Embed Size (px)
Citation preview
DOI: 10.1542/peds.104.1.43 1999;104;43-49 Pediatrics
Mandel and Merrill Weiner Sandra J. Kaplan, Victor Labruna, David Pelcovitz, Suzanne Salzinger, Francine
Comparison of Informants' ReportsPhysically Abused Adolescents: Behavior Problems, Functional Impairment, and
This information is current as of October 5, 2005
http://www.pediatrics.org/cgi/content/full/104/1/43located on the World Wide Web at:
The online version of this article, along with updated information and services, is
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275. Grove Village, Illinois, 60007. Copyright © 1999 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by on October 5, 2005 www.pediatrics.orgDownloaded from

Physically Abused Adolescents: Behavior Problems, FunctionalImpairment, and Comparison of Informants’ Reports
Sandra J. Kaplan, MD*; Victor Labruna, PhD*; David Pelcovitz, PhD*; Suzanne Salzinger, PhD‡;Francine Mandel, PhD§; and Merrill Weiner, ACSW*
ABSTRACT. Objective. This study, like earlier stud-ies that focused on younger abused children, ascertainedwhether physically abused adolescents exhibited in-creased internalizing and externalizing behaviors. Rele-vance to pediatric practice is discussed.
Design. A cross-sectional design was used to comparethe behavior of physically abused adolescents and com-parison adolescents using self-reports, parent reports,and teacher reports. The level of agreement among raterswas also examined.
Participants. The subjects were 99 physically abusedadolescents between the ages of 12 and 18 years, whowere recruited from Child Protective Services. Compari-son subjects were 99 community-recruited nonabusedadolescents who were matched for age, gender, and in-come with the abused adolescents.
Measures. The behavior of the adolescents was as-sessed using the Child Behavior Checklist, and the com-parable Youth Self-Report and Teacher Report Form,which are widely used measures of behavioral and emo-tional problems. The Child Global Assessment Scale wasalso used as a measure of functional impairment and ofthe need for mental health services.
Results. Parents and teachers rated the problems ofabused adolescents as significantly greater than the prob-lems of nonabused adolescents on all checklist subscales.Abused adolescents reported significantly greater prob-lems only on externalizing behavior subscales. In addi-tion, based on interviewer ratings, physically abused ad-olescents exhibited significantly greater functionalimpairment.
Conclusions. Similar to previous research onabused children, physically abused adolescents exhibitexternalizing and internalizing behavior problems andexperience greater functional impairment. Parent,teacher, and adolescent reports of externalizing behav-iors were similar, but physically abused adolescentsreported fewer internalizing behaviors than did theother informants. Pediatrics 1999;104:43– 49; physicalabuse, adolescent abuse, behavior problems, multipleinformants.
ABBREVIATIONS. CPS, Child Protective Services; CBCL, ChildBehavior Checklist; YSR, Youth Self-Report; TRF, Teacher RatingForm; CGAS, Child Global Assessment Scale; RMANOVA, re-peated measures ANOVA.
Adolescent physical abuse is an important, butgenerally under-studied, national publichealth issue. In a 1996 report of national
abuse statistics from Child Protective Services (CPS)from 48 states, adolescents between the ages of 12and 18 years made up 22.7% of the 258 588 totalmaltreatment cases and 31.5% of the 60 105 physicalabuse cases.1 However, despite the high percentageof cases in which adolescents are the targets of phys-ical abuse, most abuse research has focused onyounger children. This previous research has indi-cated that physical abuse is associated with a widerange of behavioral disturbances in children. Feld-man and colleagues2 reported that nonreferred phys-ically abused children (8–12 years old) were ratedsignificantly higher by their mothers and teachers onthe overall Behavior Problems scale as well as theInternalizing and Externalizing scales of the ChildBehavior Checklist (CBCL) and Teacher’s ReportForm (TRF) than were nonabused children. Internal-izing problems generally refer to problems that areprimarily distressing to the individual, including de-pression, anxiety, and somatic complaints that arenot related to a medical condition. Externalizingproblems refer to behavior that negatively affectsothers, usually behaviors that are aggressive or anti-social.
Kinard3 also found that on the CBCL the mothers ofnonreferred abused children (7–11 years old) ratedtheir children as having greater levels of behavior prob-lems, compared with mothers of nonabused children.Abused boys received significantly higher scores on alleight subscales of the CBCL, whereas abused girls wererated significantly higher on Social Problems, AttentionProblems, Delinquent Behavior, and Aggressive Be-havior scales. The teachers of abused subjects also ratedthe subjects as having significantly higher scores onmost behavior problem subscales. In addition to highermean scores on CBCL subscales, abused children hadsignificantly more frequent clinically elevated scoreson the broad-band Internalizing, Externalizing, andTotal Problem behavior scales. These studies con-firmed the findings of earlier studies, indicating thatabused children exhibit a wide variety of problembehaviors.4,5
From the *Department of Psychiatry, Division of Child and AdolescentPsychiatry, North Shore University Hospital, New York University Schoolof Medicine; ‡Division of Child Psychiatry, New York State PsychiatricInstitute; and §Department of Research, Division of Biostatistics, NorthShore University Hospital, New York University School of Medicine,Manhasset, New York.Received for publication Nov 5, 1998; accepted Feb 12, 1999.Reprint requests to (S.J.K.) Department of Psychiatry, North Shore Univer-sity Hospital, 300 Community Drive, Manhasset, NY 11030. E-mail:[email protected] (ISSN 0031 4005). Copyright © 1999 by the American Acad-emy of Pediatrics.
PEDIATRICS Vol. 104 No. 1 July 1999 43 by on October 5, 2005 www.pediatrics.orgDownloaded from

However, few studies have focused on the associ-ation between physical abuse and problem behaviorin adolescents. In addition, these abuse studies havenot used a measure of functional impairment thatprovides information on the severity of behaviorproblems that are distinct from individual symptomsand diagnoses.6 The present study examined bothbehavior problems and overall functional impair-ment in physically abused adolescents comparedwith nonabused adolescents. It was hypothesizedthat physically abused adolescents would exhibit in-creased internalizing and externalizing problem be-havior and greater functional impairment, comparedwith a sample of nonabused adolescents matched forage, race, and community income.
Only subjects who were legally documented vic-tims of abuse were included in this study, and thestudy focused solely on the physical abuse of ado-lescents, excluding victims of sexual abuse or ne-glect-only, and children younger than 12 years ofage. Behavioral measures were completed by fourgroups of informants: mothers, fathers, teachers, andthe adolescents themselves.
To assess properly the extent of the problems ex-perienced by abused adolescents, it is important toconsider the level of agreement among the ratings ofdifferent informants. Although gathering informa-tion from multiple sources is important to the devel-opment of a comprehensive understanding of behav-ior, the research literature has indicated thatagreement among informants concerning child andadolescent problems is often only modest and mayeven be contradictory. For example, clinically re-ferred children have been found to report fewerproblem behaviors (particularly externalizing behav-iors) than do their parents, whereas nonreferred chil-dren report more problem behaviors than do theirparents.7,8 Agreement between the reports of mothersand fathers has usually been only moderate, with thelevel of agreement attenuated additionally in fami-lies experiencing high levels of stress.9 The corre-spondence of parent and teacher ratings has beenreported to be even poorer.10
Although physical abuse is expected to have anegative effect on behavior, it may also influence thewillingness of both the parent and the child to ac-knowledge certain behavior problems. Abusive par-ents and their spouses have been found to report thattheir children exhibit a higher number of behaviorproblems than independent observers of these chil-dren report.11,12 Informant agreement is not alwayspoor. For example, Feldman and colleagues2 foundthat mothers and teachers produced similar behaviorratings of abused children (8–12 years old). How-ever, until the present study, there were no pub-lished studies of abused youth that included fourdifferent informant sources or that examine abusedadolescents.
The data for the present paper were drawn from acomprehensive study of the relationship betweenadolescent physical abuse and psychopathology.Previous papers have reported on the relationship ofadolescent physical abuse and/or exposure to do-mestic violence to suicide risk, psychiatric disorders,
academic performance, and family functioning inthis sample.13, 14
METHODS
SubjectsThe abuse sample consisted of 99 white adolescents between
the ages of 12 and 18 years who had been documented legally asphysically abused and entered into the New York State CentralRegister for Child Abuse and Neglect. Cases were documentedlegally when evidence was found by CPS caseworkers substanti-ating allegations of abuse made to the state’s central reportinghotline. Abused adolescents were drawn from the pool of alladolescents documented as physically abused by Nassau or Suf-folk County CPS between 1989 and 1991. Physical abuse wasdefined as physical assault of the adolescent by a parent or step-parent with resulting bodily injury evident for at least 48 hours.Physical abuse included assault with the use of an implement(belt, knife, cigarette, etc) or assault without an implement (beinghit, kicked, bitten, etc). The initial or most recent disclosure ofphysical abuse had to have occurred within 2 years of the time ofinclusion in the study. In addition, there could not have beenevidence or strong suspicion of intrafamilial sexual abuse. A re-view of CPS records indicated that a total of 974 families meteligibility criteria for inclusion in this study. Of these families,;75% were contacted by mail, and 124 families expressed aninterest in participation. A total of 25 families either did notcomplete the interview process or disclosed sexual abuse, result-ing in a final sample size of 99.
Severity of abuse was calculated from agency records using analgorithm that considered the type of injury, the type of abusivebehavior, and the need for medical attention. Severity scoresranged from 1 to 36 with an interquartile range of 2 to 6. A scoreof 3 or less was received by 50% of the group, and 86% of thegroup fell at or below a severity score of 6. Therefore, the majorityof adolescents in this study were the targets of relatively mildforms of physical abuse, consistent with previous research onadolescent abuse.15 Biological fathers were perpetrators of abuse in73% of the cases (mothers in 24% of cases and stepfathers in 12%of cases), whereas multiple perpetrators were involved in 11% ofthe cases.
Although there was no difference in severity of abuse betweenthe abuse group and the overall pool of adolescent abuse cases,CPS recommended psychotherapy for 65% of nonparticipatingadolescents, compared with 45% of participating adolescents (x2 58.59; df 5 1; P 5 .003), suggesting that individuals in the overallpool may have had more problems than did participating subjects.Additional comparisons indicated that the abuse group and theoverall pool did not differ on any of the numerous variablesdescribing demographic, family, and abuse characteristics.
Comparison subjects (n 5 99) were recruited by a marketingresearch company and were matched with abused adolescents forage, gender, and community income. There were no significantdifferences in socioeconomic status between the study groups,although divorce was more prevalent in the abuse group. Mothers(mean age 5 41.6 years) of abused adolescents were found to besignificantly younger than mothers (mean age 5 43.5 years) ofcomparison adolescents (Mann-Whitney U test 5 22.90; P , .01).No significant differences were found in the ages of the adoles-cents or fathers. The distribution of income for both groups indi-cates that each was predominantly middle-class.
The exclusion criterion of intrafamilial sexual abuse was as-sessed using a short sexual behavior questionnaire prepared forthis study. Adolescents or their parents who were found to haveintelligence quotients of #70, estimated by the Vocabulary andBlock Design Subtests of the Wechsler Intelligence Scale,16,17 werealso excluded. Comparison subjects who had experienced physicalabuse according to their responses on the Conflict TacticsScale18(CTS) were excluded as well.
ProceduresQuestionnaires were completed at home by parents and ado-
lescents. Although attempts were made to gather informationfrom both parents, some fathers declined to participate, and fa-thers were not recruited in cases in which potential harm couldcome to the family. Overall, 48% of fathers of abused adolescentsand 28% of comparison fathers did not participate.
44 BEHAVIOR PROBLEMS IN PHYSICALLY ABUSED ADOLESCENTS by on October 5, 2005 www.pediatrics.orgDownloaded from

The decision to study a white sample was made because of thedemographic characteristics of the counties in which subjects wererecruited. At the time, in these counties, most of the cases ofadolescent abuse involved white families; including the relativelysmall number of available minority subjects would not have en-abled reliable comparisons among racial and ethnic groups to bemade.
Confidentiality of information was guaranteed to all studyparticipants. Information concerning individual subjects was au-thorized by subjects to be shared with other family members onlyif there was a significant risk of death. Referrals for services weregiven to any subject in need of clinical assistance, as judged by theinterviewers or investigators.
The research procedures were approved by both the Institu-tional Review Boards of North Shore University Hospital and theNew York State Psychiatric Institute. Parents were required toprovide written informed consent, whereas adolescents providedwritten assent. Families received a maximum of $250.00 for par-ticipation in the overall research project.
MeasuresThe CBCL,19 Youth Self-Report (YSR),20 and TRF21 are standard-
ized behavior problem checklists made up of over 100 items. Theyhave been investigated extensively and have demonstrated ac-ceptable test-retest reliability and internal consistency. The valid-ity of these rating scales has been supported by their correlationswith other measures of behavior problems and by studies ofclinical populations.22 Eight subscales shared by the CBCL, YSR,and TRF have been identified. The Withdrawn, Somatic Com-plaints and Anxious/Depressed subscales measure internalizingproblems, and the Delinquent Behavior and Aggressive Behaviorsubscales assess externalizing behavior problems. The remainingshared subscales are Social Problems, Thought Problems, andAttention Problems.22 Raw scores on all scales were converted to Tscores for analyses.
The CBCL was completed by 86 mothers of abused adolescents,97 mothers of nonabused adolescents, 48 fathers of abused ado-lescents, and 57 fathers of nonabused adolescents. The YSR wascompleted by 94 of the abused adolescents and 98 of the non-abused adolescents. TRFs, completed by a teacher who was iden-tified as being familiar with the subject, were returned for 71abused adolescents and 72 nonabused adolescents.
The CGAS23 was used to measure functional impairment. It wascompleted by interviewers with at least graduate level trainingafter semistructured diagnostic interviews, which were part of thelarger study, had been conducted. All interviewers were blind tothe abuse status of subjects. The CGAS, an adaptation of theGlobal Assessment Scale,24 yields a single score that reflects theseverity of behavioral disturbance in terms of functional impair-ment rather than specific behavioral or psychiatric symptoms.CGAS scores range from 1 to 100, with scores .70 representingnormal functioning and scores of #70 indicating the need forclinical services.25 The CGAS has been found to be associated withmeasures of child social and academic competence, making it auseful complement to behavior checklists. The CGAS has beenfound to have acceptable interrater and test-retest reliability anddiscriminant validity.6,25
RESULTS
Comparison of Abused and Nonabused GroupsThe responses of the abused and nonabused sub-
jects on each behavior scale were compared using2 3 2 (abuse status 3 gender) ANOVA models. Tocompensate for the large number of comparisons,a was set at .01, with the exception of comparisonsinvolving fathers in which missing data resulted ina loss of power, and thus, a was maintained at thecustomary .05 level (see Table 1). A significantdifference was found between abused and non-abused groups on all eight of the subscales (With-drawn, Somatic Complaints, Anxious Depressed,Social Problems, Thought Problems, AttentionProblems, Delinquent Behavior, and Aggressive
Behavior) as rated by mothers. In each case, theabused subjects exhibited a greater degree of be-havior problems than the nonabused subjects. Theabused subjects also had significantly higherscores on the broad-band Internalizing, External-izing, and Total Problem scales. Paternal reportsrated abused adolescents as significantly higher onthe Internalizing, Externalizing, and Total Problemscales, as well as on all other subscales except theSomatic Complaints subscale. A comparison basedon self-reports revealed that abused adolescentsrated themselves significantly higher on the With-drawn, Thought Problems, Delinquent Behavior,and Aggressive Behavior subscales, and the TotalProblem and Externalizing scales, than did non-abused adolescents. Similar to the reports of moth-ers, teachers rated abused adolescents significantlyhigher on all eight of the cross-informant subscalesand on the Internalizing, Externalizing, and TotalProblem scales. There were no significant genderdifferences or group 3 gender interactions for anyscale or subscale that was rated by any of the fourinformants.
Cross-Informant AnalysisBivariate correlations for the combined sample
were calculated to examine the agreement betweeneach pair of informants’ scores. Furthermore, a seriesof repeated measures ANOVA (RMANOVA) wereconducted with the informant as the repeated factorand group status (abused/nonabused) as the be-tween-group factor. The interaction between abusestatus and informant was examined in eachRMANOVA to determine whether the degree ofagreement among informants’ ratings changed as afunction of abuse status. The main effects for raterand group in the RMANOVA were not examined forthe purposes of the present study, because a largernumber of subjects were available in the univariatemodels. In an effort to maximize the usable data,informants were compared 2 informants at a time,rather than all 4 simultaneously. For purposes ofthese analyses, the a level was set at .01 for theinteraction term.
Agreement among informants was highest formothers and fathers with bivariate correlations of .68for the Internalizing scale and .72 for the Externaliz-ing scale. Agreement among the reports of parentsand adolescents was somewhat lower. The correla-tion between the reports of mothers and adolescentswas .30 for the Internalizing scale and .49 for theExternalizing scale, whereas father-adolescent corre-lations were .29 and .46, respectively. Similar levelsof agreement were found between parent andteacher reports. Agreement was lowest for the re-ports of adolescents and teachers with correlations of.23 for the Internalizing scale and .34 for the Exter-nalizing scale.
Comparisons of the reports of mothers and fatherson the CBCL revealed no interaction between infor-mant and abuse status on any of the scales or sub-scales. Similarly, comparisons between fathers’ re-ports (CBCL) and adolescents’ reports (YSR), as wellas comparisons between each of the parents’ reports
ARTICLES 45 by on October 5, 2005 www.pediatrics.orgDownloaded from
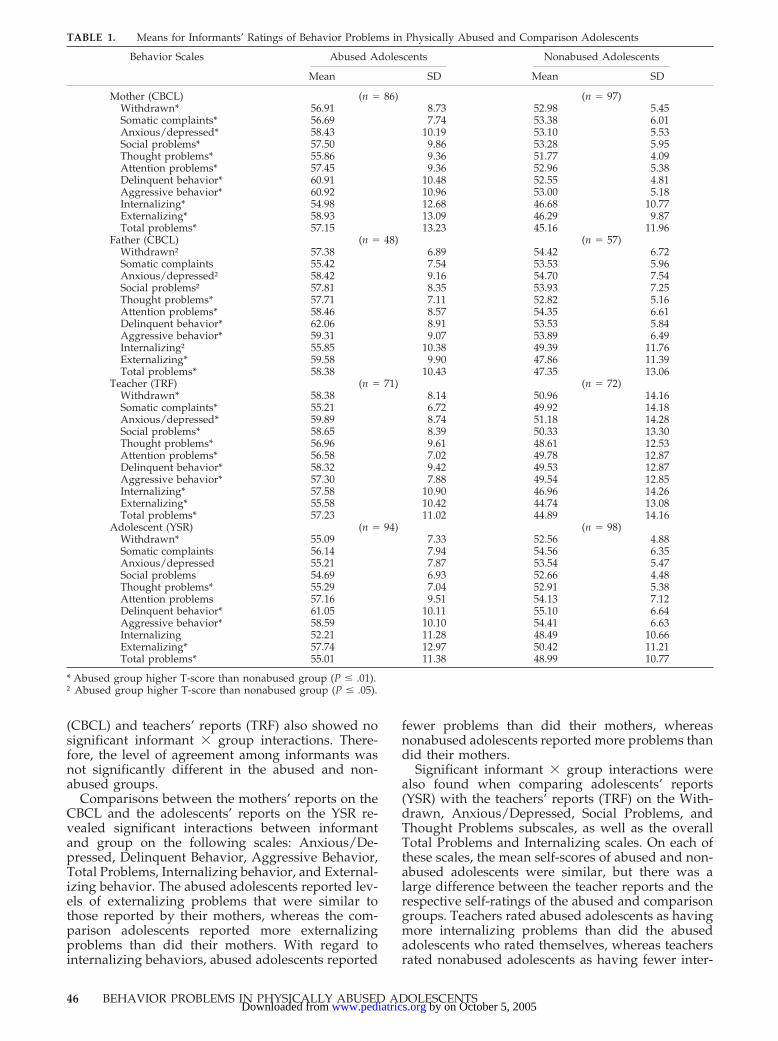
(CBCL) and teachers’ reports (TRF) also showed nosignificant informant 3 group interactions. There-fore, the level of agreement among informants wasnot significantly different in the abused and non-abused groups.
Comparisons between the mothers’ reports on theCBCL and the adolescents’ reports on the YSR re-vealed significant interactions between informantand group on the following scales: Anxious/De-pressed, Delinquent Behavior, Aggressive Behavior,Total Problems, Internalizing behavior, and External-izing behavior. The abused adolescents reported lev-els of externalizing problems that were similar tothose reported by their mothers, whereas the com-parison adolescents reported more externalizingproblems than did their mothers. With regard tointernalizing behaviors, abused adolescents reported
fewer problems than did their mothers, whereasnonabused adolescents reported more problems thandid their mothers.
Significant informant 3 group interactions werealso found when comparing adolescents’ reports(YSR) with the teachers’ reports (TRF) on the With-drawn, Anxious/Depressed, Social Problems, andThought Problems subscales, as well as the overallTotal Problems and Internalizing scales. On each ofthese scales, the mean self-scores of abused and non-abused adolescents were similar, but there was alarge difference between the teacher reports and therespective self-ratings of the abused and comparisongroups. Teachers rated abused adolescents as havingmore internalizing problems than did the abusedadolescents who rated themselves, whereas teachersrated nonabused adolescents as having fewer inter-
TABLE 1. Means for Informants’ Ratings of Behavior Problems in Physically Abused and Comparison Adolescents
Behavior Scales Abused Adolescents Nonabused Adolescents
Mean SD Mean SD
Mother (CBCL) (n 5 86) (n 5 97)Withdrawn* 56.91 8.73 52.98 5.45Somatic complaints* 56.69 7.74 53.38 6.01Anxious/depressed* 58.43 10.19 53.10 5.53Social problems* 57.50 9.86 53.28 5.95Thought problems* 55.86 9.36 51.77 4.09Attention problems* 57.45 9.36 52.96 5.38Delinquent behavior* 60.91 10.48 52.55 4.81Aggressive behavior* 60.92 10.96 53.00 5.18Internalizing* 54.98 12.68 46.68 10.77Externalizing* 58.93 13.09 46.29 9.87Total problems* 57.15 13.23 45.16 11.96
Father (CBCL) (n 5 48) (n 5 57)Withdrawn† 57.38 6.89 54.42 6.72Somatic complaints 55.42 7.54 53.53 5.96Anxious/depressed† 58.42 9.16 54.70 7.54Social problems† 57.81 8.35 53.93 7.25Thought problems* 57.71 7.11 52.82 5.16Attention problems* 58.46 8.57 54.35 6.61Delinquent behavior* 62.06 8.91 53.53 5.84Aggressive behavior* 59.31 9.07 53.89 6.49Internalizing† 55.85 10.38 49.39 11.76Externalizing* 59.58 9.90 47.86 11.39Total problems* 58.38 10.43 47.35 13.06
Teacher (TRF) (n 5 71) (n 5 72)Withdrawn* 58.38 8.14 50.96 14.16Somatic complaints* 55.21 6.72 49.92 14.18Anxious/depressed* 59.89 8.74 51.18 14.28Social problems* 58.65 8.39 50.33 13.30Thought problems* 56.96 9.61 48.61 12.53Attention problems* 56.58 7.02 49.78 12.87Delinquent behavior* 58.32 9.42 49.53 12.87Aggressive behavior* 57.30 7.88 49.54 12.85Internalizing* 57.58 10.90 46.96 14.26Externalizing* 55.58 10.42 44.74 13.08Total problems* 57.23 11.02 44.89 14.16
Adolescent (YSR) (n 5 94) (n 5 98)Withdrawn* 55.09 7.33 52.56 4.88Somatic complaints 56.14 7.94 54.56 6.35Anxious/depressed 55.21 7.87 53.54 5.47Social problems 54.69 6.93 52.66 4.48Thought problems* 55.29 7.04 52.91 5.38Attention problems 57.16 9.51 54.13 7.12Delinquent behavior* 61.05 10.11 55.10 6.64Aggressive behavior* 58.59 10.10 54.41 6.63Internalizing 52.21 11.28 48.49 10.66Externalizing* 57.74 12.97 50.42 11.21Total problems* 55.01 11.38 48.99 10.77
* Abused group higher T-score than nonabused group (P # .01).† Abused group higher T-score than nonabused group (P # .05).
46 BEHAVIOR PROBLEMS IN PHYSICALLY ABUSED ADOLESCENTS by on October 5, 2005 www.pediatrics.orgDownloaded from

nalizing behavior problems than did nonabused ad-olescents who rated themselves.
Comparison of CGAS and Clinically ElevatedAchenbach Scores
The median CGAS rating for the abuse group was68.0 (interquartile range [IQR] 5 55.0–80.0), whereasthe median rating for the nonabused subjects was 90(IQR 5 80.0–92.0). The difference between thegroups was significant, Mann-Whitney U Test; z 58.10; P , .0001.
An additional validation of the greater functionalimpairment in abused adolescents is provided by anexamination of the number of Achenbach behaviorchecklist subscales for each group designated as clin-ically elevated, defined as T scores .63.22 x2 analyseswere used to determine whether abused adolescentsreceived scores falling within the clinically elevatedrange more frequently. Significantly more abusedadolescents received clinically elevated scores on theInternalizing, Externalizing, and Total Problemscales of the CBCL as completed by mothers and theTRF as completed by teachers than did nonabusedadolescents (see Table 2).
Likewise, adolescents’ self-reports on the YSR re-vealed that significantly more abused adolescentsrated themselves within the clinically elevated rangeon all three scales. The fathers of abused subjectsmore often rated their adolescents within the clinicalrange on the Externalizing scale than did the fathersof nonabused adolescents.
DISCUSSIONThe results indicate that physically abused adoles-
cents, compared with nonabused adolescents, exhibitinternalizing and externalizing behavior problemsregardless of which adult informant rated the ado-lescents’ behavior, supporting previous researchdocumenting a significant association between phys-ical abuse and problems including anxiety, depres-sion, and aggressive behavior.26,27 The internalizingand externalizing behaviors exhibited by abused ad-olescents were severe enough to fall within the clin-
ical range of both the CBCL and the interviewer-rated CGAS. Clinical ranges for these measures weredeveloped based on the scores of children referredfor mental health services, indicating that the prob-lems experienced by abused adolescents were severeenough to warrant intervention. Although findingproblem behaviors in abuse victims is certainly notsurprising, it is important to note that in the presentstudy, these behaviors were detected in a group ofmiddle-class, white adolescents who had not gener-ally experienced severe, life-threatening abuse. Thissuggests that without the additional risk factorsfound in abuse studies of younger, more socioeco-nomically deprived groups, being raised in a house-hold in which even mild abuse occurs is associatedwith both internalizing and externalizing problems.
The finding that abused adolescents rated them-selves as having significantly more externalizingbehaviors than nonabused adolescents was un-expected, because these behaviors are often underre-ported by children on self-report measures.7,28 It ispossible that the adolescents in the present study,because they were somewhat older than subjects inprevious studies, were less likely to attempt to con-ceal their externalizing behaviors. It is also possiblethat children reared in the presence of frequent vio-lence are less likely to perceive aggression as inap-propriate and are therefore more likely to acknowl-edge openly their own aggressive and delinquentbehavior.
In contrast to the relatively high level of agreementamong informants concerning externalizing behav-ior problems, abused adolescents reported fewer in-ternalizing behaviors than did the adult informants.In addition, compared directly with nonabused ad-olescents, they reported having more problems ononly one of the internalizing subscales (Withdrawn),but they did not report more problems on the Anx-ious/Depressed and Somatic Complaints subscalesor on the overall Internalizing scale. The finding thatabused adolescents reported fewer internalizingproblems was unexpected for several reasons. Asnoted in the introduction, previous research has in-dicated that physical abuse is strongly related todepressive symptoms, and children and adolescentsgenerally report more internalizing symptoms thando their parents.
It might be argued that abused adolescents pro-vided accurate self-reports of internalizing problemsand that parents of abused adolescents were some-how biased in their ratings. However, in such a case,significant informant 3 abuse status interactionswould be expected. For example, if abuse groupparents were biased, their level of agreement withteachers would probably differ from that of non-abuse group parents. However, no informant 3abuse interactions were found for any of the combi-nations of adult informants. These findings support arecent report of the absence of an abuse 3 informantinteraction between the reports of mothers andteachers of abused children3 but contradict previousreports that the reports of parents of abuse victimsmay be biased in their view of their children’s be-havior.11,12
TABLE 2. Percentage of Clinically Elevated Ratings of Behav-ior Problems by Abuse Status
Behavior Scales Abuse Group Nonabused x2†
Mother (CBCL) (n 5 86) (n 5 86)Internalizing 22 8 6.95**Externalizing 38 3 35.90***Total problems 31 6 19.60***
Father (CBCL) (n 5 48) (n 5 57)Internalizing 21 14 .85Externalizing 27 9 6.15**Total problems 29 14 3.60
Teacher (TRF) (n 5 71) (n 5 68)Internalizing 28 7 11.16***Externalizing 20 3 10.32***Total problems 25 1 17.82***
Adolescent (YSR) (n 5 90) (n 5 94)Internalizing 13 4 4.74*Externalizing 33 8 18.25***Total problems 20 6 8.41**
* P , .05; ** P , .01; *** P , .001.† df 5 1.
ARTICLES 47 by on October 5, 2005 www.pediatrics.orgDownloaded from

Assuming that the reports of parents and teachersreflect genuine internalizing problems in abused ad-olescents, it would be helpful to understand whyabused adolescents unexpectedly did not reportthese problems. It is possible that abuse may lead todifficulty labeling feelings and emotions, which hassome support from developmental literature.29 It isalso possible that adolescents with high levels ofexternalizing behaviors, such as those found in ourabused group, are less aware of, or less likely toreport, internalizing symptoms. Herkov and Myers,30
using Minnesota Multiphasic Personality Inventoryprofiles, reported that depressed adolescents exhib-ited higher elevations on scales associated with de-pression than did adolescents with comorbid depres-sion and conduct disorder and concluded that thepresence of conduct disorder may result in adoles-cents reporting fewer symptoms of depression. Itmight also be argued that the YSR is not particularlysensitive to anxious or depressive behaviors. How-ever, the Anxious/Depressed subscale was sensitiveto behaviors of the nonabused adolescents (they re-ported more anxious/depressed behaviors than didtheir parents or teachers), indicating that the relativeabsence of reports of these problems by abused ad-olescents compared with parents and teachers maybe attributable to actual underreporting of problemsrather than to insensitivity of the instrument.
This is one of the few papers investigating thebehavioral correlates of abuse that reports on thefathers’ perceptions of their abused adolescent. Con-sidering the common view that fathers in abusivefamilies are less attentive to the distress experiencedby their children, it is intriguing that fathers gener-ally described their child in a manner similar to thatof mothers and teachers on internalizing scales. Wehave found that, in contrast to mothers, fathers in oursample are viewed by their abused children as fallinginto the category of “affectionless control.”31 Thiscategory describes parents who deal with their chil-dren in a manner that is emotionally cold as well asoverprotective.32 One might expect that the lack of aparent–adolescent emotional bond, coupled withperceived excessive paternal control, would be asso-ciated with inaccurate paternal descriptions of ado-lescents’ behavior. However, fathers’ ratings of theirabused adolescent’s behavior were similar to those ofother adult informants. This suggests that the fa-thers’ awareness of their adolescent’s behavior is astrength that may be useful in attempting to engagethem in therapeutic efforts to improve the father–adolescent relationship. However, one should usecaution in generalizing these results to fathers in allphysically abusive families because only about halfof the fathers in our abuse sample completed theparent rating forms. Because fathers were not con-tacted if doing so presented a risk of harm to theadolescent, it is likely that the most severely abusivefathers are underrepresented by this group.
Although the abuse group in the present investi-gation is one that is unique and generally under-studied, we understand that utilization of an all-white suburban sample may have yielded differentestimates of the association between adolescent
abuse and behavior and different degrees of agree-ment among informants, than would be found inother studies sampling from among minority youthor from urban settings. Therefore, the generalizabil-ity of our results to all abused adolescents may belimited. To assess properly the mental health needsof all physically abused adolescents, it is necessary toconduct similarly rigorous behavioral assessment re-search with other groups. In addition, cross-sectionalstudies such as this cannot establish a causal rela-tionship between physical abuse and adolescent be-havior. Longitudinal studies examining abuse, fam-ily variables, and subsequent behavior are needed toexamine the complex relationships among these fac-tors. Future studies should also attempt to examinerater agreement between perpetrators and nonperpe-trators of abuse to determine influence of perpetratorstatus on parents’ perception of their children. Un-fortunately, our sample sizes were not adequate toperform such an analysis.
Overall, physical abuse was related to both in-creased internalizing and externalizing behaviorproblems and increased impairment in daily func-tioning. The varied types of problems exhibited byabused adolescents affirm the need for routinescreening by pediatricians in collaboration with men-tal health professionals for possible maltreatment. Inaddition, appropriate mental health services areneeded urgently to serve abused youth. Our resultsindicate that even mild to moderate levels of physicalinjury from abuse are associated with behavior prob-lems severe enough to warrant mental health ser-vices. Because abused adolescents often reportedfewer depressive symptoms compared with ratingsby adult informants, assessment of these youth isenhanced by having a parent or teacher as an addi-tional informant when using behavior checklists.Screening by pediatricians and access to mentalhealth services will not only address abused teenag-ers’ current behavioral and emotional disorders butwill also be important in interrupting the well-known risk for transmission of abusive behavior tothe next generation.
ACKNOWLEDGMENTSThis work was supported by National Institute of Mental
Health Grant 5-RO1-MH43772.We thank the Schott Foundation for its support of our family
violence research efforts, including the funding, in part, of thisstudy.
REFERENCES1. Department of Health and Human Services. Children’s Bureau. Child
Maltreatment 1996: Reports From the States to the National Child Abuse andNeglect Data System. Washington, DC: US Government Printing Office;1998
2. Feldman RS, Salzinger S, Rosario M, Alvarado L, Caraballo L, HammerM. Parent, teacher, and peer ratings of physically abused and nonmal-treated children’s behavior. J Abnorm Child Psychol. 1995;23:317–334
3. Kinard EA. Mother and teacher assessments of behavior problems inabused children. J Am Acad Child Adolesc Psychiatry. 1995;34:1043–1053
4. Sternberg KJ, Lamb ME, Greenbaum C, et al. Effects of domestic vio-lence on children’s behavior problems and depression. Dev Psychol.1993;29:44–52
5. Kravic JN. Behavior problems and social competence of clinic-referredabused children. J Fam Violence. 1987;2:111–120
6. Weissman MM, Warner V, Fendrich M. Applying impairment criteria to
48 BEHAVIOR PROBLEMS IN PHYSICALLY ABUSED ADOLESCENTS by on October 5, 2005 www.pediatrics.orgDownloaded from

children’s psychiatric diagnosis. J Am Acad Child Adolesc Psychiatry.1990;29:789–795
7. Sawyer GS, Baghurst P, Mathias J. Differences between informantsreports describing emotional and behavioral problems in communityand clinic-referred children: a research note. J Child Psychol Psychiatr.1992;33:441–449
8. Mokros HB, Poznanski E, Grossman JA, Freeman LN. A comparison ofchild and parent ratings of depression for normal and clinically referredchildren. J Child Psychol Psychiatr. 1987;28:613–627
9. Christenson A, Margolin G, Sullaway M. Interparental agreement onchild behavior problems. Psychol Assess. 1992;4:419–425
10. Kolko DJ, Kazdin AE. Emotional/behavioral problems in clinic andnonclinic children: correspondence among child, parent, and teacherreports. J Child Psychol Psychiatr. 1993;34:991–1006
11. Reid JB, Kavanaugh K, Baldwin DV. Abusive parents’ perceptions ofchild problem behaviors: an example of parental bias. J Abnorm ChildPsychol. 1987;15:457–466
12. Mash EJ, Johnson C, Kovitz K. A comparison of the mother-childinteractions of physically abused and nonabused childen during playand task situations. J Clin Child Psychol. 1983;12:337–346
13. Kaplan S, Pelcovitz D, Salzinger S, Mandel F, Weiner M. Adolescentphysical abuse and suicide attempts. J Am Acad Child Adolesc Psychiatry.1997;36:799–808
14. Kaplan S, Pelcovitz P, Salzinger S, et al. Adolescent physical abuse: riskfor adolescent psychiatric disorders. Am J Psychiatry. 1998;155:954–959
15. Garbarino J, Schellenbach C, Sebes J. Troubled Youth, Troubled Families:Understanding Families at Risk for Adolescent Maltreatment. New York,NY: Aldine Publishing Co; 1986
16. Wechsler D. Manual for the Wechsler Intelligence Scale for Children, Revised.San Antonio, TX: The Psychological Corp; 1974
17. Wechsler D. Manual for the Wechsler Adult Intelligence Scale, Revised. SanAntonio, TX: The Psychological Corp; 1981
18. Straus M. Measuring intrafamily conflict and violence: the conflicttactics scale. J Marriage Fam. 1979;41:75–88
19. Achenbach TM. Manual for the Child Behavior Checklist/4–18 and 1991Profile. Burlington, VT: University of Vermont Department ofPsychiatry; 1991
20. Achenbach TM. Manual for the Youth Self-Report and 1991 Profile. Burl-ington, VT: University of Vermont, Department of Psychiatry; 1991
21. Achenbach TM. Manual for the Teacher’s Report Form and 1991 Profile.Burlington, VT: University of Vermont Department of Psychiatry; 1991
22. Achenbach TM. Integrative Guide to the 1991 CBCL, YSR, and TRF Profiles.Burlington, VT: University of Vermont Department of Psychiatry; 1991
23. Shaffer D, Gould MS, Brasic J, et al. A children’s global assessment scale(CGAS). Arch Gen Psychiatry. 1983;40:1228–1231
24. Endicott J, Spitzer R, Fleiss J, Cohen J. The Global Assessment Scale: Aprocedure for measuring overall severity of psychiatric disturbance.Arch Gen Psychiatry. 1976;33:766–771
25. Bird HR, Canino G, Rubio-Stipec M, Ribera JC. Further measures of thepsychometric properties of the children’s global assessment scale. ArchGen Psychiatry. 1987;44:821–824
26. Weiss B, Dodge KA, Bates, JE, Pettit GS. Some consequences of earlyharsh discipline: child aggression and a maladaptive social informationprocessing style. Child Dev. 1992;63:1321–1335
27. Flisher AJ, Kramer RA, Hoven CW, et al. Psychosocial characteristics ofphysically abused children and adolescents. J Am Acad Child AdolescPsychiatry. 1997;36:123–131
28. Stanger C, Lewis M. Agreement among parents, teachers, and childrenon internalizing and externalizing behavior problems. J Clin Child Psy-chol. 1993;22:107–115
29. Cicchetti D. How research on child maltreatment has informed thestudy of child development: perspectives from developmental psycho-pathology. In: Cicchetti D, Carlson V, eds. Child Maltreatment: Theory andResearch on the Causes and Consequences of Child Abuse and Neglect. NewYork, NY: Cambridge University Press; 1989:377–431
30. Herkov MJ, Myers WC. MMPI profiles of depressed adolescents withand without conduct disorder. J Clin Psychol. 1996;52:705–710
31. Parker GB, Barrett EA, Hickie IB. From nurture to network: examininglinks between perceptions of parenting received in childhood and socialbonds in adulthood. Am J Psychiatry. 1992;149:877–885
32. Pelcovitz D, Kaplan SJ, Salzinger, S., Ellenberg, A, Mandel F. Adolescentphysical abuse: adolescents’ perceptions of family functioning and ageat time of abuse. J Fam Violence. In press
PRESCHOOL VISION SCREENING
ConclusionsThere is a lack of good quality research into the natural history of the target
conditions, the disabilities associated with them, and the efficacy of availabletreatments. This evidence is essential to support a screening program for a nonfatalcondition for which there have been no rigorously controlled trials. An invitationto preschool vision screening carries with it the implicit assumption that screeningis going to benefit the child. In the absence of sound evidence that the targetconditions sought in these programs are disabling and that the interventionsavailable to correct them do more good than harm, the ethical basis for suchinterventions is very weak.
RecommendationsClinical PracticePurchasers and providers are advised not to implement new preschool vision
screening programs unless they have been rigorously evaluated.
Snowdon SK, Stewart-Brown SL. Preschool vision screening. Health Technol Assessment. 1997;1(8)
ARTICLES 49 by on October 5, 2005 www.pediatrics.orgDownloaded from

DOI: 10.1542/peds.104.1.43 1999;104;43-49 Pediatrics
Mandel and Merrill Weiner Sandra J. Kaplan, Victor Labruna, David Pelcovitz, Suzanne Salzinger, Francine
Comparison of Informants' ReportsPhysically Abused Adolescents: Behavior Problems, Functional Impairment, and
This information is current as of October 5, 2005
& ServicesUpdated Information
http://www.pediatrics.org/cgi/content/full/104/1/43including high-resolution figures, can be found at:
References
http://www.pediatrics.org/cgi/content/full/104/1/43#BIBLat: This article cites 22 articles, 5 of which you can access for free
Subspecialty Collections
tryhttp://www.pediatrics.org/cgi/collection/neurology_and_psychia
Neurology & Psychiatryfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.pediatrics.org/misc/Permissions.shtmltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://www.pediatrics.org/misc/reprints.shtml
Information about ordering reprints can be found online:
by on October 5, 2005 www.pediatrics.orgDownloaded from





























