-
7/27/2019 Cor Pulmonale Emedicine
1/16
emedicine.medscape.com
eMedicine Specialties > Cardiology > Myocardial Disease
and Cardiomyopathies
Cor Pulmonale
Al i A Sovar i, MD, Clinical and Research Fellow in
Cardiovascular Medicine, Section of Cardiology, University of
Illinois at ChicagoRavi H Dave, MD, Associate Professor of
Medicine, University of California at Los Angeles David Geffen
School of Medicine;Abraham G Kocheril , MD,FACC, FACP, FHRS,
Professor of Medicine, Director of Clinical Electrophysiology,
University of Illinois at Chicago
Updated: Jul 22, 2010
Introduction
Background
Cor pulmonale is defined as an alteration in the structure and
function of the right ventricle caused by a primary disorder of
the
respiratory system. Pulmonary hypertension is the common link
between lung dysfunction and the heart in cor pulmonale.
Right-sided
ventricular disease caused by a primary abnormality of the left
side of the heart or congenital heart disease is not considered
cor
pulmonale, but cor pulmonale can develop secondary to a wide
variety of cardiopulmonary disease processes. Although cor
pulmonale commonly has a chronic and slowly progressive course,
acute onset or worsening cor pulmonale with life-threatening
complications can occur.[1 ]
Pathophysiology
Several different pathophysiologic mechanisms can lead to
pulmonary hypertension and, subsequently, to cor pulmonale.
These
pathogenetic mechanisms include (1) pulmonary vasoconstriction
due to alveolar hypoxia or blood acidemia, (2) anatomic
compromise of the pulmonary vascular bed secondary to lung
disorders (eg, emphysema, pulmonary thromboembolism,
interstitial
lung disease, adult respiratory distress syndrome, and
rheumatoid disorders), (3) increased blood viscosity secondary to
blood
disorders (eg, polycythemia vera, sickle cell disease,
macroglobulinemia), (4) increased blood flow in pulmonary
vasculature, and (5)
idiopathic primary pulmonary hypertension. The result is
increased pulmonary arterial pressure.
The right ventricle (RV) is a thin-walled chamber that is more a
volume pump than a pressure pump. It adapts better to changing
preloads than afterloads. With an increase in afterload, the RV
increases systolic pressure to keep the gradient. At a point, a
further
increase in the degree of pulmonary arterial pressure produces
significant RV dilation, an increase in RV end-diastolic pressure,
and
RV circulatory collapse. A decrease in RV output with a decrease
in diastolic left ventricle (LV) volume results in decreased LV
output.
Since the right coronary artery, which supplies the RV free
wall, originates from the aorta, decreased LV output diminishes
blood
pressure in the aorta and decreases right coronary blood flow.
What ensues is a vicious cycle between decreases in LV and
RVoutput.
Genetic investigations have confirmed that morphogenesis of the
right and left ventricle originated from different sets of
progenitor
cells and sites. This polymorphism could explain the differing
rates of hypertrophy of the right and left ventricles.[2 ]
Right ventricular overload is associated with septal
displacement toward the left ventricle. Septal displacement, which
is seen on
echocardiography, can be another factor that decreases LV volume
and output in the setting of cor pulmonale and right
ventricular
enlargement. Several pulmonary diseases cause cor pulmonale,
which may involve interstitial and alveolar tissues with a
secondary
effect on pulmonary vasculature or may primarily involve
pulmonary vasculature. Chronic obstructive pulmonary disease (COPD)
is
the most common cause of cor pulmonale in the United States.
Cor pulmonale usually presents chronically, but 2 main
conditions can cause acute cor pulmonale: massive pulmonary
embolism
(more common) and acute respiratory distress syndrome (ARDS).
The underlying pathophysiology in massive pulmonary embolismcausing
cor pulmonale is the sudden increase in pulmonary resistance. In
ARDS, 2 factors cause RV overload: the pathologic
features of the syndrome itself and mechanical ventilation.
Mechanical ventilation, especially higher t idal volume, requires a
higher
transpulmonary pressure. In chronic cor pulmonale, right
ventricular hypertrophy (RVH) generally predominates. In acute
cor
pulmonale, right ventricular dilatation mainly occurs. In the
case of ARDS, cor pulmonale is associated with increased
possibility of
right to left shunt through patent foramen ovale and caries
poorer prognosis.[3 ]
Frequency
United States
z Cor pulmonale is estimated to account for 6-7% of all types of
adult heart disease in the United States, with chronic
obstructive
pulmonary disease (COPD) due to chronic bronchitis or emphysema
the causative factor in more than 50% of cases.
z At present, cor pulmonale accounts for 10-30% of decompensated
heart failure related admissions in the United States.[4 ]
z Although the prevalence of COPD in the United States is about
15 million, the exact prevalence of cor pulmonale is difficult
to
determine because it does not occur in all cases of COPD, and
the physical examination and routine tests are relatively
Seite 1 von 16Cor Pulmonale: [Print] - eMedicine Cardiology
04.10.2010http://emedicine.medscape.com/article/154062-print
-
7/27/2019 Cor Pulmonale Emedicine
2/16
insensitive for the detection of pulmonary hypertension.
z In contrast, acute cor pulmonale is usually secondary to
massive pulmonary embolism.
z Acute massive pulmonary thromboembolism is the most common
cause of acute life-threatening cor pulmonale in adults.
z In the United States, 50,000 deaths are estimated to occur per
year from pulmonary emboli and about half occur within the
first
hour due to acute right heart failure.
International
The incidence of cor pulmonale varies among different countries
depending on the prevalence of cigarette smoking, air pollution,
and
other risk factors for various lung diseases.
Mortality/Morbidity
Development of cor pulmonale as a result of a primary pulmonary
disease usually heralds a poorer prognosis. For example,
patients
with COPD who develop cor pulmonale have a 30% chance of
surviving 5 years. However, whether cor pulmonale carries an
independent prognostic value or is simply reflecting the
severity of underlying COPD or other pulmonary disease is not
clear.
Prognosis in the acute setting due to massive pulmonary embolism
or ARDS has not previously been shown to be dependent on the
presence or absence of cor pulmonale. However, a prospective,
multicenter cohort study by Volschan et al indicates that in cases
of
pulmonary embolism, cor pulmonale may be a predictor of
inhospital mortality.[5 ]
The authors collected demographic, comorbidity, andclinical
manifestation data on 582 patients admitted to emergency or
intensive care units and diagnosed with pulmonary embolism.
Assessing the information using logistic regression analysis,
the investigators built a prediction model. Their results indicated
that in
hemodynamically stable patients with pulmonary embolism, the
following factors may be independent predictors of inhospital
mortality:
z Age over 65 years
z Bed rest for longer than 72 hours
z Chronic cor pulmonale
z Sinus tachycardia
z Tachypnea
Clinical
History
Clinical manifestations of cor pulmonale generally are
nonspecific. The symptoms may be subtle, especially in early stages
of the
disease, and mistakenly may be attributed to the underlying
pulmonary pathology.
z The patient may complain of fatigue, tachypnea, exertional
dyspnea, and cough.
z Anginal chest pain also can occur and may be due to right
ventricular ischemia (it usually does not respond to nitrates)
or
pulmonary artery stretching.
z Hemoptysis may occur because of rupture of a dilated or
atherosclerotic pulmonary artery. Other conditions, such as
tumors,
bronchiectasis, and pulmonary infarction, should be excluded
before attributing hemoptysis to pulmonary hypertension.
Rarely,
the patient may complain of hoarseness due to compression of the
left recurrent laryngeal nerve by a dilated pulmonary artery.
z A variety of neurologic symptoms may be seen due to decreased
cardiac output and hypoxemia.
z In advanced stages, passive hepatic congestion secondary to
severe right ventricular failure may lead to anorexia, right
upper
quadrant abdominal discomfort, and jaundice.
z Syncope with exertion, which may be seen in severe disease,
reflects a relative inability to increase cardiac output during
exercise with a subsequent drop in the systemic arterial
pressure.
z Elevated pulmonary artery pressure can lead to elevated right
atrial, peripheral venous, and capillary pressure. By
increasing
the hydrostatic gradient, it leads to transudation of fluid and
accumulation of peripheral edema. Although this is the simplest
explanation for peripheral edema in cor pulmonale, other
hypotheses explain this symptom, especially in a fraction of
patients
with COPD who do not show increase in right atrial pressure. A
decrease in glomerular filtration rate (GFR) and filtration of
sodium and stimulation of arginine vasopressin (which decreases
free water excretion) due to hypoxemia play important
Seite 2 von 16Cor Pulmonale: [Print] - eMedicine Cardiology
04.10.2010http://emedicine.medscape.com/article/154062-print
-
7/27/2019 Cor Pulmonale Emedicine
3/16
pathophysiologic roles in this setting and may even have a role
for peripheral edema in patients with cor pulmonale who have
elevated right atrial pressure.[6 ]
Physical
Physical findings may reflect the underlying lung disease or
pulmonary hypertension, RVH, and RV failure.
z On inspection, an increase in chest diameter, labored
respiratory efforts with retractions of the chest wall, distended
neck veins
with prominent a orv waves, and cyanosis may be seen.
z On auscultation of the lungs, wheezes and crackles may be
heard as signs of underlying lung disease. Turbulent flow
through
recanalized vessels in chronic thromboembolic pulmonary
hypertension[7 ]may be heard as systolic bruits in the lungs.
Splitting
of the second heart sound with accentuation of the pulmonic
component can be heard in early stages. A systolic ejection
murmur with sharp ejection click over the region of the
pulmonary artery may be heard in advanced disease, along with a
diastolic pulmonary regurgitation murmur. Other findings upon
auscultation of the cardiovascular system may be third and
fourth sounds of the heart and systolic murmur of tricuspid
regurgitation.
z RVH is characterized by a left parasternal or subxiphoid
heave. Hepatojugular reflux and pulsatile liver are signs of RV
failure
with systemic venous congestion.
z On percussion, hyperresonance of the lungs may be a sign of
underlying COPD; ascites can be seen in severe disease.
z Examination of the lower extremities reveals evidence of
pitting edema. Edema in cor pulmonale is strongly associated
with
hypercapnia.[8 ]
Causes
Etiologies of cor pulmonale can mechanistically be categorized
in 5 groups.
1. Pulmonary vasoconstriction due to alveolar hypoxia or blood
academia: This can result in pulmonary hypertension and if the
hypertension is severe enough, it causes cor pulmonale.
2. Various lung disorders: Parenchymal or alveolar lung
disorders may anatomically compromise the vasculature beds and
cause
elevated pulmonary blood pressure. Chronic obstructive pulmonary
disorder is the most common cause of cor pulmonale.
Other lung disorders that may cause cor pulmonale are pulmonary
thromboembolism, interstitial lung disease, and adult
respiratory distress syndrome. Also, some connective tissue
disorders with pulmonary involvement may result in pulmonary
hypertension and cor pulmonale.
3. Blood disorders that are associated with increased blood
viscosity such as polycythemia vera, sickle cell disease,
macroglobulinemia
4. Increased blood flow in the pulmonary vasculature
5. Idiopathic primary pulmonary hypertension
Differential Diagnoses
Other Problems to Be Considered
Congestive (biventricular) heart failure
Primary pulmonic stenosis
Primary pulmonary hypertension
Right-sided heart failure due to congenital heart diseasesRight
heart failure due to right ventricular infarction
Ventricular septal defect
Constrictive pericarditis
High-output heart failure
Infiltrative cardiomyopathies
Atrial myxoma
Workup
Laboratory Studies
z Laboratory investigations are directed toward defining the
potential underlying etiologies as well as evaluating complications
of
cor pulmonale. In specific instances, appropriate lab studies
may include the following: hematocrit for polycythemia (which
can
be a consequence of underlying lung disease but can also
increase pulmonary arterial pressure by increasing viscosity),
serum alpha1-antitrypsin if deficiency is suspected, and
antinuclear antibody level for collagen vascular disease such
as
scleroderma. Hypercoagulability states can be evaluated by serum
levels of proteins S and C, antithrombin III, factor V
Seite 3 von 16Cor Pulmonale: [Print] - eMedicine Cardiology
04.10.2010http://emedicine.medscape.com/article/154062-print
-
7/27/2019 Cor Pulmonale Emedicine
4/16
Leyden, anticardiolipin antibodies, and homocysteine.
z Arterial blood gas tests may provide important information
about the level of oxygenation and type of acid-base disorder.
z Elevated brain natriuretic peptide (BNP) level alone is not
adequate to establish presence of cor pulmonale, but it helps
to
diagnose cor pulmonale in conjunction with other noninvasive
tests and in appropriate clinical settings. An elevated BNP
level
may actually be a natural mechanism to compensate for elevated
pulmonary hypertension and right heart failure by promoting
diuresis and natriuresis, vasodilating systemic and pulmonary
vessels, and reducing circulating levels of endothelin and
aldosterone.
Imaging Studies
A general approach to diagnose cor pulmonale and to investigate
its etiology starts with routine laboratory tests, chest
radiography,
and electrocardiography. Echocardiography gives valuable
information about the disease and its etiology. Pulmonary function
tests
may become necessary to confirm the underlying lung disease.
Ventilation/perfusion (V/Q) scan or chest CT scan may be
performed
if history and physical examination suggest pulmonary
thromboembolism as the cause or if other diagnostic tests do not
suggest other
etiologies. Right heart catheterization is the most accurate but
invasive test to confirm the diagnosis of cor pulmonale and
gives
important information regarding the underlying diseases. Any
abnormal result in each of these tests may need further
diagnostic
evaluation in that specific direction.
Imaging studies may show evidence of underlying cardiopulmonary
diseases, pulmonary hypertension, or its consequence, right
ventricular enlargement.
z Chest roentgenography: In patients with chronic cor pulmonale,
the chest radiograph may show enlargement of the central
pulmonary arteries with oligemic peripheral lung fields.
Pulmonary hypertension should be suspected when the right
descending pulmonary artery is larger than 16 mm in diameter and
the left pulmonary artery is larger than 18 mm in diameter.
Right ventricular enlargement leads to an increase of the
transverse diameter of the heart shadow to the right on the
posteroanterior view and filling of the retrosternal air space
on the lateral view. These findings have reduced sensitivity in
the
presence of kyphoscoliosis or hyperinflated lungs.
z Echocardiography: Two-dimensional echocardiography usually
demonstrates signs of chronic RV pressure overload. As this
overload progresses, increased thickness of the RV wall with
paradoxical motion of the interventricular septum during
systole
occurs. At an advanced stage, RV dilatation occurs and the
septum shows abnormal diastolic flattening. In extreme cases,
the
septum may actually bulge into the left ventricular cavity
during diastole resulting in decreased diastolic volume of LV
and
reduction of LV output.
z Doppler echocardiography is now used to estimate pulmonary
arterial pressure, taking advantage of the functional tricuspid
insufficiency that is usually present in pulmonary hypertension.
Doppler echocardiography is considered the most reliable
noninvasive technique to estimate pulmonary artery pressure. The
efficacy of Doppler echocardiography may be limited by the
ability to identify an adequate tricuspid regurgitant jet, which
may be further enhanced by using saline contrast.
z Ventilation/perfusion (V/Q) lung scanning, pulmonary
angiography, and chest CT scanning may be indicated to diagnose
pulmonary thromboembolism as the underlying etiology of cor
pulmonale. These tests may be performed early in the
diagnostic workup if any evidence of pulmonary embolism appears
in history and physical examination. The test may also be
considered later in the workup if other tests are not suggestive
of any other etiology. Pulmonary thromboembolism has a wide
range of clinical presentations from massive embolism with acute
and severe hemodynamic instability to multiple chronic
peripheral embolisms that may present with cor pulmonale.
z Ultrafast, ECG-gated CT scanning has been evaluated to study
RV function. In addition to estimating right ventricular
ejection
fraction (RVEF), it can estimate RV wall mass. I ts use is still
experimental, but with further improvement, it may be used to
evaluate the progression of cor pulmonale in the near
future.
z Magnetic resonance imaging (MRI) of the heart is another
modality that can provide valuable information about RV mass,
septal flattening, and ventricular function. [9 ]
z Radionuclide ventriculography can determine RVEF
noninvasively. Myocardial perfusion may also show a permanent
increase
in brightness of the right ventricle.[10 ]
Other Tests
Electrocardiography (ECG) abnormalities in cor pulmonale reflect
the presence of RVH, RV strain, or underlying pulmonary
disease.
These electrocardiographic changes may include the
following:
z Right axis deviation
Seite 4 von 16Cor Pulmonale: [Print] - eMedicine Cardiology
04.10.2010http://emedicine.medscape.com/article/154062-print
-
7/27/2019 Cor Pulmonale Emedicine
5/16
-
7/27/2019 Cor Pulmonale Emedicine
6/16
Medical therapy[12 ]for chronic cor pulmonale is generally
focused on treatment of the underlying pulmonary disease and
improving
oxygenation and RV function by increasing RV contractility and
decreasing pulmonary vasoconstriction. However, the approach
might
be different to some degree in an acute setting with priority
given to stabilizing the patient.
Cardiopulmonary support for patients experiencing acute cor
pulmonale with resultant acute RV failure includes fluid loading
and
vasoconstrictor (eg, epinephrine) administration to maintain
adequate blood pressure. Of course, the primary problem should
be
corrected, if possible. For example, for massive pulmonary
embolism, consider administration of anticoagulation, thrombolytic
agents
or surgical embolectomy, especially if circulatory collapse is
impending; consider bronchodilation and infection treatment in
patients
with COPD; and consider steroid and immunosuppressive agents in
infiltrative and fibrotic lung diseases.
Oxygen therapy, diuretics, vasodilators, digitalis,
theophylline, and anticoagulation therapy are all different
modalities used in the long-
term management of chronic cor pulmonale.
Oxygen therapy
Oxygen therapy is of great importance in patients with
underlying COPD[13 ], particularly when administered on a
continuous basis.
With cor pulmonale, the partial pressure of oxygen (PO2) is
likely to be below 55 mm Hg and decreases further with exercise
and
during sleep.
Oxygen therapy relieves hypoxemic pulmonary vasoconstriction,
which then improves cardiac output, lessens sympathetic
vasoconstriction, alleviates tissue hypoxemia, and improves
renal perfusion. The Nocturnal Oxygen Therapy Trial (NOTT), a
multicenter randomized trial, showed that continuous low-flow
oxygen therapy for patients with severe COPD resulted in
significantreduction in the mortality rate.[14 ]In general, in
patients with COPD, long-term oxygen therapy is recommended when
PaO2 is less
than 55 mm Hg or O2 saturation is less than 88%. However, in the
presence of cor pulmonale or impaired mental or cognitive
function, long-term oxygen therapy can be considered even if
PaO2 is greater than 55 mm Hg or O2 saturation is greater than
88%.
Although whether oxygen therapy improves survival in patients
with cor pulmonale due to pulmonary disorders other than COPD
is
not clear, it may provide some degree of symptomatic relief and
improvement in functional status. Therefore, oxygen therapy plays
an
important role in both the immediate setting and long-term
management, especially in patients who are hypoxic and have
COPD.
Diuretics
Diuretics are used in the management of chronic cor pulmonale,
particularly when the right ventricular filling volume is
markedly
elevated and in the management of associated peripheral edema.
Diuretics may result in improvement of the function of both the
right
and left ventricles; however, diuretics may produce hemodynamic
adverse effects if they are not used cautiously. Excessive
volumedepletion can lead to a decline in cardiac output. Another
potential complication of diuresis is the production of a
hypokalemic
metabolic alkalosis, which diminishes the effectiveness of
carbon dioxide stimulation on the respiratory centers and
lessens
ventilatory drive. The adverse electrolyte and acid-base effect
of diuretic use can also lead to cardiac arrhythmia, which can
diminish
cardiac output. Therefore, diuresis, while recommended in the
management of chronic cor pulmonale, needs to be used with
great
caution.
Vasodilator drugs
Vasodilator drugs have been advocated in the long-term
management of chronic cor pulmonale with modest results. Calcium
channel
blockers, particularly oral sustained-release nifedipine[15 ]and
diltiazem, can lower pulmonary pressures, although they appear
more
effective in primary rather than secondary pulmonary
hypertension.[16 ]Other classes of vasodilators, such as beta
agonists, nitrates,
and angiotensin-converting enzyme (ACE) inhibitors have been
tried but, in general, vasodilators have failed to show
sustained
benefit in patients with COPD and they are not routinely used. A
trial of vasodilator therapy may be considered only in patients
withCOPD with disproportionately high pulmonary blood pressure.
Beta-selective agonists
Beta-selective agonists have an additional advantage of
bronchodilator and mucociliary clearance effect. Right heart
catheterization
has been recommended during initial administration of
vasodilators to objectively assess the efficacy and detect the
possible adverse
hemodynamic consequences of vasodilators.
The Food and Drug Administration (FDA) has approved
epoprostenol, treprostinil, bosentan, and iloprost for treatment of
primary
pulmonary hypertension. Epoprostenol, treprostinil, and iloprost
are prostacyclin (PGI2) analogues and have potent vasodilatory
properties.[17 ]Epoprostenol and treprostinil are administered
intravenously and iloprost is an inhaler. Bosentan is a mixed
endothelin-A
and endothelin-B receptor antagonist indicated for pulmonary
arterial hypertension (PAH), including primary pulmonary
hypertension
(PPH). In clinical trials, it improved exercise capacity,
decreased rate of clinical deterioration, and improved
hemodynamics.[17 ]
The PDE5 inhibitor sildenafil has been intensively
studied[18,19,20 ]and approved by the FDA for treatment of
pulmonary hypertension.
Sildenafil promotes selective smooth muscle relaxation in lung
vasculature.[21 ]Tadalafil, another PDE5 inhibitor, was also
recently
Seite 6 von 16Cor Pulmonale: [Print] - eMedicine Cardiology
04.10.2010http://emedicine.medscape.com/article/154062-print
-
7/27/2019 Cor Pulmonale Emedicine
7/16
approved by the FDA for the treatment of PAH to improve exercise
ability.[22 ]
Not enough data are available regarding the efficacy of these
drugs in patients with secondary pulmonary hypertension such as
in
patients with COPD.
Cardiac glycosides
The use of cardiac glycosides, such as digitalis, in patients
with cor pulmonale has been controversial, and the beneficial
effect of
these drugs is not as obvious as in the setting of left heart
failure. Nevertheless, studies have confirmed a modest effect of
digitalis on
the failing right ventricle in patients with chronic cor
pulmonale.[23 ]It must be used cautiously, however, and should not
be used during
the acute phases of respiratory insufficiency when large
fluctuations in levels of hypoxia and acidosis may occur. Patients
with
hypoxemia or acidosis are at increased risk of developing
arrhythmias due to digitalis through different mechanisms
including
sympathoadrenal stimulation.
Theophylline
In addition to bronchodilatory effect, theophylline has been
reported to reduce pulmonary vascular resistance and pulmonary
arterial
pressures acutely in patients with chronic cor pulmonale
secondary to COPD.[24 ]Theophylline has a weak inotropic effect and
thus
may improve right and left ventricular ejection. Low doses of
theophylline have also been suggested to have anti-inflammatory
effects
that help to control underlying lung diseases such as COPD.[25
]As a result, considering the use of theophylline as adjunctive
therapy
in the management of chronic or decompensated cor pulmonale is
reasonable in patients with underlying COPD.
Warfarin
Anticoagulation with warfarin is recommended in patients at high
risk for thromboembolism. The beneficial role of anticoagulation
in
improving the symptoms and mortality in patients with primary
pulmonary arterial hypertension has been demonstrated in
several
studies.[26,27,28,29 ]The evidence of benefit, however, has not
been established in patients with secondary pulmonary arterial
hypertension. Therefore, anticoagulation therapy may be used in
patients with cor pulmonale secondary to thromboembolic
phenomena and with underlying primary pulmonary arterial
hypertension.
Surgical Care
Phlebotomy is indicated in patients with chronic cor pulmonale
and chronic hypoxia causing severe polycythemia, defined as
hematocrit of 65 or more. Phlebotomy results in a decrease in
mean pulmonary artery pressure, a decrease in mean pulmonary
vascular resistance,[30 ]and an improvement in exercise
performance in such patients. However, no evidence suggests
improvement
in survival. Generally, phlebotomy should be reserved as an
adjunctive therapy for patients with acute decompensation of
cor
pulmonale and patients who remain significantly polycythemic
despite appropriate long-term oxygen therapy. Replacement of
the
acute volume loss with a saline infusion may be necessary to
avoid important decreases in systemic blood pressure.
No surgical treatment exists for most diseases that cause
chronic cor pulmonale. Pulmonary embolectomy is efficacious for
unresolved pulmonary emboli, which contribute to pulmonary
hypertension. Uvulopalatopharyngoplasty in selected patients with
sleep
apnea and hypoventilation[31 ]may relieve cor pulmonale.
Single-lung, double-lung, and heart-lung transplantation are all
used to
salvage the terminal phases of several diseases (eg, primary
pulmonary hypertension, emphysema, idiopathic pulmonary
fibrosis,
cystic fibrosis) complicated by cor pulmonale. Lung
transplantation may lead to a reversal of right ventricular
dysfunction from the
chronic stress of pulmonary hypertension. However, strict
selection criteria for lung transplant recipients must be met
because of the
limited availability of organ donors.
Medication
Diuretics are used to decrease the elevated right ventricular
filling volume in patients with chronic cor pulmonale. Calcium
channel
blockers are pulmonary artery vasodilators that have proven
efficacy in the long-term management of chronic cor pulmonale
secondary to primary pulmonary arterial hypertension. New
FDA-approved prostacyclin analogues and endothelin-receptor
antagonists are available for treatment of PPH. The beneficial
role of cardiac glycosides, namely digitalis, on the failing right
ventricle
are somewhat controversial; they can improve right ventricular
function but must be used with caution and should be avoided
during
acute episodes of hypoxia.
In the management of cor pulmonale, the main indication for oral
anticoagulants is in the setting of an underlying
thromboembolic
event or primary pulmonary arterial hypertension.
Methylxanthines, like theophylline, can be used as an adjunctive
treatment for
chronic cor pulmonale secondary to COPD. Besides the moderate
bronchodilatory effect of methylxanthine, it improves
myocardial
contractility, causes a mild pulmonary vasodilatory effect, and
enhances diaphragmatic contractility.
Diuretics
Are used to decrease the elevated right ventricular filling
volume in patients with chronic cor pulmonale.
Seite 7 von 16Cor Pulmonale: [Print] - eMedicine Cardiology
04.10.2010http://emedicine.medscape.com/article/154062-print
-
7/27/2019 Cor Pulmonale Emedicine
8/16
Furosemide (Lasix)
Example of diuretic agents used in the management of chronic cor
pulmonale. Furosemide is a powerful loop diuretic that works on
thick ascending limb of Henle loop, causing a reversible block
in reabsorption of sodium, potassium, and chloride.
Dosing
Adult
20-80 mg/d PO/IV/IM; may titrate to maximum dose of 600 mg/d
Pediatric
1-2 mg/kg/dose PO; not to exceed 6 mg/kg/dose; do not administer
more frequent than q6h
1 mg/kg IV/IM slowly under close supervision; not to exceed 6
mg/kg
Interactions
Metformin decreases furosemide concentrations; furosemide
interferes with hypoglycemic effect of antidiabetic agents and
antagonizes muscle-relaxing effect of tubocurarine; auditory
toxicity appears to be increased with coadministration of
aminoglycosides
and furosemide; hearing loss of varying degrees may occur;
anticoagulant activity of warfarin may be enhanced when taken
concurrently with this medication; increased plasma lithium
levels and toxicity are possible when taken concurrently with
this
medication
Contraindications
Documented hypersensitivity; hepatic coma; anuria; concurrent
severe electrolyte depletion
Precautions
Pregnancy
C - Fetal risk revealed in studies in animals but not
established or not studied in humans; may use if benefits outweigh
risk to fetus
Precautions
Perform frequent serum electrolyte, carbon dioxide, glucose,
creatinine, uric acid, calcium, and BUN determinations during first
few
months of therapy and periodically thereafter
Calcium channel blockers
These agents inhibit movement of calcium ions across the cell
membrane, depressing both impulse formation (automaticity) and
conduction velocity.
Nifedipine (Procardia)
Especially in the sustained-release form, nifedipine is a
calcium channel blocker that has proven to be fairly effective in
the
management of chronic cor pulmonale caused by primary pulmonary
hypertension. Modifies the entry of calcium into the cells by
blocking the slow or voltage-dependent calcium channels,
resulting in vasodilation, which improves myocardial oxygen
delivery.
Sublingual administration generally is safe, despite theoretical
concerns.
Dosing
Adult
10-30 mg SR cap PO tid; not to exceed 120-180 mg/d
30-60 mg SR tab PO qd; not to exceed 90-120 mg/d
Pediatric
Not recommended
Interactions
Monitor oral anticoagulants when used concomitantly;
coadministration with any agent that can lower BP, including
beta-blockers and
opioids, can result in severe hypotension; H2 blockers
(cimetidine) may increase toxicity
Contraindications
Documented hypersensitivity
Precautions
Seite 8 von 16Cor Pulmonale: [Print] - eMedicine Cardiology
04.10.2010http://emedicine.medscape.com/article/154062-print
-
7/27/2019 Cor Pulmonale Emedicine
9/16
Pregnancy
C - Fetal risk revealed in studies in animals but not
established or not studied in humans; may use if benefits outweigh
risk to fetus
Precautions
Aortic stenosis; angina; congestive heart failure; pregnancy;
nursing mothers; may cause lower extremity edema; allergic
hepatitis
has occurred but is rare
Cardiac glycosidesThese agents decrease AV nodal conduction
primarily by increasing vagal tone.
Digoxin (Lanoxin)
Has a positive inotropic effect on failing myocardium. Effect is
achieved via inhibition of the Na+/K+-ATPase pump, leading to
increase in intracellular sodium concentration along with
concomitant increase in intracellular calcium concentration by
means of
calcium-sodium exchange mechanism. Net result is augmentation of
myocardial contractility.
Dosing
Adult
0.125-0.375 mg PO qd; may be administered qod; available in
PO/IV/IM preparations
Pediatric
8-10 mcg/kg/d PO/IV/IM; maximum dose 100-150 mcg/kg/d
Interactions
Medications that may increase digoxin levels include alprazolam,
benzodiazepines, bepridil, captopril, cyclosporine,
propafenone,
propantheline, quinidine, diltiazem, aminoglycosides, oral
amiodarone, anticholinergics, diphenoxylate, erythromycin,
felodipine,
flecainide, hydroxychloroquine, itraconazole, nifedipine,
omeprazole, quinine, ibuprofen, indomethacin, esmolol,
tetracycline,
tolbutamide, and verapamil; medications that may decrease serum
digoxin levels include aminoglutethimide, antihistamines,
cholestyramine, neomycin, penicillamine, aminoglycosides, oral
colestipol, hydantoins, hypoglycemic agents, antineoplastic
treatment
combinations (eg, carmustine, bleomycin, methotrexate,
cytarabine, doxorubicin, cyclophosphamide, vincristine,
procarbazine),
aluminum or magnesium antacids, rifampin, sucralfate,
sulfasalazine, barbiturates, kaolin/pectin, and aminosalicylic
acid
Contraindications
Documented hypersensitivity; beriberi heart disease; idiopathic
hypertrophic subaortic stenosis; constrictive pericarditis; carotid
sinus
syndrome
Precautions
Pregnancy
C - Fetal risk revealed in studies in animals but not
established or not studied in humans; may use if benefits outweigh
risk to fetus
Precautions
Hypokalemia may reduce positive inotropic effect of digitalis;
IV calcium may produce arrhythmias in digitalized patients;
hypercalcemia predisposes patient to digitalis toxicity;
hypocalcemia can make digoxin ineffective until serum calcium
levels are
normal; magnesium replacement therapy must be instituted in
patients with hypomagnesemia to prevent digitalis toxicity;
patients
diagnosed with incomplete AV block may progress to complete
block when treated with digoxin; exercise caution in
hypothyroidism,
hypoxia, and acute myocarditis
Anticoagulants
These agents may reduce incidence of embolisms when used fast,
effectively, and early.
Warfarin (Coumadin)
Most commonly used oral anticoagulant. Interferes with hepatic
synthesis of vitamin K-dependent coagulation factors. Used for
prophylaxis and treatment of venous thrombosis, pulmonary
embolism, and thromboembolic disorders.
Dosing
Adult
2-10 mg/d PO qd; adjust dose to an INR of 1.5:2 or higher
depending on the condition requiring anticoagulation
Seite 9 von 16Cor Pulmonale: [Print] - eMedicine Cardiology
04.10.2010http://emedicine.medscape.com/article/154062-print
-
7/27/2019 Cor Pulmonale Emedicine
10/16
Pediatric
Administer weight-based dose of 0.05-0.34 mg/kg/d PO/IV; adjust
dose according to desired INR
Interactions
Griseofulvin, carbamazepine, glutethimide, estrogens, nafcillin,
phenytoin, rifampin, barbiturates, cholestyramine, colestipol,
vitamin
K, spironolactone, oral contraceptives, and sucralfate may
decrease anticoagulant effects; oral antibiotics,
phenylbutazone,
salicylates, sulfonamides, chloral hydrate, clofibrate,
diazoxide, anabolic steroids, ketoconazole, ethacrynic acid,
miconazole, nalidixic
acid, sulfonylureas, allopurinol, chloramphenicol, cimetidine,
disulfiram, metronidazole, phenylbutazone, phenytoin,
propoxyphene,sulfonamides, gemfibrozil, acetaminophen, and sulindac
may increase anticoagulant effects
Contraindications
Documented hypersensitivity; severe liver or kidney disease;
open wounds; GI ulcers
Precautions
Pregnancy
D - Fetal risk shown in humans; use only if benefits outweigh
risk to fetus
Precautions
Dose needs to be adjusted to INR; caution in bleeding tendency
and hazardous active hemorrhagic conditions, malignant
hypertension, patients at high risk of recurrent trauma, (eg,
people with alcoholism or psychosis, unsupervised patients who
are
senile); warfarin anaphylaxis, hepatic, renal, thyroid,
allergic, and hematologic hypocoagulable conditions and disorders;
do not switch
brands after achieving therapeutic response; caution in active
tuberculosis or diabetes; patients with protein C or S deficiency
are at
risk of developing skin necrosis
Methylxanthines
Potentiate exogenous catecholamines and stimulate endogenous
catecholamine release and diaphragmatic muscular relaxation,
which, in turn, stimulates bronchodilation.
Theophylline (Aminophyllin, Theo-24, Theolair, Theo-Dur)
Mechanism of action is not well defined yet. Was formerly
thought that this drug increases intracellular cyclic AMP by
causing
inhibition of phosphodiesterase; however, current data do not
support that.
Dosing
Adult
Loading dose: 5.6 mg/kg IV over 20 min (based on
aminophylline)
Maintenance dose: IV infusion at 0.5-0.7 mg/kg/h; also available
in oral preparation
Pediatric
1 year: Administer as in adults
Interactions
Effects may decrease with aminoglutethimide, barbiturates,
carbamazepine, ketoconazole, loop diuretics, charcoal,
hydantoins,
phenobarbital, phenytoin, rifampin, isoniazid, and
sympathomimetics; effects may increase with allopurinol,
beta-blockers,
ciprofloxacin, corticosteroids, disulfiram, quinolones, thyroid
hormones, ephedrine, carbamazepine, cimetidine, erythromycin,
macrolides, propranolol, and interferon
Contraindications
Documented hypersensitivity; uncontrolled arrhythmias; peptic
ulcers; hyperthyroidism; uncontrolled seizure disorders
Precautions
Pregnancy
C - Fetal risk revealed in studies in animals but not
established or not studied in humans; may use if benefits outweigh
risk to fetus
Seite 10 von 16Cor Pulmonale: [Print] - eMedicine Cardiology
04.10.2010http://emedicine.medscape.com/article/154062-print
-
7/27/2019 Cor Pulmonale Emedicine
11/16
Precautions
Has low serum therapeutic-to-toxicity ratio, and, therefore,
serum level monitoring is important; peptic ulcer;
hypertension;
tachyarrhythmias; hyperthyroidism; compromised cardiac function;
do not inject IV solution faster than 25 mg/min; patients
diagnosed
with pulmonary edema or liver dysfunction are at greater risk of
toxicity because of reduced drug clearance
Endothelin receptor antagonists
Competitively bind to endothelin-1 (ET-1) receptors ETA and ETB
causing reduction in pulmonary artery pressure (PAP), pulmonary
vascular resistance (PVR), and mean right atrial pressure
(RAP).
Bosentan (Tracleer)
Endothelin receptor antagonist indicated for the treatment of
pulmonary arterial hypertension in patients with WHO Class
II-IV
symptoms, to improve exercise ability and decrease rate of
clinical worsening. Inhibits vessel constriction and elevation of
blood
pressure by competitively binding to endothelin-1 (ET-1)
receptors ETA and ETB in endothelium and vascular smooth muscle.
This
leads to significant increase in cardiac index (CI) associated
with significant reduction in pulmonary artery pressure (PAP), mean
right
atrial pressure (RAP), pulmonary vascular resistance (PVR), and,
to a lesser extent, systemic vascular resistance (SVR). Due to
teratogenic potential, can only be prescribed through the
Tracleer Access Program (1-866-228-3546).
Dosing
Adult
40 kg: 62.5 mg PO bid for 4 wk initially, then increase to 125
mg PO bid
Pediatric
Not established; 62.5 mg PO bid recommended if 12 years; not to
exceed 125 mg/d
Interactions
Toxicity may increase when administered concomitantly with
inhibitors of isoenzymes CYP450 2C9 and CYP450 3A4 (eg,
ketoconazole, erythromycin, fluoxetine, sertraline, amiodarone,
and cyclosporine A); induces isoenzymes CYP450 2C9 and CYP450
3A4 causing decrease in plasma concentrations of drugs
metabolized by these enzymes including glyburide as well as
other
hypoglycemics, cyclosporine A, hormonal contraceptives,
simvastatin, and possibly other statins; hepatotoxicity increases
with
concomitant administration of glyburide
Contraindications
Documented hypersensitivity; coadministration with cyclosporine
A or glyburide
Precautions
Pregnancy
X - Contraindicated; benefit does not outweigh risk
Precautions
Causes at least 3-fold elevation of liver aminotransferases (ie,
ALT, AST) in about 11% of patients; may elevate bilirubin
(serum
aminotransferase levels must be measured prior to initiation of
treatment and then monthly); caution in patients with mildly
impaired
liver function (avoid in patients with moderate or severe liver
impairment); not recommended while breastfeeding; monitor
hemoglobin
levels after 1 and 3 mo of treatment and every 3 mo thereafter;
exclude pregnancy before initiating treatment and prevent
thereafter
by use of reliable contraception; headache and nasopharyngitis
may occur
Ambrisentan (Letairis)
Endothelin receptor antagonist indicated for pulmonary arterial
hypertension in patients with WHO class II or III symptoms.
Improves
exercise ability and decreases progression of clinical symptoms.
Inhibits vessel constriction and elevation of blood pressure by
competitively binding to endothelin-1 receptors ETA and ETB in
endothelium and vascular smooth muscle. This leads to
significant
increase in cardiac index associated with significant reduction
in pulmonary artery pressure, mean right atrial pressure,
pulmonary
vascular resistance, and, to a lesser extent, systemic vascular
resistance (SVR). Because of the risks of hepatic injury and
teratogenic potential, only available through the Letairis
Education and Access Program (LEAP). Prescribers and pharmacies
must
register with LEAP in order to prescribe and dispense. For more
information, see http://www.letairis.com or call (866)
664-LEAP(5327).
Dosing
Seite 11 von 16Cor Pulmonale: [Print] - eMedicine Cardiology
04.10.2010http://emedicine.medscape.com/article/154062-print
-
7/27/2019 Cor Pulmonale Emedicine
12/16
Adult
5 mg PO qd initially; may increase to 10 mg PO qd if 5 mg/d
tolerated; do not chew, crush, or split tab
Pediatric
Not established
Interactions
Glycoprotein-P, OATP, UGTs (ie, 1A9S, 2B7S, 1A3S), CYP2C19, and
CYP3A substrate; coadministration with CYP3A (eg,cyclosporine,
atazanavir, clarithromycin, indinavir, itraconazole, ketoconazole,
nefazodone, nelfinavir, ritonavir, saquinavir,
telithromycin) or 2C19 inhibitors (eg, omeprazole) may decrease
elimination and therefore increase serum levels; CYP3A and 2C19
inducers (eg, rifampin) may increase metabolism and therefore
decrease serum levels
Contraindications
Pregnancy
Precautions
Pregnancy
X - Contraindicated; benefit does not outweigh risk
Precautions
Common adverse effects include peripheral edema, nasal
congestion, sinusitis, and facial flushing; caution with mild
hepatic
impairment or history of moderate-to-severe hepatic impairment;
hepatic injury may occur (monitor bilirubin, ALT, and AST values
at
baseline and then monthly); may use in women of childbearing
potential only after negative pregnancy test result and must use
2
reliable methods of contraception (unless tubal sterilization or
Copper T 380A or LNg 20 IUD inserted); may decrease hemoglobin
and hematocrit values (monitor at baseline, 1 mo, and then
periodically)
Follow-up
Further Inpatient Care
Appropriate treatment is directed both at the underlying
etiology and at correction of hypoxia when present.
Further Outpatient Care
z Patients with cor pulmonale generally require close attention
in the outpatient setting.
z Regular assessment of oxygen needs and pulmonary function are
appropriate.
z Many patients benefit from a formal program of pulmonary
rehabilitation.
Complications
Complications of cor pulmonale include syncope, hypoxia, pedal
edema, passive hepatic congestion, and death.
Prognosis
z The prognosis of cor pulmonale is variable depending upon
underlying pathology.
z Patients with cor pulmonale due to COPD have a high 2-year
mortality.
Patient Education
Patient education regarding the importance of adherence to
medical therapy is vital because appropriate treatment of both
hypoxia
and underlying medical illness can improve mortality and
morbidity.
Miscellaneous
Medicolegal Pitfalls
z Making a diagnosis of cor pulmonale should be followed by
further investigation to determine the underlying lung
pathology.
Sometimes a common lung disease such as COPD is not the only
lung pathology as the cause of cor pulmonale; other lung
diseases may coexist.
Seite 12 von 16Cor Pulmonale: [Print] - eMedicine Cardiology
04.10.2010http://emedicine.medscape.com/article/154062-print
-
7/27/2019 Cor Pulmonale Emedicine
13/16
z When diagnosing cor pulmonale, considering the possibility of
thromboembolic disease and primary pulmonary hypertension
as possible etiologies is important.
z Note the importance of continuous supplemental oxygen therapy
in appropriate patients, as well as the dangers of cigarette
smoking while using supplemental oxygen. Elevation of
carboxyhemoglobin in the blood due to smoking can significantly
decrease the effect of O2 on arterial O2 content.
Multimedia
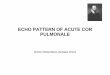
Media file 1: This ECG shows some typical abnormalities that may
be seen in cor pulmonale and other chronic
pulmonary diseases: (1) R/S ratio >1 in V1 and
-
7/27/2019 Cor Pulmonale Emedicine
14/16
(2):294-6. [Medline].
11. Urboniene D, Haber I, Fang YH, Thenappan T, Archer SL.
Validation of High-Resolution Echocardiography and Magnetic
Resonance Imaging Versus High-Fidelity Catheterization in
Experimental Pulmonary Hypertension.Am J Physiol Lung Cell
Mol Physiol. Jun 25 2010;[Medline].
12. Hoeper MM. Drug treatment of pulmonary arterial
hypertension: current and future agents. Drugs.
2005;65(10):1337-
54. [Medline].
13. Hanania NA, Ambrosino N, Calverley P, Cazzola M, Donner CF,
Make B. Treatments for COPD. Respir Med. Dec 2005;99
Suppl B:S28-40. [Medline].
14. Nocturnal Oxygen Therapy Trial Group. Continuous or
nocturnal oxygen therapy in hypoxemic chronic obstructive lung
disease: a clinical trial. Nocturnal Oxygen Therapy Trial
Group.Ann Intern Med. Sep 1980;93(3):391-8. [Medline].
15. Singh H, Ebejer MJ, Higgins DA, Henderson AH, Campbell IA.
Acute haemodynamic effects of nifedipine at rest and during
maximal exercise in patients with chronic cor pulmonale. Thorax.
Dec 1985;40(12):910-4. [Medline]. [Full Text].
16. Rich S, Kaufmann E. High dose titration of calcium channel
blocking agents for primary pulmonary hypertension: guidelines
for
short-term drug testing. J Am Coll Cardiol. Nov 1
1991;18(5):1323-7. [Medline].
17. Anderson JR, Nawarskas JJ. Pharmacotherapeutic management of
pulmonary arterial hypertension. Cardiol Rev. May-
Jun 2010;18(3):148-62. [Medline].
18. Sastry BK, Narasimhan C, Reddy NK, Raju BS. Clinical
efficacy of sildenafil in primary pulmonary hypertension: a
randomized,
placebo-controlled, double-blind, crossover study. J Am Coll
Cardiol. Apr 7 2004;43(7):1149-53. [Medline].
19. Singh TP, Rohit M, Grover A, Malhotra S, Vijayvergiya R. A
randomized, placebo-controlled, double-blind, crossover study
to
evaluate the efficacy of oral sildenafil therapy in severe
pulmonary artery hypertension.Am Heart J. Apr
2006;151(4):851.e1-
5. [Medline].
20. Gali N, Ghofrani HA, Torbicki A, et al. Sildenafil citrate
therapy for pulmonary arterial hypertension. N Engl J Med. Nov
17 2005;353(20):2148-57. [Medline].
21. Gomberg-Maitland M, McLaughlin V, Gulati M, Rich S. Efficacy
and safety of sildenafil added to treprostinil in pulmonary
hypertension.Am J Cardiol. Nov 1 2005;96(9):1334-6.
[Medline].
22. Adcirca prescribing information. Indianapolis, IN. Eli Lilly
and Company; 2009.
23. Polic S, Rumboldt Z, Dujic Z, Bagatin J, Deletis O, Rozga A.
Role of digoxin in right ventricular failure due to chronic cor
pulmonale. Int J Clin Pharmacol Res. 1990;10(3):153-62.
[Medline].
24. Matthay RA, Mahler DA. Theophylline improves global cardiac
function and reduces dyspnea in chronic obstructive lung
disease. J Allergy Clin Immunol. Oct 1986;78(4 Pt 2):793-9.
[Medline].
25. Barnes PJ. Theophylline in chronic obstructive pulmonary
disease: new horizons. Proc Am Thorac Soc. 2005;2(4):334-9;
discussion 340-1. [Medline].
26. Fuster V, Steele PM, Edwards WD, Gersh BJ, McGoon MD, Frye
RL. Primary pulmonary hypertension: natural history and the
importance of thrombosis. Circulation. Oct 1984;70(4):580-7.
[Medline].
27. Sitbon O, Humbert M, Jais X, et al. Long-term response to
calcium channel blockers in idiopathic pulmonary arterial
hypertension. Circulation. Jun 14 2005;111(23):3105-11.
[Medline].
28. Badesch DB, Abman SH, Ahearn GS, et al. Medical therapy for
pulmonary arterial hypertension: ACCP evidence-based
clinical practice guidelines. Chest. Jul 2004;126(1
Suppl):35S-62S. [Medline].
29. Johnson SR, Mehta S, Granton JT. Anticoagulation in
pulmonary arterial hypertension: a qualitative systematic review.
Eur
Respir J. Nov 2006;28(5):999-1004. [Medline].
30. Jardin F, Vieillard-Baron A. Acute cor pulmonale. Curr Opin
Crit Care. Feb 2009;15(1):67-70. [Medline].
31. Fine-Goulden MR, Manna S, Durward A. Cor pulmonale due to
congenital central hypoventilation syndrome presenting
inadolescence. Pediatr Crit Care Med. Jul 2009;10(4):e41-2.
[Medline].
32. Jardin F, Vieillard-Baron A. Monitoring of right-sided heart
function. Curr Opin Crit Care. Jun 2005;11(3):271-9. [Medline].
Seite 14 von 16Cor Pulmonale: [Print] - eMedicine Cardiology
04.10.2010http://emedicine.medscape.com/article/154062-print
-
7/27/2019 Cor Pulmonale Emedicine
15/16
33. Kingman MS, Thompson BS, Newkirk T, Torres F. Nesiritide for
pulmonary arterial hypertension with decompensated cor
pulmonale. Prog Cardiovasc Nurs. Fall 2005;20(4):168-72.
[Medline].
34. Klinger JR, Hill NS. Right ventricular dysfunction in
chronic obstructive pulmonary disease. Evaluation and
management. Chest. Mar 1991;99(3):715-23. [Medline].
35. Lee-Chiong Jr TL, Matthay RA. Pulmonary hypertension and cor
pulmonale in COPD. Semin Respir Crit Care
Med. Jun 2003;24(3):263-72. [Medline].
36. MacNee W. Pathophysiology of cor pulmonale in chronic
obstructive pulmonary disease. Part One.Am J Respir Crit Care
Med. Sep 1994;150(3):833-52. [Medline].
37. MacNee W. Pathophysiology of cor pulmonale in chronic
obstructive pulmonary disease. Part two.Am J Respir Crit Care
Med. Oct 1994;150(4):1158-68. [Medline].
38. Mahler DA, Matthay RA, Snyder PE, Wells CK, Loke J.
Sustained-release theophylline reduces dyspnea in nonreversible
obstructive airway disease.Am Rev Respir Dis. Jan
1985;131(1):22-5. [Medline].
39. Ringbaek TJ, Fabricius P, Lange P. The effect of home oxygen
therapy on hospitalization in moderate hypoxaemic
COPD. Chron Respir Dis. 2005;2(2):107-8. [Medline].
40. Wiedemann HP, Matthay RA. The management of acute and
chronic cor pulmonale. In: Scharf SM, Cassidy SS, eds. Heart-Lung
Interactions in Health and Disease. New York, NY: Marcel Dekker;
1989:915.
Keywords
cor pulmonale, pulmonary hypertension, cardiopulmonary disease,
COPD, chronic obstructive pulmonary disease, ARDS, acute
respiratory distress syndrome, right heart failure, right
ventricular failure, right ventricular hypertrophy, RVH,
pulmonary
thromboembolism, interstitial lung disease, polycythemia vera,
macroglobulinemia, pulmonary embolism, pulmonary emboli,
diastolic
pulmonary regurgitation murmur
Contributor Information and Disclosures
Author
Al i A Sovari , MD, Clinical and Research Fellow in
Cardiovascular Medicine, Section of Cardiology, University of
Illinois at ChicagoAli A Sovari, MD is a member of the following
medical societies: American College of Cardiology, American College
of Physicians,
American Heart Association, American Medical Association, and
Heart Rhythm Society
Disclosure: Nothing to disclose.
Coauthor(s)
Ravi H Dave, MD, Associate Professor of Medicine, University of
California at Los Angeles David Geffen School of Medicine
Disclosure: Nothing to disclose.
Abr aham G Kocheril , MD, FACC, FACP, FHRS, Professor of
Medicine, Director of Clinical Electrophysiology, University of
Illinois at
Chicago
Abraham G Kocheril, MD, FACC, FACP, FHRS is a member of the
following medical societies: American College of Cardiology,
American College of Physicians, American Heart Association,
American Medical Association, Cardiac Electrophysiology
Society,
Central Society for Clinical Research, Heart Failure Society of
America, and Illinois State Medical Society
Disclosure: Nothing to disclose.
Medical Editor
Gregory J Dehmer, MD, Director, Division of Cardiology, Scott
& White Healthcare; Professor of Medicine, Texas A&M
Health
Science Center College of Medicine
Gregory J Dehmer, MD is a member of the following medical
societies: American College of Cardiology, American Heart
Association,
Society for Cardiac Angiography and Interventions, and Society
of Cardiac Angiography and Interventions
Disclosure: Nothing to disclose.
Pharmacy Editor
Francisco Talavera, PharmD, PhD, Senior Pharmacy Editor,
eMedicine
Disclosure: eMedicine Salary Employment
Managing Editor
Seite 15 von 16Cor Pulmonale: [Print] - eMedicine Cardiology
04.10.2010http://emedicine.medscape.com/article/154062-print
-
7/27/2019 Cor Pulmonale Emedicine
16/16
Steven J Compton, MD, FACC, FACP, Director of Cardiac
Electrophysiology, Alaska Heart Institute, Providence and
Alaska
Regional Hospitals
Steven J Compton, MD, FACC, FACP is a member of the following
medical societies: Alaska State Medical Association, American
College of Cardiology, American College of Physicians, American
Heart Association, American Medical Association, and Heart
Rhythm Society
Disclosure: Nothing to disclose.
CME Editor
Amer Sul eman, MD, Consultant in Electrophysiology and
Cardiovascular Medicine, Department of Internal Medicine, Division
of
Cardiology, Medical City Dallas Hospital
Amer Suleman, MD is a member of the following medical societies:
American College of Physicians, American Heart Association,
American Institute of Stress, American Society of Hypertension,
Federation of American Societies for Experimental Biology,
Royal
Society of Medicine, and Society of Cardiac Angiography and
Interventions
Disclosure: Nothing to disclose.
Chief Editor
Henry H Ooi, MBBCh, BAO, MRCPI, Director, Advanced Heart Failure
and Cardiac Transplant Program, Nashville Veterans Affairs
Medical Center; Cardiologist, Heart Failure and Cardiac
Transplant Program, Vanderbilt University Medical Center
Henry H Ooi, MBBCh, BAO, MRCPI is a member of the following
medical societies: American College of Cardiology, American
Heart
Association, Heart Failure Society of America, and International
Society for Heart and Lung Transplantation
Disclosure: Nothing to disclose.
Ack now ledgments
The authors and editors of eMedicine gratefully acknowledge the
contributions of previous authors Robert S Crausman, MD, MMS and
Nidal A Yunis, MD tothe development and writing of this
article.
Further Reading
Clinical trials
Educational and Supportive Interventions to Prevent
Cardiopulmonary Rehospitalization
Identification of Genetic Markers for Cardiopulmonary Diseases
(Genotype)
1994- 2010 by Medscape.All Rights
Reserved(http://www.medscape.com/public/copyright)
Seite 16 von 16Cor Pulmonale: [Print] - eMedicine Cardiology