Rh-INCOMPATIBILITY
Hemolytic Disease of Newborn (ERYTHROBLASTOSIS FETALIS)
Dr. Muhammad Sajjad Sabir MBBS, DCH, MCPS, FCPSAssistant Prof.
Paediatrics
Hemolytic disease of newbornThe term Hemolytic disease of the
new born and fetus (HDN) is a destruction of the red blood cells
(RBCs) of the fetus and neonate by antibodies produced by the
mother
Hemolytic disease of newbornIt is a condition in which the life
span of the fetal/neonatal RBC is shortened due to maternal
allo-antibodies against red cell antigens acquired from the
fatherSORate of RBCs destruction is accelerated BUT ability of bone
marrow to respond is NORMAL
It was a major cause of fetal loss and death among newborn
babies
EtiologyRh incompatibility: Hemolytic disease occurs most
frequently develops when an Rh ve mother conceives a fetus which is
Rh +ve
ABO incompatibility: mother has blood type O and the fetus has
blood type A or B or AB
Other causes: Other Minor blood group antigens(kell, kid
)Thalassemia Autoimmune Hemolytic Anemia
The Rh factor , Rh+ and Rh- usually refers to presence or
absence of antigen-D
There are two alleles of antigen: D and d
A person who is Rh -ve has two recessive traits, dd
Anyone who has at least one D (DD or Dd) is Rh+veRh-BLOOD
GROUPING SYSTEM
Rh incompatibility:Rh incompatibility is a condition which
develops when an Rh negative mother conceives a fetus which is Rh
positive.
Isoimmunization:When the mother produces Abs directed against
fetus RBC surface AgCause Feto- maternal BleedRisk Factors of
Feto-maternal Bleed: AmniocentesisEctopic pregnancy
Fetal RBC Rh Antigen : Rh D Ag Mother produces: Anti Rh (D)
Abs
PATHOGENISIS
DEFINITION:Rh incompatibility is a condition which develops when
there is a difference in Rh blood type between that of the pregnant
mother (Rh negative) and that of the fetus (Rh positive)
Rh Type and Pregnancy A person's Rh type is generally most
relevant with respect to pregnancies
If the pregnant woman is Rh -ve and her husband Rh+ve, there is
possibility of Rh incompatibility
If the pregnant woman and her husband are Rh negative, there is
no reason to worry about Rh incompatibility
Usually placenta is barrier to fetal blood entering maternal
circulation. Sometimes during pregnancy or birth, fetomaternal
haemorrhage (FMH) can occur The womans immune system reacts by
producing anti-D antibodies that cause sensitisation
Subsequent pregnancies antibodies can cross placenta and destroy
fetal erythrocytes.
Conditions affecting 1st pregnancy
:MiscarriageAbortionFeto-maternal haemorrage
The haemolytic disease of fetus and new born caused by Rh
isoimmunisation can occur during the first pregnancy, but Usually
sensitisation during the first pregnancy or birth leads to
extensive destruction of fetal RBC during subsequent
pregnancies
Pathogenesis
Fetomaternal Hemorrhage
Maternal Antibodies formed against fetus derived antigens
During subsequent pregnancy, placental passage of maternal IgG
antibodies
Maternal antibody attaches to fetal red blood cells
Fetal red blood cell hemolysis
Pathogenesis; beforebirth
Pathogenesis; afterdelivery
Clinical Presentation
Hemolysis ed bilirubin levels
Rh incompatibility can cause symptoms ranging from very mild to
fatal.
After delivery bilirubin is no longer cleared (via placenta)
from the neonate's blood Jaundice (within 24 hours of life)
Possibility of acute or chronic Kernicterus
Sign &symptom
Mildest form- Rh incompatibility: 1-Hemolysis with the release
of free hemoglobin into the infant's circulation
2- Jaundice
Prenatal manifestations : Hydrops fetalis / Erythroblastosis
FetalisMassive fetal RBC destruction Profound anemiapallor
high-output heart failure (CCF) Enlarged liver / spleenGeneralized
Edema Ascites andRespiratory distress
Severe form- Rh incompatibility
Severe form- Rh incompatibility
1- severe forms petechiae and purpura
2- Severe anemiaFetal heart failure stillborn orDeath of infant
shortly after delivery
2- Total body swelling
3- Respiratory distress (if infant has been delivered)
4- Circulatory collapse
5- Kernicterus. (bilirubin encephalopathy) (Neurological
syndrome in extremely high levels of indirect bilirubin (>20
mg/dL).
6- It occurs several days after delivery and is characterized
initially by... A) Loss of the Moro reflex. B)Poor Feeding. C)
Decreased activity
LATER At last it may lead to death of the child immediately
after its birth
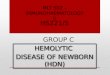
Investigations
Blood groupingMother: Rh NegativeFather: Rh PositiveBaby: Rh
PositiveDirect Coombs test: Positive in INFANTIndirect Coombs test:
Positive in MOTHERBiochemical
testHyperbilirubinemiaHypoalbuminemiaLDH: IncreaseHaptoglobin
Decrease
Blood SmearPolychromasiaAnisocytosis Erythroblasts (nucleated
RBCs) No Spherocytes
CBCTLC: normalHb: Hb MCV, MCH, HCHC : Normal or
IncreasePlatelets: Normal to Decrease Reticulocytosis (6 to
40%)
Coombs testDirect Coombs test: diagnoses HDNThe direct Coombs
test detects maternal anti-D antibodies that have already bound to
fetal RBCs This is called the direct Coombs test because the
anti-Ig binds "directly" to the maternal anti-D Ig that coats fetal
RBCs in HDN
Finds anti-D antibodies in mother's serum. If these were to come
into contact with fetal RBCs they would hemolyse them and hence
cause HDN.
This is called the indirect Coombs test because the anti-Ig
finds "indirect" evidence of harmful maternal antibodies, requiring
the addition of fetal RBCs to show the capacity of maternal anti-D
to bind to fetal RBCsIndirect Coombs test: used in the prevention
of HDN
Management
If there is evidence of erythroblastosis
Notify Pediatrics team for possibilitye delivery of a
compromised newborn
Management
ManagementBefore birth(Antenatal) options:Intrauterine RCC
transfusion - blood transfused into fetalumbilical vein or
Early induction of labor when Pulmonary maturity has been
attained, Fetal distress is present, or 35 to 37 weeks of gestation
have passed
The mother may also undergo plasma exchange to reduce
circulating levels of antibody by as much as 75%
After birth(Postnatal)Treatment depends on the severity of
condition:Phototherapy Transfusion with compatible RCC, Exchange
transfusion with a blood type compatible with both the infant and
the motherSupportive care Temperature stabilization
MonitoringSodium bicarbonate ( correction of acidosis)O2/ assisted
ventilation
Management:Phototherapy for neonate with mild jaundice
Exchange transfusion in Severe cases
For Mother (Antenatal)Rh -ve mothers (pregnant with a Rh+ve
infant are given) Rh immune globulin (RhIG) to prevent
sensitization to D antigen RhoGAM protects against the effects of
early transplacental hemorrhage (as recommended by the American
College of Gynecologists). at 28 weeks during pregnancy at 34 weeks
Plasma exchange to reduce circulating levels of antibody by as much
as 75%
Close monitoring of fetal well-being, as reflected by Rh titers,
amniocentesis results, and sonography
For Mother (Postenatal)Rh -ve mothers with Rh+ve infantInj
RhoGAM must given within 72 hours of delivery of the newborn.
Preventing HDNDetermine Rh status of the motherIf the mother is
not sensitized, reduce the risk of future sensitizationIf the
mother is sensitized, determine whether the fetus is at risk and
monitor accordinglyTo prevent Isoimmuization of yet unimmunized
mother give Anti Rh D IgG (Rhogam) IntraMuscular at 28 weeks of
gestation.
Summary:
THANK YOU