Embed Size (px)
Citation preview

3/20/2019
1
ONH Grand Rounds
Differential Diagnosis of ONH “Edema”
Beth A. Steele, OD, [email protected]
Disclosures – Dr. Beth Steele
Company Position Received
Optos Advisory Board Honorarium
Med Op Consultant Honorarium

3/20/2019
2
Some things make you look twice….
Worrisome findings….
• Elevation
• Pallor
• Discoloration
• NFL defects
• Vascular changes
Tools you have…
• Stereoscopic DFE!• Swinging flashlight test• Pupil cycle time
• Red‐free filter• SVP• VF• OCT• FAF• B‐scan
Fundus Autofluorescence
• Drusen ‐ Hyper AF
• Buried – harder to visualize
Optos.com

3/20/2019
3
DeepSuperficial
OD‐pallor
OS‐healthy
OCT‐Angiography

3/20/2019
4
9

3/20/2019
5
Causes of disc edema …
Unilateral• Vascular
• Infectious
• Diabetic Papillopathy Bilateral • Hypertensive• Toxic• Inflammatory
• Infectious• Compressive
• Hydrocephalus • IICHtn
Optic Neuritis: Most likely etiology based on age
15-19 years Post infectious (idiopathic)
20-40 years Demyelinating disease (MS)
45-55 years Non-inflammatory/
Non-Arteritic ION
50-60 years Toxic amblyopia
60+ Inflammatory/Arteritic ION
(i.e. Giant Cell Arteritis)Amos JF. Diagnosis and Management in Vision Care. 1987.

3/20/2019
6
Is it…? And if so then why is it?
Pseudopapilledema• ONH drusen
• Anatomically crowded discs
• Hyperopic disc
• Myopic / tilted / obliquely inserted disc
Myopic / tilted discs? Be careful not to hide behind a comfortable label…

3/20/2019
7
Spectral Domain OCT Clinical Tool
Papilledema Buried ONH DrusenAnatomically Crowded Disc
Topography Smooth, continuous elevation
Non‐uniform elevation Smooth, continuous elevation
RNFL scan Thicker RNFL, especially nasalSub‐retinal cavitation
Increased in acutely damaged tissue, may be decreased over time
Normal
Globeconvexity
Flattened / pushed forward
Normal/concave Normal/increasedconcavity for hyperopes

3/20/2019
8
Key features disc edema on OCT:• Smooth contour of elevation• Nasal RNFL >86um – 80% specificity• Thick hyporeflective space adjacent to disc
“lazy V” (esp nasally) – 90% specificity Johnson L. Archives of Ophth 2009.

3/20/2019
9
Or is that old news, and imaging artifact?
• EDI superior to AF… Loft et al. J Neurophthalmology 2018.
3/20/2019
10
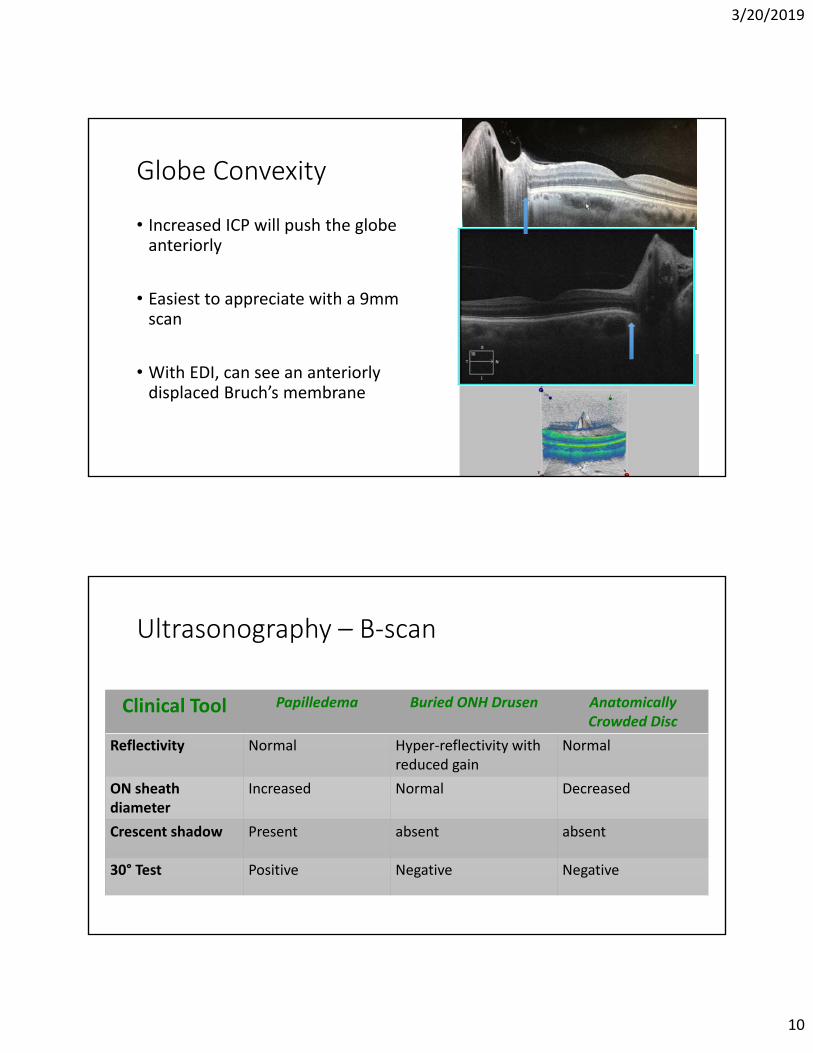
Globe Convexity
• Increased ICP will push the globe anteriorly
• Easiest to appreciate with a 9mm scan
• With EDI, can see an anteriorly displaced Bruch’s membrane
Ultrasonography – B‐scan
Clinical Tool Papilledema Buried ONH Drusen Anatomically Crowded Disc
Reflectivity Normal Hyper‐reflectivity withreduced gain
Normal
ON sheath diameter
Increased Normal Decreased
Crescent shadow Present absent absent
30° Test Positive Negative Negative

3/20/2019
11
B‐scan Ultrasonography –Review of Tools
1. ONH Sheath Diameter <5mm
2. Elevation of ONH <1mm
3. Crescent sign
4. 30 degree test • (+) when >15% ↓ in nerve sheath width following a 30‐degree eccentric gaze
• highly sensitive (100%) but non‐specific (36.4%)
Kimberly HH, et al. Acad Emerg Med. 2008.
• 20/15
• 140/90
• DFE: drance hemeOD and disc elevated nasally
43 AA Female

3/20/2019
12

3/20/2019
13
Recommendations from the ODD Consortium
• Radial ONH scans with EDI• RNFL scans (no EDI)• FAF
• Located above lamina
• Signal poor core, with superficial hyperreflectivity
• Often conglomeratesMalmqvist et al. Optic Disc ConsortiomRecommendations for Diagnosis of ODD using OCT. Neuro‐Opthalmology 2017.
24 WM

3/20/2019
14

3/20/2019
15

3/20/2019
16
Optic Disc Drusen –review and new…
• Up to 2.4% of population• Hereditary component
• 75% bilateral• Benign?
Auw‐Haedrich C, et al. Surv Ophthalmol 2002 Malmqvist L et al. J NeuroophthalmolMarch, 2016. Duncan, et al. J AAOPS, Feb, 2016. Hamann et al. Acta Ophth 2018.
Chan et al. Clin and ExpOphth July 2018.
Retrobulbar axonal degeneration due to drusen!
At what point do you lower IOP in patient with drusen?
• 71 year old with longstanding ONH drusen
• Progressive VF loss OD>OS
• IOP averages 21mmHg OU

3/20/2019
17
Decrease in IOP : • ↑of retinal ganglion cell function • Stabilizes RNFL thickness • May delay the progression of optic neuropathy
Podja‐Wilczek et al. Ophthalmic Res, 2017.

3/20/2019
18
34 WF
• 20/20, pupils normal, CF normal
• ‐7.00 OU
• BMI 31
• Denies H/A
• Elevated ONH• .1/.1 CD• +SVP
• Normal RNFL thickness
• No subretinal cavitation (but…??)

3/20/2019
19
Globe convexity is normal
Vs…
Measuring the ONH Sheath Diameter
• Axial images of the optic nerve (V and H)• 3 mm behind the posterior eye wall

3/20/2019
20
In summary…
• (‐) hyperreflectivity consistent with drusen
• (‐) crescent sign• Normal ONH sheath diameter • Normal RNFL thickness• +SVP• Normal globe convexity• Stability….
• Presumed crowded discs but careful follow up
32 AA FMSevere headaches, BMI 42

3/20/2019
21
Papilledema Suspected ? Now what…
• Brain Imaging • MRI – rule out space occupying mass • MRV – rule out cerebral venous thrombosis
• Lumbar Puncture • With opening pressure • Higher than 25/30 cm H2O is abnormal
• Referral? • Determine underlying cause/association if any
• Weight • Associated medications

3/20/2019
22
MRI features
• Order with/without contrast, T1/T2‐weighted, with fat suppression
• Empty sella
• Enlarged ON sheath
• Increased tortuosity of ON
• Flattened sclera
• Anterior protrusion of ONH
• Attenuation of cerebrovenous sinuses
MRI normal
This patient: opening pressure = 28cm H20

3/20/2019
23
Idiopathic Intracranial HTN
• 90‐98% complain of headache
• Nausea/vomiting/dizziness – 40%
• Pulsatile tinnitus – 16‐60% • Visual disturbances – 30% • No other neurologic findings (some with VIth palsy)
Mollan SP, et al. Pract Neurol 2018
IIHT – Who Gets It?
• BMI >30• >40 – worse visual outcome• Rapid weight gain – more severe
• Mostly females• Males 10% of the time • Not as likely to have H/A – may not come in
• Race – more aggressive in AA• 3 x more likely to have vision loss• 5 x increase in blindness
• Co‐morbidities • HTN• Sleep apnea
Biousse V et al. Am J Oph 2007, 2012.

3/20/2019
24
Etiologies
• Idiopathic But what causes the papilledema ?
Axoplasmic flow stasis → swollen nerve fibers → compression of venulesin the area and so venous stasis/leakage → accumula on of extracellular fluid
Associated Medications
Oral contraceptives
Steroids
Tamoxifen
Vitamin A
Nitrofurantoin
Tetracyclines
IIH Treatment Trial – JAMA, April 2014
• acetazolamide + a low‐sodium weight‐reduction diet vs. diet alone → modest improvement in visual field function
• OCT Substudy of the IITT, Ophthalmology, Sept 2015 • RNFL and Total Retinal Thickness (TRT) useful in following and monitoring response to treatment
• Better RNFL thickness, TRT, and ONH volume swelling measurements

3/20/2019
25
Acetazolamide + Low Sodium/Wt Loss Diet
• Contraindications: • Sulfa allergy?
• chemical structure different than antibiotics – little evidence of cross‐sensitivity
• consider avoiding if hx of severe reaction
• Long‐term: liver, kidney disease, severe COPD• Caution with sickle cell• Caution with low potassium
Common Side Effects
paresthesia metallic tastefatiguemalaiseGI disturbancesdecreased libido
metabolic acidosiselectrolyte imbalance (including hypokalemia)renal calculiblood dyscrasias
Than T, Smith H. http://www.reviewofoptometry.com/ce/10‐must‐have‐oral‐meds.
125,250mg tablets, and 500mg SR capsules (Diamox Sequels, DuramedPharmaceuticals)
The Idiopathic Intracranial Hypertension Treatment Trial. JAMA 2014
Treatment Goals …
• Visual Fields – for life
• OCT
• Labs ?
• Co‐management ?
Mollan SP, et al. Pract Neurol 2018Cello KE J Neuroophth 2016

3/20/2019
26
Following Tx Diamox 250mg BID… x 2 years

3/20/2019
27
34 year old Caucasian FM
• (+) H/A
• BMI 34
• Meds – Mirena IUD
• MRI – empty sella, flattened sclera, distended ONH sheaths

3/20/2019
28
• hgh
31 AAF “nasal margins mildly indistinct; RTC x 1 week for further evaluation”

3/20/2019
29
Early on – can appear as a nasal “C‐shaped” edema
• Temporal area spared
• VA often normal
6 years later….

3/20/2019
30
Those tools can miss subtle elevation….. 3 years earlier was consistent with anatomical elevation; then lost to f/u x 3 years
…3 years later patient decides to come back
• 21 AAF
• High BMI
• MRI clear
• Initial opening pressure of 52

3/20/2019
31
After 1 month of 250mg Diamox BIDstill (+) H/A

3/20/2019
32
2 mos, then 5 mos(now TID Diamox)Denies H/A
Watching VF carefully…
• H/A’s improved
• RNFL thickness reduced
• Total volume reduced

3/20/2019
33
And now… • Extracellular edema leads to venous stasis…
Other treatment options….
• Surgical – controversial and provider‐dependent • Ventricular‐peritoneal shunt • Optic nerve sheath fenestration
• Repeated lumbar puncture ? • Not well reported • Procedure ‐ causes anxiety, local discomfort, complications, headache • LP‐induced reduction of ICP is only short‐lived
• On the horizon • Topamax – off label • Bariatric surgery – in trials

3/20/2019
34
4:30 on a Friday…. • 41 year old male –has never had an eye exam
• LPE: 11 years ago• No medications• BMI 38• C/o: severe headache and blurred vision x 2 weeks
• BCVA: 20/30, 20/60 • Pupils: appeared normal • CFs: reduced OD, OS• EOM: normal • ‐SVP
Large meningioma at base of skull

3/20/2019
35
Pre/post‐surgical RNFL scans
• Can drive decisions for surgery (i.e. urgency)• ↓ing: become permanent
• Stable: may wait even if VF shows loss
• Comparison of pre‐ vs. post‐ surgical scans in neuro cases • Meningioma can grow back, so useful for monitoring progression
26 WF, “blurry vision”Hx hydracephalous, multiple previous surgeriesVA 20/40 OD, OSH/A developing with more intensity ‐SVPBMI 42
MRI “all clear”…. ICP was borderline

3/20/2019
36
67 AA F, Unexplained Pallor; 20/40 OD, OS
Optic Neuritis: Most likely etiology based on age
15-19 years Post infectious (idiopathic)
20-40 years Demyelinating disease (MS)
45-55 years Non-inflammatory/
Non-Arteritic ION
50-60 years Toxic amblyopia
60+ Inflammatory/Arteritic ION
(i.e. Giant Cell Arteritis)Amos JF. Diagnosis and Management in Vision Care. 1987.

3/20/2019
37

3/20/2019
38
Optic Neuritis in MS
• Autopsy studies – up to 99%• Often presenting sign—up to 30%
• Up to 70% develop ON throughout disease course
• 92% have eye pain
• VEP – even without VA loss ( amp, latency)
• Contrast sensitivity•OCT
• Earlier detection, often subclinical findings
Sakai, et al. J Neuroophthalmology, 2011

3/20/2019
39
OCT Findings
• Acute: thickening of inner retinal layers
• Atrophy• ≤2mos thinning
• 10–40 μm of RNFL loss within 3–6 months
• Disease activity: rate of GCL thinning
Sakai, et al. J Neuroophthalmology, 2011Behbahani R. J Neurological Sciences 2015

![Poster Q1-2020 (x) - De Groote Heide · 2020. 1. 13. · (onh zrhqvgdjdyrqg .lhqhq %rqwh 2v %xgho (onh zhnhq rs grqghugdj2shqvwhoolqj +hhpndphu 6fkhshqkxlv %xgho (onh oddwvwh ]rqgdj](https://img.dokumen.tips/doc/110x75/6104ad775e333654341d7fa2/poster-q1-2020-x-de-groote-heide-2020-1-13-onh-zrhqvgdjdyrqg-lhqhq-rqwh.jpg)



























