Embed Size (px)
Citation preview

Hemolytic Disease of the Newborn (HDN) & COOMBS TEST
Presented by:
Abbas PishdadianPhD Candidate of Immunology

Pathogenesis of HDN Maternal IgG antibodies directed against an
antigen of paternal origin present on the fetal red blood cells.
IgG antibodies cross the placenta to coat fetal antigens, cause decreased red blood cell survival (as a result of ADCC, opsonization and complement activation) which can result in anemia
2

Three Classifications of HDN
Rh – anti-D alone or may be accompanied by other Rh antibodies – anti-C, -c, -E or –e.
ABO
“Other” – unexpected immune antibodies other than anti-D – Jk, K, Fy, S, etc.
3
Rh Hemolytic Disease Anti-D is the commonest form of severe HDN. The
disease varies from mild to severe. Anti-c can range from a mild to severe disease - is the
third most common form of severe HDN Anti-E is a mild disease, Anti-e and Anti-C are rare antibody combinations (ie anti-c and anti-E antibodies
occurring together) - can be severe It doesn’t affect first child unless: 1. previous incompatible blood transfusion 2. previous abortion 3. uterine wall disruption: amniocentesis, trauma, infection, …
4

5

ABO Hemolytic Disease Mother group O, baby A or B Some group O individuals have anti-A, -B and -A,B in their
plasma with IgG class. The disease is more common and more severe in African-
American infants. ABO HDN can occur during the FIRST pregnancy and prior
sensitization is not necessary ABO HDN is less severe than Rh HDN because:
1. Amount of cross-passing Ab is less than Rh2. ABO antigens are in low numbers3. Fetal RBCs are less developed at birth4. Presence of ABO antigens in tissues and secretions
6

“Other” Hemolytic Disease
Uncommon, occurs in ~0.8% of pregnant women.
Immune alloantibodies usually due to anti-E, -c, -Kell, -Kidd or -Duffy.
Anti-K disease ranges from mild to severe over half of the cases are caused by multiple blood
transfusions is the second most common form of severe HDN
Anti-M very rare
7

HDN
Maternal antibodies destroy fetal red blood cells Results in anemia. Anemia limits the ability of the blood to carry oxygen to the baby's
organs and tissues. Baby's responds to the hemolysis by trying to make more red blood
cells very quickly in the bone marrow and the liver and spleen. Organs enlarge - hepatosplenomegaly. New red blood cells released prematurely from bone marrow and are
unable to do the work of mature red blood cells. As the red blood cells break down, bilirubin is formed.
Babies unable to get rid of the bilirubin. Builds up in the blood (hyperbilirubinemia ) and other tissues and fluids
of the baby's body resulting in jaundice. The placenta helps get rid of some of the bilirubin, but not all.
8

Clinical Presentation Varies from mild jaundice and anemia to hydrops fetalis (with ascites,
pleural and pericardial effusions) Chief risk to the fetus is anemia. Extramedullary hematopoiesis due to anemia results in
hepatosplenomegaly. Risks during labor and delivery include:
asphyxia and splenic rupture. Postnatal problems include:
Asphyxia Pulmonary hypertension Pallor (due to anemia) Edema (hydrops, due to low serum albumin) Respiratory distress Coagulopathies (↓ platelets & clotting factors) Jaundice Kernicterus (bilirubin encephalopathy: from hyperbilirubinemia) Hypoglycemia (due to hyperinsulinemnia from islet cell hyperplasia)
9
Laboratory Findings
Vary with severity of HDN and include: Anemia Hyperbilirubinemia Reticulocytosis (6 to 40%) ↑ nucleated RBC count (>10/100 WBCs) Thrombocytopenia Leukopenia Positive Direct Antiglobulin Test Hypoalbuminemia Rh negative blood type or ABO incompatibility Smear: polychromasia, anisocytosis, no spherocytes
10
Treatment of HDN Intrauterine Transfusion (IUT): ( with group O, D-negative) - Given to the fetus to prevent hydrops fetalis and fetal death.
- Can be done as early as 17 weeks, although preferable to wait until 20 weeks
Measurement of bilirubin: in cord blood and at least every 4 hours for the first 12 to 24 hours.
Phototherapy: The therapy uses a blue light (420-470 nm) that converts bilirubin so that it can be excreted in the urine and feces.
Exchange Transfusion: - if the total serum bilirubin level is approaching 20 mg/dL and continues to rise
despite intense in-hospital phototherapy. - mortality rate of approximately 1% and there may be substantial morbidity
11
Prevention 1968 RhIg first licensed for prophylactic
administration via IM route (RhoGam) RhIg (RhoGAM®) is given to the mother to
prevent immunization to the D antigen RhIg attaches to fetal RBCs in maternal
circulation and are removed in maternal spleen; this prevents alloimmunization by mother
RhIg (1 dose) is given at 28 weeks’ gestation Another dose of RhIg should be given to the mother
within 72 hours of delivery (even if stillborn)12

COOMBS TEST
The Antiglobulin Test Antiglobulin serum (Coombs’ Serum) was discovered by
Coombs in 1945. Anti-human globulin (AHG) is an IgG antibody directed
against human immunoglobulins or complement components.
Sensitization of red cells can occur in vivo or vitro. The use of AHG serum to detect sensitization of red
cells in vitro can be:One stage technique , the direct antiglobulin
test (DAT) - detection of sensitization of RBC s (coated with Abs and/or complement components) in vivo.
Two stage technique , the indirect antiglobulin test (IAT) - detection of sensitization of RBCs in vitro .
14

The Antiglobulin Test
15
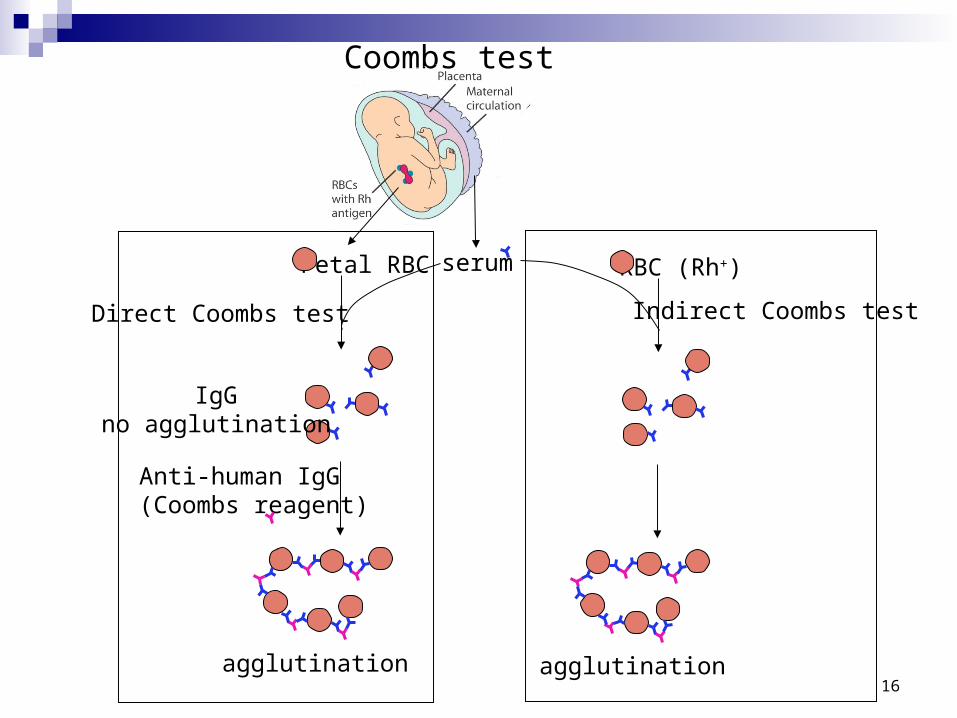
Coombs test
Fetal RBC serum
Anti-human IgG(Coombs reagent)
agglutination
RBC (Rh+)
agglutination
Direct Coombs test Indirect Coombs test
IgGno agglutination
16

Direct Coombs test (direct antiglobulin test):
This test is performed to detect anti-D antibody or other antibodies attached to the red cell surface within the blood stream.
Detects about 150 to 500 IgG or C3d molecules/cell This occurs in the following circumstances:
When there is a Rh-positive baby in the womb of a sensitized Rh-negative women; the antibodies produced in the mothers serum cross the placenta and after entering the baby's blood stream, these antibodies will attach to the baby's Rh-positive red blood cells. These coated (or sensitized) cells are clumped and removed from the circulation, causing hemolytic anemia (Hemolytic Disease of the Newborn: Erythroblastosis Fetalis). When the baby is born, the baby's blood is collected (or cord blood is collected from umbilical cord) and tested by the anti globulin Coombs test (direct) to detect anti D antibodies coated on red blood cells.
Transfusion reactions Drug induced red cells sensitization Autoimmune hemolytic anemia
17

18

Requirements: (same as that for Indirect Coombs test)
Test tubes: (10x75 mm) Pasteur pipettes (or Sampler) Incubator Centrifuge
Specimen: Blood drawn into EDTA is preferred but oxalateed, or clotted, citrated whole blood may be used (specimen need not be fasting sample)
19

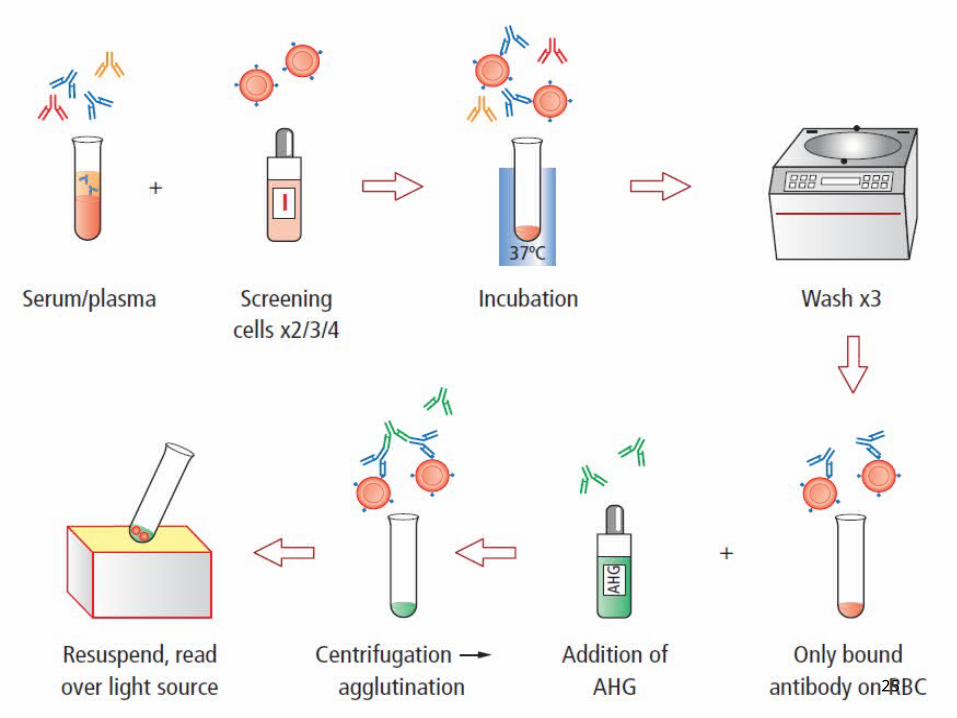
Procedure:
1. Prepare a 5 % suspension in isotonic saline of the red blood cells to be tested.
2. With clean Pasture pipette (or sampler) add one drop of the prepared cell suspension to a small tube.
3. Wash three times with normal saline to remove all the traces of serum.
4. Decant completely after the last washing
5. Add two drops of Antihuman serum.
6. Mix well and centrifuge for one minute at 1500 RPM.
7. Resuspend the cells by gentle agitation and examine macroscopically and microscopically for agglutination.
20

Indirect Coombs test (Indirect Antiglobulin test):
This test is performed to detect presence of Rh-antibodies or other antibodies in patients serum in case of the following:
Detects about 100 to 200 IgG or C3d molecules/cell1. To check whether an Rh-negative women (married to Rh-
positive husband) has developed Anti Rh-antibodies
2. Anti D may be produced in the blood of any Rh-negative person by exposure to D antigen by-
Transfusion of Rh positive blood Pregnancy, if infant is Rh positive (if father is Rh-positive) Abortion of Rh-positive fetus.
21

22

Requirements:
Test tubes: (10x75 mm) Pasteur pipettes (or Sampler) Incubator Centrifuge
Specimen: Serum (need not be fasting)
Reagents: 1. Antihuman serum2. Anti-D serum
Additional Requirements: Coombs control cells
A. Make a pooled ‘O’ Rho (D) positive cells from at least three different ‘O’ positive blood samples.
B. Wash these cells three times in normal saline (these cells should be completely free from serum with no free antibodies). Make 5 % saline
suspension of these cells
23
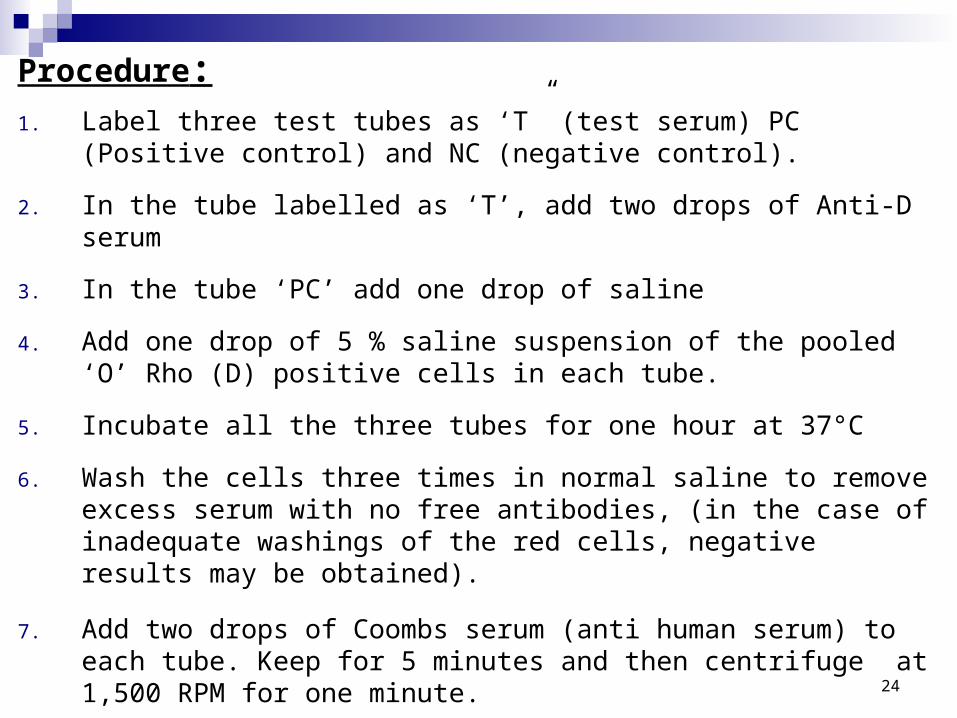
Procedure:1. Label three test tubes as ‘T” (test serum) PC (Positive control) and NC
(negative control).
2. In the tube labelled as ‘T’, add two drops of Anti-D serum
3. In the tube ‘PC’ add one drop of saline
4. Add one drop of 5 % saline suspension of the pooled ‘O’ Rho (D) positive cells in each tube.
5. Incubate all the three tubes for one hour at 37°C
6. Wash the cells three times in normal saline to remove excess serum with no free antibodies, (in the case of inadequate washings of the red cells, negative results may be obtained).
7. Add two drops of Coombs serum (anti human serum) to each tube. Keep for 5 minutes and then centrifuge at 1,500 RPM for one minute.
8. Resuspend the cells and examine macroscopically as well as microscopically 24
25
REACTION MEDIAREACTION MEDIA 22% albumin
decreases zeta potential by buffering allows Ab-coated cells to come closer together
Low Ionic Strength Solution (LISS) decreases zeta potential serum/cells very important; increase amount of serum
with caution Polyethylene glycol (PEG)
removes water, concentrating Ab use monospecific AHG with anti-IgG (else, false
positives) do not read aggl. microscopically (false positives)
26






















![Hdn 1dc Hdn 2dc Hdn 3dc [Rev 3 0] Ru Web](https://img.dokumen.tips/doc/110x75/55cf9823550346d03395cc06/hdn-1dc-hdn-2dc-hdn-3dc-rev-3-0-ru-web.jpg)