Embed Size (px)
Citation preview
1
بسم الله الرحمن
الرحیم
Atrial and Ventricular Hypertrophy
ECG Features and Common Causes
ALI BARABADI
University of Guilan
Aims and Objectives.
Understand pathophysiology of types of hypertrophy.
Common patient presentation and symptoms.
ECG appearances associated with different types of hypertrophy.
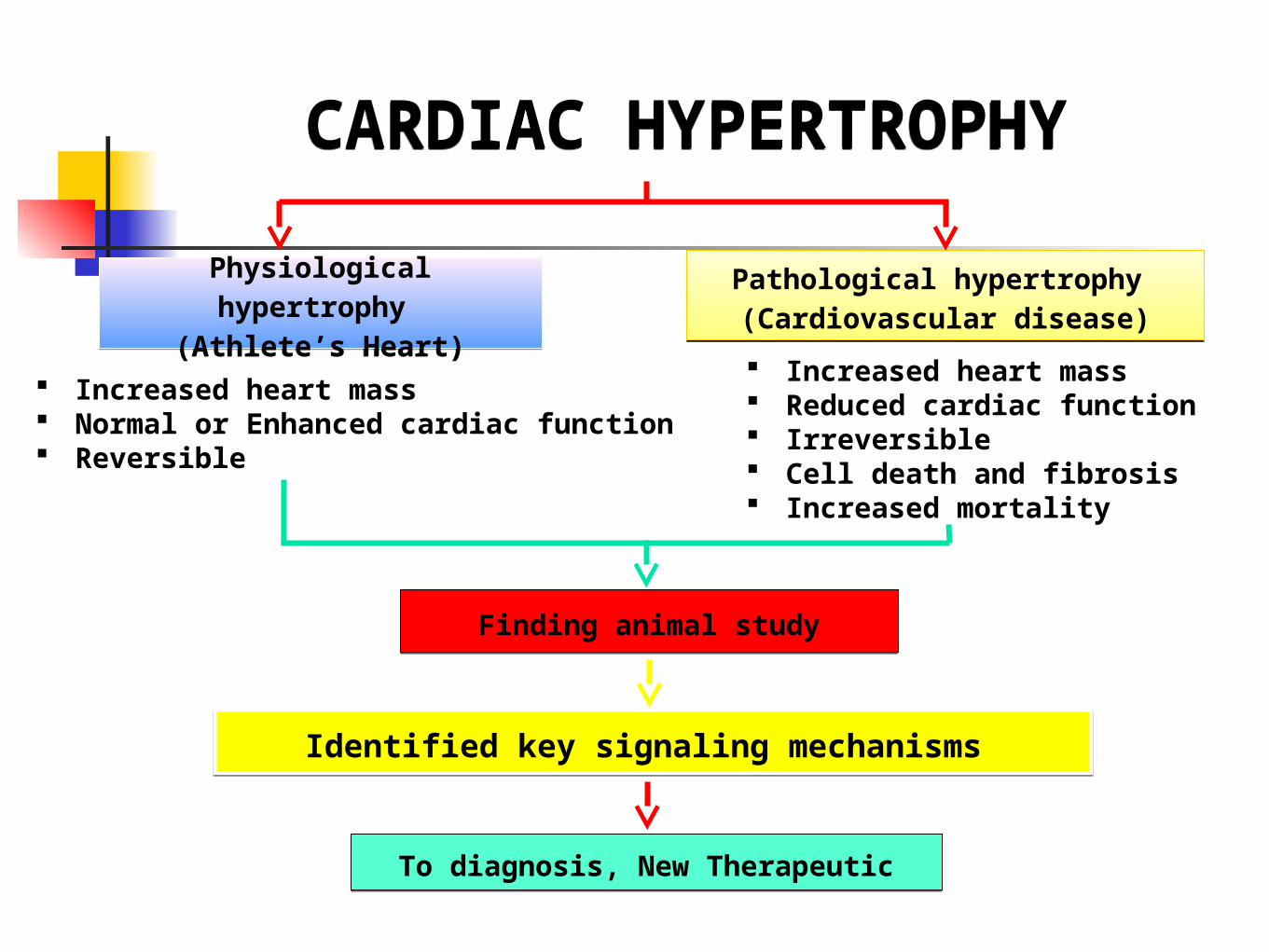
CARDIAC HYPERTROPHY
CARDIAC HYPERTROPHY
Physiological hypertrophy
(Athlete’s Heart)
Physiological hypertrophy
(Athlete’s Heart)
Pathological hypertrophy (Cardiovascular disease)
Pathological hypertrophy (Cardiovascular disease)
Finding animal studyFinding animal study
Identified key signaling mechanisms Identified key signaling mechanisms
To diagnosis, New TherapeuticTo diagnosis, New Therapeutic
Increased heart mass Normal or Enhanced cardiac function Reversible
Increased heart mass Reduced cardiac function Irreversible Cell death and fibrosis Increased mortality
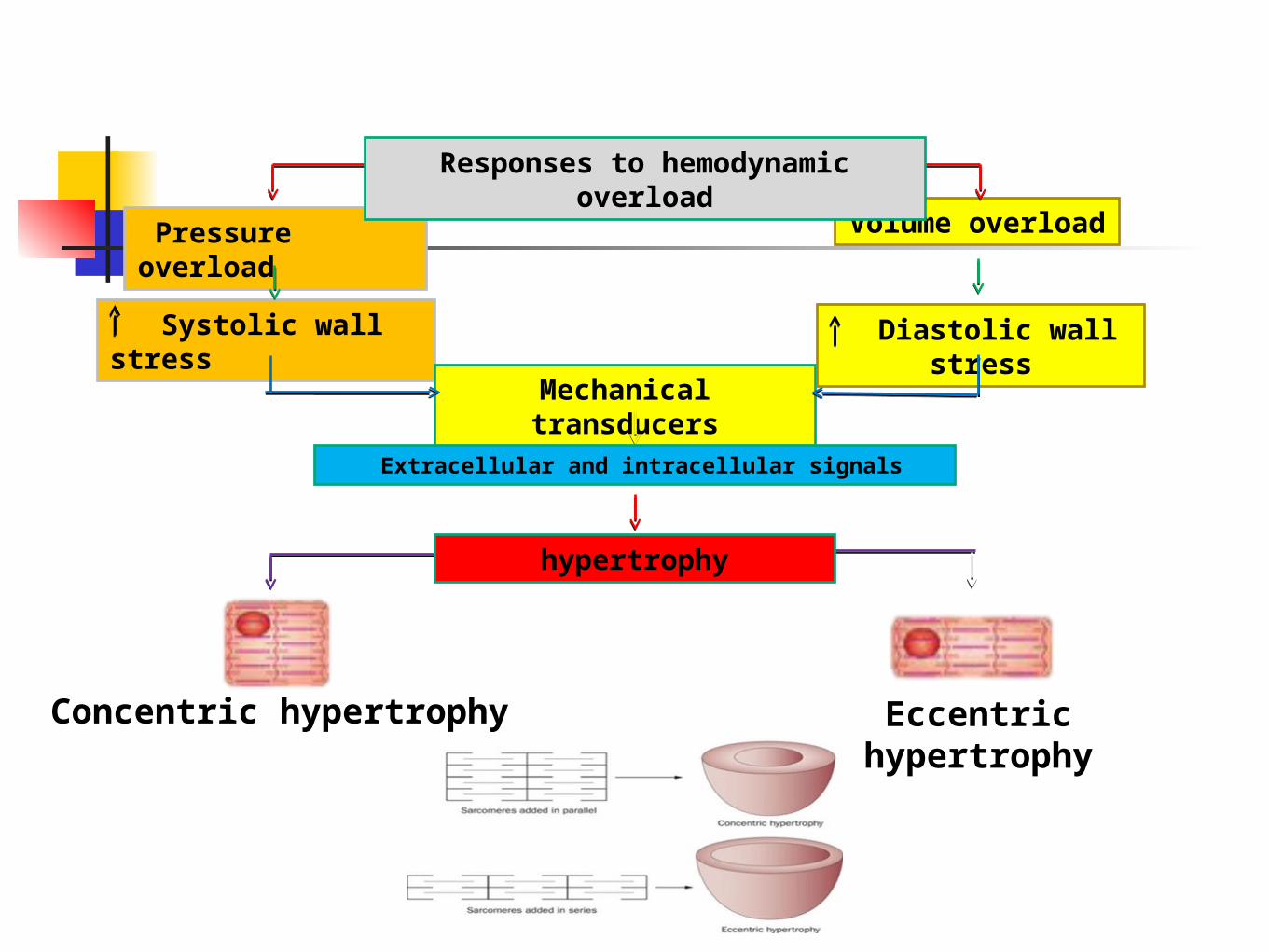
Pressure overload
Systolic wall stress
Mechanical transducers
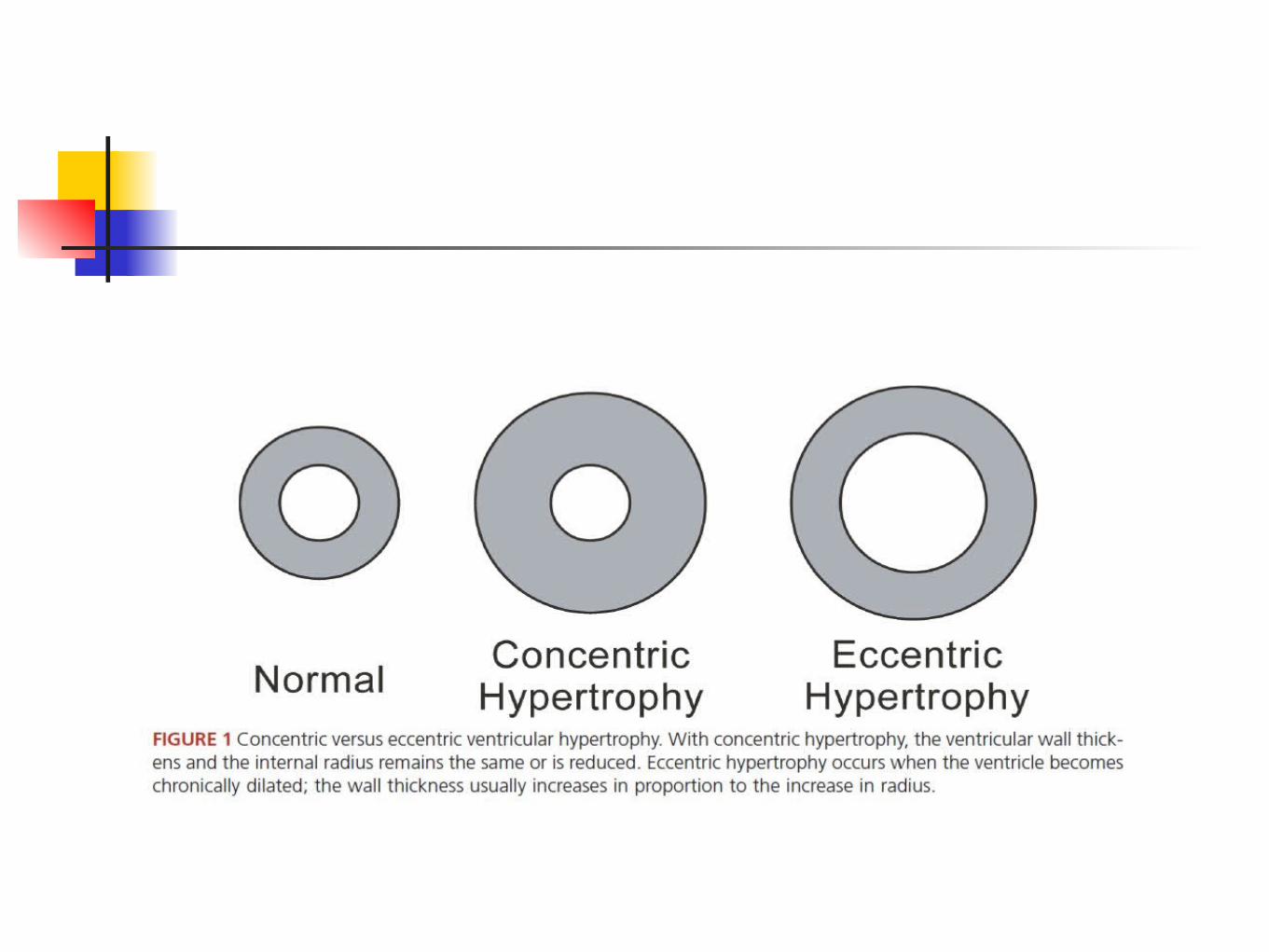
Eccentric hypertrophy
Volume overload
Diastolic wall stress
Concentric hypertrophy
Responses to hemodynamic overload
hypertrophy
Extracellular and intracellular signals
7
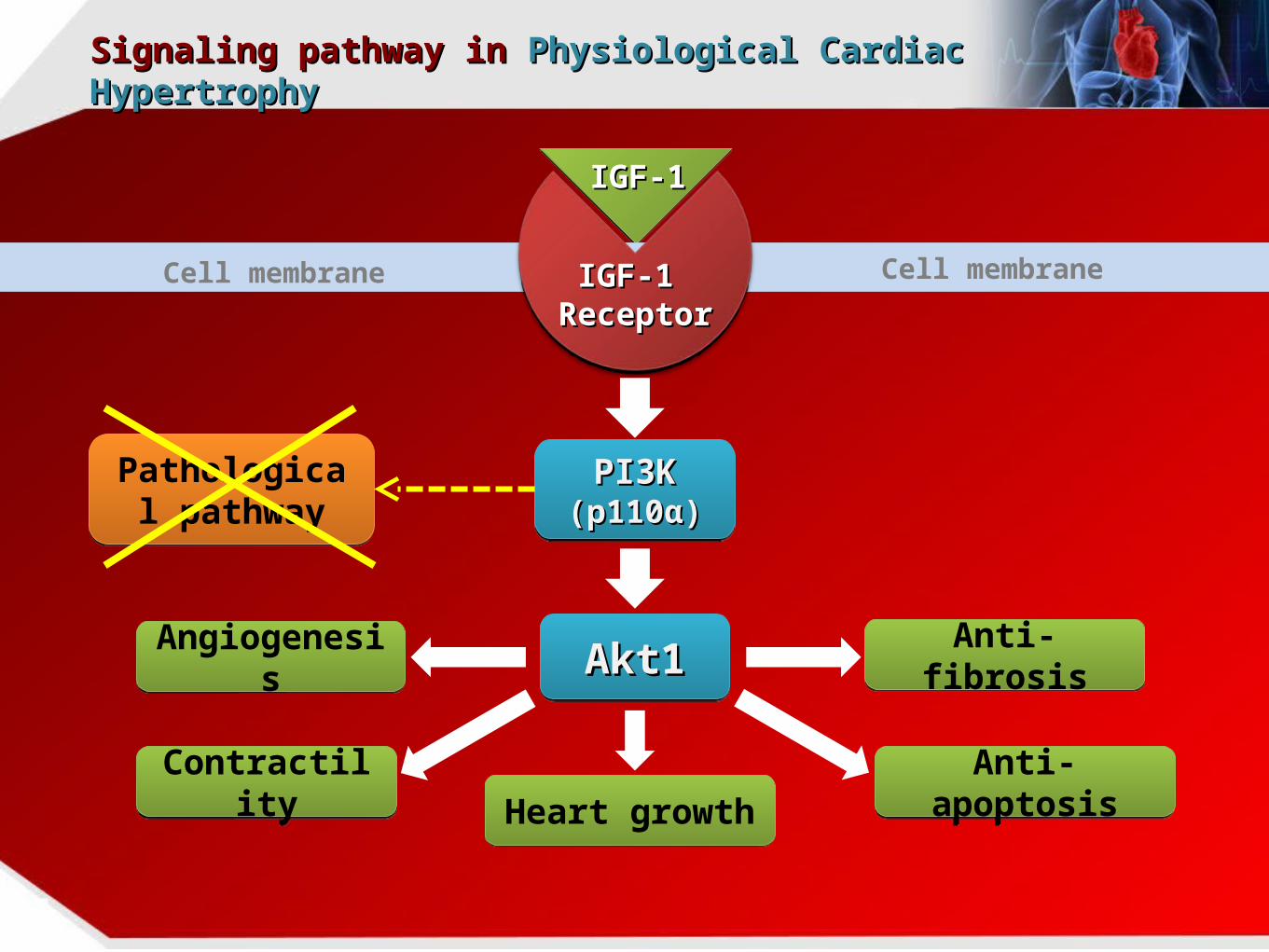
Signaling pathway in Signaling pathway in Physiological Cardiac Physiological Cardiac HypertrophyHypertrophy
PI3K PI3K (p110(p110αα))
PI3K PI3K (p110(p110αα))
Akt1Akt1Akt1Akt1Angiogenesis
Angiogenesis
Contractility
Contractility Heart
growthHeart
growth
Anti-apoptosis
Anti-apoptosis
Anti-fibrosisAnti-fibrosis
Pathological pathway
Pathological pathway
IGF-1IGF-1
IGF-1 IGF-1 ReceptorReceptor
Cell membrane Cell membrane
8
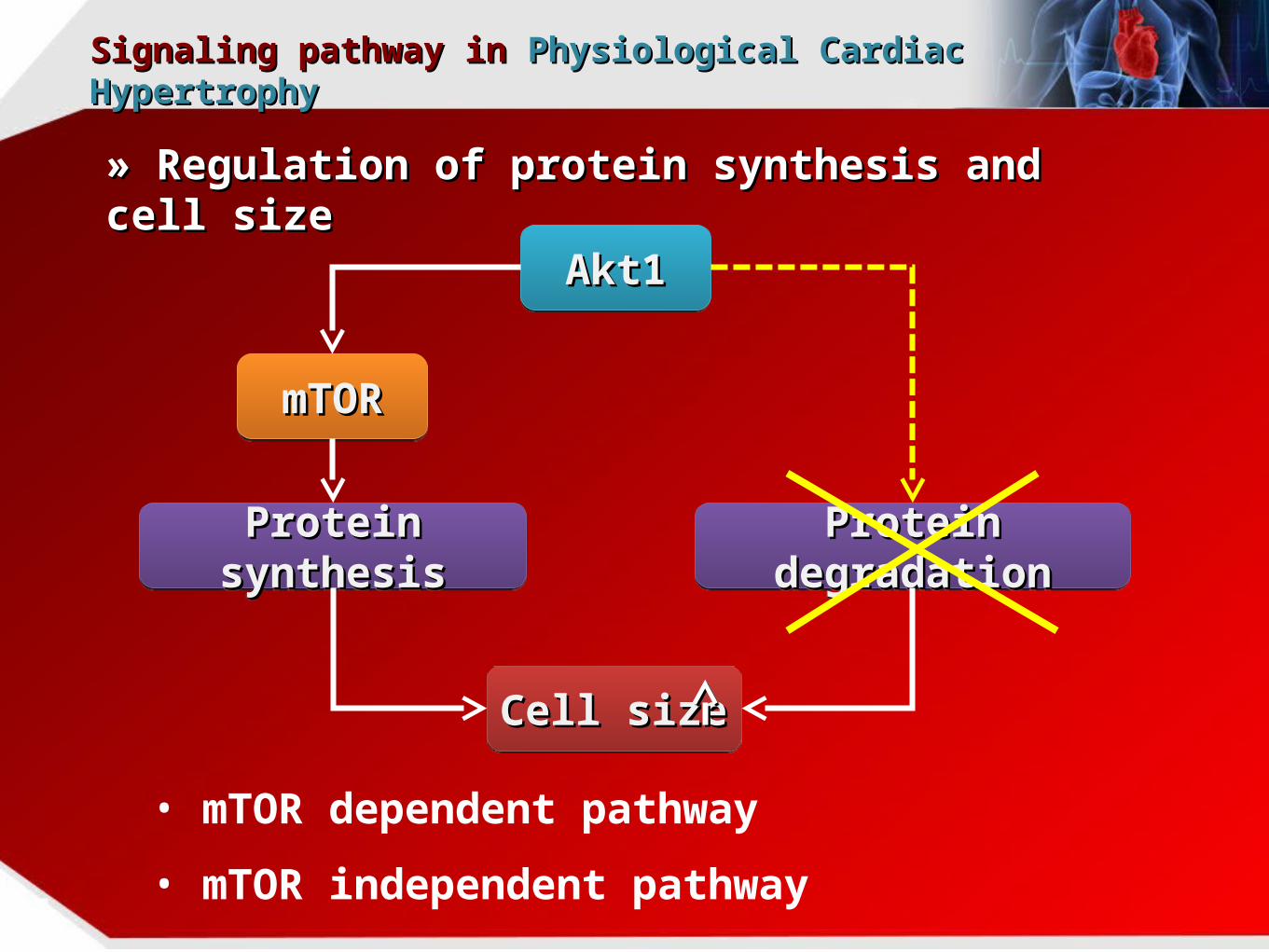
Signaling pathway in Signaling pathway in Physiological Cardiac Physiological Cardiac HypertrophyHypertrophy
• mTOR dependent pathway
• mTOR independent pathway
» Regulation of protein synthesis and cell » Regulation of protein synthesis and cell sizesize
Akt1Akt1Akt1Akt1
mTORmTORmTORmTOR
Protein synthesisProtein synthesisProtein synthesisProtein synthesis Protein degradationProtein degradationProtein degradationProtein degradation
Cell sizeCell sizeCell sizeCell size
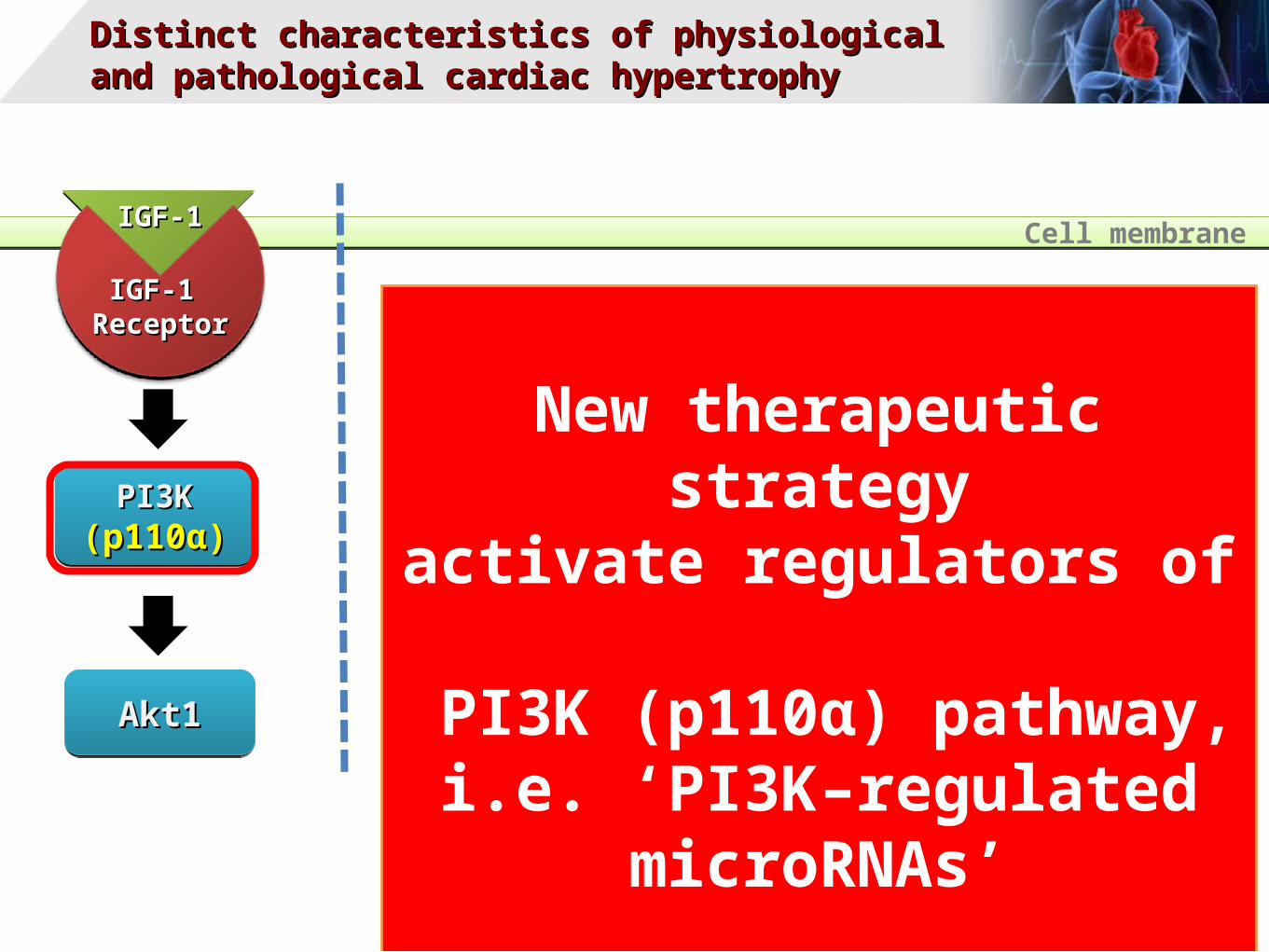
Distinct characteristics of physiological Distinct characteristics of physiological and pathological cardiac hypertrophyand pathological cardiac hypertrophy
PI3K PI3K (p110(p110αα))
PI3K PI3K (p110(p110αα))
Akt1Akt1Akt1Akt1
New therapeutic strategyactivate regulators of
PI3K (p110α) pathway,i.e. ‘PI3K–regulated microRNAs’
IGF-1IGF-1
IGF-1 IGF-1 ReceptorReceptor
Cell membrane
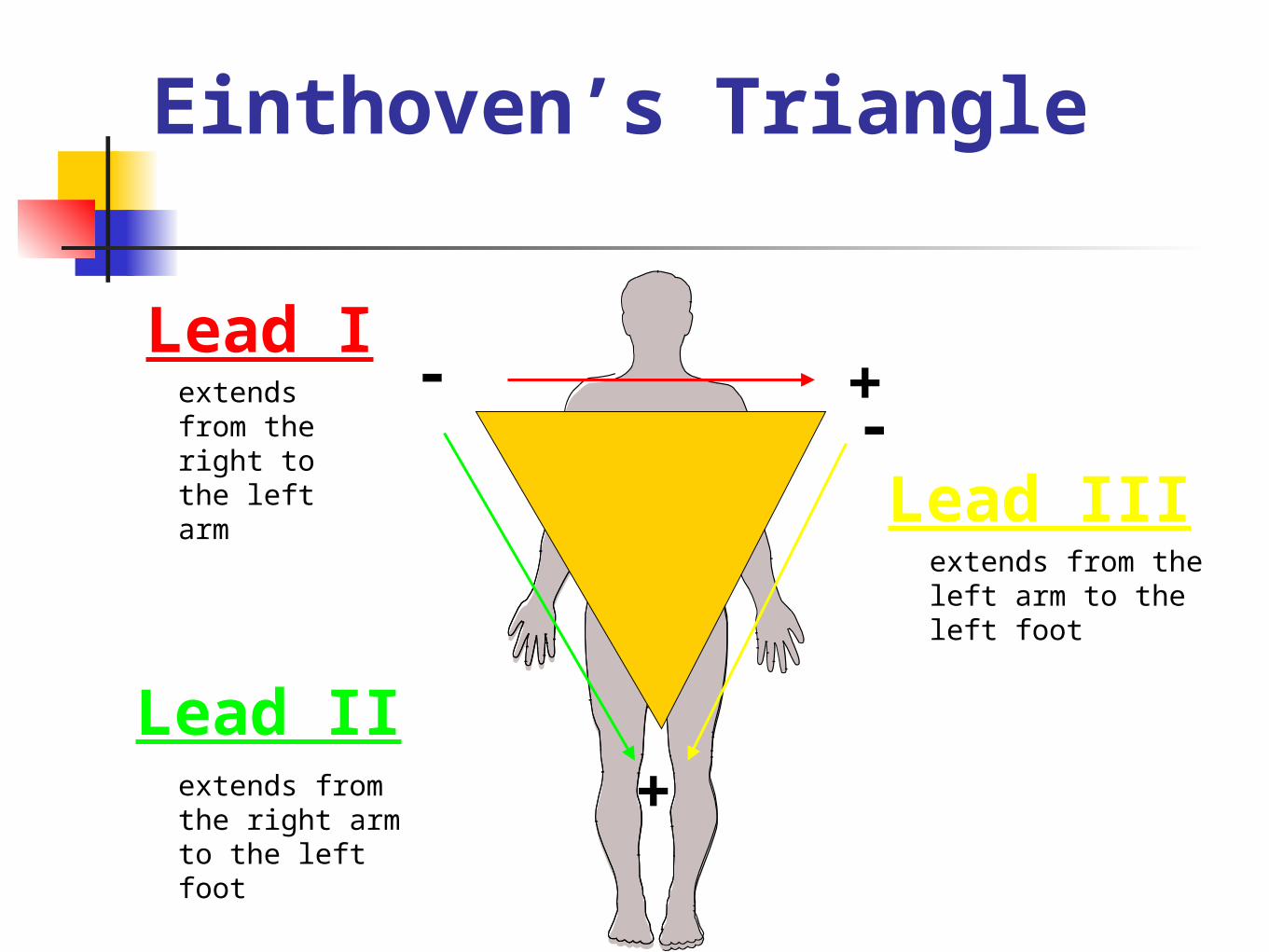
Lead Iextends from the right to the left arm
Lead IIextends from the right arm to the left foot
Lead IIIextends from the left arm to the left foot
Einthoven’s Triangle
+-
+
-
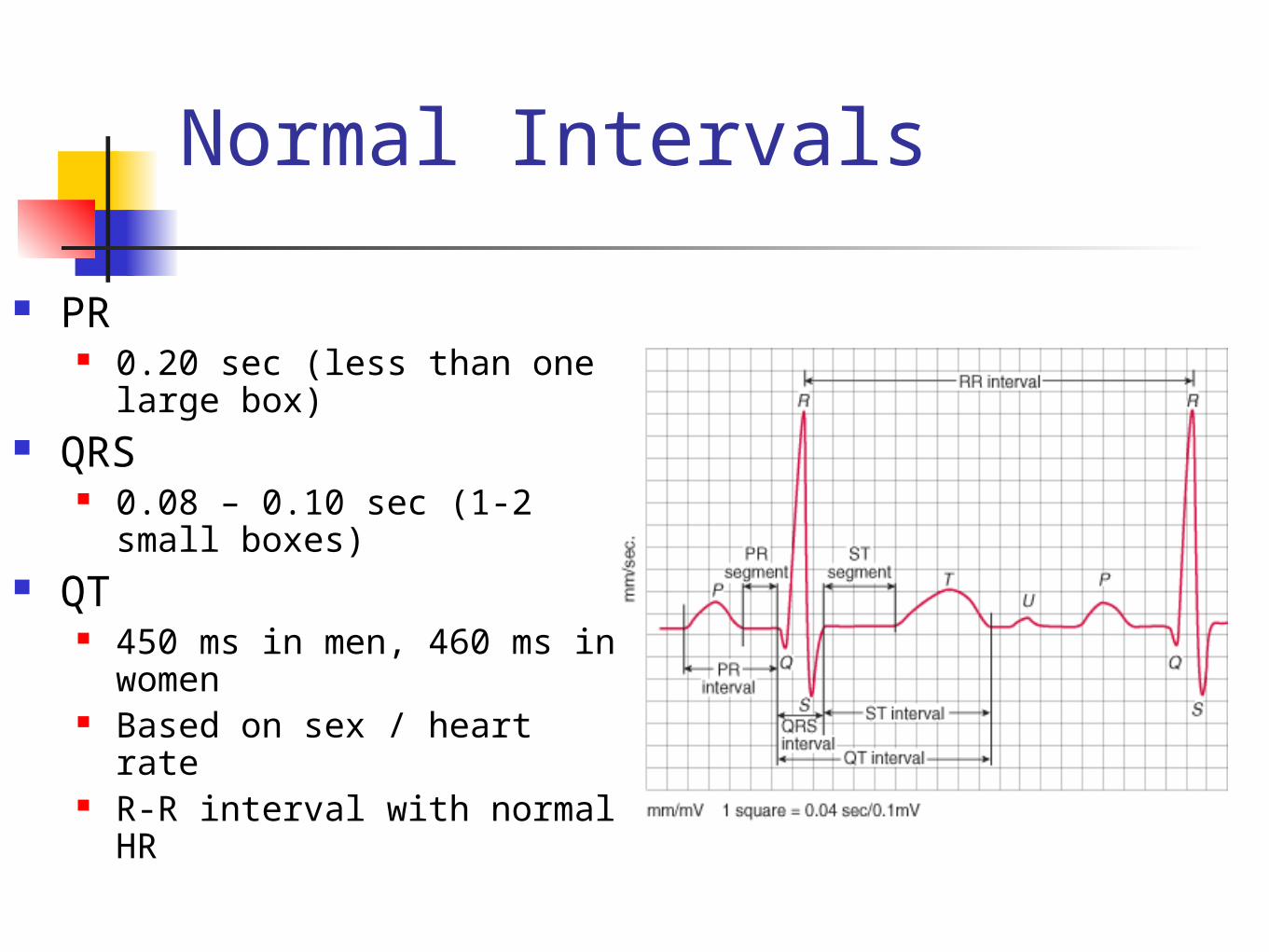
Normal Intervals
PR 0.20 sec (less than one large
box) QRS
0.08 – 0.10 sec (1-2 small boxes)
QT 450 ms in men, 460 ms in
women Based on sex / heart rate R-R interval with normal HR
Left Atrial Hypertrophy / Enlargement.
Thickening of wall. Dilatation of
chamber (enlargement).
Increased volume. Increased muscle
mass.
Some causes.
Mitral and / or aortic valve disease. Left ventricular systolic and diastolic
dysfunction. Cardiomyopathy - hypertrophic /
dilated. Atrial fibrillation. Left atrial mass. Hypertension.
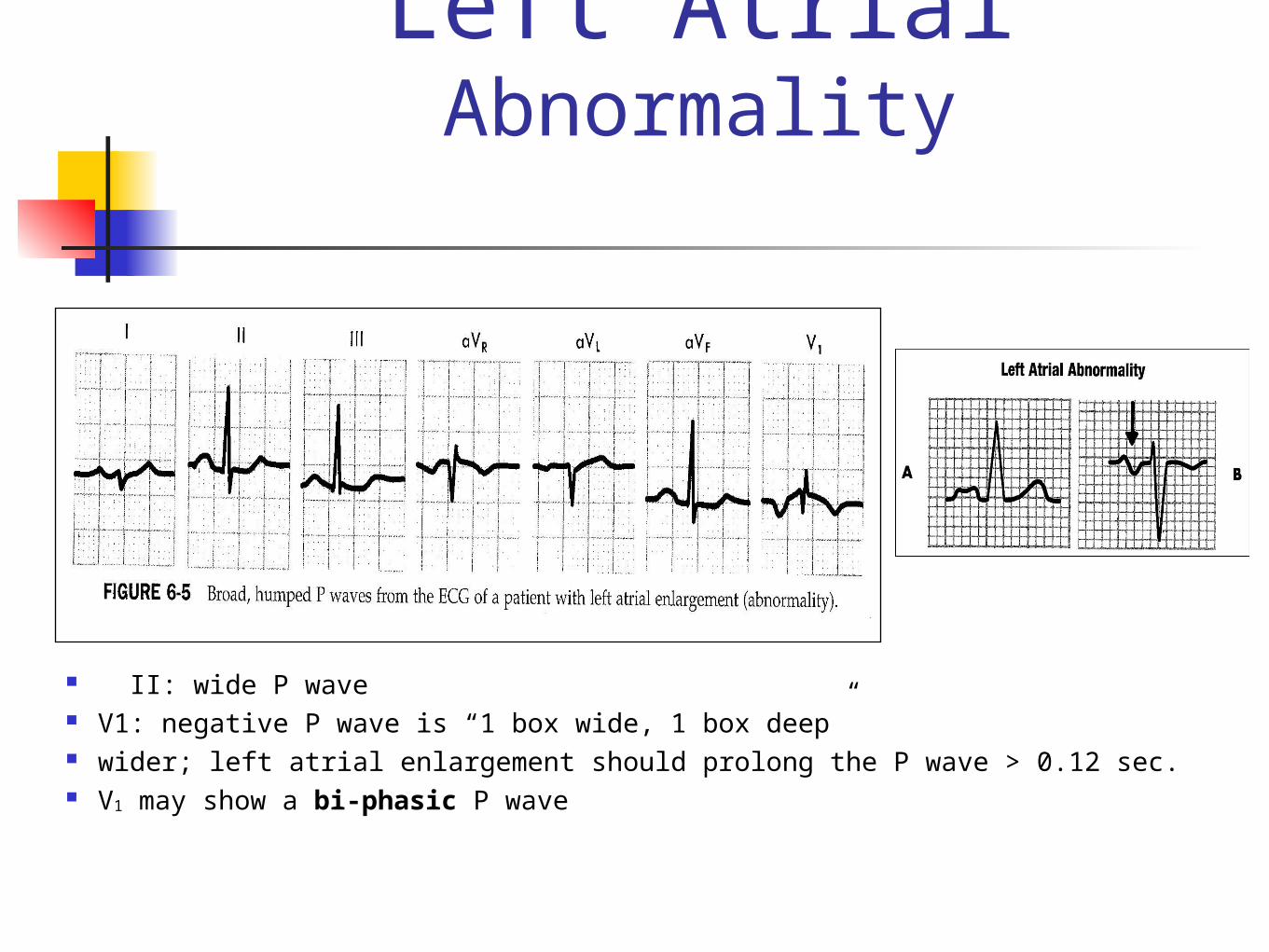
Left Atrial Abnormality
II: wide P wave V1: negative P wave is “1 box wide, 1 box deep” wider; left atrial enlargement should prolong the P wave > 0.12 sec. V1 may show a bi-phasic P wave
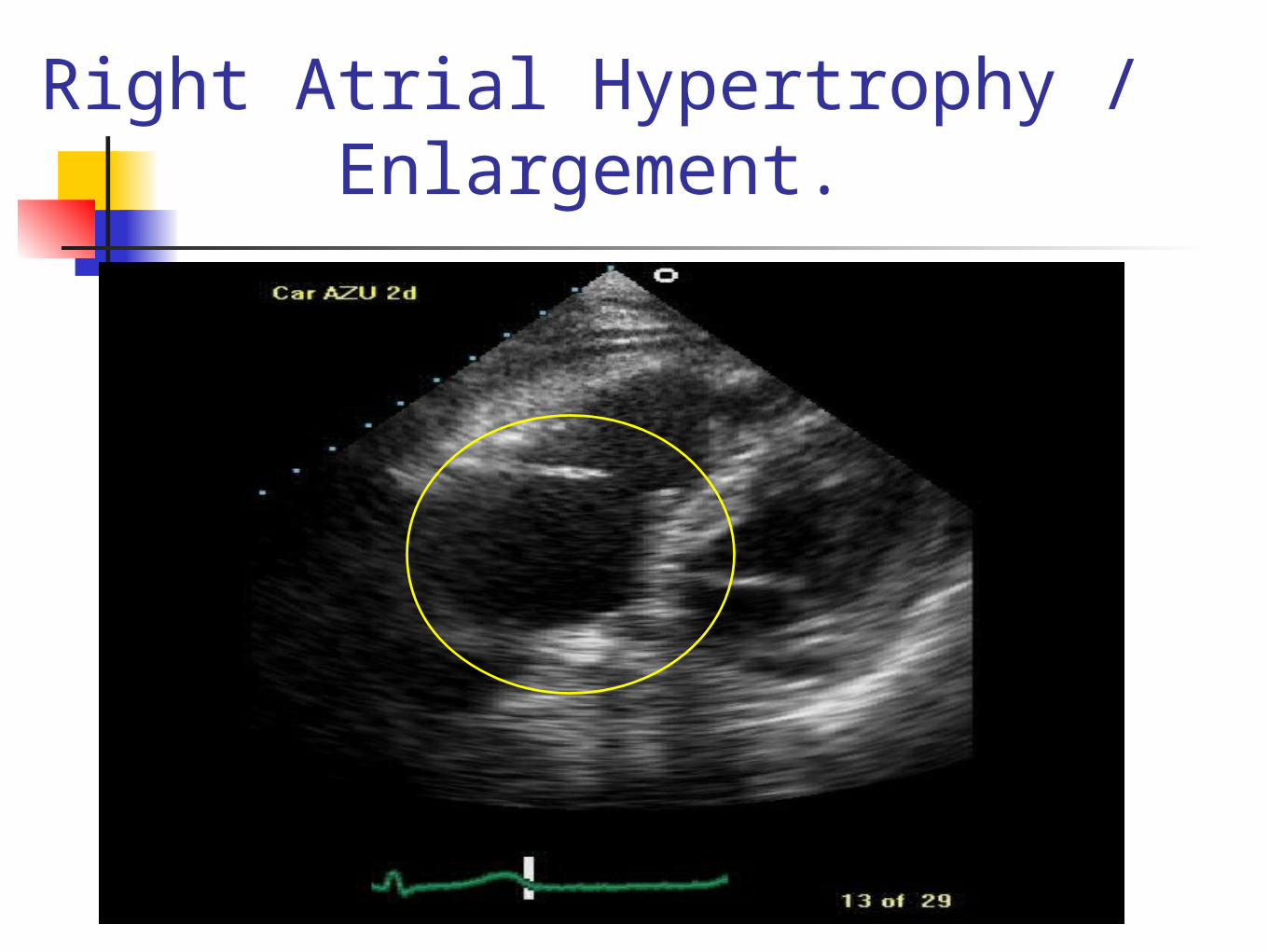
Right Atrial Hypertrophy / Enlargement.
Some causes.
Tricuspid and / or pulmonary valve disease.
Lung disease. Congenital heart disease RV systolic and diastolic dysfunction. Mitral stenosis (pressure back-up).
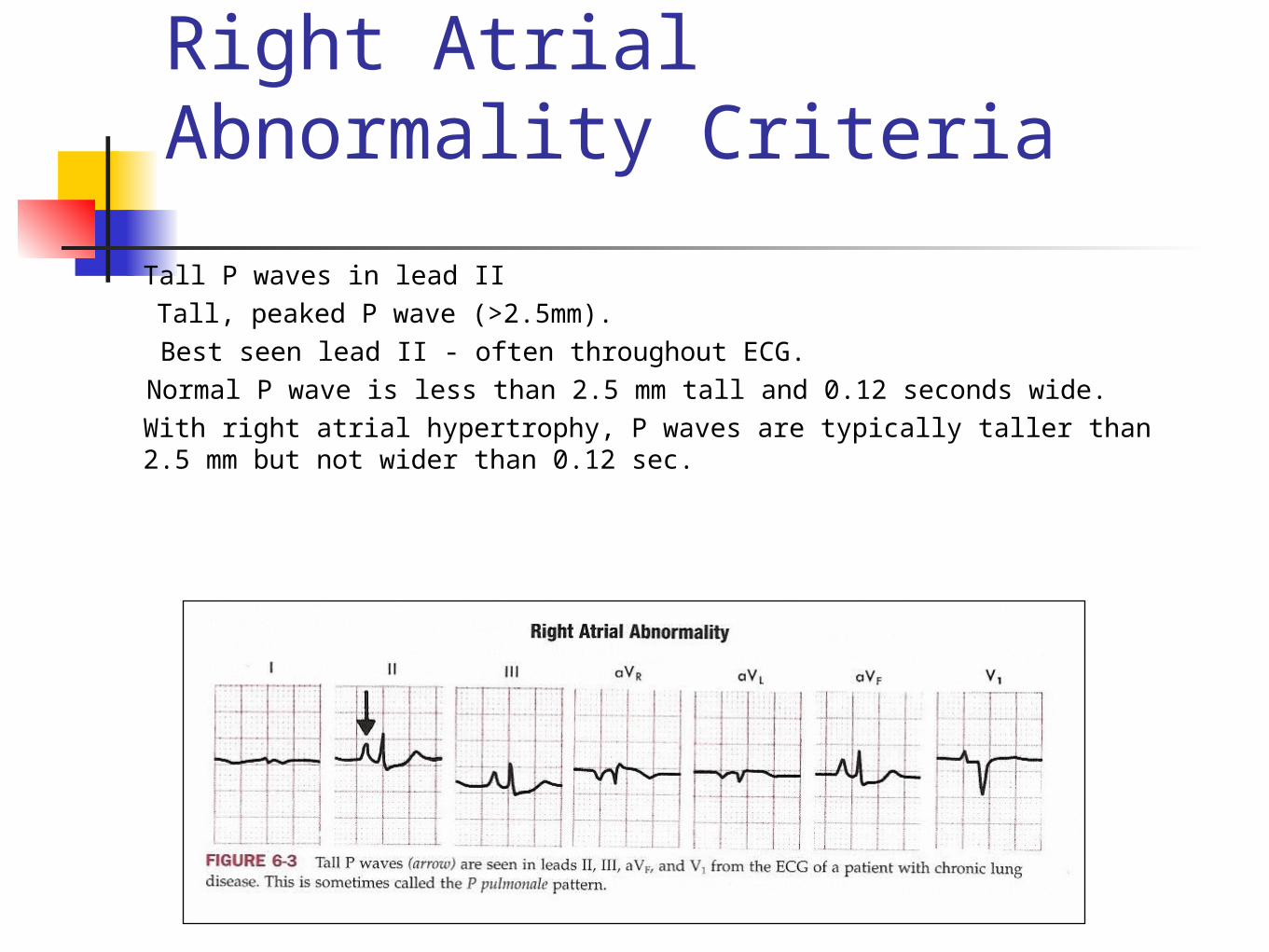
Right Atrial Abnormality Criteria
Tall P waves in lead II Tall, peaked P wave (>2.5mm). Best seen lead II - often throughout ECG. Normal P wave is less than 2.5 mm tall and 0.12 seconds wide.With right atrial hypertrophy, P waves are typically taller than 2.5 mm but not wider than 0.12 sec.
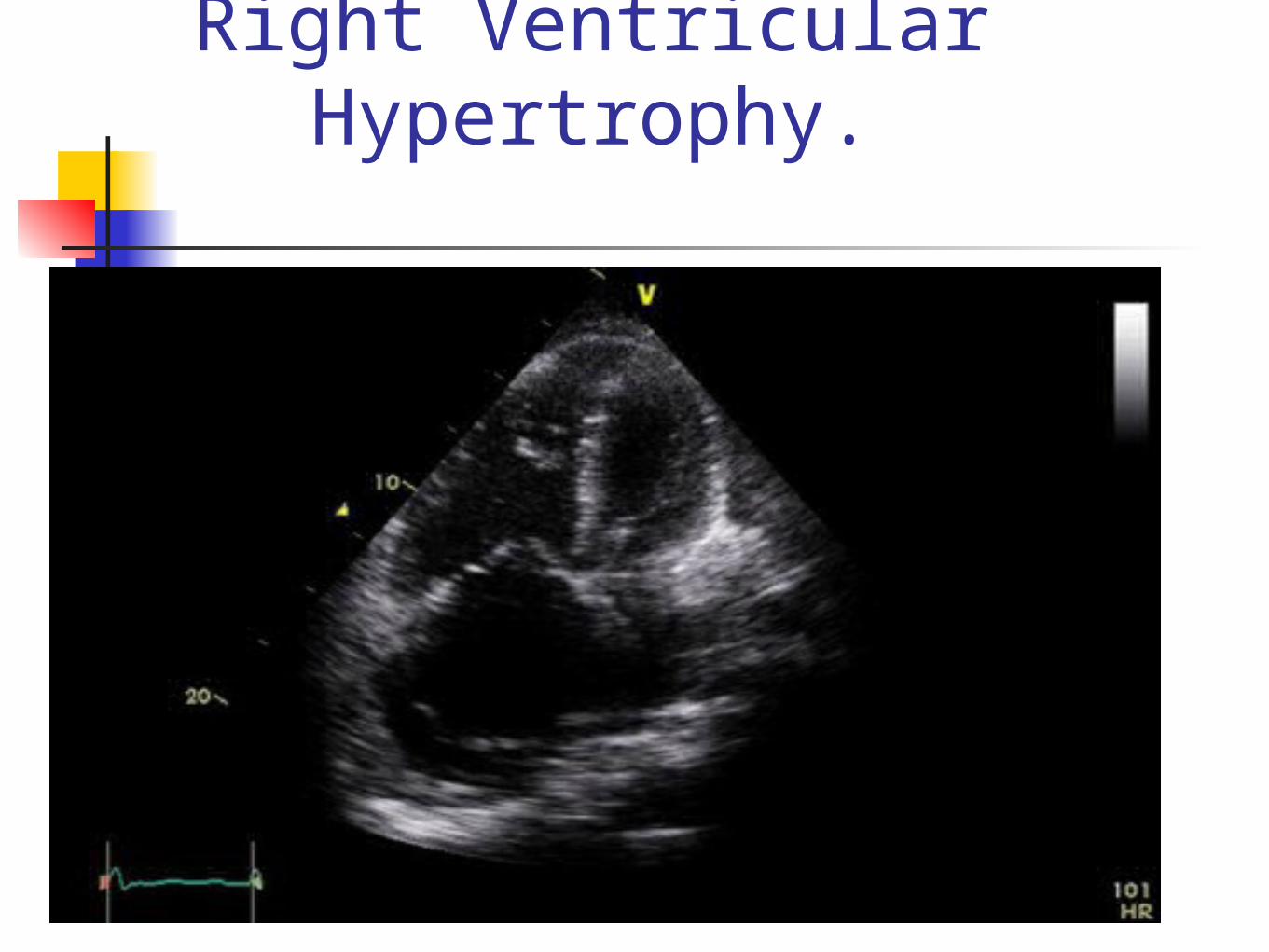
Right Ventricular Hypertrophy.
Some causes of RVH.
Pulmonary hypertension Mitral stenosis. Pulmonary valve disease. Congenital heart disease RV systolic dysfunction
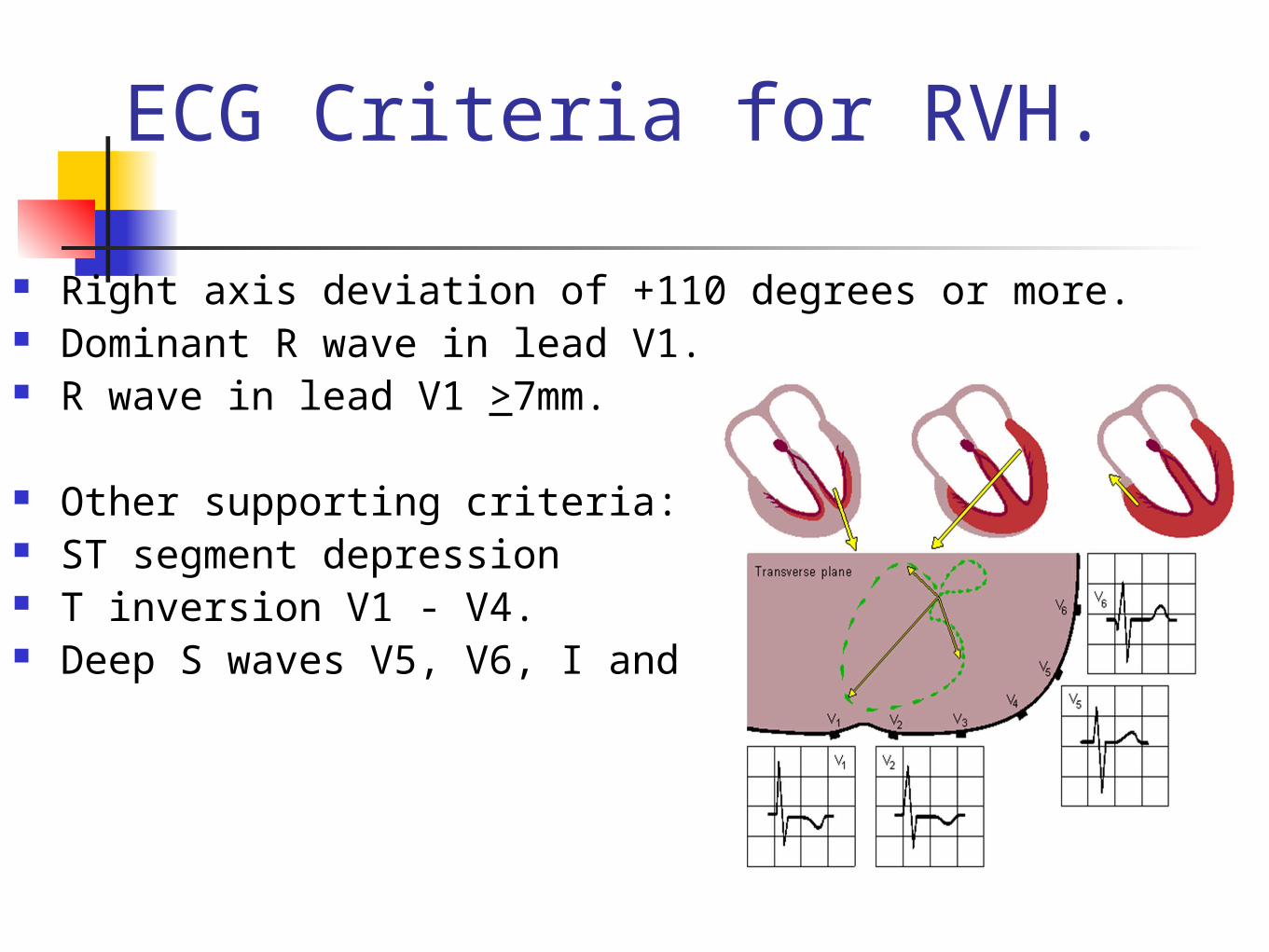
ECG Criteria for RVH.
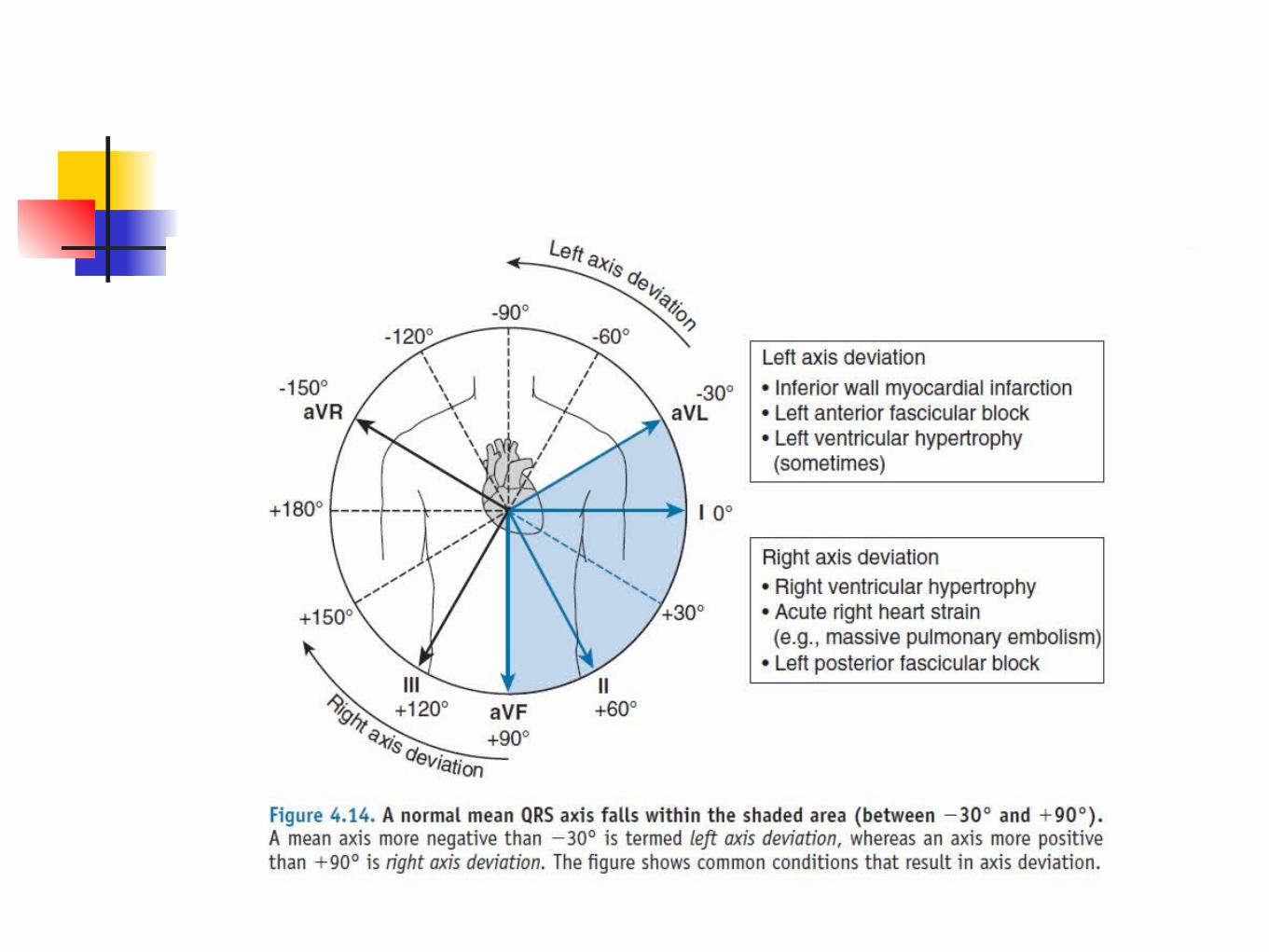
Right axis deviation of +110 degrees or more. Dominant R wave in lead V1. R wave in lead V1 >7mm.
Other supporting criteria: ST segment depression T inversion V1 - V4. Deep S waves V5, V6, I and aVL.
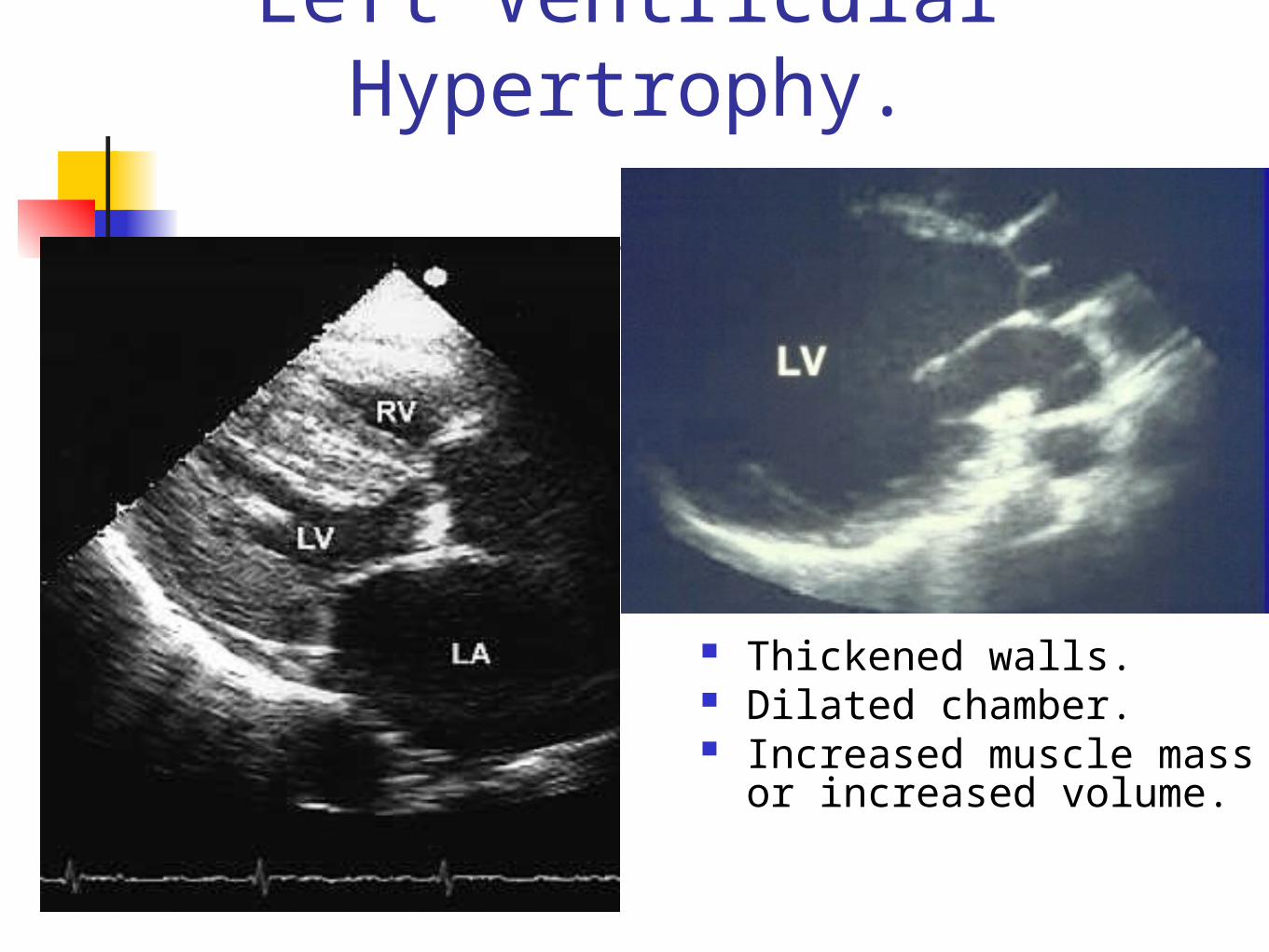
Left Ventricular Hypertrophy.
Thickened walls. Dilated chamber. Increased muscle mass
or increased volume.
Some causes of LVH.
Aortic valve disease. Coarctation of the aorta. Cardiomyopathy - dilated,
hypertrophic. Hypertension. Heart Failure - systolic.
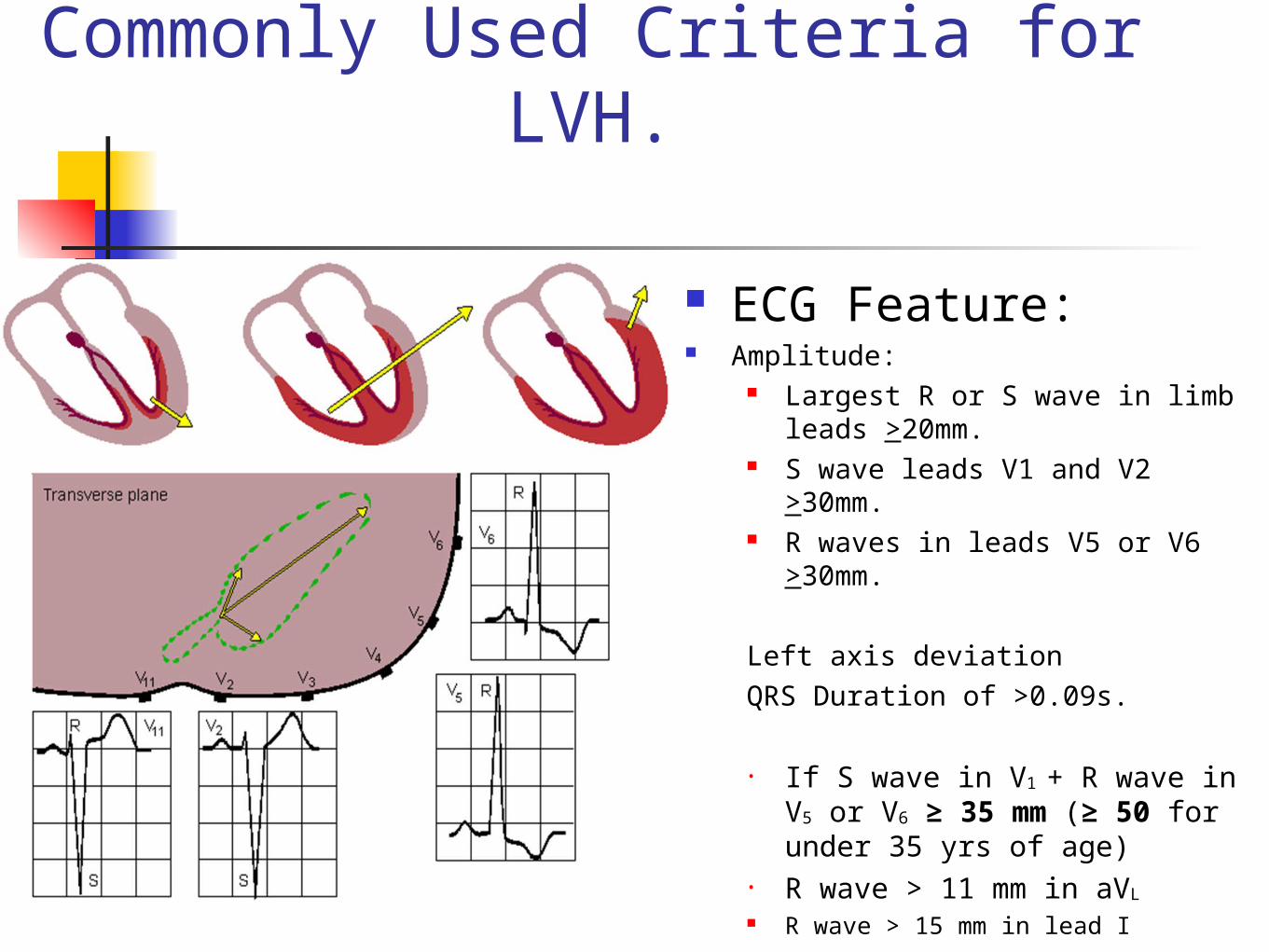
Commonly Used Criteria for LVH.
ECG Feature: Amplitude:
Largest R or S wave in limb leads >20mm.
S wave leads V1 and V2 >30mm.
R waves in leads V5 or V6 >30mm.
Left axis deviationQRS Duration of >0.09s.
• If S wave in V1 + R wave in V5 or V6 ≥ 35 mm (≥ 50 for under 35 yrs of age)
• R wave > 11 mm in aVL
R wave > 15 mm in lead I
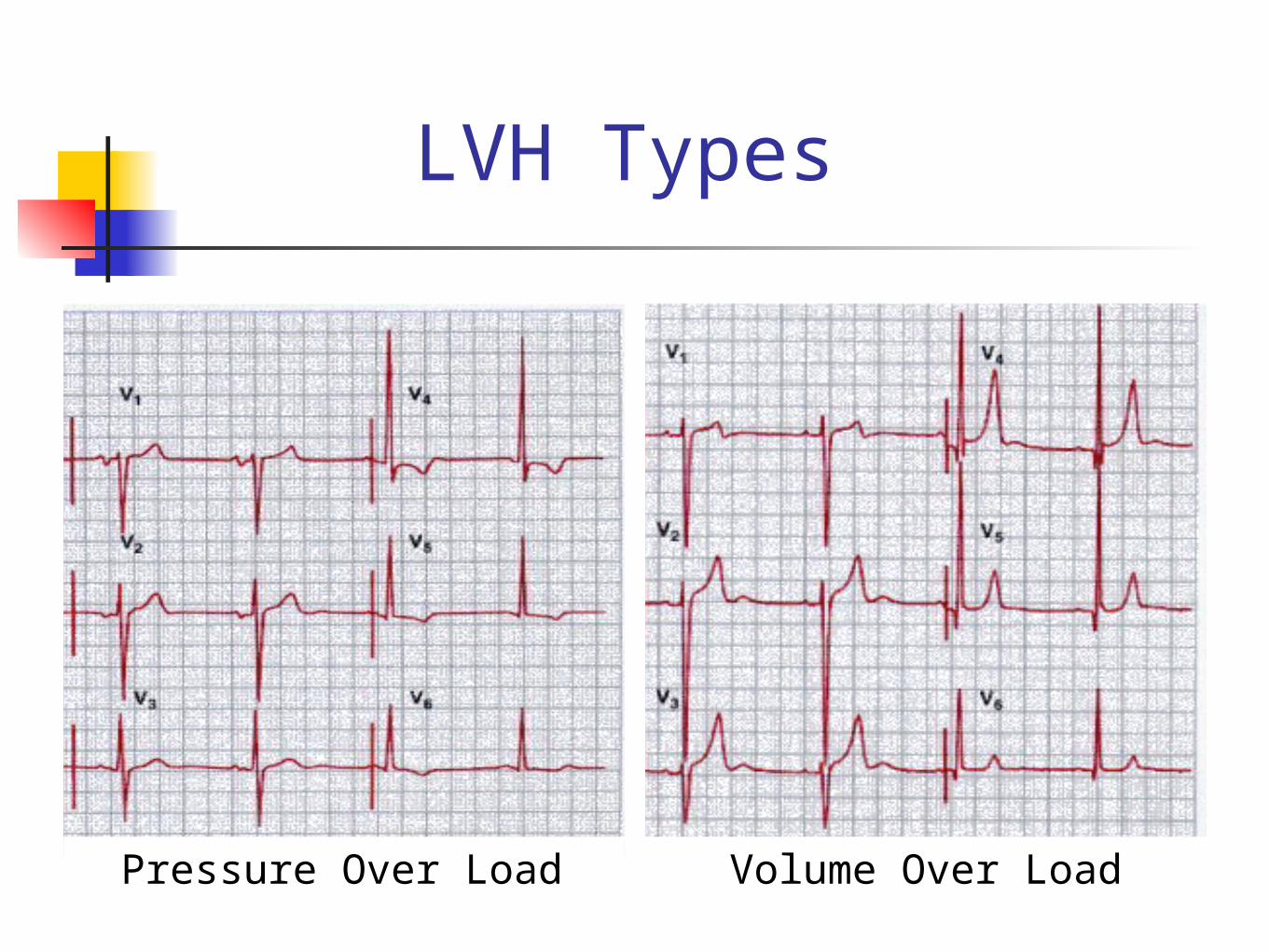
LVH Types
Volume Over LoadPressure Over Load
LVH Types
Pressure Over load Like in hypertension, IHD) Ischemic heart
disease( LV strain pattern – ST depression with T ↓
in V5, V6, L1 and aVL leadsVolume Over load Like in Mitral or Aortic regurgitation Shows prominent positive T waves in V5, V6, L1 and aVL
Conclusion.
LAH – ECG appearance and common causes.
RAH – appearance and causes. LVH – appearance, certainty of
diagnosis, causes and pitfalls. RVH – appearance, causes and
pitfalls.
Web Site Instruction
Berne and Levy Physiology, 6th Edition Bruce M. Koeppen, Bruce A. Stanton R. Klablunde -Cardiovascular Physiology Concepts -Lippincott (2005) Leonard S. Lilly-Pathophysiology of Heart Disease_ A Collaborative Project of Medical Students a
nd Faculty , Fifth Edition-Lippincott Williams & Wilkins (2010) (Expert consult) Robert O Bonow_ Eugene Braunwald_ et al-Braunwald's heart disease _ a textboo
k of cardiovascular medicine-Elsevier Saunders (2012) http://www.madsci.com/manu/ekg_hypr.htm http://library.med.utah.edu/kw/ecg/ecg_outline/Lesson7/index.html http://library.med.utah.edu/kw/ecg/ecg_outline/Lesson8/index.html

Thank you
31


















