Embed Size (px)
Citation preview

Acute Respiratory Distress Syndrome
Dr. Eric Mugambi

Historical perspective
1821 – Laennec in ‘A treatise on
diseases of the chest’
Idiopathic anasarca of the lungs
Trauma associated
World war 1 & 2
Vietnam war

Historical perspective
1950s - Advances in critical care
Respirators
Airway access
Hence the term ‘respirator lung’
Other terms related to inciting agent
Post-traumatic, shock lung, wet lung,
DaNang lung)

Historical perspective
1967 – Case series of 12 patients
acute onset
tachypnœa
hypoxæmia
loss of compliance
Ashbaugh D, Boyd Bigelow D, Petty T, Levine B. ACUTE RESPIRATORY DISTRESS IN ADULTS. The Lancet. 1967;290(7511):319-23.

Defining features
Hypoxemia
Low Pa02
Stiff lungs
Reduced compliance
Hyaline membranes
Early fibrosis in patients who died

Epidemiology
Not well characterized due to lack of uniform diagnosis
Before ICUs – most patients died No opportunity for organized
investigations US data
50,000 to 200,000 cases per year (2003) 79/100,000 – ALI 59/100,000 – ARDS 4-9% in ICU settings

Epidemiology
Substantial recovery in lung function occurs within 6-12 months In few cases muscle weakness and neuropsychiatric
problems may persist
Mortality has improved significantly from 54% in 1983 to as low as 25% in 2004 but has plateaued since then Better prognosis with younger age
Leading cause of death is multiple organ failure

Definitions
1967 – Ashbaugh et al
1988 – Murray and colleagues
1992 – American European Consensus Conference (AECC)
2012 – Berlin definition

AECC (1994)
1. Acute onset of respiratory failure
2. Bilateral infiltrates resembling pulmonary
edema
3. No evidence of left atrial pressure elevation -
PCWP <18mmhg
4. Ratio of PaO2 to FiO2 is <200mmhg –
ALI – 200<PaO2/FiO2 < 300mmHg (Desaturation)

“Acute lung injury” no longer exists
Onset of ARDS (diagnosis) must be acute, as defined as within 7 days of some defined event, which may be sepsis, pneumonia, or simply a patient’s recognition of worsening respiratory symptoms.
The Berlin definition
The ARDS Definition Task Force: JAMA. 2012;307(23):2526-2533. doi:10.1001/jama.2012.5669.

Berlin definition
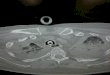
Bilateral opacities consistent with pulmonary edema must be present but may be detected on CT or chest X-ray.

There is no need to exclude heart failure in the new ARDS definition An “objective assessment“– meaning
an echocardiogram in most cases — should be performed if there is no clear risk factor present like trauma or sepsis.
Berlin definition
The ARDS Definition Task Force: JAMA. 2012;307(23):2526-2533. doi:10.1001/jama.2012.5669.

Hypoxemia

Cause of hypoxemia
Hypoventilation
Ventilation perfusion mismatch
Right to left shunt
Diffusion impairment
Reduced inspired oxygen tension
(Pio2)
Very low cardiac output

Etiology
Common causes (mnemonic PAST) Pneumonia Aspiration Shock Sepsis Trauma *Transfusion (multiple)

Other causes
Lung Contusion Near drowning Inhalational injury Reperfusion pulmonary edema
Other Cardio-pulmonary bypass Drug overdose Acute pancreatitis (alcohol increases risk!) Transfusion of blood products

Pathophysiology
Endothelial injury Increased vascular permeability – hallmark
Epithelial disruption Alveolar flooding Disorganized repair leads to fibrosis Septic shock in patients with bacterial
pneumonia Loss of type 2 cells
Impaired fluid transit – no fluid removal Loss of surfactant Loss of type 1 progenitor cells

Consequences
Impaired gas exchange leading to severe hypoxemia - 2/2 ventilation-perfusion mismatch, increase in physiologic dead space
Decreased lung compliance – due to the stiffness of poorly or non-aerated lung
Pulm HTN – 25% of pts, due to hypoxic vasoconstriction, Vascular compression by positive airway compression, airway collapse and lung parenchymal destruction




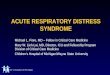
Normal BGB

Small bronchiole and alveolae

Alveoli and capillaries


Clinical Presentation
Acute onset within 12-36 hrs of inciting event, upto 5-7days
Dyspnoea, tachypnoea, hypoxemia, dry cough chest pain
O/E: tachycardia, cyanosis, tachypnoea, diffuse rales,
BGAs: resp alkalosis, hypoxemia
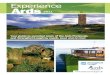
CXR: bilateral alveolar infiltrates over 75% of lung fields
No pulm venous congestion, no kerley b lines, no cardiomegaly, pleural effusions



Differential diagnoses
1. Pneumonia
2. Diffuse alveolar hemorrhage
3. Idiopathic acute eosinophilic pneumonia
4. Cryptogenic organising pneumonia
5. Acute interstitial pneumonia
6. Rapidly progressive cancer
7. Cardiogenic pulmonary edema

Management
Investigations Guided by clinical suspicion of
underlying illness (ddx) For monitoring progress in patients with
critical illness▪ Routine e.g. ABGs▪ Tests of Organ function

Management
Treat underlying illness
Minimize procedures
Prevent complications
Barotrauma
DVT
Stress ulcers
Promptly recognize nosocomial infections
Provide adequate nutrition

Therapies in ARDS
THERAPY RECOMMENDATION
Low tidal volume A (strong evidence from RCTs)
Minimize left atrial filling pressures
B (limited clinical data)
High PEEP C (recommended only as alternative)
Prone positioning C
Recruitment maneuvers C
ECMO C
High frequency ventilation D (Not recommended)
Glucocorticoids D
Surfactant, Inhaled NO, other anti-inflammatory
D

The future
Gene therapy Mesenchymal stem cells

Consequences
Impaired gas exhange leading to severe hypoxemia - 2/2 ventilation-perfusion mismatch, increase in physiologic deadspace
Decreased lung compliance – due to the stiffness of poorly or nonaerated lung
Pulm HTN – 25% of pts, due to hypoxic vasoconstriction, Vascular compression by positive airway compression, airway collapse and lung parenchymal destruction