Embed Size (px)
Citation preview

PTCA vs. CABGMERITS / DEMERITS / CHOICES
Dr. Rohan Gulabrao SonawaneResident (Internal Medicine)
Unit:Dr. V. P. Sinha
MD, DM ( Cardiology)

• INTRODUCTION
• PATIENTS SELECTION FOR REVASCULARIZATION
•WHAT IS PTCA
-Procedure- complication-Merits-Demerits
• WHAT IS CABG
- Procedure- Complication- Merits- Demerits
• CHOICES BETWEEN CABG/PTCA
• GUIDELINES
Ischemic heart disease is most commonly caused by obstruction to coronary
artery by atherosclerosis. IHD manifested as stable angina, chronic stable angina which
is progress to unstable angina/NSTEMI/STEMI. Principle for guiding patients
management on addressing following goal-
1) Use of disease modifying therapies or approaches to prolong life and reduce
major cardiovascular events such as acute MI hospitalization for ACS or HF.
2) Optimization of patients health status quality of life and functional
capacity such as angina or ischemia do not adversely affect the daily activity.
Revascularization approaches are an integral component of an overall
management strategy to improve outcome and are used when needed in addition to
optimal medical therapy.
INTRODUCTION --

PATIENTS SELECTION FOR REVASCULARIZATION :
1) Severity and presence of symptoms :Mechanical revascularization should be consider if ischemic
symptoms persist after optimization of medical therapy including strict riskfactor modification or if unacceptable side effect limit antianginal therapy.
2) Significance of coronary lesion:- presence of 70% or greater stenosis of an epicardial coronary
artery is consider to be a significant and 50% or greater for left maincoronary artery stenosis.
- for intermediate stenosis (50-70%) Fractional Flow Reserve (FFR) aninvasive physiological tool is used FFR < 0.80 (56%)is significant.

3) Anatomic consideration- Anatomical features:
- Vessel size- Extend of calcification- Tortuosity- Relationship with side branches
These characteristic may interfere revascularization success.
4) Extend of ischemia and presence of LV dysfunction :Major determinant of risk of CAD-
- Extend of ischemia- LV dysfunction- Electrical substrate- No. of vessels diseased
5) Risk of procedure: Elderly, sever underlying disease like hypertension, Diabetesmellitus, liver, lung or renal diseases.

PTCA (Percutaneous Transluminal Coronary Angioplasty)Percutaneous transluminal coronary angioplasty (PTCA) is a minimally invasive
procedure to open up blocked coronary arteries, allowing blood to circulate to the heartmuscle. It bypasses the culprit lesion but not the future culprit lesion.Devices currently in use:
- The Cutting balloon- Angioscore cathater
Patients selection for PTCA:1. The angiographic characteristics of the lesion for successful catheter based
revascularization2. The risk and potential consequences of acute failure of PTCA, which is depend
on the coronary artery anatomy (multivessel and/or diffuse disease), percentage of viablemyocardium at risk, presence of heart failure, and underlying LV function
3. The likelihood of restenosis, which has been associated with clinical (e.g.,diabetes, prior restenosis) and angiographic factors (e.g., small vessel diameter, long lesionlength, total occlusion, saphenous vein graft disease)

4. The need for complete revascularization based on the extent of CAD, volume ofmyocardium, and severity of ischemia in the distribution of the artery(ies) amenable toPTCA.
A successful balloon angioplasty is defined as the reduction of a minimumstenosis diameter to <50% with a final TIMI flow grade 3 (visually assessed by angiography)without side branch loss, flow-limiting dissection, or angiographic thrombus.

PTCA IN SUBGROUP OF PATIENTS:1. Diabetes mellitus: patietns with DM has higher risk for complication
after PTCA due to altered biology of vessels. Restenosis is more frequent in DMpatients with IHD after PTCA.
2. LV dysfunction: LV dysfunction is associated with higher in hospitaland long term mortality after PTCA.
3. Previous CABG: patients who have had CABG and later have recurrentischemia undergo revascularization with PTCA.
4. Renal insufficiency: mortality and morbidity with PTCA is related torenal disease. Contrast used during PTCA causes contrast induced nephorpathywhich is depends on dose of contrast used, hydration status of patients and pre-existing renal function.
OTHER CORONORY DEVICES
Coronary stenting:1. Bare metal stents: provide a mechanical framework that
holds the artery wall open, preventing stenosis, or narrowing, ofcoronary arteries.
2. Drug eluting stents: stents coated with drugs,These typesof stents have been shown to help prevent restenosis of the arterythrough several different physiological mechanisms, which relyupon the suppression of tissue growth at the stent site and localmodulation of the body's inflammatory and immune responses. Fivedrugs, umirolimus, zotarolimus, sirolimus, everolimus, andpaclitaxel.

Coronary Atherectomy:1. The most commonly used atherectomy device is Rotational
coronary atherectomy, which removes the atheromatous plaque bythe abrasion of inelastic calcified plaque using microscopic (20 to50 microm) diamond chips on the surface of a rapidly rotating(160,000 rpm) olive-shaped atherectomy burr. This abrasiongenerates 2- to 5 microm particles that pass through the coronarymicrocirculation for removal by the reticuloendothelial system.
2.Thrombectomy and Aspiration Devices:The AngioJet rheolytic thrombectomy catheter was
used for thrombus removal through the dissolution and aspirationof the thrombus.

3. Embolic Protection Devices:I) Distal Occlusion Devices : The GuardWireII) Distal Embolic Filters : Distal filters are advanced
across the target lesion in their smaller collapsed state, and aretaining sheath is withdrawn, allowing the filters to open and toexpand against the vessel wall. The filters then remain in place tocatch any liberated embolic material larger than the filter pore size(usually 120 to 150 ?m) during intervention.
III) Proximal Occlusion Devices: Two proximalocclusion devices are currently in use: the Proxis catheter andKerberos embolic protection system.



Factors associated with Early failure and complication after PTCA:1. Clinical variables: -women
-advanced age- DM.- unstable angina- CHF- Cardiogenic shock- Renal insufficiency-Preprocedural instability requiring intra aortic balloon pump support
- Multivessels coronary disease
2. Anatomic variability: - Multivessels CAD- Left main CA- Thrombus- Chronic total coronary occlusion
3. Procedural factors: - A higher final percentage diameter stenosis- Smaller minimal lumen diameter- Presence of a residual dissection or trans-stenotic
pressure gradient

Factors associated with Early mortality after PTCA:1. Clinical Variables :
Advanced ageFemale genderDiabetes mellitusChronic lung diseasePrior myocardial infarctionImpairment of left ventricular functionRenal dysfunctionCardiogenic shockSalvage, urgent, or emergent PCI
2. Anatomic Variables :Multivessel CADLeft main diseaseProximal left anterior descending diseaseLarge area of myocardium at riskPCI of artery supplying collaterals to large artery
COMPLICATIONS PTCA• Hematoma at insertion site
• Pseudoaneurysms
• Embolism
• Hypersensitivity to Dye
• Re-stenosis, immediately or 3-6 mo’s
• Dysrhythmias
• Vessel rupture, need for emergent CABG
• Angina, MI, and Vasospasm
• Abrupt closure of dilated segment.
• Coronary artery dissection

MERITS OF PTCA
1. Less expenssive
2. Performed during same clinical encounter as the diagnostic angiography
3. Stable patient can be discharge on same day of the procedure or next day
4. Clinical recovery is complete with in a week or less
5. Symptomatic relief can be immediate and dramatic.
6. On table mortality or morbidity is less marked
7. It can be used as a rescue procedure in previously CABG patients

DEMERITS OF PTCA1. Restenosis is the most common complication of PTCA.
2. It is related to high incidence of incomplete revascularization.
3. Relatively inefficacy in patients with severe left ventricular dysfunction.
4. Less favorable outcome in diabetes patients due to altered vascular biology.
5. Limited to specific anatomic subsets like tortusity, side branches and vessel diameter.
6. It is not suitable for chronic total occlusion due to failure of guide wire recanalizatiom
7. Lesion calcification: presence of extensive coronary calcification makes the procedure
more difficult because calcium in the vessel wall leads to irregular and inflexible lumens
and makes the delivery of guide wire, balloon and stents much more challenging.
8. Thrombus: large coronary thrombus may fragment and embolise during PTCA which
may hightens risk of procedural complication.

9. Hypersensitivity to dye limits the use of PTCA
10. Rupture of the vessels causes profuse bleeding and hematomas
11. Coronary perforation or dissection causing periprocedural MI, cardiac tamponade,
hemodynamic collapse
12. No-reflow, defined as reduced antegrade perfusion in the absence of flow limiting
stenosis
13. PTCA related MI: Increases of biomarkers >3 times the 99th percentile upper reference
limit were designated as defining PCI-related MI
CABG (Coronary Arterial Bypass Grafting)
Coronary artery bypass graft is the surgical technique which usessaphenous leg veins as grafts (SVG) or the internal mammary arterygastroepiploic/radial arteries as grafts to bypass obstructed portions of a coronaryartery. The current standard for bypass grafting advocates routine use of the leftIMA for grafting the LAD artery, with supplemental saphenous vein grafts toother vessels. It bypasses culprit as well as future culprit lesion.There are four types:
1) port access CABG using limited incision with femoral – femoral cardio-pulmonary bypass and cardiolegic arrest.
2) totally endoscopic robotically assisted CABG on arrested heart.3) Off pump CABG using standard median sternotomy with generally
small skin incision and stabilization device to reduce motion of a target vesselwhile anostomosis is performed without cardio-pulmonary bypass.
4) Minimally invasive direct CABG through left anterior thoracotomywithout cardio- pulmonary bypass.

CABG is also classified as single bypass means single coronary aretry, doublebypass means two coronary arteries are bypassed (e.g. the left anterior descending (LAD)coronary artery and right coronary artery (RCA)); a triple bypass means three vessels arebypassed (e.g. LAD, RCA, left circumflex artery (LCX)); a quadruple bypass means fourvessels are bypassed (e.g. LAD, RCA, LCX, first diagonal artery of the LAD) and so on.


Patency of graft depends on :1. Distal vasculature2. Diameter of coronary artery onto which graft is
inserted- higher graft patency rates are found when Lumina ofvessel onto which graft is inserted are greater than 1.5 mm indiameter.
3. Size of a distal vascular bed- highest rates with profusedistal vascular bed
4. Severity of coronary atherosclerosis distal to graftinsertion- distal arteries are free from athroma obstructing morethan 25% of vessel lumen.

COMPLICATION OF CABG:-Post-perfusion syndrome: a transient neurocognitive impairment associated withcardiopulmonary bypass. the incidence is decreased by off-pump coronary artery bypass,but with no difference beyond three months after surgery.
-Myocardial infarction: due to embolism, hypoperfusion, or graft failure. Elevation of the myocardial creatine kinase-MB (CK-MB) isoenzyme level more than five times the upper limit of normal is commonly considered diagnostic of MI.
- Atrial fibrilation: This arrhythmia is the most frequent complications of CABG. It occursin up to 40% of patients, primarily within 2 to 3 days. Prophylactic use of beta blockersreduces the frequency of postoperative atrial fibrillation; these should be administeredroutinely before and after CABG to patients without contraindications.
-Late graft stenosis, particularly of saphenous vein grafts due to atherosclerosis causingrecurrent angina or myocardial infarction.
-Acute renal failure due to embolism or hypoperfusion.
-Stroke secondary to embolism or hypoperfusion.
-Pneumothorax: An air collection around the lung that compresses the lung
-Hemothorax: Blood in the space around the lungs
-Pericardial tamponade: Blood collection around the heart that compresses the heart andcauses poor body and brain perfusion. Chest tubes are placed around the heart and lung toprevent this.
-Pleural effusion: Fluid in the space around the lungs. This can lead to hypoxia which canslow recovery.
-Vasoplegic syndrome, secondary to cardiopulmonary bypass and hypothermiaGrafts last 8–15 years, and then need to be replaced.

MERITS OF CABG
1. More effective in relieving symptoms of angina due to bypassing of future culprit lesion.
2. Can be performed in diabetes patients in which PTCA is ineffective due to restenosis.
3. It has the ability to revascularize the artery completely.
4. It has no limitation for anatomic subset like vessel diameter, side branches.
5. It is most preferred procedure for multivessel CAD disease, left main CAD.
6. It has no limitation over total artery occlusion, thrombus and lesion calcification.
7. It relieves symptoms dramatically in patients with co morbidities like LV dysfunction,
renal in sufficiency, hypertension.
8. Patients with more extensive and severe CAD have an increasing magnitude of benefit
from CABG
9. It has better outcome in patients with age > 65 yr
DEMERITS OF CABG1. Procedure is costly2. postoperative patient discomfort which is minimized by minimally invasive
CABG3. risk of wound infection4. Longer recovery times but this complication is minimized by Minimally
invasive CABG.5. With use of Cardio-pulmonary bypass result in the risk of bleeding, systemic
thromboembolism, renal insufficiency, myocardial stunning, stroke, cognitiveimpairment, particularly in older patients and patients with heavily calcifiedaortas which can be minimized by using Off pump techniques where cardio-pulmonary bypass is not used and procedure is performed on beating hear
6. It has very life threatening complication like hemothorax, pneumothorax,cardiac tamponade

7. Renal insufficiency: mortality and morbidity is increased in patients withimpaired renal function. Patients with evidence of renal dysfunction have a 20%higher risk of death after 1 year of procedure.
8. Reoperation for restenosis is more cumbersome
9. Periprocedural rate of stroke is high in CABG

HYBRID REVASCULARIZATION
This technique is still under study which consist ofcombining CABG with PTCA . Minimally invasive CABG on LADcoronary artery with left IMA implant to LAD artery using Off-pump CABG with PCI on remaining vessels.
Hybrid coronary revascularization may be performed in ahybrid suite in one operative setting or as a staged procedure ie PCIand CABG performed in 2 different operative suites, separated byhours to 2 days, but typically during the same hospital stay.

Choosing Among PTCA and CABG1. Single-Vessel Disease:
In patients with single-vessel disease in whom revascularization is deemed necessary and the lesion is anatomically suitable, PCI is almost always preferred over CABG.
2. left main CAD: CABG is most preferred method for revascularization than PTCA
3. Multivessel disease: -There are no difference in late mortality and MI between the
two, PTCA can be used provided that the patient accepts the distinct possibility of symptom recurrence and need for repeat revascularization.
- Patients with a single localized lesion in each affected vessel and preserved LV function fare best with PCI.
- For patients with left main CAD or severe triple-vessel CAD and LV dysfunction, CABG is generally the best approach.

4. Patients with UA/NSTEMI:- An early invasive strategy is now recommended in patients with
UA/NSTEMI who have ST-segment changes or positive troponin on admission or who evolve these high-risk features during the subsequent 24 hours.
- High-risk indicators, such as recurrent ischemia and evidence of congestive heart failure, are also indications for an early invasive strategy.
- Patients present with UA/NSTEMI within 6 months of a prior PCI and in whom restenosis may be the cause.
- Indicated in patients with UA/NSTEMI with prior CABG.Types:
1.Immediate invasive strategy with an average time of only 2 hours 2. A delayed invasive strategy, in which the average time to
catheterization was 4 days.
Percutaneous Coronary Intervention versus Coronary Artery Bypass Grafting: -CABG is recommended for patients with disease of the left main coronary artery
as well as for those with multivessel disease and impaired left ventricular function or diabetes mellitus. PCI associates with a slightly lower initial morbidity and mortality than CABG, but there is a higher need of repeated PCI.


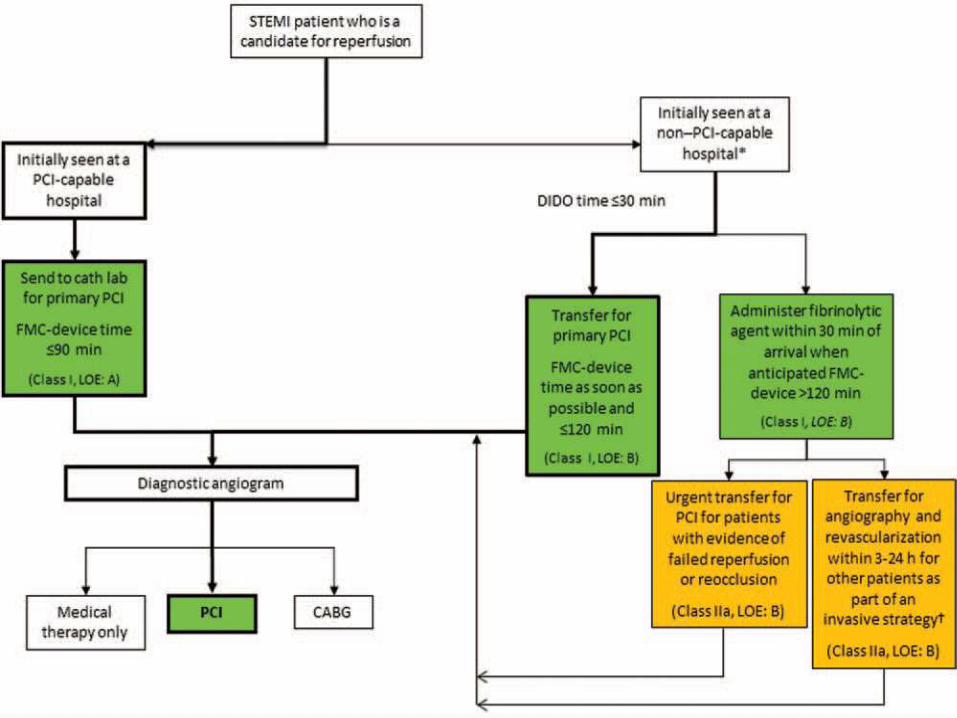
5. Patients with STEMI: PTCA or CABG is performed as an alternative to thrombolytic therapy in STEMI. If-Door to balloon time is < 90 min- PTCA can be performed if FMC to device time < 120 min or if its >120
min patient is thrombolise and then send for PCI after 3-24 hours period.- Angioplasty can be performed with in 12 hours- PTCA is preferred over thrombolysis in patients with:
- Age <75 yr- Cardiogenic shock in < 36 hrs of MI- High risk of death or development of HF- Contraindication to thrombolysis- post CABG or recent PCI
- CABG is preferred in patients with:- Coronary anatomy is not amenable to PCI like multivesssl
CAD, tortuous CA, Left main CAD- Failed PCI- Presence of cardiogenic shock after 36 hrs of MI- If patients has refractory ischemia

6. Need for Complete Revascularization:-Complete revascularization is an important goal for patients with LV
dysfunction and/or multivessel CAD.- Patients with chronic total coronary occlusion, LV dysfunction, or left
main CAD, CABG is the procedure of choice.- In patients with borderline LV function (EF from 0.40 to 0.50) and
milder degrees of ischemia, PTCA may provide adequate revascularization.
In many patients, either method of revascularization is suitable. Other factors to be considered include the following:
- Access to a high-quality team and operator .
- Patient preference- Some patients are reluctant to remain at risk for symptom recurrence and reintervention; these patients are better candidates for surgical treatment.
- Advanced patient age and comorbidity- Much older patients and those with comorbid conditions are often better candidates for PTCA.
- Younger patient age-PTCA is also often preferable for younger patients (<50 years), with the expectation that they may require CABG at some time in the future and that PCI will postpone the need for surgery.

7. Patients with Diabetes :BARI (Bypass Angioplasty Revascularization Investigation) and ATRS trial shows
poorer outcomes after PTCA than after CABG in treated diabetic patients . In the BARI 2D, current evidence supports CABG as the preferred revascularization strategy for patients with DM. A potential advantage is that bypass grafts to the mid-coronary vessel both treat the culprit lesion and may afford prophylaxis against new proximal disease progression, whereas stents only treat suitable stenotic segment(s), with no benefit against the development of new disease

8. Renal disease:Patients with renal disease is at greater risk for mortality and morbidity
due to both PTCA and CABG, but observational data has suggested that in patients with chronic dialysis CABG is preferred strategy for revascularization over PTCA.9. Women:
Women are less likely than men to be referred for coronary angiography and subsequent revascularization. Women are more sicker with respect to there male counterparts but there are similar long term outcome after surgical revascularization , gender should not be a significant factor in dicisons choosing between CABG and PTCA.10. Previous CABG:
In the patient with previous CABG who is referred for revascularization for medically refractory ischemia,
-choice of repeat CABG include vessels unsuitable for PCI, number of diseased bypass grafts, availability of the internal mammary artery for grafting, chronically occluded coronary arteries, and good distal targets for bypass graft placement.
-Factors favoring PCI over CABG include limited areas of ischemia causing symptoms, suitable PCI targets, a patent graft to the LAD artery, poor CABG targets, and comorbid conditions.
11. Older patients: Age is one of the strongest predictors of mortality, and elderly
patients present with a substantially higher clinical risk profile, the angiographic success rates and clinical benefits of PCI in elderly patients are similar to younger patients. However, increased risks of complications such as major bleeding and stroke mandate careful consideration of the benefits and risks of PTCA and CABG in elderly patients.
12 Patients who survived sudden cardiac death: CABG is preferred over PCI.
ACC/AHA GUIDELINES



Left Main CAD RevascularizationClass I
CABG to improve survival is recommended for patients with significant (>50% diameter stenosis) left main coronary artery stenosis.
(Level of Evidence: B)Class IIa
1. PCI to improve survival is reasonable as an alternative to CABG in selected stable patients with significant (>50% diameter stenosis) unprotected left main CAD with:
A) anatomic conditions associated with a low risk of PCI procedural complications and a high likelihood of good long-term outcome
B) clinical characteristics that predict a significantly increased risk of adverse surgical outcomes (Level of Evidence: B)
2. PCI to improve survival is reasonable in patients with UA/NSTEMI when an unprotected left main coronary artery is the culprit lesion and the patient is not a candidate for CABG.(Level of Evidence: B)
3. PCI to improve survival is reasonable in patients with acute STEMI when an unprotected left main coronary artery is the culprit lesion, distal coronary flow is less than TIMI (Thrombolysis In Myocardial Infarction) grade 3, and PCI can be performed more rapidly and safely than CABG.(Level of Evidence:C)
Class IIb1. PCI to improve survival may be reasonable as an alternative to CABG in selected stable
patients with significant (>50% diameter stenosis) unprotected left main CAD with: A) anatomic conditions associated with a low to intermediate risk of PCI
procedural complications and an intermediate to high likelihood of good long-term outcome
B) clinical characteristics that predict an increased risk of adverse surgical outcomes (eg, moderate-severe chronic obstructive pulmonary disease, disability from previous stroke, or previous cardiac surgery; STS-predicted risk of operative mortality >2%)(Level of Evidence: B)
Class III: HARM1. PCI to improve survival should not be performed in stable patients with significant (>50% diameter stenosis) unprotected left main CAD who have unfavorable anatomy for PCI and who are good candidates for CABG.(Level of Evidence: B)

Non–Left Main CAD RevascularizationClass I1. CABG to improve survival is beneficial in patients with significant (>70% diameter) stenoses in 3 major coronary arteries (with or without involvement of the proximal left anterior descending [LAD] artery) or in the proximal LAD plus 1 other major coronary artery.(Level of Evidence: B)
2. CABG or PCI to improve survival is beneficial in survivors of sudden cardiac death with presumed ischemia-mediated ventricular tachycardia caused by significant (>70% diameter) stenosis in a major coronary artery.(CABG Level of Evidence: B;PCI Level of Evidence: C)
Class IIa1. CABG to improve survival is reasonable in patients with significant (>70% diameter)
stenoses in 2 major coronary arteries with severe or extensive myocardial ischemia (eg,high-risk criteria on stress testing, abnormal intracoronary hemodynamic evaluation, or >20% perfusion defect by myocardial perfusion stress imaging) or target vessels supplying a large area of viable myocardium.(Level of Evidence: B)

2. CABG to improve survival is reasonable in patients with mild-moderate left ventricular (LV) systolic dysfunction (ejection fraction [EF] 35% to 50%) and significant (>70% diameter stenosis) multi-vessel CAD or proximal LAD coronary artery stenosis, when viable myocardium is present in the region of intended revascularization.(Level of Evidence:B)
3. CABG with a left internal mammary artery (LIMA) graft to improve survival is reasonable in patients with significant (>70% diameter) stenosis in the proximal LAD artery and evidence of extensive Ischemia.(Level of Evidence: B)
4. It is reasonable to choose CABG over PCI to improve survival in patients with complex 3-vessel CAD with or without involvement of the proximal LAD artery who are good candidates for CABG.(Level of Evidence:B)
5. CABG is probably recommended in preference to PCI to improve survival in patients with multivessel CAD and diabetes mellitus, particularly if a LIMA graft can be anastomosed to the LAD artery.(level of Evidence: B)
Class IIb1. The usefulness of CABG to improve survival is uncertain in patients with significant (>70%) diameter stenoses in 2 major coronary arteries not involving the proximal LAD artery and without extensive ischemia.(Level of Evidence: C)2. The usefulness of PCI to improve survival is uncertain in patients with 2- or 3-vessel CAD (with or without involvement of the proximal LAD artery) or 1-vessel proximal LAD disease.(Level of Evidence: B)3. CABG might be considered with the primary or sole intent of improving survival in patients with SIHD with severe LV systolic dysfunction (EF <35%) whether or not viable myocardium is present.(Level of Evidence: B)4. The usefulness of CABG or PCI to improve survival is uncertain in patients with previous CABG and extensive anterior wall ischemia on noninvasive testing.(Level of Evidence: B)Class III: HARM1. CABG or PCI should not be performed with the primary or sole intent to improve survival in patients with SIHD with 1 or more coronary stenoses that are not anatomically or functionally significant (eg, <70% diameter non–left main coronary artery stenosis, FFR >0.80, no or only mild ischemia on noninvasive testing), involve only the left circumflex or right coronary artery, or subtend only a small area of viable myocardium.(Level of Evidence: B)

Revascularization to Improve Symptoms With Significant Anatomic (>50% Left Main or >70% Non–Left Main CAD) or Physiological (FFR <0.80) Coronary Artery
Stenoses

Indications for PCI in STEMI

Indications for PCI of an Infarct Artery in PatientsWho Were Managed With Fibrinolytic Therapy or Who Did Not
Receive Reperfusion Therapy

CABG in Patients With STEMIClass I1. Urgent CABG is indicated in patients with STEMI and coronary anatomy not amenable to PCI who have ongoing or recurrent ischemia, cardiogenic shock, severe HF, or other high-risk features.(Level of Evidence: B)2. CABG is recommended in patients with STEMI at time of operative repair of mechanical defects.(Level of Evidence: B)Class IIa1. The use of mechanical circulatory support is reasonable in patients with STEMI who are
hemodynamically unstable and require urgent CABG.(Level of Evidence: C)Class IIb1. Emergency CABG within 6 hours of symptom onset may be considered in patients with
STEMI who do not have cardiogenic shock and are not candidates for PCI or fibrinolytic therapy.
(Level of Evidence: C)


Postprocedural Recommendations for Patients Undergoing PCI

CABG PCI
NO DIABETES AND NORMAL
LVEFDIABETES
DEPRESSED LVEF
NO DIABETES AND NORMAL
LVEFDIABETES
DEPRESSED LVEF
Two-vessel coronary artery
disease with proximal LAD
stenosis
A A A A A A
Three-vessel coronary artery
diseaseA A A U U U
Isolated left main stenosis
A A A I I I
Left main stenosis and additional
coronary artery disease
A A A I I I
ACC/AHA Appropriateness Ratings for Type of Revascularization

Hybrid Coronary Revascularization:Class IIa1. Hybrid coronary revascularization (defined as the planned combination of LIMA-to-LAD artery grafting and PCI of >1 non-LAD coronary arteries) is reasonable in patients with 1 or more of the following(Level of Evidence: B):
a. Limitations to traditional CABG, such as heavily calcified proximal aorta or poor target vessels for CABG (but amenable to PCI);
b. Lack of suitable graft conduits;
c. Unfavorable LAD artery for PCI (ie, excessive vessel tortuosity or CTO).
Class IIb1. Hybrid coronary revascularization may be reasonable as an alternative to multivessel PCI or CABG in an attempt to improve the overall risk benefit ratio of the procedures.(Level of Evidence: C)






























