Embed Size (px)
Citation preview

333C
op
yri
gh
t ©
20
00
CO
VE
R I
nc
.Personal Quick Reference Sheets
from: Rapid Interpretation of EKG’sby Dale Dubin, MD
COVER Publishing Co., P.O. Box 07037, Fort Myers, FL 33919, USA
There is no need to remove these reference pages from yourbook. To download and print them in full color, go to:
May humanity benefit from your knowledge,
(pages 333 to 346)
6th Ed.
RAPIDINTERPRETATION
OF
EKG’s
Dale Dubin, MD
Dr. Dubin’s classic, simplified methodology for understanding EKG’s
Learning Web Sites:
Physicians and medical students: www.theMDsite.com
Nurses and nurses in training: www.CardiacMonitors.com
Emergency medical personnel: www.EmergencyEKG.com
www.theMDsite.com
“Reference Sheets”

334C
op
yrig
ht ©
20
00
CO
VE
R In
c.
from: Rapid Interpretation of EKG’sby Dale Dubin, MD
COVER Publishing Co., P.O. Box 07037, Fort Myers, FL 33919, USA
Personal Quick Reference Sheets
Dubin’s Methodfor
Reading EKG’s
1. RATE (pages 65-96)
Say “300, 150, 100” …“75, 60, 50”• but for bradycardia:
rate = cycles/6 sec. strip ✕ 10
2. RHYTHM (pages 97-202)
Identify the basic rhythm, then scan tracing for prematurity,pauses, irregularity, and abnormal waves.
• Check for: P before each QRS.QRS after each P.
• Check: PR intervals (for AV Blocks).QRS interval (for BBB).
• If Axis Deviation, rule out Hemiblock.
3. AXIS (pages 203-242)
• QRS above or below baseline for Axis Quadrant(for Normal vs. R. or L. Axis Deviation).For Axis in degrees, find isoelectric QRS in a limb leadof Axis Quadrant using the “Axis in Degrees” chart.
• Axis rotation in the horizontal plane: (chest leads)find “transitional” (isoelectric) QRS.
4. HYPERTROPHY (pages 243-258)
P wave for atrial hypertrophy.R wave for Right Ventricular Hypertrophy.S wave depth in V1… + R wave height in V5 for Left Ventricular Hypertrophy.
5. INFARCTION (pages 259-308)
Scan all leads for:
• Q waves• Inverted T waves• ST segment elevation or depression
Find the location of the pathology (in the Left ventricle),and then identify the occluded coronary artery.
CheckV1 {

335C
op
yri
gh
t ©
20
00
CO
VE
R I
nc
.Personal Quick Reference Sheets
from: Rapid Interpretation of EKG’sby Dale Dubin, MD
COVER Publishing Co., P.O. Box 07037, Fort Myers, FL 33919, USA
Rate (pages 65 to 96)
Determine Rate by Observation (pages 78-88)
Bradycardia (slow rates) (pages 90-96)
• Cycles/6 second strip ✕ 10 = Rate• When there are 10 large squares between similar waves, the rate is 30/minute.
Sinus Rhythm: origin is the SA Node (“Sinus Node”), normal sinus rate is 60 to 100/minute.
• Rate more than 100/min. = Sinus Tachycardia (page 68).• Rate less than 60/min. = Sinus Bradycardia (page 67).
Determine any co-existing, independent (atrial/ventricular) rates:• Dissociated Rhythms: (pages 155, 157, 186-189) A Sinus Rhythm (or atrial rhythms) may co-exist with an independent rhythm from an automaticity focus of a lower level. Determine rate of each.
Irregular Rhythms: (pages 107-111)
• With Irregular Rhythms (such as Atrial Fibrillation) always note the general (average) ventricular rate (QRS’s per 6-sec. strip ✕ 10) or take the patient’s pulse.
Fine division/rate association: reference (page 89)
May be calculated: 1500
= RATE mm. between similar waves
300 150 100 75 60
250
214
187
167
136
125
115
107
94
88
83
79
71
68
65
62
STA
RT
“300
”
“150
”
“100
”
“75” “60” “50”
Using the triplets:Name the lines following the “Start” line.

336C
op
yrig
ht ©
20
00
CO
VE
R In
c.
from: Rapid Interpretation of EKG’sby Dale Dubin, MD
COVER Publishing Co., P.O. Box 07037, Fort Myers, FL 33919, USA
Personal Quick Reference Sheets
★ Identify basic rhythm……then scan entire tracing for pauses, premature beats,
irregularity, and abnormal waves.
★ Always:• Check for: P before each QRS.
QRS after each P.• Check: PR intervals (for AV Blocks).
QRS interval (for BBB).• Has QRS vector shifted outside normal range? (to rule out Hemiblock).
Irregular Rhythms (pages 107-111)
Sinus Arrhythmia (page 100)
Irregular rhythm that varieswith respiration.All P waves are identical.
Considered normal.
Wandering Pacemaker (page 108)
Irregular rhythm. P waveschange shape aspacemaker location varies.
Rate under 100/minute…
…but if the rate exceeds100/minute, then it is called
Multifocal Atrial Tachycardia(page 109)
Atrial Fibrillation (pages 110, 164-166)
Irregular ventricular rhythm.Erratic atrial spikes(no P waves) frommultiple atrial automaticityfoci. Atrial dischargesmay be difficult to see.
Rhythm (pages 97 to 111)

337C
op
yri
gh
t ©
20
00
CO
VE
R I
nc
.Personal Quick Reference Sheets
from: Rapid Interpretation of EKG’sby Dale Dubin, MD
COVER Publishing Co., P.O. Box 07037, Fort Myers, FL 33919, USA
Rhythm continued (pages 112 to 145)
Escape (pages 112-121) – the heart’s response to a pause in pacing
•A
n u
nh
ea
lty S
inu
s (S
A)
No
de
ma
yfa
il to
em
it a
pa
cin
g s
timu
lus
(“S
inu
s B
lock
”);
this
pa
use
ma
ye
voke
an
esc
ap
e b
ea
t fr
om
an
au
tom
atic
ity f
ocu
s.
•B
ut
a s
ick
Sin
us
(SA
) N
od
e m
ay
cea
se p
aci
ng
(“S
inu
s A
rre
st”)
,ca
usi
ng
an
au
tom
atic
ity f
ocu
s to
“esc
ap
e”
to a
ssu
me
pa
cem
ake
rst
atu
s.
•A
n ir
rita
ble
au
tom
atic
ityfo
cus
ma
y su
dd
en
lyd
isch
arg
e,
pro
du
cin
g a
:
Premature Beats (pages 122-145) – from an irritable automaticity focus
Premature Atrial Beat(pages 124-130)
Premature Ventricular Contraction(pages 135-141)PVC’s may be:multiple, multifocal, in runs, orcoupled with normal cycles.
Premature Junctional Beat(pages 131-133)
pause
AtrialEscape Beat
or
or
VentricularEscape Beat
Then…
the SA Nodeusally resumespacing.Junctional
Escape Beat
(page 119)
(page 120)
(page 121)
++++
+
+
+
+
+
+
+
+++++
++
++++
+
+
+
+
+
+
+
+++++
++
++++
+
+
+
+
+
+
+
+++++
++
(page 114)
(pages 115-116)
(page 117)
(“idiojunctional rhythm”)
(“idioventricular rhythm”)
AtrialEscape RhythmRate 60-80/min.
or
or
JunctionalEscape RhythmRate 40-60/min.
VentricularEscape RhythmRate 20-40/min.

338C
op
yrig
ht ©
20
00
CO
VE
R In
c.
from: Rapid Interpretation of EKG’sby Dale Dubin, MD
COVER Publishing Co., P.O. Box 07037, Fort Myers, FL 33919, USA
Personal Quick Reference Sheets
Atrial FlutterA continuous (“saw tooth”) rapid sequenceof atrial complexes from a single rapid-firingatrial focus. Many flutter waves needed toproduce a ventricular response. (pages 159, 160)
Ventricular Flutter (pages 161, 162) also see “Torsades de Pointes” (pages 158, 345)
A rapid series of smooth sine waves from asingle rapid-firing ventricular focus; usually ina short burst leading to Ventricular Fibrillation.
Paroxysmal Atrial TachycardiaAn irritable atrial focus discharging at150-250/min. produces a normal wavesequence, if P' waves are visible. (page 149)
• P.A.T. with blockSame as P.A.T. but only everysecond (or more) P' waveproduces a QRS. (page 150)
Paroxysmal Junctional TachycardiaAV Junctional focus produces a rapidsequence of QRS-T cycles at 150-250/min.QRS may be slightly widened. (pages 151-153)
Paroxysmal Ventricular TachycardiaVentricular focus produces a rapid(150-250/min.) sequence of (PVC-like)wide ventricular complexes. (pages 154-158)
Rhythm continued (pages 146 to 172)
multiple foci discharging
Rates: ParoxysmalTachycardia Flutter Fibrillation
150 250 350 450
Tachyarrhythmias (pages 146-172), “focus” = automaticity focus
“Sup
rave
ntri
cula
r Ta
chyc
ardi
a”(p
age
153)
Fibrillation …erratic (multifocal) rapid discharges at 350 to 450/min. (pages 167-170)
Atrial Fibrillation (pages 110, 164-166)Multiple atrial foci rapidly dischargingproduce a jagged baseline of tiny spikes.Ventricular (QRS) response is irregular.
Ventricular Fibrillation (pages 167-170)Multiple ventricular foci rapidly dischargingproduce a totally erratic ventricular rhythmwithout identifiable waves. Needs immediatetreatment.
Paroxysmal (sudden) Tachycardia …rate: 150-250/min. (pages 146-163)
fusion
Flutter …rate: 250-350/min.

339C
op
yri
gh
t ©
20
00
CO
VE
R I
nc
.Personal Quick Reference Sheets
from: Rapid Interpretation of EKG’sby Dale Dubin, MD
COVER Publishing Co., P.O. Box 07037, Fort Myers, FL 33919, USA
1° AV Block …prolonged PR interval (pages 176-178).PR interval is prolonged to greaterthan .2 sec (one large square).
2° AV Block … some P waves without QRS response (pages 179-185)
Wenckebach …PR gradually lengthens with each(pages 180-182, cycle until the last P wave in the183) series does not produce a QRS.
Mobitz …some P waves don’t produce a QRS(pages 181-183) response. If “intermittent,” an
occasional QRS is droped.
More advanced Mobitz block mayproduce a 3:1 (AV) pattern or evenhigher AV ratio (page 181).
2:1 AV Block …may be Mobitz or Wenckebach.(pages 182, 183) PR length and QRS width or
vagal maneuvers help differentiate.
3° (“complete”) AV Block …no P wave produces a QRS response (pages 186-190)
3° Block: P waves—SA Node origin.(page 188) QRS’s—if narrow, and if the
ventricular rate is 40 to 60 per min.,then origin is a Junctional focus.
3° Block: P waves—SA Node origin.(page 189) QRS’s—if PVC-like, and if the
ventricular rate is 20 to 40 per min.,then origin is a Ventricular focus.
Sinus (SA) Block (page 174)
An unhealthy Sinus (SA) Node misses one or more cycles (sinus pause)…the Sinus Node usually resumes pacing, butthe pause may evoke an “escape” responsefrom an automaticity focus. (pages 119-121)
★ Always Check:• has Axis shifted
outside Normalrange?
★ Always Check:• is QRS within
3 tiny squares?
★ A
lway
s C
hec
k:• P
R in
terv
als
less
than
one
larg
e sq
uare
?
• Is
ever
y P
wav
e fo
llow
ed b
y a
QR
S?
Rhythm: (“heart”) blocks (pages 173 to 202)
Caution:With Left BBBinfarction is difficultto determine on EKG.
Right BBB (pages 194-196) Left BBB (pages 194-197)
R
QRS in V1 or V2
R'R
QRS in V5 or V6
R'With Bundle BranchBlock the criteria for
ventricular hypertrophyare unreliable.
AV Block (pages 176-189)
Blocks that delay or prevent atrial impulses from reaching the ventricles.
Bundle Branch Block …find R,R' in right or left chest leads (pages 191-202)
Hemiblock …block of Anterior or Posterior fascicle of the Left Bundle Branch.(pages 295-305)
Anterior Hemiblock Posterior HemiblockAxis shifts Leftward ➞ L.A.D. Axis shifts Rightward ➞ R.A.D.
look for Q1S3 look for S1Q3
(pages 297-299) (pages 300-302)

340C
op
yrig
ht ©
20
00
CO
VE
R In
c.
from: Rapid Interpretation of EKG’sby Dale Dubin, MD
COVER Publishing Co., P.O. Box 07037, Fort Myers, FL 33919, USA
Personal Quick Reference Sheets
Lead AVF
Lead I
Axis (pages 203 to 242)
Extreme Right Axis Deviationlead Axis
IAVL
IIIAVF
–90°–120°–150°–180°
Right Axis Deviationlead AxisAVF
IIAVR
I
+180°+150°+120°
+90°
Left Axis Deviationlead Axis
IAVR
IIAVF
–90°–60°–30°
0°
Normal Rangelead AxisAVF
IIIAVL
I
0°+30°+60°+90°+90o
-90o
+60o
-60o
+30o
-30o
0o
0o
L.
A.
D.
Normal R
ang
e
-90o
+90o
-120o
+120o
-150o
+150o
+180o
-180o
R.
A.
D.
Extr
eme R.A.D.
General Determination of Electrical Axis (pages 203-242)
Is QRS positive ( ) or negative ( ) in leads I and AVF?Is Axis Normal? (page 227) First Determine Axis Quadrant
(pages 214-231)
Axis in Degrees (pages 233, 234) (Frontal Plane)After locating Axis Quadrant, find limb lead where QRS is most isoelectric:
Normal:{
Axis Rotation (left/right) in the Horizontal Plane (pages 236-242)
Find transitional (isoelectric) QRS in a chest lead.
transitional QRSis “isoelectric”
QRS in lead I (pages 215-222)…if the QRS is Positive (mainly abovebaseline), then the Vector points topositive (patient’s left) side.
QRS upright in I and AVF“two thumbs-up” sign
QRS in lead AVF (pages 223-226)…if the QRS is mainly Positive, thenthe Vector must point downward topositive half of the sphere.
I
AVF
I
I
AVF
I
AVF
AVFL.A.D
.
R.A.D. Norm
al
R.A
.D.
Extre
me
Patient’sRight
Patient’sLeft
V1 V2 V3 V4V5
V6rotation
Normal Range
rotationLeftward
Rightward

341C
op
yri
gh
t ©
20
00
CO
VE
R I
nc
.Personal Quick Reference Sheets
from: Rapid Interpretation of EKG’sby Dale Dubin, MD
COVER Publishing Co., P.O. Box 07037, Fort Myers, FL 33919, USA
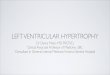
Atrial Hypertrophy (pages 245-249)
Right Atrial Hypertrophy (page 248)
• large, diphasic P wave with tall initial component
Left Atrial Hypertrophy (page 249)
• large, diphasic P wave with wide terminal component
Ventricular Hypertrophy (pages 250-258)
Right Ventricular Hypertrophy (pages 250-252)
• R wave greater than S in V1, but R wave gets
progressively smaller from V1 - V
6.
• S wave persists in V5 and V
6.
• R.A.D. with slightly widened QRS.• Rightward rotation in the horizontal plane.
Left Ventricular Hypertrophy (pages 253-257)
S wave in V1 (in mm.)
+ R wave in V5 (in mm.)
Sum in mm. is more than 35 mm. with L.V.H.
• L.A.D. with slightly widened QRS.• Leftward rotation in the horizontal plane.
Hypertrophy (pages 243 to 258)
Inverted T wave:slants downwardgradually,
but up rapidly.
terminalcomponent
Initialcomponent

342C
op
yrig
ht ©
20
00
CO
VE
R In
c.
Personal Quick Reference Sheets
from: Rapid Interpretation of EKG’sby Dale Dubin, MD
COVER Publishing Co., P.O. Box 07037, Fort Myers, FL 33919, USA
Q wave = Necrosis (significant Q’s only) (pages 272-284)
• Significant Q wave is one millimeter (one small square)wide, which is .04 sec. in duration…… or is a Q wave 1/3 the amplitude (or more)of the QRS complex.
• Note those leads (omit AVR) where significant Q’s are present… see next page to determine infarct location, and to identifythe coronary vessel involved.
• Old infarcts: significant Q waves (like infarct damage) remainfor a lifetime. To determine if an infarct is acute, see below.
ST (segment) elevation = (acute) Injury (pages 266-271) (also Depression)
• Signifies an acute process, ST segment returns tobaseline with time.
• ST elevation associated with significant Q wavesindicates an acute (or recent) infarct.
• A tiny “non-Q wave infarction” appears as significantST segment elevation without associated Q’s. Locate byidentifying leads in which ST elevation occurs (next page).
• ST depression (persistent) may represent “subendocardialinfarction,” which involves a small, shallow area just beneaththe endocardium lining the left ventricle. This is also a varietyof “non-Q wave infarction.” Locate in the same manner as forinfarction location (next page).
T wave inversion = Ischemia (pages 264, 265)
• Inverted T wave (of ischemia) is symmetrical (left halfand right half are mirror images). Normally T wave isupright when QRS is upright, and vice versa.
• Usually in the same leads that demonstrate signs ofacute infarction (Q waves and ST elevation).
• Isolated (non-infarction) ischemia may also be located;note those leads where T wave inversion occurs, thenidentify which coronary vessel is narrowed (next page).
NOTE: Always obtain patient’s previous EKG’s for comparison!
Infarction (pages 259 to 308)
Q
elevation
inversion
T

343C
op
yri
gh
t ©
20
00
CO
VE
R I
nc
.
from: Rapid Interpretation of EKG’sby Dale Dubin, MD
COVER Publishing Co., P.O. Box 07037, Fort Myers, FL 33919, USA
Personal Quick Reference Sheets
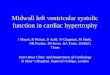
Infarction Location— and —
Coronary Vessel Involvement(pages 259 to 308)
Coronary Artery Anatomy (page 291)
Infarction Location/Coronary Vessel Involvement (pages 278-294)
Posterior• large R with
ST depression in V1 & V2• mirror test or reversed
transillumination test(Right Coronary Artery)(pages 282-286)
Inferior(diaphragmatic)Q’s in inferior leads
II, III, and AVF(R. or L. Coronary Artery)(pages 281, 294)
LateralQ’s in lateral leads I and AVL(Circumflex Coronary Artery)(pages 280, 292)
AnteriorQ’s in V1, V2, V3, and V4(Anterior Descending
Coronary Artery)(pages 278, 292)
anteriordescending
circumflex
Left CoronaryArtery
Right CoronaryArtery

344C
op
yrig
ht ©
20
00
CO
VE
R In
c.
from: Rapid Interpretation of EKG’sby Dale Dubin, MD
COVER Publishing Co., P.O. Box 07037, Fort Myers, FL 33919, USA
Personal Quick Reference Sheets
Pulmonary Embolism (pages 312, 313)
• S1Q
3
3 – wide S in I, large Q and inverted T in III
• acute Right BBB (transient, often incomplete)• R.A.D. and rightward rotation (horizontal plane)• inverted T waves V
1 ➞ V
4 and ST depression in II
Artificial Pacemakers (pages 321-326)
Modern artificial pacemakers have sensing capabilities and also provide aregular pacing stimulus. This electrical stimulus records on EKG as a tinyvertical spike that appears just before the “captured” cardiac response.
• are “triggered” (activated) whenthe patient’s own rhythm ceasesor slows markedly.
• are “inhibited” (cease pacing)if the patient’s own rhythmresumes at a reasonable rate.
• will “reset” pacing(at same rate) tosynchronize with apremature beat.
(Asynchronous) Epicardial PacemakerVentricular impulse not linked to atrial activity.
Atrial Synchronous Pacemaker (page 323)P wave sensed, then after a brief delay,
ventricular impulse is delivered.
External Non-invasive Pacemaker(page 326)
Ventricular Pacemaker (page 323)(electrode in Right Ventricle)
Atrial pacemaker (page 323)
Dual Chamber (AV sequential) Pacemaker(page 323)
Miscellaneous (pages 309 to 328)
T
PVC stops pacemaker, but…
Dem
and
Pac
emak
ers:
(pa
ge 3
22)
Pacemaker Impulse (delivery modes)pacemaker resumes in step
with premature beat.
▼ ▼ ▼ ✕
▲ ▲ ▲
pacemaker spikes
sinus rhythm ceases
patient’s sinus rhythminhibits pacemaker

345C
op
yri
gh
t ©
20
00
CO
VE
R I
nc
.Personal Quick Reference Sheets
from: Rapid Interpretation of EKG’sby Dale Dubin, MD
COVER Publishing Co., P.O. Box 07037, Fort Myers, FL 33919, USA
Miscellaneous continued
U
wide,notched
P
wide QRS
long QT interval
ST
ElectrolytesPotassium (pages 314, 315)
Increased K+ (page 314)(hyperkalemia)
Decreased K+ (pages 315)(hypokalemia)
Calcium (page 316)
Digitalis (pages 317-319)
EKG appearance with digitalis (“digitalis effect”)• remember Salvador Dali.• T waves depressed or inverted.• QT interval shortened.
Digitalis Excess Digitalis Toxicity(blocks) (irritable foci firing rapidly)• SA Block • Atrial Fibrillation• P.A.T. with Block • Junctional or Ventricular Tachycardia• AV Blocks • multiple P.V.C.’s• AV Dissociation • Ventricular Fibrillation
Quinidine (page 320)
• EKG appearance with quinidine (page 320)
• Excess quinidine or other medicationsthat block potassium channels (or evenlow serum potassium) may initiateTorsades de Pointes (page 158) Torsades de Pointes
moderate extreme
moderate extreme
Hyper Ca++ Hypo Ca++
short QT prolonged QT
wide,flat P
peaked T
wide QRS
no P
flat T
Quinidine Effects
prominentU wave
QRS widens
U wav
e

346C
op
yrig
ht ©
20
00
CO
VE
R In
c.
Personal Quick Reference Sheets
from: Rapid Interpretation of EKG’sby Dale Dubin, MD
COVER Publishing Co., P.O. Box 07037, Fort Myers, FL 33919, USA
Dubin’s Quickie Conversion—for—
Patient’s Weight from Pounds to Kilograms
Patient wt. in kg. = Half of patient’s wt. (in lb.) minus 1/10 of that value.
Examples: 180 lb. patient 160 lb. patient 140 lb. patient(becomes 90 minus 9) (becomes 80 minus 8) (becomes 70 minus 7)
is 81 kg is 72 kg is 63 kg.
Modified Leads—for—
Cardiac MonitoringLocations are approximate. Some minor adjustment of electrode posi-
tions may be necessary to obtain the best tracing. Identify the specificlead on each strip placed in the patient’s record.
IdentificationSensor Electrode Letter Color (inconsistent)
+ R (or RA) red– L (or LA) white
G* G (or RL) variable* Ground, Neutral or Reference
Practical Tips
Modified Lead I Modified Lead II
G
G
G
G
Conventional Lead MCl1
To make this MCl6
move ●● electrodeto same(mirror)position onthe patient’sleft chest.
+