Embed Size (px)
Citation preview
Meredith GartinSchool of Human Evolution and Social ChangeArizona State University
Alexandra A. BrewisSchool of Human Evolution and Social ChangeArizona State University
Norah Anita SchwartzDepartment of Population StudiesEl Colegio de la Frontera Norte (COLEF)
Nonprescription Antibiotic Therapy:Cultural Models on Both Sides of the Counter and Both Sides of the Border
Antibiotic resistance is a global public health threat exacerbated by medically unwar-ranted or improper antibiotic use. Pharmacy counters at the U.S.–Mexico borderprovide an example of where lay decisions to use antibiotics in ways considered“risky” may be initiated and negotiated. We test how cultural and public healthknowledge of antibiotics is distributed among pharmacy staff, local Mexican clients,and U.S. medical tourists in the bordertown of Nogales using a cultural consensustool. We find that shared cultural models across these groups include public healthstatements; however, other shared statements are likely to reinforce antibiotic salesat pharmacy counters by those on both sides of the purchase as economic, ratherthan therapeutic, encounters. From a public health perspective, border pharmacycounters are not a location where increased “safe” knowledge about antibiotic useis being transmitted. However, we do find a positive relationship between “safe”knowledge and reductions in risky behavior.
Keywords: [antibiotics, cultural models, Mexico, ethnopharmacology, self-medication]
Antibiotics are one of the most widely used sets of pharmaceuticals globally, andantimicrobial resistance related to antibiotic mis- and overuse is recognized as amajor global public health threat (Barbosa and Levy 2000; Cars et al. 2001; Levy1998, 2005; Wise et al. 1998). The bases of the burgeoning problem are tied towidespread use of antibiotics without medical oversight that fulfills no ostensiblemedical need (i.e., medically unnecessary lay self-medication), and the failure ofusers to take medications as directed, along with indiscriminant prescribing orrecommending of antibiotics by health workers (Guillemot et al. 1998; Kristianssonet al. 2008; WHO 2001). From the perspective of medical anthropology, medically
MEDICAL ANTHROPOLOGY QUARTERLY, Vol. 24, Issue 1, pp. 85–107, ISSN 0745-5194, online ISSN 1548-1387. C© 2010 by the American Anthropological Association. All rightsreserved. DOI: 10.1111/j.1548-1387.2010.01086.x
85

86 Medical Anthropology Quarterly
unwarranted self-medication with antibiotics is explicable at a very basic level: thehealing power ascribed to antibiotic drugs in lay models of healing is substantialand has been observed in a wide range of contexts (Adetunji 1991; Calva 1996;Chavez 1984; Finerman 1989; Hardon 1987; Kamat and Nichter 1998; Logan1983; Maiman et al. 1986; Nichter and Vuckovic 1994; Oldani 2004; Schwartz2004; Schwartz and Casillas-Miranda 1998; van der Geest 1982; van der Geestand White 1988; Vuckovic 1999). Self-medication with antibiotics tends to beconcentrated where antibiotics are readily and cheaply available over the counter(OTC); this includes Mexico along with most of Latin America (Okeke et al. 1999;Pechere 2001; Trostle 1999; Vuckovic and Nichter 1997). The ability to purchaseantibiotics OTC significantly influences not only the opportunity and likelihoodthat antibiotics will be purchased but also shapes the likelihood they will be used inways that create broader public health risks beyond those to the individual, such asevolved antibiotic resistance (McKee et al. 1999).
To address this global public health challenge, we need better culturally basedunderstandings (cultural knowledge) of why and how people use antibiotics in waysthat are not medically prescribed (Berzanskyte et al. 2006; Bojalil and Calva 1994;Grigoryan et al. 2006; Kamat and Nichter 1998; Sachs and Tomson 1992). Ar-guably, the best place to uncover these understandings is in the locations wherethose behaviors most commonly occur. Our setting, the bordertown of Nogales,Mexico, is a site of extremely intensive purchase of OTC antibiotics; there is alsosome evidence of drug resistance in this particular local community (Mainous et al.2005; McKee et al. 1999). In Tijuana, another border community, lower-incomelocals tend to use the pharmacies as primary health care providers for a numberof reasons, including avoiding the expense of seeing a physician (Schwartz 2004).Other common users of these border pharmacies are the large medical tourist pop-ulation who cross the border to make OTC purchases of drugs that are otherwiseprescription only and more expensive in the United States. Therefore, Nogales isa particularly telling location in which to consider how the sellers and purchasersof antibiotics, and different groups of purchasers, conceptualize their personal andpublic health risks, and how variations in knowledge about antibiotics shape re-ported antibiotic behaviors.
A unique feature of the study design is a focus on pharmacy staff conceptualmodels and how these might contrast and relate to their main groups of clients.A central question for the study was whether those selling antibiotics OTC anddifferent groups of clients purchasing those antibiotics in pharmacies had a sharedcultural model related to the risks of antibiotic misuse. Using a cultural consensusmodeling approach, we sought to identify how people are thinking about the risksassociated with antibiotic use. In relation to this, we wanted to know if pharmacistsconceptualize risk similarly or differently from their clients, and in what ways. Thisapproach helps us understand if “risky” antibiotic use is occurring in a contextwhere (1) pharmacists understand the risk but are not transmitting that knowledgeto clients; (2) both groups recognize the risk but are engaged in “risky” behaviorsnonetheless; or (3) neither group recognizes the risk. These three situations havequite different implications for targeting the most effective health education. Also,if there are different cultural models operating on both sides of the counter, thiswill provide insight into the social and cultural exchanges that may take place in

Nonprescription Antibiotic Therapy in Mexico 87
pharmacies, a task most often neglected in pharmacy studies (Petryna and Klienman2006).
Antibiotic Use and Resistance in Mexico and Beyond: Some Background
In a poignant presidential address to the Society of Tropical Medicine and Hygienein 1998, Richard Guerrant proposed that Americans must be concerned abouttropical medicine because, owing to our own behaviors, we are not immune tothe global threat of emerging and reemerging infectious diseases that are on therise. In June 2000, the WHO warned that increasing drug resistance could rob theworld of its opportunity to cure illness and stop epidemics. The economic impact ofantimicrobial resistance can be staggering (Paladino et al. 2002), as infections re-quire less accessible and more expensive, toxic treatments that may quickly becomeineffective (Okeke et al. 1999). More recently, Michele Barry (2003) suggested inher presidential address to the Society of Tropical Medicine and Hygiene that thepublic health response is not keeping pace with the potential for infected individuals,pathogens, and antibiotic resistance to cross borders; thus, the emergence of inter-national travel and global trade have the potential to transport multidrug-resistantorganisms into and among developed nations.
Antibiotic resistance takes its greatest toll on the global south. Multidrug-resistant bacterial strains are often associated with common “diseases of poverty,”such as tuberculosis, acute respiratory infections, and diarrhea (Byarugaba 2004).In Mexico, and most of Latin America, unwarranted self-administration ofantibiotics is common, particularly for the treatment of viral respiratory (ARI) in-fections (Pachter et al. 2002; Schwartz 2002, 2004) and self-limiting diarrheal con-ditions (Bojalil and Calva 1994). Other factors associated with antibiotic resistancein developing countries include poor quality, counterfeit, adulterated, and expireddrugs; inappropriate and unregulated use by clinicians and unskilled practitioners;misuse and unregulated distribution by the public; bioinequivalent antibiotics (notdelivering the expected amount of drug to the bloodstream) and inadequate accessto effective drugs; and the inability to pay for “appropriate, high-quality medica-tions” (Okeke et al. 1999; Planta 2007). On the northern Mexico border whereour study is set, reports are that some 75 percent of those buying antibiotics do sowithout any prescription (Casner and Guerra 1992). In a qualitative study of child-hood illness in Tijuana Mexico, Schwartz (2004) found that Mexican pharmacistsmake a distinction between “prescribing” antibiotics (which is seen as the job of thephysician) and “recommending” antibiotics, which is not prohibited by law.
In this regard, Latin Americans have been shown to rely on the recommenda-tions of nonmedical professionals (incl. pharmacists) when purchasing prescriptionproducts (Bolanos 2005; Larson et al. 2006). Pharmacists can recommend and sellantibiotics without a prescription to customers, even if the pharmacist has not ac-quired a standard pharmaceutical education (Schwartz and Casillas-Miranda 1998).Most medication is then passed to consumers without dosage information, meaningthat antibiotics are often used improperly, or at an incorrect dosage.
The practice of self-administration of antibiotics using OTC or secondhand an-tibiotics is reportedly common in Latino groups in the United States, in a man-ner that appears to track practices and ideas about antibiotics from originating

88 Medical Anthropology Quarterly
countries (Larson et al. 2003). Pylypa (2001) explains how, among Mexican im-migrants in California, the decision to self-medicate draws on a diverse set of in-formation and influences outside of biomedical arenas, including friends, family,and pharmacy staff. In the United States, common sources for Latinos to obtainantibiotics without prescriptions are local Mexican-run stores (such as bodegas), orat swap meets (Larson et al. 2006; Schwartz and Pepper 2009).
The practice of self-diagnosis is also very common in a manner that appearsto show a strong preference for antibiotics over other types of pharmaceuticals(Belongia et al. 2002; Corbett et al. 2005). A telephone survey in Colorado foundLatino respondents were less likely than others to be aware of antibiotic resistanceand less likely to be satisfied with medical consultations if an antibiotic was notprescribed (Corbett et al. 2005). Patients who self-diagnosed symptoms prior toa clinical encounter are much more likely to press for unwarranted antibiotics,and clinicians were more likely to agree (Belongia et al. 2002). Clinicians often andcommonly prescribe unnecessary antibiotic treatment (most often for ARI) based onthe strength of patient wishes for antibiotic therapy (Belongia et al. 2002; Maimanet al. 1986; Vuckovic and Nichter 1997).
The U.S.–Mexico border is a venue where cross-border transport of unregulatedantibiotics is common, especially but not only by Latinos. A study conducted inLennox, California, a predominantly foreign-born Latino community east of LosAngeles, reported that 70 percent of adults surveyed crossed the border for lower-cost medical care, 90 percent of those were uninsured, and 28 percent purchasedsome combination of antibiotics, pain medication, and contraceptives (Macias andMorales 2001). The additional time and cost of seeing a doctor is often cited asa factor in nonprescription antibiotic use by Latinos in the United States (Larsonet al. 2006; Vuckovic 1999; Vuckovic and Nichter 1997). A clinical study of Latinosin a South Carolina community reported that 45.2 percent of respondents saidthey had purchased antibiotics outside of the U.S. (Mainous et al. 2005). AnotherCalifornia-based study showed that migrants will incur greater time, cost, andrisk to cross to Tijuana to get OTC medicines (Pylypa 2001). Other social factorsassociated with border crossing for pharmaceutical needs include distrust of the U.S.medical encounter (Mainous et al. 2005), language barriers in U.S. treatment settings(Chavez 1984; Corbett et al. 2005), and greater comfort with using medicationsfrom their native country (Cespedes and Larson 2006).
Antibiotics are one of the most common OTC drugs purchased by U.S. citizensin Mexico; those crossing the border and buying drugs are not only from the borderstates but also from all parts of the United States (McKeithan and Shepherd 1996).Both the low-cost and unregulated transport of antibiotics are shared, critical factorsamong the local Latinos and the large numbers of non-Latinos who cross intoMexico to buy OTC antibiotics (and other prescription drugs; see Calvillo andLal 2003; Casner and Guerra 1992; Macias and Morales 2001; McKeithan andShepherd 1996), even among the healthy insured (Calvillo and Lal 2003). It isalso important to recognize that antibiotics are a commodity in these pharmacies,prompting competition for sales profit (see Vuckovic and Nichter 1997). The rulerequiring a written prescription for the transport of any prescription medicationpurchased in Mexico is often ignored by U.S. border-crossing guards (McKeithanand Shepherd 1996). As of this writing, border crossers are rarely if ever questioned

Nonprescription Antibiotic Therapy in Mexico 89
about the transport of pharmaceuticals; and, although car trunks are often requiredto be opened, the searching of handbags—the place in which pharmaceuticals aremost likely to be carried—appears to be almost never conducted (Schwartz, personalobservation). Thus, government regulation and oversight in the United States arecurrently considered insufficient to forestall at least some informal or unnecessarymodalities of antibiotic use.
The Border Setting and Pharmacy Counter
The borderland, small city of Nogales, Sonora, Mexico, is a diverse, dynamic place.On the U.S.–Mexico border, a number of different groups seek health care in dif-ferent ways (Macias and Morales 2001). In Nogales, locals with least means (suchas maquiladoras) use the town’s many pharmacies as a first line of treatment; localswith more resources may visit a doctor first and leave with an antibiotic prescrip-tion; those with insurance may access the Mexican socialized medical facilities inthe city; the wealthiest often choose to travel to the U.S. side of the border fortreatment. Nogales is also a staging point for those from elsewhere in Mexico andLatin America who wait to enter the United States or are returned to Mexico asdeportees, and who have little choice except for pharmacies to meet their healthneeds. In addition, under- and uninsured Anglos from Arizona and beyond (manyretirees) arrive in shuttle buses or drive to the border and then walk over (a bigdraw is low-cost dental treatments). All of these groups use the pharmacies and theseveral dozen stores that crowd the main squares of Nogales; thus, the Nogalanpharmacists serve multiple clienteles, each of whom might have a different set ofconceptual models of antibiotics, as well as other drugs.
The pharmacy counters of Nogales are often managed by staff with little or noformal medical or pharmaceutical training. Moreover, employees are often trans-ferred or moved given that the pharmacy owners may own chains of stores in thecity. The pharmacies tend to stock a limited range of antibiotics and antibioticsamples, the most popular of which are Ciprofloxin, Amoxicillin, Penicillin, andZithromax. Each pharmacy has on hand a copy of the Physician’s Desk Referencein Spanish to which the pharmacist or counter staff will refer as needed, such aswhen a client asks for information about a specific type of medication or requests amedication for a less common problem. Based on our observations in 18 differentpharmacies in Nogales, we found that the pharmacy staff rarely—if ever—diagnosedtheir clients or recommend them any specific drugs. Most clients handed a prescrip-tion or drug label to the pharmacy employee, or clients named or pointed to thedrug they want. If the drug was in stock it was always given to the client; if notavailable, the pharmacy employee would recommend another pharmacy.
Study Design
To guide the research, we posed two basic propositions related to the distribu-tion, variation, and consensus of knowledge about antibiotic use and its relatedrisks across three groups—pharmacists, medical day-tourists, and local Mexicanclientele—and one basic proposition about antibiotic practice.
90 Medical Anthropology Quarterly
(1) We anticipated that people’s reports of “risky” antibiotic behavior (i.e.,people reporting that they saved or borrowed antibiotics, and OTC pur-chasing) would be better predicted by group membership, level of education,and socioeconomic status. This was based on the two premises that (1) bet-ter educated and more affluent clientele would have more information andmore resources available to be able to minimize any perceived risk (e.g., bemore likely to use antibiotics only with prescription), and (2) more educatedclients and pharmacists would have more exposure to and thus have takenon more public health information about responsible antibiotic use. We usereported occupation as our estimator of socioeconomic status.
(2) We anticipated that pharmacists and clients would share a cultural modelabout the risks related to antibiotic use, and that this model would favorpublic health knowledge. We based this on two general understandings: (1)that public health messages can be a powerful source of knowledge, and(2) that antibiotic use is a relatively uncomplicated domain of knowledgethat might allow for easier transmission of ideas. Finding a shared culturalmodel would provide a basis for good, across-the-counter communicationbetween pharmacists and clients. We also anticipated the possibility thatlocal Mexicans, U.S. medical day-tourists, and the pharmacists could haveconceptual submodels regarding antibiotic use that are measurably distinct.
(3) We anticipated individuals with cultural models dominated by public healthknowledge would be less likely to report that they engage in risky behaviorsrelated to antibiotic use. Public health seeks to examine those behaviorsthat may be modified or changed with increased education and knowledgeabout proper health care behavior. This requires a basic understanding ofthe link between behavior and cognition; therefore, we wanted a meansto test how people’s understanding of common public health informationregarding antibiotic use and prescription might influence behavior knownto increase risk for antimicrobial resistance (i.e., borrowing, saving, andOTC purchasing of antibiotics).
The main tool we used in this study to test these last two propositions is a cul-tural consensus survey tool, a standard approach in cognitive anthropology andincreasingly in medical anthropology (Brewis and Gartin 2006; Curry et al. 2002;Pelto and Pelto 1997; Romney et al. 1986). In Phase I, 2006–07, we were concernedwith the tool development. We conducted extensive observations in the pharmacies,conducted freelists and pile sorts with pharmacists, and conducted and transcribeda series of 20 extended semistructured interviews with medical tourists and pharma-cists covering the domains of health, antibiotics, and health-seeking behavior. Wesupplemented these with the 20 transcripts collected by Schwartz during her studyof health keeping on the border between 1996 and 2001 (see Schwartz 2004). Eachof the transcripts was coded in the language in which they were collected (eitherSpanish or English) to identify cultural statements related directly or indirectly toantibiotic use. The cultural statements from the interviews (such as “Pharmacistsare more trustworthy than doctors”) were extracted by assistants, who had notconducted the interviews, searching on key terms using NVivo Qualitative DataAnalysis Software (ver. 2; see Richards 1999). This resulted in approximately 100

Nonprescription Antibiotic Therapy in Mexico 91
statements on the first pass. Further statements were then drawn from the freelistswith the pharmacists. Pharmacists in Nogales and Tijuana provided three differentfreelists: “common symptoms,” “health problems,” and “treatments.” This provedto be of limited utility when we started developing the statement lists because wefound the range of responses was very broad.
We then also conducted an analysis of key authoritative Internet webpages relatedto antibiotic on antibiotic resistance designed for a lay audience (such as the CDCand WHO websites). These were used to extract additional public health statementsthat had not emerged in interviews (e.g., “As soon as you are well, you shouldthrow away any unused antibiotics”). We describe these in the text that follows as“public health statements.” If statements that were derived from the interviews alsoappeared on the public health websites we noted them as public health statements.
In using cultural statements surveys and subjecting them to consensus analysis,important assumptions of this approach include that all the questions in the surveyare equally difficult (Romney et al. 1986), independent of respondents, and that thereis no response bias in how the informant answers including when guessing (Weller2007). Before use, the survey containing these statements was back-translated withtwo bilingual language experts, a native Sonoran Spanish speaker and a native U.S.English speaker, and pretested. The issue of homogeneity of items is a particularconcern in a dual-language situation, and we conducted several pilot tests of thetool to remove any items that pretesting proved to be difficult for some respondentsto understand. Then any repetitious statements were removed, and some statementswere reversed to discourage a response bias. The final survey tool developed in PhaseI consisted of 68 cultural statements regarding antibiotic therapy and treatment-seeking behavior, with only dichotomous true–false responses possible. Althoughthe method can be used with open-ended and multiple-choice responses, limitingoptions forces a decision (guessing is, as noted, built into the model). Limiting toonly two possible responses is the most commonly applied approach in similarhealth-related studies (see Weller 2007).
Phase II was focused on conducting the cultural consensus survey and took placeduring early to mid-2007. In addition, we collected basic demographic and healthhistory background and information about personal experience with antibiotic useand purchase on a Likert-type scale. All participants answered the same questions.
The sampling strategy for Phase II was a purposive sample in the vicinity of 18participating pharmacies and three adjacent plazas in the Nogales, Sonora, businessdistrict located within a half a mile from the U.S. border crossing and checkpoint.Both local clientele and tourists would socialize in these plazas after visiting thepharmacies. We chose these sites to recruit participants so we would not disrupt thepharmacy’s business, and we used one screener question: “Have you bought antibi-otics at one of these local pharmacies?” We did not specify the day of the purchasebecause many of the tourists were returning clients and might have not purchased anantibiotic that day, nor whether it was an OTC purchase versus prescription.
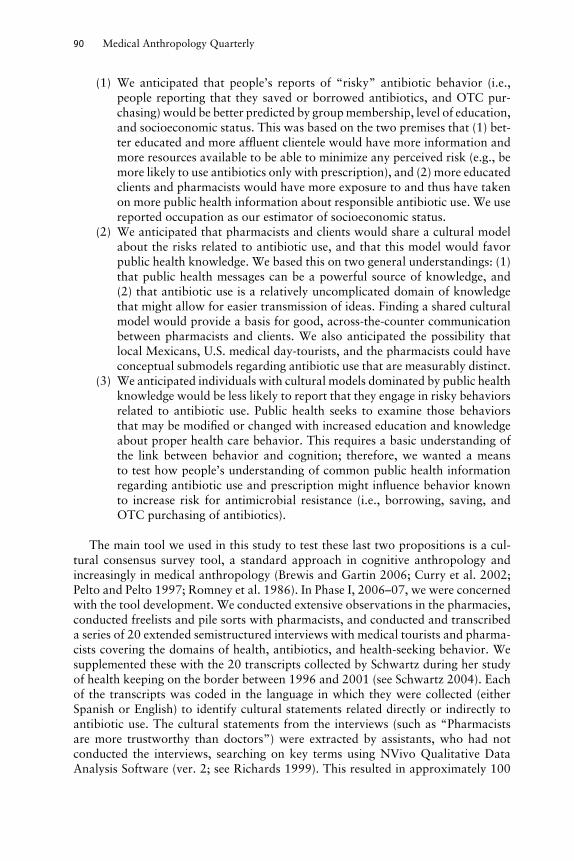
The numbers recruited in each of the main study groups were 35 U.S. medicaltourists, 35 Mexican residents of Nogales, and 27 pharmacy personnel. Table 1 de-scribes the demographic variables for our sample. Everyone in the Mexican sample,including pharmacists, currently resided in Nogales, Sonora. Eleven percent of thetourists were born in Arizona, but the majority (77 percent) were current Arizona
92 Medical Anthropology Quarterly
Table 1. Demographic Descriptors of the Sample
Pharmacy Staff Mexican Clients U.S. Tourists
GenderMale 17 (63%) 20 (57%) 12 (34%)Female 10 (37%) 15 (43%) 23 (66%)Mean Age 31 36 49
EducationLess Than High School 3 (11%) 6 (17%) 0High School Degree 13 (48%) 22 (63%) 10 (29%)Some College 4 (15%) 0 12 (34%)Technical Degree 1 (4%) 3 (8.5%) 1 (3%)Bachelors Degree 5 (19%) 1 (3%) 8 (23%)Graduate Degree 1 (4%) 3 (8.5%) 4 (11%)Speak Second Language 17 (63%) 14 (40%) 8 (23%)
OccupationNon-Healthcare Profession 0 24 (68%) 23 (66%)Retired 0 1 (3%) 10 (29%)Student 0 0 0Unemployed 0 10 (29%) 2 (6%)Mexican Healthcare 27 (100%) 0 0
Pharmacy TrainingNone 4 (15%)On-the-Job Training 20 (74%)University Courses 3 (11%)
Years Working in PharmacyRange 1–30Mean 5
residents and were also regular purchasers of other products such as diet pills, painmedication, and Viagra. The U.S. tourists also had more years of formal educationon average. Both the total Mexican client groups and the tourist group reportedmodally that they were working in blue-collar jobs or had been before retirement(Mexican clients = 54 percent; U.S. tourists = 59 percent). For those working in thepharmacies, the average number of years having worked in a pharmacy was five.Three-quarters of the employees dispensing antibiotics received on-the-job trainingonly. Half reported having a high school diploma, 15 percent had some college, and27 percent had obtained a technical degree or higher. When comparing betweenthe pharmacy staff and their Mexican clients, the pharmacy staff had more years ofeducation on average.
Informed consent was gained in both phases for the project (pretesting–pilotingand final data collection), under Arizona State University Human Subjects IRBApproval #0611001250.
Analysis
Basic statistical analyses were done using SPSS, version 16. The consensus analyseswere conducted using UCINET 6. A ratio of greater than 3 : 1 between eigenvalues

Nonprescription Antibiotic Therapy in Mexico 93
in the first two factors derived from the consensus statements was considered in-dicative of shared knowledge and, thus, the existence of a shared cultural model(see Curry et al. 2002). If cultural agreement existed, the individual loadings onthe first and second factors were examined for fit of individual responses to thegroup consensus and weighted accordingly so the most culturally correct answerfor each belief statement could be identified. This method can reasonably be ap-plied to samples of 20–25 respondents, especially if a high level of agreement exists(Curry et al. 2002; Romney et al. 1986); thus, our sample size well exceeded theminimum requirements. We then used Quadratic Assignment Procedure (QAP) cor-relation to assess whether the observed differences between the study subgroupswere significant, which was possible given samples of over 20 in each (Dressleret al. 1995; Furlow 2003; Garro 1996; Hubert and Schultz 1976). The initial stepinvolves calculating agreement matrices of the interinformant correlations for allparticipants by the causal statements. In this study, a number of 97 by 97 squarematrices are developed and tested using UCINET 6 by comparing a subgroup’smatrix against the total matrix with all participants combined (a reference ma-trix). In the reference matrix, a value of 1 indicates a high expected correlationand 0 as a low expected correlation given by the results in the agreement matrixoutput in the consensus test (see Garro 1996). The matrices used to test againstthe reference are derived from sorting the data by the independent variable (e.g.,pharmacy staff, local client group, tourist group). QAP correlation evaluates howwell the data from the variable matrix fits the model given by the reference matrix.This is given by the statistic r. The level for rejecting the null hypothesis was set atp < .05.
Results
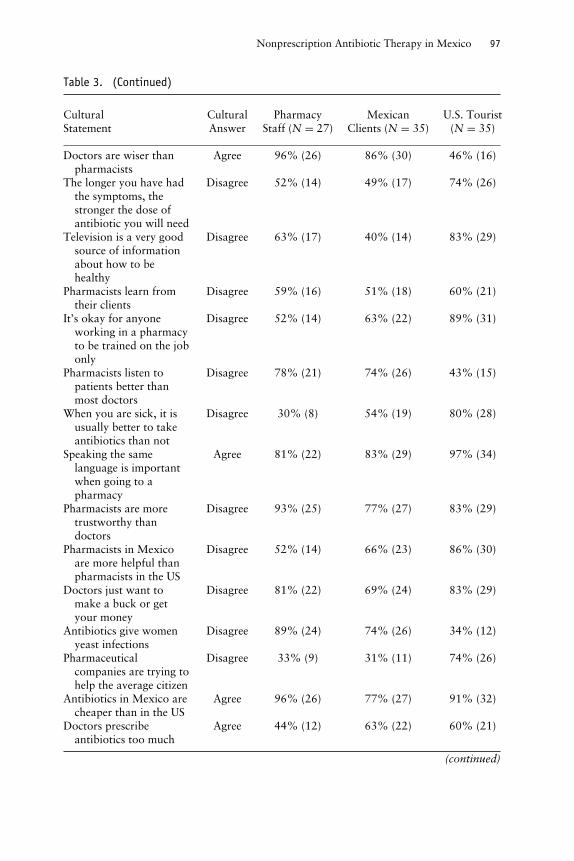
“Risky” knowledge (i.e., beliefs associated with behaviors known to promoteantibiotic resistance) varied slightly by group. Of the total sample, 16 percent be-lieved that antibiotics were a good treatment for asthma; this was much higher inMexican clients (29 percent) than U.S. ones (6 percent) (p < .05). When report-ing antibiotic use for colds, 57 percent of the total sample reported that this didnot have dangerous side effects, including 74 percent of the pharmacists. Thirty-eight percent of the total sample considered it acceptable to save antibiotics forlater use, including 52 percent of the pharmacists, and 37 percent of the total sam-ple reported that skipping an antibiotic dose did not affect its function, which ismuch higher in agreement among the pharmacists (70 percent) and the Mexicanclients (46 percent) than from the U.S. tourists (26 percent). There was consistentagreement that doctors are better as a first choice to provide medical attention;84 percent of our total sample agreed that going to the doctor is better than goingto the pharmacist and that doctors were more trustworthy (87 percent). More phar-macy staff (97 percent) agreed that doctors are the best source of knowledge versus60 percent of the tourist client sample and 71 percent of the local Mexican clientsample.
(1) Is saving or borrowing antibiotics and OTC predicted by group member-ship, occupation, and education?
94 Medical Anthropology Quarterly
Table 2. Self-Reported Behavior Regarding Antibiotic Use
Never Sometimes Often Always
I have saved antibiotics so I could use them laterPharmacists 4% (1) 63% (17) 22% (6) 11% (3)Mexican Clients 34% (12) 48% (17) 3% (1) 14% (5)U.S. Tourists 34% (12) 49% (17) 3% (1) 14% (5)
I have borrowed antibiotics from my friends or familyPharmacists 26% (7) 67% (18) 7% (2) 0Mexican Clients 40% (14) 51% (18) 6% (2) 3% (1)U.S. Tourists 40% (14) 51% (18) 6% (2) 3% (1)
I have purchased antibiotics over the counterPharmacists 0 67% (18) 19% (5) 15% (4)Mexican Clients 49% (17) 34% (12) 14% (5) 3% (1)U.S. Tourists 49% (17) 34% (12) 14% (5) 3% (1)
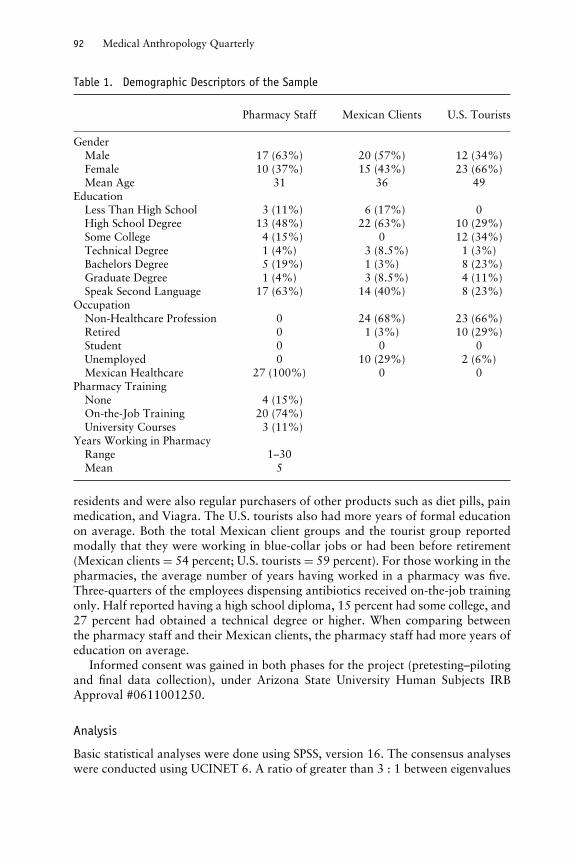
Table 2 describes reported antibiotic use patterns for the total sample and oursubgroups, based on participant reports. Our results reveal that local Mexican andU.S. tourist clients were not different in how they reported whether they saved(66 percent), borrowed (60 percent), or OTC-purchased (51 percent) antibioticsin the last 12 months. Curiously, local Mexicans and U.S. tourists reported similarbehavior patterns; we then checked these data again for entry errors and did not findany. Given the extensive piloting phase of the project, we argue that the questionswere not ambiguous; rather, a limitation of this finding may be the product of re-stricting respondents to too few response options. In addition, we did find variabilityin the pharmacy staff’s reporting of their behavior and are confident reporting theseresults.
Based on ANOVA tests (whereby Likert-type scales were converted to a continu-ous variable based on never = 0 and always = 3; see Table 2), we found that groupmembership (F[X, X] = 14.333, p < .05), education level (F[X, X] = 2.531, p <
.05), and occupation (F[X, X] = 3.444, p = < .05) were all associated with differentuse patterns within the sample. Post hoc Bonferoni test showed that pharmacistswere, in fact, more likely to engage in risky antibiotic use than their Mexican clientsor medical tourists (p = < .05). Between the clients themselves, we found that Mex-ican clients were more likely to engage in risky antibiotic use than the U.S. tourists(p = < .05). In addition, our data revealed that both Mexican clients and pharmacystaff reported twice the prevalence of antibiotic use in the previous year (mean = 2;range = 0–10) compared to those from the United States (mean = 1; range = 0–3).This difference was statistically significant according to a t test (p < .05).
(2) Is there a shared cultural model about antibiotic risk, and does it favorgeneral public health statements?
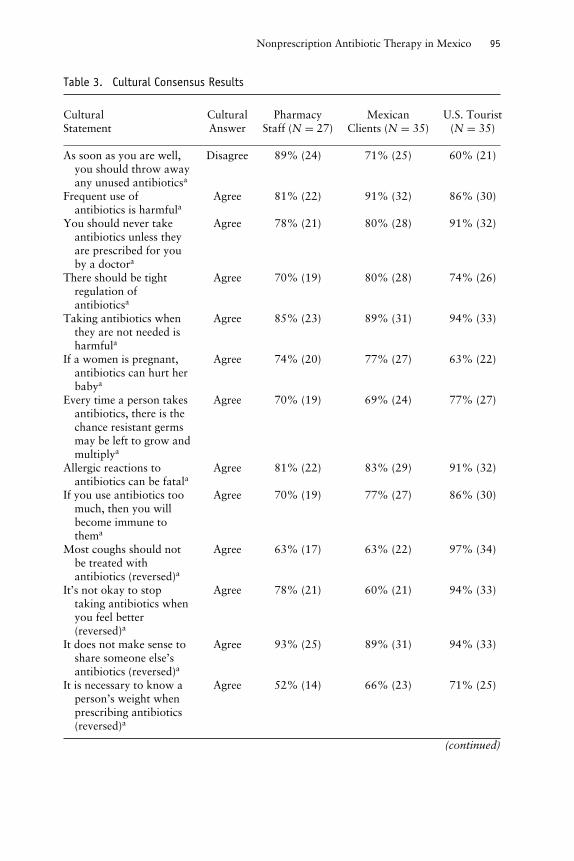
There is a shared model, and it does favor public health statements. The resultsof the consensus analysis showed agreement with a ratio 3.215 times the first andsecond eigenvalues. The responses by study groups are shown in Table 3, alongwith the list of statements and the percentages agreeing with the culturally correct
Nonprescription Antibiotic Therapy in Mexico 95
Table 3. Cultural Consensus Results
Cultural Cultural Pharmacy Mexican U.S. TouristStatement Answer Staff (N = 27) Clients (N = 35) (N = 35)
As soon as you are well,you should throw awayany unused antibioticsa
Disagree 89% (24) 71% (25) 60% (21)
Frequent use ofantibiotics is harmfula
Agree 81% (22) 91% (32) 86% (30)
You should never takeantibiotics unless theyare prescribed for youby a doctora
Agree 78% (21) 80% (28) 91% (32)
There should be tightregulation ofantibioticsa
Agree 70% (19) 80% (28) 74% (26)
Taking antibiotics whenthey are not needed isharmfula
Agree 85% (23) 89% (31) 94% (33)
If a women is pregnant,antibiotics can hurt herbabya
Agree 74% (20) 77% (27) 63% (22)
Every time a person takesantibiotics, there is thechance resistant germsmay be left to grow andmultiplya
Agree 70% (19) 69% (24) 77% (27)
Allergic reactions toantibiotics can be fatala
Agree 81% (22) 83% (29) 91% (32)
If you use antibiotics toomuch, then you willbecome immune tothema
Agree 70% (19) 77% (27) 86% (30)
Most coughs should notbe treated withantibiotics (reversed)a
Agree 63% (17) 63% (22) 97% (34)
It’s not okay to stoptaking antibiotics whenyou feel better(reversed)a
Agree 78% (21) 60% (21) 94% (33)
It does not make sense toshare someone else’santibiotics (reversed)a
Agree 93% (25) 89% (31) 94% (33)
It is necessary to know aperson’s weight whenprescribing antibiotics(reversed)a
Agree 52% (14) 66% (23) 71% (25)
(continued)
96 Medical Anthropology Quarterly
Table 3. (Continued)
Cultural Cultural Pharmacy Mexican U.S. TouristStatement Answer Staff (N = 27) Clients (N = 35) (N = 35)
Antibiotic resistance isone of the world’s mostpressing public healthproblemsa
Agree 59% (16) 74% (26) 74% (26)
Taking antibiotics forcolds has dangerousside effectsa
Disagree 74% (20) 54% (19) 49% (17)
Antibiotics should neverbe saved for next timeyou get sicka
Agree 48% (13) 40% (14) 74% (26)
If you skip an antibioticdose now and then, itwill not work ok(reversed)a
Agree 30% (8) 54% (19) 74% (26)
Antibiotics cannot beused to preventinfection (reversed)a
Agree 52% (14) 37% (13) 66% (23)
Antibiotics are not goodfor treating a fever(reversed)a
Agree 37% (10) 34% (12) 74% (26)
Antibiotics fix mostillnesses
Agree 59% (16) 66% (23) 40% (14)
Elderly need antibioticsmore often than otherpeople
Disagree 67% (18) 40% (14) 63% (22)
Antibiotics are good ifyou have asthma
Disagree 85% (23) 71% (25) 94% (33)
If you are very pale andsickly, you needantibiotics
Disagree 85% (23) 57% (20) 89% (31)
Penicillin is better thanother types ofantibiotics
Disagree 78% (21) 43% (15) 86% (30)
Diseases such as TB andchildhood earinfections are nowmore difficult to treatthan they were decadesago
Disagree 70% (19) 57% (20) 51% (18)
If you have pus, you needan antibiotic
Disagree 19% (5) 23% (8) 69% (24)
It is easy for a pharmacistto tell bacterial andviral infections apart
Disagree 67% (18) 40% (14) 69% (24)
(continued)
Nonprescription Antibiotic Therapy in Mexico 97
Table 3. (Continued)
Cultural Cultural Pharmacy Mexican U.S. TouristStatement Answer Staff (N = 27) Clients (N = 35) (N = 35)
Doctors are wiser thanpharmacists
Agree 96% (26) 86% (30) 46% (16)
The longer you have hadthe symptoms, thestronger the dose ofantibiotic you will need
Disagree 52% (14) 49% (17) 74% (26)
Television is a very goodsource of informationabout how to behealthy
Disagree 63% (17) 40% (14) 83% (29)
Pharmacists learn fromtheir clients
Disagree 59% (16) 51% (18) 60% (21)
It’s okay for anyoneworking in a pharmacyto be trained on the jobonly
Disagree 52% (14) 63% (22) 89% (31)
Pharmacists listen topatients better thanmost doctors
Disagree 78% (21) 74% (26) 43% (15)
When you are sick, it isusually better to takeantibiotics than not
Disagree 30% (8) 54% (19) 80% (28)
Speaking the samelanguage is importantwhen going to apharmacy
Agree 81% (22) 83% (29) 97% (34)
Pharmacists are moretrustworthy thandoctors
Disagree 93% (25) 77% (27) 83% (29)
Pharmacists in Mexicoare more helpful thanpharmacists in the US
Disagree 52% (14) 66% (23) 86% (30)
Doctors just want tomake a buck or getyour money
Disagree 81% (22) 69% (24) 83% (29)
Antibiotics give womenyeast infections
Disagree 89% (24) 74% (26) 34% (12)
Pharmaceuticalcompanies are trying tohelp the average citizen
Disagree 33% (9) 31% (11) 74% (26)
Antibiotics in Mexico arecheaper than in the US
Agree 96% (26) 77% (27) 91% (32)
Doctors prescribeantibiotics too much
Agree 44% (12) 63% (22) 60% (21)
(continued)
98 Medical Anthropology Quarterly
Table 3. (Continued)
Cultural Cultural Pharmacy Mexican U.S. TouristStatement Answer Staff (N = 27) Clients (N = 35) (N = 35)
Doctors need to prescribeantibiotics more oftento children
Disagree 70% (19) 63% (22) 86% (30)
Doctors must give amother a prescriptionfor her child if shereally wants one
Disagree 70% (19) 46% (16) 89% (31)
Pharmacists learn fromone another
Agree 56% (15) 71% (25) 89% (31)
Antibiotics are stronger inMexico than in the US
Disagree 70% (19) 63% (22) 94% (33)
Taking antibiotics whenyou are young builds astrong immune system
Disagree 85% (23) 77% (27) 94% (33)
You should eat yogurtwhen you are takingantibiotics
Disagree 70% (19) 46% (16) 71% (25)
Antibiotics improve theblood
Disagree 93% (25) 74% (26) 89% (31)
Some antibiotics make mefeel nauseous or dizzy
Agree 93% (25) 60% (21) 49% (17)
The customer is alwaysright
Disagree 67% (18) 77% (27) 83% (29)
Antibiotics are better forhot illnesses than coldones
Disagree 85% (23) 74% (26) 86% (30)
Animals raised for foodshould not be givenantibiotics
Agree 41% (11) 57% (20) 74% (26)
Bad reactions toantibiotics are verycommon
Agree 70% (19) 80% (28) 51% (18)
Viruses are living cells Agree 85% (23) 80% (28) 86% (30)Antibiotics give me
diarrheaDisagree 63% (17) 80% (28) 69% (24)
Antibiotics are purer inthe US than in Mexico
Disagree 100% (27) 71% (25) 69% (24)
Look at the color of thethroat to see if there isa bacterial or viralinfection
Disagree 30% (8) 31% (11) 69% (24)
Generally, going to thepharmacy is as good asgoing to the doctor
Disagree 81% (22) 71% (25) 86% (30)
(continued)
Nonprescription Antibiotic Therapy in Mexico 99
Table 3. (Continued)
Cultural Cultural Pharmacy Mexican U.S. TouristStatement Answer Staff (N = 27) Clients (N = 35) (N = 35)
Pharmacists should notrefuse to sell anantibiotic over thecounter even if theythink it is not needed
Disagree 63% (17) 54% (19) 63% (22)
Doctors are the bestsource of knowledgeabout how to behealthy
Agree 96% (26) 71% (25) 60% (21)
Pharmacists should beable to recommendantibiotics withoutgovernment oversights
Disagree 63% (17) 71% (25) 77% (27)
Doctors recommendantibiotics becausepharmaceuticals givethem lots of samples
Disagree 70% (19) 57% (20) 66% (23)
If a pharmacist refuses tosell antibiotics, apatient has the right toget angry
Disagree 56% (15) 71% (25) 71% (25)
Antibiotics kill bacteria Agree 81% (22) 89% (31) 77% (27)Antibiotics help you get
better fasterAgree 93% (25) 83% (29) 89% (31)
Anyone working at apharmacy countershould have specializedtraining in pharmacyschool
Agree 96% (26) 94% (33) 83% (29)
Antibiotics are a magicalcure
Disagree 81% (22) 69% (24) 86% (30)
Note. aPublic Health Statements.
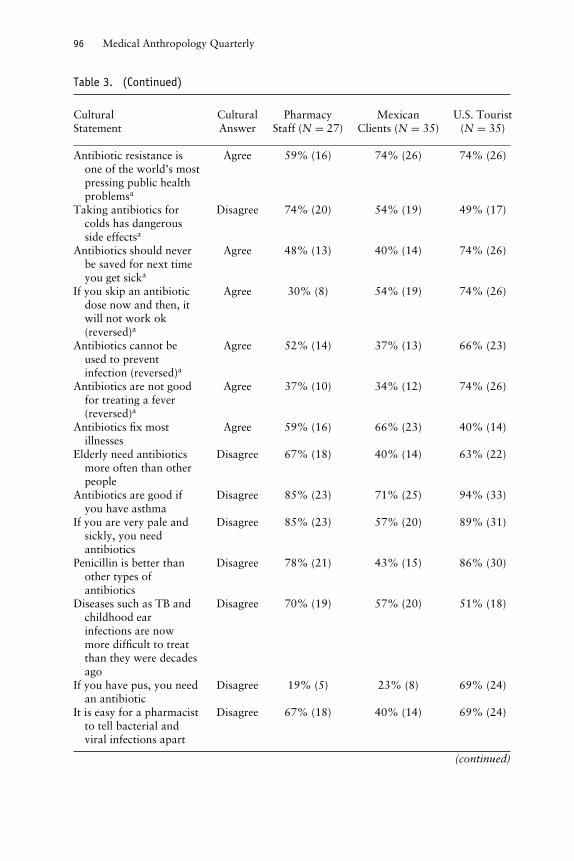
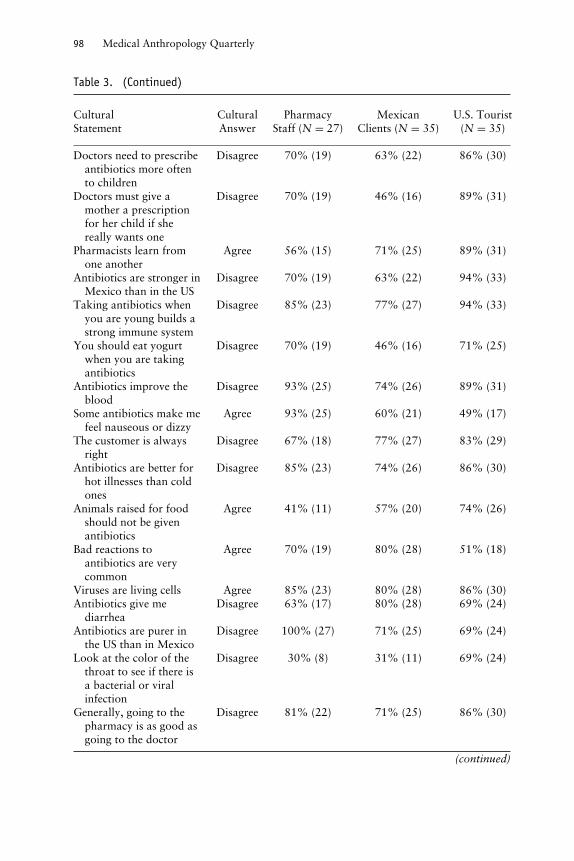
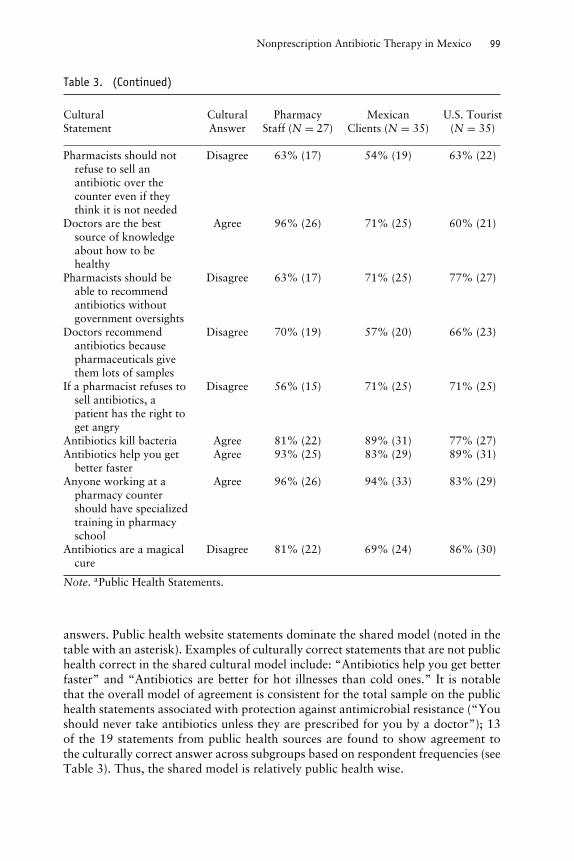
answers. Public health website statements dominate the shared model (noted in thetable with an asterisk). Examples of culturally correct statements that are not publichealth correct in the shared cultural model include: “Antibiotics help you get betterfaster” and “Antibiotics are better for hot illnesses than cold ones.” It is notablethat the overall model of agreement is consistent for the total sample on the publichealth statements associated with protection against antimicrobial resistance (“Youshould never take antibiotics unless they are prescribed for you by a doctor”); 13of the 19 statements from public health sources are found to show agreement tothe culturally correct answer across subgroups based on respondent frequencies (seeTable 3). Thus, the shared model is relatively public health wise.
100 Medical Anthropology Quarterly
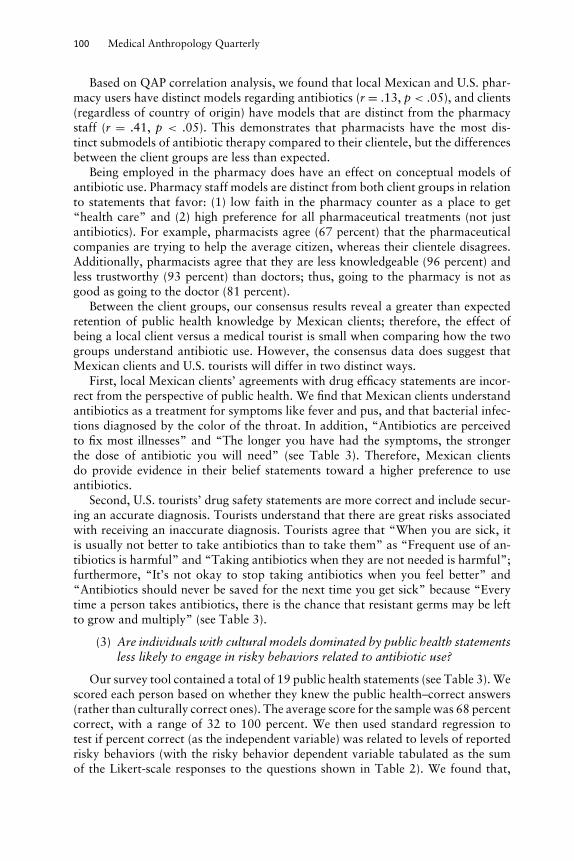
Based on QAP correlation analysis, we found that local Mexican and U.S. phar-macy users have distinct models regarding antibiotics (r = .13, p < .05), and clients(regardless of country of origin) have models that are distinct from the pharmacystaff (r = .41, p < .05). This demonstrates that pharmacists have the most dis-tinct submodels of antibiotic therapy compared to their clientele, but the differencesbetween the client groups are less than expected.
Being employed in the pharmacy does have an effect on conceptual models ofantibiotic use. Pharmacy staff models are distinct from both client groups in relationto statements that favor: (1) low faith in the pharmacy counter as a place to get“health care” and (2) high preference for all pharmaceutical treatments (not justantibiotics). For example, pharmacists agree (67 percent) that the pharmaceuticalcompanies are trying to help the average citizen, whereas their clientele disagrees.Additionally, pharmacists agree that they are less knowledgeable (96 percent) andless trustworthy (93 percent) than doctors; thus, going to the pharmacy is not asgood as going to the doctor (81 percent).
Between the client groups, our consensus results reveal a greater than expectedretention of public health knowledge by Mexican clients; therefore, the effect ofbeing a local client versus a medical tourist is small when comparing how the twogroups understand antibiotic use. However, the consensus data does suggest thatMexican clients and U.S. tourists will differ in two distinct ways.
First, local Mexican clients’ agreements with drug efficacy statements are incor-rect from the perspective of public health. We find that Mexican clients understandantibiotics as a treatment for symptoms like fever and pus, and that bacterial infec-tions diagnosed by the color of the throat. In addition, “Antibiotics are perceivedto fix most illnesses” and “The longer you have had the symptoms, the strongerthe dose of antibiotic you will need” (see Table 3). Therefore, Mexican clientsdo provide evidence in their belief statements toward a higher preference to useantibiotics.
Second, U.S. tourists’ drug safety statements are more correct and include secur-ing an accurate diagnosis. Tourists understand that there are great risks associatedwith receiving an inaccurate diagnosis. Tourists agree that “When you are sick, itis usually not better to take antibiotics than to take them” as “Frequent use of an-tibiotics is harmful” and “Taking antibiotics when they are not needed is harmful”;furthermore, “It’s not okay to stop taking antibiotics when you feel better” and“Antibiotics should never be saved for the next time you get sick” because “Everytime a person takes antibiotics, there is the chance that resistant germs may be leftto grow and multiply” (see Table 3).
(3) Are individuals with cultural models dominated by public health statementsless likely to engage in risky behaviors related to antibiotic use?
Our survey tool contained a total of 19 public health statements (see Table 3). Wescored each person based on whether they knew the public health–correct answers(rather than culturally correct ones). The average score for the sample was 68 percentcorrect, with a range of 32 to 100 percent. We then used standard regression totest if percent correct (as the independent variable) was related to levels of reportedrisky behaviors (with the risky behavior dependent variable tabulated as the sumof the Likert-scale responses to the questions shown in Table 2). We found that,

Nonprescription Antibiotic Therapy in Mexico 101
indeed, those with lower percentages of public health–correct answers to those 19statements were predicted to have higher scores for risky antibiotic behavior; therelationship was, however, not particularly strong (R2 = 0.08, p < .05).
Discussion and Conclusion
The pharmacy counters of the U.S.–Mexico border are a place where OTC antibioticpurchase is not only common, unregulated, and illegal, but also de facto toleratedand encouraged. The pharmacy counters are a place where cultural models andrelated lay medical decisions regarding antibiotic use are expressed, negotiated,and acted on. This study suggests that the substantive healing power ascribed toantibiotic drugs that has been observed in other ethnographic studies is being playedout to full effect in the bordertown pharmacies of Nogales and across all three studygroups. Even at the pharmacy counter, we see that the client is often engaging inself-medication, a pattern described previously in a range of studies (see Finerman1989; Hardon 1987; van der Geest 1982, 1988; van der Geest and White 1988)and the practice of self-medication is certainly condoned by the pharmacy staff.
Particularly, our results reflect a widespread set of beliefs related to the perceivedright to use antibiotics regardless of prescription. The domains of knowledge thatvaried across groups were more related to the use and utility of antibiotics inpersonal healing. As expected, Mexican clients found more health-related uses forantibiotics (for wider range of conditions) than did the tourist counterparts. ThatMexican clients were more likely to engage in risky antibiotic use and reportedtwice the use of antibiotics than the U.S. tourists are very compelling findings. Bothgroups of clientele report the same patterns of risky antibiotic behavior, which weadmit is ironic, but the fact that Mexicans use antibiotics more often during a year,and hence they engage in risky behavior more often, is not so surprising. BecauseMexican clients have regular access to OTC antibiotics and a preference to useantibiotics for a variety of symptoms, it stands to reason that those with the mostaccess to the border pharmacies and unregulated purchasing will engage in riskybehavior. It also stands to reason that U.S. tourists seek border pharmacies for thespecific purpose to purchase OTC antibiotics, which might provide further insightinto why both groups report similar behaviors, and this should be considered infuture inquiries.
That the pharmacy staff also engages in the risky behaviors is perhaps a moresurprising finding, and one that provides some important clues as to why pharmacystaff might not be acting as a critical filter between client beliefs and practices (i.e.,not acting via counseling as a preventive mechanism between the desire of clientsto obtain antibiotics and their purchase of them). This study found, as have others,that pharmacy staff and clients all conceptualize the exchange of medicines in termsof sales, rather than in health care terms, and the limited background training ofpharmacy staff fits with the perception on both sides of the counter that their rolein the transaction is to provide the client with what they wish to purchase, ratherthan to counsel.
Although this suggests some real challenges from a health education perspec-tive to curtailing inappropriate antibiotic use, this study also, importantly, found apositive relationship between risk knowledge and reduction in risky behavior with

102 Medical Anthropology Quarterly
regard to antibiotic usage. In this case, levels of public health knowledge aboutantibiotic risks did predict lower overall levels of antibiotic saving, sharing, andOTC purchasing across and within all groups. This is significant when consideringthe current opportunity—and the need—for high-level public health officials to reachconsumers and pharmaceutical sales personnel regarding appropriate antibioticusage.
Theoretically, it is critical to work to understand better how social meanings, notjust cultural knowledge, are applied to antibiotic use (see, e.g., Oldani 2004; Sachsand Tomson 1992; Schwartz 2002; van der Geest and White 1988) if we are to workfor safe and effective application of drugs within and across countries. The resultsof this study point to the immediacy of a concerted effort on the part of binationalpublic health organizations, the pharmaceutical industry, and consumers to addressissues related to “risky” antibiotic behavior. Ethnographic research conducted in thepopular pharmaceutical–tourist districts of Tijuana and Ensenada directly after theanthrax scare of 2001 revealed an alarming number of pharmacists displaying ban-ners proclaiming “Prevent Anthrax; Buy Cipro Cheap.” Ciproflaxin, an antibioticrequiring prescription in the United States, is often used as the drug of last resort incases of antibiotic resistance; it is readily available over the counter in Mexico. U.S.tourists, concerned with the possibility of an antibiotic shortage in the case of ananthrax “epidemic,” visited Mexican pharmacies to stock up on “Cipro.” AlthoughMexican pharmacists were promoting the sale of “Cipro,” Mexican consumers weremuch less concerned with contracting anthrax than were Americans, according tointerviews conducted with the pharmacists. Fear of a shortage of Ciproflaxin in theUnited States and the refusal of physicians to prescribe prophylactic antibiotics to“prevent” anthrax led Americans to cross the border to hoard these antibiotics.“Cipro” was displayed in pharmacy windows and sold in boxes of 10 or 12 to U.S.tourists.
On the basis of prior ethnographic research (Schwartz 2004) and our observa-tions at the counter during this study, we would suggest that the perspectives ofthe pharmacists and staff concerning the drugs they sell provide a new dimensionin understanding antibiotic purchasing and use within a broader framework thatintegrates pharmaceuticals as commodities not solely as therapeutic agents (Kamatand Nichter 1998; Oldani 2004). Today, we are dealing with a very real publichealth threat—the possibility of antimicrobial resistance related to antibiotic mis-and overuse (Barbosa and Levy 2000; Cars et al. 2001; Levy 1998, 2005; Wise et al.1998)—and the very real need for consumers and health care providers to makeinformed decisions about antibiotic therapy.
Much of the current recommendations regarding how to reduce global antibioticmisuse focus on the centrality of the primary care providers as the “front lines ofthe battle” (Planta 2007:538). In this case, no “primary care providers” occupythe “front lines,” but there are front lines—including the many pharmacy countersthat line the U.S.–Mexico border. Pharmacy employees do possess “safe” knowl-edge about antibiotic use; however, this knowledge is rarely transmitted betweenpharmacy employees and clients because the staff does not view that transmittalas a critical element in the role of pharmacy encounter. Instead, border pharmacyemployees view their role as one of vendor including negotiating or bargainingwith potential clients who reinforce this relationship as they bargain to achieve a

Nonprescription Antibiotic Therapy in Mexico 103
lower price for the medicines requested. In the end, both buyer and seller believein the fundamental right to purchase drugs over the counter without the need, orrequirement, for information concerning medical compliance or medical efficacy. Ifthe misuse of antibiotics is to be addressed on the “front lines,” then the pharmacyemployees must alter their self-image from that of seller of medications to includethat of an informed medical consultant.
References Cited
Adetunji, J. A.1991 Response of Parents to Five Killer Diseases among Children in a Yoruba Commu-
nity, Nigeria. Social Science and Medicine 32:1379–1387.Barbosa, T. M., and S. B. Levy
2000 The Impact of Antibiotic Use on Resistance Development and Persistence. DrugResistance Updates 3(5):303–311.
Barry, M.2003 Diseases without Borders: Globalization’s Challenge to the American Society of
Tropical Medicine and Hygiene: A Call for Public Advocacy and Activism. AmericanJournal of Tropical Medicine and Hygiene 69:3–7.
Belongia, E. A., T. S. Naimi, C. M. Gale, and R. E. Besser2002 Antibiotic Use and Upper Respiratory Infections: A Survey of Knowledge, Atti-
tudes, and Experiences in Wisconsin and Minnesota. Preventive Medicine 34(3):346–352.
Berzanskyte, A., R. Valinteliene, F. M. Haaijer-Ruskamp, R. Gurevicius, and L. Grigoryan2006 Self-Medication with Antibiotics in Lithuania. International Journal of Occupa-
tional Medicine and Environmental Health 19(4):147–156.Bojalil, R., and J. J. Calva
1994 Antibiotic Misuse in Diarrhea. A Household Survey in a Mexican Community.Journal of Clinical Epidemiology 47(2):147–156.
Bolanos, H.2005 Responsible Self-Medication in Latin America. Drug Information Journal 39:99–
107.Brewis, A., and M. Gartin
2006 Biocultural Constructions of Obesogenic Ecologies of Childhood: Parental Feedingversus Young Child Eating Strategies. American Journal of Human Biology 18:203–213.
Byarugaba, D. K.2004 Antimicrobial Resistance in Developing Countries and Responsible Risk Factors.
International Journal of Antimicrobial Agents 24:105–110.Calva, J.
1996 Antibiotic Use in a Periurban Community in Mexico: A Household and DrugstoreSurvey. Social Science and Medicine 47(8):1121–1128.
Calvillo, J. P., and L. Lal2003 Pilot Study of a Survey of U.S. Residents Purchasing Medications in Mexico:
Demographics, Reasons, and Types of Medications Purchased. Clinical Therapeutics25(2):561–577.
Cars, O., S. Molstad, and A. Melander2001 Variation in Antibiotic Use in the European Union. Lancet 357(9271):1851–1853.
Casner, P. R., and L. G. Guerra1992 Purchasing Prescription Medication in Mexico Without a Prescription: The Expe-
rience at the Border. Western Journal of Medicine 156(5):512–516.

104 Medical Anthropology Quarterly
Cespedes, A., and E. Larson2006 Knowledge, Attitudes, and Practices Regarding Antibiotic Use among Latinos in
the United States: Review and Recommendations. American Journal of InfectionControl 34:495–502.
Chavez, L. R.1984 Doctors, Curanderos, and Brujas: Health Care Delivery and Mexican Immigrants
in San Diego. Medical Anthropology Quarterly 15(2):31–37.Corbett, K. K., R. Gonzales, B. A. Leeman-Castillo, E. Flores, J. Maselli, and K. Kafadar
2005 Appropriate Antibiotic Use: Variation in Knowledge and Awareness by HispanicEthnicity and Language. Preventative Medicine 40(2):162–169.
Curry, M., H. F. Mathews, H. J. Daniel III, J. C. Johnson, and C. J. Mansfield2002 Beliefs about and Response to Childhood Ear Infections: A Study of Parents in
Eastern North Carolina. Social Science and Medicine 54:1153–1165.Dressler, W., G. Grell, and F. E. Viteri
1995 Intracultural Diversity and the Sociocultural Correlates of Blood Pressure: A Ja-maican Example. Medical Anthropology Quarterly 9(3):291–313.
Finerman, R.1989 Tracing Home-Based Health Care Change in an Andean Indian Community.
Medical Anthropology Quarterly 3(2):162–174.Furlow, C. A.
2003 Comparing Indicators of Knowledge within and between Cultural Domains. FieldMethods 15:51–63.
Garro, L. C.1996 Intracultural Variation in Causal Accounts of Diabetes: A Comparison
of Three Canadian Communities. Culture, Medicine, and Psychiatry 20:381–420.
Grigoryan, L., F. M. Haaijer-Ruskamp, J. G. M. Burgerhof, R. Mechtler, R. Deschepper,A. Tambic-Andrasevic, R. Andrajati, D. L. Monnet, R. Cunney, A. Di Matteo, H.Edelstein, R. Valinteliene, A. Alkerwi, E. A. Scicluna, P. Grzesiowski, A. Bara, T.Tesar, M. Cizman, J. Campos, C. Stalsby Lundborg, and J. Birkin
2006 Self-Medication with Antimicrobial Drugs in Europe. Emerging Infectious Diseases12(3):452–459.
Guerrant, R. L.1998 Why America Must Care About Tropical Medicine: Threats to Global Health and
Security from Tropical Infectious Diseases. American Journal of Tropical Medicineand Hygiene 59:3–16.
Guillemot, D., C. Carbon, B. Balkau, P. Geslin, H. Lecoeur, F. Vauzelle-Kervroedan, G.Bouvenot, and E. Eschwege
1998 Low Dosage and Long-Term Treatment of Betalactam: Risk Factors for Carriageof Penicillin Resistant Streptococcus Pneumonia. Journal of the American MedicalAssociation 279:365–370.
Hardon, A. P.1987 The Use of Modern Pharmaceuticals in a Filipino Village: Doctor’s Prescription
and Self-Medication. Social Science and Medicine 25:279–281.Hubert, L., and J. V. Schultz
1976 Quadratic Assignment as a General Data Analysis Strategy. British Journal ofMathematical and Statistical Psychology 29:190–241.
Kamat, V. R., and M. Nichter1998 Pharmacies, Self-Medication and Pharmaceutical Marketing in Bombay, India.
Social Science and Medicine 47(6):779–794.Kristiansson, C., M. Reilly, E. Gotuzzo, H. Rodriguez, A. Bartoloni, A. Thorson, T. Falken-
berg, F. Bartalesi, G. Tomson, and M. Larsson

Nonprescription Antibiotic Therapy in Mexico 105
2008 Antibiotic Use and Health-Seeking Behavior in an Underprivileged Area of Peru.Tropical Medicine and International Health 13(3):434–441.
Larson, E. L., J. Dilone, M. Garcia, and J. Smolowitz2006 Factors Which Influence Latino Community Members to Self-Prescribe Antibi-
otics. Nursing Research 55(2):94–102.Larson, E. L., S. Lin, and C. Gomez-Durate
2003 Antibiotic Use in Hispanic Households: New York City. Emerging InfectiousDiseases 9(9):1096–1102.
Levy, S.1998 The Challenge of Antibiotic Resistance. Scientific American 278(3):46–53.2005 Antibiotic Resistance: The Problem Intensifies. Advanced Drug Delivery Reviews
57(10):1446–1450.Logan, K.
1983 The Role of Pharmacists and Over the Counter Medications in the Health CareSystem of a Mexican City. Medical Anthropology Summer 1983:68–87.
Macias, E. P., and L. S. Morales2001 Crossing the Border for Health Care. Journal of Health Care for the Poor and
Underserved 12(1):77–87.Maiman L. A., M. H. Becker, and A. W. Kalic
1986 Correlates of Mothers’ Use of Medications for Their Children. Social Science andMedicine 22:41–51.
Mainous, A. G. III, A. Y. Cheng, R. C. Garr, B. C. Tilley, C. J. Everett, and M. D. McKee2005 Nonprescribed Antimicrobial Drugs in Latino Community, South Carolina.
Emerging Infectious Diseases 11(6):883–888.McKee, M. D., L. Mills, and A. G. Mainous III
1999 Antibiotic Use for the Treatment of Upper Respiratory Infections in a DiverseCommunity. Journal of Family Practice 48(12):993–996.
McKeithan, K. E., and M. D. Shepherd1996 Pharmaceutical Products Declared by US Residents on Returning to the United
States from Mexico. Clinical Therapeutics 18(6):1242–1251.Nichter, Mark, and Nancy Vuckovic
1994 Agenda for an Anthropology of Pharmaceutical Practice. Social Science andMedicine 39(11):1509–1525.
Okeke, I. N., A. Lamikanra, and R. Edelman1999 Socioeconomic and Behavioral Factors Leading to the Acquired Bacterial Resis-
tance to Antibiotics in Developing Countries. Emerging Infectious Diseases 5(1):18–26.
Oldani, M. J.2004 Thick Prescriptions: Toward an Interpretation of Pharmaceutical Sales Practices.
Medical Anthropology Quarterly 18(3):325–356.Pachter, L. M., S. Weller, R. Baer, A. Garcia de Garcia, R. Trotter II, M. Glazer, and R.
Klein2002 Variation in Asthma Beliefs and Practices among Mainland Puerto Ricans,
Mexican-Americans, Mexicans, and Guatemalans. Journal of Asthma: Official Jour-nal of the Association for the Care of Asthma 39(2):119–134.
Paladino, J. A., J. L. Sunderlin, C. S. Price, and J. J. Schentag2002 Economic Consequences of Antimicrobial Resistance. Surgical Infection 3:259–
267.Pechere, J. C.
2001 Patients’ Interviews and Misuse of Antibiotics. Clinical Infectious Diseases: AnOfficial Publication of the Infectious Diseases Society of America 33(Supp. 3):170–173.

106 Medical Anthropology Quarterly
Pelto, P. J., and G. H. Pelto1997 Studying Knowledge, Culture, and Behavior in Applied Medical Anthropology.
Medical Anthropology Quarterly 11(2):147–163.Petryna, A., and A. Kleinman
2006 The Pharmaceutical Nexus. In Global Pharmaceuticals: Ethics, Markets, Practices.Adriana Petryna, Andrew Lakoff, and Arthur Kleinman, eds. Pp. 1–32. Durham, NC:Duke University Press.
Planta, M. B.2007 The Role of Poverty in Antimicrobial Resistance. Journal of the American Board
of Family Medicine 20:533–539.Pylypa, J.
2001 Self-Medication Practices in Two California Mexican Communities. Journal ofImmigrant Health 3(2):59–75.
Richards, L.1999 Using NVivo in Qualitative Research. London: Sage.
Romney, A. K., S. C. Weller, and W. H. Batchelder1986 Culture and Consensus: A Theory of Culture as Information Accuracy. American
Anthropologist 88:313–338.Sachs, L., and G. Tomson
1992 Medicines and Culture: A Double Perspective on Drug Utilization in a DevelopingCountry. Social Science and Medicine 34(3):307–315.
Schwartz, N. A.2002 Medical Compliance and Childhood Asthma on the Mexican Border: “They Think
You Are God.” Frontera Norte 14:155–179.2004 Childhood Asthma on the Northern Mexico Border. Medical Anthropology Quar-
terly 18(2):214–229.Schwartz, N. A., and R. Casillas-Miranda
1998 Letters to the Editor, Antibiotic Prescribing and Respiratory Tract Infections.Journal of the American Medical Association 279(4):271–272.
Schwartz, N. A., and D. R. Pepper2009 Childhood Asthma, Air Quality, and Social Suffering among Mexican Americans
in the San Joaquin Valley: “Nobody Talks to Us Here.” Medical Anthropology28(4):336–367.
Trostle, J.1999 Inappropriate Distribution of Medicines by Professionals in Developing Countries.
Social Science and Medicine 42(8):1117–1120.van der Geest, S.
1982 The Illegal Distribution of Western Medicines in Developing Countries: Pharma-cists, Drug Peddlers, Injection Doctors and Others: A Bibliographic Exploration.Medical Anthropology 6:197–219.
1988 Self-Care and the Informal Sale of Drugs in South Cameron. Social Science andMedicine 25(3):293–305.
van der Geest, S., and S. R. White, eds.1988 The Context of Medicines in Developing Countries. Dordrecht, the Netherlands:
Kluwer Academic.Vuckovic, Nancy
1999 Fast Relief: Buying Time with Medications. Medical Anthropology Quarterly13(1):51–68.
Vuckovic, Nancy, and Mark Nichter1997 Changing Patterns of Pharmaceutical Practice in the United States. Social Science
and Medicine 44(9):1285–1302.
Nonprescription Antibiotic Therapy in Mexico 107
Weller, S. C.2007 Cultural Consensus Theory: Applications and Frequently Asked Questions. Field
Methods 19(4):339–368.Wise, R., T. Hart, O. Cars, M. Streulens, R. Helmuth, P. Huovinen, and M. Sprenger
1998 Antimicrobial Resistance is a Major Threat to Public Health. British MedicalJournal 317(7159):609–610.
WHO2000 Report on Infectious Diseases. Geneva: WHO.2001 WHO Global Strategy for Containment of Antimicrobial Resistance. Geneva:
WHO.





























