Embed Size (px)
Citation preview

Social Difficult ies Influence Group PsychotherapyAdherence in Abused, Suicidal African American Women
m
Dawn L. IlardiEmory University and Children’s Healthcare of Atlanta
m
Nadine J. KaslowEmory University School of Medicine
The social brain model emphasizes improving our understanding of
the relational factors that influence treatment adherence. Consistent
with this framework, which has been applied to medical adherence,
it was hypothesized that insecure attachment styles, interpersonal
hassles, and low levels of social support would explain group
psychotherapy attendance. Results from 51 abused and suicidal
low-income, African American women who attended at least 1
session of an empowerment group psychotherapy indicated that
lower attendance was related to (a) insecure attachment styles
(fearful) and (b) interpersonal hassles (perceived social differences,
lack of social acceptability, social victimization). Perceived social
support did not predict group therapy attendance. The value of
addressing attachment styles and interpersonal factors to enhance
treatment participation is underscored. & 2009 Wiley Periodicals, Inc.
J Clin Psychol 65: 1300–1311, 2009.
Keywords: social difficulties; group therapy; adherence; attachment;
abused and suicidal African American women
The factors that influence treatment adherence are dynamic and complex.Researchers have begun defining variables to improve adherence to medical andpsychological treatments. Within medicine, four models explain adherence problems(Wamboldt, 2005): silver bullet, DSM symptom checklist, biopsychosocial brain,and social brain. This study is grounded in the latter theory: the social brain modelthat hypothesizes that all humans are innately driven to create and maintain
This research was funded by a grant from the Centers for Disease Control and Prevention, NationalCenter for Injury Prevention and Control: R49CCR421767-02 entitled ‘‘Group interventions with abused,suicidal African American women’’ awarded to the last author (Kaslow).
Correspondence concerning this article should be addressed to: Nadine J. Kaslow, Emory UniversitySchool of Medicine, Department of Psychiatry and Behavioral Sciences, Grady Health System, 80 JesseHill Jr Drive NE, Atlanta, GA 30303; e-mail: [email protected]
JOURNAL OF CLINICAL PSYCHOLOGY, Vol. 65(12), 1300--1311 (2009) & 2009 Wiley Periodicals, Inc.Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10 .1002/ jc lp .20628

relationships and that brain function determines and structures an individual’spersonal and social experience (Bakker et al., 2002; Wamboldt, 2005). According tothis latter model, building a positive patient-provider relationship is key toimproving treatment adherence (Beach, Keruly, & Moore, 2006; Fuertes et al.,2007; Sajatovic, Bauer, Kilbourne, Vertrees, & Williford, 2006; Wamboldt, 2005;Zeber et al., 2008). Within psychology, the social brain model can be used tounderstand factors that interfere with a person’s ability to follow through with theprescribed treatment.A number of studies highlight how social and relational factors influence
treatment follow-through with medically ill persons. Among HIV positive AfricanAmerican women, family support and having young children increase medicationadherence and relationship problems and perceived stigma reduce such adherence(Edwards, 2006). In patients with diabetes, an insecure attachment style is related tolower medication adherence and a poor patient-provider relationship (Ciechanowski,Katon, Russo, & Walker, 2001). Interventions have begun targeting family relationsto improve adherence in families of medically ill persons (Baucom et al., 2008; Scott,Halford, & Ward, 2004).Unfortunately, the investigations on psychotherapy adherence have not been
theoretically driven. However, social and relational factors that influence psycho-logical treatment adherence identified across modalities and populations include notliving alone (Ayuso-Mateos et al., 2007; Jackson, Booth, McGuire, & Salmon, 2006)and patient collaboration in treatment decision-making (Loh, Leonhart, Wills,Simon, & Harter, 2007). Person-specific relational styles differentially predictadherence, with borderline personality characteristics positively predicting atten-dance and antisocial personality characteristics negatively predicting attendance(Hilsenrath, Holdwick, Castelbury, & Blais, 1998).In terms of group therapy, social and relational factors are key to therapeutic
engagement. The relationship between the patient and therapist at the initial contactis a strong predictor of treatment engagement (Prado, Pantin, Schwartz, Lupei,& Szapocznik, 2006). Stronger therapeutic alliances correlate with higher attendancerates (Johnson, Penn, Bauer, Meyer, & Evans, 2008). Group processes, such asgroup cohesion, predict retention (Prado et al., 2006) and moderate the link betweenparticipant age and treatment compliance (Ogrodniczuk, Piper, & Joyce, 2006b).In addition, patient specific social factors are important. Patient reports of relationalconflict (i.e., roommate difficulties, fighting with intimate partner), angry hostility,and social introversion or inhibition relate to lower attendance (MacNair-Semands,2002; MacNair & Corazzini, 1994). Patients’ perceived interpersonal distressnegatively relates to participation in supportive group therapy for adults withpersonality disorders (Ogrodniczuk, Piper, & Joyce, 2006a). Finally, individuals withsocial problems, such as social phobia, are less adherent to treatment and feel lessintegrated with members of their group (Terra et al., 2006). In summary, factorsspecific to the therapist, group members, and patient impact initial and ongoingengagement in psychotherapy, and this is consistent with the social brain model.The purpose of the current study is to investigate the use of the social brain model to
identify factors that contribute to poor group therapy attendance in a population ofindividuals likely to manifest social and relational problems, namely, low-income,abused, and suicidal African American women. This topic is important because drop-out and treatment non-engagement are significant challenges in this population. Themajority of abused women have fearful or preoccupied attachments, which along withemotional dependency makes separating from their abuser quite challenging (Bornstein,
1301Social Difficulty and Group Therapy Adherence
Journal of Clinical Psychology DOI: 10.1002/jclp

2006; Henderson, Bartholomew, & Dutton, 1997; Henderson, Bartholomew, Trinke, &Kwong, 2005). Abused women have impaired levels of social support and often arereluctant to ask members of their social support network for assistance (Levendoskyet al., 2004). However, social support protects these women from negative mentalhealth sequelae (Coker et al., 2002). In terms of suicidalilty, although no literaturecould be found to link attachment styles and suicidal behavior in adults,preoccupied/fearful attachment is a stable vulnerability factor for adult depression(Haaga et al., 2002), which is a risk factor for suicidality. In adolescents, severityof suicidal ideation is positively correlated with fearful and preoccupied attachmentstyles (Adams, Sheldon-Keller, & West, 1996; Lessard & Moretti, 1998). Further,life hassles, including interpersonal hassles, is independently a significant socialvariable that predicts suicide attempts among low-income, African Americans(Kaslow et al., 2005). In addition, one key social process associated with suicidalbehavior among African American women is a low level of perceived support(Vanderwerker et al., 2007); social support buffers abused, low-income AfricanAmerican women from attempting suicide (Kaslow et al., 1998; Kaslow et al., 2002).Additional social processes relevant in this community include high rates of intimatepartner violence (IPV), relationship discord, and child maltreatment; as well as lowlevels of family strengths and family adaptability and cohesion (Compton,Thompson, & Kaslow, 2005; Kaslow, Thompson, Brooks, & Twomey, 2000).African American women with a history of suicidal behavior and childhoodmaltreatment exhibit maladaptive relational behaviors including egocentricity, socialincompetence, high levels of alienation, and poor self-other differentiation (Twomey,Kaslow, & Croft, 2000). These studies are only a few examples of how attachmentstyles, interpersonal hassles, and social support are connected to the mental health oflow-income minority individuals, including women with a history of abuse orsuicidal behavior.Taken together, the social brain model of adherence (Wamboldt, 2005) can be
used to elucidate the social and relational factors that interfere with grouppsychotherapy attendance. The current study investigated social and relationalvariables that interfere with group psychotherapy to identify variables that can betargeted to improve adherence in low-income African American women with ahistory of suicidal behavior and IPV. It was hypothesized that maladaptiveattachment styles, more interpersonal hassles or stressors, and lower levels ofperceived social support would predict lower group psychotherapy attendance.
Method
Participants
The current sample is part of a larger study (n5 112) designed to evaluate aculturally competent intervention group versus enhanced treatment as usual for low-income, abused, and suicidal African American women. From this total sample, only51 women participated in at least one group therapy session, and thus 61 womenwere not included despite the fact that they were randomized to the activeintervention condition. Participants were recruited after seeking care at a large urbancity hospital and all reported a history of IPV and a suicide attempt in the previousyear. Women were excluded only if they had significant cognitive impairments orwere unable to complete the protocol (i.e., acutely psychotic). The mean age was 34.5(SD5 8.78) years, mean number of children was 2.41, 43% were in a relationship,
1302 Journal of Clinical Psychology, December 2009
Journal of Clinical Psychology DOI: 10.1002/jclp

53% were homeless, 37% had less than 12 years of education, 85% wereunemployed, and 50% had an income of less than $250 a month.
Procedure
Participants were recruited when they presented for emergency services after asuicide attempt or injuries after IPV, and they were referred via pager to the studyPrincipal Investigator. Research team members also recruited women at thehospital’s medical walk-in clinics. For women who met inclusion criteria, anappointment was scheduled to complete a comprehensive battery of 26 measureswith a trained interviewer that included demographic information, risk factors andprotective factors (e.g., attachment and interpersonal problems, daily life hassles,lack of social support), and intervention targets (e.g., adaptive cognitive processes,personal coping skills, social and material resources). Measures were administeredverbally to account for low levels of functional literacy, which might confound studyvariables. After completion of the measures, women were given $20 andtransportation fare. Half of all women who participated in the assessment batterywere assigned randomly to participate in the 10-,session manualized group therapyintervention and the other half were assigned to enhanced treatment as usual.
Intervention Group
The 10-session weekly psychotherapy group, entitled the Grady Nia Project: Suicide/IPV Intervention, was supportive and psychoeducational, designed to be culturallycompetent, and developed in accord with the Triadic Theory of Influence (Daviset al., 2009). Sessions were manualized and covered the following topics: grouptherapy and group process, introduction and commitment to safety, suicide and IPVeducation, and safety planning. In addition, sessions targeted reducing risk factorsand enhancing protective factors in three domains: intrapersonal, social andsituational, and cultural and environmental. The 10th session was a review andfocused on termination. Two females led the groups: one African American therapistand at least one therapist with advanced clinical training and experience.Participants also were given community referrals, other material resources asneeded, and tokens for public transportation to and from all intervention groupsessions to facilitate attendance given economic barriers.
Measures
Dependent variable. The dependent variable was group psychotherapyattendance and was coded as the number of sessions that the woman attended.
Independent variables. There were three independent variables: attachmentstyles, interpersonal hassles, and perceived social support. Thus, only the measuresused to tap these constructs are described. Attachment styles were measured via theRelationship Style Questionnaire (RSQ; Griffin & Bartholomew, 1994), a 30-itemscale used to measure self-reported relationship style or attachment patterns. Theitems are scored on a 5-point scale and total scores are obtained for four subscales(secure, fearful, preoccupied, dismissing). The RSQ has moderate to high internalconsistency and test-retest reliability as well as solid construct and convergentvalidity (Scharfe & Bartholomew, 1994; Waldinger, Schulz, Barsky, & Ahern, 2006).Internal consistency reliability for the current sample was moderately high (a5 .70).Interpersonal hassles were explored with the Survey of Recent Life Experiences
1303Social Difficulty and Group Therapy Adherence
Journal of Clinical Psychology DOI: 10.1002/jclp

(SRLE; Kohn & Macdonald, 1992), a 51-item scale that measures subjectiveexperiences of everyday stress and life hassles. Factors of interest to the current studyincluded social and cultural difficulties, social acceptability, and social victimization.Items are scored on a 4-point likert scale and total scores range from 51 to 204, withhigher scores indicating higher levels of stress. The internal consistency reliability forthe scale has been found to be high, including in the current sample, (a5 .70) and themeasure has strong construct and convergent validity (de Jong, Timmerman,& Emmelkamp, 1996; Harrington, Crowther, Henrickson, & Mickelson, 2006; Kohn& Macdonald, 1992). Perceived social support was assessed using the 12-itemMultidimensional Scale of Perceived Social Support (MSPSS; Zimet, Dahlem,Zimet, & Farley, 1988) that examines an individual’s perception of the social supportas received from family, friends, and significant others. Respondents rated on a5-point likert scale the degree to which they receive various types of instrumental andemotional support from family friends and significant others. The total score wasused. This MSPSS has solid internal consistency and test-retest reliability as well asconstruct and factorial validity (Dahlem, Zimet, & Walker, 1991; Zimet et al., 1988;Zimet, Powell, Farley, Werkman, & Berkoff, 1990), and, in this sample, had an alphaof .90.
Results
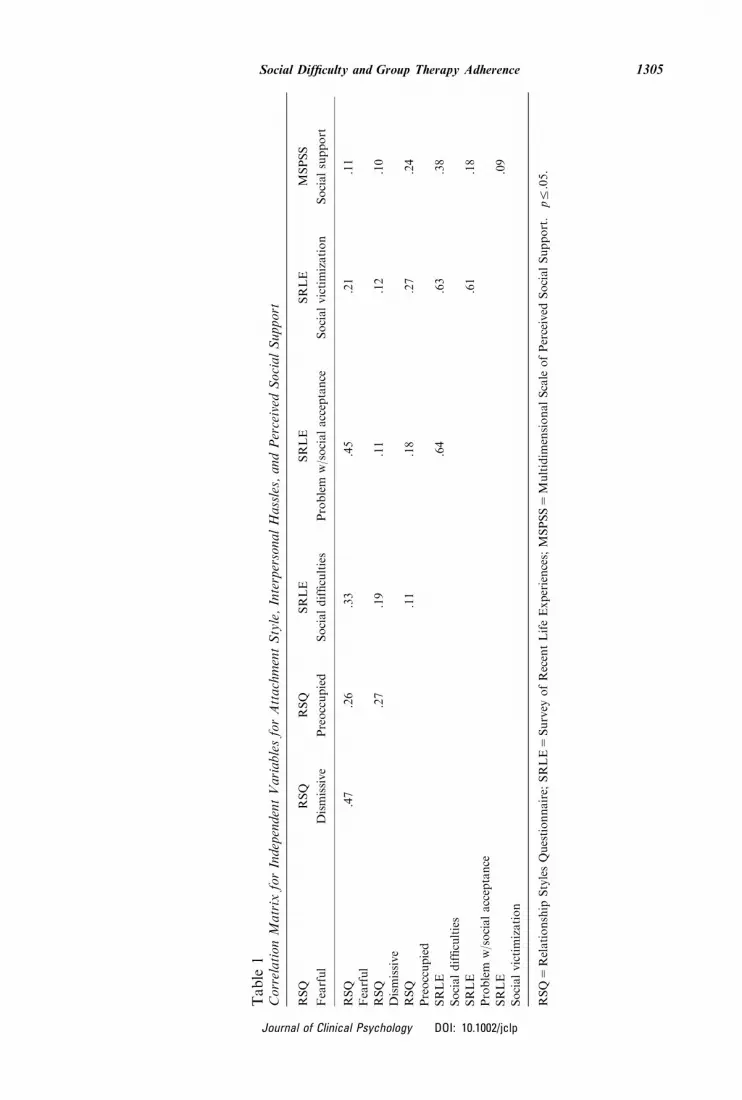
Descriptive statistics for the dependent and independent variables are as follows. Thenumber of group psychotherapy sessions attended ranged from 1 to 10 with a modeof 10 sessions (n5 21; M5 8.48, SD5 2.48). Group psychotherapy attendance waslog transformed due to significant skew. According to the RSQ, participants weremost likely to describe themselves as having a dismissive attachment style(M5 17.86, SD5 3.75), followed by fearful (M5 14.50, SD5 3.53) and preoccupied(M5 13.03, SD5 3.26) attachment styles. In terms of interpersonal hassles, socialdifficulties (M5 2.02, SD5 .66), problems with social acceptance (M5 2.28,SD5 .85), and social victimization (M5 2.53, SD5 .88) were similar across thesample. There was moderate variability across the sample for perceived socialsupport (M5 39.03, SD5 11.18). A correlation matrix for all independent variablescan be seen in Table 1. Fearful attachment style was the only attachment variablethat was correlated with interpersonal hassles, such that a more fearful style wasassociated with more social difficulties and problems with social acceptance.As expected, the subdomains of interpersonal hassles were positively interrelated.Unexpectedly, perceived social support and social difficulties were positivelycorrelated. However, this could be accounted for by the fact that greater supportmay lead to more opportunities for difficulties or that people who are sociallyisolated and, thus, have low social support actually have few social difficultiesbecause of the lack of such interaction.To test the main study hypothesis that a maladaptive attachment style, more
interpersonal hassles, and less perceived social support were predictive of poor grouptherapy attendance, hierarchical multiple regression was used. Results indicated thatattachment style (fearful, dismissive, preoccupied; F5 3.497, po.05) and inter-personal hassles (social difficulties, problems with social acceptance, and socialvictimization; F5 2.878, po.05), but not perceived social support (F5 1.61, p4.05),accounted for significant variability in group psychotherapy attendance. Morespecifically, attachment style and interpersonal hassles accounted for 24% of thevariance in psychotherapy attendance. Social support did not significantly predict
1304 Journal of Clinical Psychology, December 2009
Journal of Clinical Psychology DOI: 10.1002/jclp
Table
1CorrelationMatrix
forIndependentVariablesforAttachmentStyle,InterpersonalHassles,andPerceived
SocialSupport
RSQ
RSQ
RSQ
SRLE
SRLE
SRLE
MSPSS
Fearful
Dismissive
Preoccupied
Socialdifficulties
Problem
w/socialacceptance
Socialvictimization
Socialsupport
RSQ
.47�
.26
.33�
.45�
.21
.11
Fearful
RSQ
�.27
.19
.11
�.12
�.10
Dismissive
RSQ
.11
.18
.27
.24
Preoccupied
SRLE
.64�
.63�
.38�
Socialdifficulties
SRLE
.61�
.18
Problem
w/socialacceptance
SRLE
.09
Socialvictimization
RSQ
5Relationship
StylesQuestionnaire;
SRLE
5Survey
ofRecentLifeExperiences;MSPSS
5Multidim
ensionalScale
ofPerceived
SocialSupport.� p
r.05.
1305Social Difficulty and Group Therapy Adherence
Journal of Clinical Psychology DOI: 10.1002/jclp

attendance. With regard to incremental validity, adding interpersonal hassles to themodel after attachment style was not associated with significant improvement in theoverall model. In terms of unique predictors, the individual beta values revealed thatas symptoms of fearful attachment style increased, group psychotherapy attendancedecreased. See Table 2 for a summary of these results.
Discussion
The results from the current study partially support the hypothesis that social andrelational factors are associated with lower group psychotherapy attendance inabused, suicidal, and low-income African American women. Specifically, with thissample, findings indicated that lower attendance was related to maladaptiveattachment style, particularly the fearful type. In addition, interpersonal hassles,including perceived social differences, lack of social acceptability, and socialvictimization, were predictive of the women’s participation in group psychotherapy.However, contrary to predictions, perceived social support from friends and familywas not a significant predictor of group therapy attendance. Although bothattachment style and interpersonal hassles were independently predictive of grouppsychotherapy adherence, attachment style was the strongest independent predictor.In general, these findings are consistent with other research in accord with the socialbrain model, which reveals that relational processes affect medication adherence,psychotherapy attendance, and mental health in psychiatric/psychological patients(Ogrodniczuk et al., 2006a; Perry, Bond, & Roy, 2007), as well as medical patients(Ciechanowski et al., 2001; Edwards, 2006; Molloy, Perkins-Porras, Strike,& Steptoe, 2008; Palmer, Salcedo, Miller, Winiarski, & Arno, 2003).The relation between maladaptive attachment style and group psychotherapy
attendance is also consistent with the attachment literature, and it supports the useof attachment theory to inform group therapy practice (Flores, 2008). With regard tosuicidal and low-income African American women, many have a history of childmaltreatment and disrupted caregiver attachments (Kaslow, Thompson, Brookset al., 2000; Kaslow, Thompson, Meadows et al., 2000), which has been linked tomaladaptive relational behaviors, such as low levels of self-other differentiationand emotional involvement in relationships (Chance et al., 1996). Furthermore,the unique effects of a fearful attachment style more specifically have been
Table 2Attachment Style, Interpersonal Hassles, and Social Support Predict Group PsychotherapyAttendance
B (SE) b R2 adj DR2 adj
Attachment style .18� .25
Fearful �.005 (.05) �.435�
Dismissive �.001 (.002) �.048
Preoccupied .004 (.002) .317
Interpersonal hassles .24� .13
Social difficulties .005 (.015) �.073
Social acceptance �.022 (.011) �.425
Social victimization �.002 (.011) �.031
Social support �.001 (.003) �.048 .26 .11
�pr.05.
1306 Journal of Clinical Psychology, December 2009
Journal of Clinical Psychology DOI: 10.1002/jclp

associated with greater difficulty disengaging from the abusive relationship(Henderson et al., 1997). Thus, it is not surprising that abused women withrelational deficits had poorer adherence to a treatment that required building newrelationships (i.e., with therapists and group members).High levels of interpersonal hassles were also identified as problematic for group
psychotherapy attendance in this sample, although they did not explain a significantproportion of variance beyond that of attachment style. The correlation betweenspecific interpersonal hassles (e.g., social difficulties and lack of social acceptance)and fearful attachment style, however, helps elucidate the complexity of the relationbetween hassles and attendance, and it is consistent with the attachment research.Specifically, women with a fearful attachment style tend to have a negative view ofothers, demonstrate an avoidance approach of others, and are withdrawn andnondisclosing with others (Bartholomew & Horowitz, 1991). In other words, theinterpersonal hassles (e.g., perception of lack of social acceptance) associated with afearful attachment style reinforce problematic interpersonal patterns (e.g., avoidanceof relationships) and interfere with treatment adherence.Unlike person-specific variables described above, perceived social support did not
predict group therapy attendance in the current study. Interestingly, increased socialsupport was related to increased interpersonal hassles (i.e., social difficulty), whichsuggests that the functional quality of the social support these women received mayhave been negative (e.g., high in criticism). Social networks comprise structuralsupport (e.g., number of supporters available) and functional support (e.g.,assistance to obtain resources and emotional warmth), and the quality of thefunctional support has been associated with mental health status in abused women(Levendosky et al., 2004). Impaired social networks can be conceptualized as boththe antecedent and the consequence of interpersonal hassles among abused, suicidal,and low-income African American women. The reason why social support did notdirectly predict therapy attendance is unclear, but it raises the possibility of it being amoderator. For example, in a similar sample of suicidal African American women,social support moderated the relationship between partner abuse and suicidalbehavior (Kaslow et al., 1998). Social support may moderate, rather than directlylink, interpersonal hassles and group psychotherapy attendance.There are limitations to the current study that should be noted. The first set of
limitations pertains to the sample. The current sample size is relatively small. Inaddition, results of the current study can be generalized only to similar samples orlow-income African American women with a history of abuse and suicidal behavior.The second set of challenges with the study relates to measurement issues. Only self-report data were used to assess attachment style, interpersonal hassles, and perceivedsocial support. The lack of an interview method to examine attachment styles may beparticularly problematic. The social support measure was limited in that it did notcomprehensively assess the structure and function of the support provided by familyand friends. The third area of concern about the study design was that informationwas not available about therapeutic alliance, group processes during treatment, orthe reasons that women left the group. This information would allow formore detailed investigation of the obstacles women faced in attending grouppsychotherapy. Further, assessing the working alliance is important, as attendancedoes not necessarily mean treatment engagement and, further, it is not likely to besufficient for change. A fourth problem with the study was the failure to control forother potentially relevant variables in the analyses, such as demographic factors,Axis I and Axis II psychopathology, or seriousness of the IPV experienced. A fifth
1307Social Difficulty and Group Therapy Adherence
Journal of Clinical Psychology DOI: 10.1002/jclp

concern with the investigation is that the social brain model was not fully examined,as only some variables associated with this model were considered in thisinvestigation. The final issue relates to the question of the generalizability of thefindings to individuals from different demographic backgrounds.Taken together with the current findings, the above limitations highlight areas in
need of further research. Future directions should include larger samples ofindividuals that represent a broader range of psychopathology, ethnicity, age, andstage of change (Bliss, Ogley-Oliver, Jackson, Harp, & Kaslow, 2008). It is alsorecommended that in addition to self-report, interpersonal processes should beevaluated from the perspective of the mental health professional. This evaluationmight include an adult attachment interview, as well as group transactions. Further,it would be useful to examine not only attachment relationships but also the workingalliance, treatment engagement, and the real relationship between the women andthe group therapists (Marmarosh et al., 2009). In addition, investigations could morefully examine the social brain model. For example, they could examine key biologicalfactors including genes and activity in specific regions of the brain that are relevantto social and emotional functioning, as well as traumatic stress exposure and socialinformation processing. Finally, it would be valuable to conduct similar researchwith women from different racial/ethnic and social class backgrounds to more fullyunderstand the generalizability of the findings.In terms of directions for group psychotherapy interventions, changing attachment
styles is unrealistic. On the other hand, mindfulness of their social and relationalhistories, expectations and beliefs, skills and deficits, and relational needs mayimprove treatment engagement. To facilitate this awareness, initial mental healthscreenings should also include assessment of attachment style and interpersonalhassles. Additionally, relationship building could occur at a level of a dyad(e.g., therapist and patient, patient and patient) before engaging patients intopsychotherapy group treatment. As group dynamics and relationships evolve overtime, group dynamics should be explicitly discussed and processed. Solution-focusedcoping and explicit social skills training may be helpful to address daily interpersonalhassles that specifically interfere with group psychotherapy attendance. Character-istics related to group composition should also be considered (e.g., heterogeneityof exposure to abuse or trauma), such as to improve social isolation andstigmatization (Nicholas & Forrester, 1999) and improve clinical outcomes (Hornsey,Dwyer, & Oei, 2008).
References
Adams, K.S., Sheldon-Keller, A.E., & West, M. (1996). Attachment organization and history
of suicidal behavior in clinical adolescents. Journal of Consulting and Clinical Psychology,
64, 264–272.
Ayuso-Mateos, J.L., Pereda, A., Dunn, G., Vazquez-Barquero, J.L., Casey, P., Lehtinen, V.,
et al. (2007). Predictors of compliance with psychological interventions offered in the
community. Psychological Medicine, 37, 717–725.
Bakker, C., Gardner, R., Koliatsos, V., Kerbeshian, J., Looney, J.G., Sutton, B., et al.
(2002). The social brain: A unifying foundation for psychiatry. Academic Psychiatry,
26, 219.
Bartholomew, K., & Horowitz, L.M. (1991). Attachment styles among young adults: A test of
a four-category model. Journal of Personality and Social Psychology, 61, 226–244.
1308 Journal of Clinical Psychology, December 2009
Journal of Clinical Psychology DOI: 10.1002/jclp

Baucom, D.H., Porter, L.S., Kirby, J.S., Gremore, T.M., Wiesenthal, N., Aldridge, W., et al.
(2008). A couple-based intervention for female breast cancer. Psycho-Oncology, 10.1002/
pon.1395.
Beach, M.C., Keruly, J., & Moore, R.D. (2006). Is the quality of the patient-provider
relationship associated with better adherence and health outcomes for patients with HIV?
Journal of General Internal Medicine, 21, 661–665.
Bliss, M.J., Ogley-Oliver, E., Jackson, E.B., Harp, S., & Kaslow, N.J. (2008). African American
women’s readiness to change abusive relationships. Journal of Family Violence, 23, 161–171.
Bornstein, R.F. (2006). The complex relationship between dependency and domestic violence:
Converging psychological factors and social forces. American Psychologist, 61, 595–606.
Chance, S.E., Reviere, S.L., Rogers, J.H., James, M.E., Jessee, S., Rojas, L., et al. (1996). An
empirical study of the psychodynamics of suicide: A preliminary report. Depression, 4,
89–91.
Ciechanowski, P.S., Katon, W.J., Russo, J.E., & Walker, E.A. (2001). The patient-provider
relationship: Attachment theory and adherence to treatment in diabetes. American Journal
of Psychiatry, 158, 29–35.
Coker, A.L., Smith, P.H., Thompson, M., McKeown, R.E., Bethea, L., & Davis, K.E. (2002).
Social support protects against the negative effects of partner violence on mental health.
Journal of Women’s Health and Gender-Based Medicine, 11, 465–476.
Compton, M.T., Thompson, M.P., & Kaslow, N.J. (2005). Social environment factors
associated with suicide attempt among low-income African Americans: The protective role
of family relationships and social support. Social Psychiatry and Psychiatric Epidemiology,
40, 175–185.
Dahlem, N.W., Zimet, G.D., & Walker, R.R. (1991). The Multidimensional Scale of Perceived
Social Support: A confirmation study. Journal of Clinical Psychology, 47, 756–762.
Davis, S.P., Arnette, N.C., Bethea, K.I., Graves, K.N., Rhodes, M.N., Harp, S.E., et al.
(2009). The Grady Nia Project: A culturally competent intervention for low-income,
abused and suicidal African American women. Professional Psychology: Research and
Practice, 40, 141–147.
de Jong, G.M., Timmerman, I.G.H., & Emmelkamp, P.M.G. (1996). The Survey of Recent
Life Experiences: A psychometric evaluation. Journal of Behavioral Medicine, 19, 529–542.
Edwards, L. (2006). Perceived social support and HIV/AIDS medication adherence among
African American women. Qualitative Health Research, 16, 679–691.
Flores, P.J. (2008). Attachment theory and group psychotherapy. International Journal of
Group Psychotherapy, 58, 127–132.
Fuertes, J.N., Mislowack, A., Bennett, J., Paul, L., Gilbert, T.C., Fontan, G., et al. (2007).
The physician-patient working alliance. Patient Education and Counseling, 66, 29–36.
Griffin, D., & Bartholomew, K. (1994). Models of self and other: Fundamental dimensions
underlying measures of adult attachment. Journal of Personality and Social Psychology,
67, 430–445.
Haaga, D.A.F., Yarmus, M., Hubbard, S., Brody, C., Solomon, A., Kirk, L., et al. (2002). Mood
dependency of self-rated attachment style. Cognitive Therapy and Research, 26, 57–71.
Harrington, E.F., Crowther, J.H., Henrickson, H.C.P., & Mickelson, K.D. (2006). The
relationships among trauma, stress, ethnicity, and binge eating. Cultural Diversity and
Ethnic Minority Psychology, 12, 212–229.
Henderson, A.J.Z., Bartholomew, K., & Dutton, D.G. (1997). He loves me; he loves me not:
Attachment and separation resolution of abused women. Journal of Family Violence, 12,
169–191.
Henderson, A.J.Z., Bartholomew, K., Trinke, S.J., & Kwong, M.J. (2005). When loving
means hurting: An exploration of attachment and intimate abuse in a community sample.
Journal of Family Violence, 20, 219–230.
1309Social Difficulty and Group Therapy Adherence
Journal of Clinical Psychology DOI: 10.1002/jclp

Hilsenrath, M., Holdwick, D., Castelbury, F., & Blais, M.A. (1998). The effects of DSM-IV
cluster B personality disorder symptoms on the termination and continuation of
psychotherapy. Psychotherapy, 35, 163–176.
Hornsey, M.J., Dwyer, L., & Oei, T.P.S. (2008). Beyond cohesiveness: Reconceptualizing the
link between group processes and outcomes in group psychotherapy. Small Group
Research, 38, 567–592.
Jackson, K.R., Booth, P.G., McGuire, J., & Salmon, P. (2006). Predictors of starting and
remaining in treatment at a specialist alcohol clinic. Journal of Substance Use, 11, 89–100.
Johnson, D.P., Penn, D.L., Bauer, D.J., Meyer, P.M., & Evans, E. (2008). Predictors of the
therapeutic alliance in group therapy for individuals with treatment-resistant auditory
hallucinations. British Journal of Clinical Psychology, 47, 171–183.
Kaslow, N.J., Sherry, A., Bethea, K., Wyckoff, S., Compton, M., Bender, M., et al. (2005).
Social risk factors for suicide attempts in low income African American men and women.
Suicide and Life Threatening Behavior, 35, 400–412.
Kaslow, N.J., Thompson, M., Brooks, A., & Twomey, H. (2000). Ratings of family
functioning of suicidal and nonsuicidal African American women. Journal of Family
Psychology, 14, 585–599.
Kaslow, N.J., Thompson, M., Meadows, L., Chance, S., Puett, R., Hollins, L., et al. (2000). Risk
factors for suicide attempts among African American women. Depression and Anxiety, 12, 13–20.
Kaslow, N.J., Thompson, M., Meadows, L., Jacobs, D., Chance, S., Gibb, B., et al. (1998).
Factors that mediate and moderate the link between partner abuse and suicidal behavior in
African American women. Journal of Consulting and Clinical Psychology, 66, 533–540.
Kaslow, N.J., Thompson, M.P., Okun, A., Price, A., Young, S., Bender, M., et al. (2002). Risk
and protective factors for suicidal behavior in abused African American women. Journal of
Consulting and Clinical Psychology, 70, 311–319.
Kohn, P.M., & Macdonald, J.E. (1992). The Survey of Recent Life Experiences:
A decontaminated hassles scale for adults. Journal of Behavioral Medicine, 15, 221–236.
Lessard, J.C., & Moretti, M.M. (1998). Suicidal ideation in an adolescent clinical sample:
Attachment patterns and clinical implications. Journal of Adolescence, 21, 383–395.
Levendosky, A.A., Bogat, G.A., Theran, S.A., Trotter, J.S., von Eye, A., & Davidson, W.S.I.
(2004). The social networks of women experiencing domestic violence. American Journal of
Community Psychology, 34, 95–109.
Loh, A., Leonhart, R., Wills, C.E., Simon, D., & Harter, M. (2007). The impact of patient
participation on adherence and clinical outcome in primary care of depression. Patient
Education and Counseling, 65, 69–78.
MacNair-Semands, R.R. (2002). Predicting attendance and expectations for group therapy.
Group Dynamics: Theory, Research, and Practice, 6, 219–228.
MacNair, R.R., & Corazzini, J.G. (1994). Client factors influencing group therapy dropout.
Psychotherapy: Theory, Research, Practice, Training, 31, 352–362.
Marmarosh, C.L., Gelso, C.J., Markin, R.D., Majors, R., Mallery, C., & Choi, J. (2009). The
real relationship in psychotherapy: Relationships to adult attachments, working alliance,
transference, and therapy outcome. Journal of Counseling Psychology, 56, 337–350.
Molloy, G.J., Perkins-Porras, L., Strike, P.C., & Steptoe, A. (2008). Social networks and
parent stress as predictors of adherence to medication, rehabilitation attendance and
quality of life following acute coronary syndrome. Health Psychology, 27, 52–58.
Nicholas, M., & Forrester, A. (1999). Advantages of heterogeneous therapy groups in the
psychotherapy of the traumatically abused: Treating the problem as well as the person.
International Journal of Group Psychotherapy, 49, 323–342.
Ogrodniczuk, J.S., Piper, W.E., & Joyce, A.S. (2006a). Treatment compliance among patients
with personality disorders receiving group psychotherapy: What are the roles of
interpersonal distress and cohesion. Psychiatry, 69, 249–261.
1310 Journal of Clinical Psychology, December 2009
Journal of Clinical Psychology DOI: 10.1002/jclp

Ogrodniczuk, J.S., Piper, W.E., & Joyce, A.S. (2006b). Treatment compliance in differenttypes of group psychotherapy: Exploring the effects of age. Journal of Nervous and Mental
Disease, 194, 287–293.
Palmer, N.B., Salcedo, J., Miller, A.L., Winiarski, M., & Arno, P. (2003). Psychiatric andsocial barriers to HIV medication adherence in a triply diagnosed methadone population.
AIDS Patient Care and STDs, 17, 635–644.
Perry, J.C., Bond, M., & Roy, C. (2007). Predictors of treatment duration and retention in astudy of long-term dynamic psychotherapy: Childhood adversity, adult personality, and
diagnosis. Journal of Psychiatric Practice, 13, 221–232.
Prado, G., Pantin, H., Schwartz, S., Lupei, N., & Szapocznik, J. (2006). Predictors of
engagement and retention in a parent-centered, ecodevelopmental HIV preventiveintervention for Hispanic adolescents and their families. Journal of Pediatric Psychology,31, 874–890.
Sajatovic, M., Bauer, M.S., Kilbourne, A.M., Vertrees, J.E., & Williford, W. (2006). Self-reported medication treatment adherence among veterans with bipolar disorder.Psychiatric Services, 57, 56–62.
Scharfe, E., & Bartholomew, K. (1994). Reliability and stability of adult attachment patterns.Personal Relationships, 1, 23–43.
Scott, J., Halford, K., & Ward, B. (2004). United we stand? The effects of a couple-coping
intervention on adjustment to early stage breast or gynecological cander. Journal ofConsulting and Clinical Psychology, 72, 1122–1135.
Terra, M.B., Barros, H.M.T., Stein, A.T., Figueira, I., Athayde, L.D., Spanemberg, L., et al.
(2006). Does co-occurring social phobia interfere with alcoholism treatment adherence andrelapse? Journal of Substance Abuse Treatment, 31, 403–409.
Twomey, H., Kaslow, N.J., & Croft, S. (2000). Childhood maltreatment, object relations, andsuicidal behavior in women. Psychoanalytic Psychology, 17, 313–335.
Vanderwerker, L.C., Chen, J.H., Charpentier, P., Paulk, M.E., Michalski, M., & Prigerson, H.G.
(2007). Differences in risk factors for suicidality between African American and Whitepatients vulnerable to suicide. Suicide and Life-Threatening Behavior, 37, 1–9.
Waldinger, R.J., Schulz, M.S., Barsky, A.J., & Ahern, D.K. (2006). Mapping the road from
childhood trauma to adult somatization: The role of attachment. Psychosomatic Medicine,68, 129–135.
Wamboldt, F. (2005). Medication adherence: The social brain and consultation liaison.
Psychiatric Annals, 35, 823–827.
Zeber, J.E., Copeland, L.A., Good, C.B., Fine, M.J., Bauer, M.S., & Kilbourne, A.M. (2008).Therapeutic alliance perceptions and medication adherence in patients with bipolar
disorder. Journal of Affective Disorders, 107, 53–62.
Zimet, G.D., Dahlem, N.W., Zimet, S.G., & Farley, G.K. (1988). The Multidimensional Scale
of Perceived Social Support. Journal of Personality Assessment, 52, 30–41.
Zimet, G.D., Powell, S.S., Farley, G.K., Werkman, S., & Berkoff, K.A. (1990). Psychometriccharacteristics of the Multidimensional Scale of Perceived Social Support. Journal of
Personality Assessment, 55, 610–617.
1311Social Difficulty and Group Therapy Adherence
Journal of Clinical Psychology DOI: 10.1002/jclp





























