Embed Size (px)
Citation preview

Heel Coverage Using a Distally BasedSural Artery Fasciocutaneous Cross-legFlap: Report of a Small Series
Attilio Basile, MD,1 Marcello Stopponi, MD,1 Andrea Loreti, MD,2 andAngelo Ugo Minniti de Simeonibus, MD1
One of the goals in the management of severe open injuries of the foot is to obtain adequate soft tissuecoverage. In extreme conditions of pedal soft tissue loss, in patients who are not satisfactory candidatesfor local or free-tissue transfer, the cross-leg flap remains an option for surgical reconstruction. Wepresent the results of 7 patients with multiple lower limb open fractures associated with ipsilateraldegloving injuries, and/or secondary pressure ulcers of the hindfoot with exposure of the calcaneus, inwhich a distally based sural artery island fasciocutaneous flap, elevated from the contralateral leg andcrossed to the injured side, was used to repair the soft tissue defect of the recipient heel. All of the flapssurvived and the soft tissues healed uneventfully, thereby providing satisfactory and stable coverage ofthe calcaneal tuberosity. To the best of our knowledge, this is the first report in which this technique hasbeen used to repair hindfoot soft tissue defects associated with complex bone and vascular injuries ofthe lower limb in polytrauma patients. Level of Clinical Evidence: 4 (The Journal of Foot & Ankle Surgery47(2):112–117, 2008)
Key Words: calcaneus, cross-leg flap, degloving, fasciocutaneous flap, heel ulcer, musculoskeletal
trauma, soft tissue defectI n the presence of an extensive hindfoot soft tissue defect,without the ability to employ microsurgical free-tissuetransfer or ipsilateral fasciocutaneous or local muscularflaps, very few solutions are available for attempting cov-erage of the calcaneus and other portions of the traumatizedhindfoot. In such cases, cross-leg and cross-foot flaps can beemployed, and use of the sural artery cross-leg flap forcoverage of contralateral heel defects may be a usefuloption. One case of sural cross-leg flap has been previouslymentioned in a report of 22 patients in which the ipsilateraldistally based sural fasciocutaneous flap was used to recon-struct distal leg defects (1). The sural cross-leg flap has alsobeen used successfully to reconstruct 2 cases of chronic andinfected ulcers of the foot (2). The aim of the current reportwas to retrospectively assess the results of heel coverageusing a distally based sural artery fasciocutaneous cross-legflap in a series of patients that had sustained polytraumawith associated complex bone and soft tissue defects in-
Address correspondence to: Attilio Basile, MD, Via Nicola Pellati 45,00149 Rome, Italy. E-mail: [email protected].
1Orthopaedic Surgeon, Department of Orthopaedic and Trauma Sur-gery, Ospedale San Giovanni-Addolorata, Rome, Italy.
2Plastic Surgeon, Department of Plastic and Reconstructive Surgery,Ospedale San Giovanni-Addolorata, Rome, Italy.
Copyright © 2008 by the American College of Foot and Ankle Surgeons
1067-2516/08/4702-0006$34.00/0doi:10.1053/j.jfas.2007.12.005112 THE JOURNAL OF FOOT & ANKLE SURGERY
volving the leg and hindfoot. To the best of our knowledge,this is the first report of the results of this sural arterycross-leg flap for coverage of the heel in polytrauma pa-tients.
Patients and Methods
We retrospectively reviewed consecutive patients whowere treated at our institution by means of a distally basedsural artery fasciocutaneous cross-leg flap. To be includedin the case series, the patients had to have been admitted fortreatment of polytrauma that included leg and foot bone andsoft tissue defects, and the aforementioned cross-leg flaphad to have been employed for the coverage of a persistentheel wound. The review was undertaken by the authors,who also served as the managing surgeons for the patientsdescribed in this report.
Review of the records revealed 7 patients who met ourinclusion criteria (Table 1). All of the patients were motorvehicle accident victims and, in all of the cases, the con-tralateral limb was uninjured. Six of the patients sufferedGustilo-Anderson (G-A) grade III B open tibial fractureswhile 1 presented with a G-A grade III C injury (3). All ofthe injuries were associated with exposure of the ipsilateralheel by means of acute degloving that was sustained at thetime of the initial trauma, or due to secondary nonhealing
ulceration of the hindfoot with resultant exposure of the
posterior tuberosity of the calcaneus that developed over thecourse of the hospitalization. The patients were treatedbetween December 2002 and March 2006, at our level Itrauma center. The case series consisted of 5 males and 2females with an average age of 33.9 years (range 26 to 55years), and none of the patients were complicated with anysystemic disease comorbidities at the time of admission.Two of the patients related that they smoked 10 to 15cigarettes per day and were strongly advised to discontinuesmoking during the recovery period, and both of thesepatients fully complied with this recommendation.
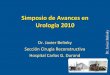
Upon admission, all of the patients underwent assessmentand resuscitation according to advanced trauma life support(ATLS, American College of Surgeons, Inc., Chicago, IL)guidelines (4). All of the patients, moreover, were admin-istered intravenous antibiotics (cefotaxime 2 g every 8 hoursfor 5 days); and neurological, thoracic, and abdominal life-threatening injuries were treated. Open fractures were man-aged with urgent debridement and irrigation, and externalfixation was used in 5 patients while immediate intramed-ullary nailing was used in 2 patients. In 1 case, categorizedas a G-A III C fracture, repair of the posterior tibial arterywas performed with an interpositional vein graft. All openwounds were packed with tobramicin-impregnated polym-ethylmethacrylate beads. Within 24 to 48 hours, patientswere taken back to the operative theater for repeat debride-ment and irrigation. The average tibial wound size after thisdebridement procedure was 13 cm � 7 cm (Figure 1). At 5to 10 days after the initial trauma, when the soft tissues wereconsidered stable, free latissimus dorsi muscle flaps wereperformed to cover the tibial defect in each patient. At 3 to10 weeks following the traumatic event, all of the patientshad been referred to our foot and ankle unit for treatment ofopen heel defects that resulted in exposure of the posterior
TABLE 1 Clinical characteristics of the case series
Patient Age (y) Gender Injuriesc
1 26 Male Degloving injury (secondarybone exposition)
No
2 36 Male Primary hindfoot soft tissuedefect
No
3 30 Female Degloving injury (secondarybone exposition)
No
4 28 Male Pressure ulcer Nos
5 29 Male Primary hindfoot soft tissuedefect
No
6 55 Male Pressure ulcer Nos
7 33 Female Primary hindfoot soft tissuedefect
No
tuberosity of the calcaneus. In each case, the heel defect had
VO
resulted from either the original trauma, or it had developedsecondary to pressure ulceration during the course of theircare. The average heel open wound size was 5 cm � 7 cm(Figure 2).
Prior to presentation to the foot and ankle service, thesepolytrauma patients had undergone a mean average of 6surgeries, including operations for either thoracic and/orabdominal, neurological, vascular, plastic reconstructive, ororthopedic interventions. Moreover, the hindfoot soft tissuedefects had been treated with repeated irrigation and de-bridement procedures and wet-to-dry dressings, or, in 4patients (beginning in 2004), vacuum-assisted wound clo-sure (V.A.C. Therapy, Kinetic Concepts, Inc., San Antonio,TX). After consideration, the plastic surgeons treating thesepatients declared that these patients were not candidates for
icalbidities
Heelwound
defect (cm)
Woundpreparation
Patients’ limbimmobilization
6 � 6 Vacuum-assistedclosure
External fixation
4 � 8 Vacuum-assistedclosure
External fixation
5 � 7 Vacuum-assistedclosure
Intramedullary nail
igaretteer)
6 � 8 Vacuum-assistedclosure
External fixation
5 � 5 Wet to dry Intramedullary nail
igaretteer)
4 � 7 Wet to dry External fixation
5 � 8 Wet to dry External fixation
FIGURE 1 Distal leg and hindfoot soft tissue defect after multipledebridement procedures.
Medomor
ne
ne
ne
ne (cmokne
ne (cmokne
a potentially complicated free tissue transfer, for the fol-
LUME 47, NUMBER 2, MARCH/APRIL 2008 113

lowing reasons: (1) poor potential vascular supply to a freetissue transfer in 1 patient with a G-A grade III C openfracture and consequent single vessel limb after a previousrevascularization used to treat the initial tibial defect; (2)relatively small heel defect with granulation tissue partiallycovering the calcaneal tuberosity in 4 cases; (3) previousfailure of the distal part of the latissimus dorsi free flap usedto cover the tibial and hindfoot defect in 1 case; and (4) thepresence of trauma-related medical and metabolic comor-bidities, namely pulmonary complications, coagulopathy,and fluid and electrolyte imbalances in 1 case. Moreover, inall 7 of these patients, a simpler local muscle flap or ipsi-lateral fasciocutaneous reconstruction was also contraindi-cated because of preexisting soft tissue damage and post-surgical scars. In 3 patients who were treated before 2004,when we did not have vacuum-assisted wound closure tech-nology at our institution, the pursuit of secondary intentionhealing by means of ongoing, repetitive wet-to-dry dressingchanges was deemed inadvisable due to the anticipatedlength of treatment that would have been necessary toachieve adequate coverage of the heel defects. In 4 of thepatients, vacuum-assisted wound closure promoted granu-
FIGURE 2 Faliure of the distal portion of the flap with resultingexposure of the posterior tuberosity of the calcaneus.
lation coverage of the heel defects; however, we considered
114 THE JOURNAL OF FOOT & ANKLE SURGERY
the use of a split-thickness skin graft in this location to beinadvisable for reasons related to graft durability. Therefore,we decided to elevate a distally based sural artery fascio-cutaneous island flap on the contralateral leg, and cross it tothe opposite lower extremity to repair the exposed region ofthe heel.
Two preoperative tests were performed on the donor site(uninjured limb) in all of the cases: (1) a simple clinicalexam to confirm the presence of a normal sensation throughthe distribution of the sural nerve, and (2) a Doppler ultra-sound evaluation of the vascular network to confirm normalblood flow in the peroneal and tibial vessels. Other reversedisland flaps such as the peroneal artery flap, anterior tibialartery flap, and posterior tibial artery flap were consideredbut excluded because it was determined that sacrifice of amajor artery constituted a potentially serious disadvantage.The instep fasciocutaneous flap raised from the plantarme-dial region of the sole between the heel and the metatarsalheads was also considered, and is known to be useful forreconstruction of weight-bearing heel defects; however, be-cause of the shortness of the pedicle, we considered it toodifficult to successfully cross. For the patients in our series,the sural artery tissue transfer remained our first choice forreconstruction because the blood supply to the flap is reli-able, elevation is relatively easy and quick, and majorarteries are not sacrificed.
Limb immobilization was obtained either by means ofexternal fixation of both legs in a comfortable position, orby means of a circumferentially applied elastic wrap. Fiveof the patients underwent application of an external fixator(Figure 3), which was first applied to the uninjured leg, andthen to the side with the tibial defect. In the 2 patients whohad undergone tibial intramedullary nailing, an elastic ban-dage was used to maintain the extremities in apposition. Inthese 2 cases, moreover, the heels were off-loaded simply
FIGURE 3 Cross-leg flap coverage of the heel.
using pillows to keep the hindfoot lifted above the support-

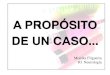
ing surface. In all of the cases, the patients were able to flexboth knees and to abduct their hips together while changingposition in bed, without pulling on the flap pedicle. Nospecific exercises were prescribed while the flap wascrossed and the legs immobilized. In all cases, the pediclewas divided 21 days postoperative, since this period of timeis generally considered enough for primary flap insettingand autonomization (Figure 4). The external fixation de-vices were subsequently removed from the uninjured legsuneventfully. In all of the cases, deep venous thrombosis(DVT) prophylaxis was instituted using 4000 internationalunits of enoxaparin daily, until full weight bearing wasresumed. Progressive weight bearing was allowed between6 and 8 weeks after the division of the cross-leg pedicle,depending upon the degree of soft tissue and bone healing.All of the patients had resumed full weight bearing by 12weeks postoperative. Thereafter, accommodative footwearwas used to protect the remodeling graft sites. The meanfollow-up time was 28 (range 13 to 50) months.
In all of the cases, the surgical procedure for execution ofthe sural artery cross-leg fasciocutaneous island flap in-volved positioning the patient supine, with additional sup-port placed beneath the contralateral buttock to effect asemi-lateral decubitus position. In no case was a tourniquetused. Careful soft tissue debridement and bone resectionwas performed at the receiving site, after which the suralnerve was marked from the midcalf between the 2 heads ofthe gastrocnemius to the midpoint between the Achillestendon and the lateral malleolus from the contralateral limb.The appropriately sized flap was marked out on this linewith the pivot point kept at least 7 cm above the lateralmalleolus. The incision was initiated at the proximal marginof the flap, and the sural nerve and associated vessels wereidentified, dissected, and then appropriately ligated and
FIGURE 4 Appearance of the flap after pedicle division. Note thesoft tissue padding of the weight-bearing area of the heel.
severed. The skin incision was then elongated distally along
VO
the line of the fascial pedicle, and the subdermal layer wasdissected to expose the sural nerve and the accompanyingvessels. The subcutaneous fascial pedicle was elevated, witha width of at least 2 cm, inclusive of the neurovascularbundle. In all of the cases, procurement of the flap wasreadily undertaken without complication, and blood losswas minimal. A number of reports have discussed the po-tential benefits of trying to preserve the sural nerve in thedonor limb, however these techniques are associated withmarkedly increased operative time (5, 6). As with all islandflaps, particular care was required during flap rotation toprevent torsion, compression, or kinking of the vascularpedicle. The skin paddle was then sutured to the defect. Thedonor site defect was skin grafted with autogneous split-thickness skin. The overall mean operative time was 106minutes (range 80 to 135 minutes).
Results
All the distally based sural fasciocutaneous cross-legflaps survived totally and the soft tissues healed unevent-fully, thereby providing satisfactory and stable coverage ofthe calcaneal tuberosity. In one patient we observed a min-imal superficial rim necrosis that appeared before pedicledivision and healed by secondary intention with localwound care.
There were no cases of infection, hematoma, or graft lossat the donor site. The only inevitable morbidity was the lackof sensation in the territory of the sural nerve on the donorlimb. In one patient (G-A grade III C), an early failure of thetibial free flap due to a deep infection was observed. Wewere not able to control the infection and a below-the-kneeamputation was performed. Interestingly, the sural arteryfasciocutaneous sural flap used to cover the heel had healeduneventfully even in this patient. At the time of final follow-up, substantial flap remodeling had occurred, and no patientexperienced local wound drainage and/or recurrent ulcer-ations, and all of the patients were able to walk on the flapwithout pain (Figure 5). Interestingly, all of the patientsdeveloped a certain degree of protective deep touch sensa-tion in the area of flap coverage of the recipient heel.
Discussion
One of the goals in the management of severe openinjuries of the foot is to obtain adequate soft tissue coverage.Defects over the weight-bearing part of the heel require awell-vascularized reconstruction having the characteristicsof stability, adequate padding and durability. Differentforms of soft tissue coverage are available, including mus-cle, fasciocutaneous, and free flaps (7). However, in thepresence of hindfoot soft tissue defects, particularly those
involving exposure of the posterior tuberosity of the calca-LUME 47, NUMBER 2, MARCH/APRIL 2008 115

neus, in patients who are not candidates for microsurgicalfree-tissue transfer, ipsilateral fasciocutaneous, or localmuscle flaps, very few solutions are available in order toattempt limb salvage. In this difficult scenario, the cross-legflap remains an option for surgical reconstruction of theheel. Classically, cross-leg flaps allow a limited amount oftissue transfer, as the pedicles are short, thick, and notcapable of being stretched. Furthermore, cross-leg flapstraditionally convey a limited arch of rotation and an unre-liable random blood supply. These limitations force thepatient into uncomfortable cross-leg postures that must bemaintained while the graft is taking at the recipient site. Asa result of these shortcomings, traditional cross-leg flapshave been associated with complications, including an in-ability to adequately cover the recipient site wound (2, 7).
In 1981, Potén (8) pointed out the significance of thefasciocutaneous circulation. Subsequently, the vascularanatomy of the skin was closely detailed and fasciocutane-ous flaps were designed with predictable circulation (9–11).In 1992, Masquelet et al (9) described skin island flapssupplied by the vascular axis of the sensitive superficialnerves of the leg. The vascular axis, which can be either atrue artery (a named anatomical vessel) or an interlacingnetwork, ensures the vascularization of the nerves, gives offseveral cutaneous branches in the suprafascial course of thenerve, and anastomoses with the septocutaneous arteriesissuing from a deep main vessel. The superficial nerves thatcourse the leg can therefore be considered as vascular relaysowing to their neurocutaneous arteries (9). The vascularsupply to the distally based sural fasciocutaneuos flap isderived from the retrograde perfusion of the arteries thataccompany the lesser saphenous vein and sural nerve. Thesearteries descend along both sides of the lesser saphenous
FIGURE 5 Long-term clinical appearance of the heel at the latestfollow-up visit. Good remodeling and padding of the heel haveoccurred.
vein, either terminating or anastomosing with the septocu-
116 THE JOURNAL OF FOOT & ANKLE SURGERY
taneous perforators of the peroneal artery 5 to 10 cm abovethe lateral malleolus. The blood supply courses in a retro-grade fashion from these perforators when the nerve and thearteries are cut proximally. The distally based lower-legfasciocutaneous and adipofascial local flaps, described byMasquelet et al (9) offer an easy and reliable surgicaloption, to free flaps in presence of distal third soft tissuesdefects of the leg and foot of small and medium extension.Their use in acute and chronic traumatic soft tissue injuries,namely degloving, crush, and avulsion injuries with result-ant loss of wound coverage, is well documented and isgaining widespread acceptance (1, 9, 11, 12). Compared tothe traditional cross-leg technique, the cross-leg island flapwith a subcutaneous pedicle based on the sural neurovas-cular bundle has provided a major improvement in flapmobility, with a longer and more pliable pedicle and apredictable blood supply.
In the series of patients described in this report, thepedicles of the cross-leg flaps were divided 21 days post-operative, as this period of time is generally consideredenough for primary flap insetting and autonomization.Much to our satisfaction, and that of the patients, all of theflaps described in this report survived completely. Acland(13) found regular flap necrosis when the pedicle vesselswere ligated at 7 days. Similarly, Serafin and colleagues(14) noted a high correlation between the timing of vesselligation and the percentage of flap survival. In our series, wealso found vacuum-assisted wound closure to be a usefuladjunct for hindfoot defects because of its ability to controlexudate and edema, to increase vascularity and decreasewound size, and to decrease bacterial colonization; how-ever, multimodal therapies including flap coverage are stilloften needed to facilitate closure after heel wounds havebeen prepared (15–18). Initially developed in the early1990s for the management of large, chronically infectedwounds that could not be closed in extremely debilitatedpatients, vacuum-assisted wound closure has, more re-cently, been used in the treatment of traumatic wounds (15,16). Although the use over bone, tendon, or hardware wasconsidered an early contraindication to the negative-pres-sure wound therapy (NPWT), there are now reports thatsupport its use in the presence of exposed deep structures(15–17). In our hands, although we were able to obtainprofuse granulation tissue covering bone, we still needed aregional flap to be rotated in order to obtain completewound coverage about the heel. Our results using NPWTwere in line with those noted in previously published re-ports, wherein Herscovici and colleagues (15) stated that theuse of a free-tissue transfer was still required in 43% of theircases, and De Franzo and colleagues (16) described suc-cessful wound coverage in 71 of 75 cases with skin and orregional muscle transfer versus free-tissue transfer after the
use of vacuum-assisted closure.
It is our opinion that the distally based sural fasciocuta-neous cross-leg flap may still be required to obtain adequatecoverage in very specific cases; even efforts to achieveclosure using NPWT. Due to the weight-bearing require-ments of the heel, and the precarious soft tissue paddingoffered by granulation tissue covering the posterior tuber-osity of the calcaneus, we did not consider the use of asplit-thickness skin graft to be a suitable option. This con-cern has also been expressed in the literature, where anumber of authors have demonstrated the failure of effortsto resurface the weight-bearing area of the heel using split-thickness skin grafts (1, 19–21). Moreover, NPWT, as wellas the use of microvascular free flaps, require relativelyexpensive instrumentation and highly skilled surgeons, andthese assets are not always readily available, particularly inunderprivileged areas of the world. In such eventualities, webelieve that the distally based sural artery fasciocutaneouscross-leg flap described in this report provides a usefuloption for reconstruction of the heel. Although we could notdraw definitive conclusions because of the small size of ourcase series, the distally based sural cross-leg flap proved tobe a valuable reconstructive option for our patients. Inconclusion, we recommend that the sural fasciocutaneouscross-leg flap be considered as a “last chance” for limbsalvage in a select cohort of patients with soft tissue defectsover weight-bearing surfaces of the hindfoot in which noother reasonable solution is available.
References
1. de Almeida OM, Monteiro AA Jr, Neves RI, de Lemos RG, Braz JC,Brechtbuhl ER, Gemperli R, Ferreira MC. Distally based fasciocuta-neous flap of the calf for cutaneous coverage of the lower leg anddorsum of the foot. Ann Plast Surg 44:367–373, 2000.
2. Atiyeh BS, Al-Amm CA, El-Musa KA, Sawwaf AW, Musharafieh RS.Distally based sural fasciocutaneous cross-leg flap: a new applicationof an old procedure. Plast Reconst Surg 111:1470–1474, 2003.
3. Gustilo RB, Anderson JT. Prevention of infection in the treatment ofone thousand and twenty-five open fractures of the long bones: retro-spective and prospective analysis. J Bone Joint Surg 58-A:453–458,1976.
4. Advanced Trauma Life Support for Doctors, ed 7, p 1–391, AmericanCollege of Surgeons, Chicago, IL, 2005.
5. Nakajima H, Imanishi N, Fukuzumi S, Minabe T, Fukui Y, Miyasaka
T, Kodama T, Aiso S, Fujino T. Accompanying arteries of the lesserVO
saphenous vein and sural nerve: anatomic study and its clinicalapplications. Plast Reconst Surg 103:104–120, 1999.
6. Yilmaz M, Karatas Q, Barutca A. The distally based sural artery islandflap: clinical experiences and modifications. Plast Reconstr Surg 102:2356–2367, 1998.
7. Chapman MV, Olson SA. Open fractures. In Rockwood and Green’sFractures in Adults, ed 4pp 305–352, edited by RW., Bucholz JD.,Heckman Court-Brown C., P., Tornetta KJ., Kova Lippincott-Raven,Philadelphia, 1996.
8. Potén B. The fasciocutaneous flap: its use in soft tissue defects of thelower leg. Br J Plast Surg 34:215–220, 1981.
9. Masquelet AC, Romana MC, Wolf G. Skin island flaps supplied by thevascular axis of the sensitive superficial nerves: anatomic study andclinical experience in the leg. Plast Reconstr Surg 89(6):1115–1121,1992.
10. Fix RJ, Vasconez LO. Fasciocutaneous flaps in reconstruction of thelower extremity. Clin Plast Surg 18:571–582, 1991.
11. Louton RB, Harley RA, Hagerty RC. A fasciocutaneous transpositionflap for coverage of defects of the lower extremity. J Bone Joint Surg71-A:988–994, 1989.
12. Touam C, Rostoucher P, Bhatia A, Oberlin C. Comparative study oftwo series of distally based fasciocutaneous flaps for coverage of thelower one-fourth of the leg, the ankle, and the foot. Plast Reconstr Surg107:383–392, 2001.
13. Acland RD. In Skin Flaps, p 100–105, edited by WC Grabb, B MyersB, Little Brown, Philadelphia, PA, 1975.
14. Serafin D, Shearin JC, Georgiade NG. The vascularization of freeflaps: clinical and experimental correlation. Plast Reconstr Surg 60:233–237, 1977.
15. Herscovici D Jr, Sanders RW, Scaduto JM, Infante A, DiPasquale T.Vacuum-assisted wound closure (VAC therapy) for the managementof patients with high-energy soft tissue injuries. J Orthop Trauma17(10):683–688, 2003.
16. DeFranzo AJ, Argenta LC, Marks MW, Molnar JA, David LR, WebbLX, Ward WG, Teasdall RG. The use of vacuum-assisted closuretherapy for the treatment of lower-extremity wounds with exposedbone. Plast Reconstr Surg 108:1184–1191, 2001.
17. Morykwas MJ, Argenta LC, Shelton-Brown EI, McGuirt W. Vacuum-assisted closure: a new method for wound control and treatment:animal studies and basic foundation. Ann Plast Surg 38(6):553–562,1997.
18. Argenta LC, Morykwas MJ. Vacuum-assisted closure. A new methodfor wound control and treatment. Clinical experience. Ann Plast Surg38(6):563–577, 1997.
19. Savk O, Savk E. Reverse sural artery flap for distal lower extremitydefects. J Dermatol 33(10):700–704, 2005.
20. Ortak T, Ozdemir R, Ulusoy MG, Tiftikcioglu YO, Karaaslan O,Kocer U, Sensoz O. Reconstruction of heel defects with a proximallybased abductor hallucis muscle flap. J Foot Ankle Surg 4(44):265–270,2005.
21. Suri MP, Patel AG, Vora HJ, Raibagkar SC, Mehta DR, Vyas UH.Post traumatic posterior heel soft defect reconstruction. Indian J Plastic
Surgery 2(38):138–143, 2005.LUME 47, NUMBER 2, MARCH/APRIL 2008 117