31:244–245.
32. Akyuz C, Yalcin B, Kutluk T, et al. Brief report: Medulloblas-toma with widespread skeletal metastases presenting with hy-percalcemia. Med Pediatr Oncol 1999;33:126–128.
33. Allen JC, Helson L. High-dose cyclophosphamide chemother-apy for recurrent CNS tumors in children. J Neurosurg 1981;55:749–756.
34. Bach M, Simpson WJ, Platts ME. Metastatic cerebellar sarcoma(desmoplastic medulloblastoma) with diffuse osteosclerosis andleukoerythroblastic anemia. Am J Roentgenol Radium TherNucl Med 1968;103:38–43.
35. Black SP, Keats TE. Generalized osteosclerosis secondary tometastatic medulloblastoma of the cerebellum. Radiology1964;82:395–400.
36. Brutschin P, Culver GJ. Extracranial metastases from medullo-blastomas. Radiology 1973;107:359–362.
37. Brydon HL, Carey MP. Medulloblastoma metastasizing toa breast fibroadenoma: A case report. Br J Neurosurg 1991;5:73–75.
38. Chamberlain MC, Silver P, Edwards MS, et al. Treatment of ex-traneural metastatic medulloblastoma with a combination of cy-clophosphamide, adriamycin, and vincristine. Neurosurgery1988;23:476–479.
39. Chan AW, Tarbell NJ, Black PM, et al. Adult medulloblastoma:Prognostic factors and patterns of relapse. Neurosurgery 2000;47:623–631.
40. Corrin B, Meadows JC. Skeletal metastases from cerebellar me-dulloblastoma. Br Med J 1967;2:485–486.
41. Donner LR. Differentiation of classic medulloblastoma intometastatic large cell medulloblastoma with focal rhabdoid dif-ferentiation in the absence of posterior fossa recurrence. ActaNeuropathol 2005;109:543–551.
42. Duffner PK, Cohen ME. Extraneural metastases in childhoodbrain tumors. Ann Neurol 1981;10:261–265.
43. Eberhart CG, Cohen KJ, Tihan T, et al. Medulloblastomas withsystemic metastases: evaluation of tumor histopathology andclinical behavior in 23 patients. J Pediatr Hematol Oncol2003;25:198–203.
44. Kessler LA, Dugan P, Concannon JP. Systemic metastases ofmedulloblastoma promoted by shunting. Surg Neurol 1975;3:147–152.
45. Kleinman GM, Hochberg FH, Richardson EP, Jr., Systemic me-tastases from medulloblastoma: Report of two cases and reviewof the literature. Cancer 1981;48:2296–2309.
46. Krouwer HG, Vollmerhausen J, White J, et al. Desmoplasticmedulloblastoma metastatic to the pancreas: Case report. Neu-rosurgery 1991;29:612–616.
47. Lassman LP. Diagnosis and management of skeletal metastasesfrom cerebellar medulloblastoma. Childs Brain 1976;2:38–45.
48. Lefkowitz IB, Packer RJ, Siegel KR, et al. Results of treatmentof children with recurrent medulloblastoma/primitive neuroec-todermal tumors with lomustine, cisplatin, and vincristine. Can-cer 1990;65:412–417.
49. Lowery GS, Kimball JC, Patterson RB, et al. Extraneural metas-tases from cerebellar medulloblastoma. Am J Pediatr HematolOncol 1982;4:259–262.
50. Lundberg JH, Weissman DE, Beatty PA, et al. Treatment of re-current metastatic medulloblastoma with intensive chemother-apy and allogeneic bone marrow transplantation. J Neurooncol1992;13:151–155.
51. Mahoney DH, Jr., Steuber CP, Sandbach JF, et al. Extraneuralmetastases from medulloblastoma: Long-term survival aftersequentially scheduled chemotherapy and radiotherapy. MedPediatr Oncol 1986;14:329–331.
52. Millot F, Delval O, Giraud C, et al. High-dose chemotherapywith hematopoietic stem cell transplantation in adults with

78 I. J. Radiation Oncology d Biology d Physics Volume 78, Number 1, 2010
bone marrow relapse of medulloblastoma: report of two cases.Bone Marrow Transplant 1999;24:1347–1349.
53. Miyake S, Toyama M, Etani B, et al. Cerebellar medulloblas-toma with postoperative extracranial spread: Report of a case.J Neurosurg 1964;21:416–418.
54. Nathanson L, Kovacs SG. Chemotherapeutic response in meta-static medulloblastoma: Report of two cases and a review of theliterature. Med Pediatr Oncol 1978;4:105–110.
55. Parkinson D, Ross RT, Shields CB. Metastatic medulloblas-toma. Can J Neurol Sci 1974;1:253–254.
56. Paulino AC. Long-term survival in a child with extraneural me-tastasis from medulloblastoma treated with chemo-radiother-apy. Med Pediatr Oncol 2003;40:396–397.
57. Ramsay DA, Bonnin J, MacDonald DR, et al. Medulloblasto-mas in late middle age and the elderly: Report of 2 cases. ClinNeuropathol 1995;14:337–342.
58. Spencer CD, Weiss RB, Van Eys J, et al. Medulloblastoma met-astatic to the marrow. Report of four cases and review of the lit-erature. J Neurooncol 1984;2:223–235.
59. Stolzenberg J, Fischer JJ, Kligerman MM. Extradural metastasisin medulloblastoma 10 years after treatment. Report of a case.Am J Roentgenol Radium Ther Nucl Med 1970;108:71–74.
60. Vanneste JA. Subacute bilateral malignant exophthalmos due toorbital medulloblastoma metastases. Arch Neurol 1983;40:441–443.
61. Vieco PT, Azouz EM, Hoeffel JC. Metastases to bone in medul-loblastoma. A report of five cases. Skeletal Radiol 1989;18:445–449.
62. Watterson J, Simonton SC, Rorke LB, et al. Fatal brain stem ne-crosis after standard posterior fossa radiation and aggressivechemotherapy for metastatic medulloblastoma. Cancer 1993;71:4111–4117.
63. Wendland MM, Shrieve DC, Watson GA, et al. Extraneuralmetastatic medulloblastoma in an adult. J Am Stat Assoc2006;78:191–196.
64. Lassman LP, Pearce GW, Banna M, et al. Vincristine sulphatein the treatment of skeletal metastases from cerebellar medullo-blastoma. J Neurosurg 1969;30:42–49.
65. Kaplan EL, Meier P. Nonparametric estimation from incom-plete observations. J Am Stat Assoc 1958;54:457–481.
66. Liwnicz BH, Rubinstein LJ. The pathways of extraneural spreadin metastasizing gliomas: A report of three cases and critical re-view of the literature. Hum Pathol 1979;10:453–467.
67. Karajannis M, Allen JC, Newcomb EW. Treatment of pediatricbrain tumors. J Cell Physiol 2008;217:584–589.
68. Barai S, Bandopadhayaya GP, Julka PK, et al. Cerebellar me-dulloblastoma presenting with skeletal metastasis. J PostgradMed 2004;50:110–112.
69. Grundy P, Breslow N, Green DM, et al. Prognostic factors forchildren with recurrent Wilms’ tumor: Results from the Secondand Third National Wilms’ Tumor Study. J Clin Oncol 1989;7:638–647.
70. Leavey PJ, Mascarenhas L, Marina N, et al. Prognostic factorsfor patients with Ewing sarcoma (EWS) at first recurrence fol-lowing multi-modality therapy: A report from the Children’sOncology Group. Pediatr Blood Cancer 2008;51:334–338.





![Spinal Metastasis of Medulloblastoma in Adults: A Case Report · 2015. 1. 6. · systemic metastasis [1]. Our patient had neither tumor recurrence in the posterior fossa nor systemic](https://img.dokumen.tips/doc/110x75/5fda06f185061512a942751d/spinal-metastasis-of-medulloblastoma-in-adults-a-case-2015-1-6-systemic-metastasis.jpg)