Embed Size (px)
Citation preview
In Post CABG SurgeryIn Post CABG Surgery
PUSAT JANTUNG NASIONAL HARAPAN KITAPUSAT JANTUNG NASIONAL HARAPAN KITAJAKARTAJAKARTA
20082008
ASPILETASPILETSSBY :BY :
ARI PNARI PN
Platelets are particles (actually remnants of cells) circulating in the blood that are necessary in order for blood clots to form. Platelets initiate the formation of blood clots by clumping together, a process called platelet aggregation.
Clumps of platelets then are further bound together by a protein (fibrin) formed from clotting factors present in the blood. The clumps of platelets and fibrin make up the blood clot.
Platelets AggregationPlatelets Aggregation
Blood clots are important because they stop us from bleeding when we get cut. However, if a blood clot forms inside an artery , it blocks the flow of blood to the tissue that the artery supplies, and that can damage the tissue.
For example, a blood clot that forms in a coronary artery supplying blood to heart muscle causes a heart attack, and a blood clot that forms in an artery supplying blood to the brain causes a stroke.
Platelets AggregationPlatelets Aggregation
Platelets AggregationPlatelets Aggregation
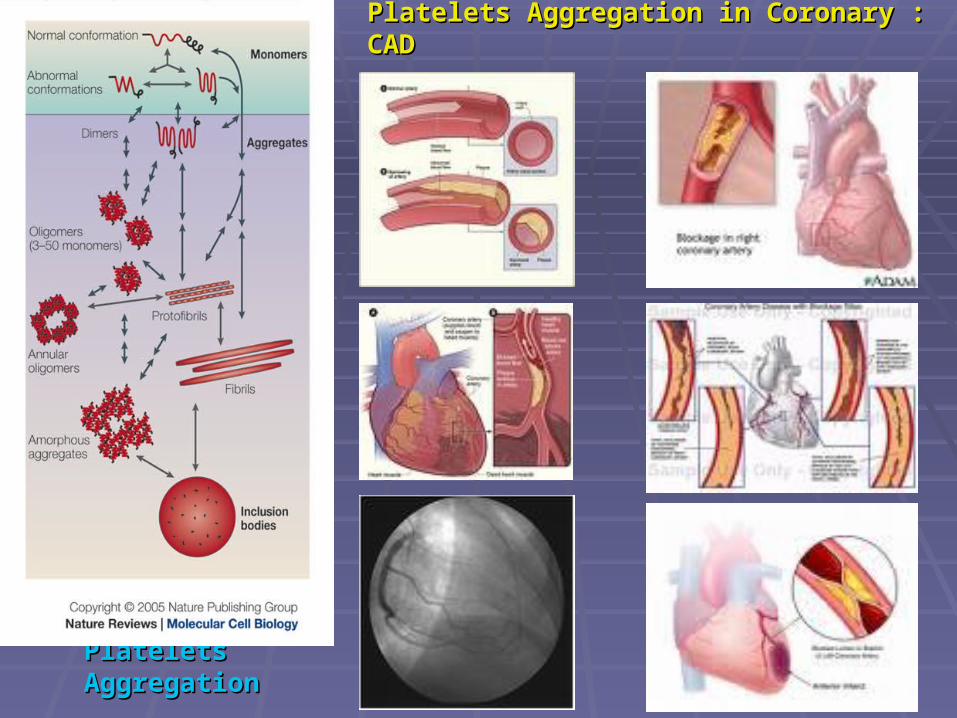
Platelets Aggregation in Coronary : CADPlatelets Aggregation in Coronary : CAD
Antiplatelet agents are medications that block the formation of blood clots by preventing the clumping of platelets.
There are three types of antiplatelet agents: aspirin, the thienopyridines, and the glycoprotein IIb/IIIa inhibitors.
These agents differ in four ways: the way in which they prevent platelets from clumping, their potency (how strongly they prevent clumping), how rapidly they work, and their cost.
Anti platelets AgentsAnti platelets Agents
What ASPILET ?What ASPILET ?
Anticoagulants, Antiplatelets & Fibrinolytics (Thrombolytics)
Acetylsalicylic acid anhihidrat molecul
2-hidroksibenzoat acid
= 2-hidroksibenzenkarboksilat acid = salisilat acid
Aspilets® Molecul Model
Treatment of mild to moderate pain, inflammation, and fever;
may be used as prophylaxis of myocardial infarction; prophylaxis of stroke and/or transient ischemic episodes;
management of rheumatoid arthritis, rheumatic fever, osteoarthritis, and gout (high dose);
adjunctive therapy in revascularization procedures : (coronary artery bypass graft [CABG], percutaneous transluminal coronary angioplasty [PTCA], carotid endarterectomy)
IndicationsIndications
hypersensitivity to salicylates, other NSAIDs, or any component of the formulation;
asthma; rhinitis;nasal polyps; inherited or acquired bleeding disorders (including
factor VII and factor IX deficiency); do not use in children (<16 years of age) for viral
infections (chickenpox or flu symptoms), with or without fever;
pregnancy (3rd trimester especially)
ContraindicationsContraindications
Serious side effects of aspirin such as bleeding ulcers or intracranial bleeding are rare (less than 1% of patients) among patients taking moderate doses of aspirin, e.g., 325 mg/d.
Serious side effects of aspirin should be even lower with low doses such as 75-160 mg/d. However, the actual incidence of serious bleeding with long-term use of low dose aspirin has not been determined clearly.
Side EffectSide Effect

Cardiovascular: Hypotension, tachycardia, dysrhythmias, edema
Central nervous system: Fatigue, insomnia, nervousness, agitation, confusion, dizziness, headache, lethargy, cerebral edema, hyperthermia, coma
Gastrointestinal: Nausea, vomiting, dyspepsia, epigastric discomfort, heartburn, stomach pains, gastrointestinal ulceration (6% to 31%), gastric erosions, gastric erythema, duodenal ulcers
Side effectSide effect
DRUG INTERACTIONS
Anticoagulants: See WARNINGS. Hypoglycemic Agents: See WARNINGS. Uricosuric Agents: Aspirin may decrease the effects of probenecid, sulfinpyrazone, and phenylbutazone. Spironolactone: See PRECAUTIONS. Alcohol: Has a synergistic effect with aspirin in causing gastrointestinal bleeding. Corticosteroids: Concomitant administration with aspirin may increase the risk of gastrointestinal ulceration and may reduce serum salicylate levels. Pyrazolone Derivatives (phenylbutazone, oxyphenbutazone, and possibly dipyrone): Concomitant administration with aspirin may increase the risk of gastrointestinal ulceration.
DRUG INTERACTIONS
Nonsteroidal Antiinflammatory Agents: Aspirin is contraindicated in patients who are hypersensitive to nonsteroidal antiinflammatory agents. Urinary Alkalinizers: Decrease aspirin effectiveness by increasing the rate of salicylate renal excretion. Phenobarbital: Decreases aspirin effectiveness by enzyme induction. Phenytoin: Serum phenytoin levels may be increased by aspirin. Propranolol: May decrease aspirin's antiinflammatory action by competing for the same receptors. Antacids: Enteric-coated aspirin should not be given concurrently with antacids, since an increase in the pH of the stomach may effect the enteric coating of the tablets.
Heparin and low molecular weight heparins: Concurrent use may increase the risk of bleeding.
Drug IntercationsDrug Intercations
۩ Use with caution in patients with platelet and bleeding disorders, renal dysfunction, dehydration, erosive gastritis, or peptic ulcer disease.
۩ Heavy ethanol use (>3 drinks/day) can increase bleeding risks. Avoid use in severe renal failure or in severe hepatic failure.
۩ Discontinue use if tinnitus or impaired hearing occurs.
Warnings/Precautions
۩ Caution in mild-moderate renal failure (only at high dosages).
۩ Patients with sensitivity to tartrazine dyes, nasal polyps and asthma may have an increased risk of salicylate sensitivity.
۩ Surgical patients should avoid ASA if possible, for 1-2 weeks prior to surgery, to reduce the risk of excessive bleeding.
Warnings/Precautions
As with all drugs which may affect hemostasis, bleeding is associated with aspirin. Hemorrhage may occur at virtually any site.
Risk is dependent on multiple variables including dosage, concurrent use of multiple agents which alter hemostasis, and patient susceptibility. Many adverse effects of aspirin are dose-related, and are rare at low dosages.
Other serious reactions are idiosyncratic, related to allergy or individual sensitivity.
Accurate estimation of frequencies is not possible. The reactions listed below have been reported for aspirin.
Adverse Reactions
Aspirin when taken together with an anti-coagulant such as Coumadin or Lovenox, can greatly impair the
body's ability to form blood clots, resulting in excessive bleeding spontaneously, from ulcers, or related to a
procedure. Therefore, patients on such combinations must be closely monitored by a doctor.
Aspirin can raise levels of uric acid in the blood and may need to be avoided in patients with increased uric acid
levels or gout.
Aspirin can increase the effect of medications used for lowering blood sugar levels in patients with diabetes, resulting in abnormally low blood sugar levels. Blood
sugar levels may need to be more closely monitored.
Drug InteractionDrug Interaction
Certain NSAIDs, particularly ibuprofen (Motrin, Advil), if taken just before aspirin or in multiples
doses each day, can reduce the antiplatelet effects of aspirin and theoretically render aspirin
less effective in preventing heart attacks and ischemic strokes. The ibuprofen molecule is
believed to adhere to the COX-1 enzyme, thus keeping aspirin from reaching the enzyme.
Drug InteractionDrug Interaction
Aspirin prevents blood from clotting by blocking the production of thromboxane A-2, a chemical that platelets produce that causes them to clump. Aspirin accomplishes this by inhibiting the enzyme cyclo-oxygenase-1 (COX-1) that produces thromboxane A-2. While other NSAIDs also inhibit the COX-1 enzyme, aspirin is the preferred NSAID for use as an antiplatelet agent because its inhibition of the COX-1 enzyme lasts much longer than the other NSAIDs. Thus, aspirin's antiplatelet effect lasts for days while the other NSAIDs' antiplatelet effects last for only hours.
How Aspilets Work ?How Aspilets Work ?
Low doses (75 mg/day), complete inhibition of the COX-1 enzyme and maximal antiplatelet effect may take several days.
At a dose of 160-325 mg/day, the maximal antiplatelet effect of aspirin occurs within 30 minutes.
Thus aspirin at low doses (75-150 mg/day) is used for the long-term prevention of heart attacks and strokes,
whereas moderate doses (160-325 mg/day) of aspirin are used in situations where an immediate antiplatelet effect is needed (such as in the treatment of acute heart attacks and unstable angina).
How quickly do antiplatelet agents work?
Overdosage of 200-500 mg/kg is in the fatal range
WARNINGWARNING
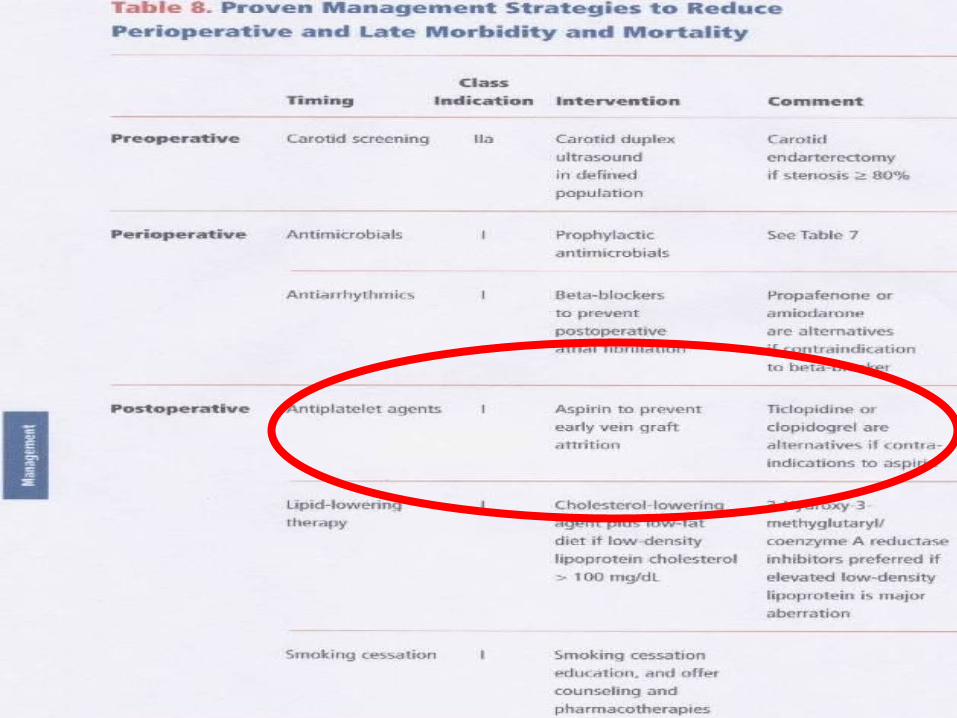
©In rare instances, PTCA may be technically impossible to do, and coronary artery bypass graft surgery (CABG) becomes necessary to improve the flow of blood to the heart.
©Some patients with heart attacks are treated with thrombolytic agents (medications that dissolve clots) to open blocked arteries. In all of these instances, there is a risk that blood clots will form again inside the arteries leading to further heart attacks.
©In all these instances, aspirin has been shown to be beneficial in preventing new clots, thus reducing the risk of heart attacks and improving both short- and long
Considering Aspilets In CABG Considering Aspilets In CABG SurgerySurgery
Pathophysiological process of CHD has not been altered. Secondary prevention of CHD and antiplatelet drugs are one of the most important aspects of medical therapy.
Patients with successful CABG will still have an increased long-term risk of angina, myocardial infarction (MI), or stroke, as the underlying : restenosis
Considering Aspilets In Post Considering Aspilets In Post CABG SurgeryCABG Surgery
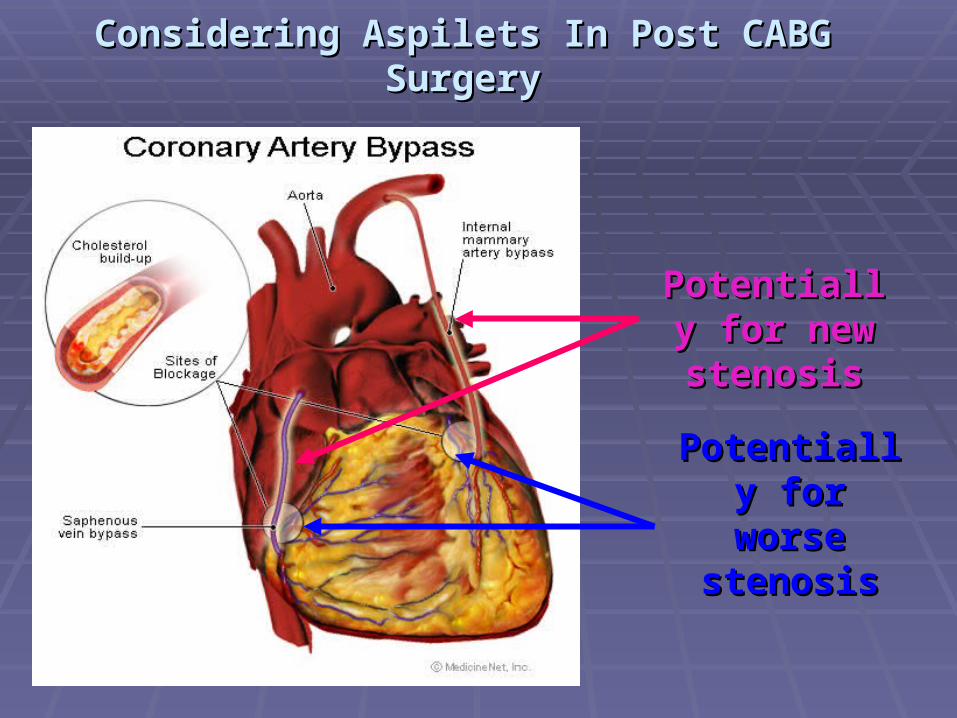
Considering Aspilets In Post CABG SurgeryConsidering Aspilets In Post CABG Surgery
Potentially Potentially for new for new stenosisstenosis
Potentially Potentially for worse for worse stenosisstenosis
Considering Aspilets In Post CABG SurgeryConsidering Aspilets In Post CABG SurgeryDebate : How Early Give AspiletsDebate : How Early Give Aspilets
Dr Dennis T Mangano (Ischemia Research and Education Foundation, Dr Dennis T Mangano (Ischemia Research and Education Foundation, San Francisco) and colleagues for the Multicenter Study of San Francisco) and colleagues for the Multicenter Study of
Perioperative Ischemia Research GroupPerioperative Ischemia Research Group
aspirin ranging from a total of 80 mg to a aspirin ranging from a total of 80 mg to a total of 650 mg within 48 hours of surgery total of 650 mg within 48 hours of surgery
Aspirin therapy was safe and was not Aspirin therapy was safe and was not associated with increased risk of bleeding, associated with increased risk of bleeding,
gastritis, infection, or impaired wound gastritis, infection, or impaired wound healing.healing.

Considering Aspilets In Post CABG SurgeryConsidering Aspilets In Post CABG SurgeryDebate : How Early Give AspiletsDebate : How Early Give Aspilets
Report By: Ghassan Musleh Report By: Ghassan Musleh Search checked by Joel Dunning - Search checked by Joel Dunning - RCS Research FellowRCS Research Fellow Institution: Manchester Royal Infirmary Institution: Manchester Royal Infirmary
There is good evidence that aspirin given There is good evidence that aspirin given <6 hours post surgery optimally reduces <6 hours post surgery optimally reduces graft occlusion, without an increase in graft occlusion, without an increase in bleeding.bleeding.
Considering Aspilets In Post CABG SurgeryConsidering Aspilets In Post CABG SurgeryDebate : How Early Give AspiletsDebate : How Early Give Aspilets
Karen Okrainec, BSc, MScKaren Okrainec, BSc, MSc Department of Epidemiology and Biostatistics, McGill Department of Epidemiology and Biostatistics, McGill
University, Montreal, Quebec, CanadaUniversity, Montreal, Quebec, Canada Two of the eight trials that examined the Two of the eight trials that examined the effect of aspirin on graft occlusion found effect of aspirin on graft occlusion found aspirin to be beneficial when administered aspirin to be beneficial when administered within one day after CABG within one day after CABG
Considering Aspilets In Post CABG SurgeryConsidering Aspilets In Post CABG SurgeryDebate : How Early Give AspiletsDebate : How Early Give Aspilets
How about PJNHK?How about PJNHK?
Considering some research result above, some Considering some research result above, some policy must be discussed between practioners policy must be discussed between practioners and expert of therapy in PJNHK. Some how that and expert of therapy in PJNHK. Some how that considered by therapy on going CABG surgery.considered by therapy on going CABG surgery.
Thank YouThank You
REFERENCESREFERENCES
Antithrombotic Trialists' Collaboration Collaborative meta-analysis of Antithrombotic Trialists' Collaboration Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high-risk patients BMJ 2002;324:71-86.infarction, and stroke in high-risk patients BMJ 2002;324:71-86.[Abstract/Free Full Text][Abstract/Free Full Text]
ACC/AHA Task Force on Practice Guidelines Guidelines for coronary artery ACC/AHA Task Force on Practice Guidelines Guidelines for coronary artery bypass graft surgery J Am Coll Cardiol 1999;34:1262-1346.[Free Full Text]bypass graft surgery J Am Coll Cardiol 1999;34:1262-1346.[Free Full Text] Goldman S, Copeland J, Moritz T, et al. Long-term graft patency (3 years) after Goldman S, Copeland J, Moritz T, et al. Long-term graft patency (3 years) after coronary artery surgeryEffects of aspirin: results of a VA cooperative study. coronary artery surgeryEffects of aspirin: results of a VA cooperative study. Circulation 1994;89:1138-1143.[Abstract/Free Full Text] Circulation 1994;89:1138-1143.[Abstract/Free Full Text]
rooks N, Wright J, Sturridge M, et al. Randomised placebo controlled trial of rooks N, Wright J, Sturridge M, et al. Randomised placebo controlled trial of aspirin and dipyridamole in the prevention of coronary vein graft occlusion Br aspirin and dipyridamole in the prevention of coronary vein graft occlusion Br
Heart J 1985;53:201--207.[Abstract/Free Full Text]Heart J 1985;53:201--207.[Abstract/Free Full Text]
REFERENCESREFERENCESGavaghan TP, Gebski V, Baron DW. Immediate postoperative aspirin improves vein graft patency early and late after coronary artery bypass graft surgeryA placebo-controlled, randomized study. Circulation 1991;83:1526-1533.[Abstract/Free Full Text]
McEnany MT, Salzman EW, Mundth ED, et al. The effect of antithrombotic therapy on patency rates of saphenous vein coronary artery bypass grafts J Thorac Cardiovasc Surg 1982;83:81-89.[Abstract]
Sharma GV, Khuri SF, Josa M, Folland ED, Parisi AF. The effect of antiplatelet therapy on saphenous vein coronary artery bypass graft patency Circulation 1983;68:II218-21. Brown BG, Cukingnan RA, DeRouen T, et al. Improved graft patency in patients treated with platelet-inhibiting therapy after coronary bypass surgery Circulation 1985;72:138-146.[Abstract/Free Full Text]