Embed Size (px)
Citation preview

Overview • Physical exam & anatomy
• Lacerations
• Fractures & Dislocations
• Arthritis, Contracture, Deformity
• Carpal Tunnel
• Infection
• On the horizon

• Distal phalanx
• Middle phalanx
• Proximal phalanx
• Metacarpal
• DIP joint• PIP joint• MCP
joint

• Proximal row– Scaphoid– Lunate– Triquetrum– Pisiform
• Distal row– Trapezium– Trapezoid– Capitate
– Hamate
• Radius• Ulna

• A thorough exam can diagnose most injuries. Try to avoid wound exploration
• Apply direct pressure to bleeders rather than blindly clamping or tying off vessels

• Assess active motion– Flexor digitorum
profundus (FDP)• Ask patient to flex DIP
while examiner stabilizes the PIP and MCP in extension
– Flexor digitorum sublimus (FDS)
• Hold all fingers extended except affected finger, then ask the patient to flex affected finger

• Assess digital perfusion– Color– Turgor– Capillary refill < 2 seconds– Digital Allen’s test
• Nerves– Radial digital nerve– Ulnar digital nerve

Treatment• Thorough I&D• Tetanus
– Booster if > 5 years– Immunoglobulin
• >10 year since last immunization• Manure, puncture wounds, wounds >6 hours old
• Antibiotics– 1st generation cephalosporin for complex
wounds (Cefadroxil, Cephalexin)– 3 – 5 day course

• Suture of simple superficial lacerations
• Surgical repair of complex deep wounds

Mammalian Bites
• 80-90% of all bites are dog bites• I&D and then loose closure• Debride puncture wounds (cats) – do not suture• Consider tetanus and rabies prophylaxis• Antibiotic goal is to cover:
– Staphylococci, Streptococci, anaerobes, and Pasteurella species.
– Augmentin 875 BID– 3 - 5 day course
• Human bites– Fight bite – I&D in OR

• Dog bites – Staphylococcus species – Streptococcus species – Eikenella species – Pasteurella species – Proteus species – Klebsiella species – Haemophilus species – Enterobacter species – DF-2 or Capnocytophaga
canimorsus – Bacteroides species – Moraxella species – Corynebacterium species – Neisseria species – Fusobacterium species – Prevotella species – Porphyromonas species
• Cat bites – Pasteurella species – Actinomyces species – Propionibacterium
species – Bacteroides species – Fusobacterium species – Clostridium species – Wolinella species – Peptostreptococcus
species – Staphylococcus species – Streptococcus species

• Assess neurovascular status
• Reduce dislocations/deformity urgently
• Open fractures– Emergency operative care for I&D, IV abx– Not the same operative urgency as lower
extremity injuries
• Splint for comfort and stability

Phalanx fractures• Deforming forces
– Flexor tendons– Extensor tendons– Difficult to maintain
reduction
– Operative management often required for displaced fractures – CRPP vs. ORIF
• Rotational deformity

Metacarpal fracture
• Acceptable angulation up to 40° in some cases
• Boxer’s fracture – 5th metacarpal neck

Carpal fractures
• Scaphoid– TTP in “snuff box”
• Thumb spica even if normal x-rays
– Poor vascularity• Slow to heal• Non-unions common
– MRI can help to diagnose acute non-displaced fractures

Distal radius fractures
• “Colles fracture”• Fall onto outstretched
hand• Closed reduction
required for displaced fractures
• Beware of open fracture – open ulnar puncture

• Operative intervention for unstable fractures– ORIF now more common than ex fix– Locking technology

Fragility fracture
• Fracture from low-energy events
• Hip, spine, proximal humerus, distal radius
• DEXA scan
• Labs to exclude other causes
• Treatment – Bisphosphonates– Hormone replacement

Ganglion
• 60% of hand lesions
• Benign fluid filled sac– Not a true cyst – lacks epithelial
lining– Glucosamine, albumin,
hyaluronic acid, globulin
• Communicates with joint or tendon sheath
• Women > men = 3:1• Soft, mobile, transilluminates

Treatment
• Observation – up to 50% spontaneous resolution
• Aspiration– +/- steroid injection– >50% recurrence– Avoid aspiration for volar ganglion
• Surgical excision– <5% recurrence– Open or arthroscopic

Basal Joint Arthritis
• Symptoms – Pain at base of thumb
at carpo-metacarpal joint
– Pain with heavy grip and pinch
• Lifting pots• Turning keys
• X-rays– Spurs/osteophytes– Collapsed joint space

Treatment
• Initial– Thumb spica splint– NSAIDs– Activity modification
• Injection – steroid
• Surgery– Resect trapezium– +/- LRTI

Dupuytren’s Contracture• Contracture of palmar
fascia• Progressive deformity• Men >> Women• Autosomal dominant• Northern European/
Scandanavian/British

Treatment
• Surgical excision– Painful nodules– Contracture > 30°
• Needle aponeurotomy• Collagenase
– Injected into cord– Recent FDA approval

Carpal tunnel syndrome
• Median nerve compressed by transverse carpal ligament at wrist

Symptoms
• Pain & numbness• Grip weakness• Women > Men• Nocturnal pain• Only associated
occupational risk:– Jack hammer use

Treatment
• R/o cervical etiology• Night splinting• +/- Injection• Surgical release
– Open– Endoscopic

Paronychia
• S Aureus• Pseudomonas• Candida
• Acute treatment: – warm soaks
– 1st gen cephalosporin
– 3-5 days
• Abscess: office I&D
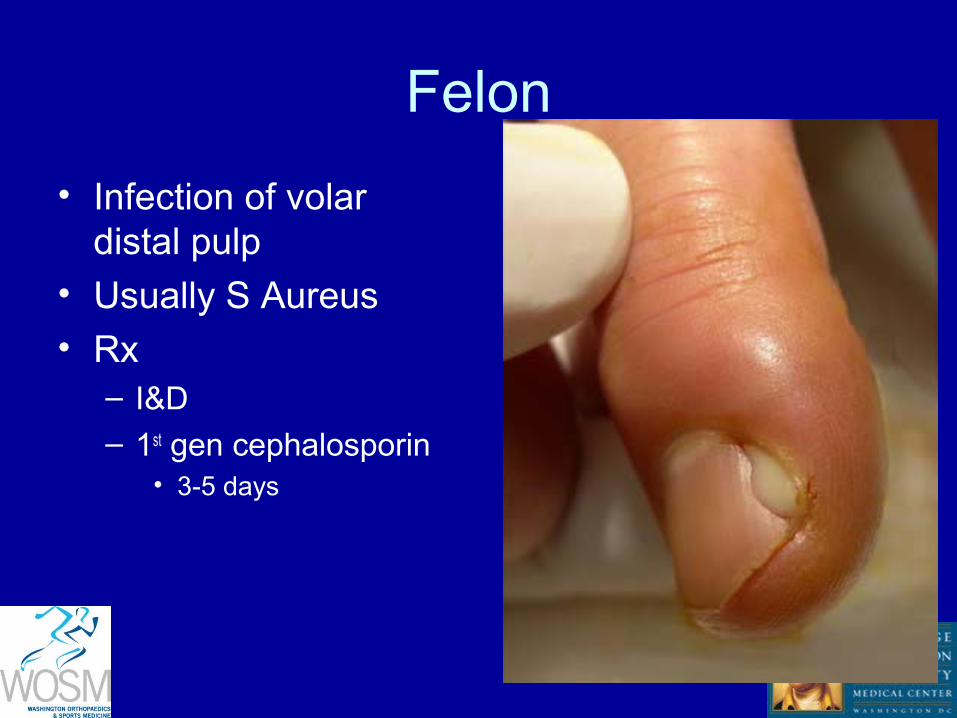
Felon
• Infection of volar distal pulp
• Usually S Aureus• Rx
– I&D – 1st gen cephalosporin
• 3-5 days

Supporative Flexor Tenosynovitis
• Infection of flexor tendon sheath
• S Aureus & Gr A Beta Hemolytic Strep

Kanavel’s Cardinal Signs
• Flexed posture• Pain with passive
extension• Fusiform swelling –
“Sausage digit”• Tenderness along
flexor tendon

Platelet-Rich Plasma
• Autologous blood with platelet concentration > baseline values
• Growth factors recruit reparative cells, enhance healing

Growth Factors in PRP• Platelet-derived growth factor
– Platelets Stimulates cell replication, angiogenesis, mitogen for fibroblasts
• Vascular endothelial growth factor– Platelets Angiogenesis
• Transforming growth factor-β1– Platelets Key regulator in balance between fibrosis and myocyte
regeneration• Fibroblast growth factor
– Platelets Stimulates proliferation of myoblasts,angiogenesis• Epidermal growth factor
– Platelets Proliferation of mesenchymal and epithelial cells, potentiation of other growth factors
• Hepatocyte growth factor– Plasma Angiogenesis, mitogen for endothelial cells, antifibrotic
• Insulin-like growth factor-1– Plasma Stimulates myoblasts and fibroblasts, mediates growth and
repair of skeletal muscle

• Exciting treatment option
• Lots of potential• Excellent safety profile• Awaiting definitive
supporting evidence