Embed Size (px)
Citation preview
Ideas and Innovations
The Cone Flap: A New and VersatileFasciocutaneous FlapWilfredo Calderón, F.A.C.S., Patricio Andrades, M.D., Patricio Leniz, M.D., Ph.D.,José Luis Piñeros, M.D., Sergio Llanos, M.D., Ricardo Roa, M.D., and Osvaldo Irribarren, M.D.Santiago, Chile
Fasciocutaneous flaps have enjoyed consid-erable success in both the clinical and experi-mental fields.1,2 One of the most difficult areasof the body to repair is the distal lower extrem-ity, especially when bone is exposed. In thesecases, local myocutaneous flaps, muscularflaps, microsurgery, and cross-leg flaps havehistorically been utilized to obtain a durableclosure.3 Fasciocutaneous flaps have been dem-onstrated to be reliable, simple, and fast surgi-cal solutions for moderate distal lower extrem-ity defects.4–13 From our point of view, theproblem with these flaps is how to close thedonor site. The purpose of this report is toshow our experience with a novel procedurefor direct closure of the donor site of fasciocu-taneous flaps using a combined technique of arotation flap and a classic V-Y advancementflap.
PATIENTS AND METHODS
From August of 2000 through June of 2002,25 patients were operated on by the staff of theDepartment of Plastic Surgery of the Hospitaldel Trabajador, in Santiago, Chile. All the pa-tients were men (age range, 20 to 52 years)with exposed bone (tibia) in the distal portionof the leg, with traumatic defects ranging from2 to 5 cm in diameter and no osteomyelitis.1Success in the lower extremity was followed byapplication to other parts of the body, includ-ing the elbow (two patients), plantar region(four patients), great toe (one patient), arm(one patient), nose (one patient), and calvaria(two patients). In total, this represents a series
of 36 cases. All patients were evaluated clini-cally and photographically at 1-year follow-up.
The surgical technique consisted of a rota-tion fasciocutaneous flap to cover the primarydefect and a V-Y fasciocutaneous flap to closethe donor site (Fig. 1). To obtain good ad-vancement of the V-Y flap, we cut the fascia tothe underlying muscle, all around the V flap.This allowed for good flap advancement andcomplete coverage of the defect created by therotation flap. Both flaps are classified as Cor-mack and Lamberty type A.14
RESULTS
All the flaps survived completely, despite su-tures under tension in some patients. All of thepatients with lower extremity flaps walked after5 days with elastic support. There was no skinnecrosis in our series. The wounds healed well,without dehiscence, and scarring was minimal.There was no significant long-term edema orpain, and postoperative sensation remained in-tact (Figs. 2 through 4).
DISCUSSION
When a skin defect is present in the distalportion of the leg, closure is not easy becausethis area is marginally perfused, the skin is thinand tight, and the defect is frequently associ-ated with an underlying fracture. The surgicaloptions for skin coverage of the distal leg mayinclude muscular, myocutaneous, neurocuta-neous, fasciocutaneous, and free flaps.3 Fascio-cutaneous flaps have been demonstrated to besafe and reliable in the coverage of small de-
From the Department of Burn and Plastic Surgery, Hospital del Trabajador and the Plastic and Reconstructive Surgery Unit, Clinical HospitalJ. J. Aguirre, University of Chile School of Medicine and Diego Portales University. Received for publication November 3, 2003; revised February12, 2004.
DOI: 10.1097/01.PRS.0000138754.97774.08
1539
fects in this area.6–8 Their vascularity has beenstudied extensively,9 and they have the greatadvantage of preserving sensitivity.4,5 Unfortu-nately, they are not useful in larger defects,they are less resistant to infection than muscu-lar flaps are,2 and they always leave a complexdonor-site defect.
Usually, the donor-site defect of a fasciocu-taneous flap is repaired with a partial-thicknessskin graft. This type of repair leave poor skincoverage, with frequent ulceration, loss of sen-sitivity, skin retraction, pigmentation, and hy-pertrophic scars.15 A good option for avoidingthese complications is to use another flap fordonor-site coverage.16–18 A fasciocutaneous flapfor closure of this donor site is preferable be-cause it has better vascular security and a better
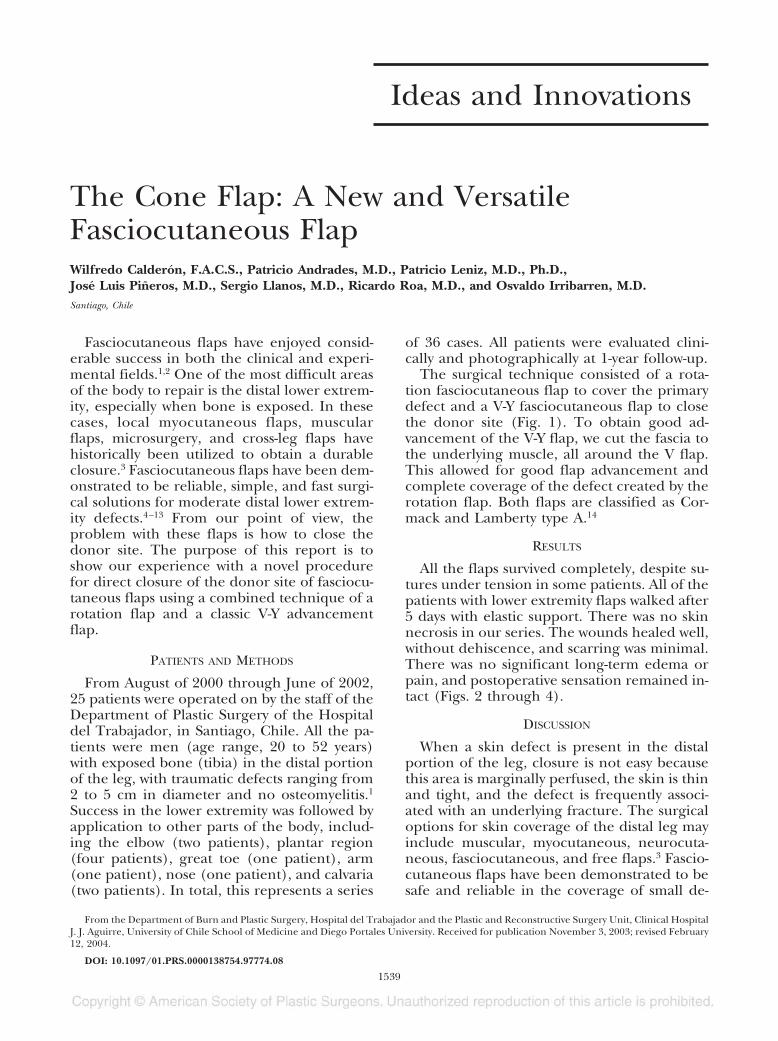
FIG. 1. Cone flap design. (Left) Original defect and rota-tion flap design. (Center) Rotation of flap and V-Y advance-ment flap design for secondary defect coverage. (Right) Finalresult.
FIG. 2. (Above, left) Small defect of the lower leg and bone exposure. (Above, center and right) Intraoperative viewsof cone flap elevation. (Below) Immediate and long-term results are shown.
1540 PLASTIC AND RECONSTRUCTIVE SURGERY, November 2004
mobilization rate. In addition, it decreases theuse of other, lower-quality or more complexcoverage options, and it offers better aestheticresults and restored sensitivity. In this respect,the V-Y advancement flap has been the mostused for these purposes.19–21
A local fasciocutaneous flap alone can beused in small lower extremity defects that per-mit primary closure of the donor site. The“cone” flap expands this indication to largerlesions under the same principles. It shouldnot be used in small defects because one flapcould be enough. It is also not indicated in
large defects because they are usually associ-ated with infection and comminuted fracturesand no skin is available. For these reasons, thebest indications are medium-size defects (5 to10 cm) with adequate surrounding tissue, sim-ple underlying fractures, and lower grades ofcontamination.
In this work, we present a new alternative fordonor-site closure of a rotation flap with a V-Yadvancement flap. We named it the “cone” flapbecause of the final shape that results after thesurgery. It is a simple and easy-to-learn tech-nique that is useful in the coverage of small tomedium-size defects in the distal leg and otherlocations. Preserving all the fasciocutaneouscharacteristics, the cone flap has a low compli-cation rate and adequate long-term results.The disadvantages are the suture tension andthe fact that it is not indicated in larger orinfected defects. We recommend this easy tech-nique, as we have improved our surgical timesand complication rates with good patientacceptance.
Wilfredo Calderón, M.D.Hospital del TrabajadorRamón Carnicer 185-5° PisoProvidencia, Santiago, [email protected]
ACKNOWLEDGMENT
We thank Dr. Luis Vasconez for reviewing and improvingour manuscript.
REFERENCES
1. Ponten, B. The fasciocutaneous flap: Its use in soft tis-sue defects of the lower leg. Br. J. Plast. Surg. 34: 215,1981.
2. Calderón, W., Chang, N., and Mathes, S. J. Comparisonof the effects of bacterial inoculation in musculocu-taneous and fasciocutaneous flaps. Plast. Reconstr.Surg. 77: 785, 1986.
3. Masquelet, A., and Gilbert, A. Flaps in Limb Reconstruc-tion. London: Martin Dunitz, 1995.
4. Fix, R. J., and Vasconez, L. O. Fasciocutaneous flaps inreconstruction of the lower extremity. Clin. Plast. Surg.18: 571, 1991.
5. Tolhurst, D. E., Haeseker, B., and Zeeman, R. J. Thedevelopment of the fasciocutaneous flap and its clin-ical applications. Plast. Reconstr. Surg. 71: 597, 1983.
6. Healy, C., Tiernan, E., Lamberty, B. G., and Campbell,R. C. Rotation fasciocutaneous flap repair of lowerlimb defects. Plast. Reconstr. Surg. 95: 243, 1995.
7. Hallock, G. G. Distal lower leg local random fasciocu-taneous flaps. Plast. Reconstr. Surg. 86: 304, 1990.
8. Hallock, G. G. Local fasciocutaneous flaps for cutane-ous coverage of lower extremity wounds. J. Trauma 29:1240, 1989.
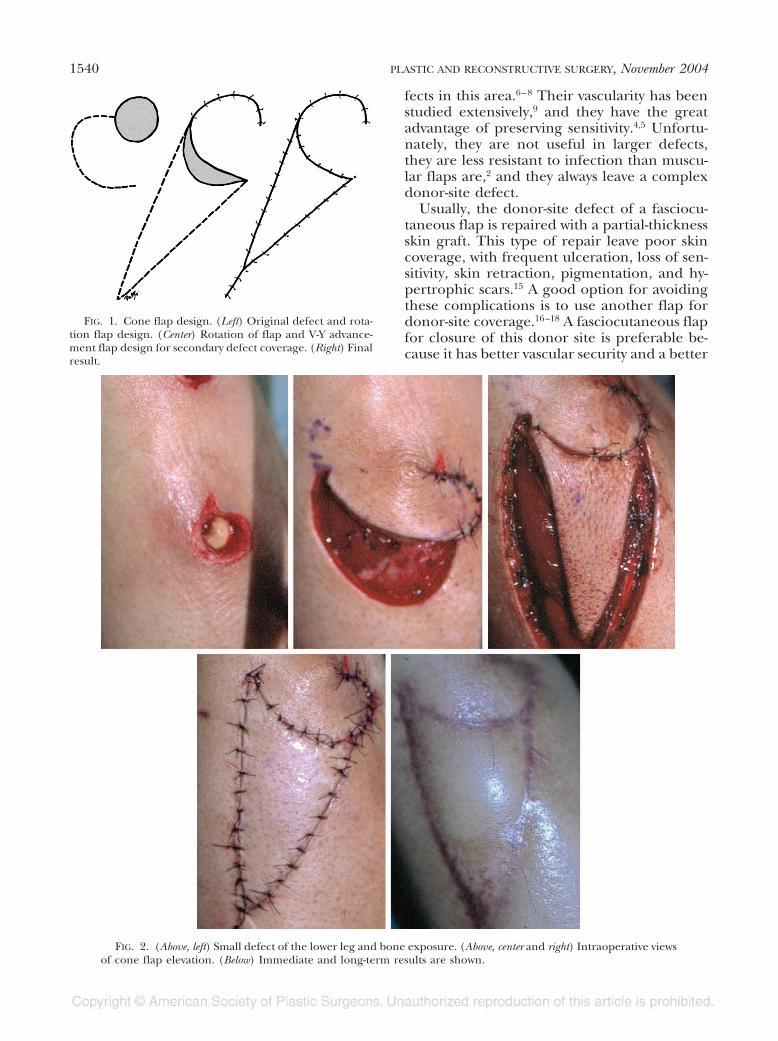
FIG. 3. Another distal medium-size leg defect (above)treated with the cone flap technique. (Center) Rotation flap,V-Y flap design, and (below) long-term results are shown.
Vol. 114, No. 6 / THE CONE FLAP 1541
9. Whetzel, T. P., Barbard, M. A., and Stokes, R. B. Arterialfasciocutaneous vascular territories of the lower leg.Plast. Reconstr. Surg. 100: 1172; discussion 1184, 1997.
10. Hallock, G. G. Clinical scrutiny of the de facto superiorityof proximally versus distally based fasciocutaneousflaps. Plast. Reconstr. Surg. 100: 1428, 1997.
11. Amarante, J., Costa, H., Reis, J., and Soares, R. A newdistally based fasciocutaneous flap of the leg. Br. J.Plast. Surg. 39: 338, 1986.
12. De Almeida, O. M., Monteiro, A. A., Jr., Neves, R. I.,et al. Distally based fasciocutaneous flap of thecalf for cutaneous coverage of the lower legand dorsum of the foot. Ann. Plast. Surg. 44: 367;discussion 373, 2000.
13. Shaw, A. D., Ghosh, S. J., and Quaba, A. A. The islandposterior calf fasciocutaneous flap: An alternative tothe gastrocnemius muscle for cover of knee and tibialdefects. Plast. Reconstr. Surg. 101: 1529, 1998.
14. Lamberty, B. G., and Cormack, G. C. Fasciocutaneousflaps. Clin. Plast. Surg. 17: 713, 1990.
15. Hallock, G. G. Complications of 100 consecutive local fas-ciocutaneous flaps. Plast. Reconstr. Surg. 88: 264, 1991.
16. Karacalar, A. Combined use of V-Y advancement flapand rotation flap. Plast. Reconstr. Surg 106: 1223, 2000.
17. Venkataramakrishnan, V., Mohan, D., and Villafane, O.Perforator based V-Y advancement flaps in the leg.Br. J. Plast. Surg. 51: 431, 1998.
18. Blair, J. W., Bainbridge, L. C., and Knight, S. L. Double V-Yadvancement flaps in the reconstruction of skin defectsof the anterior lower limb. Br. J. Plast. Surg. 46: 644, 1993.
19. Dini, M., Innocenti, A., Russo, G. L., and Agostini, V.The use of the V-Y fasciocutaneous island advance-ment flap in reconstructing postsurgical defects of theleg. Dermatol. Surg. 27: 44, 2001.
20. Niranjan, N. S., Price, R. D., and Govilkar, P. Fascialfeeder and perforator-based V-Y advancement flaps inthe reconstruction of lower limb defects. Br. J. Plast.Surg. 53: 679, 2000.
21. Penington, A. J., and Mallucci, P. Closure of electiveskin defects in the leg with a fasciocutaneous V-Y islandflap. Br. J. Plast. Surg. 52: 458, 1999.
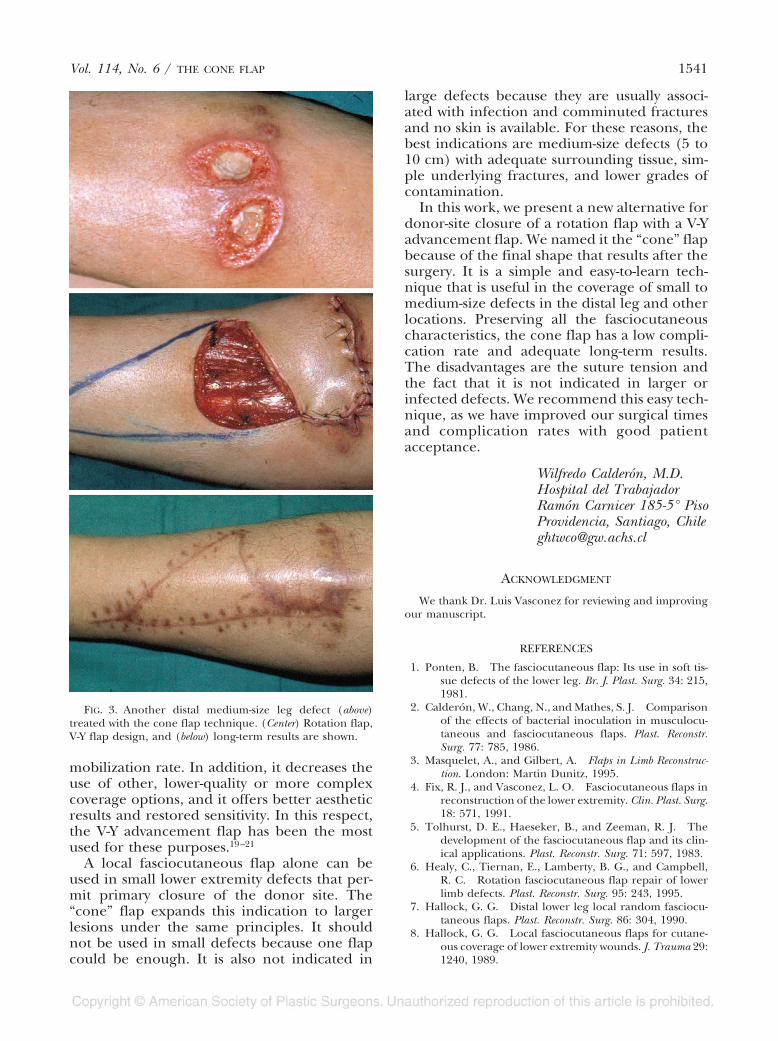
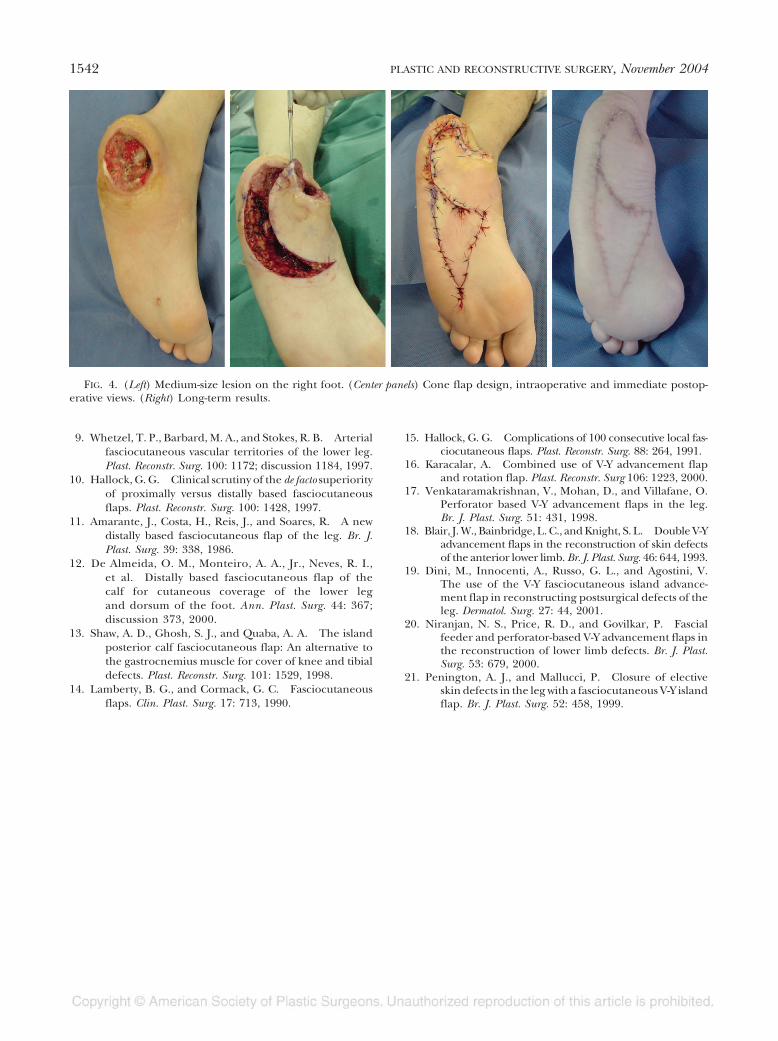
FIG. 4. (Left) Medium-size lesion on the right foot. (Center panels) Cone flap design, intraoperative and immediate postop-erative views. (Right) Long-term results.
1542 PLASTIC AND RECONSTRUCTIVE SURGERY, November 2004