Embed Size (px)
Citation preview

Dallas Presbyterian HospitalInternal Medicine Resident Lecture
August 28, 2008Samir Shah, MD
Neurology Consultants of Dallas
STROKE, SUBARACHNOID HEMORRHAGE AND HYPOTHERMIA
FOR CARDIAC ARREST
-Andy Rekito

Quick Stroke Facts - 2008FACT: About 780,000 Americans suffer a new or recurrent stroke each year. That means, on average, a stroke occurs every 40 seconds.
FACT: Stroke kills nearly 150,000 people each year. That’s about 1 of every 16 deaths. It remains the #3 cause of death behind heart disease and cancer. An American dies of a stroke every 3 minutes.
FACT: Americans will pay about $63 billion in 2007 for stroke related medical costs and disability.
American Heart Association. Heart Disease and Stroke Statistics — 2008 Update. Dallas, Tex.: American Heart Association; 2008.

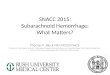
Prevalence of Stroke by Age and Sex
NHANES: 1999-2002
Source: CDC/NCHS and NHLBI.
1.1
3.1
6.6
11.5
0.41.2
12.0
0.3 0.82.1
3.0
6.3
0
2
4
6
8
10
12
14
20-34 35-44 45-54 55-64 65-74 75+
Ages
Per
cen
t o
f P
op
ula
tio
n
Men Women
`
FACT: Prevalence of stroke in the US is 5.7 million people (2004). 15-30% of stroke victims are permanently disabled.

Definitions – So We’re All on the Same Page
An established and universally accepted definition for stroke by the World Health Organization is "acute neurologic dysfunction of vascular origin . . . with symptoms and signs corresponding to the involvement of focal areas of the brain."
Stroke. 1989 Oct;20(10):1407-31.

BEFORE
Stroke has also been described as the rapid onset of neurological deficits that persist for at least 24 hours and are caused either by intracerebral or subarachnoid hemorrhage or by partial or complete blockage of a blood vessel supplying or draining a part of the brain, leading to the infarction of brain tissue. A stroke is distinguished from a transient ischemic attack (TIA) by the fact that neurological deficits in TIAs clear spontaneously within 24 hours.

NOW
Clinical, experimental, and imaging data have shown that the 24-hour criterion is inaccurate in suggesting an absence of brain injury and often results in uncertainty — on the part of patients and practitioners alike — about what to do when a TIA occurs. In short, the 24-hour definition of TIA is outdated, confusing, and potentially misleading…

NEW DEFINITIONa TIA is a brief episode of neurologic dysfunction caused by focal brain or retinal ischemia, with clinical symptoms typically lasting less than one hour, and without evidence of acute infarction. The corollary is that persistent clinical signs or characteristic imaging abnormalities define infarction — that is, stroke (N Engl J Med 2002;347:1713-1716).

THEREFORE
The development of symptoms of acute brain ischemia constitutes a medical emergency and transient symptoms do not exclude the possibility of associated brain infarction.
TIME=BRAIN
Now, let’s talk about how we evaluate and manage stroke.We will focus on ischemic stroke…

Consult for a 68 year-old man that has new right-sided weakness and is “talking funny.” It started a few hours ago.

What Else Could It Be?Stroke Mimics
AbcessSubdural and Epidural HematomasTumorsGiant aneurysmsVascular malformations (AVMs)Hypertensive EncephalopathyEncephalitis/cerebritisSeizure/Todd’s paralysisMigraineMetabolic-Hypoglycemia/HyperglycemiaCerebral venous thrombosisPsychogenicDeficit from previous stroke made worse by general medical condition

When presented with acute onset neurological dysfunction, stroke should always be on your differential and one of the first goals in the evaluation is differentiating hemorrhagic stroke from ischemic stroke
All patients, with few exceptions should undergo STAT cranial imaging. In other words, GET A NON-CONTRAST HEAD CT (MRI if available STAT).
Quickly Narrow the Differential With Imaging

What Else to Ask for Over the Phone?
ALL stroke patients should get immediate
CBC with plateletsBedside glucosePTT, PT (INR)Chem 7 (Chem 10)EKG, continuous cardiac monitoringIV access, 0.9% NS (no glucose)NPO?Troponin

What’s the Cardiac Workup for?Not infrequently, patients with acute cerebral ischemia have concomitant acute myocardial ischemia
In addition cardiac evaluation helps determine etiology of the cerebral event
Several small studies have shown that patients with TIA and
stroke have a high prevalence of asymptomatic CHD. These studies suggest that 20% to 40% of stroke patients may have
abnormal tests for silent cardiac ischemia.
2% to 5% of patients with acute ischemic stroke have fatal cardiac-related events in the short term after stroke.
Circulation. 2003;108:1278.

Other Acute Studies
Urine pregnancy testUrine toxicologyHypercoagulable screenCXRType and Screen

What are the risk factors for ischemic stroke?

Risk Factors for Ischemic Stroke
Risks that can be controlled or treated
High Blood PressureSmokingDiabetes MellitusPrior TIA Atrial FibrillationOther Heart DiseaseCarotid Artery Disease or atherosclerosis in another arterial bedCertain blood disordersSickle Cell DiseaseHypercholesteremiaPhysical Inactivity, ObesityExcessive alcoholIllicit drugsHRT
Risks that cannot change
AgePrior stroke or MIGenderHeredity/Ethnicity

2.64.0 5.4
8.4
1.1 2.0
19.1
22.4
14.8
27.0
6.33.5
0
5
10
15
20
25
30
A B C D E F
Es
tim
ate
d 1
0-Y
ea
r R
ate
(%
)
Men Women
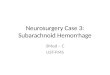
Estimated 10-Year Stroke Risk in 55-Year-Old Adults According to Levels of Various Risk Factors - Framingham Heart Study
AA BB CC DD EE FFSystolic BPSystolic BP 95-10595-105 130-148130-148 130-148130-148 130-148130-148 130-148130-148 130-148130-148DiabetesDiabetes NoNo NoNo YesYes YesYes YesYes YesYesCigarettesCigarettes NoNo NoNo NoNo YesYes YesYes YesYesPrior Atrial Fib.Prior Atrial Fib. NoNo NoNo NoNo NoNo Yes Yes YesYesPrior CVDPrior CVD NoNo NoNo NoNo NoNo NoNo YesYes
Source: Stroke 1991;22:312-318.

General elderly male population 0.6 -------Asymptomatic carotid disease 1.3 3.4Transient monocular blindness 2.2 3.5Transient ischemic attack 3.7 2.3Minor stroke 6.1 3.2Major stroke 9.0 3.5Symptomatic carotid stenosis >70% 15 2.0
Annual Probability(%) Stroke Vascular Death
Cerebrovascular Features
Estimates of Vascular Event Rates for Persons With Various Features of Atherothrombotic Cerebrovascular Disease
Stroke. 1997;28:1507-1517.

Risk Factors for Intracerebral and Subarachnoid Hemorrhage
++ indicates strong evidence; +, moderate positive evidence; ?, equivocal evidence; –, moderate inverse evidence; and 0, no relation.
Age ++ +
Women - +
Race/ethnicity + +
Hypertension ++ +
Cigarette smoking ? ++
Heavy use of alcohol ++ ?
Anticoagulation ++ ?
Amyloid angiopathy ++ 0
Hypocholesterolemia ? 0
Oral Contraceptives 0 ?
ICH SAH
Stroke. 1997;28:1507-1517.

What Else Will You Ask?
Exact time of onset or last time the patient was last seen at baselineHistory of seizures? Any seizure activity prior to onset of symptomsMigraine headachesTrauma or neck injury in the preceding daysRecent illnessesVomiting, change in level of consciousnessAllergies MedicationsAssociated symptoms (?chest pain)

What to Do on Exam?
ABCs firstVital Signs: especially notice BP and don’t forget weightCardiac, vascular, extremity examinationDirected and focused exam based on history - NIHSS

NIH Stroke Scale – focuses on 5 major areas
Level of consciousness
Visual function
Motor function
Sensation and neglect
Cerebellar function
NIHSS is easily performed, reliable and valid. It is strongly associated with outcome with and without thrombolytics, and can predict those patients likely to develop hemorrhagic complications from thrombolytic use.

www.ferne.org

Goal of History and Physical Is to Localize Lesion and Its
Vascular Supply
Knowing the location of the lesion and its vascular supply allow you to begin to speculate on the underlying pathophysiology as different stroke mechanisms characteristically affect certain cerebral vessels.

Blood Supply of the Brain
Anterior Circulation: Two ICAs which divide into ACA and MCA. Each ICA supplies roughly two fifths of the brain by volume.
Posterior Circulation: Two Vertebrals which join to form the Basilar which then forms PCAs. The posterior circulation supplies roughly one fifth of the brain.

Source: Loyola University Neurovascular Tutorial




Four Divisions of the Vertebral Artery




Stroke Mechanisms
Can simplify stroke mechanisms or etiologies into 5 categories
ISCHEMIA1. Thrombosis (60%)2. Embolism (20%)3. Decreased Systemic PerfusionHEMORRHAGE4. Intracerebral Hemorrhage (12%)5. Subarachnoid Hemorrhage (8%)

Common Stroke MechanismsThe Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy
STROKE
Ischemic Stroke
Primary HemorrhageIntraparenchymalSubarachnoid
Atherosclerotic Cerebrovascular
Disease(“Large Artery”)
Hypoperfusion Arteriogenic Emboli
Penetrating Artery Disease
(“Lacunes”)
Cardiogenic Embolism
Cryptogenic Stroke
Other, Unusual Causes
Prothrombotic StatesDissectionsArteritisMigraine/vasospasmDrug AbuseMany More
Atrial Fibrillation
Valve Disease
Ventricular Thrombi
Many Others
15%85%
20% 25% 20% 30% 5%

You are done thinking of stroke mechanisms and you are almost at the ER when you get paged by the doctor that the patient has a blood pressure that is “sky high” at 182/102 and that he is going to give him some oral clonidine to take care of it.
What should you tell her?

Cerebral Autoregulation:It may not be working
DO NOT TREAT BP IN ACUTE ISCHEMIC STROKE UNLESS BP>200-220/100-120

The patient’s daughter is at the bedside. She tells you that her dad had some right sided weakness yesterday that resolved in 25 minutes and that’s why she brought him in. She says his new symptoms on the right started in the hospital just 45 minutes ago. She says he has some kind of heart problem but hasn’t been taking any of his medications. She’s not sure what he was taking and is worried about his talking.
The Patient Encounter

You examine the patient and with your excellent neurological skills quickly realize that his “talking funny” is actually an expressive aphasia and that he has a right facial droop, a left gaze preference, 2/5 right arm weakness and 4/5 right leg weakness.
All the labs you wanted are unrevealing, and the EKG shows evidence of LVH, but otherwise ok. The nurse tells you that the monitor went off a little while ago for a rapid, irregular heart rate.
You are astute enough to realize that this guy is in the usual 3 hour window for acute stroke therapy and decide to go look at the CT scan.

Now what?

Hyperdense MCA Sign

Insular Ribbon Sign
Loss of Gray-White Junction

The New England
Journal of Medicine©Copyright, 1995, by the Massachusetts Medical Society
Volume 333 DECEMBER 14, 1995 Number 24
TISSUE PLASMINOGEN ACTIVATOR FOR ACUTE ISCHEMIC STROKE
THE NATIONAL INSTITUTE OF NEUROLOGICAL DISORDERS AND STROKE rt-PA STROKE STUDY GROUP*
IV t-PA FDA approved for use in acute ischemic stroke < 3 hours from onset in 1996. As compared with patients given placebo, patients treated with t-PA were at least 30 percent more likely to have minimal or no disability at three months on the assessment scales.

The Use of IV t-PA
Eligibility
Age 18 or olderClinical diagnosis of ischemic stroke causing a measurable neurological deficitTime of symptom onset well established to be less than 180 minutes before treatment would begin

Contraindications
Evidence of intracranial hemorrhage on pretreatment CTClinical presentation suggestive of SAH, even with normal CTActive internal bleedingKnown bleeding diathesis, including but not limited to:
Platelet count < 100,000/mm3
Patient has received heparin within 48 hours and has an elevated aTT (greater than upper limit of normal for laboratory)Current use of oral anticoagulants or recent use with an elevated prothrombin time > 15 seconds
Within 3 months any intracranial surgery, serious head trauma, or previous strokeOn repeated measurements, systolic blood pressure greater than 185 mmHg or diastolic blood pressure greater than 110 mmHg at the time treatment is to begin, and the patient requires aggressive treatment to reduce blood pressure to within these limitsHistory of intracranial hemorrhageKnown AVM or aneurysm

Warnings
Only minor or rapidly improving stroke symptomsHistory of GI or Urinary tract hemorrhage within 21 daysRecent arterial puncture at a noncompressible siteRecent lumbar punctureAbnormal blood glucose (<50 or >400 mg/dL)Post myocardial infarction pericarditisPatient was observed to have a seizure at the same time the onset of stroke symptoms were observed

Other relative contraindications (not NINDS)
Bacterial endocarditis or CNS lesion likely to hemorrhage after t-PA
Significant trauma within 3 months
CPR with chest compressions within past 10 days
Major surgery within past 14 days, minor surgery within past 10 days
Pregnant (up to 10 days postpartum) or nursing woman
Life expectancy < 1 year from other causes
Peritoneal dialysis or hemodialysis

What to Tell the Family
After you determine your patient’s eligibility based on NINDS criteria, you go and talk with the daughter about the risks and benefits
What are the risks?Bleeding and its complications (6% vs <1%) and allergic reaction (1 to 2%)
She asks what is the benefit?Patient’s treated with t-PA were at least 30% more likely to have minimal or no disability at three months despite increased risk of hemorrhage. ARR=16%, NNT=6 (Similar to CEA for symptomatic carotid stenosis)

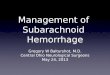
Copyright ©1999 American Heart Association
Grotta, J. C. Stroke 1999;30:1722-1728
Distribution of outcomes on NIH Stroke Scale (NIHSS) (top), Barthel index (middle), and Rankin scale (bottom) in parts 1 and 2 combined of the NINDS
rtPA Stroke Study

You write to administer t-PA at 0.9mg/kg (max 90mg) infused over 60 minutes with 10% of the dose administered as a bolus over 1 minute. You ensure that BPs have been consistently less than 185/110 prior to administration. You also make sure that no other antithrombotics or anticoagulants will be given in the next 24 hours and write for a Head CT in 24 hours. You also write orders for ICU admission as you know the patient will need close BP monitoring over the next 24 hours per NINDS protocol to maintain BP<180/105.

Let’s Get Serious
Only a small fraction of ischemic strokes (likely 1-3%) are treated with IV t-PA, mostly because patients arrive to medical attention after the 3 hour time window. At places without 24 hour neurointerventional capability, what do we do for a stroke acutely when the patient is not eligible for IV t-PA?

This CT has a clear hypodensity. This patient is not eligible for IV-tPA given days duration of symptoms. In patients that do not receive thrombolysis: In the acute period, all ischemic stroke patients should receive 160-325mg of ASA within 48hours of onset. (some may advocate acute anticoagulation for certain stroke subtypes).Antithrombotic and Thrombolytic Therapy for Ischemic Stroke: The
Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy

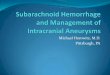
Copyright ©2000 American Heart Association
Chen, Z. et al. Stroke 2000;31:1240-1249
Absolute effects in CAST and IST of early use of aspirin in 40 000 randomized patients with suspected acute ischemic stroke
For every 1000 acute strokes treated with ASA, 7 fewer early recurrent ischemic strokes were observed and 13 fewer patients will be dead or dependent at 6 months at the expense of two or more ICHs.

All stroke patients should be admitted to the hospital for observation, diagnostic evaluation, and determination of treatment for secondary stroke prevention. All patients should be admitted to a stroke unit or when not available to a cardiac monitored bed with staffing to perform frequent neurological checks.
As already discussed, thrombolysis patients need ICU care.
Admit the Patient

Where would you admit this patient?

How about this patient?

Let’s say the patient’s symptoms resolved by the time you got there and he now feels fine and wants to go home

TIAs carry a substantial short term risk of stroke, hospitalization for cardiovascular events, and death. Of 1,707 TIA patients evaluated in an emergency department of a large health care plan, 180 patients or 10 percent developed stroke within 90 days. 91 patients or 5 percent did so within 2 days. Predictors of stroke: more than 60 years of age, DM, focal symptoms of weakness or speech impairment, and TIA lasting longer than 10 minutes (JAMA 2000;284:2901-6).
PATIENT IS AT HIGH RISK AND NEEDS TO BE ADMITTED

Evaluation During Admission
1. Labs: LFTs, fasting lipid profile and glucose, QID bedside glucose and SSI. Consider Hypercoagulable workup, ESR, ANA, hsCRP, HbA1c, homocysteine, LP
2. Imaging: All patients should have MRI imaging of brain and vascular imaging of head and neck. Consider TCD, PET, SPECT or other study based on clinical findings
3. Echocardiogram: all patient should have echo – TTE when h/o of CAD or abnormal EKG or lacunar event. All others TEE (more sensitive and cost effective in evaluation of stroke. Ann Intern Med. 1997 Nov 1;127(9):775-87.)
4. Rehabilitation evaluation5. Bedside or formal swallow evaluation6. Medications: Home medications except BP meds. Restart or add
after patient stable for >48hrs. Again, in general do not treat BP unless >220/120 in the acute phase
7. DVT and GI prophylaxis if indicated

Hospital Initiation of Secondary Prevention
All patients receive statin with goal LDL<100. Established evidence in patients with CAD and atherosclerotic ischemic stroke. Atorvastatin 80mg qd SPARCL
All patients given BP meds with goal <140/90 or <130/80 with DM or renal disease. Prefer ACEI or ARB and thiazide diuretic PROGRESS (B-blocker if CAD)
Smoking Cessation
Diet and Exersice Regimen
Stroke Education

Antithrombotic / Anticoagulant Therapy
In patients who have experienced a noncardioembolic stroke or TIA, we recommend treatment with an anti-platelet agent. Aspirin at a dose of 50 to 325mg qd; the combination of aspirin, 25mg and extended-release dipyridamole, 200mg bid; or clopidogrel, 75mg qd, are all acceptable options for initial therapy
No good evidence on what to do if patient already on therapy
In patients with Afib who have suffered a recent stroke or TIA, we recommend long-term oral anticoagulation, INR range 2-3
?Best treatment in cryptogenic stroke, PFO, aortic disease, post-MI
?Use of IV Heparin in certain situations—brain goal PTT of 45-65Antithrombotic and Thrombolytic Therapy for Ischemic Stroke: The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy

Copyright restrictions may apply.
Kidwell, C. S. et al. JAMA 2004;292:1823-1830.
Acute Intraparenchymal Hematoma Imaged With Computed Tomography and With Magnetic Resonance Imaging









The Ischemic Penumbra
Approximated by PWI-DWI MRI Mismatch and used to help guide interventional acute stroke therapies…

IA t-PA within 6 hours of stroke onset in anterior circulation and 24+ hours in posterior circulation
Mechanical Clot removal within 8+ hours of ischemic stroke (MERCI) Stroke. 2005;36:1432.



Subarachnoid Hemorrhage
Causes:Aneurysm (80% of non-traumatic cases)TraumaVascular MalformationsTumorsInfectionVenous Thrombosis

Subarachnoid Hemorrhage(Aneurysmal)
Demographics:Mean age = 55 yearsWomen 1.6X > MenBlacks > WhitesAverage Case Fatality Rate > 50%

Subarachnoid Hemorrhage(Aneurysmal)
Risk Factors:SmokingHypertensionCocaine UseHeavy alcohol useFirst degree relatives with SAH

Subarachnoid Hemorrhage
Clinical Features:Sudden severe headache (thunderclap headache)NauseaVomitingNeck PainPhotophobiaLoss of consciousness
Retinal hemorrhages (subhyaloid hemorrhage)MeningismusLocalizing neurological signs

Subarachnoid Hemorrhage
Diagnostic Evaluation:Head CT
Sensitivity > 90% in first 24 hoursSensitivity drops to 50% at 1 week
Lumbar PunctureFinding to look for is xanthochromia (12 hours to develop)

Subarachnoid Hemorrhage
Treatment:Blood Pressure
Low before aneurysm securedHigh after aneurysm secured
Treat hyperglycemia and hyperthermiaDVT prophylaxis (Heparin after aneurysm secured)Nimodipine 60mg PO q 4 hours X 21 daysSecure aneurysm
Neurosurgical ClippingEndovascular Coiling (favored in ISAT)

Subarachnoid Hemorrhage
Complications:Rebleeding (7%)Vasospasm (46%) Highest incidence 3-12 days after SAH
Screen with TCDTreat with Hypervolemia and Induced HypertensionAngiography
Hydrocephalus (20%)EVDPermanent Shunt
Seizures (30%)Antiepileptics for 1 week to 1 month

Unconscious adult patients with spontaneous circulation after out-of-hospital cardiac arrest should be cooled to 32°C
to 34°C for 12 to 24 hours when the initial rhythm was ventricular fibrillation (VF).
HYPOTHERMIA
Such cooling may also be beneficial for other rhythms or in-hospital cardiac arrest.
Circulation. 2003;108:118