Embed Size (px)
Citation preview

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 1
Welcome to
Copyright ©2014 EDUCATA. This presentation is not to be copied in whole or in part without the express permission of EDUCATA.
How to Navigate EDUCATA
From Vent to Rehab: Treatment of the ICU Patient
Part II: Understanding Diagnostic Testing, Including Lab Assessment
and Priorities in Treatment
Ellen Hillegass PT, Ed.D., CCS, FAACVPR, FAPTA

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 2
Assessment of Chart Findings
What is important?
What are the implications?
Components of Chart
• Diagnostic testing
– Cardiac diagnostics
– Pulmonary diagnosticsPulmonary diagnostics
• Laboratory information
• Other
Diagnostic Testingcardiac
• Holter monitoring
• Echocardiography
• Chest x‐ray
• Coronary catheterization
• Intravascular lt d i i
• 12 lead ECG
• Exercise testing
• Stress thallium
ultrasound imaging (IVUS)
• Multislice CT imaging

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 3
Holter Monitor
Holter Monitor
• Used to assess for arrhythmias, particularly life‐threatening arrhythmias.
• Worn for 24 – 48 hours.
• Used on outpatient basis. Patient may have described symptoms of:
– Palpitations
– Syncope
– Skips in pulse
Echocardiography

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 4
Echocardiography
• Valve dysfunction
– Mitral most common, aortic, pulmonic or tricuspid
• Chamber size determined
Noninvasive diagnostic test to determine:
• Ventricular size/ventricular hypertrophy
• Ejection fraction
– EF > 55 – 60 is normal
– 40 – 60 is considered dysfunction
– < 30 – 40 is failure
• Can be used with stress test for diagnosis of perfusion.
Chest X-Ray
Chest X-Ray
• Chest x‐ray looks at heart and lungs to identify:
– Rib fractures– Rib fractures
Ch i l di
– Hyperinflation
Fl id/ i filt t– Chronic lung disease
– Flattened diaphragm
• Limitations of CXR:
– Only 2‐dimensional.
– Cannot see behind structures.
– Chronic lung disease
– Flattened diaphragm
– Fluid/or infiltrates
– Size of heart

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 5
12 Lead ECG
Abnormal 12 Lead ECG
Exercise Testing
• Utilized to evaluate chest pain/ischemia.
• Diagnostic for males, requires additional diagnostic procedures for improved
iti it / ifi it f f lsensitivity/specificity for females.
– Thallium or stress echo
• Utilized with metabolic cart to determine true max VO2 or to determine cardiac versus pulmonary impairment.

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 6
Exercise Testing With Metabolic Cart
Stress Thallium
Stress Thallium
• Radionucleotide used to assess perfusion defects during stress tests.
• Inject dye at peak exercise, then patient is placed supine under a nuclear scanner toplaced supine under a nuclear scanner to assess for distribution of dye.
• Patient returns 3‐4 hours later and another scan is performed at rest to see if redistribution has occurred.
• Can also do test with pharmacologic stress.

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 7
Pharmacologic Stress Test
• Medications used:
– Adenosine
– Dipyridamole
– Dobutamine
• Used when patient cannot perform exercise.
• Adenosine and dipyridamole cause vasodilation, whereas dobutamine increases work on heart.
Coronary Catheterization
Coronary Catheterization
• Performed when coronary blockages are suspected.
– As result of stress test.
Upon ER admission due to chest pain or abnormal– Upon ER admission, due to chest pain or abnormal ECG.
• Dye is injected into orifices of coronary arteries and evaluated for amount of blockage in each artery, as well as injection of dye in ventricle to see pumping of heart (kinesis).

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 8
Intravascular Ultrasound Imaging (IVUS)
A
B
Multi-Slice CT multiplanar reconstruction of R coronary
Image from www.medscape.com. Source: Eur Heart J. ©2008, Oxford University Press.
MR Angiography of Brain
Image from www.youtube.com. Source: Philips Healthcare and the Philips Learning Center.

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 9
MR Angiography
Image from www.youtube.com. Source: Philips Healthcare and the Philips Learning Center.
Diagnostic Testingpulmonary
• Chest x‐ray
• Bronchography
• CT and spiral CTCT and spiral CT
• Ventilation perfusion scans
• Bronchoscopy/sputum sample
• Pulmonary function testing
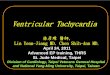
Bronchiectasis on Chest X-Ray and Bronchogram
A B
Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 10
Bronchiectasis on Chest X-Ray and Bronchogram
A B
CT of Normal Mediastinum and Hilum
A B
C D
CT of Normal Mediastinum and Hilum
• CXR simply does not pick up the abnormalities if tumor is small.
• Low dose CT to chest is now the gold standard for assessment of lung cancer but extremelyfor assessment of lung cancer, but extremely expensive.
– American Lung Association: Low dose CT could reduce lung cancer mortality by up to 20%.
– Criteria: Current or former smokers, ages 55 – 74.
– Smoking history of at least 30 pack years.
American Lung Association 2012.

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 11
CT of Lung Cancer
Lung cancer revealed by CT lung screening.
Image from www.cedars‐sinai.edu.
Spiral CT of Chest
Image © Nevit Dilmen found at Wikimedia Commons.
PET Scan

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 12
Ventilation-Perfusion Scan
RAO Ant LAO Lt Lat
Images from www.med.harvard.edu.
LPO Post RPO Rt Lat
Anterior Posterior
Ventilation-Perfusion Scan
• V/Q scans used to be considered the gold standard for identifying a pulmonary embolus.
• Studies have shown that the sensitivity of V/Q scans is only about 50 – 60%.scans is only about 50 60%.
• Many individuals are undergoing V/Q scans to rule out PE, and the scans may NOT be detecting PE.
• Spiral CT may be the gold standard now for PE, but radiation is disadvantage.
• KEY factor: The individual reading the scans.
Pulmonary Function Testing
Diagnostic Testing

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 13
Pulmonary Function Testing
Lung Volumes and Capacities
Static Lung Volumes
• Total lung capacity (TLC)
• Vital capacity (VC)
• Inspiratory reserve
Dynamic Lung Volumes
• Forced expiratory volume in 1 second (FEV 1.0)
• Forced vital capacity (FVC)p yvolume (IRV)
• Expiratory reserve volume (ERV)
• Residual volume
• Dynamic volumes tell you about airway resistance/ obstructive problems
• Patient actively performs spirometry with forced flows.
Interpretation of PFT Results
• Determine if results are...
– Normal or abnormal
i i b i– Restrictive or obstructive
• If obstructive, is this reversible?
• Watch for patient effort….

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 14
PFT Interpretation
40
PFT Interpretation
41
PFT Interpretation
42
Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 15
PFT InterpretationSo what can we learn from this test?
• Individual is most likely an athlete in good physical condition, but
• They most likely have some type of obstructive airway disease, like exercise‐induced asthma.
• Example of how a full workup can pick up something other tests might miss.
PROPERTIES
On passing, 'Finish' button: Goes to Next Slide
On failing, 'Finish' button: Goes to Next Slide
Allow user to leave quiz: After user has completed quiz
User may view slides after quiz: At any time
Show in menu as: Multiple items
Laboratory Information
ABGs
CBC
Cardiac‐Specific
Nutrition

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 16
Arterial Blood Gases (ABGs)
• Purpose: acid base regulation
– Acidosis: pH < 7.35
– Alkalosis: pH > 7.45
• Normal values:
– pH: 7.35 – 7.45
– pCO2: 35 – 45
– pO2: > 80
– HCO3: 22 – 26
Arterial Blood Gases (ABGs)primary respiratory conditions: abnormal pCO2
Acidosis
• pH < 7.35, pCO2 > 45
• Example:
pH: 7 32
Alkalosis
• pH > 7.45, pCO2 < 35
• Example:
pH: 7 48– pH: 7.32
– pCO2: 55
• Clinical example: Patient heavily sedated – slow breathing and retaining CO2.
– pH: 7.48
– pCO2: 30
• Clinical example: Patient in pain, rapid shallow respirations.
Arterial Blood Gases (ABGs)primary metabolic conditions: abnormal HCO3
Acidosis
• pH < 7.35, HCO3 < 22
• Example:
pH: 7 32
Alkalosis
• pH > 7.45, HCO3 > 26
• Example:
pH: 7 48– pH: 7.32
– HCO3: 18
• Clinical scenario: Patient with diabetic ketoacidosis.
– pH: 7.48
– HCO3: 29
• Clinical scenario: Patient with flu, frequent vomiting.
Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 17
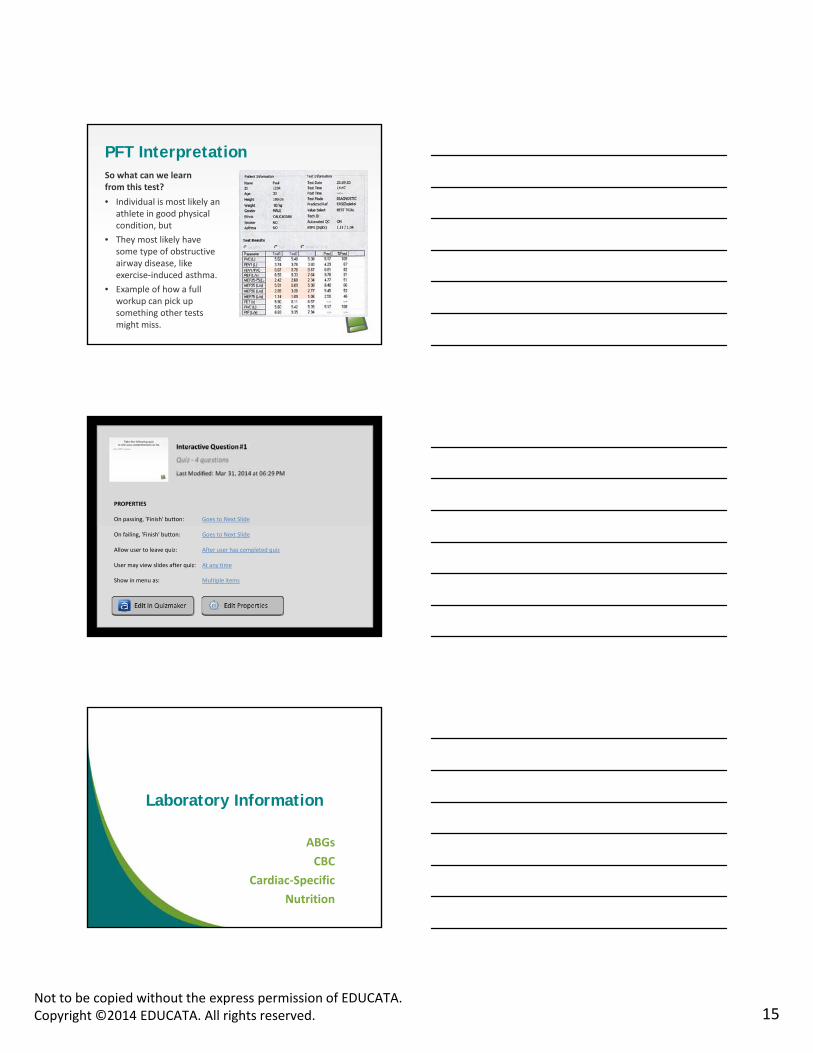
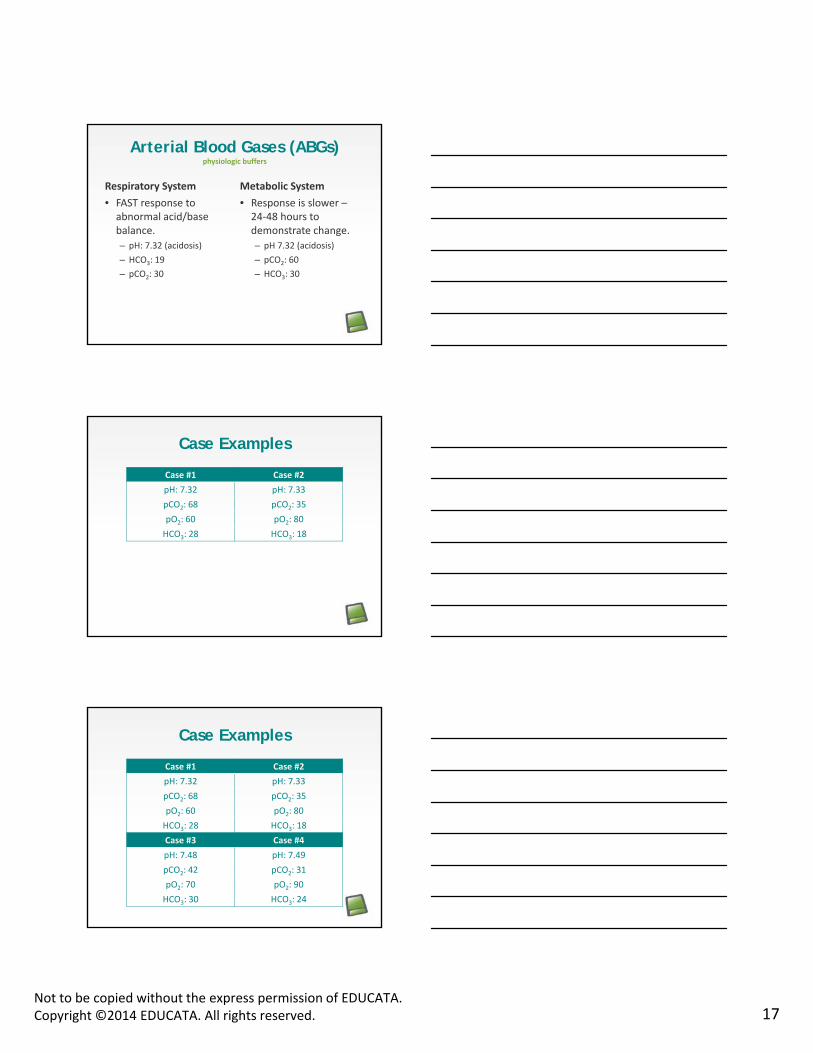
Arterial Blood Gases (ABGs)physiologic buffers
Respiratory System
• FAST response to abnormal acid/base balance.
Metabolic System
• Response is slower –24‐48 hours to demonstrate change.
– pH: 7.32 (acidosis)
– HCO3: 19
– pCO2: 30
g
– pH 7.32 (acidosis)
– pCO2: 60
– HCO3: 30
Case Examples
Case #1 Case #2
pH: 7.32 pH: 7.33
pCO2: 68 pCO2: 35
pO2: 60 pO2: 80
HCO3: 28 HCO3: 18
Case Examples
Case #1 Case #2
pH: 7.32 pH: 7.33
pCO2: 68 pCO2: 35
pO2: 60 pO2: 80
HCO3: 28 HCO3: 18
Case #3 Case #4
pH: 7.48 pH: 7.49
pCO2: 42 pCO2: 31
pO2: 70 pO2: 90
HCO3: 30 HCO3: 24

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 18
Other Important Lab Valuescomplete blood count
• Normal values:
– Red blood cells
– Hemoglobin
Other Important Lab Valuescomplete blood count
• Normal values:
– Red blood cells
– Hemoglobin
– White blood cells (4,000 – 11,000)
– Platelets (NL: 150,000 – 400,000)
Other Important Lab Valuescardiac‐specific lab values
• Troponin
• CPK (creatinine phosphokinase)
– MB isoenzyme is specific for cardiac injury.
• Lactic dehydrogenase (LDH)
– 5 isoenzymes
• C‐reactive protein (CRP)
• Homocysteine
• Lipoprotein (a)

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 19
Other Important Lab Valuesliver enzymes
• AST
• Bilirubin
• Alkaline phosphataseAlkaline phosphatase
Other Important Lab Valuesother heart/kidney values
• Blood urea nitrogen (BUN)
• Creatinine (↑ in kidney disease)
• BNP (> 700 decompensated heart failure)BNP (> 700 decompensated heart failure)
Other Important Lab Valuesblood coagulation
• PT/PTT
– PT NL: 11 – 16 secs
• D dimer to assess for excess clotting.
– Elevated D dimer means increased risk of clotting.
• INR
– NL is 0.8 – 1.2.
– Anticoagulation up to about 2.5 (keep between 2 – 3).

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 20
Other Important Lab Valuesnutrition values
• Albumin (↓ with malnourishment)
• Total protein
Other Important Lab Valueselectrolytes
• Na+ (NL = 135 – 145 mEq/L)
• K+ (NL = 3.5 – 5.0 mEq/L)
• Mg+ (1.5 – 2.0 mEq/L):Mg+ (1.5 2.0 mEq/L): ↓ in malabsorption syndrome and pancreatitis, including with frequent antacid use
PROPERTIES
On passing, 'Finish' button: Goes to Next Slide
On failing, 'Finish' button: Goes to Next Slide
Allow user to leave quiz: After user has completed quiz
User may view slides after quiz: At any time
Show in menu as: Multiple items

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 21
Physical Assessment of the ICU Patient
What is important?
What are the implications?
Bedside Assessment
• Cognition/delirium/orientation
• Risk assessment: Are they mobile, or will they be difficult to mobilize and mobility will be an assisted process?– DVT, PE, pneumonia, contracture, integument
• Hemodynamic stability• Hemodynamic stability– Vital signs and vital sign responses to activity
• Pulmonary status
– Ventilator settings?
– Risk for pneumonia?
• Integumentary status
• Musculoskeletal status
• Neuromuscular
Physical Assessment
• Supine
• Sit
Amount of assist and vital sign responses to:
– Optimal for heart and lung auscultation, skin check
• Stand
• ADL
• Ambulation

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 22
VS Responses to Activitypatient #1
Activity HR BP SpO2 Symptoms
Supine 72 124/78 96 Tired
Sit 84 110/70 94 TiredSit 84 110/70 94 Tired
ADL sit 96 118/78 94 Tired
Stand 108 94/68 93SOB/light‐headed
Ambulation (6’) 114 110/78 94 Fatigue
VS Responses to Activitypatient #2
Activity HR BP SpO2 Symptoms
Supine 80 irreg 118/72 96 None
Sit 90 irreg 120/70 96 NoneSit 90 irreg 120/70 96 None
ADL sit 100 irreg 126/76 96 Tired
Stand 100 irreg 114/72 96 Tired
Ambulation 110 irreg 92/60 94 SOB, fatigue
VS Responses to Activitypatient #3
Activity HR BP SpO2 Symptoms
Supine 100 120/76 93 SOB
Sit 106 124/74 92 SOBSit 106 124/74 92 SOB
ADL sit 120 134/72 89SOB
increased
Stand 110 120/70 91 SOB
Ambulation (10’) 120 132/80 88 Severe SOB

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 23
Developing a Plan of Care and Treatment Priorities/
Interventions Based Upon Assessment Findings
What is important?
What are the implications?
Treatment Priorities
• Cognition/alertness
– Reduce deep sedation
• Cardiopulmonary
P t l i f ti– Prevent pulmonary infections
– Maintain adequate SpO2
– Monitor VS with activity
• Integumentary
• Musculoskeletal
• Neuromuscular
ICU Priorities for Mechanically Ventilated Patients
• Sedation and paralysis administration
• Mechanical ventilation d
• Maintenance of skin integrity
• Physical activityorders
• Stress ulceration prophylaxis
• Deep venous thrombosis prophylaxis
• Nutritional support
• Treatment of sleep deprivation
• Prevention or treatment of infectious complications
• Prevention of aspiration
American College of Chest Physicians.

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 24
ICU Priorities for Mechanically Ventilated Patients
• Keep in mind the importance of physical activity.
• Once a patient is stable, physical activity should be part of his or her daily routine.
• Look at the protocols from the American College of Chest Physicians for more guidance at www.chestnet.org.
American College of Chest Physicians.
Goals
• Reducing oversedation.
• Increasing early activity.
• Encouraging sleep to reduce delirium and toEncouraging sleep to reduce delirium and to allow for physical conditioning and weaning from mechanical ventilation.
• Airway protection in newly extubatedpatients.
Early Activity Requirements
Neurologic criteria: Patient responds to verbal stimulation.
– Purposeful response.
Respiratory criteria: FiO2 no greater than 0.6 and PEEP ≤ 10 cm H20.
Circulatory criteria: Absence of orthostatic hypotension and catecholamine drips.
ASSESS CRITERIA DAILY.

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 25
Pulmonary Problem List
Decreased oxygenation
Decreased ventilation
Decreased airway clearance
Decreased lateral costal expansion
Decreased diaphragmatic excursion
Increased amount of secretions
Increased retention of secretions
Poor mobility
Decreased thoracic mobility
Decreased diaphragmatic mobility
Increased risk for pulmonary dysfunction
Infection/inflammation
Interventions for Pulmonary Issuesimprove oxygenation
• O2
• Positioning
• Breathing exercises
• Mobilization of secretions
Interventions for Pulmonary Issuesimprove ventilation
• Mobilization of secretions
• Positioning
• Breathing exercises

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 26
Incentive Spirometry
Breathing Exercises
• Diaphragmatic
• Pursed lip
• Segmental breathing
Breathing Exercises
• Maximal inspiration hold
• Active cycle breathing
• Inspiratory muscle training

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 27
Interventionsimproving airway clearance
• Abdominal support
• Abdominal strengthening
• Positioning
• Cough instruction
Interventionsmobilizing secretions
• Postural drainage
• Percussion/vibration
• Mobility• Mobility
• Breathing exercises
• Cough
• Humidity/medications
Airway Clearance Devices

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 28
Airway Clearance Devicesthe vest
Cough Assist
Monitoring and Titrating
• O2 is a drug… Always check the order.
• Look at ABGs.
• Check O2 saturation measures.
• Compare the patient report vs. the numbers.
• Review other vital signs.

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 29
PROPERTIES
On passing, 'Finish' button: Goes to Next Slide
On failing, 'Finish' button: Goes to Next Slide
Allow user to leave quiz: After user has completed quiz
User may view slides after quiz: At any time
Show in menu as: Multiple items
Mobility Aids
Developing a Plan of Care
Dynamic Tilt TableMoveo

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 30
Dynamic Tilt TableMoveo
Dynamic Tilt TableHocomo
Overhead Device

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 31
Standing Aid Arjo
Standing Aid Arjo Sara Plus for standing/walking
Standing Aid Arjo Sara Plus

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 32
Improving Mobility and Posture
• Thoracic mobility techniques
– Pulleys
– Side‐lying stretch
• Thoracic postural exercises
– UE exercises seated on therapy ball
• Paced BREATHING!!!
– Prone extension
Strength
• Anterior neck flexors
• Rhomboids
• Middle and lower trapezii
• Lattisimus
Incorporate Functional Strengthening Into Daily Activities

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 33
Flexibility
• Posterior cervical
• Pectoral muscles
• Anterior deltoidsAnterior deltoids
• Sternocleidomastoids
Yoga
Interventions for Cardiac Patients
• Therapeutic exercise
– Aerobic capacity/ endurance conditioning
– Balance coordination and agility training
• Functional training in self‐care and home management
– ADL trainingagility training
– Flexibility exercises
– Gait and locomotion training
– Relaxation
– Strength, power, and endurance training for ventilatory muscles
– Device and equipment use and training
• Airway clearance techniques
• Education

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 34
Heart Failure Patients
• Frequent bouts of activity with rest in between.
• Teach patients about:
– Daily weighing to check for changes in fluid.
– Daily checks on activity by instructing in RPE or dyspnea monitoring.
– Watching for dyspnea when laying down.
– Energy conservation.
Modified Dyspnea
Scalebreathing
Scale Severity
0 Nothing at all
12
Very slight
34
Slight
56
Moderate
78
Severe
910
Very severeMaximum
Evidence for Exercise
• Bicycle ergometer training (ET) versus aerobic and strength training (CT) resulted in:
Strength and endurance training vs. endurance training alone.
strength training (CT) resulted in:
– Improved EF in CT group by 18% over 3 months.
– Decreased EF in ET alone group (‐11.4%).
– Delagardelle C, Feiereisen P, Autier P, Shita R, Krecke R, Beissel J. Strength/endurance training versus endurance training in congestive heart failure. Med Sci Sports Exerc. 2002 Dec;34(12):1868‐72.

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 35
Case Study #1
• Patient with decompensated heart failure. Admitted with one‐week history of worsening dyspnea and weight gain of 8 lbs.
• Once stabilized, ,– Exercise interventions:
• Multiple bouts of walking with frequent rest.
• Strength training consisting of UE functional strengthening and LE strengthening with chair rises.
– Education: teaching self management with weight monitoring and RPE monitoring of all activities.
Case Study #2COPD
• Patient admitted for acute exacerbation.
• Once ABGs show pH in normal range, begin activity– Breathing exercises
– Mobility out of bed
– Optimize oxygen – maintain SpO2 > 90
– LE strengthening: EOB to stand activities
– Short bouts of walking, coordinating breathing exercises and frequent rests
• Education
PROPERTIES
On passing, 'Finish' button: Goes to Next Slide
On failing, 'Finish' button: Goes to Next Slide
Allow user to leave quiz: After user has completed quiz
User may view slides after quiz: At any time
Show in menu as: Multiple items

Not to be copied without the express permission of EDUCATA.Copyright ©2014 EDUCATA. All rights reserved. 36
In Conclusion
• I hope that this helps you understand more about working with ICU patients, including
– Lab tests
Diagnostic tests– Diagnostic tests
– Therapeutic interventions
– Treatment for the pulmonary system
• This should make you more comfortable when working with critical patients and making clinical decisions.