Embed Size (px)
Citation preview

Fasciocutaneous Free Flaps For Hypopharyngeal Fasciocutaneous Free Flaps For Hypopharyngeal ReconstructionReconstruction
Ayman AbdelAyman Abdel--Wahab Amin, MDWahab Amin, MDAssociate Professor of Surgical OncologyAssociate Professor of Surgical Oncology
National Cancer InstituteNational Cancer InstituteCairo, EgyptCairo, Egypt
Fellowship, Head and Neck Oncology & Reconstructive MicrosurgeryFellowship, Head and Neck Oncology & Reconstructive MicrosurgeryUniversity of MiamiUniversity of Miami
IntroductionIntroduction
•• Carcinoma of the hypopharynx is a devastating Carcinoma of the hypopharynx is a devastating disease.disease.
•• Surgical resection (TLP+ND) remains the Surgical resection (TLP+ND) remains the mainstay of treatment.mainstay of treatment.
•• Total esophagectomy for oncologic needsTotal esophagectomy for oncologic needs•• Reconstruction of surgical defects represents a Reconstruction of surgical defects represents a
major challenge for head and neck oncologic major challenge for head and neck oncologic surgeons.surgeons.
Goals of ReconstructionGoals of Reconstruction
•• ReRe--establishment of the continuity of alimentary tractestablishment of the continuity of alimentary tract•• The ideal technique is controversial:The ideal technique is controversial:
•• One stageOne stage•• High success rateHigh success rate•• Low mortality and morbidityLow mortality and morbidity•• Less complicationsLess complications•• Short hospitalizationShort hospitalization•• Provide the greatest potential for neoProvide the greatest potential for neo--pharyngeal speechpharyngeal speech
Options for Reconstruction of Options for Reconstruction of PharyngoPharyngo--esophageal Segmentesophageal Segment
•• Early procedures: Multiple stages Early procedures: Multiple stages •• Regional cutaneous flaps e.g. deltopectoralRegional cutaneous flaps e.g. deltopectoral•• Regional myocutaneous F as trapeziusRegional myocutaneous F as trapezius•• Pedicled myocutaneous F as PMMCPedicled myocutaneous F as PMMC•• Colon bypass & Gastric pull upColon bypass & Gastric pull up•• Microvascular FTT:Microvascular FTT:
•• Visceral: free jejunum & gastroVisceral: free jejunum & gastro--omental flapsomental flaps•• Fasciocutaneous: RF, Scapular, LA, PLT, and ALTFasciocutaneous: RF, Scapular, LA, PLT, and ALT

Gastric Pull Up? Gastric Pull Up? Why not??Why not??
•• Non anatomicalNon anatomical•• Non physiological: Denervated stomachNon physiological: Denervated stomach•• Significant mortality (8Significant mortality (8--13%) and morbidities (13%) and morbidities (Gilbert 2004Gilbert 2004))•• Prolonged ileusProlonged ileus•• Hyperalimentation: More likelyHyperalimentation: More likely•• Not suitable for cardiac and pulmonary diseasesNot suitable for cardiac and pulmonary diseases•• Indicated: Total esoph for oncologic clearanceIndicated: Total esoph for oncologic clearance
Patients & MethodsPatients & Methods
•• Over 3 yrs period at NCIOver 3 yrs period at NCI•• A total of 23 patientsA total of 23 patients•• All underwent TLP & reconstruction using FFFAll underwent TLP & reconstruction using FFF•• FFF included RF (9), PLT (7), ALT (5) & LA (2)FFF included RF (9), PLT (7), ALT (5) & LA (2)•• External monitor in allExternal monitor in all•• Frozen section of distal stumpFrozen section of distal stump

Radial Forearm FlapRadial Forearm Flap(Chinese Flap)(Chinese Flap)
•• Developed in China by Yang in 1987 Developed in China by Yang in 1987 •• Initially described for burn contracture of cervical Initially described for burn contracture of cervical
skinskin•• Soutar et al for H & N reconstructionSoutar et al for H & N reconstruction•• Radial A, cephalic V, Venae comitantesRadial A, cephalic V, Venae comitantes•• Lat intermuscular septum bet BR & FCRLat intermuscular septum bet BR & FCR•• Urken: Neurofacut F (med or lat antecubital N)Urken: Neurofacut F (med or lat antecubital N)

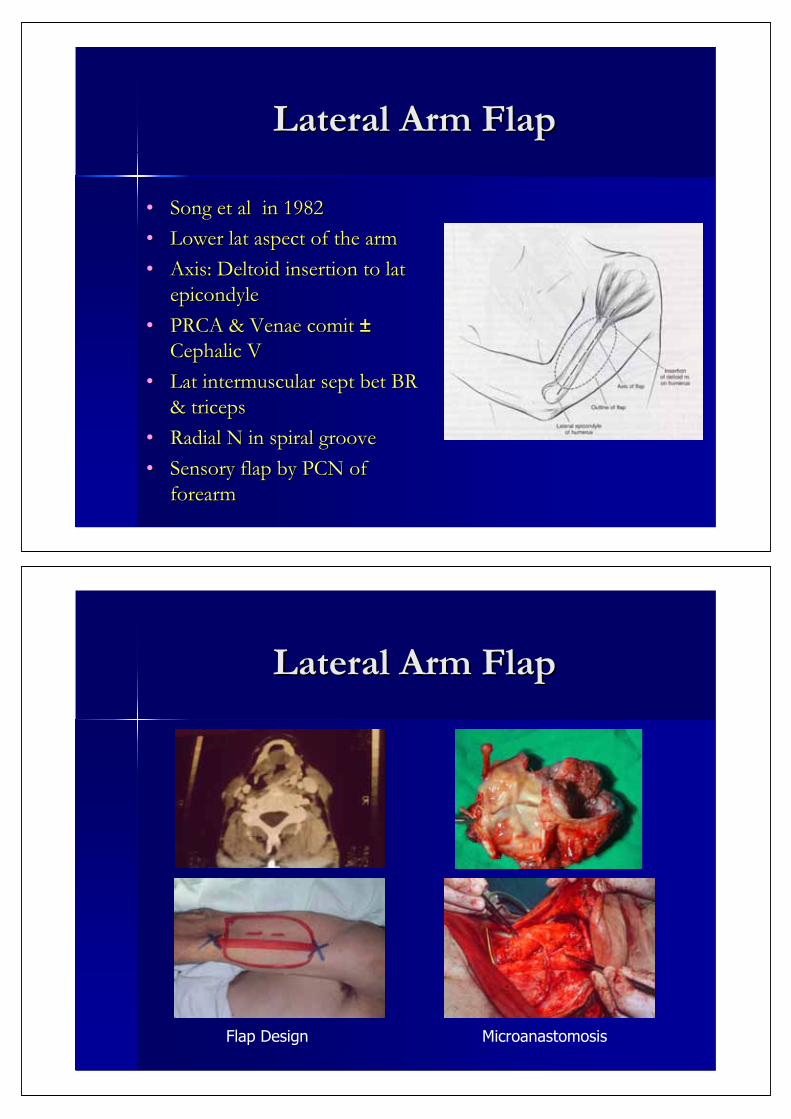
Lateral Arm FlapLateral Arm Flap
•• Song et alSong et al in 1982in 1982•• Lower lat aspect of the armLower lat aspect of the arm•• Axis: Deltoid insertion to lat Axis: Deltoid insertion to lat
epicondyleepicondyle•• PRCA & Venae comit PRCA & Venae comit ±±
Cephalic VCephalic V•• Lat intermuscular sept bet BR Lat intermuscular sept bet BR
& triceps& triceps•• Radial N in spiral grooveRadial N in spiral groove•• Sensory flap by PCN of Sensory flap by PCN of
forearmforearm
Lateral Arm FlapLateral Arm Flap
Flap Design Microanastomosis
Lateral Arm FlapLateral Arm Flap
Early POST op
Ba Swallow
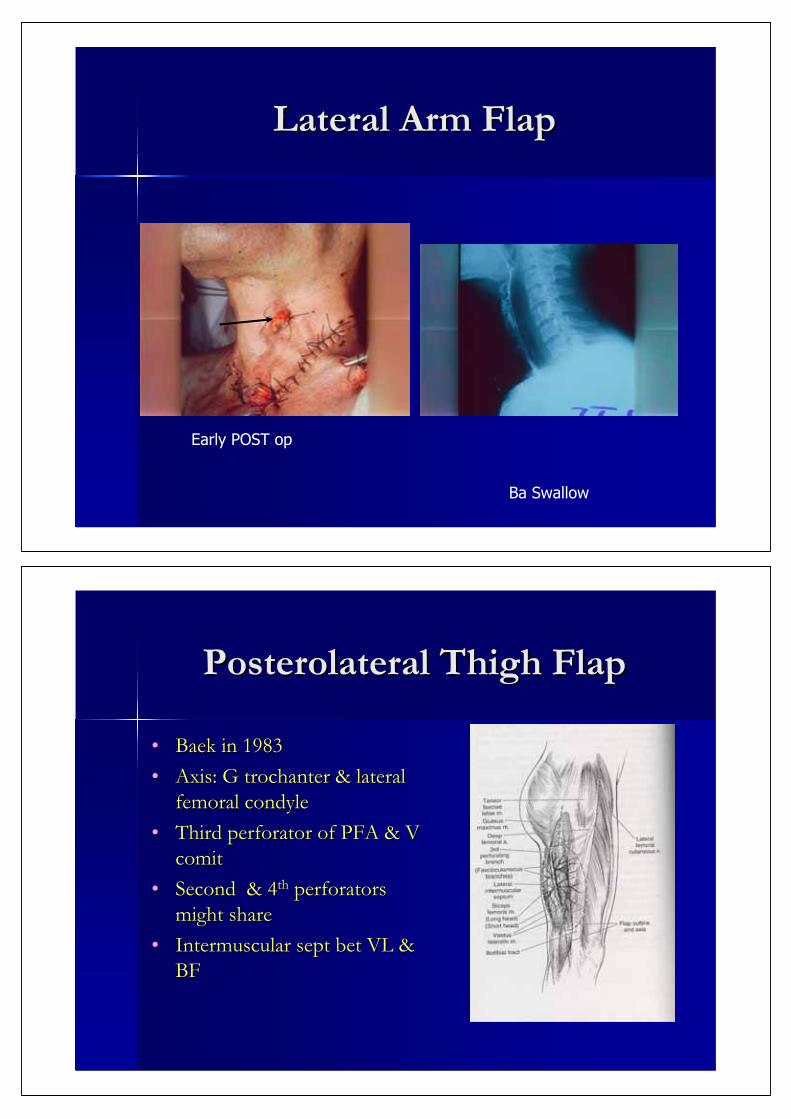
Posterolateral Thigh FlapPosterolateral Thigh Flap
•• Baek in 1983Baek in 1983•• Axis: G trochanter & lateral Axis: G trochanter & lateral
femoral condylefemoral condyle•• Third perforator of PFA & V Third perforator of PFA & V
comitcomit•• Second & 4Second & 4thth perforators perforators
might sharemight share•• Intermuscular sept bet VL & Intermuscular sept bet VL &
BFBF

Posterolateral Thigh FlapPosterolateral Thigh Flap
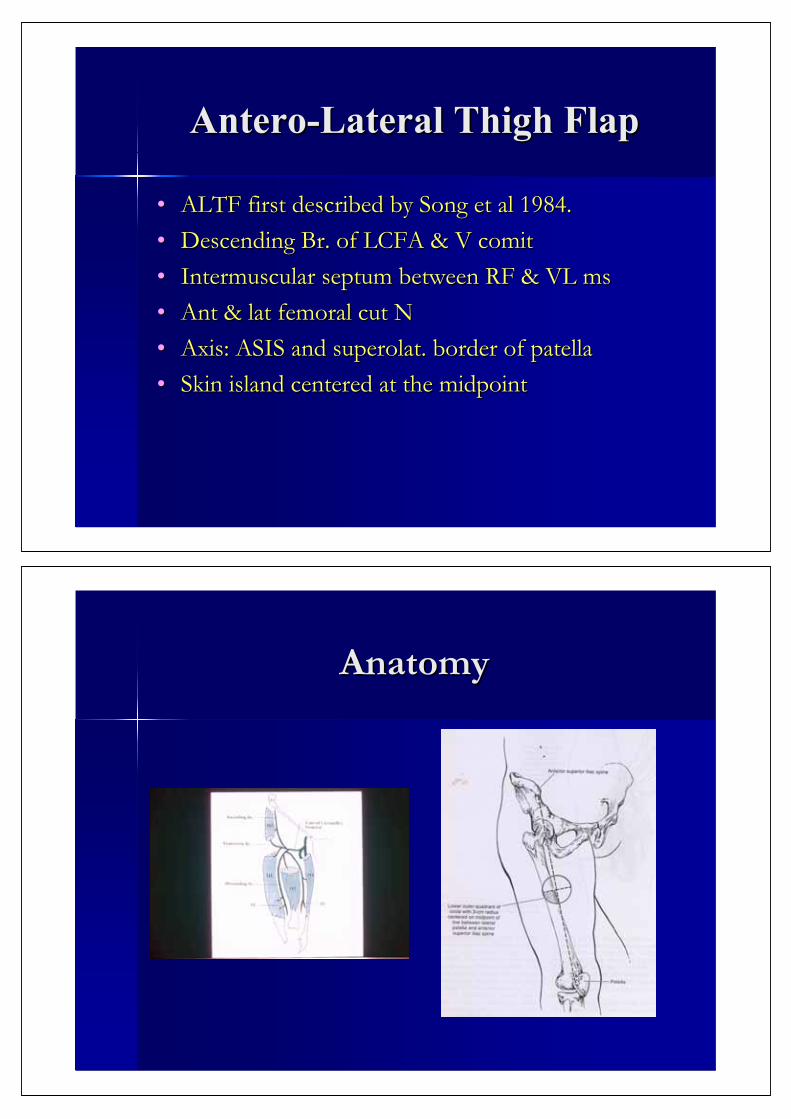
AnteroAntero--Lateral Thigh FlapLateral Thigh Flap
•• ALTF first described by Song et al 1984.ALTF first described by Song et al 1984.•• Descending Br. of LCFA & V comitDescending Br. of LCFA & V comit•• Intermuscular septum between RF & VL msIntermuscular septum between RF & VL ms•• Ant & lat femoral cut NAnt & lat femoral cut N•• Axis: ASIS and superolat. border of patellaAxis: ASIS and superolat. border of patella•• Skin island centered at the midpointSkin island centered at the midpoint
AnatomyAnatomy
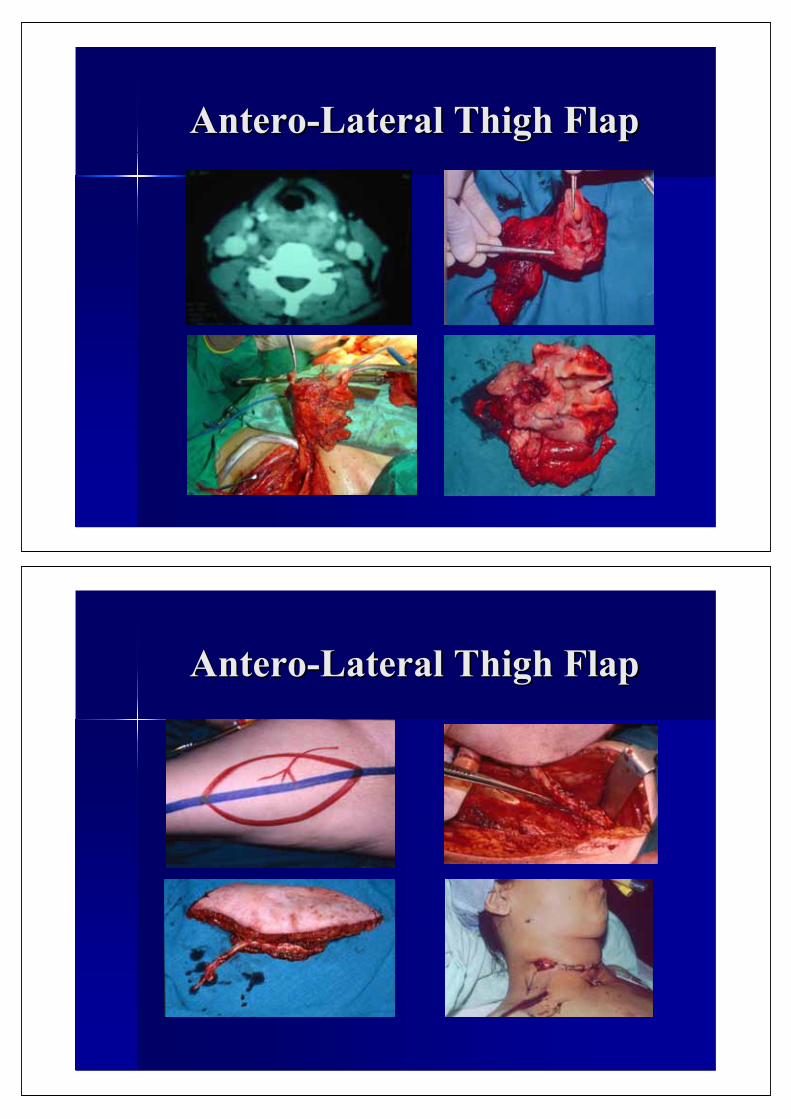
AnteroAntero--Lateral Thigh FlapLateral Thigh Flap
AnteroAntero--Lateral Thigh FlapLateral Thigh Flap
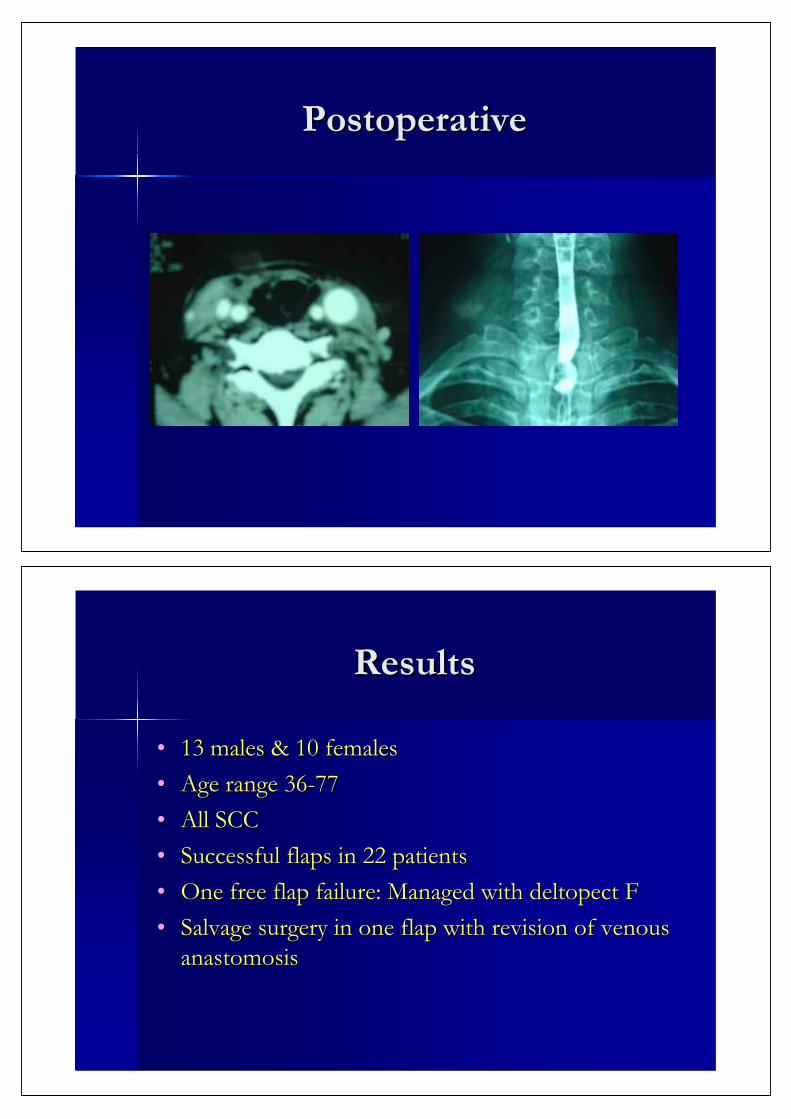
PostoperativePostoperative
ResultsResults
•• 13 males & 10 females13 males & 10 females•• Age range 36Age range 36--7777•• All SCCAll SCC•• Successful flaps in 22 patientsSuccessful flaps in 22 patients•• One free flap failure: Managed with deltopect FOne free flap failure: Managed with deltopect F•• Salvage surgery in one flap with revision of venous Salvage surgery in one flap with revision of venous
anastomosisanastomosis
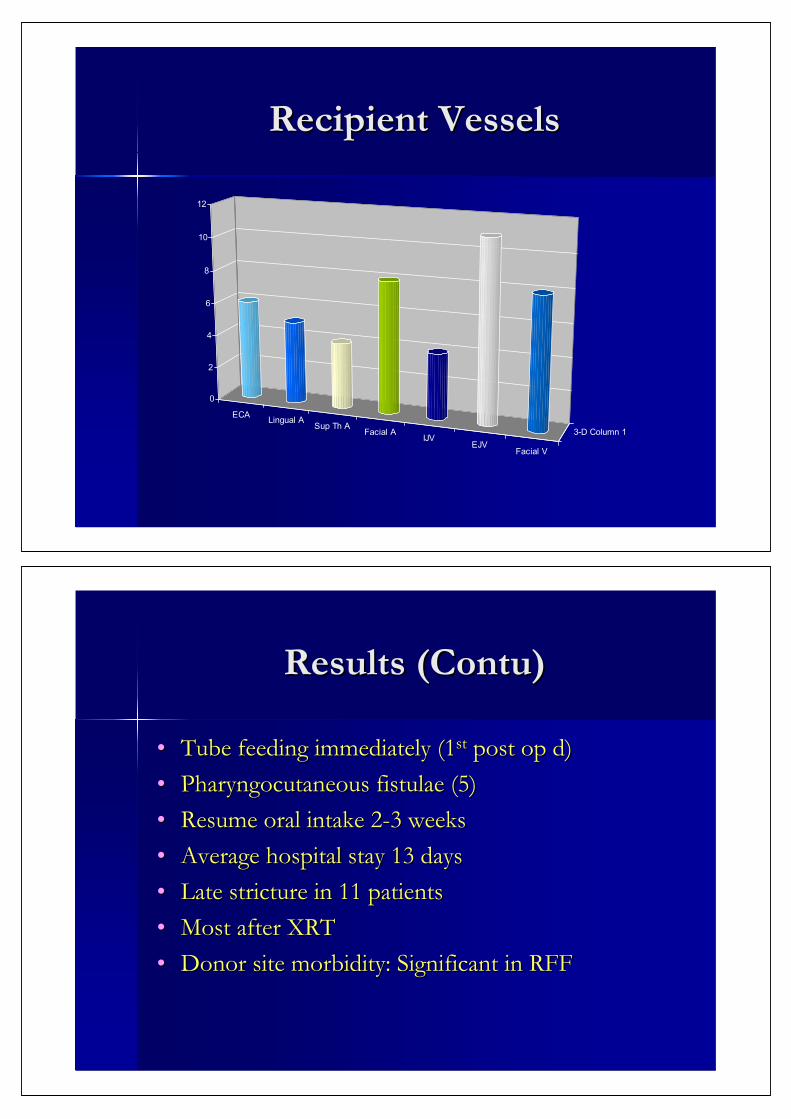
Recipient VesselsRecipient Vessels
ECA Lingual ASup Th A
Facial AIJV
EJVFacial V
3-D Column 1
0
2
4
6
8
10
12
Results (Contu)Results (Contu)
•• Tube feeding immediately (1Tube feeding immediately (1stst post op d)post op d)•• Pharyngocutaneous fistulae (5)Pharyngocutaneous fistulae (5)•• Resume oral intake 2Resume oral intake 2--3 weeks3 weeks•• Average hospital stay 13 daysAverage hospital stay 13 days•• Late stricture in 11 patientsLate stricture in 11 patients•• Most after XRTMost after XRT•• Donor site morbidity: Significant in RFFDonor site morbidity: Significant in RFF
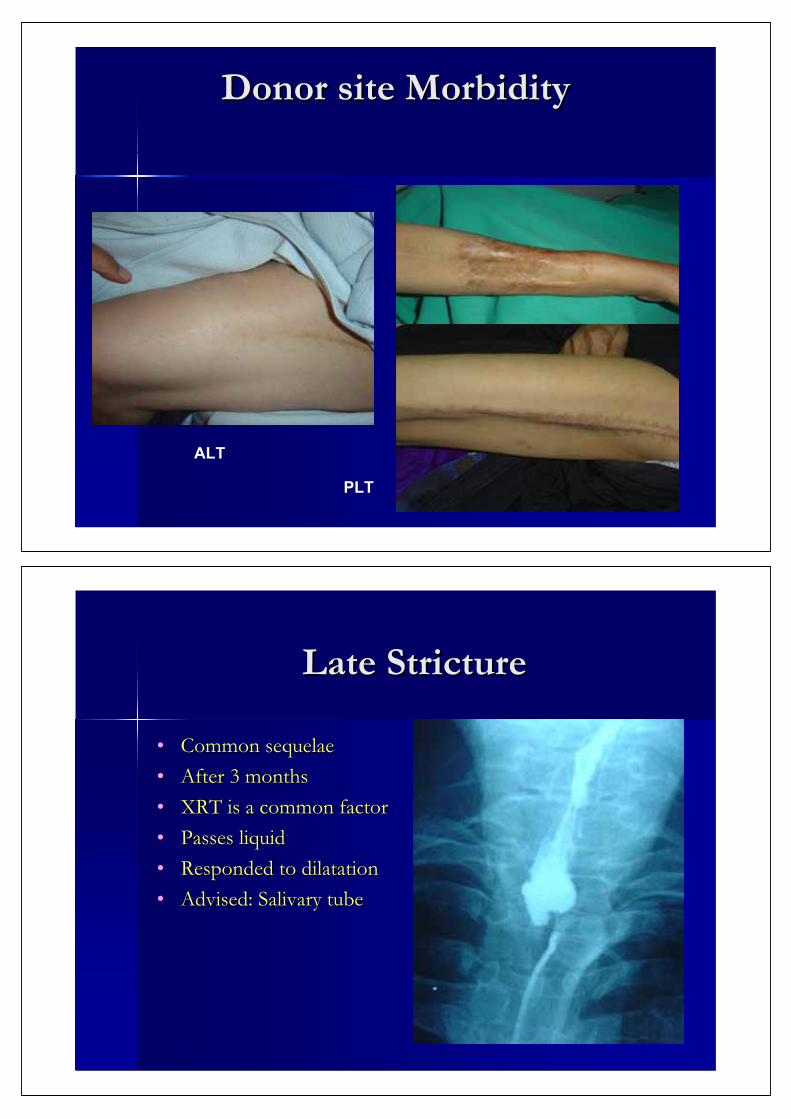
Donor site MorbidityDonor site Morbidity
ALT RF
PLT
Late StrictureLate Stricture
•• Common sequelaeCommon sequelae•• After 3 monthsAfter 3 months•• XRT is a common factorXRT is a common factor•• Passes liquidPasses liquid•• Responded to dilatationResponded to dilatation•• Advised: Salivary tube Advised: Salivary tube
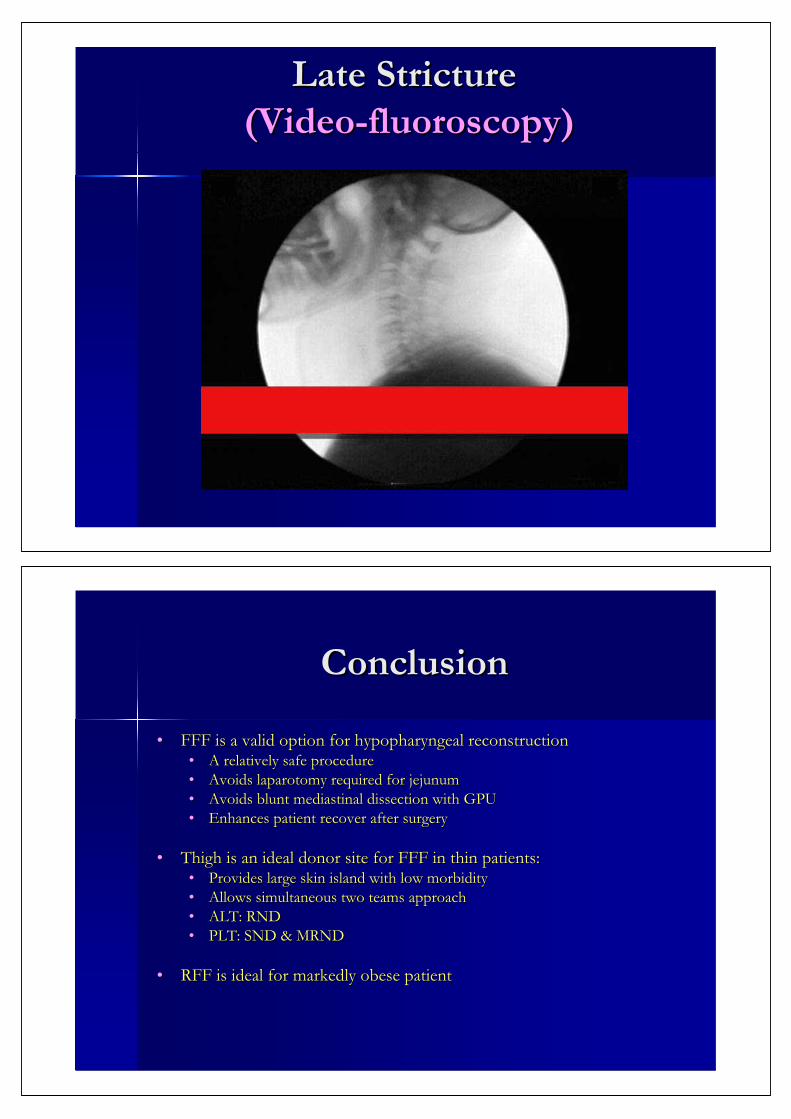
Late Stricture Late Stricture (Video(Video--fluoroscopy)fluoroscopy)
ConclusionConclusion
•• FFF is a valid option for hypopharyngeal reconstructionFFF is a valid option for hypopharyngeal reconstruction•• A relatively safe procedureA relatively safe procedure•• Avoids laparotomy required for jejunumAvoids laparotomy required for jejunum•• Avoids blunt mediastinal dissection with GPUAvoids blunt mediastinal dissection with GPU•• Enhances patient recover after surgeryEnhances patient recover after surgery
•• Thigh is an ideal donor site for FFF in thin patients:Thigh is an ideal donor site for FFF in thin patients:•• Provides large skin island with low morbidityProvides large skin island with low morbidity•• Allows simultaneous two teams approachAllows simultaneous two teams approach•• ALT: RNDALT: RND•• PLT: SND & MRNDPLT: SND & MRND
•• RFF is ideal for markedly obese patientRFF is ideal for markedly obese patient
NCI, Cairo University