Embed Size (px)
Citation preview

case records of the massachusetts general hospital
T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 357;21 www.nejm.org november 22, 2007 2167
Founded by Richard C. Cabot Nancy Lee Harris, m.d., Editor Eric S. Rosenberg, m.d., Associate EditorJo-Anne O. Shepard, m.d., Associate Editor Alice M. Cort, m.d., Associate EditorSally H. Ebeling, Assistant Editor Christine C. Peters, Assistant Editor
From the Cardiovascular Division, Brig-ham and Women’s Hospital (M.S.S.); the Cardiology Division (M.S.S., K.-K.P., J.L.M.) and the Departments of Radiology ( J.-A.O.S.) and Pathology ( J.R.S., M.P.F.), Massachusetts General Hospital; and the Departments of Medicine (M.S.S., K.-K.P., J.L.M.), Radiology (J.-A.O.S.), and Pathol-ogy ( J.R.S., M.P.F.), Harvard Medical School — all in Boston.
N Engl J Med 2007;357:2167-78.Copyright © 2007 Massachusetts Medical Society.
Pr esen tation of C a se
Dr. Jeffrey O. Greenberg (Medicine): A 31-year-old woman was admitted to this hospital because of facial swelling, fever, and hypotension.
The patient had relapsing and remitting multiple sclerosis, associated with severe fatigue. Three weeks before admission, her neurologist prescribed modafinil to treat the fatigue. One week later, periorbital erythema, a clear conjunctival discharge, and a raised erythematous and pruritic rash developed on her face and scalp. She discontinued modafinil and used over-the-counter diphenhydramine, but the rash did not improve. Three days later, she went to the emergency room of a hospital near her home for evaluation. Cyproheptadine was prescribed, but the pharmacy dispensed perphenazine in error. Two days later, she was reevaluated at the same facility; the medication error was noted, and prednisone (60 mg) and cyprohepta-dine were begun. The facial rash improved transiently, but 5 days before admission, it recurred, and similar lesions developed on her back and chest.
On examination by a physician at this hospital the next day, there was swelling around the eyes, nose, and left ear, and an urticarial rash on the torso. Cyprohepta-dine was stopped, and diphenhydramine and ranitidine were added. During the next 2 days, painful swelling under the left mandible and pain in the hips developed, and facial swelling and erythema near the left eye increased. She returned to the hospital near her home and was given doxycycline for possible cellulitis of the face. The day before admission, increased facial swelling with discomfort in the left ear, blurred vision, pelvic pain, and dysuria had developed and she returned to the emer-gency department of that hospital.
She appeared anxious. The temperature was 37.5°C, the blood pressure 131/74 mm Hg, the pulse 148 beats per minute, and the oxygen saturation 96% while she was breathing ambient air. There was a maculopapular facial rash and swelling of the face, left parotid gland, and left external auditory canal, with bilateral cervical lymphadenopathy. Levels of serum glucose and electrolytes and tests of liver and renal function were normal; results of other laboratory tests are shown in Table 1. Ninety minutes after arrival, meperidine and promethazine were administered, followed by diphenhydramine and famotidine. Shortly thereafter, she reported light-headedness; the blood pressure was transiently 70/40 mm Hg, and the tempera-
Case 36-2007: A 31-Year-Old Woman with Rash, Fever, and Hypotension
Marc S. Sabatine, M.D., M.P.H., Kian-Keong Poh, M.D., Jessica L. Mega, M.D., Jo-Anne O. Shepard, M.D., James R. Stone, M.D., Ph.D., and Matthew P. Frosch, M.D.
Downloaded from www.nejm.org on November 28, 2007 . Copyright © 2007 Massachusetts Medical Society. All rights reserved.

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 357;21 www.nejm.org november 22, 20072168
Tabl
e 1.
Res
ults
of L
abor
ator
y Te
sts.
Var
iabl
eR
efer
ence
Ran
ge, A
dults
*O
ther
Hos
pita
lTh
is H
ospi
tal
At
Pres
enta
tion
Day
of T
rans
fer,
15
Hr
afte
r Pr
esen
tatio
n1.
5 H
r af
ter
A
rriv
al
16–2
2 H
r af
ter
Arr
ival
35 H
r af
ter
A
rriv
al61
Hr
afte
r
Arr
ival
Hem
atoc
rit (
%)
36.0
–46.
0 46
.442
.044
.739
.139
.931
.0
Hem
oglo
bin
(who
le b
lood
) (g
/dl)
12.0
–16.
0 16
.014
.615
.513
.413
.611
.5
Whi
te-c
ell c
ount
(pe
r m
m3 )
4,50
0–11
,000
9,40
09,
200
11,0
009,
500
12,7
0011
,900
Diff
eren
tial c
ount
(%
)
Neu
trop
hils
40–7
071
.168
.175
7976
Ban
d fo
rms
4
Lym
phoc
ytes
22–4
414
.615
.614
1215
Eosi
noph
ils0–
87.
17.
07
60
Mon
ocyt
es4–
116.
98.
84
33
Bas
ophi
ls0.
30.
5
Aty
pica
l lym
phoc
ytes
2
Plat
elet
cou
nt (
per
mm
3 )15
0,00
0–35
0,00
027
2,00
030
0,00
024
4,00
022
7,00
023
1,00
0
Cre
atin
e ki
nase
(U
/lite
r)40
–150
2,87
23,
098
2,57
4
Cre
atin
e ki
nase
MB
isoe
nzym
e (n
g/m
l)0–
6.9
31.8
38.8
52.2
Trop
onin
T (
ng/m
l)0–
0.09
1.04
1.48
3.95
NT-
pro-
BN
P (p
g/m
l)†
0–45
07,
988
* R
efer
ence
val
ues
are
affe
cted
by
man
y va
riab
les,
incl
udin
g th
e pa
tient
pop
ulat
ion
and
the
labo
rato
ry m
etho
ds u
sed.
The
ran
ges
used
at
Mas
sach
uset
ts G
ener
al H
ospi
tal a
re fo
r ad
ults
w
ho a
re n
ot p
regn
ant
and
do n
ot h
ave
med
ical
con
ditio
ns t
hat
coul
d af
fect
the
res
ults
. The
refo
re, t
hese
ran
ges
may
not
be
appr
opri
ate
for
all p
atie
nts.
† N
T-pr
o-B
NP
deno
tes
N-t
erm
inal
frag
men
t of
pro
–bra
in (
B-t
ype)
nat
riur
etic
pep
tide.
Downloaded from www.nejm.org on November 28, 2007 . Copyright © 2007 Massachusetts Medical Society. All rights reserved.

case records of the massachusetts gener al hospital
n engl j med 357;21 www.nejm.org november 22, 2007 2169
ture 38.5°C. Electrocardiography showed bor-derline sinus tachycardia and mild right-axis deviation. Clindamycin, prednisone, and addi-tional diphenhydramine were administered, fol-lowed by acetaminophen and hydrocodone. Ap-proximately 18 hours after arrival, she was transferred to the emergency department of this hospital for otolaryngologic evaluation of the fa-cial and neck swelling.
Multiple sclerosis had been diagnosed 4 years earlier during an episode of optic neuritis; a hyper-intense lesion consistent with a plaque was seen on magnetic resonance imaging (MRI). Her symp-toms included blurred vision, tingling and weak-ness in the left leg and arm, and extreme fatigue. Methylprednisolone infusions were given intermit-tently for exacerbations. Other medications in the past had included copaxone, amantadine, and daclizumab.
She had bipolar disorder, which was being treat-ed with sertraline and oxcarbazepine. Electrocar-diograms (ECGs) and echocardiograms were nor-mal 2 years before admission. She was allergic to amoxicillin and doxycycline, which had caused gastrointestinal distress, blurred vision, and a rash. She lived with her husband and child, smoked 5 to 10 cigarettes daily, drank alcohol rarely, and did not use illicit drugs. There was a family his-tory of coronary artery disease, hypertension, and bipolar disorder, and an aunt had systemic lupus erythematosus.
On examination, the blood pressure was 118/70 mm Hg, the pulse 135 beats per minute, and the temperature 38.9°C; the respirations were 20 breaths per minute, and the oxygen saturation was 99% while she was breathing ambient air. She appeared ill. The physical examination was unchanged. Results of laboratory tests are shown in Table 1; specimens of blood were sent for cul-ture. Computed tomographic (CT) scans of the neck showed a mass, 2 cm in diameter in the inferior left masseter muscle near the angle of the jaw, enlarged cervical lymph nodes, and acute and chronic sinusitis. An ECG revealed sinus tachycardia at a rate of 120 beats per minute and nonspecific ST-segment and T-wave abnormali-ties. Radiographs of the pelvis and chest were nor-mal. Vancomycin, levofloxacin, clindamycin, and stress-dose corticosteroids were administered.
The next morning, 21 hours after arrival in the emergency department, she reported chest tightness, worse with inspiration. An electrocar-diogram (Fig. 1 in the Supplementary Appendix,
available with the full text of this article at www.nejm.org) showed sinus tachycardia at 112 beats per minute and ST-segment elevation of 1 to 2 mm in leads I, aVL, V4, and V5. Results of laboratory tests are shown in Table 1. Heparin and metopro-lol were administered intravenously. The blood pressure fell to 92/53 mm Hg and then to 71/30 mm Hg, and dopamine and saline were infused intravenously. Transthoracic echocardiography re-vealed mild left ventricular dysfunction with in-ferior and septal wall-motion abnormalities, a left ventricular ejection fraction of 43%, and a small pericardial effusion with partial right atrial inver-sion. She was admitted to the cardiac intensive care unit 28 hours after arrival in the emergency department.
On arrival in the intensive care unit, the blood pressure was 149/119 mm Hg, with a pulsus paradoxus of 7 mm Hg, the pulse 135 beats per minute, and the temperature 38.5°C; the respira-tions were 20 breaths per minute, and the arte-rial oxygen saturation was 97% while the patient was breathing 6 liters of oxygen by nasal cannula. Crackles were heard over both lung bases. The jugular venous pressure was 11 cm of water; there was no Kussmaul’s sign, and no extra heart sounds were heard. The arms and legs were warm, with no edema. An ECG showed sinus tachycardia at 140 beats per minute and diffuse ST-segment elevation of 1 mm or more in leads I, aVL, V2 through V6, and II.
The next morning, a chest radiograph showed perihilar pulmonary edema. The heart and medi-astinum were normal. Repeated transthoracic echocardiography showed deterioration of left ven-tricular function, with an ejection fraction of 32%, increased thickness of the left ventricular wall, right ventricular dysfunction, a small circumfer-ential pericardial effusion, right atrial and right ventricular inversions, and marked respiratory vari-ations of the mitral and tricuspid inflow according to Doppler signals. The patient was taken to the cardiac catheterization laboratory, and a pulmonary arterial line was placed; mean right atrial, right ventricular end-diastolic, and mean pulmonary capillary wedge pressures were 20 to 25 mm Hg. The cardiac output was 2.2 liters per minute. Peri-cardiocentesis was performed, revealing a mean pericardial pressure of 23 mm Hg. After 150 ml of pink, slightly turbid fluid was aspirated, the cardiac output rose to 3.3 liters per minute. Coro-nary angiography revealed no stenoses.
The aspirated fluid contained 1530 white cells
Downloaded from www.nejm.org on November 28, 2007 . Copyright © 2007 Massachusetts Medical Society. All rights reserved.

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 357;21 www.nejm.org november 22, 20072170
per cubic millimeter, with 63% eosinophils; the protein level was 4.5 g per deciliter, the amylase level was 21 U per liter, and the lactic dehydro-genase level was 744 U per liter. A Gram’s stain revealed no microorganisms. Solumedrol (1 g dai-ly) was started intravenously.
The same day, pathological examination of a fine-needle aspiration of the mass in the left jaw revealed skeletal muscle with mixed inflamma-tory cells, including eosinophils; flow cytometry disclosed polyclonal CD19+ B cells and CD4+ and CD8+ T cells. Serum protein electrophoresis and levels of immunoglobulins were normal, a test for antinuclear antibodies was positive at a titer of 1:40 in a speckled pattern, and other autoanti-body testing was negative. Other test results are shown in Table 1.
On the fourth hospital day, a chest radiograph showed increased pulmonary edema. Another transthoracic echocardiogram showed no pericar-dial effusion, but there was further decline of function of both ventricles, with a left ventricu-lar ejection fraction of 16%.
A diagnostic procedure was performed.
Differ en ti a l Di agnosis
Dr. Marc S. Sabatine: May we review the imaging studies?
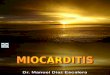
Dr. Jo-Anne O. Shepard: A CT scan of the facial bones and neck (Fig. 1A), performed after the intravenous administration of contrast material, showed a rounded opacity with peripheral en-hancement in the left masseter muscle, with cen-tral necrosis, which was suspicious for a small abscess, and left cervical lymphadenopathy. On the second hospital day, perihilar interstitial pul-monary edema was evident on chest radiographs (Fig. 1B); the edema increased by day 4. The heart size remained normal, despite the presence of a small pericardial effusion.
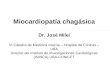
Dr. Kian-Keong Poh: The first transthoracic echo-cardiogram shows mild left ventricular systolic dysfunction with hypokinesia of the inferior and septal walls and a small circumferential pericar-dial effusion resulting in right atrial inversion. The next day, there was increased left ventricular wall thickness and a further decrease in left ven-tricular systolic function, right ventricular systolic dysfunction with persistence of the pericardial effusion, and right atrial collapse (Fig. 2A, and Video 1 in the Supplementary Appendix). Pulsed-
wave Doppler studies of the mitral inflow (Fig. 2B) and tricuspid inflow and aortic outflow showed clinically significant respiratory variations, con-sistent with increased intrapericardial pressure.
Dr. Jessica L. Mega: Cardiac catheterization showed
16p6
AUTHOR Sabatine
FIGURE 1 a&b of 3
JOB: ISSUE:
4-CH/T
RETAKE 1st
2nd
SIZE
ICM
CASE
EMail LineH/TCombo
Revised
AUTHOR, PLEASE NOTE: Figure has been redrawn and type has been reset.
Please check carefully.
REG F
FILL
TITLE3rd
Enon ARTIST:
11-22-07
mst
35721
A
B
Figure 1. Radiologic Images.
A CT scan of the facial bones and neck on the first hos-pital day (Panel A) shows a rounded opacity with periph-eral enhancement and central necrosis in the left sub-mandibular region, which suggested a small abscess (arrow). A chest radiograph on the second hospital day (Panel B) reveals perihilar pulmonary edema.
Downloaded from www.nejm.org on November 28, 2007 . Copyright © 2007 Massachusetts Medical Society. All rights reserved.

case records of the massachusetts gener al hospital
n engl j med 357;21 www.nejm.org november 22, 2007 2171
an elevated right atrial pressure of 22 mm Hg, a right ventricular end-diastolic pressure of 22 mm Hg, and a mean pulmonary-capillary wedge pressure of 25 mm Hg (Fig. 2 in the Supplemen-tary Appendix). The pericardial pressure was ele-vated, at 23 mm Hg, equal to the mean right atrial pressure (Fig. 3A in the Supplementary Appendix). In addition, there was marked varia-tion in the aortic pressure tracing with respira-tions (Fig. 3B in the Supplementary Appendix). After fluid was aspirated from the pericardial space, the pericardial pressure was 10 mm Hg and the aortic pressure tracing normalized (Fig. 3C and 3D in the Supplementary Appendix). Before the procedure, the cardiac index was 1.3 liters per minute per square meter of body-surface area, with a stroke volume index of 9 ml per square
meter. After the procedure, the cardiac index improved to 1.9 liters per minute per square meter, with a stroke volume index of 16 ml per square meter.
Dr. Poh: Echocardiography performed 1 day after the pericardial drainage revealed no peri-cardial effusion. However, the left and right ventricular functions had deteriorated further; in particular, the left ventricle showed diffuse and severe involvement, with hypokinesia in all walls. The left ventricular ejection fraction was 16%, contributed mainly by its base (Video 2 in the Supplementary Appendix). There was echocardio-graphic documentation of a rapidly progressive process over a few days, resulting in biventricular failure.
Dr. Sabatine: I participated in this patient’s care and am aware of the diagnosis. Three weeks be-fore this 31-year-old woman presented to this hospital, periorbital erythema, a conjunctival dis-charge, and a pruritic facial rash developed after she had started taking modafinil. Despite treat-ment with antihistamines and corticosteroids, her symptoms persisted. At another hospital, a low-grade fever, left facial swelling, and transient hypotension were noted. She was transferred here for evaluation of a possible facial abscess. How-ever, her course took an unexpected turn when chest pain developed, and she was found to have ST-segment elevation and elevated cardiac bio-markers of necrosis. Although initially there was concern about an acute coronary syndrome, the patient’s sex and age, the diffuse nature of the ST-segment elevation, the relatively minor degree of elevation of biomarkers, and the mild diffuse left ventricular dysfunction that did not match the ECG changes all pointed to myopericarditis.
There were several early clues to the severity of this patient’s hemodynamic compromise. Hypo-tension that developed in response to treatment with a beta-blocker showed that she was depen-dent on sympathetically mediated increases in heart rate and contractility to maintain blood pressure. This finding suggests a greatly reduced stroke volume, most commonly seen in cases of hypovolemic shock. Yet after aggressive fluid re-suscitation, although her blood pressure returned to normal, she had a narrow pulse pressure, con-sistent with a low stroke volume. This observa-tion, coupled with elevated jugular venous pulsa-tions and crackles over the lung fields, suggested profound myocardial dysfunction caused by im-
16p6
AUTHOR Sabatine
FIGURE 2a&b of 3
JOB: ISSUE:
4-CH/T
RETAKE 1st2nd
SIZE
ICM
CASE
EMail LineH/TCombo
Revised
AUTHOR, PLEASE NOTE: Figure has been redrawn and type has been reset.
Please check carefully.
REG F
FILL
TITLE3rd
Enon ARTIST:
11-22-07
mst
35721
A
B
PE
LV
RVRA
LA
Figure 2. Echocardiographic Images.
A transthoracic echocardiogram (Panel A) on the second hospital day at the apical four-chamber window shows a small pericardial effusion (PE) and right atrial inversion (arrow). LA denotes left atrium, RA right atrium, LV left ventricle, and RV right ventricle. A pulsed-wave Doppler echocardiogram (Panel B) shows significant respiratory variation of the transmitral flow velocities, with a de-crease in inspiration.
Downloaded from www.nejm.org on November 28, 2007 . Copyright © 2007 Massachusetts Medical Society. All rights reserved.

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 357;21 www.nejm.org november 22, 20072172
paired contractility, pericardial tamponade, or, as it turns out in this case, both.
Although the list of cardiomyopathies is exten-sive, the rapid deterioration of systolic function in this patient suggests an acute myocarditis. An-other possibility that was briefly considered was cardiac involvement by a sarcoma or a lymphoma because of her fever, soft-tissue mass, and cervi-cal lymphadenopathy. However, myocardial in-volvement by tumor typically presents with re-strictive physiology and arrhythmias, rather than with rapidly progressive systolic dysfunction, and neither fine-needle aspiration of the mass nor cy-tologic examination of the pericardial fluid re-vealed malignant tumor.
Infectious Myocarditis
Several forms of myocarditis merit consideration in this case.1 Viral myocarditis is often preceded by a viral prodrome, although this finding is nei-ther sensitive nor specific. Presentations range from slow development of heart failure to rapid de-velopment of cardiogenic shock. The ECG often shows nonspecific ST-segment and T-wave abnor-malities; echocardiographic findings range from a nondilated left ventricle seen in the acute phase to a spherical, dilated left ventricle in the chronic phase. This patient’s presentation is best described as fulminant myocarditis, which has a distinct on-set, a nondilated and thickened left ventricle, and severe systolic dysfunction leading to cardiogenic shock.2 Patients either recover spontaneously or die.3 Bacterial myocarditis was a possibility in this patient because of her possible abscess. However, one would have expected a purulent pericardial fluid and distributive shock requiring vasopres-sors. Lyme disease can manifest with rash and myocarditis, but the latter is usually mild. Rick-ettsial disease presents with rash, fever, hypoten-sion, and only a mild myocarditis.
Autoimmune myocarditis
Autoimmune myocarditides should be considered in this young woman with an autoimmune disor-der (multiple sclerosis), a rash, and a family his-tory of systemic lupus erythematosus. Both sys-temic lupus erythematosus and polymyositis can be associated with pericarditis and myocarditis, but the myocarditis tends to be mild. This patient did not have rheumatologic, dermatologic, or se-rologic manifestations of those disorders.
Idiopathic isolated giant-cell myocarditis
Idiopathic giant-cell myocarditis is a fulminant disease that typically affects persons in their fourth and fifth decades.4 Approximately 20% of patients have an autoimmune disorder, although giant-cell myocarditis has not been described in association with multiple sclerosis. Patients often report antecedent symptoms of a viral upper re-spiratory tract infection, and chest pain is un-common. Symptoms of heart failure develop over a period of weeks to months, with a rapid dete-rioration of cardiac function during the final stages of the disease. Conduction-system disease and ventricular tachycardia may occur because of infiltration of the fascicles and myocardium, but ST-segment elevation is extremely rare. On echo-cardiography, left ventricular dilatation without hypertrophy is seen, with segmental or diffuse areas of hypokinesis. The pericardial effusion with eosinophils, the chest pain, and the ST-segment elevation seen in this patient are not typical fea-tures of idiopathic giant-cell myocarditis.
Eosinophilic cardiomyopathies
Eosinophilic cardiomyopathies include a range of clinical presentations and pathological findings (Table 2). Löffler’s endocarditis5 is a restrictive cardiomyopathy due to endomyocardial disease with mural thrombi (so-called thrombotic endo-carditis) and is secondary to eosinophilia from many causes. Endomyocardial fibrosis6 is a restric-tive cardiomyopathy affecting persons in tropical climates in whom peripheral eosinophilia is in-consistent. In both these disorders, which prob-ably represent a continuum,7 the disease typically develops gradually over a period of months to years. In contrast, this patient had a rapid decline in left ventricular function.
Acute eosinophilic myocarditis
Acute eosinophilic myocarditis (also known as hypersensitivity myocarditis) is caused by a drug hypersensitivity reaction8 and is characterized by fever, rash, peripheral eosinophilia, and elevated biomarkers of necrosis.9 ECG occasionally shows ST-segment elevation. Echocardiography reveals mild systolic dysfunction, increased wall thick-ness due to edema, and occasionally a pericardial effusion. Heart failure is typically mild, and pa-tients die of arrhythmias, rather than pump dys-function.10 Many drugs have been implicated in
Downloaded from www.nejm.org on November 28, 2007 . Copyright © 2007 Massachusetts Medical Society. All rights reserved.

case records of the massachusetts gener al hospital
n engl j med 357;21 www.nejm.org november 22, 2007 2173
Tabl
e 2.
Eos
inop
hilic
Car
diom
yopa
thie
s.
Feat
ure
Hyp
erse
nsiti
vity
M
yoca
rditi
sA
cute
Nec
rotiz
ing
Eosi
noph
ilic
Myo
card
itis
Löff
ler’
s En
doca
rditi
sEn
dom
yoca
rdia
l Fib
rosi
s
Dem
ogra
phic
sA
nyO
ccas
iona
l his
tory
of a
llerg
ic
diso
rder
sM
ale,
tem
pera
te c
limat
esTr
opic
al c
limat
es
Prec
ipita
ntM
edic
atio
nM
edic
atio
n, v
iral
infe
ctio
n, o
r an
y ca
use
of e
osin
ophi
liaA
ny c
ause
of e
osin
ophi
lia, i
nclu
ding
dru
g hy
pers
ensi
tivity
re
actio
n, p
aras
itic
infe
ctio
n, a
llerg
ic d
isor
der,
vas
culi-
tides
(e.g
., C
hurg
–Str
auss
syn
drom
e, p
olya
rter
itis
no-
dosa
), h
yper
eosi
noph
ilic
synd
rom
e, e
osin
ophi
lic le
u-ke
mia
, oth
er m
alig
nanc
ies
(e.g
., H
odgk
in’s
dis
ease
)
Any
cau
se o
f eos
inop
hilia
, inc
lud-
ing
drug
hyp
erse
nsiti
vity
rea
c-tio
n, p
aras
itic
infe
ctio
n, a
llerg
ic
diso
rder
, vas
culit
ides
(e.
g.,
Chu
rg–S
trau
ss s
yndr
ome,
pol
y-ar
teri
tis n
odos
a), h
yper
eosi
no-
phili
c sy
ndro
me,
eos
inop
hilic
le
ukem
ia, o
ther
mal
igna
ncie
s (e
.g.,
Hod
gkin
’s d
isea
se)
Tem
poA
cute
and
tran
sien
tA
cute
and
sev
ere
Suba
cute
Gra
dual
Clin
ical
pre
sent
atio
nU
sual
ly fe
ver
and
rash
Mild
hea
rt fa
ilure
Arr
hyth
mia
s
Som
etim
es fe
ver
and
rash
Che
st p
ain
Fulm
inan
t hea
rt fa
ilure
Usu
ally
feve
r an
d ra
shR
ight
-sid
ed m
ore
ofte
n th
an le
ft-s
ided
hea
rt fa
ilure
Embo
lic e
vent
s
Rig
ht-s
ided
mor
e of
ten
than
left
-si
ded
hear
t fai
lure
Perip
hera
l eos
inop
hilia
Som
etim
esU
sual
lyA
lmos
t alw
ays
Rar
ely
Bio
mar
kers
of n
ecro
sis
Mod
estly
ele
vate
dEl
evat
edN
orm
alN
orm
al
ECG
Non
spec
ific
ST-s
egm
ent
and
T-w
ave
abno
r-m
aliti
es
Sinu
s ta
chyc
ardi
aST
-seg
men
t ele
vatio
nLo
w v
olta
ge
Non
spec
ific
ST-s
egm
ent a
nd T
-wav
e ab
norm
aliti
esN
onsp
ecifi
c ST
-seg
men
t and
T-w
ave
abno
rmal
ities
Echo
card
iogr
aphy
Mild
sys
tolic
dys
func
tion
Occ
asio
nal p
eric
ardi
al
effu
sion
Seve
re s
ysto
lic d
ysfu
nctio
nIn
crea
sed
wal
l thi
ckne
ssPe
rica
rdia
l effu
sion
Res
tric
tive
card
iom
yopa
thy
Mur
al th
rom
biTh
rom
botic
veg
etat
ions
Mitr
al a
nd tr
icus
pid
regu
rgita
tion
Res
tric
tive
card
iom
yopa
thy
Org
aniz
ed m
ural
thro
mbi
Mitr
al a
nd tr
icus
pid
regu
rgita
tion
Path
olog
yEo
sino
phili
c in
filtr
ate
Mild
nec
rosi
sEo
sino
phili
c in
filtr
ate
Seve
re n
ecro
sis
Occ
asio
nal g
iant
cel
ls
Mild
eos
inop
hilic
infil
trat
eEn
dom
yoca
rdia
l thi
cken
ing
and
fibro
sis
Ove
rlyi
ng th
rom
bosi
s
Occ
asio
nally
eos
inop
hilic
infil
trat
eEn
dom
yoca
rdia
l thi
cken
ing
and
fibro
sis
Occ
asio
nal o
rgan
ized
thro
mbo
sis
Prog
nosi
sSe
lf-lim
ited
Poor
Irre
vers
ible
Irre
vers
ible
Downloaded from www.nejm.org on November 28, 2007 . Copyright © 2007 Massachusetts Medical Society. All rights reserved.

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 357;21 www.nejm.org november 22, 20072174
acute eosinophilic myocarditis (Table 3),9,10 in-cluding tetracyclines,10 carbamazepine,11 and per-phenazine.12 When I saw this patient, I found no reports that associated modafinil with acute eo-sinophilic myocarditis. The time of onset after starting a drug varies from days to months. The incidence of acute eosinophilic myocarditis ranges from more than 40% of patients recently taking sulfonamides8 to less than 1% of patients taking clozapine.13
Acute necrotizing eosinophilic myocarditis
A fulminant form of hypersensitivity myocarditis, called acute necrotizing eosinophilic myocarditis, presents with severe heart failure that develops within days to a week.14-19 Although initiation of a new medication is often the precipitant (espe-cially in patients with a history of an allergic dia-thesis), cases occur in the setting of viral or para-sitic infection, the Churg–Strauss syndrome, or the hypereosinophilic syndrome. Fever and rash are common. The presentation often mimics that of acute myocardial infarction, with chest pain, ST-segment elevation, and elevated biomarkers of necrosis.20 Blood eosinophilia is present in most cases but can be mild. Echocardiography typically reveals normal chamber size (reflecting the sud-den onset of the process and lack of time for dilatation), increased wall thickness (probably re-flecting edema), and severe, biventricular diffuse systolic dysfunction. A pericardial effusion is seen in 75% of cases, occasionally causing tampon-ade.21 The mortality exceeds 50%, and the median survival is only a few days. Treatment consists of high-dose corticosteroids,9,19,22 pharmacologic or mechanical ventricular support, or both.23
Summary
In view of the tempo and severity of this patient’s disease, I thought that the most likely diagnoses were fulminant viral myocarditis, idiopathic giant-cell myocarditis, and acute necrotizing eosinophilic myocarditis. The chest pain, ST-segment elevation, lack of conduction block, and presence of a peri-cardial effusion make idiopathic giant-cell myo-carditis unlikely. The exposure to drugs associated with hypersensitivity myocarditis, the rash and fe-ver, and the eosinophil-rich pericardial effusion favor acute necrotizing eosinophilic myocarditis over fulminant viral myocarditis. Since the treat-ment of these three diseases differs, a specific diagnosis is important. Histologic examination would most clearly differentiate these entities, and thus the diagnostic procedure was an endomyo-cardial biopsy.
DR . M A RC S . S A B ATINE’S DI AGNOSIS
Acute necrotizing eosinophilic myocarditis due to a hypersensitivity reaction.
Pathol o gic a l Discussion
Dr. James R. Stone: Examination of the specimen from the endomyocardial biopsy revealed an ex-tensive inflammatory infiltrate composed mostly of eosinophils and macrophages and associated with myocyte necrosis (Fig. 3A). Immunohisto-chemical analysis showed that the lymphocytes were almost entirely CD3+ T cells, with a predom-inance of CD4+ over CD8+ cells (Fig. 4 in the Supplementary Appendix). There was no endocar-dial thickening or necrotizing vasculitis, nor were
Table 3. Medications Implicated in Hypersensitivity Myocarditis (Acute Eosinophilic Myocarditis and Acute Necrotizing Eosinophilic Myocarditis).*
Antibiotics Sulfonamides, beta-lactams, tetracyclines, aminoglycosides, trimethoprim, antiarrhythmics (quinidine, procainamide, lidocaine)
Cardiac medications Methyldopa, dobutamine, thiazides, furosemide
Antiepileptics Phenytoin, carbamazepine
Psychotropics Tricyclic antidepressants, phenothiazine antipsychotics, clozapine
Antimyocobacterials Streptomycin, isoniazid
Miscellaneous Nonsteroidal antiinflammatory drugs, methylxanthines, sulfonylureas
* The list, which is not meant to be comprehensive, includes medications that have been implicated at least twice on the basis of temporal association with onset of hypersensitivity myocarditis; causality is impossible to prove. More com-monly implicated medications are in bold.
Downloaded from www.nejm.org on November 28, 2007 . Copyright © 2007 Massachusetts Medical Society. All rights reserved.

case records of the massachusetts gener al hospital
n engl j med 357;21 www.nejm.org november 22, 2007 2175
there any giant cells. Focally, the inflammatory infiltrate was associated with small interstitial vessels, a feature that has been referred to as non-necrotizing vasculitis. There was no viral cyto-pathic effect or intracellular parasites, and spe-cial stains for organisms were negative.
In the absence of evidence of infection, the histologic findings on the endomyocardial biopsy are that of an acute necrotizing eosinophilic myo-carditis.16,18,19,24,25 In this patient, they are most likely a manifestation of a severe form of drug-induced hypersensitivity myocarditis.
Dr. Mega: At the time of the ventricular biopsy, an intraaortic balloon pump was placed because of deteriorating left ventricular function. The pa-tient then returned to the cardiac care unit, and methylprednisolone (1 mg per day) was contin-ued. Initially, her clinical status improved, and the dopamine dose was reduced. However, on the evening of the fourth hospital day, a refractory ventricular tachyarrhythmia developed, and she died. An autopsy was performed.
Dr. Stone: The heart was enlarged (468 g), with mild biventricular dilatation and a mottled ap-pearance of the ventricular myocardium (Fig. 3B, and Fig. 5 in the Supplementary Appendix), re-flecting necrosis involving about 80% of the myocardium (Fig. 3C). Around the outer portions of the zones of necrosis, there was an intense inflammatory infiltrate (Fig. 3C, inset, top) con-sisting predominantly of eosinophils and macro-phages, as observed in the endomyocardial biop-sy. In the central portions of the necrotic zones, macrophage giant cells were present and were engulfing necrotic myocytes (Fig. 3C, inset, bot-tom). As in the biopsy specimen, the T cells were predominantly CD4+ (Fig. 6 in the Supplemen-tary Appendix). The wall of the coronary sinus, containing cardiac myocytes, also showed inflam-matory infiltration and necrosis (Fig. 7 in the Supplementary Appendix). The inflammation in the heart extended into the epicardium, and there was focal eosinophilic vasculitis of the epicardial veins (Fig. 8 in the Supplementary Appendix). Stains of the myocardium for microorganisms were negative.
Skeletal muscle from the deltoid, diaphragm, and extraocular muscles showed similar changes (Fig. 8 in the Supplementary Appendix). Retro-spective analysis of the fine-needle aspirate from the left masseter muscle revealed eosinophils,
macrophages, and fragments of necrotic skeletal muscle and macrophage giant cells (Fig. 9 in the Supplementary Appendix). In the liver, small zones of necrosis in a random distribution were seen to contain inflammatory cells, predominant-ly macrophages with lesser numbers of T cells and rare eosinophils (Fig. 10 in the Supplemen-tary Appendix). There was no viral cytopathic ef-fect, and in situ hybridization for Epstein–Barr vi-rus RNA was negative.
These findings indicate the presence of a se-vere systemic necrotizing inflammatory reaction, associated with eosinophils and giant cells. Sev-eral systemic processes can result in giant cells in the heart, including sarcoidosis, acute rheu-matic fever, rheumatoid disease, antineutrophil cytoplasmic antibody–associated vasculitides, and amyloidosis, as well as mycobacterial, parasitic, and fungal infections, none of which are present in this case. Both giant cells and eosinophils may be present in giant-cell myocarditis, hypersensi-tivity myocarditis, and acute necrotizing eosino-philic myocarditis.
Giant-cell myocarditis occurs in two distinct forms: idiopathic isolated giant-cell myocarditis and thymoma-associated giant-cell polymyositis. Idiopathic isolated giant-cell myocarditis is limit-ed to the heart,4,26 with infiltration of myocar-dium by lymphocytes, macrophages, giant cells, and eosinophils and marked necrosis, whereas in thymoma-associated giant-cell polymyositis, a sim-ilar inflammatory infiltrate involves both cardi-ac and skeletal muscles.27,28 In giant-cell myocar-ditis, the T lymphocytes show a predominance of CD8+ over CD4+ staining,29 and the giant cells are typically proximate to both viable and dead myocytes, suggesting that they have an active role in the killing of myocytes.
Hypersensitivity myocarditis is often defined as a histologic pattern in which there is infil-tration of the myocardium by eosinophils, mac-rophages, and lymphocytes with minimal to no necrosis of myocytes.8-10 When necrotizing drug-induced hypersensitivity reactions are found, names such as drug-induced acute necrotizing eosinophilic myocarditis16,18,19,24,25 or drug- induced giant-cell myocarditis have been used30-32; however, these are probably the extreme end of the spectrum of hypersensitivity myocarditis. In cases of acute necrotizing eosinophilic myocardi-tis, as opposed to cases of giant-cell myocarditis,
Downloaded from www.nejm.org on November 28, 2007 . Copyright © 2007 Massachusetts Medical Society. All rights reserved.

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 357;21 www.nejm.org november 22, 20072176
giant cells may be seen only in areas of necrotic myocytes, where they are engaged in the removal of opsonin-coated myocyte debris, and the T cells are predominantly CD4+.33 Thus, this case has both morphologic and immunophenotypic fea-tures of acute necrotizing eosinophilic myocardi-tis. At autopsy, both necrotizing and non-necrotiz-ing cases of drug-induced eosinophilic myocarditis may have extracardiac involvement, as was seen in this case; most commonly, the liver is involved, and on rare occasions other organs are involved,
including the lung, the kidney, and skeletal mus-cle.8-10,30-32
This patient died in 2006. Since then, the pack-age insert for modafinil has been modified to include a warning relating to multiorgan hyper-sensitivity reactions.
Dr. Matthew P. Frosch: The brain and spinal cord were also examined. The plaques of multiple scle-rosis that had been identified by imaging studies were confirmed by gross and microscopical ex-amination of the brain, showing loss of myelin
39p6
A B
D E
C
AUTHOR Sabatine
JOB: ISSUE:
4-CH/T
RETAKE 1st2nd
SIZE
ICM
CASE
EMail LineH/TCombo
Revised
AUTHOR, PLEASE NOTE: Figure has been redrawn and type has been reset.
Please check carefully.
REG F
FILL
TITLE3rd
Enon ARTIST:
11-22-07
mst
35721
FIGURE 3a-e
Figure 3. Pathological Findings.
Panel A (hematoxylin and eosin) shows an inflammatory infiltrate with associated myocyte necrosis. A higher-power view (Panel A, inset) shows the infiltrate to be composed primarily of eosinophils and macrophages, with fewer lymphocytes. A formalin-fixed cut section of the heart at autopsy (Panel B) shows the left ventricular free wall as viewed from a posterior perspective. The aortic valve is in the upper right corner. The left circumflex artery, at the upper edge of the panel, is free of clinically significant atherosclerosis. The left ventricular myocardium shows diffuse mottling indicative of necrosis. A section of the myocardium (Panel C, hematoxylin and eosin) shows an in-flammatory infiltrate with associated myocyte necrosis in the bottom left corner, as it borders healthy myocardium in the upper right corner. A giant cell is present on the far left edge of the panel (arrow). A higher-power view of the edge of the inflammatory infiltrate (Panel C, inset, top) shows the infiltrate to be composed primarily of eosinophils and macrophages, with fewer lymphocytes. A higher-power view of the center of the zones of necrosis (Panel C, inset, bottom) shows the presence of macrophage giant cells engulfing ne-crotic myocyte debris. Microscopical examination of deep white matter reveals the presence of an area of demyelination with focal loss of myelin and relative axonal preservation (Panel D, arrows; axon stain not shown). A vessel with perivascular lymphocytic cuffing is evi-dent as well (arrowhead). A higher-magnification view of the blood vessel illustrates the perivascular lymphocytic infiltrate; eosinophils are not present (Panel D, inset, Luxol fast blue–hematoxylin and eosin). Perivascular inflammation, consisting predominantly of lymphocytes, is present in the dorsal horn of the lumbar spinal cord (Panel E).
Downloaded from www.nejm.org on November 28, 2007 . Copyright © 2007 Massachusetts Medical Society. All rights reserved.

case records of the massachusetts gener al hospital
n engl j med 357;21 www.nejm.org november 22, 2007 2177
(Fig. 3D) with relative axonal preservation. Al-though the plaques were chronic, there was mod-erate perivascular inflammation (Fig. 3D, inset) consisting of T cells with a predominance of CD4+ cells (Fig. 11 in the Supplementary Appendix).
Inflammation was also present in the spinal cord, most prominently in the dorsal horn (Fig. 3E), associated with gliosis but not demyelina-tion. There was also inflammation in the lepto-meninges and in the proximate portion of the peripheral nerve (Fig. 12 in the Supplementary Appendix). Even though none of these lesions contained eosinophils, the distribution of the inflammatory process (both central and periph-eral nervous systems) and the absence of associ-ated active demyelination suggests that these rep-resent involvement by the systemic necrotizing hypersensitivity reaction rather than a manifes-tation of multiple sclerosis.
Dr. Aaron Baggish (Cardiology Division): The cause of death in this patient was a malignant ventricular tachyarrhythmia in the context of clin-ically improving heart failure. Do you think there
is a role for treating such patients with prophylac-tic antiarrhythmic therapy?
Dr. Sabatine: Extrapolating from the literature on myocardial infarction, pharmacologic arrhyth-mia prophylaxis does not appear to be benefi-cial; rather, patients should be monitored close-ly and arrhythmias treated immediately.
A nat omic a l Di agnosis
Acute necrotizing eosinophilic myocarditis asso-ciated with a systemic necrotizing inflammatory process also involving skeletal muscle, the liver, and the spinal cord, most consistent with a severe drug-induced hypersensitivity reaction.
Dr. Sabatine reports receiving research grants from Sanofi–Aventis and Schering-Plough, research reagents from Roche, diaDexus, and Singulex, and lecture and consulting fees from Bristol-Myers Squibb, Sanofi–Aventis, diaDexus Novartis, and Daiichi Sankyo; Dr. Mega, grant support from Schering-Plough; Dr. Shepard, consulting fees from R2 Technology; Dr. Stone, consulting fees from Merck, MuscleTech, GNC Corporation, and Wal-Mart; and Dr. Frosch, consulting fees from Biogenidec and Bristol-Myers Squibb. No other potential conflict of interest rele-vant to this article was reported.
References
Feldman AM, McNamara D. Myocar-ditis. N Engl J Med 2000;343:1388-98.
Lieberman EB, Hutchins GM, Hersko-witz A, Rose NR, Baughman KL. Clinico-pathologic description of myocarditis. J Am Coll Cardiol 1991;18:1617-26.
Mason JW, O’Connell JB, Herskowitz A, et al. A clinical trial of immunosup-pressive therapy for myocarditis. N Engl J Med 1995;333:269-75.
Cooper LT Jr, Berry GJ, Shabetai R. Idiopathic giant-cell myocarditis — natu-ral history and treatment. N Engl J Med 1997;336:1860-6.
Löffler W. Endocarditis parietalis fi-broplastica mit bluteosinophilie. Schweiz Med Wochenschr 1936;66:817.
Davies JNP. Endomyocardial fibrosis in Africans. East Afr Med J 1948;25:10-4.
Roberts WC, Liegler DG, Carbone PP. Endomyocardial disease and eosinophilia: a clinical and pathologic spectrum. Am J Med 1969;46:28-42.
French AJ, Weller CV. Interstitial myo-carditis following the clinical and experi-mental use of sulfonamide drugs. Am J Pathol 1942;18:109-21.
Fenoglio JJ Jr, McAllister HA Jr, Mul-lick FG. Drug related myocarditis. I. Hy-persensitivity myocarditis. Hum Pathol 1981;12:900-7.
Burke AP, Saenger J, Mullick F, Vir-mani R. Hypersensitivity myocarditis. Arch Pathol Lab Med 1991;115:764-9.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
Salzman MB, Valderrama E, Sood SK. Carbamazepine and fatal eosinophilic myo-carditis. N Engl J Med 1997;336:878-9.
Ansari A, Maron BJ, Berntson DG. Drug-induced toxic myocarditis. Tex Heart Inst J 2003;30:76-9.
Killian JG, Kerr K, Lawrence C, Celer-majer DS. Myocarditis and cardiomyopa-thy associated with clozapine. Lancet 1999; 354:1841-5.
Langsjoen PH, Stinson JC. Acute fatal allergic myocarditis: report of a case. Dis Chest 1965;48:440-1.
Barrett DA II, Dalldorf FG, Barnwell WH II, Hudson RP. Allergic giant cell myo-carditis complicating tuberculosis chemo-therapy. Arch Pathol 1971;91:201-5.
Herzog CA, Snover DC, Staley NA. Acute necrotising eosinophilic myocardi-tis. Br Heart J 1984;52:343-8.
Taliercio CP, Olney BA, Lie JT. Myo-carditis related to drug hypersensitivity. Mayo Clin Proc 1985;60:463-8.
deMello DE, Liapis H, Jureidini S, Nouri S, Kephart GM, Gleich GJ. Cardiac localization of eosinophil-granule major basic protein in acute necrotizing myo-carditis. N Engl J Med 1990;323:1542-5.
Getz MA, Subramanian R, Logemann T, Ballantyne F. Acute necrotizing eosino-philic myocarditis as a manifestation of severe hypersensitivity myocarditis: ante-mortem diagnosis and successful treat-ment. Ann Intern Med 1991;115:201-2.
11.
12.
13.
14.
15.
16.
17.
18.
19.
Galiuto L, Enriquez-Sarano M, Reeder GS, et al. Eosinophilic myocarditis man-ifesting as myocardial infarction: early diagnosis and successful treatment. Mayo Clin Proc 1997;72:603-10.
Kazama R, Okura Y, Hoyano M, et al. Therapeutic role of pericardiocentesis for acute necrotizing eosinophilic myocardi-tis with cardiac tamponade. Mayo Clin Proc 2003;78:901-7.
Kim CH, Vlietstra RE, Edwards WD, Reeder GS, Gleich GJ. Steroid-responsive eosinophilic myocarditis: diagnosis by en-domyocardial biopsy. Am J Cardiol 1984; 53:1472-3.
Cooper LT, Zehr KJ. Biventricular assist device placement and immunosup-pression as therapy for necrotizing eosin-ophilic myocarditis. Nat Clin Pract Car-diovasc Med 2005;2:544-8.
Aggarwal A, Bergin P, Jessup P, Kaye D. Hypersensitivity myocarditis presenting as cardiogenic shock. J Heart Lung Trans-plant 2001;20:1241-4.
Lee C-W, Mitchell RN, Horan RF, Cas-tells MC. Cardiogenic shock and periph-eral eosinophilia in a young woman. Ann Allergy Asthma Immunol 2005;95:229-33.
Rosenstein ED, Zucker MJ, Kramer N. Giant cell myocarditis: most fatal of auto-immune diseases. Semin Arthritis Rheum 2000;30:1-16.
Burke JS, Medline NM, Katz A. Giant
20.
21.
22.
23.
24.
25.
26.
27.
Downloaded from www.nejm.org on November 28, 2007 . Copyright © 2007 Massachusetts Medical Society. All rights reserved.

n engl j med 357;21 www.nejm.org november 22, 20072178
case records of the massachusetts gener al hospital
Lantern Slides Updated: Complete PowerPoint Slide Sets from the Clinicopathological Conferences
Any reader of the Journal who uses the Case Records of the Massachusetts General Hospital as a teaching exercise or reference material is now eligible to receive a complete set of PowerPoint slides, including digital images, with identifying legends, shown at the live Clinicopathological Conference (CPC) that is the basis of the Case Record. This slide set contains all of the images from the CPC, not only those published in the Journal. Radiographic, neurologic, and cardiac studies, gross specimens, and photomicrographs, as well as unpublished text slides, tables, and diagrams, are included. Every year 40 sets are produced, averaging 50-60 slides per set. Each set is supplied on a compact disc and is mailed to coincide with the publication of the Case Record.
The cost of an annual subscription is $600, or individual sets may be purchased for $50 each. Application forms for the current subscription year, which began in January, may be obtained from the Lantern Slides Service, Department of Pathology, Massachusetts General Hospital, Boston, MA 02114 (telephone 617-726-2974) or e-mail [email protected].
cell myocarditis and myositis: associated with thymoma and myasthenia gravis. Arch Pathol 1969;88:359-66.
Namba T, Brunner NG, Grob D. Idio-pathic giant cell polymyositis: report of a case and review of the syndrome. Arch Neurol 1974;31:27-30.
Litovsky SH, Burke AP, Virmani R. Gi-ant cell myocarditis: an entity distinct from sarcoidosis characterized by multi-phasic myocyte destruction by cytotoxic
28.
29.
T cells and histiocytic giant cells. Mod Pathol 1996;9:1126-34.
Ishikawa H, Kaneko H, Watanabe H, Takagi A, Ming ZW. Giant cell myocardi-tis in association with drug-induced skin eruption. Acta Pathol Jpn 1987;37:639-44.
Adachi Y, Yasumizu R, Hashimoto F, et al. An autopsy case of giant cell myo-carditis probably due to a non-steroidal anti-inflammatory drug. Pathol Int 2001; 51:113-7.
30.
31.
Daniels PR, Berry GJ, Tazelaar HD, Cooper LT. Giant cell myocarditis as a man-ifestation of drug hypersensitivity. Cardio-vasc Pathol 2000;9:287-91.
Gravanis MB, Hertzler GL, Franch RH, et al. Hypersensitivity myocarditis in heart transplant candidates. J Heart Lung Trans-plant 1991;10:688-97.Copyright © 2007 Massachusetts Medical Society.
32.
33.
Downloaded from www.nejm.org on November 28, 2007 . Copyright © 2007 Massachusetts Medical Society. All rights reserved.







![Caso Clinico Colitis Eosinofilica Final[1]](https://img.dokumen.tips/doc/110x75/5571fc1e49795991699688c8/caso-clinico-colitis-eosinofilica-final1.jpg)