Embed Size (px)
DESCRIPTION
These slides will discuss the hemolytic disease of the newborn generally , especially the RH incompatibility between mother and child and their effects ..
Citation preview
Rh isoimmunization &
Hemolytic disease of newborn
Done by : Interns of group DMCH , Makkah , Saudi Arabia
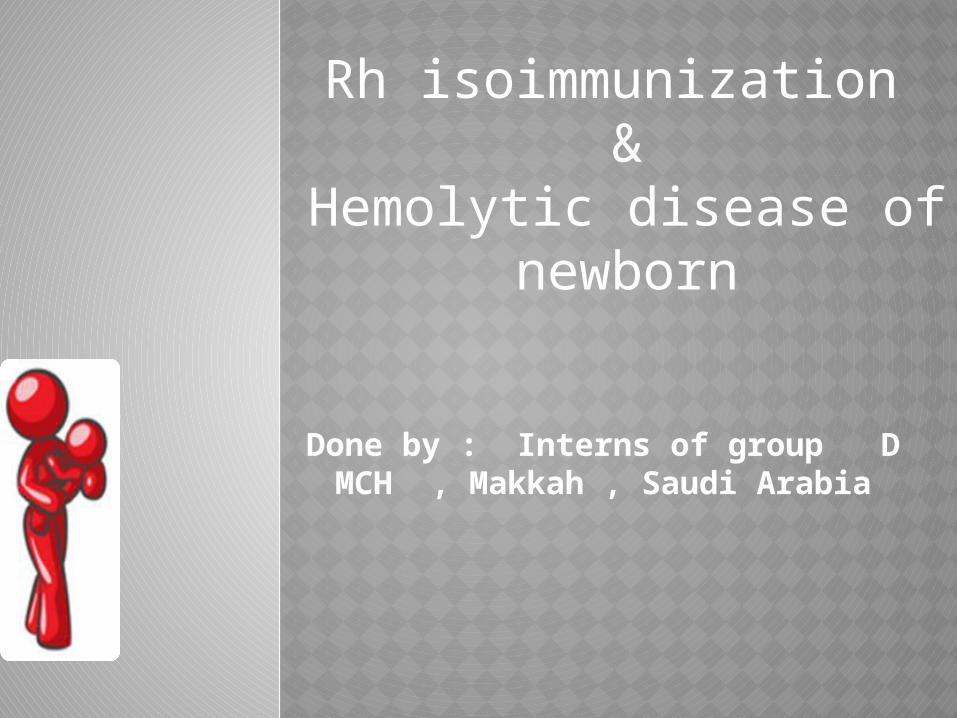
Isoimmunization occurs when a woman produces Antibodies directed against foreign RBC surface Antigens , often those of her fetus.
DEFINITION
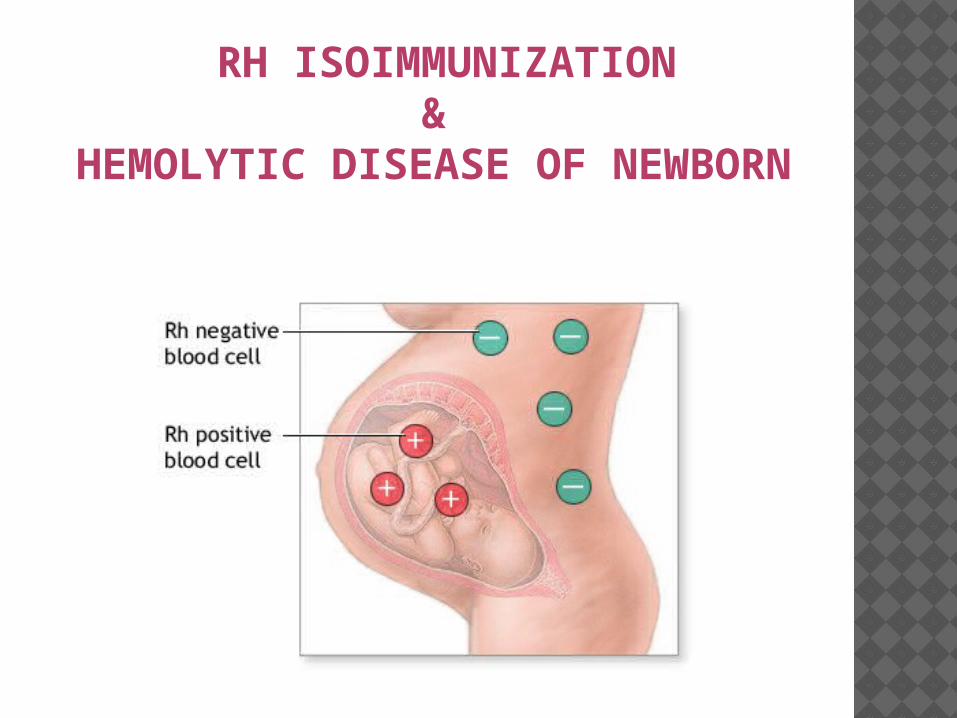
RH ISOIMMUNIZATION &
HEMOLYTIC DISEASE OF NEWBORN
CASE:A 34 years old patient PG , at 9 weeks gestation .
She came to ER complain of abdominal pain and
vaginal bleeding .
A urine pregnancy test was positive 3 weeks ago.
She denies passage of any tissue vaginally .
On examination the cx was dilated .
Investigation reveals that the pt is anemic and
blood type of B-ve and indirect coombs test (AAT) is
negative The patient admitted and prepared for
emergency D/C
What is the most important thing should given to
this patient before discharge?.
WHAT IS THE CAUSES!!?
The most common cause of
Isoimmunization is
FETO-MATERNAL BLEEDING
PATHOPHYSIOLOGYWhen any foreign RBCs comes to the mother , her lymphocytes get activated to produce Antibodies which will destroy those RBCs, and the mother will be (RH Sensitized).
Actually , that is not a problem in the initial pregnancy ,,, But if she get pregnant again with RH +ve fetus , Those Abs will cross the placenta and start destroying fetal blood cells causing hemolysis .
PATHOPHYSIOLOGYThe baby gets Anemic , RES activated , liver & spleen & BM get enlarged ,causing increasing in immature RBCs (erythroblasts).
The hemolysis continue and the RES can not handle it any more so complications presents.
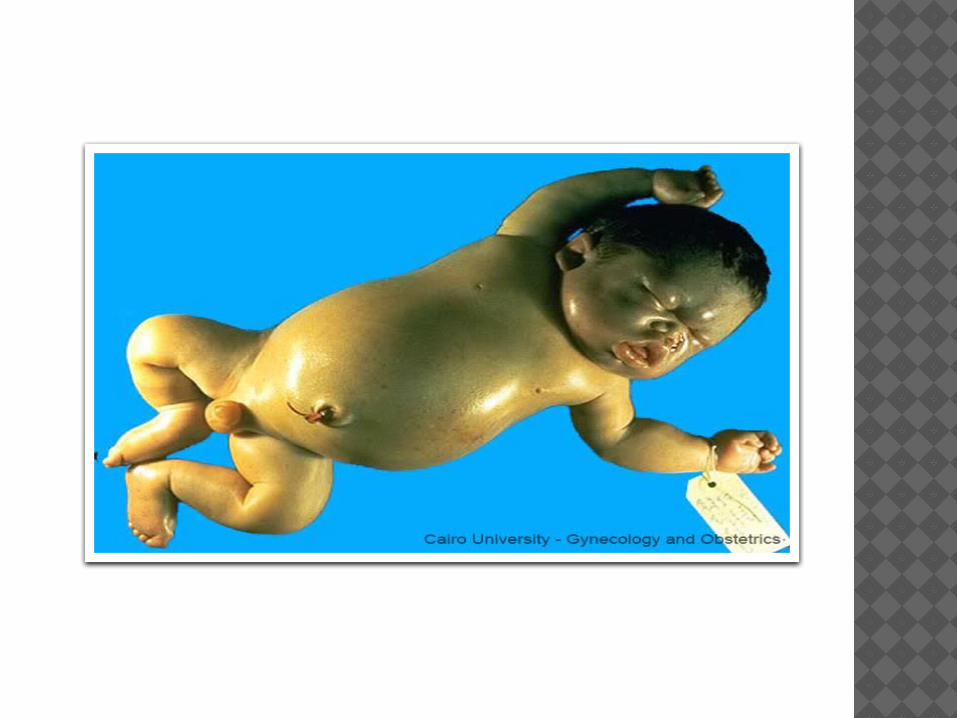
OUTCOMES
The outcomes will varies from:• Mild Anemia and Jaundice .• Severe jaundice and kernicterus.• As severe as erythroblastosis
Fetalis and death in utero..
PATHOPHYSIOLOGY
And this is what it called
Hemolytic Disease of the newborn(HDN)
CAUSE!! Maternal
Fetal
1st exposure
CAUSE!! Maternal
Fetal
2nd exposure

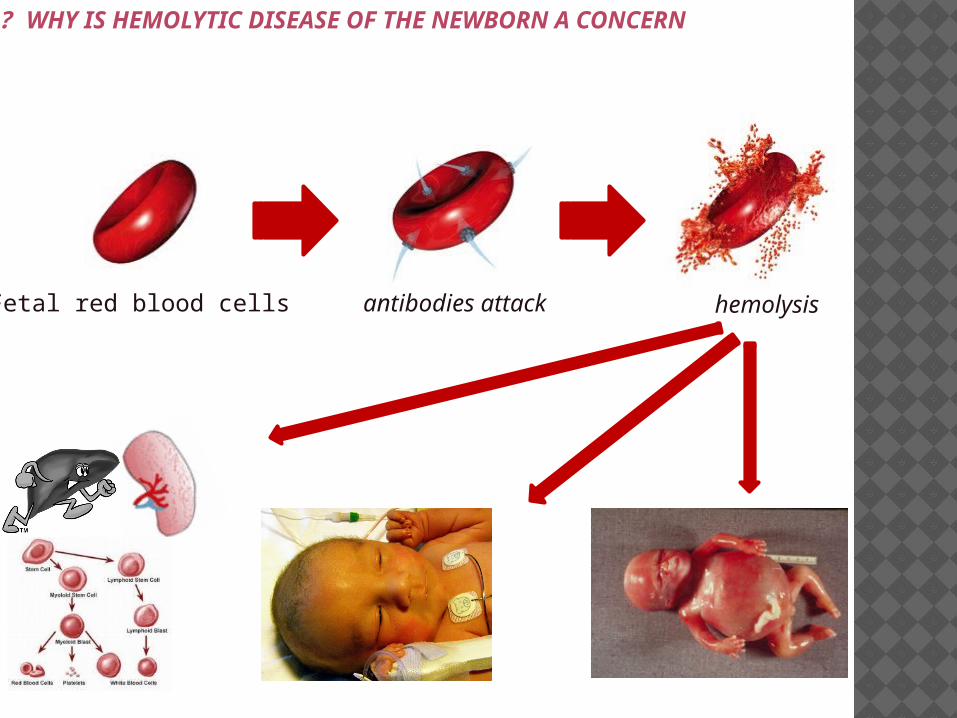
Fetal red blood cells antibodies attack hemolysis
WHY IS HEMOLYTIC DISEASE OF THE NEWBORN A CONCERN ?
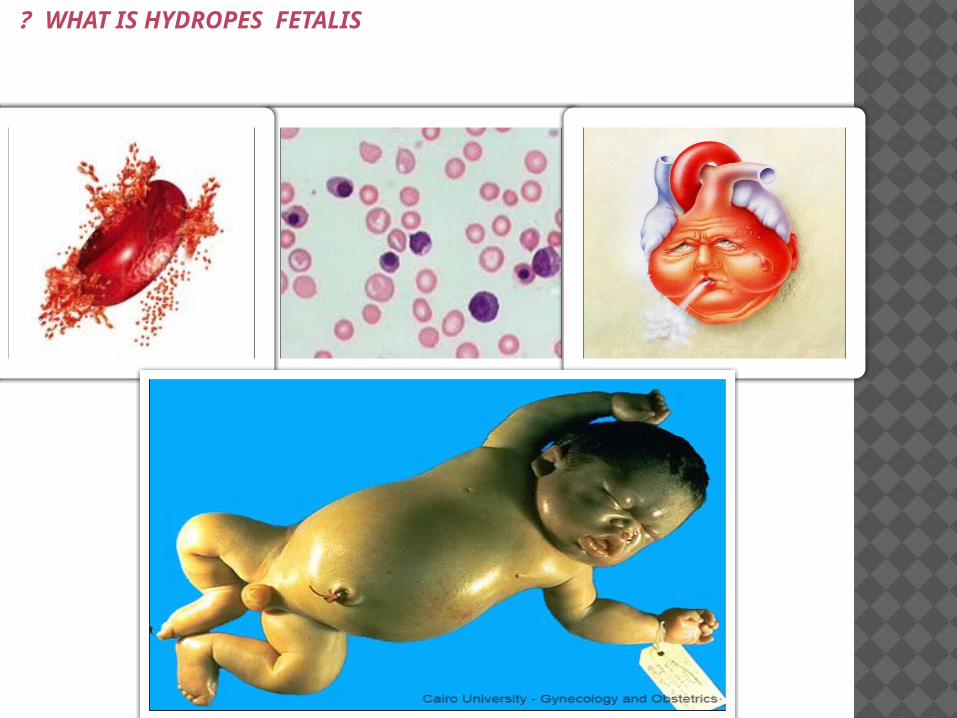
WHAT IS HYDROPES FETALIS ?
What is the risk of
ABO incompatibility On the risk of
Isoimmunization ?
They protects against it ..
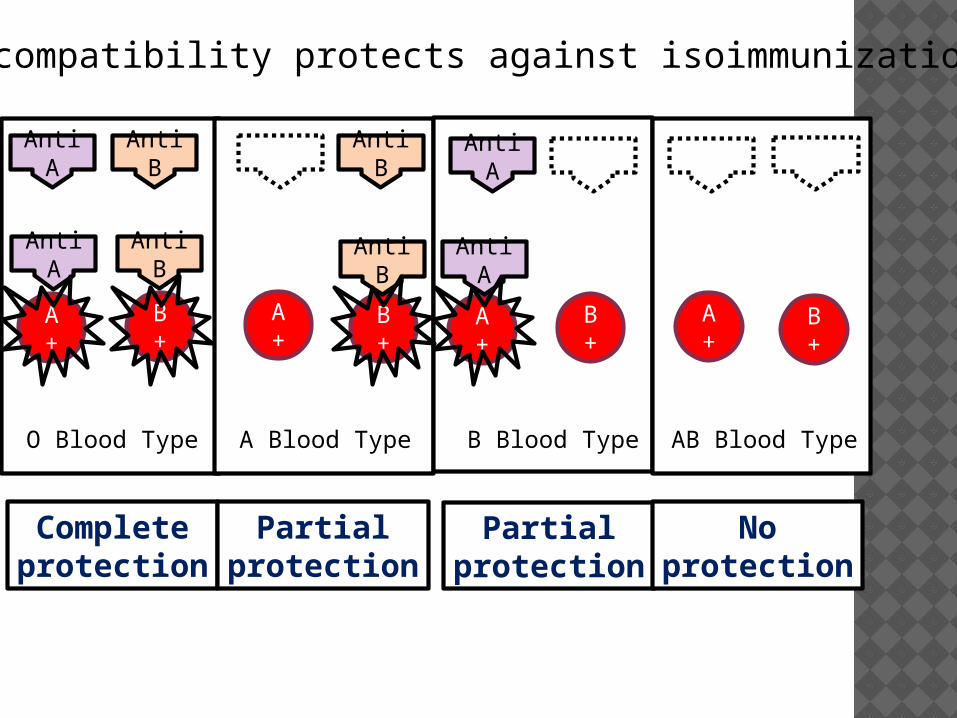
ABO incompatibility protects against isoimmunization
Anti A
Anti B
Anti B
Anti A
O Blood Type AB Blood TypeB Blood TypeA Blood Type
A+
B+
A+
B+
A+
B+
A+
B+
Completeprotection
Partialprotection
Partialprotection
Noprotection
Anti A
Anti B
Anti B
Anti A
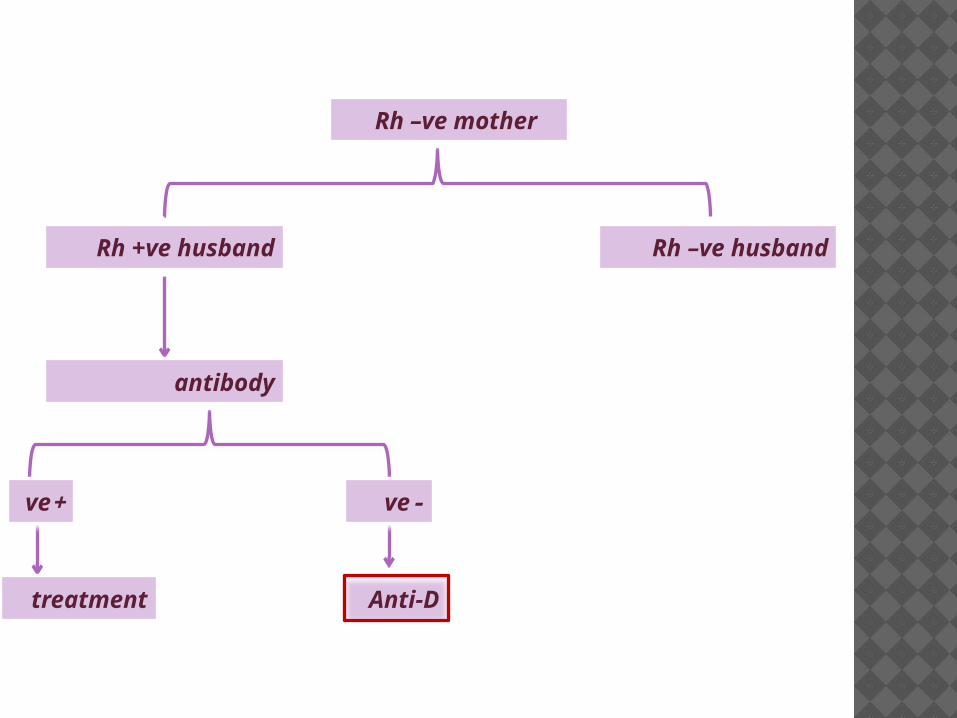
Rh –ve mother
Rh +ve husband Rh –ve husband
antibody
Anti-D
treatment
-ve+ve
HOW TO MANAGE HDN
1) Is the fetus at risk?2) Is the fetus anemic?3) Is the anemia severe enough so
we need to intervene?
1 )Is the fetus at risk?
5 factors must be present :1) Is mother Ag –ve ?2) Is father Ag +ve ?3) Are AAT is +ve ?4) Are Ab associated with HDN ?5) Is Ab titer > 1:8 ?
Low titer
High titer
1 : 21 : 41 : 8 1 : 161 : 321 : 641 : 1281 : 2561 : 5121 : 10241 : 20481 : 4096
Negligible
Significant
2 )Is the fetus Anemic?
3 investigation :1) Amniocentesis looking for
amniotic fluid bilirubin.2) Cordocentesis looking for fetal
hematocrit.3) U/S looking for MCA peak
velocity.
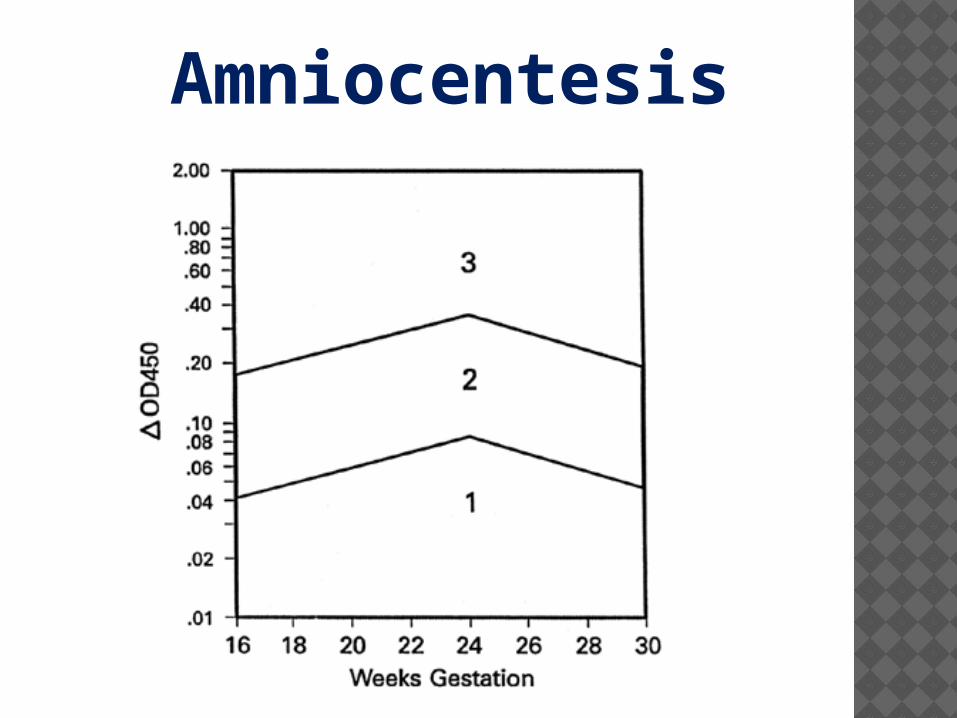
Amniocentesis
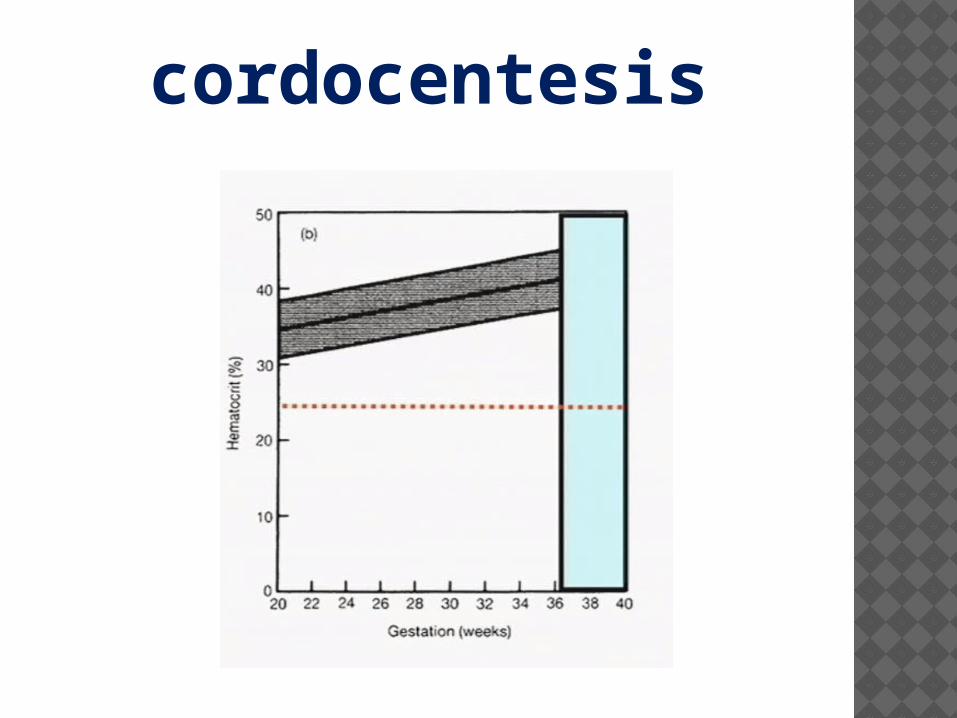
cordocentesis
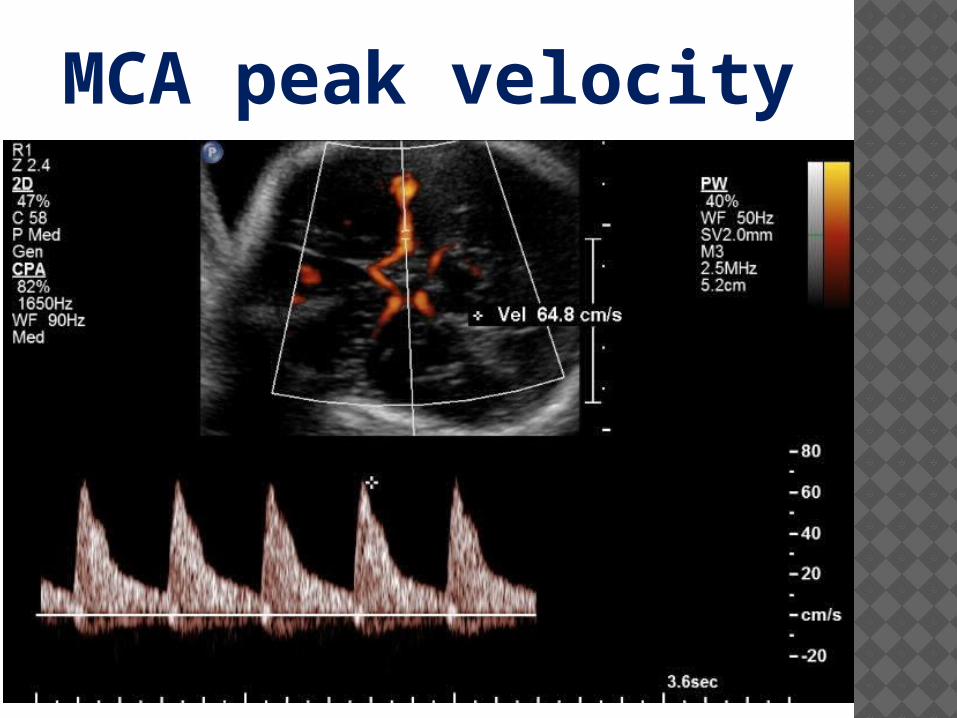
MCA peak velocity

3 )Is intervention needed?
1) Amniocentesis : bilirubin in zone III.
2) Cordocentesis : HCT < 25 .3) U/S : MCA peak velocity is high.
According to GA :If < than 34 weeks gestation : IUT.If > than 34 weeks gestation : Delivery.
INTERVENTIONS
HOW TO PREVENT? By giving Anti D Ig ( RhoGAM ) .It is passively injected IM and it lysis any (D+ RBCs) before lymphocytes activated.We give it routinely at 28 weeks gestation to any (Rh-ve) mother . And after delivery if the fetus is (Rh+ve).Additional dose in special times mainly after CVS , amniocentesis , abortions , D&C ectopic preg. , APH , ECV .

Maternal Fetal
anti-D
WHAT IS THE MECHANISM OF ACTION OF ANTI –D ?
ANTI –D .…
routineFMH300 MCG
KLEIHAUER TEST
FOR 15 ML FETAL RED BLOOD CELL

KLEIHAUER-BETKE SMEAR
EVIDENCE BASED MEDICINE
What is the indications of giving anti-DOn evidence based medicine ?

ALL RECOMMENDATIONS ARE LASTLY
UPDATED AT 14-2-2014
RECOMMENDATION
• All Rh(D)-negative pregnant women should undergo an antibody screen at the first prenatal visit. If the initial screen is negative, a routine repeat screen at 28 weeks of gestation is optional.
RECOMMENDATION
The following recommendations apply to women who are Rh(D)-negative and whose fetus is, or may be, Rh(D)-positive:
We recommend routine administration of anti-D immune globulin early in the third trimester . The optimum dose regimen in the United States is 300 micrograms at 28 weeks of gestation. This practice reduces the incidence of antenatal isoimmunization from 2 to 0.1 %.
RECOMMENDATION
We recommend administration of antenatal anti-D immune globulin when there is an increased risk of fetomaternal hemorrhage. Some examples include miscarriage, abortion, ectopic pregnancy, multifetal reduction, amniocentesis, chorionic villus sampling, blunt abdominal trauma, external cephalic version, antepartum bleeding, and fetal death. We administer 300 micrograms.
RECOMMENDATION
Repeat dosing for situations where there may be an ongoing risk for fetomaternal hemorrhage (such as chronic placental abruption or placenta previa with intermittent vaginal bleeding) can be managed with serial determinations of the maternal indirect Coombs every three weeks with repeat dosing if it is found to be negative.
We recommend administration of anti-D immune globulin within 72 hours of delivery of an Rh(D)-positive infant. We administer 300 micrograms and also test for excessive fetomaternal hemorrhage in case additional doses are needed.
If anti-D immune globulin is inadvertently omitted after delivery, we recommend giving it as soon as possible after recognition of the omission . Partial protection is afforded with administration within 13 days of the birth, and there may be an effect as late as 28 days after delivery.
.
RECOMMENDATION
within 72 hours of delivery to a postpartum nonsensitized Rh-negative
woman.
all Rh-negative nonsensitized women at 28
week of gestation.
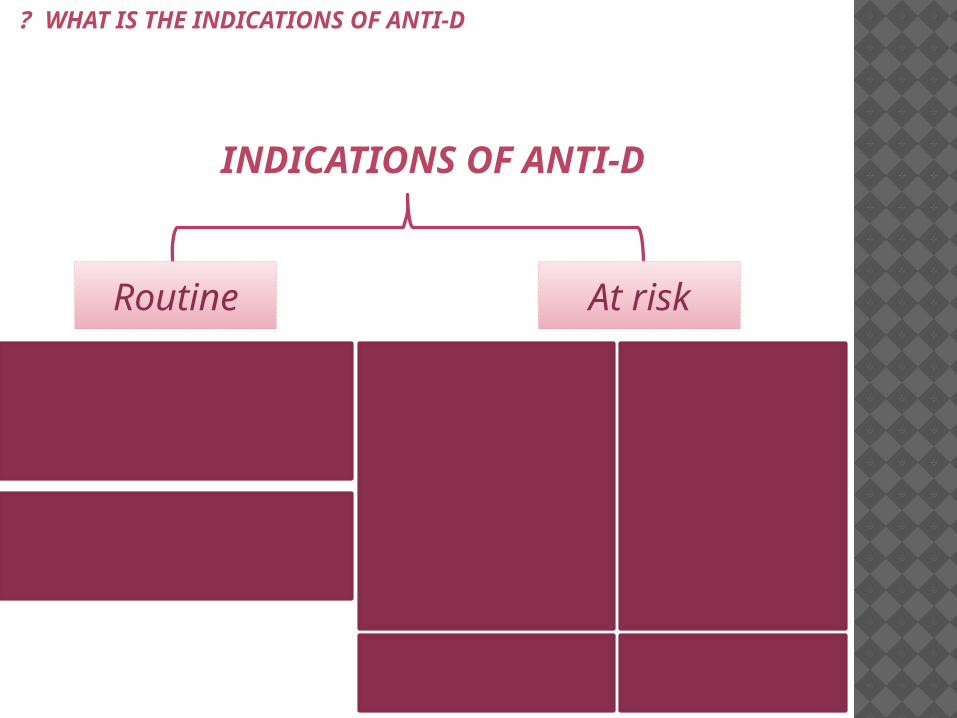
INDICATIONS OF ANTI-D
Bleeding Early :
ectopic pregnancyAbortion
Molar pregnancy APH:
Placenta breviaAbruptio placenta
Vasa brevia
invasive prenatal
procedures
amniocentesis chorion villus
samplingfetal blood sampling
external version of the fetus
abdominal trauuma
At riskRoutine
WHAT IS THE INDICATIONS OF ANTI-D ?

Thank
you