Embed Size (px)
Citation preview

Interrelationship of Pulp and Systemic Disease
Fig 20-1 Evaluation of the presence of HIV in human dental pulp using in situ hybridization histochemistry. Dental pulp tissue from an HIV-positive patient was fixed, sectioned, and incubated with one of two biotinylated oligonucleotide probes complementary to a region of messenger RNA specific to HIV. Sections were incubated, washed, and developed. A positive signal is visible as a dark spot in the figure. (Reprinted from Glick et al'5 with permission.)
Several oral lesions have been shown to occur
in association with HIV-induced immunosuppres
sion.9-11 The most strongly associated lesions in adult patients are mucosa! and include candidia
sis (erythematous and pseudomembranous), hairy
leukoplakia, Kaposi sarcoma, non-Hodgkin lym
phoma, and periodontal disease (linear gingival
erythema, necrotizing ulcerative gingivitis, and nec
rotizing ulcerative periodontitis).12 For pediatric pa
tients, the most strongly associated lesions are can
didiasis (erythematous, pseudomembranous, and
angular cheilitis), herpes simplex infection, linear
gingival erythema, parotid enlargement, and recurrent aphthous stomatitis (minor, major, and herpetiform). The risk of developing these lesions is inverse
ly related to the CD4+ counts. Thus, the presence of
oral lesions may serve as good clinical markers to
signal a loss in therapeutic efficacy of ART.13·14
Although HIV has been identified in dental
pulp15 and in periradicular lesions of pulpal origin,16
its direct contribution to pulpal disease remains
unknown (Fig 20-1 ). Studies to assess the caries risk in HIV-infected patients have yielded conflict
ing results, and it is likely that numerous factors, such as the patient's immune status, dietary habits, medication profile, and salivary status, all contribute
to caries risk.17-19 The impaired immune response observed in patients with low CD4+ counts does not appear to be associated with an increase in endo
dontic complications after root canal treatment,20·21 and three recent studies have confirmed that HIV
infected patients respond well to and benefit from
indicated root canal therapy.22-24
472
Herpesvirus infections
Herpesviruses are ubiquitous pathogens that have
the ability to establish latency in the infected host.25
There are eight identified human herpesviruses: her
pes simplex virus 1 (HSV-1), herpes simplex virus 2
(HSV-2), varicella zoster virus (VZV), Epstein-Barr virus
(EBV), cytomegalovirus (CMV), human herpesvirus 6,
human herpesvirus 7, and human herpesvirus 8.26 Pri
mary infections are often asymptomatic and typically
occur during childhood.
The pathophysiology of HSV-1 viral infection is
well established. During the primary infection, the
virus is transported via retrograde axonal transport
to regional sensory ganglia (typically the trigeminal
ganglia), where it establishes latency.27 During the
latent phase, the virus exists in a quiescent immuno
logically shielded state. However, shedding of HSV
has been demonstrated in the saliva of asympto
matic healthy adults. Although the clinical relevance of this finding remains to be determined, it reinforces
the need for strict adherence to infection-control
procedures in the dental office to minimize the risk
of occupational exposure.26
Clinically apparent recurrent infections are esti
mated to occur in 15% to 40% of individuals har
boring latent HSV-1.28 Well-documented triggers
associated with HSV recurrence include sunlight,
trauma, menstruation, fever, immunosuppression,
decompression of the trigeminal nerve, and irritation
by dental instruments. Three clinical forms of recur
rence are recognized: (1) recurrent herpes labialis, (2) intraoral recurrence, and (3) recurrence mimicking
a primary infection. lntraoral recurrent lesions typi
cally present as a focal clustering of vesicles affect
ing the keratinized mucosa (gingiva or hard palate).
The vesicles quickly rupture and coalesce to form
the characteristic shallow erosion. The pain may be
so severe as to interfere with eating and speaking.
HSV-1 infection has been proposed as a potential etiologic factor of pulpal necrosis and should be
considered in the differential diagnosis of odontalgia (see chapter 19). However, the overall impact of
HSV infection on pulpal disease remains unknown. In one study assessing 31 patients with an apical abscess or cellulitis of pulpal origin, HSV was detected (using polymerase chain reaction) in only 1 of 31 specimens.29 In contrast, another study revealed the
presence of HSV in 15 of 50 necrotic pulps assessed by polymerase chain reaction.30
www.shayanNemodar.com
Infectious Diseases
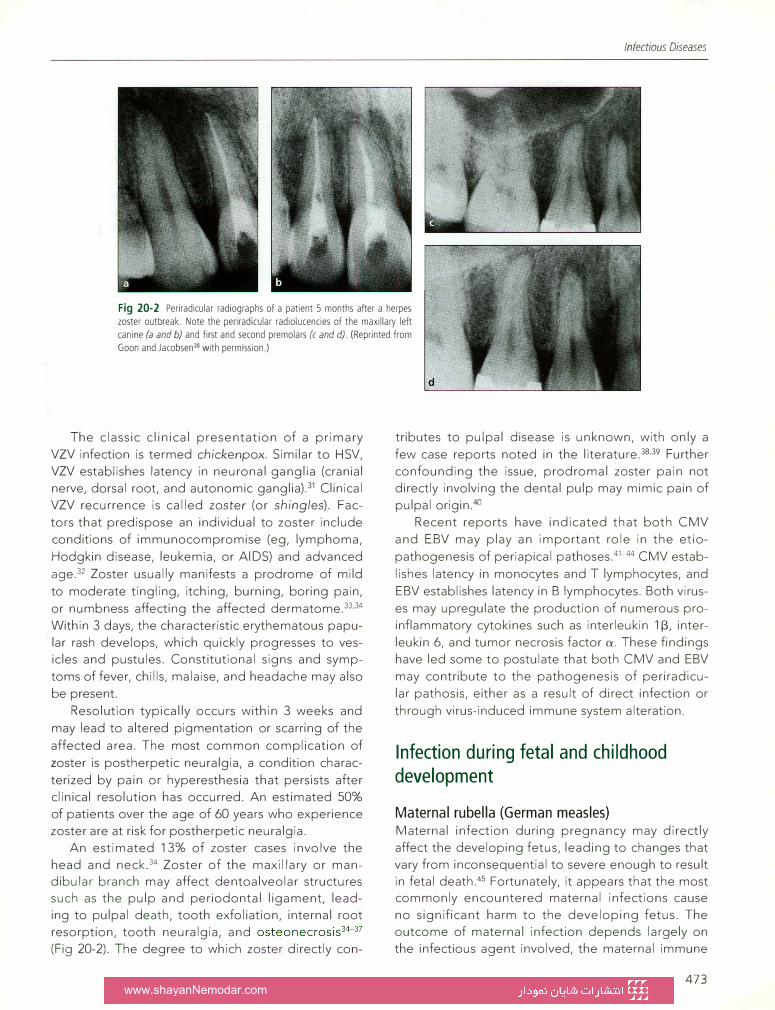
Fig 20-2 Periradicular radiographs of a patient 5 months after a herpes
zoster outbreak. Note the periradicular radiolucencies of the maxillary left
canine (a and b) and first and second premolars (c and d). (Reprinted from
Goon and Jacobsen38 with permission.)
The classic clinical presentation of a primary VZV infection is termed chickenpox. Similar to HSV, VZV establishes latency in neuronal ganglia (cranial nerve, dorsal root, and autonomic ganglia).31 Clinical VZV recurrence is called zoster (or shingles). Fac
tors that predispose an individual to zoster include conditions of immunocompromise (eg, lymphoma,
Hodgkin disease, leukemia, or AIDS) and advanced
age.32 Zoster usually manifests a prodrome of mild
to moderate tingling, itching, burning, boring pain,
or numbness affecting the affected dermatome.33·34 Within 3 days, the characteristic erythematous papular rash develops, which quickly progresses to vesicles and pustules. Constitutional signs and symp
toms of fever, chills, malaise, and headache may also
be present.
Resolution typically occurs within 3 weeks and
may lead to altered pigmentation or scarring of the
affected area. The most common complication of
zoster is postherpetic neuralgia, a condition charac
terized by pain or hyperesthesia that persists after clinical resolution has occurred. An estimated 50% of patients over the age of 60 years who experience zoster are at risk for postherpetic neuralgia.
An estimated 13% of zoster cases involve the head and neck.34 Zoster of the maxillary or mandibular branch may affect dentoalveolar structures such as the pulp and periodontal ligament, leading to pulpal death, tooth exfoliation, internal root resorption, tooth neuralgia, and osteonecrosis34-37 (Fig 20-2). The degree to which zoster directly con-
d
tributes to pulpal disease is unknown, with only a
few case reports noted in the literature.38·39 Further confounding the issue, prodromal zoster pain not directly involving the dental pulp may mimic pain of pulpal origin.40
Recent reports have indicated that both CMV and EBV may play an important role in the etio
pathogenesis of periapical pathoses.41-44 CMV estab
lishes latency in monocytes and T lymphocytes, and
EBV establishes latency in B lymphocytes. Both virus
es may upregulate the production of numerous proinflammatory cytokines such as interleukin 113, interleukin 6, and tumor necrosis factor a. These findings have led some to postulate that both CMV and EBV may contribute to the pathogenesis of periradicu
lar pathosis, either as a result of direct infection or
through virus-induced immune system alteration.
Infection during fetal and childhood development
Maternal rubella (German measles) Maternal infection during pregnancy may directly affect the developing fetus, leading to changes that vary from inconsequential to severe enough to result in fetal death.45 Fortunately, it appears that the most commonly encountered maternal infections cause no significant harm to the developing fetus. The outcome of maternal infection depends largely on the infectious agent involved, the maternal immune
473 www.shayanNemodar.com
Interrelationship of Pulp and Systemic Disease
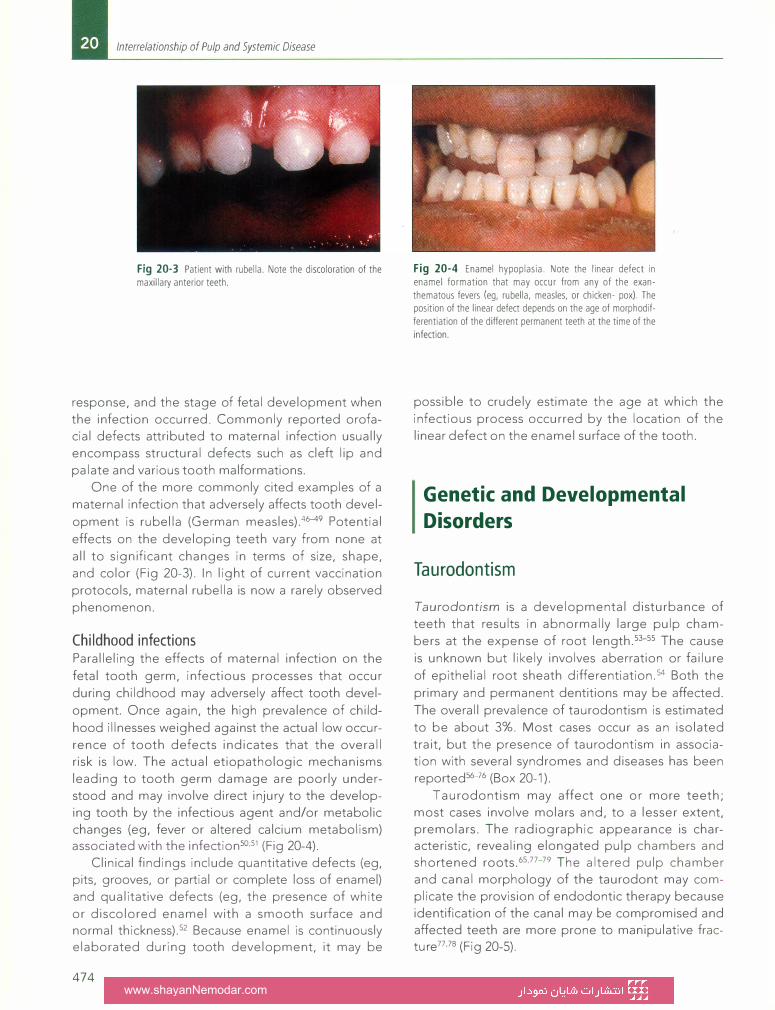
Fig 20-3 Patient with rubella. Note the discoloration of the maxillary anterior teeth.
response, and the stage of fetal development when the infection occurred. Commonly reported orofacial defects attributed to maternal infection usually encompass structural defects such as cleft lip and
palate and various tooth malformations.
One of the more commonly cited examples of a
maternal infection that adversely affects tooth devel
opment is rubella (German measles).46-49 Potential
effects on the developing teeth vary from none at
all to significant changes in terms of size, shape,
and color (Fig 20-3). In light of current vaccination
protocols, maternal rubella is now a rarely observed
phenomenon.
Childhood infections
Paralleling the effects of maternal infection on the
fetal tooth germ, infectious processes that occur
during childhood may adversely affect tooth devel
opment. Once again, the high prevalence of child
hood illnesses weighed against the actual low occur
rence of tooth defects indicates that the overall risk is low. The actual etiopathologic mechanisms
leading to tooth germ damage are poorly understood and may involve direct injury to the developing tooth by the infectious agent and/or metabolic changes (eg, fever or altered calcium metabolism) associated with the infection50·51 (Fig 20-4).
Clinical findings include quantitative defects (eg, pits, grooves, or partial or complete loss of enamel) and qualitative defects (eg, the presence of white
or discolored enamel with a smooth surface and normal thickness).52 Because enamel is continuously elaborated during tooth development, it may be
474
Fig 20-4 Enamel hypoplasia. Note the linear defect in enamel formation that may occur from any of the exanthematous fevers (eg, rubella, measles, or chicken- pox). The position of the linear defect depends on the age of morphodifferentiation of the different permanent teeth at the time of the infection.
possible to crudely estimate the age at which the
infectious process occurred by the location of the linear defect on the enamel surface of the tooth.
Genetic and Developmental
Disorders
Taurodontism
Taurodontism is a developmental disturbance of
teeth that results in abnormally large pulp cham
bers at the expense of root length.53-55 The cause
is unknown but likely involves aberration or failure
of epithelial root sheath differentiation.54 Both the
primary and permanent dentitions may be affected.
The overall prevalence of taurodontism is estimated
to be about 3%. Most cases occur as an isolated
trait, but the presence of taurodontism in association with several syndromes and diseases has been
reported56-76 (Box 20-1 ).
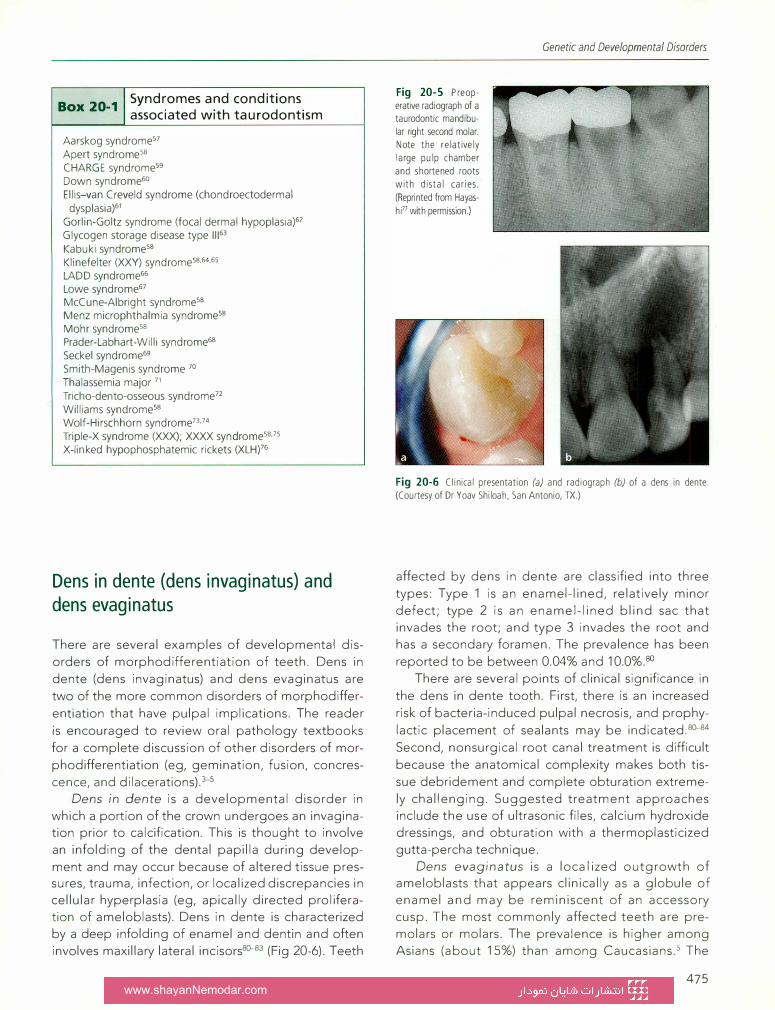
Taurodontism may affect one or more teeth; most cases involve molars and, to a lesser extent, premolars. The radiographic appearance is characteristic, revealing elongated pulp chambers and shortened roots.65·77-79 The altered pulp chamber and canal morphology of the taurodont may complicate the provision of endodontic therapy because identification of the canal may be compromised and affected teeth are more prone to manipulative fracture77·78 (Fig 20-5).
www.shayanNemodar.com
Box 20_1 I Synd�omes a�d conditions
_ associated with taurodont1sm
Aarskog syndrome57 Apert syndrome58 CHARGE syndrome59 Down syndrome60 Ellis-van Creveld syndrome (chondroectodermal
dysplasia)61 Gorlin-Goltz syndrome (focal dermal hypoplasia)62 Glycogen storage disease type 11163 Kabuki syndrome58 Klinefelter (XXY) syndromess.54.5s
LADD syndrome66 Lowe syndrome67 McCune-Albright syndrome58 Menz microphthalmia syndromess Mohr syndromess Prader-Labhart-Willi syndrome68 Seckel syndrome69 Smith-Magenis syndrome 70 Thalassemia major 71 Tricho-dento-osseous syndrome72 Williams syndromess Wolf-Hirschhorn syndrome73.74 Triple-X syndrome (XXX); XXXX syndromessJs X-linked hypophosphatemic rickets (XLH)76
Dens in dente (dens invaginatus) and dens evaginatus
There are several examples of developmental dis
orders of morphodifferentiation of teeth. Dens in
dente (dens invaginatus) and dens evaginatus are
two of the more common disorders of morphodiffer
entiation that have pulpal implications. The reader
is encouraged to review oral pathology textbooks
for a complete discussion of other disorders of mor
phodifferentiation (eg, gemination, fusion, concres
cence, and dilacerations)_:>-s Dens in dente is a developmental disorder in
which a portion of the crown undergoes an invagination prior to calcification. This is thought to involve
an infolding of the dental papilla during develop
ment and may occur because of altered tissue pressures, trauma, infection, or localized discrepancies in cellular hyperplasia (eg, apically directed proliferation of ameloblasts). Dens in dente is characterized by a deep infolding of enamel and dentin and often
involves maxillary lateral incisors80-83 (Fig 20-6). Teeth
Fig 20-5 Preoperative radiograph of a taurodontic mandibular right second molar. Note the relatively large pulp chamber and shortened roots with distal caries.
(Reprinted from Hayas
hi77 with permission.)
Genetic and Developmental Disorders
Fig 20-6 Clinical presentation (a) and radiograph (b) of a dens in dente. (Courtesy of Dr Yoav Shiloah, San Antonio, TX.)
affected by dens in dente are classified into three
types: Type 1 is an enamel-lined, relatively minor
defect; type 2 is an enamel-lined blind sac that invades the root; and type 3 invades the root and has a secondary foramen. The prevalence has been
reported to be between 0.04% and 10.0%.80
There are several points of clinical significance in
the dens in dente tooth. First, there is an increased
risk of bacteria-induced pulpal necrosis, and prophy
lactic placement of sealants may be indicated.80-84
Second, nonsurgical root canal treatment is difficult
because the anatomical complexity makes both tis
sue debridement and complete obturation extreme
ly challenging. Suggested treatment approaches include the use of ultrasonic files, calcium hydroxide dressings, and obturation with a thermoplasticized gutta-percha technique.
Dens evaginatus is a localized outgrowth of ameloblasts that appears clinically as a globule of enamel and may be reminiscent of an accessory cusp. The most commonly affected teeth are pre
molars or molars. The prevalence is higher among Asians (about 15%) than among Caucasians.5 The
475 www.shayanNemodar.com
Interrelationship of Pulp and Systemic Disease
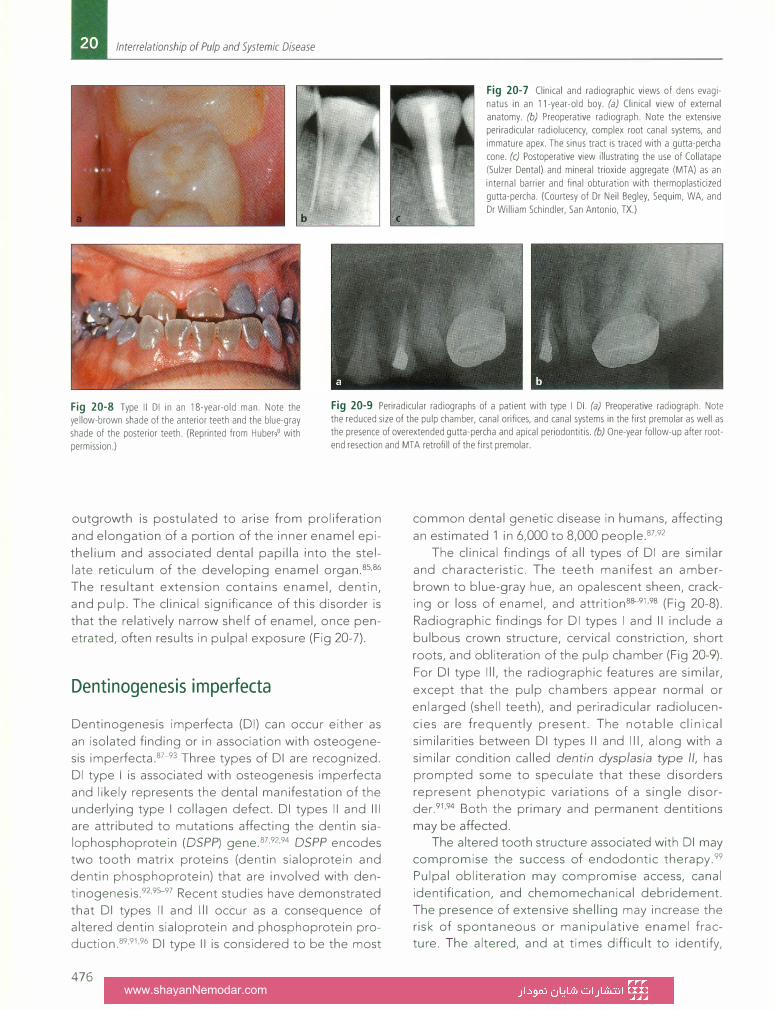
Fig 20-7 Clinical and radiographic views of dens evaginatus in an 11-year-old boy. (a) Clinical view of external anatomy. (b) Preoperative radiograph. Note the extensive periradicular radiolucency, complex root canal systems, and immature apex. The sinus tract is traced with a gutta-percha cone. (c) Postoperative view illustrating the use of Collatape (Sulzer Dental) and mineral trioxide aggregate (MTA) as an
internal barrier and final obturation with thermoplasticized gutta-percha. (Courtesy of Dr Neil Begley, Sequim, WA, and Dr William Schindler, San Antonio, TX.)
Fig 20-8 Type II DI in an 18-year-old man. Note the yellow-brown shade of the anterior teeth and the blue-gray shade of the posterior teeth. (Reprinted from Huber90 with permission.)
Fig 20-9 Periradicular radiographs of a patient with type I DI. (a) Preoperative radiograph. Note the reduced size of the pulp chamber, canal orifices, and canal systems in the first premolar as well as the presence of overextended gutta-percha and apical periodontitis. (b) One-year follow-up after rootend resection and MT A retrofill of the first premolar.
outgrowth is postulated to arise from proliferation
and elongation of a portion of the inner enamel epi
thelium and associated dental papilla into the stel
late reticulum of the developing enamel organ.85·86
The resultant extension contains enamel, dentin,
and pulp. The clinical significance of this disorder is
that the relatively narrow shelf of enamel, once pen
etrated, often results in pulpal exposure (Fig 20-7).
Dentinogenesis imperfecta
Dentinogenesis imperfecta (DI) can occur either as
an isolated finding or in association with osteogene
sis imperfecta.87-93 Three types of DI are recognized.
DI type I is associated with osteogenesis imperfecta
and likely represents the dental manifestation of the underlying type I collagen defect. DI types II and Ill
are attributed to mutations affecting the dentin sialophosphoprotein (OSPP') gene.87·92·94 DSPP encodes two tooth matrix proteins (dentin sialoprotein and
dentin phosphoprotein) that are involved with den
tinogenesis.92·%-97 Recent studies have demonstrated that DI types II and Ill occur as a consequence of altered dentin sialoprotein and phosphoprotein production.89·91·96 DI type II is considered to be the most
476
common dental genetic disease in humans, affecting
an estimated 1 in 6,000 to 8,000 people.87·92
The clinical findings of all types of DI are similar
and characteristic. The teeth manifest an amber
brown to blue-gray hue, an opalescent sheen, cracking or loss of enamel, and attrition8B-91·98 (Fig 20-8).
Radiographic findings for DI types I and II include a
bulbous crown structure, cervical constriction, short
roots, and obliteration of the pulp chamber (Fig 20-9).
For DI type Ill, the radiographic features are similar,
except that the pulp chambers appear normal or
enlarged (shell teeth), and periradicular radiolucen
cies are frequently present. The notable clinical
similarities between DI types II and Ill, along with a
similar condition called dentin dysplasia type II, has prompted some to speculate that these disorders
represent phenotypic variations of a single disor
der.91·94 Both the primary and permanent dentitions
may be affected. The altered tooth structure associated with DI may
compromise the success of endodontic therapy.99 Pulpal obliteration may compromise access, canal
identification, and chemomechanical debridement. The presence of extensive shelling may increase the risk of spontaneous or manipulative enamel fracture. The altered, and at times difficult to identify,
www.shayanNemodar.com
Genetic and Developmental Disorders
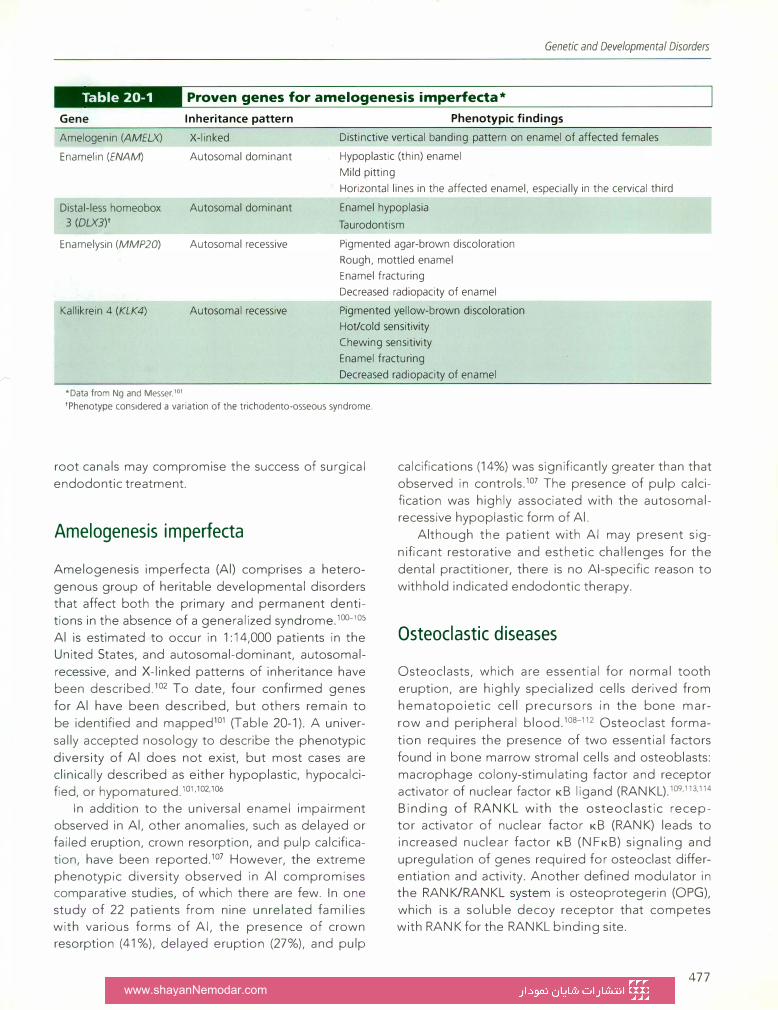
II ftjtjtjfJ•lm Proven genes for amelogenesis imperfecta*
Gene Inheritance pattern Phenotypic findings
Amelogenin (AMELXJ
Enamelin (ENAM)
X-linked
Autosomal dominant
Distinctive vertical banding pattern on enamel of affected females
Hypoplastic (thin) enamel
Mild pitting
Horizontal lines in the affected enamel. especially in the cervical third
Distal-less homeobox
3 (OLX3)t Autosomal dominant Enamel hypoplasia
Taurodontism
Enamelysin (MMP20) Autosomal recessive Pigmented agar-brown discoloration
Rough, mottled enamel
Enamel fracturing
Kallikrein 4 (KLK4) Autosomal recessive
Decreased radiopacity of enamel
Pigmented yellow-brown discoloration
Hot/cold sensitivity
Chewing sensitivity
Enamel fracturing
Decreased radiopacity of enamel
*Data from Ng and Messer. 101
'Phenotype considered a variation of the trichodento-osseous syndrome.
root canals may compromise the success of surgical
endodontic treatment.
Amelogenesis imperfecta
Amelogenesis imperfecta (Al) comprises a hetero
genous group of heritable developmental disorders that affect both the primary and permanent dentitions in the absence of a generalized syndrome.100-105
Al is estimated to occur in 1:14,000 patients in the United States, and autosomal-dominant, autosomalrecessive, and X-linked patterns of inheritance have been described.102 To date, four confirmed genes
for Al have been described, but others remain to be identified and mapped101 (Table 20-1). A univer
sally accepted nosology to describe the phenotypic
diversity of Al does not exist, but most cases are clinically described as either hypoplastic, hypocalcified, or hypomatured.101·102·106
In addition to the universal enamel impairment observed in Al, other anomalies, such as delayed or failed eruption, crown resorption, and pulp calcification, have been reported.107 However, the extreme phenotypic diversity observed in Al compromises comparative studies, of which there are few. In one study of 22 patients from nine unrelated families with various forms of Al, the presence of crown resorption (41%), delayed eruption (27%), and pulp
calcifications (14%) was significantly greater than that observed in controls.107 The presence of pulp calcification was highly associated with the autosomalrecessive hypoplastic form of Al.
Although the patient with Al may present sig
nificant restorative and esthetic challenges for the
dental practitioner, there is no Al-specific reason to
withhold indicated endodontic therapy.
Osteoclastic diseases
Osteoclasts, which are essential for normal tooth
eruption, are highly specialized cells derived from hematopoietic cell precursors in the bone mar
row and peripheral blood.10a-112 Osteoclast forma
tion requires the presence of two essential factors
found in bone marrow stromal cells and osteoblasts: macrophage colony-stimulating factor and receptor activator of nuclear factor KB ligand (RANKL).109·113·114 Binding of RANKL with the osteoclastic receptor activator of nuclear factor KB (RANK) leads to increased nuclear factor KB (NFKB) signaling and upregulation of genes required for osteoclast differentiation and activity. Another defined modulator in the RANK/RANKL system is osteoprotegerin (OPG), which is a soluble decoy receptor that competes with RANK for the RAN KL binding site.
477 www.shayanNemodar.com

Interrelationship of Pulp and Systemic Disease
It appears that most processes affecting bone
resorption and tooth eruption act through modulation of the balance of RANKL and OPG108-112
for RANK. Disease states that result in reduced
osteoclastic activity (eg, osteopetrosis, cleidocranial
dysplasia, and pyknodysostosis) commonly exhibit
phenotypic delay or failure of tooth eruption, while
disease states that result in increased osteoclastic
activity (eg, Paget disease of bone [PDB] and juve
nile Paget disease) manifest accelerated tooth loss.
Paget disease of bone (osteitis deformans) PDB is a heterogenous, focal, progressive bone dis
ease characterized by active bone turnover.114·115 The
risk of developing PDB increases with age, affect
ing an estimated 1 % of individuals over the age of
40 years in the United States.116 Men are at slightly
greater risk than women. In addition to a genetic
predisposition, other yet to be defined environ
mental factors likely contribute to the disease pro
cess.111.118
Mutations affecting the sequestosome 1 gene are
found in up to 50% and 30% of patients with familial
and sporadic cases of PDB, respectively.119 Sequesto
some 1 (also known as p62) is an important scaffold
protein in the NFKB pathway. In terms of environ
mental factors, some have proposed that a latent
paramyxoviral infection (eg, measles, canine distemper virus, or respiratory syncytial virus) contributes to
PDB, but this issue remains unresolved.113·118·120 PDB may affect one (monostotic) or a few (poly
ostoti c) bones, and most cases are asympto
matic and discovered incidentally.116·118.121 The
most commonly affected sites include the pelvis,
skull, vertebra, femur, and tibia. Affected bones
usually manifest an initial osteolytic phase, followed
by a mixed osteolytic/osteosclerotic phase, which
ultimately progresses to a disorganized osteosclerotic phase. In reality, all three arbitrary phases of
PDB may exist concurrently. Common clinical signs
and symptoms include osseous distortion or expan
sion and mild to moderate, deep, aching bone pain. Elevated serum total alkaline phosphatase levels are
reflective of the increased bone activity and characteristic for the disease. While osteosarcoma is a rare
complication of PDB, most cases of adult osteosarcoma occur in patients with PDB.113
Skull involvement is estimated to occur in about 27% of patients and may result in hearing loss and vestibular problems in up to 89% of those affected.122 It is postulated that, in addition to direct auditory
478
nerve impingement, the disease may adversely alter
the bone density, mass, and structure of the auditory complex to contribute to hearing compromise.
Numerous dental abnormalities, such as malocclu
sion, hypercementosis, tooth mobility, root resorp
tion, pulp calcification, osteomyelitis, poorly fitting
prostheses, and excessive postsurgical bleeding,
have been associated with PDB.122·123 However, these
findings are largely based on anecdotal case reports,
and their true prevalence is unknown. In a cross
sectional survey of 292 patients with PDB, 93% of
those with maxillomandibular involvement related having dental problems, compared to only 10% of
those with skull or other distant bone involvement.122
However, compared to controls, the patients with
dental problems reported no significant difference in
edentulism, tooth movement, change in bite, change
in denture fit, periodontal disease, or need for endodontic treatments. Many of the dental changes associated with PDB are likely explained by the dynamic
nature of the disease. During the osteolytic phase,
tooth mobility, shifting, and increased postsurgical
bleeding may occur. More mature pagetoid changes
affecting the jaws may manifest as malocclusion and/
or deformity and result in an increased risk of osteo
myelitis.
Potential radiographic changes associated with
PDB reflect the brisk osteoclastic and osteoblastic
nature of the disease.121·124 The characteristic lytic
sign of PDB affecting the skull is osteoporosis cir
cumscripta, whereas the characteristic sclerotic sign
is the cotton wool appearance. An overall mosaic
of lytic and sclerotic findings is frequently noted.
Potential radiographic findings of PDB involving
the jaws include hypercementosis, thickening of the
periodontal ligament space, root resorption, and
pulpal obliteration.123·125-129
Hypercementosis has been reported to occur frequently in PDB, and its presence is considered highly suggestive of PDB.123·126·127 Large amounts of cementum may be deposited in the apical two
thirds of the roots, giving the tooth the appearance of a baseball bat (Fig 20-10). The cementum
may appear to be fused with the adjacent sclerotic bone130 (Fig 20-11), resulting in ankylosis.128 In such a
scenario, the involved teeth will be abnormally firm.
Lytic activity around an involved tooth may affect the lamina dura to produce a widened periodontal ligament space. In contrast to primary or secondary hyperparathyroidism, which manifests generalized thickening of the periodontal ligament space, in
www.shayanNemodar.com

Genetic and Developmental Disorders
Fig 20-10 Ground section of a maxillary second premolar showing the extensive hypercementosis associated with Paget disease.
Fig 20-11 Characteristic intraoral radiographic features of Paget disease. Note the variable appearance of the canal space, periodontal ligament space, and lamina dura. (a) Areas of radiolucency. (b) Isolated sclerosis. (c) Isolated sclerosis and distal root resorption of the maxillary second molar. (d) Isolated sclerosis and hypercementosis of the second premolar. (Reprinted from Barnett and Elfenbein130 with permission.)
PDB the widening is restricted to involved teeth. An additional lytic change that may occur is root resorption, which may clinically manifest as mobility. Paralleling the concurrent mixed lytic and sclerotic processes affecting the bone, lytic changes may affect some teeth while other teeth may demonstrate hypercementosis.
The potential for pagetoid changes to affect the pulp has been proposed, but few reports addressing the issue exist.125•128•129 In one case report evaluating a mandibular third molar, internal resorption of the dentin, direct apposition of cellular hard tissue partially occluding the coronal pulp, and dystrophic calcification in the radicular region of the pulp were noted. The overall mosaic pattern observed was similar to that typically observed in the bone and cementum.125 These potential radiographic findings may interfere with endodontists' ability to establish a proper working length, prompting some to recommend the use of an apex locator to establish the canal length.123
Disturbances of vitamin D metabolism
The primary regulator of calcium homeostasis and subsequent bone and dentin mineralization in the body is bioactive vitamin D {1a,25-dihydroxyvitamin 03).131-133 Numerous rachitic conditions relating to specific alterations in vitamin D metabolism have been identified. Both vitamin D-dependent rickets type I (VDDRI) and vitamin D-dependent rickets type II (VDDRll) are rare recessive disorders, while X-linked hypophosphatemic rickets (XLH) is passed as an X-linked dominant trait. The phenotypic presentations of all three forms of rickets have much in common, but subtle variations do exist.
Vitamin D-dependent rickets type 1 VDDRI manifests as deficient 1-a-hydroxylase production, and the responsible mutation has been mapped to chromosome 12.131 1-a-hydroxylase is a member of the cytochrome P450 superfamily of enzymes and is required for normal vitamin D activation. It acts on the circulating vitamin D precursor 25-hydroxyvitamin D
3 to form bioactive vitamin
D.132•134 Originally believed to be restricted to the kidney, 1-a-hydroxylase expression and activity occur at several extrarenal sites, including skin, lymph nodes, colon, pancreas, brain, endothelial cells, and bone.
479 www.shayanNemodar.com

Interrelationship of Pulp and Systemic Disease
Prominent clinical features of VDDRI include stunted growth, skeletal abnormalities, genu valgum, rachitic rosary, open fontanels, pathologic fractures, muscle weakness, and convulsions. Common laboratory findings include hypocalcemia, hypophosphatemia, elevated parathyroid hormone, high alkaline phosphatase, normal levels of vitamin D precursors, and low levels of bioactive vitamin D. A single case report of the dental findings in a patient with VDDRI noted the presence of enamel hypoplasia, large quadrangular pulp chambers, and short roots.133 The administration of physiologic levels of bioactive vitamin D (1a,25-dihydroxyvitamin D3) is the treatment of choice. Such therapy bypasses the deficient enzyme, thereby fostering normal development.
Vitamin D-dependent rickets type II Mutational abnormalities mapped to chromosome 12 underlie VDDRll.131 In this scenario, the vitamin D receptor is adversely affected, resulting in endorgan resistance to vitamin D modulation. The resultant defective intestinal calcium absorption leads to hypocalcemia and rickets. Laboratory findings include hypocalcemia, elevated parathyroid hormone levels, and hypophosphatemia. Vitamin D precursor levels are normal, and bioactive vitamin D levels are elevated. The elevated levels of bioactive vitamin D help to distinguish VDDRI from VDDRll.131
The clinical findings of VDDRll are often severe and usually apparent within a few months of birth.131 The clinical phenotype is similar to that for VDDRI. However, a fairly characteristic feature of VDDRll is sparse body hair, or a/opecia universa/is, the presence of which appears to correlate well with disease severity. Medical therapy is limited and consists of calcium infusion and the administration of pharmacologic levels of precursor and bioactive vitamin D. Because neither of these approaches addresses the receptor deficiency, results have been mixed.
Only a single report is available in the English literature addressing the dental findings associated with VDDRll.135 The authors reported on the dental findings in three children with VDDRll. Two of the three children, both girls, exhibited no evidence of enamel hypoplasia but did manifest enlarged pulp chambers and thin dentin. Both responded well to medical therapy and experienced normal root canal and pulp chamber development. The other child, a boy, presented with a more severe phenotypic presentation of VDDRI I than the two
480
girls. On initial examination, an abscessed primary maxillary first molar was noted, and his teeth also exhibited enlarged pulp chambers and thin dentin. The abscessed tooth was extracted and submitted for histologic assessment. The histologic findings showed abundant interglobular dentin and a lack of a predental layer. This child did not respond to medical therapy, and the dental defects persisted.
X-linked hypophosphatemic rickets The most prevalent form of rickets is caused by mutations affecting the PHEX gene (phosphateregulating gene with homology of endopeptidases that maps to the X chromosome) and is termed X-linked hypophosphatemia.136 The mutation responsible for XLH has been mapped to Xp22.2-p22.1, and the incidence is estimated at 1 in 20,000 persons.70·136-138 Patients with XLH experience impaired 1-a-hydroxylase activity, reduced phosphate resorption in the kidney and intestine, hypophosphatemia, and hyperphosphaturia. The current medical treatment of choice is the prompt institution of supplemental vitamin D and phosphate therapy.
The main clinical features include severe bony deformities, impaired growth, short stature, frontal bossing, craniotabes, and a square-shaped head. The dental findings affect both the primary and permanent dentitions and include enlarged pulp chambers, enlarged pulp horns, hypocalcified and interglobular dentin, short roots, taurodontism, poorly defined lamina dura, and hypoplastic alveolar ridges70·133·138 (Figs 20-12 and 20-13). The severity of the clinical and radiographic dental lesions is influenced by the patient's age, the type of teeth (prenatal or postnatal odontogenesis), and whether the patient was undergoing therapy prior to the time of examination.
The finding of prominent pulp horns extending up to the dentinoenamel junction in both dentitions is regarded by some as pathognomonic for XLH.137·139 These abnormalities place the XLH patient at risk for spontaneous dental abscesses, which occur frequently and often without any evidence of preexisting trauma or caries.70·137·138·140·141 It is likely that attrition of the enamel allows bacterial entry into the dentinal tubules and pulp.70·142·143 Although endodontic treatment is clearly [ndicated in many instances, the underlying structural defects associated with XLH may compromise the clinician's ability to obtain an adequate obturation seal.
www.shayanNemodar.com
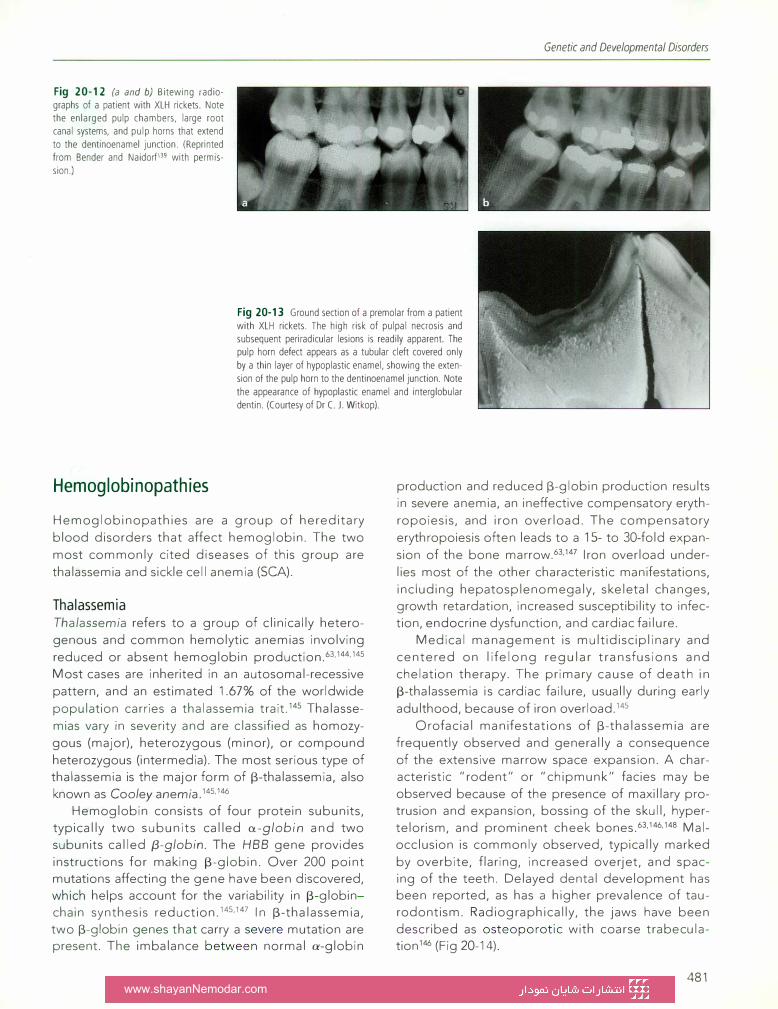
Fig 20-12 (a and b) Bitewing radiographs of a patient with XLH rickets. Note the enlarged pulp chambers, large root canal systems, and pulp horns that extend to the dentinoenamel junction. (Reprinted from Bender and Naidorf139 with permission.)
Genetic and Developmental Disorders
Fig 20-13 Ground section of a premolar from a patient with XLH rickets. The high risk of pulpal necrosis and subsequent periradicular lesions is readily apparent. The pulp horn defect appears as a tubular cleft covered only by a thin layer of hypoplastic enamel, showing the extension of the pulp horn to the dentinoenamel junction. Note the appearance of hypoplastic enamel and interglobular dentin. (Courtesy of Dr C. J. Witkop).
Hemoglobinopathies
Hemoglobinopathies are a group of hereditary
blood disorders that affect hemoglobin. The two
most commonly cited diseases of this group are
thalassemia and sickle cell anemia (SCA).
Thalassemia Thalassemia refers to a group of clinically hetero
genous and common hemolytic anemias involving
reduced or absent hemoglobin production.63·144·145
Most cases are inherited in an autosomal-recessive
pattern, and an estimated 1.67% of the worldwide
population carries a thalassemia trait.145 Thalasse
mias vary in severity and are classified as homozy
gous (major), heterozygous (minor}, or compound
heterozygous (intermedia). The most serious type of thalassemia is the major form of 13-thalassemia, also
known as Cooley anemia.145·146
Hemoglobin consists of four protein subunits, typically two subunits called a-globin and two subunits called {3-globin. The HBB gene provides
instructions for making 13-globin. Over 200 point mutations affecting the gene have been discovered, which helps account for the variability in 13-globinchain synthesis reduction.145•147 In 13-thalassemia, two 13-globin genes that carry a severe mutation are present. The imbalance between normal a-globin
production and reduced 13-globin production results in severe anemia, an ineffective compensatory eryth
ropoiesis, and iron overload. The compensatory
erythropoiesis often leads to a 15- to 30-fold expan
sion of the bone marrow.63•147 Iron overload under
lies most of the other characteristic manifestations,
including hepatosplenomegaly, skeletal changes, growth retardation, increased susceptibility to infection, endocrine dysfunction, and cardiac failure.
Medical management is multidisciplinary and
centered on lifelong regular transfusions and
chelation therapy. The primary cause of death in
13-thalassemia is cardiac failure, usually during early
adulthood, because of iron overload.145
Orofacial manifestations of 13-thalassemia are
frequently observed and generally a consequence
of the extensive marrow space expansion. A characteristic "rodent" or "chipmunk" facies may be
observed because of the presence of maxillary protrusion and expansion, bossing of the skull, hyper
telorism, and prominent cheek bones.63·146·148 Malocclusion is commonly observed, typically marked
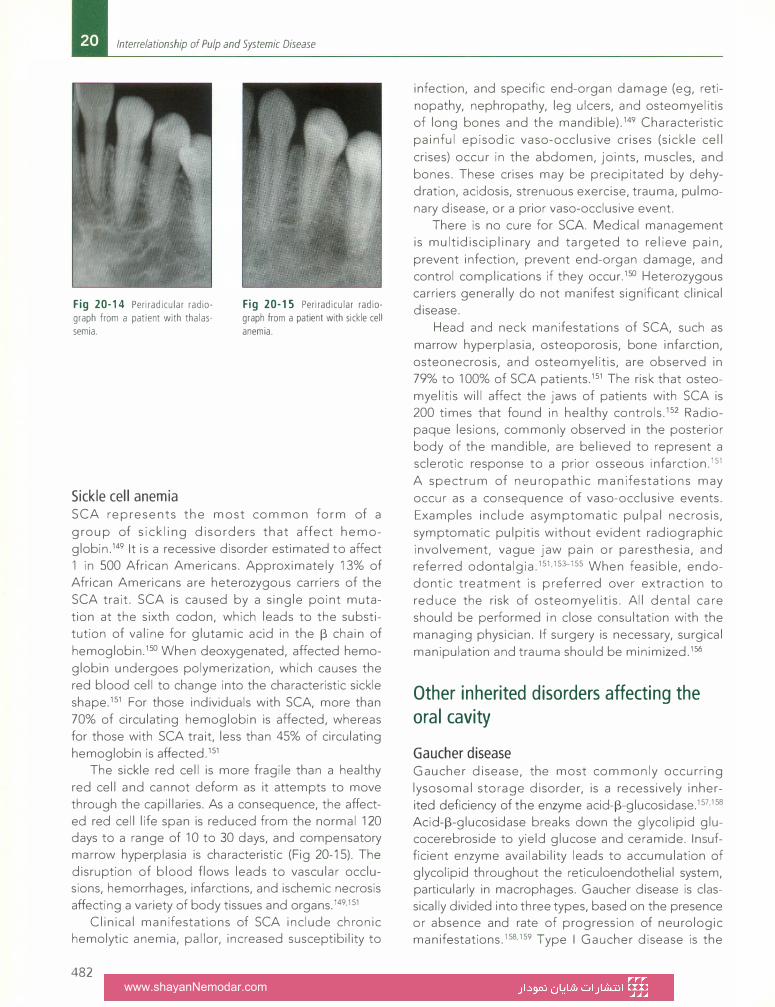
by overbite, flaring, increased overjet, and spacing of the teeth. Delayed dental development has been reported, as has a higher prevalence of taurodontism. Radiographically, the jaws have been
described as osteoporotic with coarse trabeculation 146 (Fig 20-14).
481 www.shayanNemodar.com
Interrelationship of Pulp and Systemic Disease
Fig 20-14 Periradicular radio
graph from a patient with thalas
semia.
Sickle cell anemia
Fig 20-15 Periradicular radio
graph from a patient with sickle cell
anemia.
SCA represents the most common form of a
group of sickling disorders that affect hemoglobin.149 It is a recessive disorder estimated to affect 1 in 500 African Americans. Approximately 13% of African Americans are heterozygous carriers of the
SCA trait. SCA is caused by a single point muta
tion at the sixth codon, which leads to the substitution of valine for glutamic acid in the 13 chain of
hemoglobin.150 When deoxygenated, affected hemo
globin undergoes polymerization, which causes the red blood cell to change into the characteristic sickle
shape.151 For those individuals with SCA, more than
70% of circulating hemoglobin is affected, whereas for those with SCA trait, less than 45% of circulating
hemoglobin is affected.151 The sickle red cell is more fragile than a healthy
red cell and cannot deform as it attempts to move through the capillaries. As a consequence, the affected red cell life span is reduced from the normal 120 days to a range of 10 to 30 days, and compensatory marrow hyperplasia is characteristic (Fig 20-15). The disruption of blood flows leads to vascular occlusions, hemorrhages, infarctions, and ischemic necrosis affecting a variety of body tissues and organs.149·151
Clinical manifestations of SCA include chronic hemolytic anemia, pallor, increased susceptibility to
482
infection, and specific end-organ damage (eg, reti
nopathy, nephropathy, leg ulcers, and osteomyelitis of long bones and the mandible).149 Characteristic
painful episodic vaso-occlusive crises (sickle cell
crises) occur in the abdomen, joints, muscles, and
bones. These crises may be precipitated by dehydration, acidosis, strenuous exercise, trauma, pulmo
nary disease, or a prior vaso-occlusive event. There is no cure for SCA Medical management
is multidisciplinary and targeted to relieve pain,
prevent infection, prevent end-organ damage, and control complications if they occur.150 Heterozygous carriers generally do not manifest significant clinical disease.
Head and neck manifestations of SCA, such as
marrow hyperplasia, osteoporosis, bone infarction,
osteonecrosis, and osteomyelitis, are observed in
79% to 100% of SCA patients.151 The risk that osteo
myelitis will affect the jaws of patients with SCA is 200 times that found in healthy controls.152 Radiopaque lesions, commonly observed in the posterior body of the mandible, are believed to represent a sclerotic response to a prior osseous infarction.151
A spectrum of neuropathic manifestations may
occur as a consequence of vaso-occlusive events.
Examples include asymptomatic pulpal necrosis,
symptomatic pulpitis without evident radiographic involvement, vague jaw pain or paresthesia, and referred odontalgia.151·153-155 When feasible, endodontic treatment is preferred over extraction to
reduce the risk of osteomyelitis. All dental care
should be performed in close consultation with the
managing physician. If surgery is necessary, surgical
manipulation and trauma should be minimized.156
Other inherited disorders affecting the oral cavity
Gaucher disease Gaucher disease, the most commonly occurring
lysosomal storage disorder, is a recessively inherited deficiency of the enzyme acid-13-glucosidase.157·158
Acid-13-glucosidase breaks down the glycolipid glucocerebroside to yield glucose and ceramide. Insufficient enzyme availability leads to accumulation of glycolipid throughout the reticuloendothelial system, particularly in macrophages. Gaucher disease is classically divided into three types, based on the presence or absence and rate of progression of neurologic manifestations.158·159 Type I Gaucher disease is the
www.shayanNemodar.com
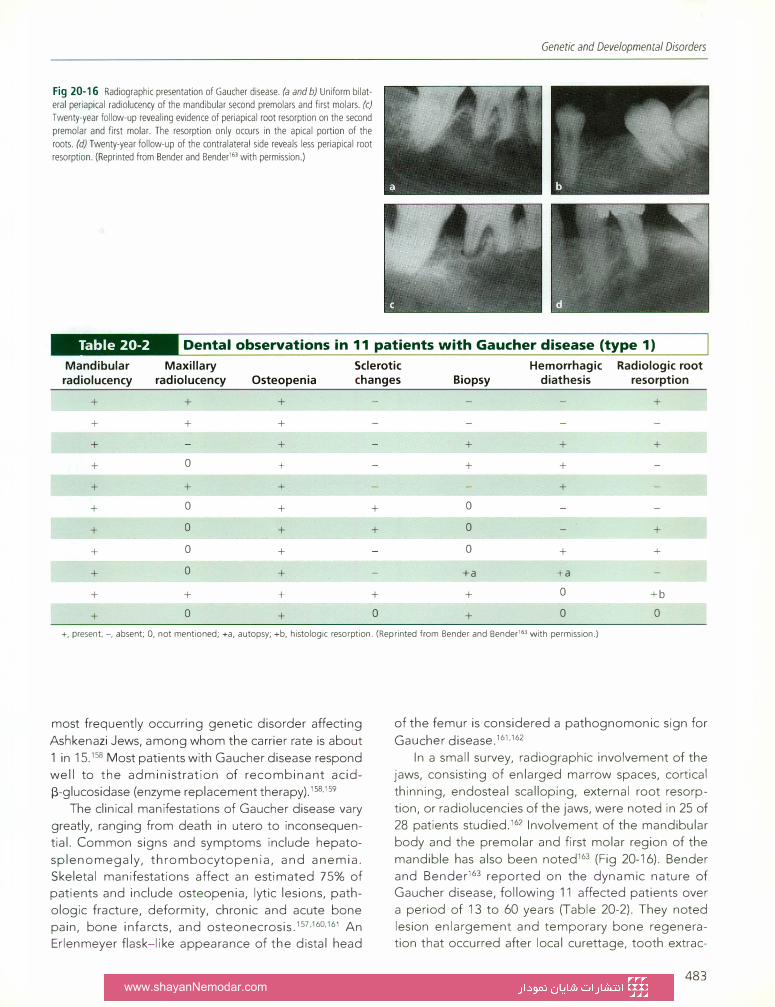
Fig 20-16 Radiographic presentation of Gaucher disease. (a and b) Uniform bilat
eral periapical radiolucency of the mandibular second premolars and first molars. (c) Twenty-year follow-up revealing evidence of periapical root resorption on the second
premolar and first molar. The resorption only occurs in the apical portion of the
roots. (d) Twenty-year follow-up of the contralateral side reveals less periapical root
resorption. (Reprinted from Bender and Bender163 with permission.)
Genetic and Developmental Disorders
II m�CEJ•Ell Dental observations in 11 patients with Gaucher disease (type 1)
Mandibular Maxillary Sclerotic Hemorrhagic Radiologic root radiolucency radiolucency Osteopenia changes Biopsy diathesis resorption
+ + + +
+ + +
+ + + + +
+ 0 + + +
+ + + +
+ 0 + + 0
+ 0 + + 0 +
+ 0 + 0 + +
+ 0 + +a +a
+ + + + + 0 +b
+ 0 + 0 + 0 0
+, present;-, absent; 0, not mentioned; +a, autopsy; +b, histologic resorption. (Reprinted from Bender and Bender'" with permission.)
most frequently occurring genetic disorder affecting Ashkenazi Jews, among whom the carrier rate is about 1 in 15.158 Most patients with Gaucher disease respond well to the administration of recombinant acid�-glucosidase (enzyme replacement therapy).15s.159
The clinical manifestations of Gaucher disease vary greatly, ranging from death in utero to inconsequential. Common signs and symptoms include hepatosplenomegaly, thrombocytopenia, and anemia. Skeletal manifestations affect an estimated 75% of patients and include osteopenia, lytic lesions, pathologic fracture, deformity, chronic and acute bone pain, bone infarcts, and osteonecrosis.157·160·161 An Erlenmeyer flask-like appearance of the distal head
of the femur is considered a pathognomonic sign for Gaucher disease.161•162
In a small survey, radiographic involvement of the jaws, consisting of enlarged marrow spaces, cortical thinning, endosteal scalloping, external root resorption, or radiolucencies of the jaws, were noted in 25 of 28 patients studied.162 Involvement of the mandibular body and the premolar and first molar region of the mandible has also been noted163 (Fig 20-16). Bender and Bender163 reported on the dynamic nature of Gaucher disease, following 11 affected patients over a period of 13 to 60 years (Table 20-2). They noted lesion enlargement and temporary bone regeneration that occurred after local curettage, tooth extrac-
483 www.shayanNemodar.com
Interrelationship of Pulp and Systemic Disease
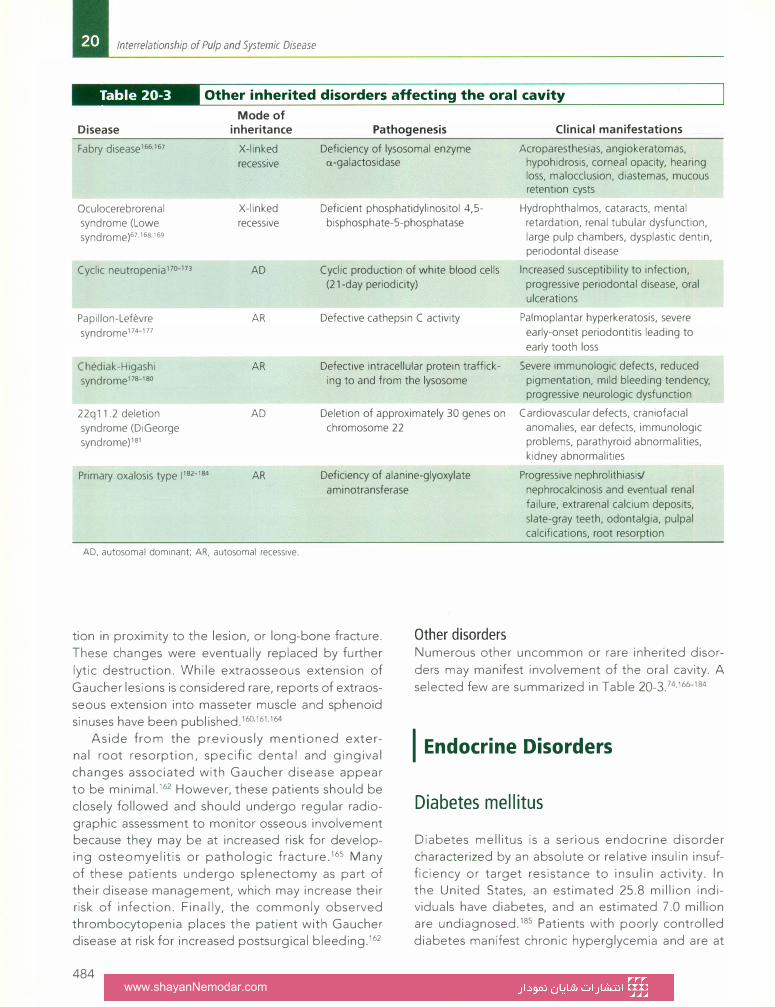
II @tjtfJ•f 111 Other inherited disorders affecting the oral cavity
Mode of Disease
Fabry disease166·167
Oculocerebrorenal syndrome (Lowe syndrome)67.16s.169
Cyclic neutropenia 110-173
Papi I Ion-Lefevre syndrome174-177
Chediak-Higashi syndrome 11s-1so
22q11.2 deletion syndrome (DiGeorge syndrome)181
Primary oxalosis type 11s2-1s4
inheritance
X-linked recessive
X-linked recessive
AD
AR
AR
AD
AR
AD, autosomal dominant; AR, autosomal recessive.
Pathogenesis
Deficiency of lysosomal enzyme a-galactosidase
Deficient phosphatidylinositol 4,5-bisphosphate-5-phosphatase
Cyclic production of white blood cells (21-day periodicity)
Defective cathepsin C activity
Defective intracellular protein trafficking to and from the lysosome
Deletion of approximately 30 genes on chromosome 22
Deficiency of alanine-glyoxylate aminotransferase
Other disorders
Clinical manifestations
Acroparesthesias, angiokeratomas, hypohidrosis, corneal opacity, hearing loss, malocclusion, diastemas, mucous retention cysts
Hydrophthalmos, cataracts, mental retardation, renal tubular dysfunction, large pulp chambers, dysplastic dentin, periodontal disease
Increased susceptibility to infection, progressive periodontal disease, oral ulcerations
Palmoplantar hyperkeratosis, severe early-onset periodontitis leading to early tooth loss
Severe immunologic defects, reduced pigmentation, mild bleeding tendency, progressive neurologic dysfunction
Cardiovascular defects, craniofacial anomalies, ear defects, immunologic problems, parathyroid abnormalities, kidney abnormalities
Progressive nephrolithiasis/ nephrocalcinosis and eventual renal failure, extrarenal calcium deposits, slate-gray teeth, odontalgia, pulpal calcifications, root resorption
tion in proximity to the lesion, or long-bone fracture.
These changes were eventually replaced by further
lytic destruction. While extraosseous extension of
Gaucher lesions is considered rare, reports of extraos
seous extension into masseter muscle and sphenoid
sinuses have been published.160·161·164
Numerous other uncommon or rare inherited disor
ders may manifest involvement of the oral cavity. A
selected few are summarized in Table 20-3.74·16b--184
Aside from the previously mentioned exter
nal root resorption, specific dental and gingival
changes associated with Gaucher disease appear
to be minimal.162 However, these patients should be
closely followed and should undergo regular radio
graphic assessment to monitor osseous involvement because they may be at increased risk for develop
ing osteomyelitis or pathologic fracture.165 Many
of these patients undergo splenectomy as part of
their disease management, which may increase their
risk of infection. Finally, the commonly observed
thrombocytopenia places the patient with Gaucher
disease at risk for increased postsurgical bleeding.162
484
I Endocrine Disorders
Diabetes mellitus
Diabetes mellitus is a serious endocrine disorder
characterized by an absolute or relative insulin insuf
ficiency or target resistance to insulin activity. In the United States, an estimated 25.8 million individuals have diabetes, and an estimated 7.0 million
are undiagnosed.185 Patients with poorly controlled
diabetes manifest chronic hyperglycemia and are at
www.shayanNemodar.com

increased risk for myriad complications, including infection.186-189 The five classic complications of diabetes are (1) retinopathy, (2) nephropathy, (3) neuropathy, (4) macrovascular disease, and (5) impaired wound healing.187,189-191
Hyperglycemia leads to the creation and accu
mulation of advanced glycation end-products
(AGEs), which are believed to contribute directly to the etiopathogenesis of diabetes.187·189·191-196 AGEs impair normal homeostatic collagen turnover, leading to the accumulation of a more mature, less soluble collagen in the vessel wall; subsequent vessel wall thickening and reduction in lumen size; and a decrease in tissue perfusion.187·189·195 AGE-altered collagen is also more prone to bind with low-density
lipoprotein to form atheromas, which contribute to
large vessel disease.187 At the immunologic level, hyperglycemia results in impaired chemotaxis, adherence, and phagocytosis of polymorphonuclear leukocytes.187 AGE interaction with monocytes and macrophages results in the creation of a proinflammatory phenotype.187,191,193.197
While it is axiomatic that adequate medical control of diabetes is essential to the maintenance of oral health, the impact of poor oral health (eg, periodontitis or periradicular abscess) on the control
and progression of diabetes must be understood.
A two- to three-times greater rate of periodontal disease has been observed in individuals with
diabetes. This is understandable, given the fact that the typical area of the susceptible periodontium is roughly the size of the palm.198 Such a large inflammatory burden may negatively impact glucose control in the diabetic patient and confer an increased risk of developing diabetes-related complications.188-191,194, 197-199
Although there are few studies addressing the
relationship between diabetes and pulpal disease, logical points of intersection to consider would include diabetes-induced microvascular, neuropathic, and inflammatory changes. It appears that diabetic patients in need of endodontic treatment are more likely to present with larger periradicular lesions, harbor more virulent pathogens, experience perioperative symptoms, and experience a higher incidence of
therapeutic failure than control patients.186·200-205 The increased risk of infection and potential poor
wound healing observed in the diabetic patient has led some to advocate the administration of antimicrobial prophylaxis prior to dental treatment, particularly in the individual with poorly controlled diabe-
Endocrine Disorders
tes.206 However, there have been no studies directly addressing the issue, and the overall complexity of diabetes would seem to confound any attempted study. It is clear that any infection, including pulpal disease, in the diabetic patient must be man
aged promptly and aggressively. As a rule, diabetic patients under good disease control can be gener
ally regarded as normal patients, whereas patients who are either suspected of having diabetes or
whose diabetes seems under poor control should be referred for medical evaluation prior to the delivery of dental care. Medical consultation is further recommended for any anticipated dental treatment, such as extensive surgery, that can adversely impact the patient's glucose control.
Adrenal dysfunction
Cortisol, a naturally occurring glucocorticoid of the adrenocortex, and the catecholamine epinephrine are the primary modulators of the stress response.207-210 Cortisol stimulates peripheral fat and protein catabolism to serve as substrates for the hepatic production of glucose.211 Well-established anti-inflammatory and immunomodulatory effects of cortisol include preventing leukocyte migration from the circulation
into the extravascular space, reducing the accumulation of monocytes and granulocytes at inflammatory sites, and suppressing the production of numerous cytokines and other proinflammatory mediators. Cortisol also acts in a permissive role to allow other hormones such as catecholamines and angiotensin II to modulate cardiac contractility, vascular tone, and blood pressure.212-214 Finally, cortisol provides negative feedback to the hypothalamus and the anterior
pituitary gland (hypothalamic-pituitary-adrenal [HPA]
axis) in regulating corticotropin-releasing hormone
and adrenocorticotropin-releasing hormone.207·210·215 Conditions of insufficient cortisol production,
regardless of the etiology, are termed Addison disease. 216 Most cases of glucocorticoid deficiency develop insidiously, presenting with nonspecific signs and symptoms such as lethargy, anorexia, nausea, weight loss, and hypoglycemia. These
patients are typically prescribed empirical replacement glucocorticoid therapy.217 Conditions of endogenous cortisol excess are termed Cushing syndrome.211·218·219 However, the most frequent cause of glucocorticoid excess is iatrogenic. The clinical findings of cortisol excess correspond directly to the
485 www.shayanNemodar.com

Interrelationship of Pulp and Systemic Disease
severity and duration of glucocorticoid excess and
include truncal obesity, violaceous striae of the skin,
buffalo hump, facial fullness (moon facies), facial
plethora, acne, hirsutism, easy bruising, muscle wast
ing, and myopathy.
There are no disease-specific oral manifestations
of Addison disease. Some individuals manifest a
patchy brown (bronzing) pigmentation of the face
(with superimposed areas of vitiligo}, the buccal
mucosa, the tongue, and, less frequently, the lips
and gingivae. Head and neck manifestations of
Cushing syndrome include facial plethora, moon
face, hirsutism, and acne. Affected children may
exhibit delayed or arrested dental development
paralleling the overall growth retardation that may
occur with glucocorticoid excess.220·221 Chronic expo
sure to excess glucocorticoid appears to stimulate odontoblast-like cells within the dental pulp, result
ing in narrowing of the dental pulp chamber or com
plete pulpal obliteration222-224 (Fig 20-17).
Patients with Addison disease are inherently
unable to produce sufficient levels of adrenocorti
cotropic hormone or cortisol to meet physiologic
demand. Similarly, chronic exogenous glucocorticoid
exposure can suppress the HPA axis, and therefore
patients on chronic glucocorticoid therapy may not
be able to produce sufficient levels of adrenocorti
cotropic hormone and cortisol to meet physiologic
demand.211·225--227 The concern in clinical practice is
that, for either situation, an overwhelming stressor
(surgery, sepsis, or fever) may precipitate an Addisonian crisis (adrenal insufficiency with hypotension
and shock).22&-230 Accordingly, supplemental gluco
corticoids ("stress dose" steroids) are recommend
ed perioperatively for patients with documented or
presumed HPA axis suppression when they are to
undergo a stressful medical procedure. Fortunately,
486
-
.. ..... -
Fig 20-17 Comparison of predentin thickness in teeth collected from a healthy patient (a) and a patient who was chronically treated with gluco
corticoids, suffering from renal failure, and undergoing dialysis (b). The predentin is about four times wider in the healthy patient than it is in the chronically ill patient (hematoxylin-eosin stain). (Reprinted from Wysocki et al224 with permission.)
it appears that the risk of an Addisonian crisis dur
ing an outpatient dental procedure is low or very
low.217·23° Consequently, patients need only to take
their usual daily glucocorticoid dose on the day of
the procedure. If moderate or major surgical stress is
anticipated under general anesthesia and the patient
has documented or presumed HPA axis suppression,
then appropriate stress doses of perioperative ste
roids are indicated.
I Cancer
There are few reports of malignancies affecting the
dental pulp. The risk that a primary malignancy will
arise from pulpal tissue appears to be extremely
remote.231 In reviewing the dental literature pub
lished over a 100-year span (1870 to 1970), Stanley129
reported fewer than 20 case reports of pulpal cancer.
Furthermore, if a primary pulpal malignancy were to
develop, the enclosed nature of the pulp chamber
increases the likelihood that the tumor growth will adversely interrupt the pulpal vascular network, result
ing in self-strangulation. A more likely, albeit still rare,
scenario occurs when the pulp or periradicular area is
infiltrated by a hematologic malignancy or is the tar
get of a solid tumor metastasis.232-251
Regardless of the specific malignancy involved,
the presenting signs and symptoms are often nonspecific and mimic routine inflammatory pulpal or
periodontal disease.235•237•238·243·244 Thus, the pres
ence of findings such as odontalgia, percussion
sensitivity, periradicular radiolucencies, and gingival
inflammation and swelling often raise little suspicion.
However, the presence of more worrisome findings,
www.shayanNemodar.com
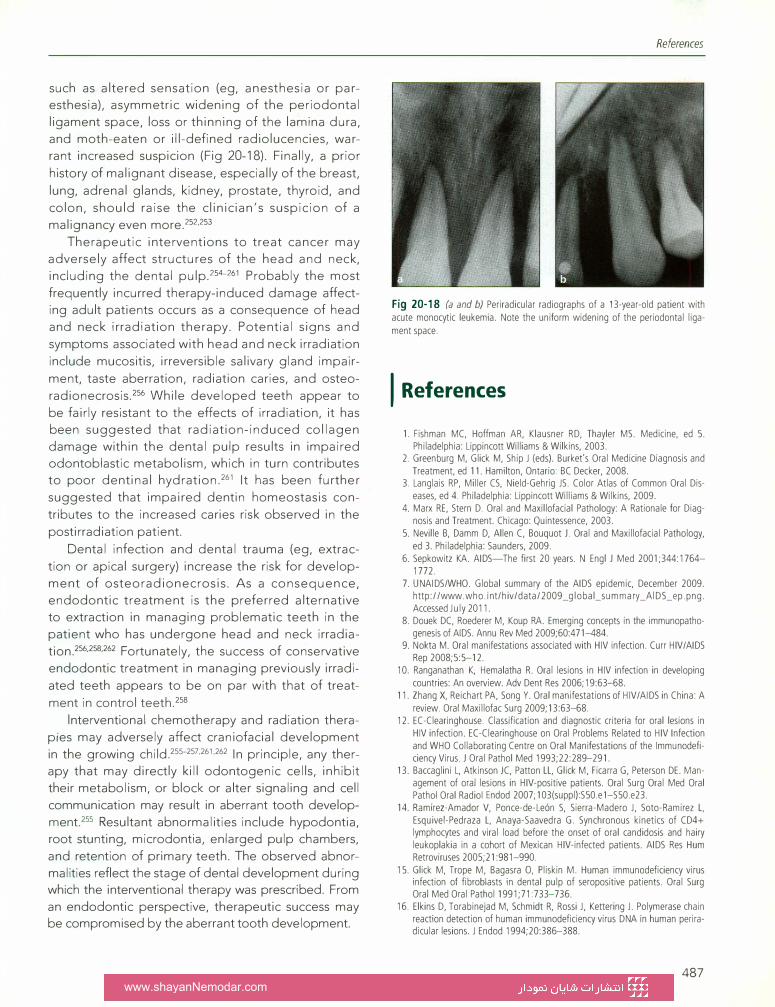
such as altered sensation (eg, anesthesia or paresthesia), asymmetric widening of the periodontal
ligament space, loss or thinning of the lamina dura,
and moth-eaten or ill- defined radiolucencies, war
rant increased suspicion (Fig 20-18). Finally, a prior
history of malignant disease, especially of the breast,
lung, adrenal glands, kidney, prostate, thyroid, and
colon, should raise the clinician's suspicion of a
malignancy even more.252,253
Therapeutic interventions to treat cancer may
adversely affect structures of the head and neck,
including the dental pulp.254-261 Probably the most
frequently incurred therapy-induced damage affecting adult patients occurs as a consequence of head
and neck irradiation therapy. Potential signs and
symptoms associated with head and neck irradiation
include mucositis, irreversible salivary gland impair
ment, taste aberration, radiation caries, and osteo
radionecrosis.256 While developed teeth appear to
be fairly resistant to the effects of irradiation, it has been suggested that radiation-induced collagen
damage within the dental pulp results in impaired odontoblastic metabolism, which in turn contributes to poor dentinal hydration.261 It has been further
suggested that impaired dentin homeostasis con
tributes to the increased caries risk observed in the
postirradiation patient.
Dental infection and dental trauma (eg, extrac
tion or apical surgery) increase the risk for develop
ment of osteoradionecrosis. As a consequence,
endodontic treatment is the preferred alternative to extraction in managing problematic teeth in the
patient who has undergone head and neck irradia
tion.256·258·262 Fortunately, the success of conservative
endodontic treatment in managing previously irradi
ated teeth appears to be on par with that of treat
ment in control teeth.258
lnterventional chemotherapy and radiation thera
pies may adversely affect craniofacial development
in the growing child.255-257·261·262 In principle, any therapy that may directly kill odontogenic cells, inhibit
their metabolism, or block or alter signaling and cell
communication may result in aberrant tooth develop
ment.255 Resultant abnormalities include hypodontia, root stunting, microdontia, enlarged pulp chambers,
and retention of primary teeth. The observed abnor
malities reflect the stage of dental development during which the interventional therapy was prescribed. From
an endodontic perspective, therapeutic success may be compromised by the aberrant tooth development.
References
Fig 20-18 (a and b) Periradicular radiographs of a 13-year-old patient with acute monocytic leukemia. Note the uniform widening of the periodontal ligament space.
I References
1. Fishman MC, Hoffman AR, Klausner RD, Thayler MS. Medicine, ed 5. Philadelphia: Lippincott Williams & Wilkins, 2003.
2. Greenburg M, Glick M, Ship J (eds). Burket's Oral Medicine Diagnosis and Treatment, ed 11. Hamilton, Ontario: BC Decker, 2008.
3. Langlais RP, Miller CS, Nield-Gehrig JS. Color Atlas of Common Oral Diseases, ed 4. Philadelphia: Lippincott Williams & Wilkins, 2009.
4. Marx RE, Stern D. Oral and Maxillofacial Pathology: A Rationale for Diagnosis and Treatment. Chicago: Quintessence, 2003.
5. Neville B, Damm D, Allen C, Bouquot J. Oral and Maxillofacial Pathology, ed 3. Philadelphia: Saunders, 2009.
6. Sepkowitz KA. AIDS-The first 20 years. N Engl J Med 2001;344:1764-1772.
7. UNAIDS/WHO. Global summary of the AIDS epidemic, December 2009. http://www. who. i nt/h iv/data/2009 _global_summary _Al DS_ep .png. Accessed July 2011.
8. Douek DC, Roederer M, Koup RA. Emerging concepts in the immunopathogenesis of AIDS. Annu Rev Med 2009;60:471-484.
9. Nokta M. Oral manifestations associated with HIV infection. Curr HIV/AIDS Rep 2008;5:5-12.
10. Ranganathan K, Hemalatha R. Oral lesions in HIV infedion in developing countries: An overview. Adv Dent Res 2006; 19:63-68.
11. Zhang X, Reichart PA, Song Y. Oral manifestations of HIV/AIDS in China: A review. Oral Maxillofac Surg 2009;13:63-68.
12. EC-Clearinghouse. Classification and diagnostic criteria for oral lesions in HIV infection. EC-Clearinghouse on Oral Problems Related to HIV Infection and WHO Collaborating Centre on Oral Manifestations of the Immunodeficiency Virus. J Oral Pathol Med 1993;22:289-291.
13. Baccaglini L, Atkinson JC, Patton LL, Glick M, Ficarra G, Peterson DE. Management of oral lesions in HIV-positive patients. Oral Surg Oral Med Oral Pathol Oral Radio I Endod 2007; 103(suppl):S50.e1-S50.e23.
14. Ramirez-Amador V, Ponce-de-Leon S, Sierra-Madero J, Soto-Ramirez L, Esquivel-Pedraza L, Anaya-Saavedra G. Synchronous kinetics of CD4+ lymphocytes and viral load before the onset of oral candidosis and hairy leukoplakia in a cohort of Mexican HIV-infected patients. AIDS Res Hum Retroviruses 2005;21 :981-990.
15. Glick M, Trope M, Bagasra 0, Pliskin M. Human immunodeficiency virus infection of fibroblasts in dental pulp of seropositive patients. Oral Surg Oral Med Oral Pathol 1991;71 :733-736.
16. Elkins D, Torabinejad M, Schmidt R, Rossi J, Kettering J. Polymerase chain reaction detection of human immunodeficiency virus DNA in human periradicular lesions. J Endod 1994;20:386-388.
487 www.shayanNemodar.com
Interrelationship of Pulp and Systemic Disease
17. Castro GF, Souza IP, Lopes S, Stashenko P, Teles RP. Salivary lgA to cariogenic bacteria in HIV-positive children and its correlation with caries prevalence and levels of cariogenic microorganisms. Oral Microbiol lmmunol 2004;19:28 1-288.
18. Frezzini C, Leao JC, Porter S. Current trends of HIV disease of the mouth. J Oral Pathol Med 2005;34:5 13-531.
19. Hodgson TA, Greenspan D, Greenspan JS. Oral lesions of HIV disease and HAART in industrialized countries. Adv Dent Res 2006; 19:57-62.
20. Cooper H. Root canal treatment in patients with HIV infection. Int Endod J 1993;26:369-371.
2 1. Glick M, Abel S, Muzyka B, Delorenzo M. Dental complications after treating patients with AIDS. J Am Dent Assoc 1994; 126:296-30 1.
22. Alley BS, Buchanan TH, Eleazer PD. Comparison of the success of root canal therapy in HIV/AIDS patients and non-infected controls. Gen Dent 2008;56:155-157.
23. Shetty K, Garcia J, Leigh J. Success of root canal therapy in HIV-positive patients. Gen Dent 2006;54:397-402.
24. Suchina JA, Levine D, Flaitz CM, Nichols CM, Hicks MJ. Retrospective clinical and radiologic evaluation of nonsurgical endodontic treatment in human immunodeficiency virus (HIV) infection. J Contemp Dent Pract 2006;7: 1-8.
25. Miller CS, Berger JR, Mootoor Y, Avdiushko SA, Zhu H, Kryscio RJ. High prevalence of multiple human herpesviruses in saliva from human immunodeficiency virus-infected persons in the era of highly active antiretroviral therapy. J Clin Microbiol 2006;44:2409-2415.
26. Miller CS, Avdiushko SA, Kryscio RJ, Danaher RJ, Jacob RJ. Effect of prophylactic valacyclovir on the presence of human herpesvirus DNA in saliva of healthy individuals after dental treatment. J Clin Microbiol 2005;43:2173-2 180.
27. Scott DA, Coulter WA, Lamey PJ. Oral shedding of herpes simplex virus type 1: A review. J Oral Pathol Med 1997;26:44 1-447.
28. Huber MA. Herpes simplex type-1 virus infection. Quintessence Int 2003;34:453-467.
29. Chen V, Chen Y, Li H, Kent K, Baumgartner JC, Machida CA. Herpesviruses in abscesses and cellulitis of endodontic origin. J Endod 2009;35: 182-188.
30. Nishiyama SA, Nakano V, Velasquez-Melendez G, Avila-Campos MJ. Occurrence of herpes simplex virus 1 and three periodontal bacteria in patients with chronic periodontitis and necrotic pulp. Can J Microbiol 2008;54:326-330.
31. Gilden DH, Cohrs RJ, Mahalingam. VZV vasculopathy and postherpetic neuralgia: Progress and perspectives on antiviral therapy. Neurology 2005;64:2 1-25.
32. Mori I, Nishiyama Y. Herpes simplex virus and varicella-zoster virus: Why do these human alphaherpesviruses behave so differently from one another? Rev Med Virol 2005; 15:393-406.
33. Roxas M. Herpes zoster and postherpetic neuralgia: Diagnosis and therapeutic considerations. Altern Med Rev 2006; 11: 102-113.
34. Tidwell E, Hutson B, Burkhart N, Gutmann JL, Ellis CD. Herpes zoster of the trigeminal nerve third branch: A case report and review of the literature. Int Endod J 1999;32:6 1-66.
35. Jain MK, Manjunath KS, Jagadish SN. Unusual oral complications of herpes zoster infection: Report of a case and review of literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010 Nov;1 10:e37-e41.
36. Mendieta C, Miranda J, Brunet LI, Gargallo J, Berini L. Alveolar bone necrosis and tooth exfoliation following herpes zoster infection: A review of the literature and case report. J Periodontol 2005;76: 148-153.
37. Ramchandani PL, Mellor TK. Herpes zoster associated with tooth resorption and periapical lesions. Br J Oral Maxillofac Surg 2007;45:71-73.
38. Goon W, Jacobsen P. Prodromal odontalgia and multiple devitalized teeth caused by a herpes zoster infection of the trigeminal nerve: Report of a case. J Am Dent Assoc 1988; 166: 500-504.
39. Rauckhorst AJ, Baumgartner JC. Zebra. XIX. Part 2. Oral herpes zoster. J Endod 2000;26:469-471.
40. Fristad I, Bardsen A, Knudsen GC, Molven 0. Prodromal herpes zoster-A diagnostic challenge in endodontics. Int Endod J 2002;35: 10 12- 1016.
41. Sabeti M, Simon JH, Slots J. Cytomegalovirus and Epstein-Barr virus are associated with symptomatic periapical pathosis. Oral Microbial lmmunol 2003; 18:327-328.
488
42. Sabeti M, Slots J. Herpesviral-bacterial coinfection in periapical pathosis. J Endod 2004;30:69-72.
43. Slots J, Nowzari H, Sabeti M. Cytomegalovirus infection in symptomatic periapical pathosis. Int Endod J 2004;37:519-524.
44. Yildirim S, Yapar M, Kubar A, Slots J. Human cytomegalovirus, EpsteinBarr virus and bone resorption-inducing cytokines in periapical lesions of deciduous teeth. Oral Microbiol lmmunol 2006;21: 107- 1 1 1.
45. Ornoy A, Tenenbaum A. Pregnancy outcome following infections by coxsackie, echo, measles, mumps, hepatitis, polio and encephalitis viruses. Reprod Toxicol 2006;2 1 :446-457.
46. Glick M, Goldman HS. Viral infections in the dental setting: Potential effects on pregnant HCWs. J Am Dent Assoc 1993; 124: 79-86.
47. Guggenheimer J, Nowak A, Michaels R. Dental manifestations of the rubella syndrome. Oral Surg Oral Med Oral Pathol 197 1;32:30-37.
48. Gullikson JS. Tooth morphology in rubella syndrome children. ASDC J Dent Child 1975;42:479-482.
49. Hall R. Prevalence of developmental defects of tooth enamel (DDE) in a pediatric hospital department of dentistry population. Adv Dent Res 1989;3:114-119.
50. Edwards MJ. Review: Hyperthermia and fever during pregnancy. Birth Defects Res A Clin Mol Teratol 2006;76:507-5 16.
5 1. Tung K, Fujita H, Yamashita Y, Takagi Y. Effect of turpentine-induced fever during the enamel formation of rat incisor. Arch Oral Biol 2006;51: 464-470.
52. Lygidakis NA, Dimou G, Marinou D. Molar-incisor-hypomineralisation (MIH). A retrospective clinical study in Greek children. II. Possible medical aetiological factors. Eur Arch Paediatr Dent 2008;9:207-2 17.
53. Constant DA, Grine FE. A review of taurodontism with new data on indigenous southern African populations. Arch Oral Biol 200 1;46: 102 1-1029.
54. Gedik R, �imen M. Mutiple taurodontism: Report of case. ASDC J Dent Child 2000;67:216-217.
55. Sert S, Bayirh G. Taurodontism in six molars: A case report: J Endod 2004;30:601-602.
56. Atkinson JC, Harvey KE, Domingo DL, et al. Oral and dental phenotype of dyskeratosis congenita. Oral Dis 2008; 14:4 19-427.
57. Dayal PK, Chaudhary AR, Desai Kl, Joshi HN. Aarskog syndrome. A case report. Oral Surg Oral Med Oral Pathol 1990;69:403-405.
58. Jafarzadeh H, Azarpazhooh A, Mayhall JT. Taurodontism: A review of the condition and endodontic treatment challenges. Int Endod J 2008;41 :375-388.
59. Grimm SE 3rd, Thomas GP, White MJ. CHARGE syndrome: Review of literature report of case. Coloboma, heart disease, atresia of choanae, retarded mental development, genital hypoplasia, ear abnormalitiesdeafness. ASDC J Dent Child 1997;64:2 18-221,228.
60. Rajic' Z, Mestrovic SR. Taurodontism in Down's syndrome. Coll Antropol 1998; 22(supp1):63-67.
61. Hunter ML, Roberts GJ. Oral and dental anomalies in Ellis van Creveld syndrome (chondroectodermal dysplasia): Report of a case. Int J Paediatr Dent 1998;153- 157.
62. McNamara T, Trotman CA, Hahessy AM, Kavanagh P. Focal dermal hypoplasia (Goltz-Gorlin) syndrome with taurodontism. Spec Care Dentist 1996; 16:26-28.
63. Baccetti T, Pierleoni L, Filippi L, Donati MA, Tollaro I, Zammarchi E. Dental and craniofacial findings in a child affected by glycogen storage disease type Ill. J Clin Pediatr Dent 1994;19:55-60.
64. Joseph M. Endodontic treatment in three taurodontic teeth associated with 48,XXXY Klinefelter syndrome: A review and case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008; 105:670-677.
65. Yeh SC, Hsu TY. Endodontic treatment in taurodontism with Klinefelter's syndrome: A case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999;88:612-6 15.
66. Guven Y, Rosti RO, Tuna EB, Kayserili H, Aktoren 0. Orodental findings of a family with lacrimo-auriculo-dento digital (LADD) syndrome. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008; 106:e33-e44.
67. Tsai SJ, O'Donnell D. Dental findings in an adult with Lowe's syndrome. Spec Care Dentist 1997; 17:207-2 10.
68. Bassarelli V, Baccetti T, Bassarelli T, Franchi L. The dentomaxillofacial characteristics of the Prader-Labhart-Willi syndrome. A clinical case report. Minerva Stomatol 1991;40:8 1 1-819.
www.shayanNemodar.com
69. Seymen F, Tuna B, Kayserli H. Seckel syndrome: Report of a case. J Clin Pediatr Dent 2002;26:305-309.
70. Tomona N, Smith AC, Guadagnini JP, Hart TC. Craniofacial and dental phenotype of Smith-Magenis syndrome. Am J Genet 2006;140:2556-2561.
71. Hazza'a AM, Al-Jamal G. Radiographic features of the jaws and teeth in thalassaemia major. Dentomaxillofac Radial 2006;35:283-288.
72. Spangler GS, Hall Kl, Kula K, Hart TC, Wright JT. Enamel structure and composition in the tricho-dento-osseous syndrome. Connect Tissue Res 1998;39: 165-167.
73. Babich SB, Banducci C, Teplitsky P. Dental characteristics of the WolfHirschhorn syndrome: A case report. Spec Care Dentist 2004;24:229-231.
74. Johnston NJ, Franklin DI. Dental findings of a child with Wolf-Hirschhorn syndrome. Int J Paediatr Dent 2006; 16: 139-142.
75. Varrela J, Alvesalo L. Taurodontism in females with extra X chromosomes. J Craniofac Genet Dev Biol 1989;9: 129-133.
76. Seow WK, Needleman HL, Holm IA. Effect of familial hypophosphatemic rickets on dental development: A controlled, longitudinal study. Pediatr Dent 1995;17:346-350.
77. Hayashi Y. Endodontic treatment in taurodontism. J Endod 1994;20: 357-358.
78. Prakash R, Chenduran V, Ballal S, Velmurugan N, Kandaswamy D. Endodontic management of taurodontic teeth. Indian J Dent Res 2005; 16: 177-181.
79. Witkop CJ Jr, Keenan KM, Cervenka J, Jaspers MT. Taurodontism: An anomaly of teeth reflecting disruptive developmental homeostasis. Am J Med Genet Suppl 1998;4:85-97.
80. Alani A, Bishop K. Dens invaginatus. Part 1: Classification, prevalence and aetiology. Int Endod J 2008;41: 1123-1136.
81. Bishop K, Alani A. Dens invaginatus. Part 2: Clinical, radiographic features and management options. Int Endod J 2008;41: 1137-1154.
82. Sathorn C, Parashos P. Contemporary treatment of class II dens invaginatus. Int Endod J 2007;40:308-316.
83. Schmitz MS, Montagner F, Flores CB, Morari VH, Quesada GA, Gomes BP. Management of dens invaginatus type I and open apex: Report of three cases. J Endod 2010;36:1079-1085.
84. De Sousa SM, Bramante CM. Dens invaginatus: Treatment choices. Endod Dent Traumatol 1998; 14: 152-158.
85. Levitan ME, Himel VT. Dens evaginatus: Literature review, pathophysiology, and comprehensive treatment regimen. J Endod 2006;32:1-9.
86. Vasudev SK, Goel BR. Endodontic management of dens evaginatus of maxillary central incisors: A rare case report. J Endod 2005;31 :67-70.
87. Barron MJ, McDonnell ST, Mackie I, Dixon MJ. Hereditary dentine disorders: Dentinogenesis imperfecta and dentine dysplasia. Orphanet J Rare Dis 2008;3:31.
88. Bailleul-Forestier I, Berdal A, Vinckier F, de Ravel T, Fryns JP, Verloes A. The genetic basis of inherited anomalies of the teeth. Part 2: Syndromes with significant dental involvement. Eur J Med Genet 2008;51 :383-408.
89. Dong J, Gu T, Jeffords L, MacDougall M. Dentin phosphoprotein compound mutation in dentin sialophosphoprotein causes dentinogenesis imperfecta type Ill. Am J Med Genet A 2005; 132A:305-309.
90. Huber MA. Osteogenesis imperfecta. Oral Surg Oral Med Oral Pathol Oral Radial Endod 2007; 103:314-320.
91. Kim JW, Hu JC, Lee JI, et al. Mutational hot spot in the DSPP gene causing dentinogenesis imperfecta type II. Hum Genet 2005; 116: 186-191.
92. MacDougall M, Dong J, Acevedo AC. Molecular basis of human dentin diseases. Am J Med Genet A 2006;140:2536-2546.
93. Song Y, Wang C, Peng B, et al. Phenotypes and genotypes in 2 DGI families with different DSPP mutations. Oral Surg Oral Med Oral Pathol Oral Radial Endod 2006; 102:360-374.
94. Malmgren B, Lindskog S, Elgadi A, Norgren S. Clinical, histopathologic, and genetic investigation in two large families with dentinogenesis imperfecta type II. Hum Genet 2004;114:491-498.
95. MacDougall M. Dental structural diseases mapping to human chromosome 4q21. Connect Tissue Res 2003;44(suppl 1):285-291.
96. McKnight DA, Simmer JP, Hart PS, Hart TC, Fisher LW. Overlapping DSPP mutations cause dentin dysplasia and dentinogenesis imperfecta. J Dent Res 2008;87: 1108-1111.
References
97. Qin C, Baba 0, Butler WT. Post-translational modifications of sibling proteins and their roles in osteogenesis and dentinogenesis. Crit Rev Oral Biol Med 2004; 15: 126-136.
98. Malmgren B, Lindskog S. Assessment of dysplastic dentin in osteogenesis imperfecta and dentinogenesis imperfecta. Acta Odontol Scand 2003;61 :72-80.
99. Pettiette MT, Wright JT, Trope M. Dentinogenesis imperfecta: Endodontic implications. Case report. Oral Surg Oral Med Oral Pathol Oral Radial Endod 1998;86:733-737.
100. Hu JC, Yamakoshi Y. Enamelin and autosomal-dominant amelogenesis imperfecta. Crit Rev Oral Biol Med 2003; 14:387-398.
101. Ng FK, Messer LB. Dental management of amelogenesis imperfecta patients: A primer on genotype-phenotype correlations. Pediatr Dent 2009;31 20-30.
102. Nusier M, Yassin 0, Hart TC, Samimi A, Wright JT. Phenotypic diversity and revision of the nomenclature for autosomal recessive amelogenesis imperfecta. Oral Surg Oral Med Oral Pathol Oral Radial Endod 2004;97: 220-230.
103. Simmer JP, Hu JC. Dental enamel formation and its impact on clinical dentistry. J Dent Educ 2001;65:896-905.
104. Stephanopoulos G, Garefalaki ME, Lyroudia K. Genes and related proteins involved in amelogenesis imperfecta. J Dent Res 2005;84:1117-1126.
105. Wright JT, Hart PS, Aldred MJ, et al. Relationship of phenotype and genotype in X-linked amelogenesis imperfecta. Connect Tissue Res 2003;44(suppl 1):72-78.
106. Aldred MJ, Savarirayan R, Crawford PJ. Amelogenesis imperfecta: A classification and catalogue for the 21st century. Oral Dis 2003;9: 19-23.
107. Collins MA, Mauriello SM, Tyndall DA, Wright JT. Dental anomalies associated with amelogenesis imperfecta: A radiographic assessment. Oral Surg Oral Med Oral Pathol Oral Radial Endod 1999;88:358-364.
108. Heinrich J, Bsoul S, Barnes J, Woodruff K, Abboud S.CSF-1, RANKL and OPG regulate osteoclastogenesis during murine tooth eruption. Arch Oral Biol 2005;50:897-908.
109. Helfrich MH. Osteoclast diseases and dental abnormalities. Arch Oral Biol 2005; 50: 115-122.
110. Liu D, Yao S, Pan F, Wise GE. Chronology and regulation of gene expression of RANKL in the rat dental follicle. Eur J Oral Sci 2005; 113:404-409.
111. Wise GE. Cellular and molecular basis of tooth eruption. Orthod Craniofac Res 2009; 12:67-73.
112. Wise GE, Yao S, Odgren PR, Pan F. CSF-1 regulation of osteoclastogenesis for tooth eruption. J Dent Res 2005;84:837-841.
113. Helfrich MH. Osteoclast diseases. Microsc Res Tech 2003;61 :514-532. 114. Sun SG, Lau YS, ltonaga I, Sabokbar A, Athanasou NA. Bone stromal cells
in pagetic bone and Paget's sarcoma express RANKL and support human osteoclast formation. J Pathol 2006; 209: 114-120.
115. Falchetti A, Masi L, Brandi ML. Paget's disease of bone: There's more than the affected skeletal-A clinical review and suggestions for the clinical practice. Curr Opin Rheumatol 2010;22:410-423.
116. Whyte MP. Paget's disease of bone. N Engl J Med 2006;355:593-600. 117. Cooper C, Harvey NC, Dennison EM, van Staa TP. Update on the epide
miology of Paget's disease of bone. J Bone Miner Res 2006;21(suppl 2): P3-P8.
118. Seton M. Paget's disease: Epidemiology and pathophysiology. Curr Osteoporos Rep 2008;6: 125-129.
119. Daroszewska A, Ralston SH. Mechanisms of disease: Genetics of Paget's disease of bone and related disorders. Nat Clin Pract Rheumatol 2006;2:270-277.
120. Friedrichs WE, Reddy SV, Bruder JM, et al. Sequence analysis of measles virus nucleocapsid transcripts in patients with Paget's disease. J Bone Miner Res 2002; 17: 145-151.
121. Theodorou DJ, Theodorou SJ, Kakitsubata Y. Imaging of Paget disease of bone and its musculoskeletal complications: Review. AJR Am J Roentgenol 2011; 196(6 suppl):S64-S75.
122. Wheeler TT, Alberts MA, Dolan TA, McGorray SP. Dental, visual, auditory and olfactory complications in Paget's disease of bone. J Am Geriatr Soc 1995;43: 1384-1391.
123. Bender IB. Paget's disease. J Endod 2003;29:720-723.
489
www.shayanNemodar.com
Interrelationship of Pulp and Systemic Disease
124. Brouard R, Wybier M, Miquel A, Laredo JD. The lucent rim: A radiographic and computed tomography sign of Paget's disease of the skull. Eur Radiol 2006;16:1308-1311.
125. Aldred MJ, Cooke BE. Paget's disease of bone with involvement of the dental pulp. J Oral Pathol 1989; 18: 184-185.
126. Lucas RB. The jaws and teeth in Paget's disease of bone. J Clin Pathol 1955;8: 195-200.
127. Rao VM, Karasick D. Hypercementosis-An important clue to Paget disease of the maxilla. Skeletal Radiol 1982;9: 126-128.
128. Smith SJ, Eveson JW. Paget's disease of bone with particular reference to dentistry. J Oral Pathol 1982;10:233-247.
129. Stanley HR. The effect of systemic disease on the human pulp. Oral Surg Oral Med Oral Pathol 1972;33:606-648.
130. Barnett F, Elfenbein L. Paget's disease of the mandible: A review and report of a case. Endod Dent Traumatol 1985;1 :39-42.
131. Malloy PJ, Pike JW, Feldman D. The vitamin D receptor and the syndrome of hereditary 1,25-dihydroxyvitamin D-resistant rickets. Endocr Rev 1999;20: 156-188.
132. van Driel M, Koedam M, Buurman CJ, et al. Evidence for auto/paracrine actions of vitamin D in bone: 1a-hydroxylase expression and activity in human bone cells. FASEB J 2006;20:2417-2419.
133. Zambrano M, Nikitakis NG, Sanchez-Quevedo MC, Sauk JJ, Sedano H, Rivera H. Oral and dental manifestations of vitamin D-dependent rickets type I: Report of a pediatric case. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003;95:705-709.
134. Hewison M, Zehnder D, Bland R, Stewart PM. la-hydroxylase and the action of vitamin D. J Mol Endocrinol 2000;25: 141-148.
135. Kikuchi K, Okamoto T, Nishina M, Takeda E, Kuroda Y, Miyao M. Vitamin D-dependent rickets type II: Report of three cases. ASDC J Dent Child 1988;55:465-468.
136. Sabbagh Y, Jones AO, Tenenhouse HS. PHEXdb, a locus-specific database for mutations causing X-linked hypophosphatemia. Hum Mutat 2000; 16: 1-6.
137. Chaussain-Miller C, Sinding C, Wolikow M, Lasfargues JJ, Godeau G, Garabedian M. Dental abnormalities in patients with familial hypophosphatemic vitamin D-resistant rickets: Prevention by early treatment with 1-hydroxyvitamin D. J Pediatr 2003; 142:324-331.
138. Pereira CM, de Andrade CR, Vargas PA, Coletta RD, de Almeida OP, Lopes MA. Dental alterations associated with X-linked hypophosphatemic rickets. J Endod 2004;30:241-245.
139. Bender IB, Naidorf I. Dental observations in vitamin D-resistant rickets with special reference to periapical lesions. J Endod 1985;11 :514-520.
140. Baroncelli GI, Angiolini M, Ninni E, Galli V, Saggese R, Giuca MR. Prevalence and pathogenesis of dental and periodontal lesions in children with X-linked hypophosphatemic rickets. Eur J Paediatr Dent 2006;7:61-66.
141. Goodman JR, Gelbier MJ, Bennett JH, Winter GB. Dental problems associated with hypophosphataemic vitamin D resistant rickets. Int J Paediatr Dent 1998;8: 19-28.
142. Hillmann G, Geurtsen W. Pathohistology of undecalcified primary teeth in vitamin D-resistant rickets. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1996;82:218-224.
143. Murayama T, lwatsubo R, Akiyama S, Amano A, Morisaki I. Familial hypophosphatemic vitamin D-resistant rickets: Dental findings and histologic study of teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000;90: 310-316.
144. Hazza'a AM, Al-Jamal G. Dental development in subjects with thalassemia major. J Contemp Dent Pract 2006;7:63-70.
145. Rund D, Rachmilewitz E. 13-Thalassemia. N Engl J Med 2005;353: 1135-1146.
146. Abu Alhaija ES, Hattab FN, al-Omari MA. Cephalometric measurements and facial deformities in subjects with 13-thalassaemia major. Eur J Orthod 2002;24:9-19.
147. Olivieri NF. The 13-thalassemias. N Engl J Med 1999;341:99-109. 148. Amini F, Jafari A, Eslamian L, Sharifzadeh S. A cephalometric study on cra
niofacial morphology of Iranian children with 13-thalassemia major. Orthod Craniofac Res 2007; 10:36-44.
149. da Fonseca MA, Oueis HS, Casamassimo PS. Sickle cell anemia: A review for the pediatric dentist. Pediatr Dent 2007;29: 159-169.
150. Stuart MJ, Nagel RL. Sickle-cell disease. Lancet 2004;364:1343-1360.
490
151. Kavadia-Tsatala S, Kolokytha 0, Kaklamanos EG, Antoniades K, Chasapopoulou E. Mandibular lesions of vasoocclusive origin in sickle cell hemoglobinopathy. Odontology 2004;92:68-72.
152. Lawrenz DR. Sickle cell disease: A review and update of current therapy. J Oral Maxillofac Surg 1999;57:171-178.
153. Bishop K, Briggs P, Kelleher M. Sickle cell disease: A diagnostic dilemma. Int Endod J 1995;28:297-302.
154. Demirba� Kaya A, Aktener BO, Unsal C. Pulpal necrosis with sickle cell anaemia. Int Endod J 2004;37:602-606.
155. Kelleher M, Bishop K, Briggs P. Oral complications associated with sickle cell anemia: A review and case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1996;82:225-228.
156. Olaitan A, Amuda J, Adekeye E. Osteomyelitis of the mandible in sickle cell disease. Br J Oral Maxillofac Surg 1997;35:190-192.
157. Jmoudiak M, Futerman AH. Gaucher disease: Pathological mechanisms and modern management. Br J Haematol 2005; 129: 178-188.
158. Sidransky E. Gaucher disease: Complexity in a "simple" disorder. Mol Genet Metab 2004;83:6-15.
159. Germain DP. Gaucher's disease: A paradigm for interventional genetics. Clin Genet 2004;65:77-86.
160. Poll LW, Koch JA, vom Dahl S, et al. Extraosseous manifestation of Gaucher's disease type I: MR and histological appearance. Eur Radiol 2000; 10: 1660-1663.
161. Poll LW, Koch JA, vom Dahl S, et al. Type I Gaucher disease: Extraosseous extension of skeletal disease. Skeletal Radiol 2000;29: 15-21.
162. Carter LC, Fischman SL, Mann J, Elstein D, Stabholz A, Zimran A. The nature and extent of jaw involvement in Gaucher disease: Observations in a series of 28 patients. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;85:233-239.
163. Bender IB, Bender AL. Dental observations in Gaucher's disease: Review of literature and two case reports with 13- and 60-year follow-ups. Oral Surg Oral Med Oral Pathol 1996;82:650-659.
164. Karabulut N, Ahmetoglu A, Ariyurek M, Erol C, GOrakan F. Obliteration of maxillary and sphenoid sinuses in Gaucher's disease. Br J Radiol 1997;70:533-535.
165. Wasserstein MP, Martignetti JA, Zeitlin R, et al. Type 1 Gaucher disease presenting with extensive mandibular lytic lesions: Identification and expression of a novel acid 13-glucosidase mutation. Am J Med Genet 1999;84:334-339.
166. Baccaglini L, Schiffmann R, Brennan MT, Lancaster HE Jr, Kulkarni AB, Brahim JS. Oral and craniofacial findings in Fabry's disease: A report of 13 patients. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2001;92: 415-419.
167. Eng CM, Germain DP, Banikazemi M, et al. Fabry disease: Guidlines for the evaluation and mangement of milti-organ system involvement. Genet Med 2006;8:539-548.
168. Harrison M, Odell EW, Sheehy EC. Dental findings in Lowe syndrome. Pediatr Dent 1999;21 :425-428.
169. Lin T, Orrison BM, Leahey AM, et al. Spectrum of mutations in the OCRL 1 gene in the Lowe oculocerebrorenal syndrome. Am J Hum Genet 1997;60:1384-1388.
170. Dale DC, Person RE, Bolyard AA, et al. Mutations in the gene encoding neutrophil elastase in congenital and cyclic neutropenia. Blood 2000;96:2317-2322.
171. Horvvitz M, Benson KF, Person RE, Aprikyan AG, Dale DC. Mutations in ELA2, encoding neutrophil elastase, define a 21-day biological clock in cyclic haematopoiesis. Nat Genet 1999;23:433-436.
172. Nakai Y, Ishihara C, Ogata S, Shimono T. Oral manifestations of cyclic neutropenia in a Japanese child: Case report with a 5-year follow-up. Pediatr Dent 2003;25:383-388.
173. Pernu HE, Pajari UH, Lanning M. The importance of regular dental treatment in patients with cyclic neutropenia. Follow-up of 2 cases. J Periodontal 1996;67:454-459.
174. Ahuja V, Shin RH, Mudgil A, Nanda V, Schoor R. Papillon-Lefevre syndrome: A successful outcome. J Periodontal 2005;76:1996-2001.
175. Hart TC, Hart PS, Bowden DW, et al. Mutations of the cathepsin C gene are responsible for Papillon-Lefevre syndrome. J Med Genet 1999;36:881-887.
www.shayanNemodar.com
176. Hart TC, Stabholz A, Meyle J, et al. Genetic studies of syndromes with severe periodontitis and palmoplantar hyperkeratosis. J Periodontal Res 1997;32(1 Pt 2):81-89.
177. Ullbro C, Twetman 5. Review paper: Dental treatment for patients with Papillon-Lefevre syndrome (PLS). Eur Arch Paediatr Dent 2007;8(suppl 1 ): 4-11.
178. Delcourt-Debruyne EM, Boutigny HR, Hildebrand HF. Features of severe periodontal disease in teenager with Chediak-Higashi syndrome. J Periodontol 2000;71 :816-824.
179. Karim MA, Suzuki K, Fukai K, et al. Apparent genotype-phenotype correlation in childhood, adolescent, and adult Chediak-Higashi syndrome. Am J Med Genet 2002; 108: 16-22.
180. Shibutani T, Gen K, Shibata M, Horiguchi Y, Kondo N, lwayama Y. Longterm follow-up of periodontitis in a patient with Chediak-Higashi syndrome. A case report. J Periodontol 2000;71: 1024-1028.
181. Baldini A. DiGeorge syndrome: An update. Curr Opin Cardiol 2004;19:201-204.
182. Danpure CJ. Molecular aetiology of primary hyperoxaluria type 1. Nephron Exp Nephrol 2004;98:e39-e44.
183. Moskow B. Periodontal manifestations of hyperoxaluria and oxalosis. J Periodontol 1989;60:271-278.
184. Rahima M, DiMauro M. Primary hyperoxaluria in a pediatric dental patient: A case report. Pediatr Dent 1992;14:260-262.
185. Centers for Disease Control and Prevention. National Diabetes Fact Sheet 2011. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, 2011. http://www.cdc.gov/diabetes/pubs/ pdf/ndfs_2011.pdf. Accessed July 2011.
186. Fouad AF. Diabetes mellitus as a modulating factor of endodontic infections. J Dent Educ 2003;67:459-467.
187. Mealey BL. Diabetes and periodontal disease: Two sides of a coin. Compend Conlin Educ Dent 2000;21 :943-946,948,950,952-954.
188. Peleg AY, Weerarathna T, McCarthy JS, Davis TM. Common infections in diabetes: Pathogenesis, management and relationship to glycaemic control. Diabetes Metab Res Rev 2007;23:3-13.
189. Scannapieco FA. Position paper of the American Academy of Periodontology: Periodontal disease as a potential risk factor for systemic diseases. J Periodontol 1998;69:841-850.
190. Grossi SG. Treatment of periodontal disease and control of diabetes: An assessment of the evidence and need the need for future research. Ann Periodontol 2001;6:138-145.
191. Soory M. Hormone mediation of immune responses in the progression of diabetes, rheumatoid arthritis and periodontal diseases. Curr Drug Targets Immune Endocr Metabol Disord 2002;2: 13-25.
192. Abularrage CJ, Sidawy AN, Aidinian G, Singh N, Weiswasser JM, Arora S. Evaluation of the microcirculation in vascular disease. J Vase Surg 2005;42:574-581.
193. Bierhaus A, Humpert PM, Morcos M, et al. Understanding RAGE, the receptor for advanced glycation end products. J Mol Med 2005;83:876-886.
194. Garcia RI, Henshaw MM, Krall EA. Relationship between periodontal health and systemic health. Periodontol 2000 2001;25:21-36.
195. Miley DD, Terezhalmy GT. The patient with diabetes mellitus: Etiology, epidemiology, principles of medical management, oral disease burden, and principles of dental management. Quintessence Int 2005;36:779-795.
196. Sampathkumar R, Balasubramanyam M, Rema M, Premanand C, Mohan V. A novel advanced glycation index and its association with diabetes and microangiopathy. Metabolism 2005;54: 1002-1007.
197. Grossi SG, Skrepcinski FB, Decaro T, Zambon JJ, Cummins D, Genco RJ. Response to periodontal therapy in diabetics and smokers. J Periodontol 1996;67: 1094-1102.
198. Mealey BL, Rose LF. Diabetes mellitus and inflammatory periodontal diseases. Curr Opin Endocrinol Diabetes Obes 2008; 15: 135-141.
199. Chandu A, Macisaac RJ, Smith AC, Bach LA. Diabetic ketoacidosis secondary to dento-alveolar infection. Int J Oral Maxillofac Surg 2002;31: 57-59.
200. Bender IB. Diabetes mellitus and the dental pulp. J Endod 2003;29: 383-389.
201. Britto LR, Katz J, Guelmann M, Heft M. Periradicular radiographic assessment in diabetic and control individuals. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003;96:449-452.
References
202. Fouad FF, Burleson J. The effect of diabetes mellitus on endodontic treatment outcome: Data from an electronic patient record. J Am Dent Assoc 2003; 134:43-51.
203. Leite MF, Ganzerla E, Marques MM, Nicolau J. Diabetes induces metabolic aleterations in dental pulp. J Endod 2008;34: 1211-1214.
204. Schulze A, Schiinauer M, Busse M. Sudden improvement of insulin sensitivity related to an endodontic treatment. J Periodontol 2007;78:2380-2384.
205. Segura-Egea JJ, Jimenez-Pinzon A, Rios-Santos JV, Velasco-Ortega E, Cisneros-Cabello R, Poyato-Ferrera M. High prevalence of apical periodontitis amongst type 2 diabetic patients. Int Endod J 2005;38:564-569.
206. Huber MA, Terezhalmy GT. The patient with a transient bacteremia. Gen Dent 2005;53: 130-143.
207. Chrousos GP, Kino T. Glucocorticoid action networks and complex psychiatric and/or somatic disorders. Stress 2007;10:213-219.
208. Makino S, Hashimoto K, Gold PW. Multiple feedback mechanisms activating corticotropin-releasing hormone system in the brain during stress. Pharmacol Biochem Behav 2002;73: 147-158.
209. Negrao AB, Deuster PA, Gold PW, Chrousos GP. Individual reactivity and physiology of the stress response. Biomed Pharmacother 2000;54: 122-128.
210. Tsigos C, Chrousos GP. Hypothalamic-pituitary-adrenal axis, neuroendocrine factors and stress. J Psychosom Res 2002;53:865-871.
211. Shibli-Rahhal A, Van Beek M, Schlechte JA. Cushing's syndrome. Clin Dermatol 2006;24:260-265.
212. Marik PE, Zaloga GP. Adrenal insufficiency in the critically ill. A new look at an old problem. Chest 2002; 122: 1784-1796.
213. Udelsman R, Norton JA, Jelenich SE, et al. Response of the hypothalamicpituitary-adrenal and renin-angiotensin axes and the sympathetic system during controlled surgical and anesthetic stress. J Clin Endocrinol Metab 1987;64:986-994.
214. Zaloga GP, Marik P. Hypothalamic-pituitary-adrenal insufficiency. Crit Care Clin 2001;17:25-41.
215. Newton R. Molecular mechanisms of glucocorticoid action: What is important? Thorax 2000;55:603-613.
216. Coursin DB, Wood KE. Corticosteroid supplementation for adrenal insufficiency. J Am Med Assoc 2002;287:236-240.
217. Huber MA, Terezhalmy GT. Risk stratification and dental management of patients with adrenal dysfunction. Quintessence Int 2007;38:325-338.
218. Bornstein SR. Predisposing factors for adrenal insufficiency. N Engl J Med 2009;360:2328-2339.
219. Tsigos C, Chrousos GP. Differential diagnosis and management of Cushing's syndrome. Ann Rev Med 1996;47:443-461.
220. Magiakou MA, Mastorakos G, Oldfield EH, et al. Cushing's syndrome in children and adolescents. N Engl J Med 1994;331 :629-636.
221. Boscaro M, Barzon L, Fallo F, Sonino N. Cushing's syndrome. Lancet 2001; 357:783-791.
222. Alliot-Licht B, Bluteau G, Magne D, et al. Dexamethasone stimulates differentiation of odontoblast-like cells in human dental pulp cultures. Cell Tissue Res 2005;321:391-400.
223. Huang GT, Shagramanova K, Chan SW. Formation of odontoblast-like cells from cultured human dental pulp cells on dentin in vitro. J Endod 2006;32: 1066-1073.
224. Wysocki GP, Valey TD, Ulan RA. Predentin changes in patients with chronic renal failure. Oral Surg Oral Med Oral Pathol 1983;56: 167-173.
225. Salem M, Tainsh RE Jr, Bromberg J, Loriaux DL, Chernow B. Perioperative glucocorticoid coverage. A reassessment 42 years after emergence of a problem. Ann Surg 1994;219:416-425.
226. Schiff RL, Welsh GA. Perioperative evaluation and management of the patient with endocrine dysfunction. Med Clin North Am 2003;87: 175-192.
227. Schlaghecke R, Kornely E, Santen RT, Ridderskamp P. The effect of longterm glucocorticoid therapy on pituitary-adrenal responses to exogenous corticotropin-releasing hormone. N Engl J Med 1992;326:226-230.
228. Graham GW, Unger BP, Coursin DB. Perioperative management of selected endocrine disorders. Int Anesthesiol Clin 2000;38:31-67.
229. Kehlet H, Binder C. Adrenocortical function and clinical course during and after surgery in unsupplemented glucocorticoid-treated patients. 1973;45: 1043-1048.
491 www.shayanNemodar.com
Interrelationship of Pulp and Systemic Disease
230. Miller CS, Little JW, Falace DA. Supplemental corticosteroids for dental patients with adrenal insufficiency. Reconsideration of the problem. J Am Dent Assoc 2001;132:1570-1579.
231. Neuhaus K. Teeth: Malignant neoplasms in the dental pulp? Lancet Oncol 2007;8:75-78.
232. Ahmad S, Roberts GJ, Lucas VS, Barrett AW, Harkness W. Metastatic infiltration of the dental pulp by medulloblastoma. J Oral Pathol Med 2002;31 :244-245.
233. Baumgartner JC, Heggers JP, Harrison JW. The incidence of bacteremias related to endodontic procedures. I. Nonsurgical endodontics. J Endod 1976;2:135-140.
234. Bavitz JB, Patterson OW, Sorensen S. Non-Hodgkin's lymphoma disguised as odontogenic pain. J Am Dent Assoc 1992; 123:99-100.
235. Bornstein MM, von Arx T, Altermatt HJ. Loss of pulp sensitivity and pain as the first symptoms of a Ewing's sarcoma in the right maxillary sinus and alveolar process: Report of a case. J Endod 2008;34:1549-1553.
236. Heng C, Heng J. Implications of malignant lymphoma on a periapical mandibular lesion. Gen Dent 1995;43:454-458.
237. Hiraki A, Nakamura S, Abe K, et al. Numb chin syndrome as an initial symptom of acute lymphocytic leukemia: Report of three cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1997;83:555-561.
238. Kanas R, Jensen J, DeBoom G. Painful, nonhealing tooth extraction socket. J Am Dent Assoc 1986; 113:441-442.
239. Keyes GG, Balaban FS, Lattanzi DA. Periradicular lymphoma: Differentiation from inflammation. Oral Surg Oral Med Oral Pathol 1988;66:
230-235.
240. Landesberg R, Yee H, Datikashvili M, Ahmed A. Unilateral mandibular lip anesthesia as the sole presenting symptom of Burkitt's lymphoma: Case report and review of the literature. J Oral Maxillofac Surg 2001;59:
322-326.
241. Levi PA Jr, Kim OM, Harsfield SL, Jacobson ER. Squamous cell carcinoma presenting as an endodontic-periodontic lesion. J Periodontol 2005;76: 1798-1804.
242. Maygarden S, Askin F, Burkes E, McMillan C, Sanders J. Isolated extramedullary relapse of acute myelogenous leukemia in a tooth. Mod Pathol 1989;2:59-62.
243. Morgan L. Infiltrate of chronic lymphocytic leukemia appearing as a periapical radiolucent lesion. J Endod 1995;21 :475-478.
244. Peterson D, Gerad H, Williams L. An unusual instance of leukemic infiltrate. Diagnosis and management of periapical tooth involvement. Cancer 1983;51: 1716-1719.
245. Pruckmayer M, Glaser C, Marosi C, Leitha T. Mandibular pain as the leading clinical symptom for metastatic disease: Nine cases and review of the literature. Ann Oncol 1998;9:559-564.
492
246. Selden H, Mannhoff D, Hatges N, Michel R. Metastatic carcinoma to the mandible that mimicked pulpal/periodontal disease. J Endod 1998;24:267-270.
247. Shankar S. Dental pulp metastases and pan-osseous mandibular involvement with mammary adenocarcinoma. Br J Oral Maxillofac Surg 1984;22:455-461.
248. Svoboda W, Aaron G, Albano E. North American Burkitt's lymphoma presenting with intraoral symptoms. Pediatr Dent 1991;13:52-58.
249. Thompson 10, Phillips VM, Kalan M. Metastatic squamous cell carcinoma manifesting as a periapical lesion. J Dent Assoc S Afr 1992;47:481-483.
250. Todd H, Langeland K. Pulpal destruction of neoplastic etiology. J Endod 1987; 13:299-301.
251. Tsui S, Wong M, Lam W. Burkitt's lymphoma presenting as mandibular swelling-Report of a case and review of publications. Br J Oral Maxillofac Surg 2000;38:8-11.
252. D'Silva NJ, Summerlin DJ, Cordell KG, et al. Metastatic tumors in the jaws: A retrospective study of 114 cases. J Am Dent Assoc 2006; 137: 1667-1672.
253. Kuttan NA, Flemming DK, Dane JN, Ang DB. Metastatic lesion of the anterior mandible with an occult primary: A case report. Spec Care Dentist 2006;26:76-80.
254. Dahlliif G. Craniofacial growth in children treated for malignant disease. Acta Odontol Scand 1998;56:378-382.
255. Hiiltta P, Hovi L, Saarinen-Pihkala UM, Peltola J, Alaluusua S. Disturbed root development of permanent teeth after pediatric stem cell transplantation. Dental root development after SCT. Cancer 2005; 103: 1484-1493.
256. Huber MA, Terezhalmy GT. The head and neck radiation oncology patient. Quintessence Int 2003;34:693-717.
257. Kaste SC, Hopkins KP, Jones D, Crom D, Greenwald CA, Santana VM. Dental abnormalities in children treated for acute lymphoblastic leukemia. Leukemia 1997;11:792-796.
258. Lilly JP, Cox D, Arcuri M, Krell KV. An evaluation of root canal treatment in patients who have received irradiation to the mandible and maxilla. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;86:224-226.
259. Minicucci EM, Lopes LF, Crocci AJ. Dental abnormalities in children after chemotherapy treatment for acute lymphoid leukemia. Leuk Res 2003;27:45-50.
260. Oguz A, Cetiner S, Karadeniz C, Alpaslan G, Alpaslan C, Pinarli G. Longterm effects of chemotherapy on orodental structures in children with nonHodgkin's lymphoma. Eur J Oral Sci 2004; 112:8-11.
261. Springer IN, Niehoff P, Warnke PH, et al. Radiation caries-Radiogenic destruction of dental collagen. Oral Oncol 2005;41 :723-728.
262. Kielbassa AM, Attin T, Schaller HG, Hellwig E. Endodontic therapy in a postirradiated child: Review of the literature and report of a case. Quintessence Int 1995;26:405-411.
www.shayanNemodar.com
Page numbers followed by "f" denote figures; "t" tables; and "b" boxes
A A fibers, 135--137, 148, 150f, 434 Aj3 fibers, 136--137 Acetaminophen, 193-195, 200 Acid etching
description of, 48, 340 illustration of, 49f microcirculatory effects, 126 reactionary dentin stimulated by, 38
Actinomyces species, 214, 220, 234, 37 6f Adaptive immune responses, 285-287 Adaptive immunity, 329 Addison disease, 485--486 AO fibers, 137, 167, 177-178 Adhesion molecules, 247-248, 250 Adhesion restorations, 323, 344 Adhesive dentistry, 323 Adhesive luting cements, 323 Adhesive resin systems, 312-313 Adhesives, 312-313
chronologic classification of, 337 etch-and-rinse, 336 self-etching, 336
Adrenal dysfunction, 485--486 Advanced glycation end-products, 485 Afferent nerve fibers, 147 Aging
biologic changes associated with, 431-436 blood vessels affected by, 432-434 cellular behavior affected by, 432 degenerative processes induced by, 431 dentinal sensitivity and, 177 dentinogenesis changes, 431, 438-440 disease versus, 422 intratubular and intertubular dentin formation
secondary to, 440 odontoblast changes secondary to, 427, 429-
430 oral health during, 421 overview of, 421 oxidative stress theory of, 423-424 process of, 421-425 pulp capping considerations, 441-442 pulp testing responses to evaluate effects of,
436-437 pulpal changes secondary to, 425-442 pulpodentin complex changes secondary to,
334,427,440-442 radiographic signs of, 441 root canal revascularization using blood clotting
affected by, 101 senescence and, 421-423 sensory nerves affected by, 434-436 telomeres, 423-425, 431
Airborne particle abrasion, 367-368 Allergy-induced sinusitis, 455 Allodynia, 449
central mechanisms of, 171-173, 172b characteristics of, 169t, 169-170 definition of, 169
Index
peripheral mechanisms of, 170b, 170--171 Allogeneic bone marrow transplantation, 93-94 Allogeneic stem cells, 95 a-Adrenergic receptors, 118f Amalgam, 344 Ameloblasts, 4, 17f Amelogenesis imperfecta, 477, 477t Amelogenins, 316 Anemia
Cooley, 481 sickle cell, 464, 481-482, 482f
Antigen I/Ii, 221 Antigen-presenting cells, 80, 269-270 Antigen-presenting dendritic cells, 277-278 Anti-inflammatory cytokines, 268-269 Antimicrobial agents, 208 Apical foramen, 101, 375, 3811 Apical periodontitis
definition of, 206, 222, 278 external root resorption and, 404-405 periapical responses, 277-282 persistence of, 232f pulpal responses, 277-278 radiograph of, 206f symptomatic, 231 treatment of, 234-235
Apoptosis, 33, 311 Arachidonic acid metabolites, 250--252, 254-
255, 290--291 Archaea, 231 Argon laser, 359 Arterioles, 109-110, 11 Of, 1211, 127f Arteriovenous anastomosis
shunts, 111 Y-shaped, 112f
Atypical odontalgia, 461-462 Autologous stem cells, 94-95, 104 Avulsion, 386 Axon degeneration, 147
B B cells, 80, 279, 283b Bacteria
antibacterial agents, 221 beneficial types of, 214 in biofilm
community lifesty le of, 207-208 intercommunication among, 208-209 quorum sensing, 208-209
cariogenic, 213-215, 216t coaggregation of, 210 endodontic infections, 222 endodontic-periodontal diseases caused by,
377-378 fluoride effects on metabolism by, 222 Gram-negative, 227b Gram-positive, 227b microleakage of, 303, 343 mutans streptococci, 213-214 nutrients for, 230 primary intraradicular infections caused by,
226--228, 227b proteolytic, 377
pulpal healing affected by, 302-303 Streptococcus mutans, 214
Bacterial sinusitis, 455 Basement membrane, 73 Bay cysts, 3811, 381-382 Bead implantation assays, 6, 6f Bell stage, of tooth development, 3f, 4 j3-Adrenergic receptors, 119 Bifidobacterium species, 215 Bioactive molecule-containing materials, 315--
317 Biofilm, plaque
antimicrobial resistance of, 208 bacteria in. See Bacteria, in biofilm. caries formation secondary to, 211-212. See
also Caries. characteristics of, 207 definition of, 206--207 disease enhancement, 208 endodontic-periodontal infections caused by,
379 extracellular matrix formation, 207 formation of, 209f, 209-210 illustration of, 207f infectious, 379 microcolonies in, 207
Bleaching intracoronal, 410 lasers for, 367
Blood clotting, for root canal revascularization, 100--101, 102t
Blood vessels aging effects on, 432-434 arterioles, 109-110, 11 Of, 1211, 127f capillaries, 110--111 venules, 111
Bonding. See Dentin bonding. Bone morphogenetic proteins
BMP-4, 11 calcitonin gene-related peptide effects, 63 enamel knots and, 14 expression of, 111 function of, 77, 97t odontoblast differentiation, 355 source of, 97t tooth development role of, 10--11, 11 f
Bone sialoprotein, 18, 18t, 20, 211, 74 Bradykinin, 123, 256 Bud stage, of tooth development, 2, 3f
c C fibers, 135--137, 148-150, 434 Calcific metamorphosis, 314 Calcitonin gene-related peptide, 63, 70, 121-
123, 136, 139,243-247,434,436 Calcium hydroxide, 305
antimicrobial properties of, 308-309 caustic actions of, 308 dentin adhesives vs, 312-313 dentinal bridges created using, 308-310, 314 description of, 71, 308 mineral trioxide aggregate vs, 314 outcomes of, 310
493 www.shayanNemodar.com
Index
pulp inflammatory responses caused by, 315 reactionary dentin deposition affected by, 342 reparative dentin formation, 308 resin-modified glass ionomers vs, 312 zinc oxide-eugenol vs, 318
Calcospherites, 31, 31f, 48 Cancer. 486-487 Candida albicans, 378 Cannabinoid receptors, 164 Cap stage, of tooth development, 2-3, 3f Capillaries, 11�111 Capillary filtration, 114 Capillary network, 111 Capsaicin, 122, 149, 245, 462 Carbohydrates, 213, 220 Caries
antibacterial control for. 22�221 bacteria associated with, 213--215, 216t, 22�
221, 224 categories of, 211-212 cavitation caused by, 217f characteristics of, 325--328 childhood, 215, 343 deep, 217f, 332f definition of, 211 dendritic cells' response to, 85 dentinal, 216f, 216t, 216-218, 326, 327f-328f description of, 205 diagnosis of. 218f, 218--219 diet and, 218, 220 ecological plaque hypothesis of, 212-213,
213f economic burden of, 206 enamel, 211 etiology of, 212-215, 317 fluoride for. 221-222 global prevalence of, 205--206 hand instruments used to remove, 318 immunocompetent cells' response to, 85--86 nonspecific plaque hypothesis of, 212 nursing, 215 occlusal, 216t, 307f, 330f, 332f pathogenesis of, 212 prevalence of, 205 prevention of, 22�222 primary, 212, 325 progression of, 327 progressive, 206f pulp exposure caused by, 224, 224f pulpal responses to, 331 radiographs of, 218, 218f recurrent, 211-212, 218-219 remaining, 212 root, 211, 216t saliva and, 218, 220 secondary, 211, 325 sequelae of, 205 smooth surface, 216t specific plaque hypothesis of, 212 treatment of, 219-220, 326 vaccine for. 221 white-spot lesion presentation of, 211, 211 f zone of destruction, 216, 217f
Carious dentin, 324 Cavity preparation
dentin permeability effects, 61-62 heat production during
causes of, 335 inflammation secondary to, 170
immunocompetent cells' response to, 84-85 mechanical stimuli during, 353--355 odontoblast disruptions caused by, 75, 341 pulpal injury caused by, 334--335 tertiary dentinogenesis effects, 35 thermal stimuli during, 349-353
CD4' T cells, 279 CD8' T cells, 279 Cell adhesion molecules, 248
494
Cell-rich layer of Hiihl, 28, 41 Cell-rich zone, 68 Cementoblasts, 282, 398 Cementodentin junction, 405 Cementoenamel junction, 56, 353 Cementum, 58, 398--399 Central sensitization, 171-173 Cervical loop, 4 C-factor. 338--339 Charcot-Leyden crystals, 383, 384f Chediak-Higashi syndrome, 484t Chemoattractants
in leukocyte adhesion, 250 transforming growth factor-[31, 41
Chemokines, 269, 282, 287 Chickenpox, 473 Childhood caries, 215, 343 Chlorhexidine gluconate, 221, 319 Cholesterol crystals, 382, 382f Chronic paroxysmal hemicrania, 457 Chronic periapical lesions, 281 Circulatory system. See Microcirculatory system,
of pulp. Clotting system, 257-259 Cluster headache, 457-458 co2 lasers, 361-362 Coaggregation, 210 Cocci, 227b, 229 Cold stimuli, for pulpal vitality testing, 179-180 Collagen
age-related changes in, 427-428 basement membrane expression of, 14-15 biosynthesis of. 71-72 characteristics of, 67 chemical composition of, 70 definition of, 70, 76 degradation of, 71 dentin types of, 16 intraluminal, SH odontoblast synthesis of, 29 in pulp, 7�71 reverse transcriptase-polymerase chain reaction
amplification of, 9f structure of, 70 type I, 70 type II, 70 type Ill, 70 type V, 70 type VI, 70
Collagen fibrils, 31, 7�71, 71f Colony-stimulating factor. 97t Connective tissue
definition of, 67 extracellular matrix, 67 function of, 67
Continuous capillary, 111 Convergence theory, 176-177, 448--449 Cooley anemia, 481 Core-binding factor a1, 12, 13f, 432 Coronal leakage, 384-385 Coronal pulp, 71f Coronal restoration, 385 Corticosteroids, 195 Crown fracture, 304, 385 Crown-root fracture, 385--386 Cushing syndrome, 485-486 Cusp
fracture of, 385 morphogenesis of, 14, 15f
Cyclic neutropenia, 484t Cyclo-oxygenases
arachidonic acid metabolites synthesized by, 25�251
inhibitors of, 194 Cyclophosphamide, 283--284 Cysteine cathepsins, 318, 326 Cysts, 381f, 381-382 Cytokines
anti-inflammatory, 268--269 functional studies of, 292-293 inflammatory role of, 263 osteoclast activity inhibited by, 292 proinflammatory, 264-268, 265f, 287-289,
291-293 secretion of, 263
Cytomegalovirus, 231, 379 Cytotoxic T cells, 79, 278
D Deafferentation, 461-462 Decorin, 18t 72, 73f Deep caries, 217f Defensins, 270 Demineralization
description of, 212 fluoride effects on, 221-222
Dendritic cells, 82-84, 83f, 279-280, 283b, 400 Dens evaginatus, 475-476 Dens in dente (dens invaginatus), 475f, 475-476 Dental epithelium, 4 Dental follicle, 2, 4 Dental follicle progenitor cells, 95 Dental plaque. See Plaque. Dental pulp constructs, 98--100, 99f, 102t Dentin. See also Pulpodentin complex.
acid etching of, 48, 49f apical, 59-60 axial, 56 caries-affected, 325--326, 327f-328f carious, 324, 328 characteristics of, 52-53, 53t, 62 coefficients of thermal expansion, 350 collagen types in, 16 composition of, 52, 52t, 335 definition of, 48 depth-related changes in structure of, 5�52 exposure of, 62 formation of, 16 grinding of, effect on pulpal blood flow, 125f hereditary opalescent, 476 intertubular. 32, 49, 440 intratubular. 49, 440 laser effects, 361 mantle, 31, 48, 53t mineralization of, 16, 3�31 morphology of, 48--50 nerve endings in, 136f neuronal desensitivity, 187-190 noxious substance permeation in, �2 periluminal, 49 peritubular. 32, 32f. 49, 52, 438 permeability
cavity preparations effect, 61-62 cementum effects, 58--59 dentinal thickness and, 56f depth, 54 description of, 69 factors that affect, 56, 69 illustration of, 55f importance of, 441 noxious substances, �2 pulpal blood flow effects, 61 restorative procedures effect, 61-62 smear layer effects, 57-59 tubular occlusion, 328 types of, 54 uniformity of, 55, 58
physical characteristics of, 52-53, 53t porosity of, 54-55 primary, 27, 28f, 48 reactionary
cavity etching stimulation of, 38 cellular signaling of, 38 definition of, 34, 78, 324 deposition areas for, 334 ethylenediaminetetraacetic acid effects, 38
www.shayanNemodar.com
production of, 333 remaining dentinal thickness effects, 37-38 restorative materials effect on formation of,
342-343 remaining thickness, 37-38, 325, 334--335 remodeling of, 30 reparative, 34, 78, 308, 324 resorption of, 411 root
impermeability of, 58 mechanics of, 53-54 permeability of, 56f, 56-60
sclerotic description of, 327 illustration of, 32f permeability of, 56
secondary, 27, 33-34, 48--49, 78, 430, 433, 438--439
secretory model of, 29-30, 32-33 softness of, 52 tensile strength of, 52-53 tertiary, 27, 34--35, 49, 49f, 78, 317, 324 thermal properties of, 335, 349, 350t thickness of, 49, 325 trauma-induced exposure of, 224 water content of, 51-52
Dentin adhesives, 312-313 Dentin bonding
glass ionomers for, 312, 337-338 history of, 335 limitations of, 338-340 polymerization shrinkage concerns, 338 pulp affected by, 340--341 resin-based materials for, 335-337, 336f resin-modified glass ionomers for, 312, 338
Dentin chips, 99, 304--305 Dentin dysplasia, 476 Dentin matrix
composition of, 17-18 growth factors in, 36 lateral branches of, 30, 30f odontoblast-like cell differentiation induced
by, 41 remodeling of, 29-30 secondary, 34 vesicle, 31f
Dentin matrix protein 1, 18, 18t, 20, 21f, 430 Dentin phosphoproteins, 18-19, 29 Dentin sialophosphoprotein, 8, 17-19, 310, 476 Dentin sialoprotein, 18, 74, 76, 476 Dentinal bridge
calcium hydroxide for creating, 308-310 defects, 43 formation of, 43, 71 vital pulp therapy and, 306-307
Dentinal caries, 216f, 216t, 216-218 Dentinal fluid, 52f, 55f
description of, SO flow
evaporative, 352 sensitivity management by reduction of,
186-187 pain perception secondary to movement of,
177 Dentinal sensitivity
age and, 177 characteristics of, 177-178 desensitizing agents for
fluoride-containing medications, 189 guanethidine, 189-190 potassium-containing dentrifices, 188-189,
188t-189t strontium chloride solutions, 189
diagnosis of, 190--191 hydrodynamic theory of, 177-178 inflammation effects, 178 lasers for, 365-367 management of, 185-190
mechanisms of, 177-178 neuronal desensitivity, 187-190 neurophysiology of, 151-152 overview of, 185-186 prevalence of, 185-186 risk factors, 185
Dentinal tubules aging changes, 441 anatomy of, 223 bacteria in, 51f caries infections in, 317 cocci in, 229f convergence of, 49 density of, 51t, 54--56, 57f, 60, 324 diameter of, 51t exposed,373-374,374f innervation of, 177 microleakage, 60 permeability
description of, 50, 54 sensitivity management by reductions in,
186-187 scanning electron micrograph of, 223f sclerosis effects, 319, 331 shape of, 30, 31f, 31-32
Dentinoenamel junction, 48-50, 216 Dentinogenesis
aging effects on, 431, 438-440 definition of, 430 glycosaminoglycans' role in, 72 primary, 31-33, 430 reactionary
biologic processes, 35f-36f, 35-37 definition of, 35, 331, 333 factors that affect, 37-38 histomorphometric findings, 37-38 odontoblast upregulation during, 35-37 restorative materials that cause, 35-36
reparative biologic processes during, 35f collagen fibrils in, 72 definition of, 333 dentin bridge formation vs, 43 description of, 38 fibrodentin matrix secreted before, 39 histologic findings, 38, 39f matrices secreted during, 38, 39f-40f odontoblast-like cell differentiation, 41-43 progenitor cell recruitment in, 40-41 tertiary dentinogenesis and, 39
secondary, 33-34 tertiary
cavity preparation materials that affect, 35-36 description of, 34--35 transforming growth factor-j31 's role in, 36
Dentinogenesis imperfecta, 16, 17f, 476f, 476-477
Dentrifices, 188-189, 188t-189t Developmental malformations, 387 Diabetes mellitus, 484-485 Digastric muscle, 454f DiGeorge syndrome, 285-286, 484t Direct pulp capping, 340 Discontinuous capillary, 111 Diversity of microbiota, 226 DNA chips, 22 Dysfunctional pain, 175
E Ecological plaque hypothesis, 212-213, 213f Ectomesenchyme, 2 EDTA-soluble dentin matrix protein preparation,
342 Eicosanoids. See Arachidonic acid metabolites. Elderly, 421 Embryonic stem cells, 93-94 Enamel caries, 211 Enamel cracks, 224
Index
Enamel fracture, 385 Enamel knots, 14, 15f Enamel matrix derivative, 316 Endocrine disorders
diabetes mellitus, 484-485 glucocorticoid excess, 485-486
Endodontic disease periodontal disease and, 389-392, 389f-392f primary, 388, 392
Endodontic infections archaea, 231 characteristics of, 225b description of, 222 extraradicular, 234 fungi that cause, 231 microbiota associated with, 226-228, 227b,
228f, 230--232 pathogenesis of, 222-224 persistent, 225b persistent intraradicular, 225b, 232-234 primary intraradicular
characteristics of, 225b, 226 description of, 225-226 geographic influences, 228-229 microbiota associated with, 226-228, 227b, 228f,
230 routes of, 223f secondary intraradicular, 225b, 232-234 treatment of, 234--235, 406 types of, 225-234 viruses that cause, 231-232
Endodontic therapy microcirculatory system effects, 126 pain continuance after
description of, 173-174 local anesthetics for, 195-196 management strategies for, 199-200 nonsteroidal anti-inflammatory drugs for, 193-
194, 199-200 Endodontic-periodontal diseases
anatomical relationships, 373-375 contributing factors
avulsion, 386 coronal leakage, 384 crown fracture, 385 crown-root fracture, 385-386 developmental malformations, 387 enamel fracture, 385 luxation, 386 perforation, 386-387 poor endodontic treatment, 384 root fracture, 386, 390 trauma, 385-386
differential diagnosis of, 388-392 etiology of
bacteria, 377-378 Charcot-Leyden crystals, 383, 384f cholesterol crystals, 382, 382f foreign bodies, 380, 380f-381f fungi, 376f, 378 infectious biofilms, 379 live pathogens, 375-379 nonliving pathogens, 380--383 Rushton hyaline bodies, 383, 383f Russell bodies, 382f, 382-383 viruses, 379
overview of, 37 3 portals of exit, 374--375 prognosis for, 392-393
Endogenous opioid peptides, 164 Endothelin 1, 123, 243 Endothelin receptor A, 243 Endothelin receptor B, 243 Enterococcus faecalis, 233 Eosinophils, 283b Epidermal growth factor, 97t Episodic neuropathic pain, 458 Epithelial rests of Malassez, 380
495
www.shayanNemodar.com
Index
Epitheliated granuloma, 380 Epstein-Barr virus, 231-232, 379, 473 Erupting teeth, 142 Er:YAG lasers, 362-36S Etch-and-rinse adhesives, 336 Etchants, 36 Etching. See Acid etching. Ethylenediaminetetraacetic acid, 36, 38, 103,
342, 361 Evaporative fluid flow, 3S2 Evolutionary theory, 422 Excimer lasers, 36S Excitatory amino acids, 162, 16S External root resorption. See Root resorption,
external. Extracellular matrix
basement membrane, 73 collagen. See Collagen . dentin, 9, 440 fibronectin, 73--74 growth factors in, 42 laser capture microdissection studies of, 9 odontoblast secretion modulated by, 33 plaque biofilm formation of, 207 tooth morphogenesis role of, 14--1 S
Extrusive luxation, 386
F Fabry disease, 484t Fenestrated capillary, 111 Fermentable carbohydrates, 213, 220 Fibrillar proteins, 67 Fibrinogen, 2S7, 3S4 Fibroblast(s)
connective tissue remodeling, 79 definition of, 78 functions of, 67 illustration of, 78f interleukin-1 effects, 264 mitotic activity of, 78 morphology of, 78 substance P effects, 70
Fibroblast growth factors, 10--11, 14, 97t Fibrodentin, 39 Fibronectin, 73f. 73-74 Fibronectin-binding protein, 333 Fluorescent antibody cell sorting, 96 Fluoride
caries prevention using, 221-222 dentinal sensitivity managed using, 189
Foreign bodies, 380, 380f-381f FOXP3+CD2S+ cells, 280 Fractures, 385--386 Free radicals, 423--424 Fungi, 231, 376f, 378 Fusobacterium species, 217
G G proteins, 14S Gap junctions, 7 6, 136f Gaucher disease, 482-484, 483f, 483t Gene regulation, 422 Genetic and developmental disorders
amelogenesis imperfecta, 477 dens in dente, 47Sf, 475-476 dentinogenesis imperfecta, 16, 17f, 476f, 47&--
477 Gaucher disease, 482-484, 483f, 483t hemoglobinopathies, 481-482 hypophosphatemic rickets, 479-481, 481f sickle cell anemia, 481-482, 482f taurodontism, 474, 47Sf thalassemia, 481, 482f
German measles, 473--47 4 Glass ionomers
conventional, 337, 337f description of, 312 resin-modified, 312, 338
Glia, 16S
496
Glial-derived neurotrophic factor, 137 Glossopharyngeal neuralgia, 4S9-460 G lucocorticoid excess, 48S-486 Glucocorticoids, 19S Glycosaminoglycans, 4, 67, 72 Golgi complex, 74--7S, 434 G-protein-coupled receptors, 14S Gram-negative bacteria, 227b Gram-positive bacteria, 227b Granulocyte colony-stimulating factor, 284 Granulocyte-macrophage colony-stimulating factor,
287 Growth factors
angiogenic, 36 definition of, 10, 77, 97 in dentin matrix, 36 function of, 97t insulin-like, 36 odontoblast-like cell differentiation induced
by, 42 orthodontic therapy effects, 127 regenerative medicine use of, 9&--98 types of, 97t
Growth-associated protein-43, 137 Guanethidine, 189-190 Gutta-percha, 3S&--3S8
H Hageman factor, 2S7 Hartwig's epithelial root sheath, 397 Hayflick phenomenon, 423 Headache
cluster, 4S7-4S8 migraine, 4SS-4S7
Healing bacteria effects on, 302-303 with cementum, 402 osseous replacement for, 402-403, 403f
Heat shock proteins, 33S, 432 Helper T cells, 79, 278, 280, 291-292 Hemoglobinopathies, 481-482 Hemorrhage control, 305--306 Hereditary opalescent dentin, 476 Herpes zoster, 460 Herpesvirus, 379, 472-473, 473f Heterotypic assays, Sf Histamine, 123, 242 Homeostatic regeneration, 91 Homotypic assays, Sf Horizontal gene transfer, 208 Hot stimuli, for pulpal vitality testing, 179 Human immunodeficiency virus, 286, 379, 471-
472 Humeral immunity, 281-282 Hydroxyapatite crystals
carbonated, 221 characteristics of, SO formation of, 29 nucleation of, 31
Hyperalgesia, 148 central mechanisms of, 171-173, 172b characteristics of, 169t, 169-170 definition of, 169 peripheral mechanisms of, 170b, 170--171
Hyperesthesia, 460 Hyperglycemia, 48S Hyperparathyroidism, 478-479 Hypersensitivity. See Dentinal sensitivity. Hypoesthesia, 460 Hypophosphatemic rickets, 479-481, 481f
Ibuprofen, 193-194 Immune responses
adaptive, 285--287 innate, 283-28S periapical, 277-282
Immunity, 277 lmmunocompetent cells
caries-induced response, 85--86 cavity preparation and restoration effects,
84--8S dendritic cells, 82--84 lymphocytes, 79--81 macrophages, 81--82
Immunodeficiencies description of, 283 innate responses, 283--28S specific responses, 285--287
lmmunoglobulins, 270, 281, 426 Indirect pulp capping, 317-319 Infection. See also Endodontic infections.
in childhood development, 473--474 cytochemical responses to, 139-14S in fetal development, 473--474 intraradicular. See lntraradicular infections. structural responses to, 139-14S
Inflammation dentinal sensitivity caused by, 178 heat-induced, 170--171 humeral immunity in, 281-282 management of, 403 mediators of. See Inflammatory mediators. microcirculatory system effects, 127-128 neuropeptides' role in, 243--247 prostaglandins' role in, 2S1 resident cells in, 282 response to, 16&--167 restorative materials and procedures that
cause, 343f root resorption induced by, 401-402
Inflammatory cyst, 381f Inflammatory mediators
arachidonic acid metabolites, 2S0--2S2, 2S4--2SS, 290--291
chemokines, 269 cytokines, 263--264, 26&--269. See alsoCytokines. defensins, 270 description of. 127-128, 241 drugs that block, 192-19S function of, 241 histamine, 123, 242 immunoglobulins, 270 maresins, 2SS microcirculatory system effects, 127-128 nerve functions affected by, 171-172 neuropeptides, 243--247, 3S4 nitric oxide, 261t, 261-262, 3SS nociceptors sensitized by, 160 nucleotide-binding oligomerization domains,
267-268 odontoblast production of, 242 oxygen-derived free radicals, 262-263 periapical, 287-293 plasma proteases
clotting system, 2S7-2S9 complement system, 2S&--2S7 fibrinolytic systems, 2S7-2S9 kinin system, 2S6 lysosomal enzymes, 260--261 matrix metalloproteinases, 260--261 protease inhibitors, 261
platelet-activating factor, 2S6 protectins, 2SS regulatory mechanisms, 168--169 resolvins, 2SS root resorption, 399 serotonin, 242-243
Inflammatory pain characteristics of, 16&--177 nonsteroidal anti-inflammatory drugs for,
193-- 194, 199-200 Injury-induced regeneration, 91 Innate immunity
adaptive immunity and, transition between, 329
deficiencies in, 283-28S description of, 277
www.shayanNemodar.com
toll-like receptors, 266--267 Innervation
agents involved in, 138t axonal transport, 134, 135f developing teeth, 142 erupting teeth, 142 neuropeptide-rich fibers, 134 overview of, 133-137 parasympathetic, 138 peptidergic, 143-145 primary teeth, 142 pulpal, 141, 1411 sensory neurons, 134f, 134-135, 434 sympathetic, 138
lntegrins, 77, 250, 397 lntercellular cell adhesion molecules, 248, 250 lnterleukin-1, 264, 289 Interleukin- la, 288 lnterleukin-1 f3, 287-289 lnterleukin-2, 268 lnterleukin-6, 268-269, 287-288, 399 lnterleukin-8, 287 lnterleukin-11, 288, 399-400 Internal root resorption. See Root resorption, internal. lnterneurons, 162-163 Interstitial pressure
microvascular exchange effects on, 114-116 pulpal, 115--116
Interstitial space, 114 lntertubular dentin, 32, 49, 440 lntracanal irrigants, 100, 235 lntracoronal bleaching, 410 lntraligamentary injections, of local anesthetics,
198 lntraluminal collagen, 511 lntraradicular infections
persistent, 225b, 232-234 primary
characteristics of, 225b, 226 description of, 225--226 geographic influences, 228-229 microbiota associated with, 226-228, 227b,
228f, 230 secondary,225b,232-234
lntratubular dentin, 49, 440 Ion channels, 145--147 Irreversible pulpitis, 450-451 lrrigants, 100, 235
J Junctional epithelium, 134-135
K Kallikrein, 123 Kinin system, 256 Kininogens, 256 Knockout mice, for tooth development studies,
7-8, 12 Korff fibers, 68, 71, 73
L Lactobacilli, 214 Lamina phase, of tooth development, 2, 3f Laser(s)
argon, 359 co,, 361-362 dentinal injury caused by, 361-362 dentinal sensitivity treated with, 365--367 description of, 358-359 Er:YAG, 362-365 excimer, 365 Nd:YAG, 359, 365--366 pulpal responses, 359-361 root canal use, 361 ruby, 361 schematic diagram of, 359f soft tissue uses of, 367 tooth bleaching use of, 367
types of, 358-359 wavelengths of, 359f
Laser capture microdissection, 9 Laser Doppler flowmetry, 127-128 Lateral luxation, 386 Lateral periodontitis, 406 Leukemia, 487f Leukocyte adhesion
chemotactic factors involved in, 250 margination, 247 molecules involved in, 247-248, 250
Leukocyte adhesion deficiency-1, 250, 283 Leukocyte adhesion deficiency-2, 248, 283 Leukotrienes
B., 311 description of, 252
L-form bacteria, 378 Lidocaine, 196-197 Linear coefficient of thermal expansion, 350--351 Lipopolysaccharides, 217, 267, 281 Lipoteichoic acid, 264, 269, 282, 329 Lipoxins, 252, 254-255, 255 Lipoxygenase, 252, 254-255 Local anesthetics
circulatory effects, 124-125 intraligamentary injections of, 198 intraosseous administration of, 197-198 pain block using, 450 pain localization using, 177 pain management using, 195--198 speed of injection, 197
Lowe syndrome, 484t Luxation, 386 Lymphatic vessels, 112-114 Lymphocytes. See B cells; T cells. Lysosomal enzymes, 260--261
M Macrophages, 811, 81-82, 287-288 Magnetic resonance imaging, 104 Major histocompatibility complex molecules, 80--
84, 83f, 269-270, 354 Mantle dentin, 31, 48, 53t Maresins, 255 Margination, 247 Masseter muscle, 454f Maternal rubella, 473-474 Matrix metalloproteinases
aging effects on, 425 collagen degradation by, 339 definition of, 30, 326 dentin remodeling, 261 extracellular matrix degradation caused by, 261 inhibitors of, 339-340 odontoblast expression by, 30 odontoblast synthesis of, 76-77 source of, 326 tooth morphogenesis role of, 15
Mechanoreceptors, 135 Medial pterygoid muscle, 454f Medullary dorsal horn, 160f, 162 Membrane attack complex, 256 Membrane receptors, 145--147 Mesenchymal cells, undifferentiated, 68, 79 Mesenchyme, dental
enamel knot formation regulated by, 14 molecules that affect, 10
Metarterioles, 110 Microarrays, 22, 22f Microbiota
definition of, 226 diversity of, 226 ecology of, 230--231 in endodontically treated teeth, 233-234 primary intraradicular infections caused by,
226-228, 227b, 228f, 230 Microcirculatory system, of pulp. See also Pulpal
blood flow. arterioles, 109-110, 1101, 1211, 127f
capillaries, 110--111 description of, 109 diagnostic uses of, 128 endodontic therapy effects, 126 inflammatory mediators effect, 127-128 local anesthetics effect, 124-125 lymphatic vessels, 112-114 microcirculation, 114-115 orthodontic therapy effects, 126-127 orthognathic surgery effects, 127 restorative procedures effect, 125--126 schematic diagram of, 11 Of transcapillary exchange, 114-115 venules, 111
Microcomputed tomography, 431 Microsurgery, 437f Migraine, 455-457
Index
Mineral trioxide aggregate, 307, 313-315, 315f Mitochondrial DNA, 423 Mitochondrial respiratory system, 423 Moire interferometry, 350 Monocytes, 283b Multiple sclerosis, 465 Mutans streptococci, 213-214 Myelin, 146, 146f Myofascial pain, 452-454
N Naloxone, 164-165 Natural killer T cells, 280 Nd:YAG laser, 359, 365--366 Nerve degeneration, 147 Nerve fibers
Af3, 136-137 activation of, 1511 A8, 137 antigen-presenting cells and, 270 chemical signaling, 138 cytochemical features of, 137 immunochemistry of, 140f inflammation effects, 171-172 odontoblasts and, 177 patterns of, 140f pulpal interactions with, 139 sprouting of, 141, 171, 243 types of, 136-137
Nerve growth factor, 97t, 136-137, 434 Neuritic pain, 460-461 Neurokinin A, 143, 243 Neurons, 164 Neuropathic pain
continuous, 460-462 definition of, 458 description of, 174-175, 175f episodic, 458
Neuropeptide Y, 119, 1201, 143, 243, 245--246, 354 Neuropeptides, 122f, 143, 243-247, 354, 434 Neuropulpal interactions
agents involved in, 138b schematic diagram of, 134f
Neutrophils, 262, 283b Niches, 93 Nitric oxide, 261t, 261-262, 355 Nociceptors
central sensitization activated by, 172 drugs that block release or actions of inflammatory
mediators, 192-195 interneurons effect, 163, 163f neurophysiology of, 147-153 sensitization of, 170 signal transmission pathways, 160--166
Nodes of Ranvier, 146 Noncollagenous proteins, 18, 18t Nonodontogenic pain
atypical odontalgia, 461-462 cardiac origin of, 462-463 causes of, 451-453 clinical features of, 452b cluster headache, 457-458
497 www.shayanNemodar.com
Index
deafferentation origin of, 461-462 glossopharyngeal neuralgia, 459-460 migraine, 455-457 myofascial pain, 452-454 psychogenic origin, 463--464 systemic disorders that cause, 464-465 trigeminal autonomic cephalgia, 457-458 trigeminal neuralgia, 458-459 zoster, 473
Nonspecific plaque hypothesis, 212 Nonsteroidal anti-inflammatory drugs, 193-194,
199-200 Notch signaling, 41, 310, 432 Nucleotide-binding oligomerization domains,
267-268 Nucleus caudalis, 162-164 Nursing caries, 215
0 Occlusal adjustment, for pain management, 191 Occlusal caries, 216t, 307f, 330f, 332f Oculocerebrorenal syndrome, 484t Odontalgia
atypical, 461-462 diagnosis of, 190-191 incidence of, 185, 447
Odontoblast age-related changes in, 426, 429-430 calcium transport system, 30 cavity preparation effects on, 341 cell body of, 74-75 characteristics of, 68 collagen synthesis, 29 cultures for studying, 6, 9 death of, 43 definition of, 4, 47, 76 differentiation of
bone morphogenetic proteins, 355 collagen fibers in, 71 core-binding factor a 1 's role in, 12, 14 fibronectin effects, 73 morphologic changes, 15-16 signaling interactions that influence, 10-15 steps involved in, 15 studies of, 9 terminal events in, 16f, 73
fibronectin effects on, 73 functions of, 76-78, 138, 355 glycosaminoglycans effect, 72 Golgi complex, 74-75 illustration of, 6f, 48f inflammatory mediators produced by, 242 injury response of, 77-78 innate immunity functions of, 77 integrins secreted by, 77 junctions of, 75-76, 136f life cycle of, 399f matrix metalloproteinase synthesis by, 76-77 mitochondria of, 75 morphology of, 15-16, 28, 68, 430 nerve fibers and, 177 osteoclast vs, 400 phenotype of, 28--29 predentin secretion by, 16f progenitor cells for, 40-41 pulp and, relationship between, 28--29 restorative materials effect on, 341-342 secondary, 78 secretory behavior of, 29f, 29-31, 33, 76-77 sensory fibers and, interactions between, 138 structure of, 74-76 synthesis functions of, 76-77 toll-like receptor 4, 102 tooth sensation role of, 138 type I collagen in, 17f ultrastructural appearance of, 28f
Odontoblast layer characteristics of, 68--69
498
definition of, 111 illustration of, 68f
Odontoblast process, 47, 75, 75f, 440 Odontoblastoid cells, 96 Odontocytes, 431 Odontogenesis. See Tooth development. Odontogenic pain, 191-199, 447, 451b. See also
Pain. Odontogenic toothache, 449b, 450f, 451 Oligonucleotide arrays, 22 Opioids, 196 Opsonization, 270 Orthodontics, 126-127 Orthognathic surgery, 126-127 Osseous replacement, 402-403, 403f Osteitis deform ans. See Paget disease of bone. Osteocalcin, 18t Osteoclast(s), 477
calcified tissue resorption by, 400 extracellular protein binding, 397 mediators that affect functioning of, 399 odontoblast vs, 400
Osteoclast-activating factor, 288 Osteoclastic diseases, 477-478 Osteoimmunology, 400 Osteonectin, 18t, 74 Osteopontin, 18, 18t, 21, 211, 401 Osteoprotegerin, 398, 477-478 Oxidative stress, 423--424 Oxygen-derived free radicals, 262-263
p Paget disease of bone, 415, 478-479, 4791 Pain
classification systems for, 452 diagnostic approach, 190-191, 465 dysfunctional, 175 endogenous analgesic system activated by,
165 incidence of, 159, 185 inflammatory. See Inflammatory pain. local anesthetic blocking of, 450 myofascial, 452-454 neuritic, 460-461 neuropathic
continuous, 460-462 definition of, 458 description of, 174-175, 175f episodic, 458
nonodontogenic. See Nonodontogenic pain. nonpharmacologic treatment of, 191-192 odontogenic, 191-199, 447, 451b perception of
drugs that block, 198--199 mechanisms, 159-160, 164-166
postendodontic therapy, 173-174 prostaglandins' role in, 251-252 pulpal vitality testing to diagnosis, 178--180 referred, 176-177, 447-448, 448f-4491 site of, 449-451 source of, 449-451 transmission of
drugs that block, 195-198 physiologic mechanisms, 160-166
treatment of corticosteroids, 195 cyclo-oxygenase inhibitors, 194 glucocorticoids, 195 nonpharmacologic, 191-192 nonsteroidal anti-inflammatory drugs, 193-
194, 199-200 pharmacologic, 192-199 strategies for, 199-200
Papillon-Lefevre syndrome, 484t Parasympathetic nerves
pulpal blood flow regulated by, 120-121 tooth innervation by, 138
Peptidergic innervation, 143-145 Peptidoglycans, 264
Periapical bone loss, 288--289 Periapical immune responses, 277-282 Periapical inflammation
humeral immunity in, 281-282 mediators of, 287-293 resident cells in, 282
Periapical lesions chronic, 281 definition of, 277 description of, 281 illustration of, 376f, 380f, 384f immune cells in, 278--281
Periapical replacement resorption, 404 Periluminal dentin, 49 Periodontal disease
endodontic disease and, 389-392, 3891-392f. See also Endodontic-periodontal diseases.
primary, 388, 3891-390f, 393 Periodontal ligament-derived stem cells, 7, 7f Periodontitis
apical. See Apical periodontitis. lateral, 406 progressive, 390
Peritubular dentin, 32, 32f, 48, 52, 440 Permeability
capillary, 127 dentin. See Dentin, permeability.
Phospholipids, 2511 Pink tooth, 412 Plaque
accumulation of, 206f acid production by, 214 beneficial bacteria in, 214 biofilm. See Biofilm, plaque. definition of, 206 developmental stages of, 209-210 mechanical removal of, 220
Plasma cells, 283b Plasma exudate, 305-306 Plasma proteases
clotting system, 257-259 complement system, 256-257 fibrinolytic systems, 257-259 kinin system, 256 lysosomal enzymes, 260-261 matrix metalloproteinases, 260-261 protease inhibitors, 261
Plasticity embryonic stem cells, 93 trigeminal ganglion, 140-141
Platelet-activating factor, 256 Platelet-derived growth factor, 97t Platelet-endothelial cell adhesion molecule, 248 Polymerization shrinkage, 338--339, 341 Polymorphonuclear neutrophils, 278--279, 285 Porcine enamel matrix, 316 Porphyromonas species, 217 Postherpetic neuralgia, 473 Postnatal stem cells, 93-94, 98 Potassium-containing dentrifices, 188t, 188--189 Predentin, 16f, 47-48, 48f, 71-72, 411-412, 433,
486f Prekallikrein, 256 Pressure resorption, 403--404 Pre-trigeminal neuralgia, 458 Prevotella species, 217 Primary caries, 212 Primary dentinogenesis, 31-33, 430 Primary endodontic disease, 388, 392 Primary hyperparathyroidism, 478-479 Primary oxalosis type I, 484t Primary periodontal disease, 388, 3891-390!, 393 Primary teeth, 142 Progenitor cells
chemoattractants, 41 definition of, 92 dental follicle, 95 description of, 310 mesenchymal cells, 40
www.shayanNemodar.com
regenerative medicine use of, 92-95 in reparative dentinogenesis, 40--41
Progressive periodontitis, 390 Proinflammatory cytokines, 264-268, 265f, 287-289,
291-293 Projection neurons, 163-164 Prostaglandins
description of, 123, 168, 251-252, 290 E2, 282
Prosthetic procedures, 125--126 Protease inhibitors, 15, 261 Protectins, 255 Protein kinases, 164 Proteoglycans
bacterial penetration prevented by, 73 definition of, 67 in extracellular matrix, 18t hydrophilicity of, 72 structure of, 72
Proteolytic bacteria, 377 Pulp
adhesion molecules in, 247-248, 250 age-related changes in, 425--442 biology of, 21-22 blood vessels of, 432-434 caries-induced exposure of, 224, 224f cellular arrangement of, 68f, 68--69 circulatory system of. See Microcirculatory system. clonal lines for studying, 6 collagen types in, 70-71 coronal, 711, 429f crown fracture involving, 385 dendritic cells of, 82-84 dentin bonding effects on, 340-341 edema of. 305 elasticity of, 71 exposure of, 302f, 303-305 features of, 68--69 innervation of, 141, 1411 low-compliance environment of, 69 mineralization of, 437 necrosis of, 404-405 nerve fibers of. See Nerve fibers. odontoblasts of. See Odontoblast. radicular, 429f recession of, 33 responses of, 277-278 revascularization of. 407 root resorption role of. 401-402 sensory innervation of. 70 size reductions in, 438 structural organization of, 68--69 sympathetic nervous system innervation of, 118 testing responses of, for aging evaluations,
436-437 tissue engineering of, 103 vascular responses of, 242 vasculature of. See Microcirculatory system. vitality of. See Vital pulp.
Pulp capping adhesive systems for, 312-313 in aging tissue, 441-442 dentin bridge formation as indication of, 43 dentinal bridge effects on, 306-307 direct, 340 exposure duration effects on, 303 hemorrhage control before, 305--306 indirect, 317-319 materials for
calcium hydroxide. See Calcium hydroxide. dentin adhesives, 312-313 description of, 305--306, 311 experimental bioactive molecule-containing
materials, 315--317 glass ionomers, 312 mineral trioxide aggregate, 313-315, 315f zinc oxide-eugenol, 318
microbial leakage effects on, 310
Pulp core, 69 Pulp proper, 69 Pulp space infection
description of, 404 external root resorption caused by, 404-408 prevention of. 407 treatment of, 407-408
Pulp stem cells description of, 95--96 pulp constructs created from, 98-100, 99f, 102t smear layer attachment of, 102, 103f
Pulp stones, 437-438 Pulpal blood flow
bacterial effects, 127-128 calculation of, 114 dentin grinding effects on, 125f histamine effects, 242 inflammatory mediators effect, 69 measurement of, 116-117 neuropeptides' effect on, 122f prosthetic procedures' effect on, 125--126 regulatory mechanisms of
a-adrenergic receptors, 118f endocrine factors, 123 metabolism, 117-118 neuronal, 118-123 neurotransmitters, 122 paracrine factors, 123 parasympathetic nerves, 120-121 peptidergic afferent fibers, 121-123 schematic diagram of, 115f, 117f sympathetic nerves, 118-120 trigeminal sensory nerves, 126
restorative procedures' effect on, 125-126 sensory nerve denervation effects on, 1211 stimulation of, 61
Pulpal infection. See also Endodontic infections. caries. See Caries. protective immunity against, 282-287
Pulpal injury. See also Tooth injury. cavity preparation as cause of, 334-335 description of, 77-78 healing after, 302-303 microleakage, 343 pulp capping for. See Pulp capping. reasons for, 301 root resorption caused by, 402-403 signaling molecules contributing to, 43f
Pulpal interstitial pressure, 115--116 Pulpal nerves
degeneration of, 147 sensory functions of, 148-150, 152-153
Pulpitis immune cells in, 277-278 management of, 190-199 opioids for, 198 pain caused by, 147, 190-199 silent, 147
Pulpodentin complex. See also Dentin; Pulp. age-related changes in, 427, 440--442 caries
defense responses to, 329-331, 330f-3311 description of. 325 injury responses to, 328-329 responses to, 328-333
characteristics of, 69-70, 223 defense responses by, 329-331, 330f-3311 definition of, 1 functions of, 91 injury response
to caries, 328-329 cavity preparation, 334 description of, 77-78 neuroanatomical responses, 141 signaling molecules contributing to, 43f stimuli that cause, 139 summary of, 344-345
permeability of, 324-325
repair capacity of, 334 structure of, 47-48, 48f, 324-325
Pulse oximetry, 128
Q Ouorum sensing, 208-209
R Radiographs
aging, 441 apical periodontitis, 206f caries, 218, 218f
Index
external root resorption, 413, 414f, 415 internal root resorption, 412-413, 412f, 415
Raman spectroscopy, 431 RANKL, 282, 398, 401, 477-478 Reactionary dentin
cavity etching stimulation of, 38 cellular signaling of, 38 definition of, 34, 78 deposition areas for, 334 ethylenediaminetetraacetic acid effects, 38 production of, 333 remaining dentinal thickness effects, 37-38 restorative materials' effect on formation of, 342-
343 Reactionary dentinogenesis
biologic processes, 35f-36f, 35--37 definition of, 35, 331, 333 factors that affect, 37-38 histomorphometric findings, 37-38 odontoblast upregulation during, 35--37 restorative materials that cause, 35--36
Reactive oxygen species, 423 Receptor activator of nuclear factor Kf3 ligand. See
RAN KL. Recombinant human bone morphogenetic proteins,
91, 310 Recombinant human insulin-like growth factor 1,
97-98 Recurrent caries, 211-212, 218-219 Referred pain, 176-177, 447-448, 448f-449f Regeneration
definition of, 92 history of, 91 homeostatic, 91 injury-induced, 91
Regenerative endodontics challenges associated with, 104b delivery improvements for, 103-104 dental pulp constructs for, 98-100, 99f, 102t objectives of, 92 outcome measurements, 104 postnatal stem cells for, 98-99, 99f, 102t research priorities for, 102-104 root canal revascularization using blood clotting,
100-101, 102t Regenerative medicine
foundations of, 92-98 growth factors, 96-98 history of, 91 progenitor cells, 92-95 stem cells. See Stem cells.
Regulatory T cells, 278, 280, 291 Remaining caries, 212 Remaining dentinal thickness, 37-38, 325, 334-335,
355 Remineralization
description of, 212 fluoride effects on, 222
Renal dystrophy, 415 Reparative dentin, 34, 78, 308 Reparative dentinogenesis
biologic processes during, 35f collagen fibrils in, 72 definition of, 333 dentin bridge formation vs, 43 description of, 38 fibrodentin matrix secreted before, 39
499 www.shayanNemodar.com
Index
histologic findings, 39f matrices secreted during, 38, 39f-40f odontoblast-like cell differentiation, 41-43 progenitor cell recruitment in, 40--41 tertiary dentinogenesis and, 39
Reparative tertiary dentinogenesis, 316 Replicative senescence, 423 Resident cells, 282 Resin-based materials, 335-337, 336f-337f Resin-modified glass ionomers, 312, 338 Resolvins, 255 Restorative dentistry, 323 Restorative materials and procedures
bacterial microleakage, 303, 343 calcium hydroxide . See Calcium hydroxide. dentin permeability effects, 61-62 inflammation caused by, 343f microcirculatory effect, 125-126 mineral trioxide aggregate, 313--315, 31 Sf odontoblast survival affected by, 341-342 physical properties of, 349-351 reactionary dentin formation affected by, 342-
343 specific heat of, 349-350 tertiary dentinogenesis effects, 35-36 thermal conductivity of, 349 thermal diffusivity of, 350 tooth-colored, 344 toxicity of, 303 zinc oxide-eugenol, 318
Revascularization of root canals using blood clotting, 100-101, 102t
Reverse transcriptase-polymerase chain reaction, 9f
Rickets hypophosphatemic, 479-481, 4811 vitamin D-dependent, 479-480
Root canals accessory, 37 4 disinfection of, 102 filling stage of, bacteria present at, 232-233 infections of. See Endodontic infections. laser therapy of, 361 lateral, 374 pulp stem cell attachment to, 103f revascularization of, using blood clotting,
100-101, 102t sodium hypochlorite-irrigated, 57f
Root caries, 211, 216t Root dentin
impermeability of, 58 mechanics of, 53--54 permeability of, 56f, 56-60
Root fracture, 386, 390 Root perforation, 386--387 Root resorption
cervical, 408 external
apical periodontitis and, 404-405 description of, 402 diagnostic features of, 413, 414b, 415 diffuse injury, 402-403 lateral periodontitis with, 406 localized injury, 402 pressure-induced, 403-404 pulp space infection, 404-408 radiographic findings, 413, 414f, 415 sulcular infection, 408-410 vitality testing, 415
histologic appearance of, 399f inflammation-induced, 401-402 inflammatory mediators involved in, 399 internal
characteristics of, 411 clinical manifestations of, 412 description of, 411 diagnostic features of, 413, 414b, 415 etiology of, 4111, 411-412 histologic appearance of, 411 f, 412
500
pink tooth, 412, 415 radiographic findings, 412-413, 412f, 415 treatment of, 412-413 vitality testing, 415
mechanisms of, 397-401 misdiagnoses, 415 Paget disease of bone and, 415. See a/so
Paget disease of bone. pulpal role in, 401-402 renal dystrophy and, 415 requirements for, 401 resistance to, 397-398 subepithelial inflammatory, 408-410, 415 systemic causes of, 415-416
Rubella, 473-474, 474f Ruby lasers, 361 Ruffini mechanoreceptors, 135 Rushton hyaline bodies, 383, 383f Russell bodies, 382f, 382-383
s Saliva, 218, 220, 222 Scaffolds,99-100, 102 Sclerotic dentin
description of, 327 illustration of, 32f permeability of, 56
Secondary caries, 211 Secondary dentin, 27, 33--34, 48-49, 78, 430, 433,
439,440 Selectins, 248 Self-etching adhesives, 336 Senescence,421-423 Sensitivity. See Dentinal sensitivity. Sensory fibers
injury responses of, 139 odontoblast and, interactions between, 138
Sensory neurons, 134f, 134-135, 434 Serotonin, 242-243 Severe combined immunodeficiency, 285-286 Shingles, 473 Sickle cell anemia, 464, 481-482, 482f Silent pulpitis, 147 Single-bottle adhesive systems, 336 Sinus headache, 454 Sinusitis, 455, 460 Small integrin-binding ligand, N-linked glyco
protein family, 18 Smear layers
creation of, 57, 335 description of, 57 illustration of, 58f permeability effects, 58 pulp stem cell attachment to, 102, 103f removal of, 103, 341 treatment of, 58
Smear plugs, 57 Smooth surface caries, 216t Sodium channels, 146 Sodium hypochlorite, 235 Somatoform pain disorder, 464 Specific plaque hypothesis, 212 Spirochetes, 378 Starling forces, 114-115, 116 Stellate reticulum, 4 Stem cells, 41
advantages of, 94-95 allogeneic, 95 from apical papilla, 95 autologous, 94-95, 104 definition of, 92 developmental stages of, 94f differentiation of, 7 embryonic, 93--94 from human exfoliated deciduous teeth, 7,
7f, 95 isolation and identification of, 96 niches of, 93 osteogenic induction of, 7f
overview of, 91-92 periodontal ligament-derived, 7, 7f postnatal, 93--94, 98 "-
protein expression by, 96 pulp. See Pulp stem cells. source-based classification of, 94 tooth-derived, 6-7, 7f umbilical cord, 94 xenogeneic, 95
Sternocleidomastoid muscle, 454f Stratum intermedium, 4 Streptococcus mutans, 214 Subepithelial inflammatory root resorption,
408-410,415 Subluxation, 386 Substance P, 70, 121-123, 243--247, 334 Sulcular infection, 408-410 Suppressor T cells, 291 Sympathetic nerves
pulpal blood flow regulated by, 118-120 tooth innervation by, 119f, 138
Systemic disorders
T
herpesvirus infections, 472-473, 473f human immunodeficiency virus, 471-472 nonodontogenic pain caused by, 464-465 Paget disease, 478-479, 479f rubella, 473-474, 474f
T cells, 283b caries-induced response, 85-86 CD4+, 279 CDS+, 279 cytotoxic, 278 description of, 79-80 helper, 278, 280, 291 illustration of, 80f mechanism of activation, 80 natural killer, 280 regulatory, 278, 280, 291 suppressor, 291
Taurodontism, 474, 475b, 475f Telomeres, 423-425, 431 Temporalis muscle, 454f Temporomandibular dysfunction, 453-454 Terminal arteriole, 110 Terminal capillary network, 68 Tertiary dentin, 27, 34-35, 49, 49f, 78, 317, 324 Tertiary dentinogenesis
cavity preparation materials that affect, 35-36
description of, 34-35 reparative, 316 transforming growth factor-fl1 's role in, 36
T halassemia, 481, 482f T hermal allodynia, 449 T hermal stimuli
cavity preparation, 349-353 laser treatment, 358-366
Thromboxanes, 251-252 Tight-junction capillary, 111 Tissue development stages, 94f T issue engineering
definition of, 92 pulp, 103 scaffolds for, 99-100
Toll-like receptors, 77, 102, 266f-267f, 266-267, 282, 287-288, 329
Tooth bleaching, 367 Tooth development
description of, 1-2 enamel knots, 14 epithelial-mesenchymalsignalinginteractions
during, 10f experimental systems for
description of, 4 knockout mice, 7-8 laser capture microdissection, 9 tooth organ culture systems, 4-6, Sf
www.shayanNemodar.com
transgenic mice, 7--8 general features of, 2 stages of, 2-4, 3f
Tooth injury. See also Pulpal injury. axonal degeneration secondary to, 147 classification of, 139 cytochemical responses to, 139-145 delayed neural reactions to, 141 human teeth studies of, 141-142 ion channels, 145--147 membrane receptors, 145--147 stimuli that cause, 139 structural responses to, 139-145 trigeminal nerve and ganglion plasticity, 140-141
Tooth organ culture systems, 4--6, Sf Toothache, odontogenic, 449b, 450f, 451 Tooth-colored restorative materials, 344 Tooth-derived stem cell lines, 6--7, 7f Tooth-signaling molecules, 1 Transcapillary exchange, 114-115 Transcription factors
core-binding factor a 1, 12, 13f definition of, 10 function of, 10
Transdentinal permeability, SSf Transforming growth factor-a, 97t Transforming growth factor-fl, 97t Transforming growth factor-[l 1, 430
chemotactic role of, 41 etchants that solubilize, 36 inflammatory role of, 269 odontoblast secretion, 33 odontoblast-like cell differentiation induced by,
41-42, 42f production of, 293 reactionary dentinogenesis role of, 36 receptors, 38
transgenic mice studies of, 8 Transgenic mice
development of, 7-8 tooth development studies using, 7f, 7--8
Transient receptor potential ion channels, 145 Transient receptor potential vanilloid 1, 462 Transmigration, 248 Transmitted-light photoplethysmography, 128 Trauma
dentin exposure caused by, 224 endodontic-periodontal diseases secondary to,
385--386 Trephination, 191-192 Treponema species, 378 Trigeminal autonomic cephalgia, 457-458 Trigeminal ganglion
dental nerve cell bodies, 137f plasticity of, 140-141
Trigeminal neuralgia, 458-459 Trigeminal sensory neurons, 162 Trigeminovascular system, 455 Trigger points, 452 True combined endodontic-periodontal disease,
391f-392f, 391-392 Tubular sclerosis, 219 Tumor necrosis factor, 264, 284 Tunnel defects, 43
u Ultrasound, 333 Umbilical cord stem cells, 94 Undifferentiated mesenchymal cells, 68, 79
v Vascular cell adhesion molecule, 248 Vascular endothelial growth factor, 329 Vasoactive intestinal peptide, 120-121, 143, 243
Vasoactive neuropeptides, 329 Vasoconstrictors, 124 Veil/one/la species, 214 Venular network, 111 Venules, 111 Viruses, 231-232, 379 Vital pulp
Index
external root resorption prevented by maintenance of, 407
testing of description of, 178-180 root resorption diagnosis, 415
Vital pulp therapy. See also Pulp capping. dentin adhesives for, 312-313 dentinal bridge effects, 306-307 description of, 301 mineral trioxide aggregate for, 313-315, 31 Sf resin-modified glass ionomers for, 312
Vitamin D metabolism disorders, 479-481 Vitamin D-dependent rickets, 479-480 Voltage-gated ion channels, 145
w Wide dynamic range projection neurons, 164
x Xenogeneic stem cells, 95 X-linked hypophosphatemic rickets, 479-481, 4811
z Zinc oxide-eugenol, 318 Zone of destruction, 216, 217f Zone of Hohl, 96 Zone of Weil, 68, 113 Zoster, 473, 473f
501
www.shayanNemodar.com





























