Embed Size (px)
Citation preview

Ventricular Hypertrophy in Pediatric EKG
Marc FrancisR4 FRCPC EmergencyYear 1 PEM Fellow

Objectives
I do not want to:• Make you memorize
pages of numbers• Make you memorize
tables• Make you never
want to see another pediatric EKG
• Make you fall asleep
I do want to:• Give you a bedside
approach to rapidly looking for LVH and RVH

Ventricular Hypertrophy
• RVH and LVH can be markers of significant disease states
• Congenital Heart disease• Shunts• Pulmonary HTN• Renal Failure
• Hypertrophy produces abnormalities on EKG• QRS axis• QRS voltages• R/S ratio• T axis

The Problem
• Damn kids keep growing!!!– They start life with dominance of the RV– By 6-8 weeks they have corrected to a LV
dominated system– The normal intervals and wave amplitudes
change as they age– They finally fall in line and become “big
people” only when they are 16 years old

Solutions
Option 1:
Memorize a ton of charts and tables of normal values
Option 2:
Keep these in your palm pilot to reference every 5-10 minutes until step one has occurred
Option 3:
Ignore any and all EKGs done in the Peds ED

The “Alternative” Solution
Step 1:
Remember a few simple screening parameters that will allow you to rapidly assess an EKG to look for RVH and LVH in pediatric patients
Step 2:
Let the cardiologist remember all the numbers and charts

RVH

CRITERIA FOR RVH
1) RAD for the patient's age 2) Increased rightward and anterior QRS voltages
a) R in V1, V2, or aVR greater than the upper limits of normal for the patient's age
b) S in I and V6 greater than the upper limits of normal for the patient's age *Note: Assumes QRS is not widened for age indicating abnormal
conduction delay
3) Abnormal R/S ratio in favor of the RVa) R/S ratio in V1 and V2 greater than the upper limits
of normal for ageb) R/S ratio in V6 less than 1 after one month of age

1) RAD for patient age
Lead I = 0° Lead AVL = -30°
Lead II = +60° Lead AVR = -150°
Lead AVF = +90°
Lead III = +120°

Mean and Ranges of Normal QRS Axes by Age
Age Mean (Range)
1 wk-1 mo +110° (+30 to +180)
1-3 mo +70° (+10 to +125)
3 mo-3 yr +60° (+10 to +110)
Older than 3 yr +60° (+20 to +120)
Adult +50° (-30 to +105)

2) Increased rightward and anterior QRS voltages
• R in V1, V2, or aVR greater than the upper limits of normal for the patient's age
• S in I and V6 greater than the upper limits of normal for the patient's age

R and S Voltages: Mean (and Upper Limits of Normal) According to Lead and Age
Age R voltage in V1 S voltage in V6
0-1 mo 15 (25) 4 (12)
1-6 mo 11 (20) 2 (7)
6 mo-1yr 10 (20) 2 (6)
1-3yr 9 (18) 2 (6)
3-8yr 7 (18) 1 (5)
8-12yr 6 (16) 1 (4)
12-16yr 5 (16) 1 (5)
Young Adults 3 (14) 1 (13)
*Voltages are measured in millimeters, when 1 mV = 10 mm paper

3) Abnormal R/S ratio in favor of the RV
• R/S ratio in V1 and V2 greater than the upper limits of normal for age
• R/S ratio in V6 less than 1 after one month of age

R/S Ratio: Mean and Upper and Lower Limits of Normal According to Age V1
Lead VIAge LLN Mean ULN0-1mo 0.5 1.5 191-6mo 0.3 1.5 S=06mo-1yr 0.3 1.2 61-3yr 0.5 0.8 23-8yr 0.1 0.65 28-12yr 0.15 0.5 112-16yr 0.1 0.3 1Adults 0.0 0.3 1*LLN = lower limits of normal; ULN = upper limits of normal
From Guntheroth WB: Pediatric Electrocardiography. Philadelphia, WB Saunders, 1965

Screening criteria for RVH
1) RAD greater than +120° in any child over 1 month is highly suggestive of RVH
2) Upright T in V1 • In patients > 3 days and < 6yr old • Provided that the T is upright in the left precordial
leads (V5, V6)
3) Q wave in V1 always suggests RVH
4) S wave > R wave in Lead V6

LVH

CRITERIA FOR LVH
1) LAD for the patient's age2) QRS voltages in favor of the LV
a) R in I, II, III, aVL, aVF, V5, or V6 greater than the upper limits of normal for age
b) S in V1 or V2 greater than the upper limits of normal for age
3) Abnormal R/S ratio in favor of the LV– R/S ratio in V1 and V2 less than the lower
limits of normal for the patient's age

1) LAD for patient age
Lead I = 0° Lead AVL = -30°
Lead II = +60° Lead AVR = -150°
Lead AVF = +90°
Lead III = +120°

Mean and Ranges of Normal QRS Axes by Age
Age Mean (Range)
1 wk-1 mo +110° (+30 to +180)
1-3 mo +70° (+10 to +125)
3 mo-3 yr +60° (+10 to +110)
Older than 3 yr +60° (+20 to +120)
Adult +50° (-30 to +105)

2) QRS voltages in favor of the LV
• R in I, II, III, aVL, aVF, V5, or V6 greater than the upper limits of normal for age
• S in V1 or V2 greater than the upper limits of normal for age

R Voltages: Mean (Upper Limits of
Normal) According to Lead and Age R voltage
Age Lead I Lead II Lead III0-1mo 4(8) 6(14) 8(16)1-6mo 7(13) 13(24) 9(20)6mo-1yr 8(16) 13(27) 9(20)1-3yr 8(16) 13(23) 9(20)3-8yr 7(15) 13(22) 9(20)8-12yr 7(15) 14(24) 9(24)12-16yr 6(13) 14(24) 9(24)Young Adults 6(13) 9(25) 6(22)*Voltages are measured in millimeters, when 1 mV = 10 mm paper
From Park MK, Guntheroth WG: How to Read Pediatric ECGs, 3rd ed. St. Louis, Mosby, 1992.

S Voltages: Mean (Upper Limits of
Normal) According to Lead and Age S voltage
Age Lead VI Lead V20-1mo 10(20) 20(35)1-6mo 7(18) 16(30)6mo-1yr 8(16) 17(30)1-3yr 13(27) 21(34)3-8yr 14(30) 23(38)8-12yr 16(26) 23(38)12-16yr 15(24) 23(48)Young Adults 10(23) 14(36)*Voltages are measured in millimeters, when 1 mV = 10 mm paper
From Park MK, Guntheroth WG: How to Read Pediatric ECGs, 3rd ed. St. Louis, Mosby, 1992.

3) Abnormal R/S ratio in favor of the LV
• R/S ratio in V1 and V2 less than the lower limits of normal for the patient's age
*Note that lead V2 is in ½ normal standardization

R/S Ratio: Mean and Upper and Lower Limits of Normal According to Age V1
Lead VIAge LLN Mean ULN0-1mo 0.5 1.5 191-6mo 0.3 1.5 S=06mo-1yr 0.3 1.2 61-3yr 0.5 0.8 23-8yr 0.1 0.65 28-12yr 0.15 0.5 112-16yr 0.1 0.3 1Adults 0.0 0.3 1*LLN = lower limits of normal; ULN = upper limits of normal
From Guntheroth WB: Pediatric Electrocardiography. Philadelphia, WB Saunders, 1965

Screening Criteria for LVH
1) LAD less than +10° is highly suggestive of LVH
2) S wave in lead V1 greater than 20mm
3) Q in V6, ≥5 mm suggests LVH• With LV diastolic overload

In Summary
If under 1 month all bets are off!!!
Step 1– Look at the axis:
• > +120° suggests RVH• < +10° suggests LVH
Step 2– Look at lead V1:
• Upright T or Q-wave in V1 suggests RVH• Large S wave >20mm suggests LVH

In Summary
• Step 3– Look at lead V6:
• S wave > R wave suggests RVH• Q wave > 5mm suggests LVH

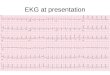
Case 1
• 1 month old with heart murmur

Case 2
• 8yo with heart murmur

Case 3
• 4yo Female with CP

Case 4
• 2yo M

Case 5
• 8mo Female

Questions???

References
• Park: Pediatric Cardiology for Practitioners, 4th ed., Copyright © 2002 Mosby, Inc.
• Guntheroth WB: Pediatric Electrocardiography. Philadelphia, WB Saunders, 1965.
• Park MK, Guntheroth WG: How to Read Pediatric ECGs, 3rd ed. St. Louis, Mosby, 1992.