Embed Size (px)
DESCRIPTION
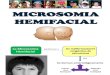
craniofacial microsomia is a variable hypoplasia of the face involing the structures derived from the 1st and 2nd branchial arches.
Citation preview

CRANIOFACIAL CRANIOFACIAL MICROSOMIAMICROSOMIA
DR ALAMZEB KHANDR ALAMZEB KHANDEPARTMENT OF PLASTIC AND DEPARTMENT OF PLASTIC AND RECONSTRUCTIVE SURGERYRECONSTRUCTIVE SURGERY
King abdulaziz specialist hospital King abdulaziz specialist hospital
Taif, saudi arabiaTaif, saudi arabia


INTRODUCTIONINTRODUCTION
Craniofacial microsomia, a variable hypoplasia of the skeleton as well as of the overlying soft tissue, is the second most common congenital syndrome of the head and neck region, withan incidence as high as 1 in 3,500 live births.

ETIOLOGYETIOLOGY
Many theories regarding the etiology but The most commonly accepted is a teratogen theory of a vascular insult, with hemorrhage and hematoma formation in the developing first and second branchial arches and subsequent maldevelopment of the latter.


DERIVATIVES OF FIRST BRANCHIAL DERIVATIVES OF FIRST BRANCHIAL ARCHARCH

DERIVATIVES OF SECOND BRANCHIAL DERIVATIVES OF SECOND BRANCHIAL ARCHARCH


Goldenhar SyndromeGoldenhar Syndrome Also called Oculoauriculovertebral dysplasia or Also called Oculoauriculovertebral dysplasia or
Branchial arch syndrome. Branchial arch syndrome. Characterized by multiple anomalies of the ocular, Characterized by multiple anomalies of the ocular,
cardiac, skeletal and central nervous system. cardiac, skeletal and central nervous system. Ten percent of those affected are mentally retarded. Ten percent of those affected are mentally retarded. Classic triad of the syndrome includes: Classic triad of the syndrome includes:
Hemifacial microsomia Hemifacial microsomia Epibulbar dermoids or dermolipomas Epibulbar dermoids or dermolipomas Deformity of the ears with pre-auricular appendages. Deformity of the ears with pre-auricular appendages.
Associated malformations include orbital hypoplasia, Associated malformations include orbital hypoplasia, upper lid colobomas, nasolacrimal duct obstruction, upper lid colobomas, nasolacrimal duct obstruction, strabismus, iris coloboma, persistent papillary strabismus, iris coloboma, persistent papillary membrane, hypoplasia of the pinna, absent external membrane, hypoplasia of the pinna, absent external auditory meatus, fusion of cervical vertebrae, renal auditory meatus, fusion of cervical vertebrae, renal agenesis and multicystic kidney.agenesis and multicystic kidney.

PRUZANSKY’S CLASSIFICATIONPRUZANSKY’S CLASSIFICATION Type I. Mild hypoplasia
of the ramus, and the body of the mandible is minimally or slightly affected.
Type II. The condyle and ramus are small; the head of the condyle is flattened; the glenoid fossa is absent; the condyle is hinged on a flat, often convex, infratemporal surface; the coronoid may be absent.
Type III. The ramus is reduced to a thin lamina of bone or is completely absent. There is no evidence of a temporomandibular joint.



Microtia typesMicrotia types

PREOPERATIVE ASSESSMENT
COMPLETE HISTORYCOMPLETE HISTORY PHYSICAL EXAMINATIONPHYSICAL EXAMINATION PHOTOGRAPHS (PHOTOGRAPHS (Frontal,
Lateral,oblique, Submental Vertex, And Occlusal Views)
CEPHALOGRAMS (posteroanterior, lateral, and basilar)
PANORAMIC ROENTGENOGRAM (panorex)
THREE DIMENSIONAL CT SCAN



3-D CT SCAN3-D CT SCAN


Occular dermoidOccular dermoid


TREATMENT


YOUNGER THAN TWO YEARS OF AGE Excision of the preauricular skin tags and
cartilage remnants Correction of macrostomia Patient with involvement of the fronto-orbital
region, characterized by severe retrusion of the
supraorbital bar and frontal bone, a fronto-orbital advancement–cranial vault remodeling can be performed as a combined craniofacial surgical procedure.
Mandibular distraction for patients with sleep apneoa


No treatment is required for No treatment is required for Pruzansky type I
mandible and a horizontal occlusal plane distraction osteogenesis is required for
Pruzansky II In the patient with a Pruzansky type III
a preliminary costochondral rib graftreconstruction should be performed at approximately age 4 years.
TWO TO SIX YEARS OF AGE

BETWEEN 6 AND 14 YEARS OF AGE
Orthodontic treatment.Orthodontic treatment. Ear reconstruction.(rib cartilage Ear reconstruction.(rib cartilage
is large enough at 6 years)is large enough at 6 years) Soft-tissue augmentation, often by Soft-tissue augmentation, often by
free-tissue transfer.(,subcutaneous free-tissue transfer.(,subcutaneous volumizers, dermal fillers, fat volumizers, dermal fillers, fat grafts , local flaps and grafts , local flaps and microvascular free flaps etcmicrovascular free flaps etc

AFTER 14 YEARS OF AGE
Bone grafting to deficient Bone grafting to deficient areas of the facial skeleton.areas of the facial skeleton.
Orthognathic surgery.Orthognathic surgery.